")
Back to Journals » Research and Reports in Neonatology » Volume 10
Poor Universal Coverage of Immediate Essential Newborn Care at Hospitals of Wollega Zones, The Case of Western Ethiopia
Authors Kasaye HK , Yilma MT , Bobo FT , Fekadu G
Received 28 April 2020
Accepted for publication 11 August 2020
Published 9 September 2020 Volume 2020:10 Pages 37—46
DOI https://doi.org/10.2147/RRN.S260369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Schelonka
Habtamu Kebebe Kasaye,1 Mekdes Tigistu Yilma,2 Firew Tekle Bobo,2,3 Ginenus Fekadu4
1Wollega University, Institute of Health Sciences, School of Nursing and Midwifery, Department of Midwifery, Nekemte, Ethiopia; 2Wollega University, Institute of Health Sciences, Department of Public Health, Nekemte, Ethiopia; 3Australian Centre for Public and Population Health Research, Faculty of Health, University of Technology Sydney, Sydney, New South Wales, Australia; 4Wollega University, Institute of Health Sciences, Department of Pharmacy, Nekemte, Ethiopia
Correspondence: Habtamu Kebebe Kasaye P.O. Box: 395, Nekemte, Ethiopia
Tel +251913426539
Email [email protected]
Background: Thousands of neonates die annually in Ethiopia related to preventable causes. Low-quality care enhances neonatal morbidity and mortality unless remedial action is taken based on evidence. Here, we show the magnitude of essential newborn care service provisions and factors contributing to substandard care.
Methods: We conducted a cross-sectional study in four hospitals of Wollega Zones from April to August 2017. We calculated 390 samples using Epi-info stat calc using necessary assumptions. A systematic random sampling method was used to select study participants. Non-participatory observations of essential newborn care service provisions were conducted using a World Health Organization checklist. We used binary logistic regression models to identify the independent predictors and reported variables having P-values less than 0.05 at 95% confidence intervals of odds ratios as significantly associated variables.
Results: A total of 375 childbirths were observed and among these, only 11 (2.9%) neonates were given all components of immediate essential newborn care, while 315 (84.0%) of the newborns initiated early breast-feeding, 131 (34.9%) kept warm, 108 (28.8%) got disease prevention measures (89 (23.7%) helped to breathe, and only 14 (3.7%) kept clean immediately following the birth. Maternal highest annual income, maternal age, need of resuscitation, presence of assistant to a birth attendant, childbirth during the weekends were statistically significantly associated with immediate essential neonatal care categories in various predictive level.
Conclusion: The essential newborn care provided for the neonates during childbirth at the health facilities was found to be poor. Continued efforts at improving access to quality essential newborn care provided for neonates are required. Hospital administrators need to consider enhancing the number of skilled delivery attendants, and enforcing implementations of essential newborn care standards is mandatory to protect the lives of neonates.
Keywords: essential, newborn, care, Wollega, Ethiopia
Introduction
Essential Newborn Care (ENC) is care required to be applied immediately for every newborn baby regardless of where the delivery took place or the baby’s size and should be continued for at least the first 7 days after birth. Following delivery, the transition from the fetus to neonate represents a series of dramatic physiologic changes. Those changes need skilled personnel interventions to ensure that it occurs with the least possible problem.1
To minimize problems neonates encounter, the World Health Organization (WHO) sets the standards of care that encompass a series of 10 steps, which in turn has a set of activities. These recommended essential newborn care include dry and stimulate, evaluate breathing, cord care, keep the newborn warm, initiate breastfeeding in the first 1 hr, administer prophylactic antibiotics into eyes, administer vitamin K intramuscularly, place the newborn’s identification bands on the wrist and ankle, weigh the newborn when it is stable and warm, and record all observations of the baby.2
The implementations of these cares minimize the incidence of neonatal morbidity and mortality.3 Even though there was a substantial decline (51%) in the global neonatal mortality rate (NMR) since 1990, high NMR is concentrated in Sub-Saharan Africa (40/1000) and South Asia (26.9/1000). More than a million of these neonatal deaths occur on their first day of life, which would have been minimized if ENC had implemented it appropriately.4,5 The neonatal mortality impact is more significant in Sub-Saharan Africa (SSA), where the unassertive progress of the reduction of neonatal mortality has shown, and two-thirds of countries in this region are at risk of missing the Sustainable Development Goal by the year 2030.6,7
Ethiopia is also among SSA countries where about 81,000 neonatal deaths occur annually. It accounts for 42% of all deaths in children younger than 5 years of age, and the risk of death is highest in the first 24 hrs of life. The infant mortality rate in 2011 was 59 deaths per 1000 live births, and this figure declined to 48 deaths per 1000 live births in 2016, from which neonatal mortality accounts 29 deaths per 1000 live births. The newborn mortality reduced at slower rate (41%) as compared to under-five (60%) and infant mortality (50%) since 2000.8,9
WHO recommends implementation of ENC for every baby based on evidenced positive outcomes in improving neonatal well-being. However, many African newborns do not have access to quality health care. This low provisions of ENC had been putting neonates at an increased risk of illness and death.1,10–15 Even though each step of essential newborn care is designed based on priority problems or its impact on neonatal life, most studies from different parts of the world indicated incomplete or inappropriate essential newborn.16,17
Ethiopian health sector transformation plan (HSTP) (2015/16–2019/20) has targeted to reduce neonatal mortality to 10 deaths per 1000 live births by the year 2020.18 The achievement of this target could not be successful in the absence of quality of maternal and neonatal care during childbirth and early postnatal care. Studies conducted in Ethiopia19–22 tried to measure essential newborn care practiced by mothers at the community level.
Determining ENC provision in the health facilities will enable enhancement of the quality of care and helps to work on the priority area for the reduction of neonatal mortality. Similarly, identifying the underlying factors related to facility readiness and the competency of the provider in skill and maternal characteristics that determine ENC implementation are also crucial for the success of both the transformational and SDG plans. Therefore, we aimed to determine the proportion of immediate essential newborn care provision by care providers and identify social determinants and characteristics of birth that affect essential newborn care at general public hospitals in Wollega Zones of Oromia Region, Ethiopia.
Methods
Study Setting and Populations
A facility-based cross-sectional quantitative study was conducted from April to August 2017 in the western part of the country. The Ethiopian health service is structured in a three-tier system that includes primary, secondary, and tertiary levels. The primary level is composed of health posts, health centers, and a primary hospital, which altogether provides services for about a hundred thousand populations. Besides, a primary hospital serves as a referral center for health centers and provides emergency surgical services, including cesarean sections, and gives access to blood transfusion service. The secondary level of health care includes general hospitals that provide inpatient and ambulatory services to an average of 1,000,000 people while the tertiary level operates with a specialized hospital, which serves an average of five million people.18
The referral system between the three-level or tier enables patients to obtain comprehensive emergency obstetrics and newborn care (CEmONC) from primary hospital, secondary and tertiary health-care levels because Health Centers only provide basic emergency obstetrics and newborn care (BEmONC). All three-levels of health facilities provide immediate essential newborn care for the newborns delivered at the health facilities.23
We conducted this study in four zones of Wollega in Oromia regional state, including Kellem Wollega, West Wollega, East Wollega, and Horo Guduru Wollega. We observed the essential newborn care provided for newborns born in Dembidollo, Nedjo, Nekemte, and Shambu public Hospitals, one general hospital from each zone. All live-born newborns care, including twins were observed, while the mothers of those selected newborns were also included by default to get data from mothers.
Measurements
The outcome variable was Essential Newborn Care services provided for the babies immediately after delivery in the health facilities. To measure these cares accurately, we classified the WHO recommended essential newborn care components2 into five composite categories. The five essential newborn care classes were keeping the baby warm, helping the baby breathe, keeping the delivery procedure and baby clean, early initiation of breastfeeding, and provision of tetracycline prophylactic eye care and vitamin K. Each of these categories contains individual elements, which were assessed as yes, no, or not applicable part according to the care needed for the section under investigation as detailed in the checklist we have used. ENC was considered as provided if all of the components were given to the neonate as summarized in Table 1.
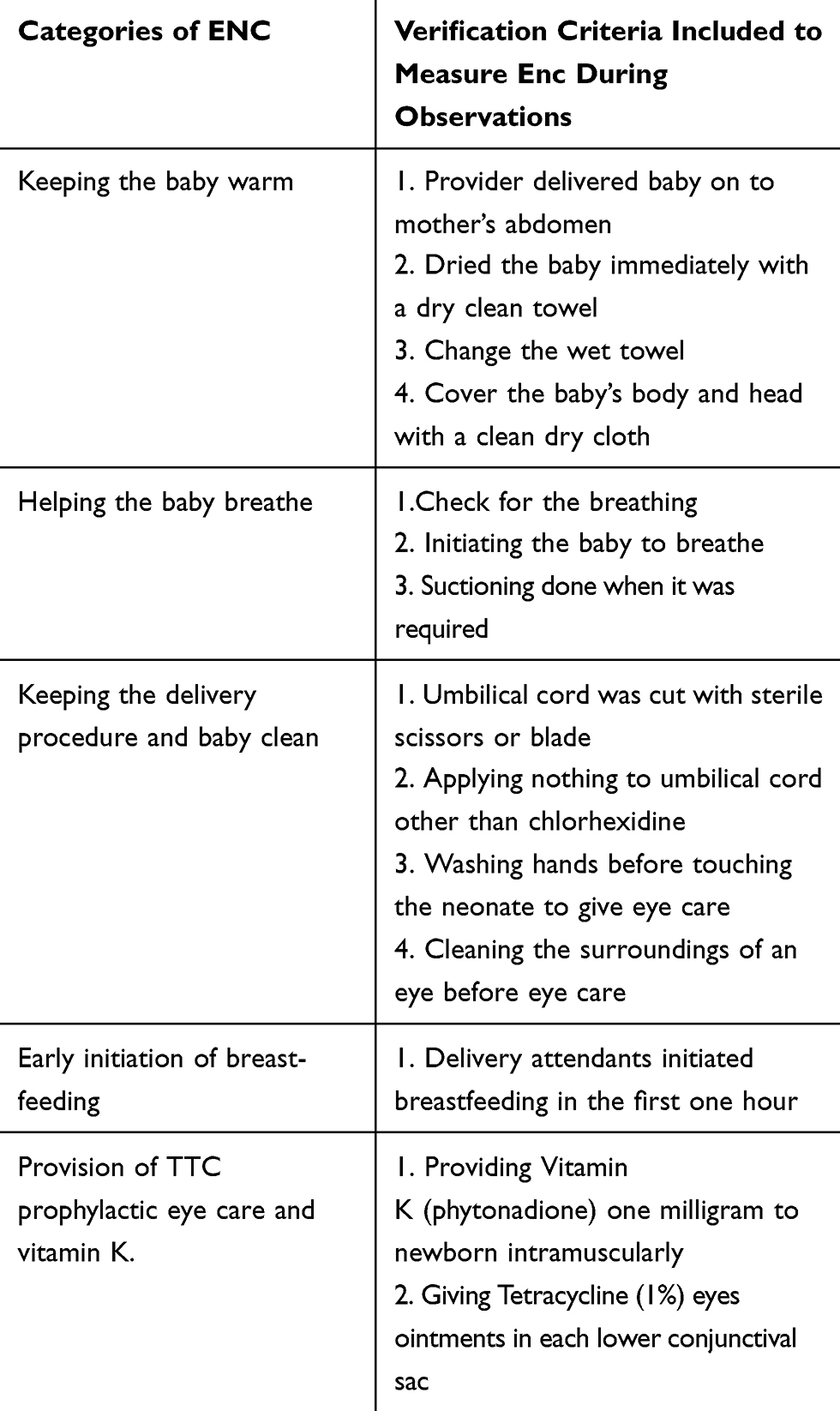 |
Table 1 Categories of Essential Newborn Care and Their Verifying Criteria |
Sample Size and Sampling Technique
We calculated sample size using Epi Info Stat Calc version 7, considering the following assumptions: the percentage of all essential newborn care elements 18%,16 a confidence level of 95%, and a marginal error of 4%. With the above assumptions, the required sample size was 354 newborns, and by taking an additional 10% compensation for non-respondents’, the total sample size was 390 mother-child pairs.
We selected by default one general Hospital from each zone, as three of them have one general Hospital except West Wollega, which have two general Hospitals (Gimbi and Nedjo General Hospitals) where we purposively selected Nedjo General Hospital because of better client flow. The determined sample was allocated proportionally to each Hospital based on the childbirth flow throughout the year before the data collection. Accordingly, 135 from Nekemte, 116 from Dembidollo, 54 from Shambu, and 85 from Nedjo Hospitals mother-child pairs were included in the study using systematic random sampling methods. The systemic sampling method was implemented in each Hospital separately based on monthly childbirth flow and in an interval of three for Nekemte and Dembidollo Hospitals. At the same time, every other delivery was observed at Nedjo and Shambu General Hospitals after the first births were included by lottery in all cases. The data collectors randomly selected childbirth to be observed when they encountered more than one delivery simultaneously.
Data Collection and Instrumentation
A checklist adopted from the WHO essential newborn care protocol was used to observe services provided for the newborns. Data about service provision were collected by following and evaluating the services offered by delivery attendants. Maternal background characteristics were collected from the mothers at the end of the observation while they were in the postnatal ward. Non-participatory observations employed without exposing the information to the care providers, and the providers did not know as they have been observed for the service they were providing. The data collectors were Intern BSc midwifery students from Wollega University who were not involved in attending delivery while collecting the data.
Independent Variables
Independent variables were identified based on previous studies conducted on essential newborn care. We grouped these variables into two categories that include sociodemographic factors and obstetric factors. Sociodemographic factor includes maternal age, educational status, marital status, place of residence, and income. To identify the economic status of the parents of the neonate, we asked the mother for the average annual income. The participants’ yearly income was categorized into five quantiles from lowest to highest categories through univariate analysis. Obstetric factors include the parity, number of previous alive children the mother had, the gestational age of the recent birth, and the presence of an assistant. Additional variables we assessed include maternal HIV status of the mother, day and time of delivery.
Data Quality Management and Analysis
One Matron Nurse supervised the whole data collection in each hospital. All data collectors and supervisors were given training about the essential newborn care before their engagement in the data collection process. After data collection, data were checked for completeness by supervisors and investigators. The data were then cleaned, coded, and entered into Epi-info Version 7 and exported to STATA version 13 for analysis.
To assess factors associated with essential newborn care, we used binary logistic regression models. Four models were built to identify the factors associated with keeping the newborn warm, helping baby breathe, helping baby feed, and disease prevention. We were unable to build the model for keeping the baby clean because of insufficient sample size; in our case, a minimal number of neonates were kept clean. We first conducted bivariable logistic regression with each potential risk factor, and those independent variables, which had p-values less than 0.2 were taken into multivariable logistic regression in all models to control the effects of confounding variables. The models’ fitness was assessed by Hosmer and Lemeshow goodness of fit test. The adjusted odds ratios (AOR) with 95% Confidence Intervals (CI) and p-values of less than or equals to 0.05 measured factors significantly associated with each category of essential newborn care. The detailed findings of the study are presented using tables, graph, and texts.
Results
Sociodemographic and Economic Characteristics of Newborns Mothers
We observed 375 childbirths that were included in the analysis. Nearly three out of four women were between the ages of 20 and 29 with a median age of 25 years old, the Interquartile range of 7 years at childbirth, and minimum age 18 and a maximum 42years. The majority of the women were married 351 (93.6%), 320 (85.3%) were Oromo, and 214 (57.1%) were protestant religion followers. About one-fourth (24.5%) of all women did not attend any formal education, while nearly half 183 (48.8%) of the total women were not employed. Regarding the residence of the women 196 (52.3%) were from rural and 86 (22.9%) of them were in lower economic status (Table 2).
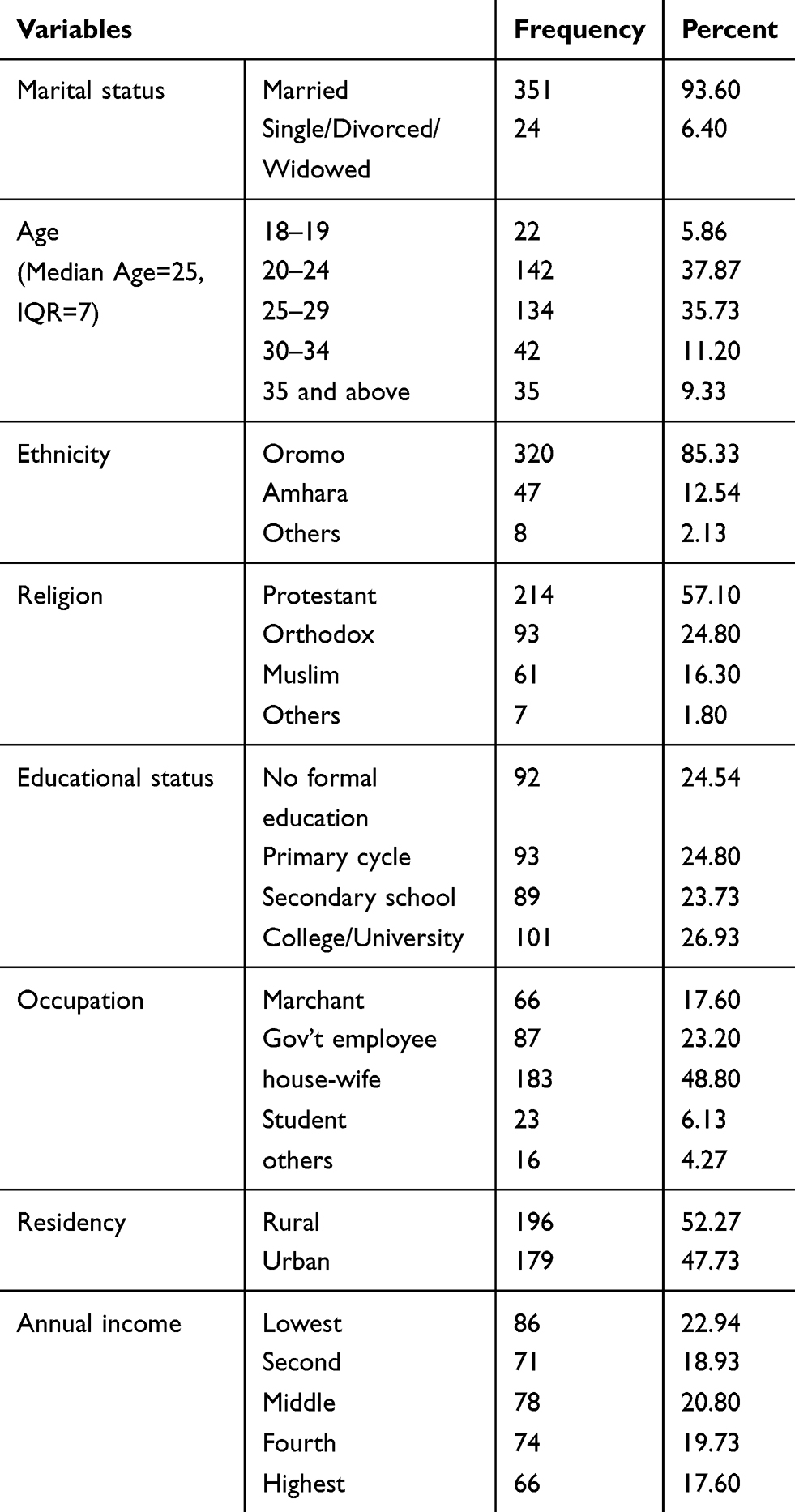 |
Table 2 Sociodemographic and Economic Status of the Mothers’ of the Newborns That Childbirth Attended at Hospitals of Wollega Zones, West Ethiopia, 2017 (n=375) |
Obstetrics Characteristics
Nearly one out of three mothers (31.7%) were prime parous, and one out of every 10 (n=41, 10.9%) mothers have four and above children. The majority of the indexed deliveries (n=304, 81.1%) took place at term with the mean gestational age of 39.0 weeks, and most of the mothers gave childbirth on working 240 (64.0%) and in the daytime 236 (62.9%). Nearly one out of four childbirth attendants 96 (25.6%) had no assistant (Table 3).
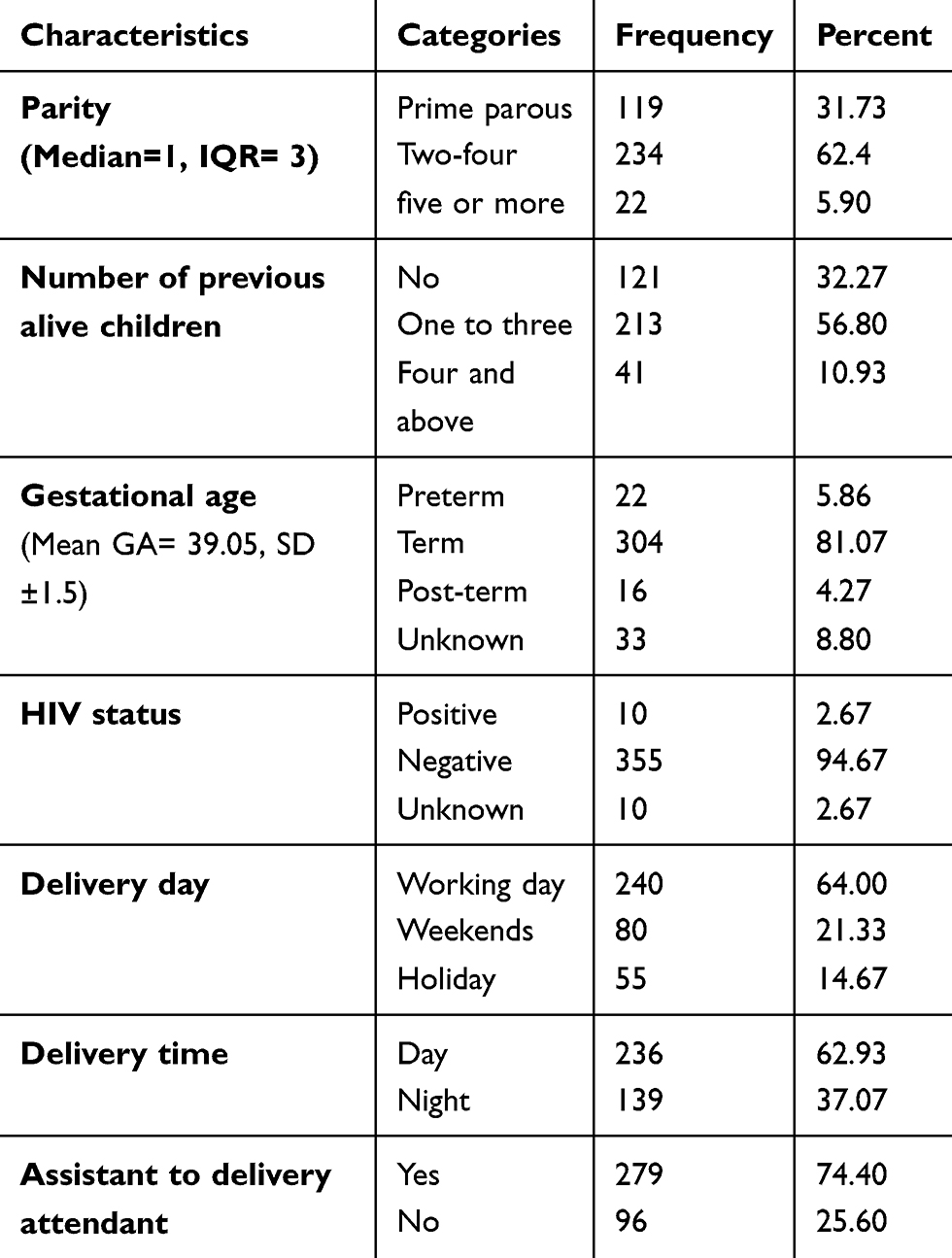 |
Table 3 Obstetric and Related Factors of the Women Give Childbirth at Hospitals of Wollega Zones, West Ethiopia, 2017 (n=375) |
Proportions of Provided Essential Newborn Care
Overall only 11 (2.9%, 95% CI [1.65, 5.2]) newborns received essential newborn care immediately after delivery. The composite categories of essential newborn care given for neonates lie between 14 (3.7%) to 315 (84.0%) for keeping newborns clean and helping newborns to feed, respectively. From individual elements of the categories under each composite category range from very low in the skin to skin practice (8.8%) and as high as 100% for cord clamping. Among indicators of keeping newborn clean, about 98.9% of the cord-cutting was undertaken by sterile scissors or blade, while only 6.1% of care providers washed their hands with soap and water before starting to give eye care (see Figure 1).
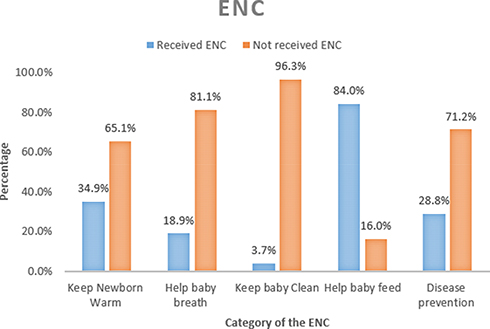 |
Figure 1 Immediate Essential Newborn Care Service provided to newborns at Hospitals, output of composite observation for each category, West Ethiopia, 2017. |
Early initiation of breastfeeding was found to be the most practiced essential newborn care, about 315 (84.0%, 95% CI [80.0, 87.4]) newborns were initiated to breastfeeding within 1 hr of delivery. From the neonates that did not initiate breastfeeding within 1 hr, 19 (31.7%) were given resuscitation and unstable even after the procedure, and breastfeeding was not possible in the first hour of life.
The thermal care was provided to 131 (34.9%, 95% CI [30.3, 39.9]) newborns. The overall composite indicators for helping baby to breathe and keeping the baby clean were found to be 89 (23.7%, 95% CI [19.7, 28.3] and 14 (3.7%, 95% CI [2.14, 6.0]) respectively. About 55 (14.7%) neonates needed resuscitation to breathe spontaneously. The remaining immediate essential newborn care category that healthcare providers need to give for the neonates is providing disease prevention measures like eye care and vitamin K provision, which found to be 108 (28.8%, 95% CI [24.4, 33.6]) (Table 4).
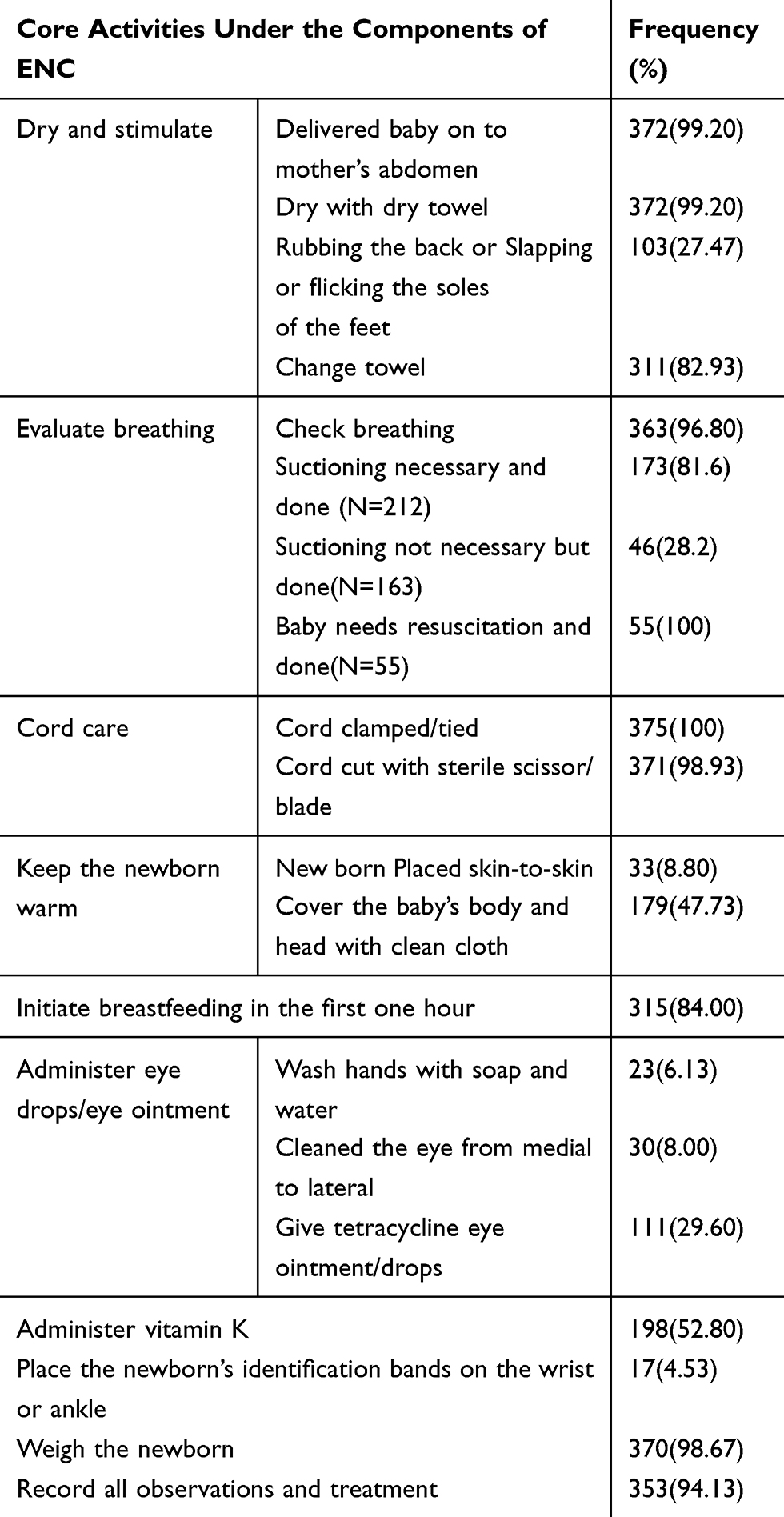 |
Table 4 Description of Sub-Components of Essential Newborn Care at Hospitals of Wollega Zones, West Ethiopia, 2017 (n=375) |
Factors Predicting Immediate Essential Newborn Care
In bi-variable logistic regression, maternal age, maternal employment status, wealth quantile, the timing of delivery, number of the child alive, presence of assistant, and the need for resuscitation were associated with each immediate essential newborn care a p-value less than 0.2.
Neonates born to richer mothers (AOR= 2.8, 95% Confidence Interval (CI) [1.4, 5.7]) and highest (AOR=2.4, 95% CI [1.1, 5.4]) annual income, birthday on weekends (AOR=1.9, 95% CI [1.0, 3.6]), presence of assistants to the delivery attendant (AOR=1.8, 95% CI [1.0, 3.6]) and resuscitation (AOR= 4.1, 95% CI [2.1, 8.1]) were significantly associated with keeping newborn warm. Presence of the assistants to the delivery attendant (AOR=3.7, 95% CI [1.7, 7.8]) and resuscitation (AOR= 2.5, 95% CI [1.3, 4.7]) were significantly associated with helping the baby breathe at p-value less than 0.05 (see Table 5).
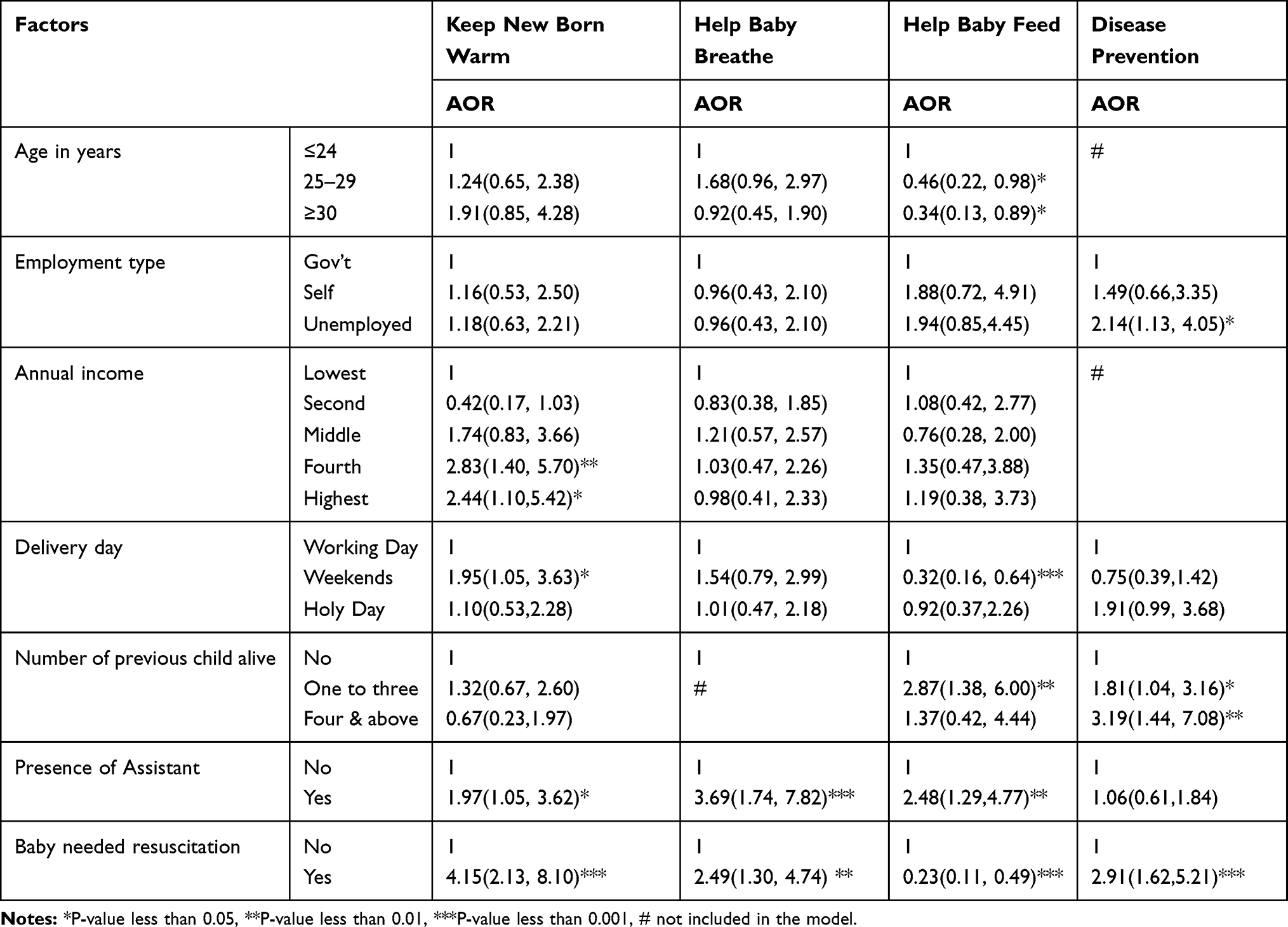 |
Table 5 Multivariate Logistic Regression Model Analysis of Factors Associated with ENC Service Provision to Newborns Delivered at Hospitals of Wollega Zones, Western Ethiopia, 2017 |
Neonates born to mothers in the age range of 25–29 (AOR= 0.46, 95% CI [0.2, 0.9]) and 30 and above (AOR=0.3, 95% CI [0.1, 0.9]), birth day on weekends (AOR=0.3, 95% CI [0.2, 0.6]), having three and less children (AOR= 2.9, 95% CI [1.4, 6.0]), presence of assistants to delivery attendant (AOR= 2.5, 95% CI [1.3,4.8]) and resuscitation (AOR= 0.2, 95% CI [0.1, 0.5]) were significantly associated with helping baby feed while unemployed mothers (AOR= 2.1, 95% CI [1.1, 4.0]), having three and less (AOR= 1.8, 95% CI [1.0, 3.2]) and four and above (AOR= 3.2, 95% CI [1.4, 7.1]) children and need of resuscitation (AOR= 2.9, 95% CI [1.6, 5.2]) were significantly associated with disease prevention practice at p-value less than 0.05 as noted in Table 5.
Discussion
Out of 375 observed childbirths, only 11 (2.9%, 95% CI [1.65, 5.17]) neonates received all components of immediate essential newborn care. The result of essential newborn care provision we observed in this study is an aggregate of all essential newborn cares, discussed in subsequent paragraphs. A total of 315 (84.0%, 95% CI [80.03, 87.45]) newborns started feeding breast milk within 1 hr which is comparable with the study conducted in Northeast Ethiopia,24 by the initiatives of health-care providers or mothers themselves. Even though early initiation of breastfeeding was found higher than other findings,25,26 it was not adequate as every child needs to get breastfeeding as early as possible after delivery, preferably within 1 hr of birth. Instability of some neonates after delivery contributed to the increment of the neonates those who did not feed breast early. Delaying breastfeeding exposes the neonate to be at higher risk of morbidity and mortality.27,28 Therefore, to prevent these devastating results in neonates, early initiation of breastfeeding is mandatory as it contains all the nutrients the infants need in the first 6 months of life.29
The thermal-care was provided to 131 (34.93%, 95% CI [30.28, 39.89]) newborns. This finding is much lower than other results in Ethiopia30,31 and abroad,32,33 the difference could be due to the way other studies assessed thermal care. Those studies measured thermal care using a single practice like rubbing of the child after delivery. At the same time evaluated the condition after observing an additional element of keeping newborn warm which includes initiating the neonate, checking for breathing and suctioning on demand. Perhaps it could also be due to health service delivery difference between the study area and facilities. But it is in line with the report from Ghana,34 as they used a composite scale to measure the implementation of newborn care.
The neonates born to mothers who had a better annual income received more care than those whose mothers are in the lowest annual income. When it comes to demanding attention from health-care providers, the client with low financial capacity tends to relate every service with the payments. As a result, they shy away from requesting care,35 which was also observed in the context of this study. Unlike indigent clients, individuals from higher economic status demand a high level of care, and they might obtain better care for their newborns. Mothers who have high financial income are more likely to higher education and awareness regarding the cares needed for their neonates, and they will seek more attention as compared to those in low economic status. Childbirth assisted skilled attendants were kept warm twice more likely than their counterparts. Similarly, neonates, those required the resuscitation were kept warm four times than those who did not. Neonates those in need of resuscitations are more susceptible to further complications like hypothermia, and so they might receive more attention to prevent hypothermia through various thermal care.
While the fetus is in the uterus, the fetal lung and other respiratory tract are not functional until the baby starts to take the first breath after delivery.36 The delivery attendant needs to assists the baby to starts its breathing through immediate newborn care; otherwise, the neonate’s life will be endangered, mainly if there was meconium aspiration.37,38 Related to this, 89 (23.73%, 95% CI [19.71, 28.29]) babies received cares to strengthen the efforts of the babies to breathe, help the baby to breathe. Though there had been similar evidence about the importance of this care,10,39 the newborn care to support a child to breathe in this study was low. It could be attributed to lack of in-service help baby breathe training for midwives and other care providers those involved in attending childbirth, which needs immediate attention.
As the maternal age increases, the probability of having more childbirth increases, and so do the experiences they have for neonatal care as supported by a study from Ghana.34 In our study, maternal age was found to be an independent predictor for helping baby feed. In contrast to those mothers who have the high number of children, which might make them fade up to feed their newborns, the mothers in their young age practiced newborn feeding in the first hour of the birth of the child. The instability of the neonate and necessity of resuscitation minimized the probability of breastfeeding because, the resuscitation procedure might take longer even more than 1 hr, which could contribute for delay of the breastfeeding within 1 hr if the baby stays unstable after resuscitation. Similarly, the presence of assistance, the need for resuscitation increased their probability to receive care related to helping the baby breathe.
Keeping the baby clean 14 (3.7%, 95% CI [2.1, 6.0]) was found to be notably lower than other studies,30,31,34 probably because we did not assess the cleanness of care unlike those studies merely by considering clean cord care. Even though handwashing is the most valuable practice in infection prevention, most of the care providers observed in this study failed to do so. The providers did not practice handwashing, notably after they conducted delivery. The reason might be because most of the providers washed their hands at the beginning of assisting birth and proceed to baby care by changing their glove instead of washing their hands for the second time before touching the baby. Such behavior might arise from lack of water source or alternative ways of handwashing in the facilities, but not applies for all. There might be individuals lacking the passion of adhering to the standard of care due to negligence or other personality reasons. Such individual behavior could expose newborns to potentially infectious disorders originating from their mothers or other nosocomial infections.
In another way, disease prevention measures like eye care with tetracycline 1% eye ointment and vitamin K provision not given for all newborns, as only 108 (28.8%, 95% CI [24.4, 33.5]) newborns received both. This finding is lower than in other previous studies.17,31 In Ethiopia, regular working days are from Monday to Friday, at which public facilities operate routine services, including health facilities. Weekends and holidays covered as duty days and, during these days, the numbers of health-care providers assigned to health facilities are limited, so do the care provided for neonates. In agreement with this, the neonates born during the weekends did not start breastfeeding early after delivery as compared to those who born on working days.
The finding of this study may be better if we also identified the gap of service provision from health-care providers. So, we recommend further investigations which encompass the view of health-care providers on immediate essential newborn care for further actions needed to be delivered.
Conclusions
The immediate essential newborn cares provided for neonates delivered at hospitals we observed were poor per the expectations of the service for every neonate. The importance of keeping infection prevention and patient safety principle need to be implemented with all care providers comprehensively. Hospital administrators need to consider enhancing the number and skill of delivery attendants through providing in-service training on essential newborn care, and enforcing implementations of essential newborn care standards is mandatory to protect the life of neonates.
Abbreviations
AOR, adjusted odds ratio; BEmONC, basic emergency obstetrics and newborn care; CEmONC, comprehensive emergency obstetrics and newborn care; CI, confidence interval; ENC, essential newborn care; HSTP, health sector transformation plan; NMR, neonatal mortality rate; SSA, Sub-Saharan Africa; SDG, sustainable development goals; WHO, World Health Organization.
Ethics Approval and Informed Consent
We obtained the ethical clearance from the Institutional Review Committee of Wollega University and, the letter of this review was given to the hospital administrator. We received permission from hospital managers to proceed with our investigations. Observational data were collected blindly without informing the service provider to reduce the bias during data collection, which was approved by the ethical review committee of the Wollega University. The results of the observation could have been affected if the providers knew that the childbirth was under investigation. The review committee took this under consideration and approved the data collection through observation of actual service delivery. The data collectors explained the aim of the study to the mothers and received written informed consent from each mother after childbirth to collect data related to sociodemographic status and obstetric related variables. Therefore, we confirm that our study was conducted in accordance to the Declaration of Helsinki.
Acknowledgments
We want to thank Wollega University for the financial support for the study. Our gratitude also goes to administrators of hospitals where the study took place, and data collectors, supervisors, and participants.
Author Contributions
All authors made a significant contribution in the article in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chomba E, McClure EM, Wright LL, Carlo WA, Chakraborty H, Harris H. Effect of WHO Newborn Care Training on Neonatal Mortality by Education. Ambul Pediatr. 2008;8(5):300–304. doi:10.1016/j.ambp.2008.04.006
2. WHO. WHO recommendations on Postnatal care of the mother and newborn 2013. World Heal Organ [Internet]; 2013 1–72. Available from: http://apps.who.int/iris/bitstream/10665/97603/1/9789241506649_eng.pdf.
3. Akter T, Dawson A, Sibbritt D. What impact do essential newborn care practices have on neonatal mortality in low and lower-middle income countries? Evidence from Bangladesh. Journal of Perinatology. 2016 Mar;36(3):225–30.
4. Save the Children. Surviving the First Day: State of the World’s Mothers 2013. Westport, CT; 2013.
5. Hug L, Alexander M, You D, Alkema L. National, regional, and global levels and trends in neonatal mortality between 1990 and 2017, with scenario-based projections to 2030: a systematic analysis. Lancet Glob Heal [Internet]. 2019;7(6):e710–20. doi:http://dx.doi.10.1016/S2214-109X(19)30163-9
6. WHO. Postnatal Care: opportunities for Africa’s Newborns [Internet]; 2016. Available from: http://www.who.int/maternal_child_adolescent/topics/newborn/postnatal_care/en/.
7. Ma LH, Alexander M, You D, Alkema L, Group UNI, Estimation M. Articles National, regional, and global levels and trends in neonatal mortality between 1990 and 2017, with scenario-based projections to 2030: a systematic analysis. Lancet Glob Heal. 2019;7(6):e710–20. doi:http://dx.doi.10.1016/S2214-109X(19)30163-9
8. Central Statistical Agency. [Ethiopia] and ICF International. 2012. Ethiopia Demographic and Health Survey 2011. Addis Ababa, Ethiopia and Calverton, Maryland, USA: Central Statistical Agency and ICF International.
9. Central Statistical Agency (CSA) [Ethiopia] and IC. Ethiopia Demographic and Health Survey 2016: Key Indicators Report. Ethiopia, and Rockville, Maryland, USA. CSA and ICF: Addis Ababa; 2016.
10. Enweronu-Laryea C, Robertson NJ. Helping babies breathe can reduce deaths with the right combination of training and expertise. Acta Paediatr Int J Paediatr. 2017;106(10):1552–1553. doi:10.1111/apa.13988
11. Mahmood I, Jamal M, Khan N. Effect of mother-infant early skin-to-skin contact on breastfeeding status: a randomized controlled trial. J Coll Physicians Surg Pak. 2011;21:601–605. doi:10.2011/JCPSP.601605
12. WHO. Protecting, promoting and supporting breastfeeding in facilities providing maternity and newborn services: the revised: baby-friendly Hospital Initiative [Internet]. Who; 2017. 1–136 p. Available from: http://apps.who.int/iris/bitstream/handle/10665/259386/9789241550086-eng.pdf;jsessionid=8060A65B979756A6CBE752A434EE3ACA?sequence=1%0Ahttp://apps.who.int/iris/bitstream/handle/10665/259386/9789241550086-eng.pdf?sequence=1%0Ahttp://www.who.int/elena/titles.
13. Khan J, Vesel L, Bahl R, Martines JC. Timing of Breastfeeding Initiation and Exclusivity of Breastfeeding During the First Month of Life: effects on Neonatal Mortality and Morbidity—A Systematic Review and Meta-analysis. Matern Child Health J. 2014;19(3):468–479. doi:10.1007/s10995-014-1526-8
14. Van Den Broek NR, Graham WJ. Quality of care for maternal and newborn health: the neglected agenda. BJOG An Int J Obstet Gynaecol. 2009;116(SUPPL. 1):18–21. doi:10.1111/j.1471-0528.2009.02333.x
15. Wall SN, Lee AC, Carlo W, Goldenberg R, Niermeyer S, Darmstadt GL, Keenan W, Bhutta ZA, Perlman J, Lawn JE. Reducing intrapartum-related neonatal deaths in low-and middle-income countries—what works?. In Seminars in perinatology 2010 Dec 1;34(6):395–407. WB Saunders.
16. Getachew A, Ricca J, Cantor D, et al. Quality of Care for Prevention and Management of Common Maternal and Newborn Complications: a Study of Ethiopia ’ s Hospitals. Matern Chid Heal Integr Progr. 2011;61.
17. Sobel HL, Silvestre MAA, Mantaring JBV, Oliveros YE, Nyunt-U S. Immediate newborn care practices delay thermoregulation and breastfeeding initiation. Acta Paediatr Int J Paediatr. 2011;100(8):1127–1133. doi:10.1111/j.1651-2227.2011.02215.x
18. MOH. Health Sector Transformation Plan. Addis Ababa: Ethiopian Federal Ministry of Health (FMOH). 2015.
19. Misgna HG, Gebru HB, Birhanu MM. Knowledge, practice and associated factors of essential newborn care at home among mothers in Gulomekada District, Eastern. BMC Pregnancy Childbirth. 2016. 1–8
20. Berhea TA, Belachew AB, Abreha GF. Knowledge and practice of Essential Newborn Care among postnatal mothers in Mekelle City, North Ethiopia: A population-based survey. 2018 Aug;13(8):e0202542.
21. Chichiabellu TY, Mekonnen B, Astawesegn FH, Demissie BW, Anjulo AA. Essential newborn care practices and associated factors among home delivered mothers in Damot pulasa Woreda, southern Ethiopia. Reproductive health. 2018 Dec 1;15(1):162.
22. Mersha A, Assefa N, Teji K, Shibiru S, Darghawth R, Bante A. Essential newborn care practice and its predictors among mother who delivered within the past six months in Chencha District, Southern Ethiopia, 2017. PloS one. 2018 Dec 11;13(12):e0208984.
23. Basic Emergency Obstetrics and Newborn Care (BEmONC). Training Manual [Internet]. Ethiopia:Addis Ababa; 2013. Available from: http: pdf.usaid.gov/pdf.docs/PA00JX4F.pdf.
24. Semanew Y, Etaye M, Tizazu A, Abebaw D, Gebremedhin T. Newborn care practices and its determinants among postnatal mothers in Dessie Referral Hospital, Northeast Ethiopia. BMC Res Notes. 2019;12(1):1–6. doi:10.1186/s13104-019-4133-3
25. Ekubay M, Berhe A, Yisma E. Initiation of breastfeeding within one hour of birth among mothers with infants younger than or equal to 6 months of age attending public health institutions in Addis Ababa, Ethiopia. Int Breastfeed J. 2018;13(1):1–7. doi:10.1186/s13006-018-0146-0
26. Tariku A, Biks GA, Wassie MM, Worku AG, Yenit MK. Only half of the mothers practiced early initiation of breastfeeding in Northwest Ethiopia, 2015. BMC Res Notes. 2017;10(1):1–7. doi:10.1186/s13104-017-2823-2
27. Smith ER, Hurt L, Chowdhury R, Sinha B, Fawzi W, Edmond KM. Delayed breastfeeding initiation and infant survival: A systematic review and meta-analysis. PLoS One. 2017;12(7):1–16.
28. Edmond KM. Delayed Breastfeeding Initiation Increases Risk of Neonatal Mortality. Pediatrics. 2006;117(3):e380–6.
29. Walker A. Breast Milk as the Gold Standard for Protective Nutrients. J Pediatr. 2010;156(2 SUPPL.):S3–7. doi:http://dx.doi.10.1016/j.jpeds.2009.11.021
30. Callaghan-koru JA, Rawlins B, Callaghan-koru JA, et al. Newborn care practices at home and in health facilities in 4 regions of Ethiopia. BMC Pediatrics. 2013;13. doi:10.1186/1471-2431-13-198
31. Berhe M, Medhaniye AA, Kahsay G, Birhane E, Abay M. Essential neonatal care utilization and associated factors among mothers in public health facilities of Aksum Town, North Ethiopia, 2016. PLoS One. 2017;12(4):1–11. doi:10.1371/journal.pone.0175902
32. Khanal V, Gavidia T, Adhikari M, Mishra SR, Karkee R. Poor thermal care practices among home births in nepal: further analysis of nepal demographic and health survey 2011. PLoS One. 2014;9:2. doi:10.1371/journal.pone.0089950
33. Sami S, Kerber K, Kenyi S, et al. State of newborn care in South Sudan’s displacement camps: A descriptive study of facility-based deliveries. Reprod Health. 2017;14(1):1–12. doi:10.1186/s12978-017-0417-z
34. Saaka M, Ali F, Vuu F. Prevalence and determinants of essential newborn care practices in the Lawra District of Ghana. BMC Pediatr. 2018;18(1):1–12. doi:10.1186/s12887-018-1145-4
35. Pega F, Valentine NB, Rasanathan K, et al. The need to monitor actions on the social determinants of health. Bull World Health Organ. 2017;95(11):784–787. doi:10.2471/BLT.16.184622
36. Ryan G, Somme S, Crombleholme TM. Airway compromise in the fetus and neonate: prenatal assessment and perinatal management. Semin Fetal Neonatal Med. 2016 Aug 1;21(4):230–239 WB Saunders.
37. Ryan G, Somme S, Crombleholme TM. Airway compromise in the fetus and neonate: prenatal assessment and perinatal management. Semin Fetal Neonatal Med. 2016;21(4):230–239doi:10.1016/j.siny.2016.03.002
38. Lee J, Romero R, Lee KA, et al. Meconium aspiration syndrome: A role for fetal systemic inflammation. Am J Obstet Gynecol. 2016:214(3); 366.e1366.e9.
39. Claassen CC, Largaespada-Beer N, Mendez-Peraza E, et al. Belize National Implementation of Helping Babies Breathe and Essential Care for Every Baby Programs. Pediatrics. 2018:141(1) Meeting Abstract; 454 LP454.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.