")
Back to Journals » International Medical Case Reports Journal » Volume 14
Poor Outcome in Camel-Related Eye Trauma with Ruptured Globe
Authors Albazei AI, Ahmed OH, AlAli NM, Alselaimy RM, Alreshidi SO, Magliyah MS , Albalawi HB
Received 3 February 2021
Accepted for publication 17 March 2021
Published 7 April 2021 Volume 2021:14 Pages 219—222
DOI https://doi.org/10.2147/IMCRJ.S305158
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Alanuad I Albazei,1 Omar H Ahmed,1 Naif M AlAli,2 Ruba M Alselaimy,3 Shaker O Alreshidi,4 Moustafa S Magliyah,5,6 Hani B Albalawi2
1Department of Ophthalmology, King Khalid Hospital, Tabuk, Saudi Arabia; 2Department of Ophthalmology, Tabuk University, Tabuk, Saudi Arabia; 3Faculty of Medicine, King Saud University, Riyadh, Saudi Arabia; 4Almajmaah University, Almajmaah, Saudi Arabia; 5Department of Ophthalmology, Prince Mohammed Medical City, Aljouf, Saudi Arabia; 6Vitreoretinal Division, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia
Correspondence: Moustafa S Magliyah
Vitreoretinal Division, King Khaled Eye Specialist Hospital, Al- Oruba Street, PO. Box 7191, Riyadh, 11462, Saudi Arabia
Tel +966 11 482 1234 Ext. 2655
Fax +966 11 4821234 Ext. 2764
Email [email protected]
Purpose: To report the poor visual outcome of ruptured globe caused by camel bites.
Observations: A 48-year-old camel caregiver presented to the emergency department after being bitten by a camel in the left side of his face. Ophthalmic examination revealed a superior scleral wound from 9 to 2 o’clock, about 6 mm from the limbus extending to the equator with prolapse of uveal and vitreous tissues, an opaque cornea, total hyphema, diffuse subconjunctival hemorrhage, and a lower lid laceration involving the lid margin and the nasolacrimal duct. The patient has undergone surgical repairs of ruptured globe and lid laceration, followed by retinal detachment surgery. Following these surgical interventions, the patient preserved a light perception vision with flat retina.
Conclusion: Camel-related injuries might primarily involve the ophthalmic structures, especially in camel bites. Camel-related eye trauma might lead to poor visual and anatomical outcomes which might not improve following surgical interventions.
Keywords: camel attack, ruptured globe, trauma, retinal detachment, animal-related injury, camel-related injury
Plain Language Summary
Camel-related injuries can be life threatening and in globe-involving cases, poor visual and anatomical outcomes. This case shows that serious visual and anatomical consequences might not improve following surgical interventions.
Introduction
Human eye is the third most commonly affected organ by traumatic injuries after upper and lower extremities.1 Outcomes of ocular trauma are variable and might end up with total blindness. In fact, trauma is considered to be a major cause of global blindness, affecting 1.6 million people worldwide.2 The prevalence of unilateral vision loss in Saudi Arabia caused by eye trauma is about 6.8/1000 persons.3,4 Animal-related injuries (ARI) vary according to the type of animal and its availability in the community. Camel, which is a commonly raised domestic animal in Saudi Arabia might lead to ARI. Camel-related injury (CRI) is the most common cause of ARI in Saudi Arabia, comprising 77% of all ARI and about 15% of CRI are bite injuries.5
Camel bite injuries can lead to severe maxillofacial injuries including injuries to the orbit, nose, mandible, and zygoma. However, the clinical and visual outcomes of these injuries are not well described with only few cases documented in the literature. For humans interacting with or taking care of camels, a higher incidence of camel bite injuries is believed to increase during the breeding season which is from December to March. During breeding season, male camels become more aggressive and difficult to handle.6 This poses a higher risk for camel caregivers to CRI, including bite injuries. In this paper, we report the visual and anatomical outcomes in a camel caregiver who was bitten by a camel.
Case Report
A 48-year-old male camel caregiver presented to the emergency department of King Khalid Hospital in Tabuk city 2 hours after being bitten on the left side of his face and the left eye by a 13-year-old camel. The injury has occurred in the desert pasture while the shepherd was trying to feed the camel. The camel became aggressive and gripped the caregiver’s face.
Upon general examination, he was conscious, oriented, distressed and vitally stable There were multiple lacerations on the left side of his face and multiple fractures in the left forearm.
The patient had 20/20 vision in the right eye and light perception (LP) vision in the left eye. Biomicroscopic examination of the right eye was normal, while in the left eye showed superior scleral wound from 9 to 2 o’clock, about 6 mm from the limbus extending to the equator with prolapse of uveal and vitreous tissues, an opaque cornea, total hyphema, diffuse subconjunctival hemorrhage, and a lower lid laceration involving the lid margin and the nasolacrimal duct (Figure 1).
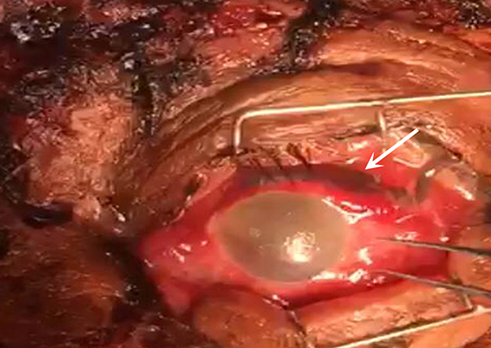 |
Figure 1 Anterior segment photo of the left eye taken intraoperatively showing superior scleral wound with uveal prolapse (arrow), corneal edema and subconjunctival hemorrhage. |
The patient was given a 0.5 mL tetanus toxoid vaccine intramuscularly and was admitted to the hospital. Computed tomography (CT) showed ruptured left globe (Figure 2). Prophylactic vancomycin and ceftazidime were given intravenously for 5 days. The patient was taken to the operation room and a primary repair of the ruptured globe was performed with excision of exposed dead uveal tissue, and closure of the lower lid laceration.
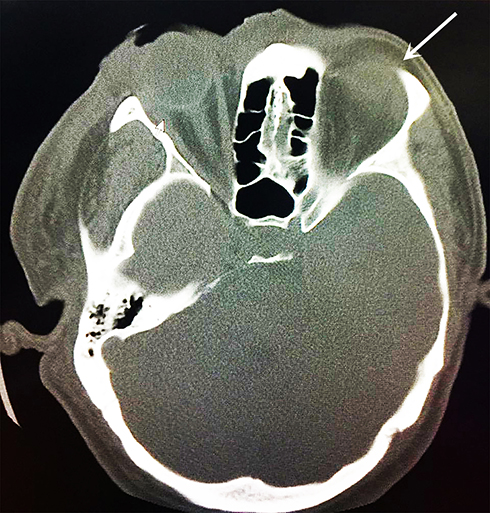 |
Figure 2 Computed tomography (CT) of the brain and orbit showing ruptured globe on the left side (arrow). |
Examination of the left eye on the first postoperative day revealed light perception vision with an edematous hazy cornea, preventing further view to the anterior chamber and fundus. Ultrasound B-scan imaging revealed a total rhegmatogenous retinal detachment (RRD) (Figure 3). Pars plana vitrectomy with silicone oil tamponade was performed and the patient preserved LP vision with a flat retina in the left eye for 6 months after the second surgical intervention.
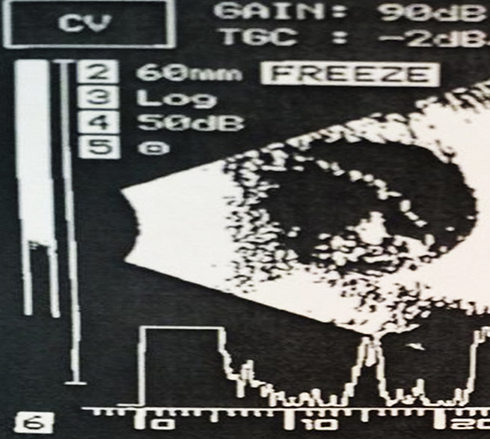 |
Figure 3 Ultrasound B-scan of the left eye showing a total rhegmatogenous retinal detachment. |
Discussion
In Saudi Arabia, camels are used as a source of milk, food, and for racing competitions. About 77% of ARI in Saudi Arabia are camel related. Camel caregivers are believed to be more prone to CRI, especially male camels.5
Majority of CRI occurs during the breeding season which is from December to March when male camels become more aggressive and might behave unpredictably.6 In our case, the CRI occurred during in February at the midst of the breeding season.
CRI can cause serious and life-threatening traumatic injuries, as camels have special dentation. Anatomical dental structure of camels includes around 34 teeth including four sharp and long canine teeth in mature camels. Also, camels have strong jaw which can open widely helping them to exert high pressure leading to serious injuries. There is variation in camel bite injury and they vary from small wounds to extensive lacerations. The mechanism of a camel bite is characterized by its complexity as injuries do not result from the bite only. Camel bites might involve shaky movements and pulling of bitten human parts which might lead to serious life-threatening injuries including head trauma and intracranial bleeding.7
Balac et al reported the only case of a ruptured globe in the literature that caused by a camel bit that end-up by evisceration.8 Unlike the previous report, the globe was preserved in our case and ended up with light-perception vision. Both cases show that a CRI with ruptured globe might lead to deleterious visual outcomes. To the best of our knowledge, this is the first case reported in Saudi Arabia and the second case reported worldwide of a camel-related eye injury.
Conclusion
This case serves as a reminder that camel bite may result in serious sequelae affecting the patient’s quality of life. Moreover, it also emphasizes that recognizing different mechanisms of injury and vulnerable groups is important for effective prevention strategies. Camel caregivers are considered to be at risk of such injuries and attention and education are needed to maintain their safety especially during the breeding season.
Abbreviations
ARI, animal-related injury; CRI, camel-related injury; CT, computed tomography; LP, light perception; RRD, rhegmatogenous retinal detachment.
Ethics Statement
This study was conducted in compliance with the Declaration of Helsinki. The patient has provided written informed consent for publication of this case, his details and accompanying images. This project was exempted from review by the institutional review board at Tabuk university.
Consent for Publication
Written informed consent for publication of this case, his details and accompanying images was obtained.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that this study has received no financial support.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Norbder E. Injuries as a public health problem in subSaharan Africa: epidemiology and prospects for control. East Afr Med J. 2000;77(1):1–43.
2. MacEwen CJ. Ocular injuries. J R Coll Surg Edinb. 1999;44(5):317–323.
3. Ballal SG. Ocular trauma in an iron forging industry in the eastern province, Saudi Arabia. Occup Med (Chic Ill). 1997;47(2):77–80. doi:10.1093/occmed/47.2.77
4. Tabbara KF, Ross-Degnan D. Blindness in Saudi Arabia. JAMA. 1986;255(24):3378–3384. doi:10.1001/jama.1986.03370240048035
5. Janjua KJ, Van den Berg AA. Animal injuries presenting to Riyadh Armed Forces Hospital: a survey. Trop Doct. 1994;24(2):84. doi:10.1177/004947559402400220
6. Kain R, Arya S. Camel bite: an uncommon mode of maxillofacial injury, its mechanism and fatality: case series and review of literature. Natl J Maxillofac Surg. 2015;6(2):172. doi:10.4103/0975-5950.183868
7. Abu-Zidan FM, Eid HO, Hefny AF, Bashir MO, Branicki F. Camel bite injuries in United Arab Emirates: a 6 year prospective study. Injury. 2012;43(9):1617–1620. doi:10.1016/j.injury.2011.10.039
8. Balac K, Al-Ali MA, AlMahmoud T, Abu-Zidan FM. Globe rupture caused by a camel bite. Trauma Case Rep. 2019;21:100202. doi:10.1016/j.tcr.2019.100202
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.