")
Back to Journals » Open Access Emergency Medicine » Volume 14
Portrait of the Emergency Department at Orotta National Referral and Teaching Hospital in Asmara, Eritrea: A Prospective Observational Study
Authors Mengistu ST , Achila OO , Negash ST, Tesfaldet Y, Tewolde NY, Yohannes NA, Embaye PT, Yemane F, Abraha B, Hagos G, Tewolde Y
Received 20 December 2021
Accepted for publication 6 April 2022
Published 28 April 2022 Volume 2022:14 Pages 195—215
DOI https://doi.org/10.2147/OAEM.S352638
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Samuel Tekle Mengistu,1 Oliver Okoth Achila,2 Simon Tesfay Negash,3 Yonathan Tesfaldet,4 Naod Yeibyo Tewolde,5 Nahom Asmerom Yohannes,6 Peniel Tsehaye Embaye,7 Fanus Yemane,3 Beyene Abraha,7 Goitom Hagos,8 Yoseph Tewolde9
1Nakfa Hospital, Ministry of Health Northern Red Sea Branch, Nakfa, Eritrea; 2Department of Clinical Laboratory Sciences, Orotta College of Medicine and Health Sciences, Asmara, Eritrea; 3Adi Keih Hospital, Adi-Keih, Eritrea; 4Akurdet Hospital, Akurdet, Eritrea; 5Ghindae Hospital, Ghindae, Eritrea; 6Gedem Naval Hospital, Gedem, Eritrea; 7Department of Clinical Sciences, Orotta College of Medicine and Health Sciences, Asmara, Eritrea; 8Department of Internal medicine, Orotta College of Medicine and Health Sciences, Asmara, Eritrea; 9Department of Surgery, Orotta College of Medicine and Health Sciences, Asmara, Eritrea
Correspondence: Samuel Tekle Mengistu, General Practitioner, Nakfa Hospital, Northern Red Sea Ministry of Health, Nakfa, P.O. Box - 5659, Asmara, Eritrea, Tel +2917535772, Email [email protected]
Background: Provision of high-quality emergency care for acute, life-threatening illnesses can significantly reduce DALY and mortality in sub-Saharan Africa. Here, we present data on the profile of an Emergency Department (ED) in the largest referral hospital in Eritrea and potential gaps for intervention.
Patients and Methods: This was a prospective single-center observational study of 1093 patients who presented to the ED between September and October of 2020. Data were collected using a questionnaire from the patients’ interview, observation and medical record review. The data were summarized using descriptive statistics and where applicable logistic regressions were performed.
Results: The median age was 45.0 years among the patients. In terms of acuity, 741 (68.5%), 283 (26.2%), 48 (4.4%), 10 (0.9%) patients were triaged as green, yellow, red, and black, respectively. In addition, the number of self-referred patients was 857 (79.1%) and among all the visitors, 376 (34.9%) used Ambulance service. The median ± IQR for ED length of stay (LOS) was 2.7 (1.4– 10.0) Hours. Further, 154 (14.4%) patients stayed in the ED for > 24 hours. The hospitalization rate was 146 (14.7%). In the multivariate analysis, higher likelihood of prolonged ED LOS was observed in: medical department patients (aOR = 3.53, 95% CI = 2.03– 6.14); patients referred from primary health-care centers (aOR = 2.63, 95% CI = 1.10– 6.30) and hospital (aOR = 3.70, 95% CI = 2.15– 6.37). Prolonged ED LOS was also associated with prior emergency visit (aOR = 1.96, 95% CI = 1.13– 3.40); consultation (aOR = 12.27, 95% CI = 6.98– 21.56); the need for inpatient admission (aOR = 2.34, 95% CI = 1.38– 3.96); and the need for investigation and treatment (aOR = 2.03, 95% CI = 1.07– 3.85).
Conclusion: Improvements regarding ED specialist personnel, inpatient ward capacity, availability of investigations throughout the day and night shifts, amendments in referral system, strengthening ED and critical care capacity in zonal referral hospitals, and access to quality care among the non-communicable disease patients may ameliorate most of the bottlenecks observed in this set-up.
Keywords: emergency department, ED LOS, emergency medical services systems, Eritrea, Sub-Saharan Africa, chief complain
Introduction
Recent attention has highlighted the need for effective emergency medical care services (EMS) in low- and middle-income countries (LMIC).1 For instance, some studies have suggested that 54% (24,300,000/45,000,000) of deaths in LMICs could be mitigated by expanding or improving pre-hospital and facility-based emergency care systems.2 This finding was reiterated by the Disease Control Priorities in Developing Countries project report which suggested that 45% of mortality and 36% of Disability-Adjusted Life Years (DALYs) in LMIC can be prevented by high-quality emergency care.3 The importance of ED is also underscored by the World Health Organization (WHO) argument that expanding and integrating EMS into existing public health and primary care services is a fundamental priority for healthcare service improvement globally4 – a 2019 World Health Assembly resolution on emergency care (WHA72.16) indicated that emergency care is
An essential component of quality care and that millions of deaths and long-term disabilities could be prevented if emergency care exist and patients reach them in time.4
Although the importance of EMS is well documented;5 services in sub-Saharan Africa (SSA) have been described as overstretched and overburdened.6 Emphasizing this point, some investigators have noted that these systems are not only under-developed;7,8 they also lack surge capacity and resilience.5 Fundamental barriers include a high volume of critically ill patients – even in non-crisis situations; a general shortage of essential equipment and supplies; inadequate manpower (EM specialists) and under-developed research infrastructure and capacity – the limited research that exists has been described as small, ad hoc efforts, in individual facilities.5
These factors work in isolation or in concert to undermine the functioning of EDs in LMICs in multiple ways. These include high mortality – median mortality within EDs in LMIC was approximately 1.8% (IQR 0.2–5.1%);5 overcrowding of facilities, increased workload, staff frustration, delayed medical evaluation at triage, poor quality of care, poor patient’s outcome, non-compliance with treatment guidelines, provider errors, inadequate inpatient capacity, increased chance of avoidable and costly hospital readmissions, among others.2,9 Additionally, unpredictable fluctuations in demand and supply that are often experienced in LMICs may undermine accurate modeling of future demand and workload. In turn, this may undermine staff scheduling and resource allocation or reallocation.10 Another impactful factor that complicates the situation in ways that may not be apparent to the casual observer is the fact that the application of care guidelines from high-income countries (HICs) to LMICs is hindered by the paucity of data and heterogeneity of practices.7,11 According to some authors, the differences in epidemiology, organization, and practices observed in LMICs suggest that enhance research output can make EDs more effective and responsive.7,12
Without a doubt, most of the barriers highlighted in the foregoing paragraph can be addressed by improvement in data collection practices and high-quality research on EMS. This was indeed, the goal of the Collaborative for Enhancing Emergency Care Research in LMICs (CLEER) project. The WHO4 and the African Federation for Emergency Medicine have persistently called for continued and broadened research.2 Multiple research themes have been suggested including the need for national or regional data on acute care delivery systems;8,13 specific emergency disease burdens, factors that drive patients to seek care in EDs;5 and resource availability and emergency service delivery structure7 or mortality patterns across the acute care continuum.2 Focus on chief complaints or ED syndromic surveillance is predicated on the realization the information may enhance preparedness/situational awareness and disease control capabilities particularly when intra-country and inter-country comparisons are undertaken.8,13 Data on arrival and throughput, including daily or seasonal patterns of patient flows, can also inform resource allocation, staffing and the development of locally relevant interventions.
Here, we have undertaken the first descriptive analysis ofa functioning ED in Eritrea. In the process, we draw attention to the magnitude and factors associated with prolonged ED length of stay (ED bottle necks) and predictors of hospitalization. It is our opinion that this study provides vital information that can be used to identify disease patterns in the country, refine triaging strategies, or training ED personnel, among others. The data can also be pooled for a better understanding of multiple themes on EMS across SSA.
Patients and Methods
Study Area
Eritrea is a country in East Africa with a land area of 124,000 square kilometers. The country has a population of 5.7 million inhabitants. Health care is delivered through a three-tiered system of hospitals stratified into primary, secondary, and tertiary health-care facilities. Primary health care is provided through a network of some community hospitals, health centers, health stations, and community-based health services providing basic services including; antenatal care, Extended program of immunization, and Integrated management of childhood illness. They contain few beds for acute care as they are most distant from secondary level services. Community-based health services have coverage of an estimated 2000 to 3000 people. They provide services by empowering communities, mobilizing and maximizing resources via Community Health Workers (CHA) under the leadership of the Village Health Committee. Health stations (HS) offer facility-based primary health-care services to a catchment population of approximately 5000–10,000 and it is staffed by nurses, associate nurses, and laboratory technicians. Currently, there are around 170 HS in the country. HS is accountable to the nearest health center (around 52 health centers exist up today). Community Hospital is the referral facility for the primary health-care level of service delivery serving a community of approximately 50,000–100,000 people. They provide all services as the lower-level facilities. Additionally, they provide obstetric and general surgical services nearest to provide vital lifesaving surgical intervention closest to the people.
Secondary health service is provided by zonal referral hospitals and second-contact hospitals which serve as referral facilities for the lower level facilities as well as teaching/training institutions for middle and operational level professionals. Tertiary health service serves not only as national referral facilities but as centers of excellence for specialized training/education, and research. The overall number of hospitals in secondary and tertiary level 21 and 2, respectively, today.
Study Center and Design
This was a prospective single-center observational (with 24-hour surveillance) study. The study was conducted at the ED wing (a separate area of 18 bedded ward) of Orotta national teaching and referral hospital in Asmara, Eritrea. The ED follows the historical model that subdivides emergencies into “medical” and “surgical” cases. Established in 2005, the facility serves as the ED of last resort in the country. According to the latest reports, the ED has >16,000 ED visits per year. It has around 40 staff members (including technical, finance, and pharmacy members). The facility also serves as a teaching center for medical and nursing students in the country.
Study Participants and Data Collection
All patients (>15-year-old) who came to the ED between the 14th of September to 13th of October of 2020 were sequentially included in the study. Data was collected by a semi-structured interviewer-administered questionnaire that was developed through a review of published literatures14–16 (see Appendix 1) and medical records. Face content and validation of the questionnaire was undertaken by a team of experts in internal medicine, surgery, and nursing specialty in emergency and critical care. Then, it was pretested for a week on around 100 patients. Collected variables included demographic information (age, sex, address), arrival pattern (day of the week, arrival hour), referral source (self, primary care centers, hospitals), arrival mode (walk-in, ambulance, other means), triage level or condition/acuity level on arrival, ED LOS, prior emergency visits, comorbidity, care (investigations, procedures, consultations, and treatment) and disposition.
Research Metrics and Definition
A Manchester Triage System (MTS) (a process-oriented triage scale) was used in this study (see Appendix 2). Junior doctors and nurses perform triage based on multiple parameters – blood pressure (BP), blood oxygen saturation, pulse rate, respiratory rate, temperature, and the reaction level scale. Based on these parameters, a color-coded five-level management urgency scale is computed. The disparate color codes are defined as follows:
- Red: potentially life-threatening situation if treatment is not commenced.
- Yellow: urgent cases where they should be seen within half an hour.
- Green: semi-urgent, can be seen in an hour.
- White: non-urgent, can lapse up to 2 hours.
- Black: a dead body.
- Vital sign/s: were deemed abnormal if temperature, blood pressure, pulse rate, or respiratory rate were out of range.
- Consciousness: patients were deemed unconscious if Glasgow Coma Scale (GCS) was <8.
- Death: ED-specific mortality was defined as deaths occurring within 24 hours.
- The diagnosis was established based on the impression of the physicians in the ED after clinical assessment.
- Prolonged ED LOS refers to patients with ED LOS >24 hours.
Data Processing and Analysis
The collected data were checked for completeness, consistency and accuracy. Data were coded, entered and cleaned using Cspro v7.0 and exported to SPSS for analysis. All analyses were conducted in IBM SPSS Statistics (SPSS Inc., Version 26.0, Chicago, IL, USA). Depending on data characteristics, absolute counts, frequencies, mean ± standard deviation (SD), or median ± interquartile range (IQR) were used to describe baseline patient characteristics. Multiple data stratification strategies were employed including department in charge, age, arrival shifts, and duration of stay in ED. Differences in all key variables at baseline between these strata were determined using Pearson’s χ2 test for categorical variables. One-way ANOVA or equivalence non-parametric statistics (Mann Whitney U and Kruskal Wallis) were employed to evaluate the difference in means or medians for continuous variables. Binary logistic regression models were used to determine the odds of ED stay >24 hours. In the multivariable analysis, variables were selected if p < 0.25 in the univariate analysis of prolonged ED stay. A backward-selection procedure was used to create the adjusted models, with a variable being included in the model if it resulted in an improvement in the model fit. The level of statistical significance was set at a p-value <0.05 for all analyses.
Ethical Considerations and Consent
Before the start of this study, the researchers obtained approval from the head of the Ministry of Health (MOH) research Ethics and Protocol review committee with a letter of reference: 09/20, the medical director of Orotta Hospital, the Departments of Surgery and Internal Medicine. Informed verbal consent to participate in the study was obtained from participants and this was approved by the ethics committee. All the data collected from the records and observation of the patients were anonymized at all levels and confidentiality was maintained throughout the study. The ethical committee waived consent for publication in place of the participants. This study conforms to the principles outlined in the Declaration of Helsinki.
Results
Emergency Department’s Population Characteristics
During a month study period, 1093 patients presented at the ED. Key demographic and clinical characteristics are shown in Table 1. Most patients were male 618 (56%) from Asmara 769 (70.7%). The median age was 45.0 years (IQR: 28.0–65.0). However, the median age was higher (50.0 years: IQR: 30.5–66.0) in the medical unit when compared to the surgical unit (37.00 years: IQR: 24.0–60.0). Age-specific differences were also observed in patients attending the two departments: 205 (51.2%) patients in the surgical department were between >18–35 years and 225 (66.8%) patients in the medical department were >60 years. Following a Manchester Triage System, 741 (68.5%) were triaged green; 283 (26.2%) were triaged yellow; 48 (4.4%) were triaged red. In addition, a majority of patients were self-referred 857 (79.1%) and had stable vital signs 802 (73.8%). All documented procedures are shown in Table 2.
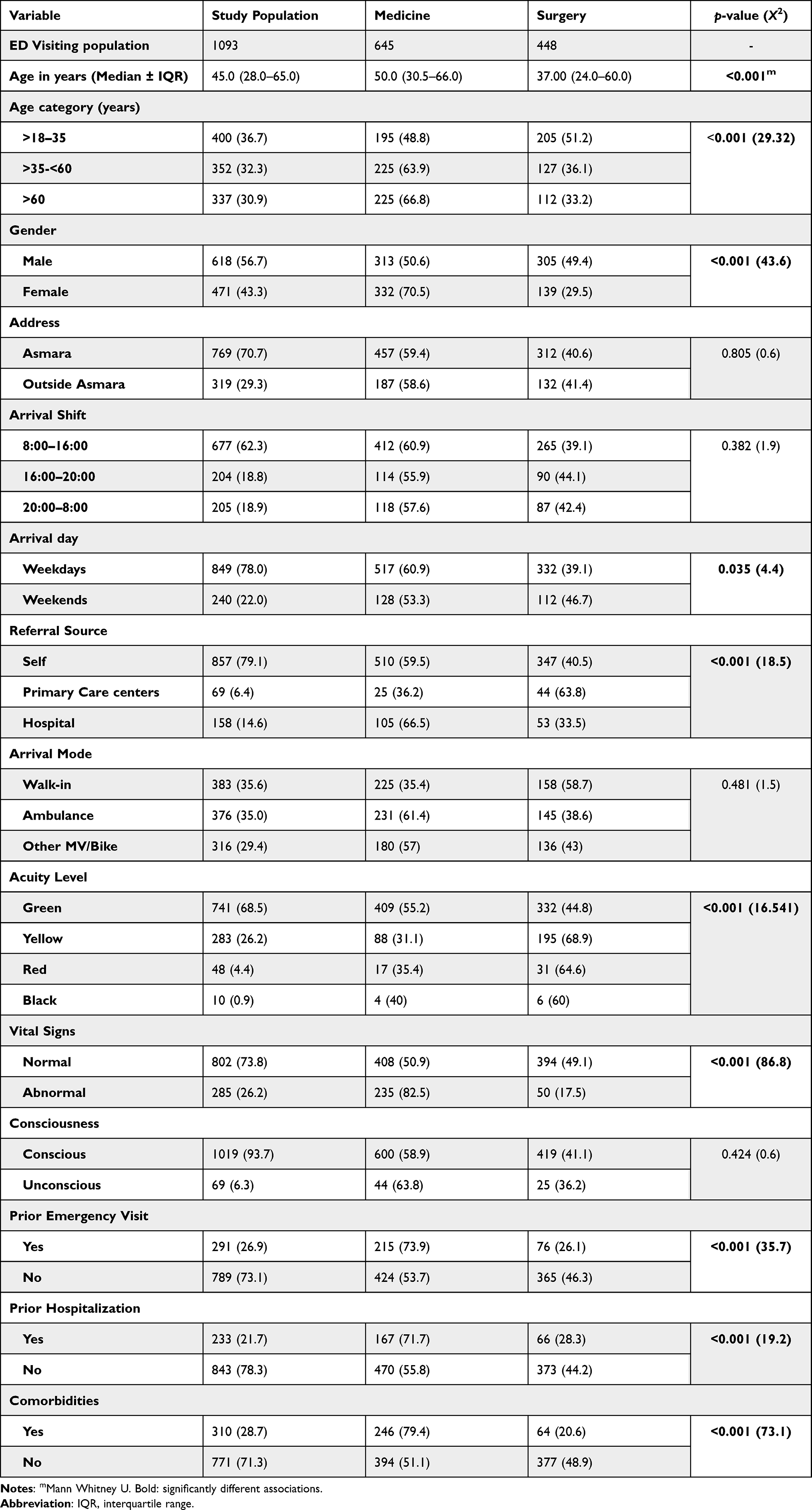 |
Table 1 Socio-Demographic, Clinical Characteristics, Presentation Time and ED-Related Factors of Patients Who Visited the Adult ED of ONRH, Asmara, Eritrea, 2020 |
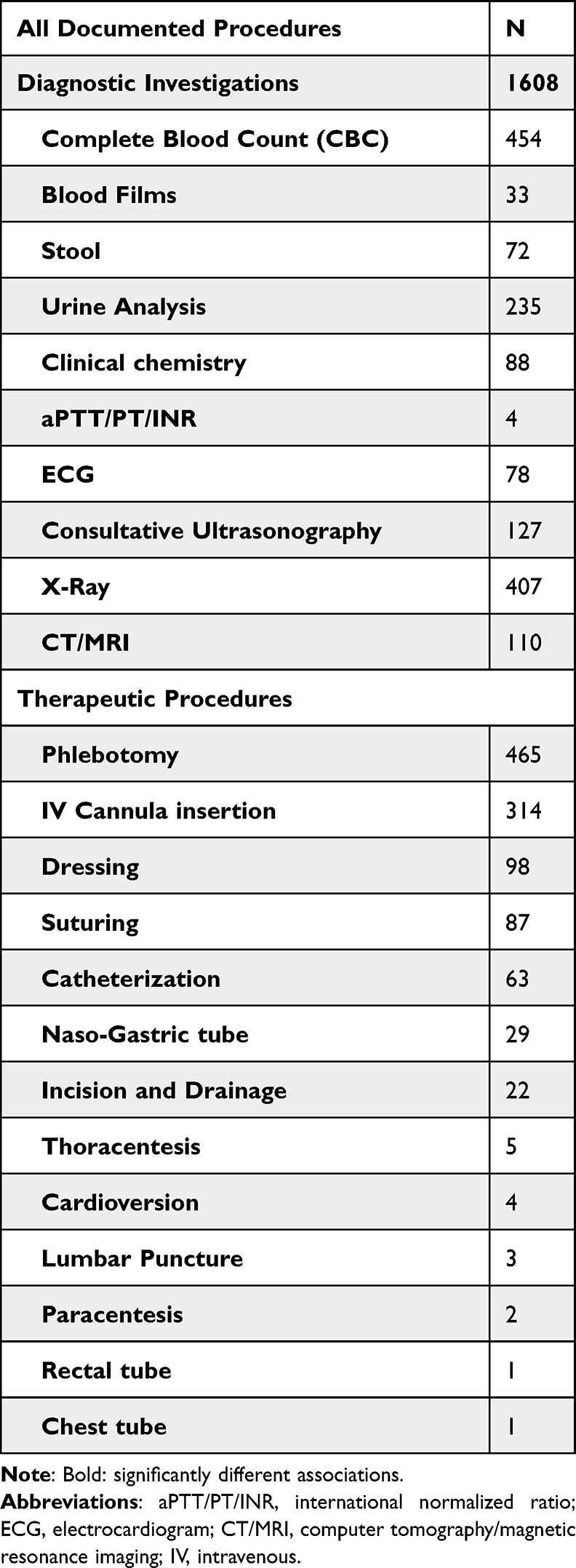 |
Table 2 Frequency Distribution of All Documented Procedures and Investigations of Patients Who Visited the Adult ED of ONRH, Asmara, Eritrea, 2020 |
Frequency of Specific Comorbidities
The distribution of comorbidities among the study participants is shown in Figure 1. According to our result, 310 (28.7%) of the study participants had comorbidities. A significant proportion of the patients had hypertension 64 (22%) or chronic complications associated with hypertension 31 (4%); and Diabetes mellitus (DM) 40 (14%) or chronic complications associated with DM 58 (20%). Additional illnesses, not shown in Figure 1 included psychiatric disorders (13), epilepsy (6), hypothyroidism (7), hemophilia (2), and benign prostatic hypertrophy (BPH) (4).
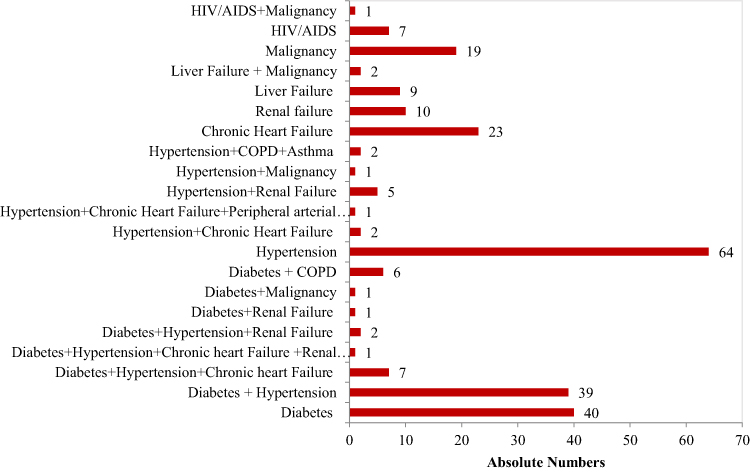 |
Figure 1 Frequency of comorbidities in patients attending the Adult ED of ONRH, Asmara, Eritrea, 2020. |
Mode of Arrival and Associated Factors
The mean age ± SD for disparate modes of arrivals was as follows: walk-in (41.22 ±18.77 years), ambulance (51.69±28.17 years), and bike/other motor vehicles (48.04±23.88 years), p-value <0.001. In terms of proportions, 384 (35.7%) walked to the facility; 376 (34.9%) used an ambulance, and 316 (29.4%) used Bike/other motor vehicles. A weekend vs weekday and shift analysis also demonstrated a significant difference in modes of transport – weekdays (walk-in (69 (29.9%)), ambulance (98 (41.0%)) and bikes/other motor vehicles (72 (30.1%))) vs weekends (walk-in (315 (37.6%)), ambulance (278 (33.2%)) and bikes/other motor vehicles (72 (29.2%)), p value = 0.026. Figure 2 demonstrates the overall utilization of various transport modes per shift. Among patients who were referred by HC/C/CH or hospitals, 78.3 (54%) and 132 (83.5%) came by ambulances. In contrast, only 189 (22.4%) of self-referred patients used an ambulance. The top 5 leading causes of ambulance transport in the top 5 presenting problems among (inter-facility transfers) IFTs were (in order of decreasing frequency): 52 (60.5%) neurologic illness; acute abdominal pain 14 (48.3%); cardiovascular illness, 33 (45.2%); respiratory illness 32 (36.0%) and GIT illness 61 (16.7%).
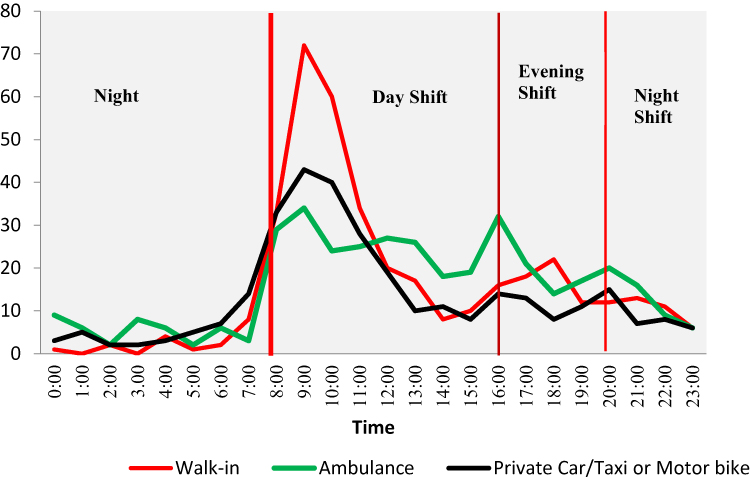 |
Figure 2 Relationship between mode of transport and patient inflow per hour and shift in the Adult ED of ONRH, Asmara, Eritrea, 2020. |
Presenting Illnesses
The classification of presenting illnesses is shown in Figure 3. The top six Organ system diagnoses for all patients were Traumatic injury 278 (26.1%); Gastrointestinal (GIT) illness 182 (17.1%); Genito-urinary (GUS) illness 116 (10.9%); respiratory Illness 91 (8.5%); Neurologic syndromes 86 (8.1%); and Cardiovascular illness 76 (7.1%). Among the top six chief complaints; higher acuity presentation (Red and Yellow) was most prevalent in patients with cardiovascular illness 43 (58.1%); respiratory illness 45 (50%); neurologic illness 33 (38.4%); gastro-intestinal illness 50 (27.6%); traumatic injury 55 (19.8%) and GUS illness 25 (21.6%).
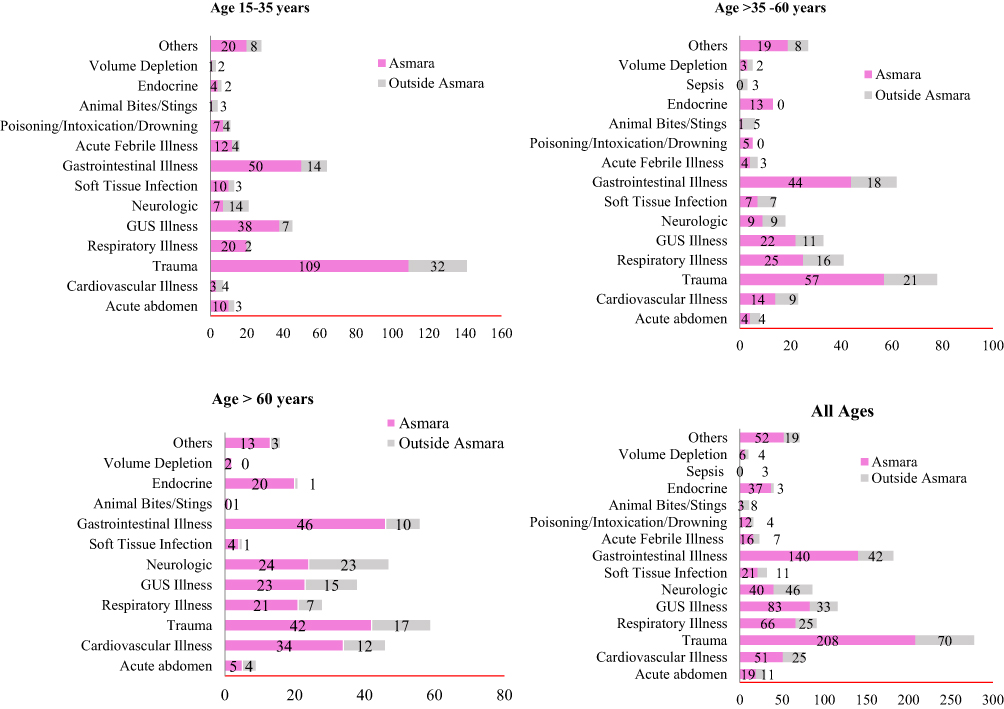 |
Figure 3 Stacked bar graphs for distribution of presenting illness stratified by address and age in the Adult ED of ONRH, Asmara, Eritrea, 2020. |
Arrival Time and Day of Week or Shift
Analysis of patients’ flow indicated that 663 (62.8%), 195 (18.5%), and 197 (18.7%) of the participants came during the Day Shift (8:00 −16:00 hours), Evening Shift (>16:00–20: 00 hours) and Night Shift (>20:00t - <8: 00), respectively. Additional analysis shows that most patients arrived at 9–10 am. In the following sequence, 60 (78.9%), 155 (55.8%), 58 (63.7), 78 (67.2%), 50 (58.1%), 120 (66.3%) patients with CVD illness, traumatic injuries, respiratory illness, GUS problems, neurologic and GIT illness presented during the Day shift. When stratified by acuity level (See Figure 4), the flow of relatively sicker (red and yellow patients) showed less variability during the 24-hour surveillance compared to greenly triaged patients.
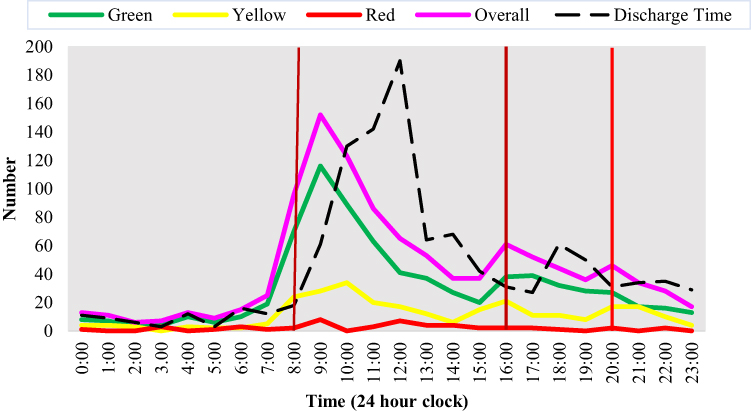 |
Figure 4 Arrival time and discharge time of patients presenting to the emergency department by existing Triage system in the Adult ED of ONRH, Asmara, Eritrea, 2020. |
Average Time or Median for Emergency Department-Boarded Inpatient (Hours) per Population Characteristics
The median ± IQR for ED LOS was 2.67 (1.42–10.00) hours. The mean± SD ED LOS was 11.86±24.78 hours (95% CI, 10.36–13.36 hours) and the 5% trimmed mean was 7.59 hours. ED LOS was associated with multiple variables including Address – shorter for patients from Asmara (2.00 (1.00–6.00) hours vs 4.00 (2.00–23.47 hours)) for patients outside Asmara, p-value <0.001. Longer for patients referred by hospitals (19.50 (3.00–43.75) hours compared to self-referred patients 2.40 (1.50–5.00) or patients referred by primary care centers (4.00 (3.00–24.00 hours)), p-value <0.001. LOS was significantly longer (p-value <0.001) for patients with a Red acuity profile (24 (3.00–72.00) hours compared to yellow (10.08 (2.00–28.83) hours or green patients 3 (2.00–14.75) hours). Extended LOS was also related to consciousness (Conscious patients vs unconscious patients = 4.00 (2.0–23.0) vs 6.00 (2.0–27.3) hours, p-value <0.001); vital signs (Normal vs Abnormal = 3.00 (2.00–20.00) vs 6.00 (2.00–27.25) hours, p-value <0.001); prior hospitalization (No vs Yes = 3.00 (2.00–21.23) vs 8.00 (3.00–29.00), p-value <0.001); presence of comorbidities (No vs Yes = 3.00 (2.00–22.00) vs 6.00 (3.00–27.50)). See Table 3 for additional information on the department in charge, mode of transport, and investigation or treatment.
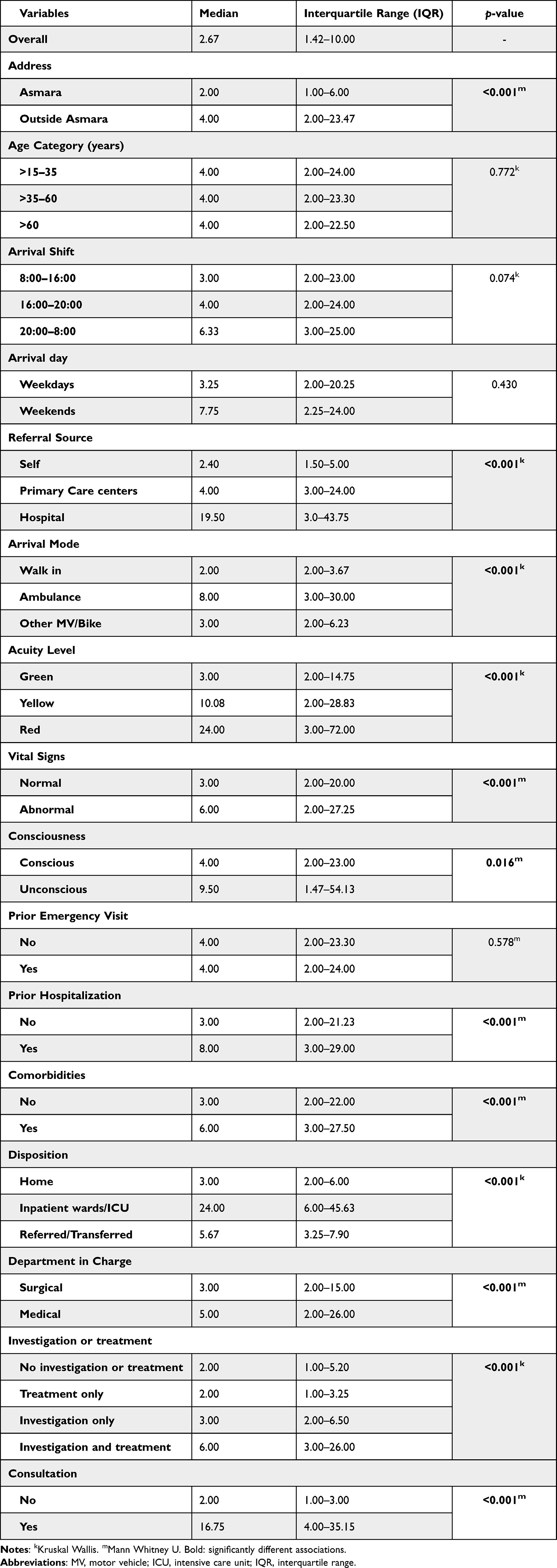 |
Table 3 Median Time for Length of Stay in Emergency Department per Patients’ Clinical, ED and Care Characteristics Who Visited the Adult ED of ONRH, Asmara, Eritrea, 2020 |
Factors Associated with Prolonged ED Stay (> 24 Hours)
Among all the visitors (1093 patients), 154 (14.4%) had an ED LOS>24 hours. In particular, 798 (76.1%) stayed for <12 hours; 93 (8.5%) stayed for 12–24 hours; 87 (8.0%) stayed for 24–48 hours and 70 (6.4%) stayed for ≥48 hours. In the bivariate analysis, we demonstrated a significant relationship between prolonged ED LOS and age category: >15–35 years (335 (87.9%) vs 46 (12.1%)); >35–60 years (274 (84.0%) vs 52 (16.0%)); >60 years (252 (81.0%) vs 59 (19.0%)); p value = 0.042. Additional factors included address (Asmara: 685 (88.8%) vs 81 (11.2%) and residence outside Asmara (216 (74.0%) vs 76 (26.0%), p value <0.001); department in charge (medical: 478 (80.5%) vs 116 (19.5%) and surgical (380 (90.3) vs 41 (9.7%)), p value <0.001). Referral source, arrival mode, acuity level, prior hospitalization, prior emergency visit, and comorbidity were also linked to prolonged stay. See Table 4. Further, analysis of the relationship between prolonged ED LOS and final diagnosis demonstrated that 11 (40.7%), 27 (41.5%), 20 (23.8%), 25 (31.2%), 11 (28.2%) of the patients presented with acute abdominal pain, CVD, respiratory illness, neurological and endocrine problems, respectively. In contrast, 250 (94.3%) of the patients presenting with traumatic injury were disposed of within the first 24 hours.
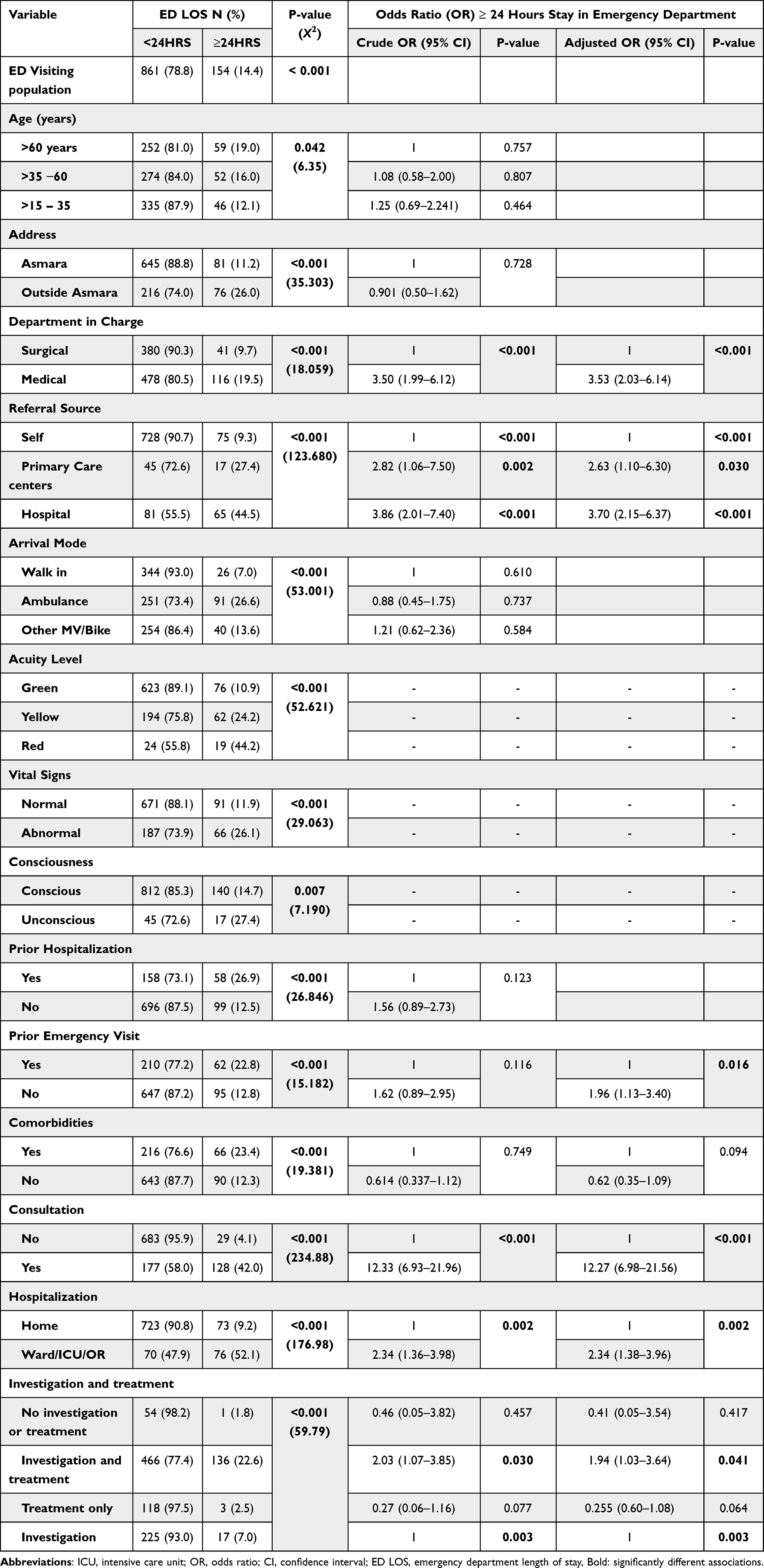 |
Table 4 Multivariable Analysis of Factors Associated with Prolonged ED Length of Stay (>1 Day) Among Patients Who Visited the Adult ED of ONRH, Asmara, Eritrea, 2020 |
Logistic Regression: Independent Factors Associated with Prolonged ED LOS
Multivariate logistic regression identified multiple predictors of prolonged ED LOS (≥24 hours) (Table 4). Higher likelihood of prolonged ED LOS was observed in: medical department patients (aOR = 3.53, 95% CI = 2.03–6.14, p-value <0.001); Patients referred by primary health centers (aOR = 2.63, 95% CI = 1.10–6.30, p < 0.001) and Hospital (aOR = 3.70, 95% CI = 2.15–6.37, p < 0.001) had higher odds of prolonged stay. Higher odds of prolonged ED LOS were also associated with prior emergency visit (aOR = 1.96, 95% CI = 1.13–3.40, p = 0.016); the need for consultation (aOR = 12.27, 95% CI = 6.98–21.56, p < 0.001); hospitalization (aOR = 2.34, 95% CI = 1.38–3.96, p < 0.002); and Investigation and treatment (aOR = 2.03, 95% CI = 1.07–3.85, p = 0.030).
Disposition and Associated Factors
Of all patients presenting to the ED, 883 (77.2%) were discharged home, 58 (5.4%) were referred or transferred, 164 (15.2%) were admitted to the Ward/ICU/OR and 24 (2.2) died either on arrival or within the ED. Home disposition was higher in patients from Asmara 631 (75.8%); self-referred patients 713 (86.0%); walk-in patients (353 (42.9%); patients without comorbidities 614 (74%), among others. Mortality was highest in patients who came in while unconscious 20 (73.3%). Additional associations are shown in Table 5.
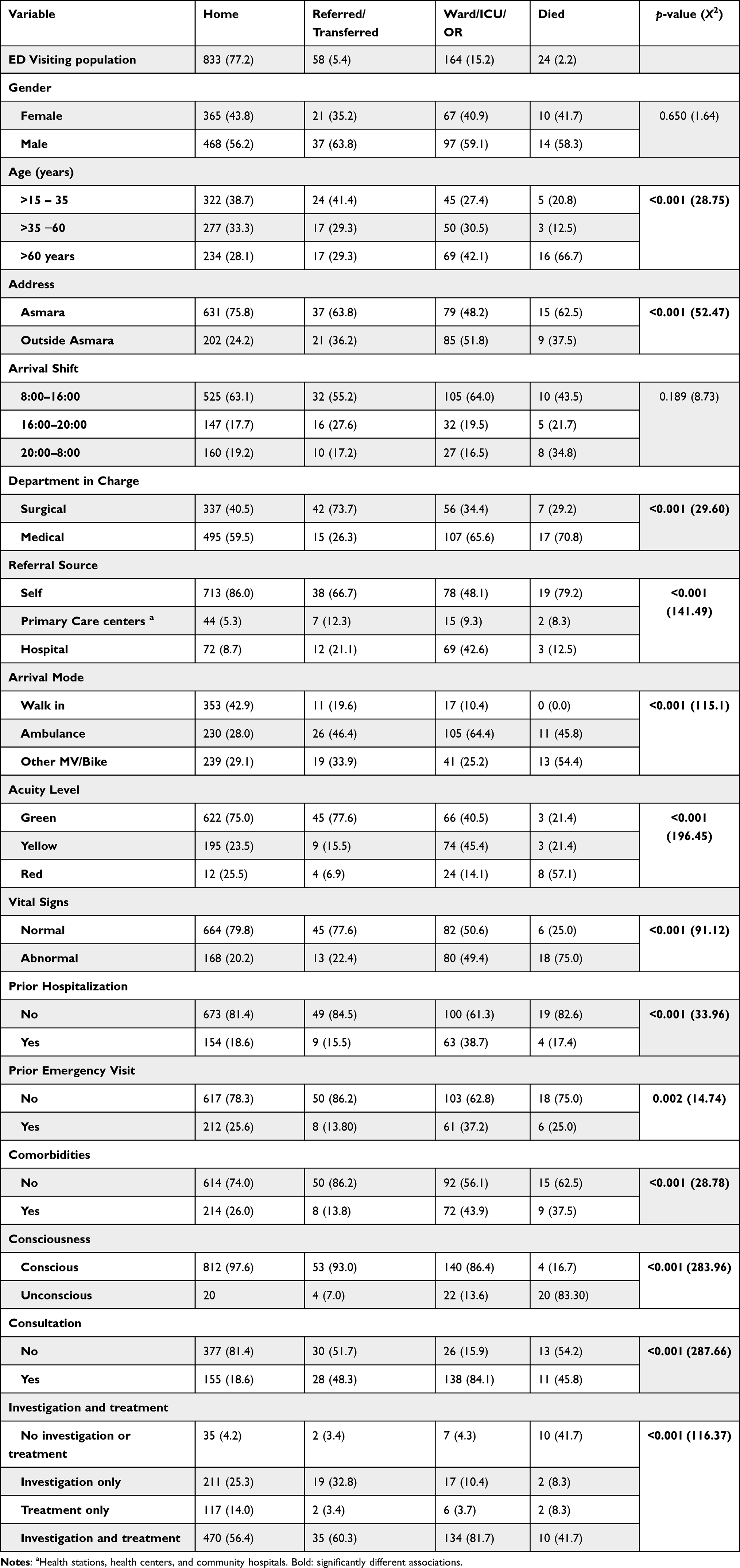 |
Table 5 Final Disposition per Socio-Demographic, Clinical Characteristics, Presentation Time and ED-Related Factors of Patients Who Visited the Adult ED of ONRH, Asmara, Eritrea, 2020 |
Hospitalizations and Associated Factors
By restricting the analyses to the Home vs Hospital; we demonstrated that likelihood of hospitalization was higher in primary care centers referred patients (aOR = 2.43, 95% CI = 1.19–4.96), p-value = 0.015) and Hospital referred patients (aOR = 5.90, 95% CI = 3.55–9.78), p-value < 0.001). Other factors included arrival mode: higher in patients who arrived in via Ambulance (aOR = 3.60, 95% CI = 1.95–6.65), p-value <0.001); other MV/bikes (aOR = 3.10, 95% CI = 1.65–5.77), p-value <0.001); patients with abnormal vital signs (aOR = 2.83, 95% CI = 1.83–4.37), p-value <0.001); Prior Hospitalization (aOR = 2.14, 95% CI = 1.36–3.38), p value=0.001); and presence of comorbidities (aOR = 1.63, 95% CI = 1.03–2.58). In contrast, likelihood of hospitalization was lower in patients who did not receive any investigation or treatment (aOR = 0.23, 95% CI = 0.8–0.66), p value = 0.006); and those whose recieved treatment only (aOR = 0.161, 95% CI = 0.046–0.56), p value = 0.004). See Table 6 for more information.
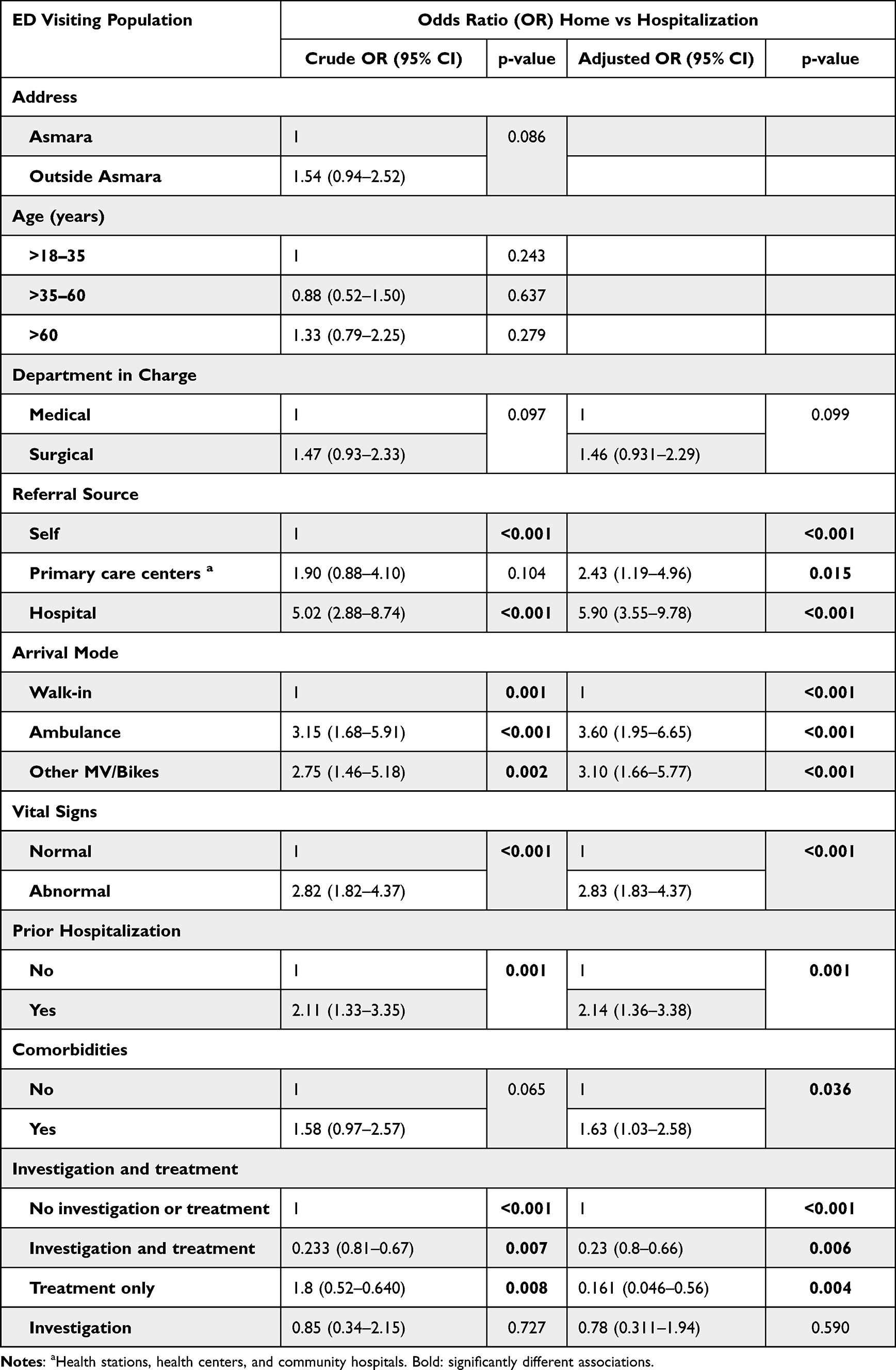 |
Table 6 Multivariable Analysis of Factors Associated with Hospitalization Among Patients Who Visited the Adult ED of ONRH, Asmara, Eritrea, 2020 |
Discussion
Targeted capacity and quality augmentation of emergency care delivery in SSA are currently ranked as a mission-critical priority by multiple agencies and organizations (AU).4 Underscoring this point, WHO, in a dated communication, exhorted member states to undertake a comprehensive assessment of pre-hospital and emergency care needs - the need for identification of unmet needs was also emphasized in this communiqué.4 Despite the growing calls for improvements in research; there has been limited progress in data gathering – reports from LMICs comprised ~ 2–5% (Mean = 3.2%, ±SD: 0.9%) of published reports per annum over the last decade.7 This, in general, has stymied EMS improvement or implementation of context-specific interventions in the region. In this study, we were able to provide the first, albeit limited, data on the profile of an ED in the largest referral facility in Eritrea.
There were several interesting findings from this study. First, the median age of patients attending this facility was relatively high [45 years (IQR: 28.0–65.0)] and a significant age disparity was observed in patients from the medical department [50.0 years (IQR: 30.5–66.0) vs 37.00 years (IQR: 24.0–60.0)] in Surgical department. These estimates are generally higher than what has been reported for the continent which is 35 years (IQR: 6.9–41.0).5 The observed disparity may be related to the nature of the population in the catchment area. Traumatic injuries are more common in younger populations and this may depress median age. Following this logic, the inter-departmental disparity in age may be associated with the nature of patients visiting these departments – relatively young trauma patients (generally free from chronic conditions) in surgical departments and relatively older patients with emergencies associated with specific non-communicable diseases (NCDs) (mostly Diabetes mellitus (DM) and Hypertension) in the medical department.
An equally important finding was the fact that a large proportion of self-referred patients (79.1%) had non-urgent conditions (green and white). The reported proportion is nearly similar to what has been reported in other jurisdictions - 88.2% in some parts of South Africa (SA).17 The rates of emergency (Red) presentations were relatively low (4.4%) - a phenomenon that is common in the region.18 High volumes of self-referred patients in SSA have been attributed to multiple factors including the absence of 24-hour access to primary care facilities/or limited access to other types of care, including convenience settings.14,19,20 There is also a perception that one might have better access to expert consultation and therapeutic or diagnostic services during the day shift.18 We believe that most of these factors may be operational in this setting. Indeed, under-developed primary health care (PCP) in Eritrea may also push patients to seek care in the referral EDs. On the whole, self-referral may have negative consequences for tertiary EDs – it imposes an unnecessary burden on EMS and may thus lead to a reduction in quality of care.
The pattern of arrival in this department was not unique and was quite similar to what has been observed in other settings.18 In general, the peak arrival time was between 7.00 AM – 1.00 PM and Mondays had the largest patient load. The surges were also limited to patients who were triaged as green or yellow. Possible explanations of the Monday morning peaks include limited access to health facilities on Saturdays and Sundays. Similarly, the early morning (7 AM) surge in caseload may be attributed to several things including lack of transport (particularly at night), and absence of 24-hour, 7 days-a-week, ambulance service. Out-flow of patients or redirection of patients from the out-patient department (OPD) may also explain these mid-morning surges.
Another important finding in this study was the significant gap in prehospital/or Out of Hospital Emergency Care (OHEC). This finding is not unique and is typical in the region.21 Investigators in the region have described OHEC, as under-developed or entirely lacking. Preclinical transport is mostly dominated by informal modalities; thus, patients do not receive a timely, safe, on-scene evaluation, stabilization, and transportation to EDs.20 More importantly, ambulances, which transport a relatively small fraction of patients, lack trained personnel (no trained physicians or mid-level providers) or basic life support (BLS) systems. Prior geo-spatial studies have reported long transit time for patients (in Eritrea, 57·4% (55·5–59·8) of the population are outside 2-hours travel time to a hospital).13 Consequently, prehospital mortality is relatively high in SSA.5 These descriptions, with some exceptions, are true for this setting. According to our analysis, 376 (34.9%) used ambulances and the rest used informal transport modalities. After adjusting for reference sources, we noted that a disproportionate number of the patients who used ambulance services were referred - 78.3 (54%) by HC/C/CH and 132 (83.5%) by hospitals. Further, those who came by ambulance were more likely to have pre-existing comorbidity (diabetes, hypertension, malignancy, among others).
Besides the low ambulance coverage, several important facts can be gleaned from our data. First, the case-mix associated with inter-facility transfers (IFTs) can be useful as a monitoring and evaluation tool to identify areas that may be targeted to improve service delivery. In this setting, deficiencies in lower-tier facilities (eg, regional referral hospitals); particularly the ability to manage acute phases of specific NCDs or emergencies associated with specific organ systems, are apparent. Secondly, the large number of NCD-associated IFTs may also point to poor health literacy. Highlighting this phenomenon, some investigators22 have asserted that due to poor health literacy, patients with relatively advanced stages of illness are presenting to inadequately equipped facilities. This, in turn, prompts prompt transfer to, at times, distant higher tier facilities. Overall, and considering the deficiencies in our study; there is a need for more research on pre-hospital EMS in Eritrea.
To understand, training or capacity needs in an ED, chief complaints or array of infections and NCDs presenting acutely should be understood.7 In general, our finding suggests that EDs in Eritrea are currently dealing with the triple burden of trauma, infectious diseases, and NCDs.5,7,18 The leading causes of ED visitation were (in order of decreasing frequency): traumatic injuries, GIT and GUS complaints, and chronic heart failure (CHF). As highlighted in a majority of published studies,15,20 traumatic injuries were more frequent in young males (15–35 years) - an economically productive part of the population. Unlike other studies in the region,15,23 most of these injuries were not linked to motor vehicle accidents. In contrast, bicycle accidents triaged as non-urgent (Green, 222 (80.1%) were more common. Therefore, our data shows that most patients with traumatic injuries in this setting can be managed in PCPs. However, this will require basic training in the management of traumatic injuries and better triaging techniques for prompt transfer of complex cases to better-resourced EDs.
By superimposing the case-mix data and data on the number of imaging procedures ordered (mostly X-Rays) during the study period; we also noted another important gap. Namely, that expanding the use of ED point-of-care ultrasonography (ED PoCUS) in this facility may solve a variety of diagnostic needs. In general, ED PoCUS can be used for multiple procedures – goal-directed echocardiography; ultrasonography in cardiac arrest; thoracic ultrasonography; screening abdominal ultrasonography; focused assessment with sonography for trauma (FAST); examination for DVT and PE; abdominal ultrasonography; soft tissue and musculoskeletal ultrasonography and ultrasonography for procedure guidance, among others.24,25 More importantly, several studies in SSA have demonstrated the substantial benefits of ED PoCUS in poorly resourced settings. ED PoCUS can promote faster diagnosis; enhance diagnostic accuracy; definitive treatment and reduce ED LOS. When used for procedure guidance, ED PoCUS can also reduce associated complications.24 In all, this data has overall implications for infrastructure and training needs in the country.
Further, age-related disparities in disease burden were also uncovered – atherosclerosis disease-related complications were disproportionately high in the older patients (Age >60 years) surpassing even traumatic injuries in proportions if binary classification is employed. In contrast, a similar age disparity was not observed for GIT or GUS (infectious disease-related illnesses). Altogether, the concurrent epidemic of infectious diseases and NCDs in Eritrea is supported by epidemiological data/estimates. For example, WHO estimates suggest that CVD-related mortality in Eritrea is disproportionately high (Males: 388.1 vs Females: 282.2 per 100,000).26 The large proportion of patients with advanced presentations of specific comorbidities adds to the veracity of these estimates. An inevitable consequence of the changing disease patterns in countries like Eritrea is the high mix of young and elderly patients in EDs in the country. In addition, the large number of patients referred by lower-tier facilities is a crude indicator of the large emergency care caseloads and the dire need for improvements in EMS in these facilities.
The fact that EDs in SSA are dominated by young and old patients is important in multiple respects. First, the observed case mix suggests that EMS in countries like Eritrea should augment the capability to deal with traumatic injuries; infectious disease complications, and time-sensitive presentations of multiple NCDs. Another imperative is the need to focus on specific groups of patients. For example, geriatric patients often present with emergencies associated with multiple comorbidities that require multidisciplinary interventions. Taking into account the changing case-mix in EDs; experts on the state of EMS in SSA have proposed several solutions. Logically, primary prevention initiatives, particularly efforts directed at a reduction in incidence, hence, the prevalence of NCDs; and optimization of clinical management has been emphasized. System reconfiguration or the need for horizontal integration of emergency care systems in some jurisdictions has been suggested.22 According to these experts, such attempts should simultaneously address existing deficiencies (basic infrastructure, equipment, and education needs for emergency services) in higher-tier institutions; while scaling up access to basic emergency care services at lower-tier facilities (community health centers, health stations, among others).22
Currently, a patient’s ED LOS or specific-hour wait time target is regarded as a major indicator of overall efficiency and quality service. Literature suggests that prolonged ED LOS has multiple negative effects both on patients and health delivery systems. For example, LOS is a major risk factor for hospital-acquired pneumonia in blunt trauma patients27 and has a 15–30% higher rate of mortality.28 In general, ED LOS across SSA varies significantly. A recent study in Ethiopia reported an ED LOS of 4 hours (IQR: 1.6–13.5).16 Higher values, 7.7 hours (IQR: 3.3–40.8) have been reported in a systematic review.5 In this study, the ED LOS was much lower: 2.67 hours (IQR: 1.42–10.00). Interestingly, the values are much lower than what has been reported in some high-income countries (HIC) (176–480 min).29 On the surface, these results appear to suggest that EDs in SSA are more efficient than facilities in HIC. However, other workers have convincingly demonstrated that countries with well-developed primary health-care (PCP) systems tend to have a lower number of self-referred (mostly green) patients. Therefore, patients presenting in EDs in some HIC have a higher level of acuity thus prolonged ED LOS. After adjusting for acuity levels in this study, ED LOS was substantially higher: 10.08 hours (IQR: 2.00–28.83) for yellow patients and 24 hours (IQR: 3.00–72.00) for red patients.
Therefore, the ED LOS in this facility is not favorable. Multiple input, throughput, and output factors were associated with prolonged ED LOS. Input factors included a large number of non-urgent (Green) patients – this may trigger overcrowding and attendant negative repercussions.9 Throughput factors (operational bottlenecks and inefficiencies) included the need for consultations. Typically, inexperienced physicians (interns or junior doctors), working under the supervision of a relatively small number of senior physicians, staff the ED. Complex cases will require consultation. In the simplest scenario, this will lead to prolonged ED LOS considering the large caseloads borne by senior physicians in the facility. Predictably, the need for consultation was the strongest predictor of prolonged ED LOS in this study (aOR = 12.27, 95% CI = 6.98–21.56, p < 0.001). Additional throughput factors included a requirement for investigation procedures and treatment (a proxy for long turnaround time for investigations - radiological and laboratory). Output factors or institutional inefficiencies with upstream effects on ED operations were also detected. Lack of bed capacity in the facility was highlighted by the connection between ED LOS and hospitalization. In other words, some patients had extended ED LOS because of a lack of bed space in the inpatient wards. Similar to data from LMIC, additional associations were patient-specific factors – patients in the medical department were generally older; had a variety of comorbidities; were more likely to have acute presentations; were more likely to be referred; and thus, arrive at the facility in an ambulance. The associations described in this study have been uncovered by some investigators in the region. In Ethiopia, a recent study reported a connection between prolonged ED LOS and limited bed capacity in inpatient wards; long turn-around time for a laboratory test, and radiological services.15
Limitations of the Study
Although this study has uncovered several important findings; it has some limitations. The fact that it is a single-center study in an urban hospital is limiting. This imposes constraints on the generalizability of our findings. However, the fact that this is the ED-of-last-resort in the country should not be missed. Another important concern was the duration of the study – one month. Therefore, it was not possible to investigate seasonal shifts in ED visits or disease patterns. This notwithstanding, we are confident that the minimum required data for this type of study was met. Additionally, there are some standardization issues. For example, a lack of consensus on how to classify specific variables, eg, chief complaints, among others; may marginally undermine comparisons across with similar studies in the region.
Conclusion
This study is a source of useful information on the state of emergency care services in Eritrea. A higher likelihood of prolonged ED LOS was observed in medical department patients; patients from PCPs; hospital referred patients and patients with a prior emergency visit. The need for consultation; hospitalization or investigation and treatment was also associated with prolonged ED LOS. The findings of this study suggest that there is a need to reconfigure EMS in the country. Such attempts should simultaneously address existing deficiencies (basic infrastructure, equipment, and education needs for emergency services) in higher-tier institutions; while scaling up access to basic emergency care services at lower-tier facilities (community health centers, health stations, among others).
Data Sharing Statement
All data generated or analyzed during this study are available from corresponding author upon reasonable request.
Acknowledgments
We would like to acknowledge Dr. Habte Beletse, Dr. Samuel Fissehay and all emergency department staff for helping in data collection and cleaning.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study has not received any funding.
Disclosure
The authors declare that they have no competing interests.
References
1. Reynolds TA, Calvello EJB, Broccoli MC, et al. AFEM consensus conference 2013 summary: emergency care in Africa—where are we now? Afr J Emerg Med. 2014;4:158–168. doi:10.1016/j.afjem.2014.07.004
2. Thind A, Hsia R, Mabweijano J, Hicks ER, Zakariah AMC. Chapter 14: prehospital and emergency care. In: Debas T, Donkor P, Gawande A, Jamison DT, Kruk MMC, editors. Essential Surgery: Disease Control Priorities. World Bank; 2015.
3. Kobusingye OC, Hyder AA, Bishai D, et al. Emergency Medical Services. World Bank; 2006.
4. World Health Organization. World health assembly update. Available from: https://www.who.int/newsroom/detail/25-05-2019-world-health-assembly-update.
5. Obermeyer Z, Abujaber S, Makar M, et al. Emergency care in 59 low- and middle-income countries: a systematic review. Bull World Health Organ. 2015;93(8):577–586G. doi:10.2471/BLT.14.148338
6. Brugnolaro V, Fovino LN, Calgaro S, et al. Pediatric emergency care in a low-income country: characteristics and outcomes of presentations to a tertiary-care emergency department in Mozambique. PLoS One. 2020;15(e0241209):e0241209. doi:10.1371/journal.pone.0241209
7. Aluisio AR, Waheed S, Cameron P, et al. Clinical emergency care research in low-income and middle-income countries: opportunities and challenges. BMJ Glob Heal. 2019;4(Suppl 6):e001289. doi:10.1136/bmjgh-2018-001289/
8. Calvello E, Reynolds T, Hirshon JM, et al. Emergency care in sub-Saharan Africa: results of a consensus conference. Afr J Emerg Med. 2013;3:42–48. doi:10.1016/j.afjem.2013.01.001
9. Hesselink G, Őzcan Sir SY, Schoon Y. Effectiveness of interventions to alleviate emergency department crowding by older adults: a systematic review. BMC Emerg Med. 2019;19. doi:10.1186/s12873-019-0288-4
10. Jones SS, Thomas A, Evans RS, et al. Forecasting daily patient volumes in the emergency department. Acad. Emerg Med. 2008;15:159–170. doi:10.1111/j.1553-2712.2007.00032.x
11. Hodkinson PW, Pigoga JL, Wallis L. Emergency healthcare needs in the Lavender Hill suburb of Cape Town, South Africa: a cross-sectional, community-based household survey. BMJ Open. 2020;10:e033643. doi:10.1136/bmjopen-2019-033643
12. Hertz JT, Reardon JM, Rodrigues CG, et al. Acute myocardial infarction in Sub-Saharan Africa: the need for data. PLoS One. 2014;9(e96688):e96688. doi:10.1371/journal.pone.0096688
13. Ouma PO, Maina J, Thuranira PN, et al. Access to emergency hospital care provided by the public sector in sub-Saharan Africa in 2015: a geocoded inventory and spatial analysis. Lancet Glob Heal. 2018;6(3):e342–e350. doi:10.1016/S2214-109X(17)30488-6
14. Thijssen WAMH, Kraaijvanger N, Barten DG, Boerma MLM, Giesen P, Wensing M. Impact of a well-developed primary care system on the length of stay in emergency departments in the Netherlands: a multicenter study. BMC Health Serv Res. 2016;16. doi:10.1186/s12913-016-1400-z
15. Alemu GH, Negari KG, Rodamo KM, Hirigo AT. Factors associated with the length of stay in emergency departments in Southern-Ethiopia. BMC Res Notes. 2019;12. doi:10.1186/s13104-019-4271-7
16. Ahmend AA, Ibro SA, Melkamu G, Seid SS, Tesfaye T. Length of stay in the emergency department and its associated factors at Jimma Medical Center, Southwest Ethiopia. Open Access Emerg Med. 2020;12:227–235. doi:10.2147/OAEM.S254239
17. Van Wyk PS. The after-hours case mix of patients attending the George Provincial Hospital Emergency Centre. S Afr Fam Pr. 2014;56:1–6.
18. Meyer NT, Meyer GD. What presents to a rural district emergency department: a case mix. Afr J Prm Heal Care Fam Med. 2020;12:a2275.
19. Heinert SW, Mumford M, Kim SE, Hossain MM, Amashta ML, Massey M. User characteristics of a low-acuity emergency department alternative for low-income patients. West J Emerg Med. 2020;21. doi:10.5811/westjem.2020.8.47970
20. Mould-Millman NK, Dixon JM, Sefa N, et al. The state of Emergency Medical Services (EMS) systems in Africa. Prehosp Disaster Med. 2017;32:1–11. doi:10.1017/S1049023X17000061
21. Mould-Millman NK, Naidoo R, de Vries S, Stein C, Wallis LA; AFEM Consensus Conference, 2013. AFEM out-of-hospital emergency care workgroup consensus paper: advancing out of-hospital emergency care in Africa-advocacy and development. Afr J Emerg Med. 2014;4:90–95. doi:10.1016/j.afjem.2014.02.001
22. Touray S, Sanyang B, Zandrow G, Touray I. Incidence and outcomes after out-of-hospital medical emergencies in Gambia: a case for the integration of prehospital care and Emergency Medical Services in primary health care. Prehosp Disaster Med. 2018;33:650–657. doi:10.1017/S1049023X1800105X
23. McKenna P, Heslin SM, Viccellio P, Mallon WK, Hernandez C, Morley EJ. Emergency department and hospital crowding: causes, consequences, and Cures. Clin Exp Emerg Med. 2019;6:189–195. doi:10.15441/ceem.18.022
24. Reynolds TA, Amato S, Kulola I, Chen CJJ, Mfinanga J. Impact of point-of-care ultrasound on clinical decision-making at an urban emergency department in Tanzania. PLoS One. 2018;13(e0194774):e0194774. doi:10.1371/journal.pone.0194774
25. Gingrich AS, Saul T, Lewiss RE. Point-of-care ultrasound in a resource-limited setting: diagnosing intussusception. J Emerg Med. 2013;45:e67–e70. doi:10.1016/j.jemermed.2013.03.030
26. Whitson MR, Mayo PH. Ultrasonography in the emergency department. Crit Care. 2016;20. doi:10.1186/s13054-016-1399-x
27. Tarr BG, Kaye AJ, Wiebe DJ, Gracias VH, Schwab CW, Reilly PM. Emergency department length of stay: a major risk factor for pneumonia in intubated blunt trauma patients. J Trauma Acute Care Surg. 2007;63:9–12. doi:10.1097/TA.0b013e31805d8f6b
28. Forero R, Hillman KM, McCarthy S, Fatovich DM, Joseph AP, Richardson DB. Access block and ED overcrowding. Emerg Med Australas. 2010;22:119–135. doi:10.1111/j.1742-6723.2010.01270.x
29. Pines JM, Mullins PM, Cooper JK, et al. National trends in emergency department use, care patterns, and quality of care of older adults in the United States. J Am Geriatr Soc. 2013;61:12–17. doi:10.1111/jgs.12072
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.