")
Back to Journals » OncoTargets and Therapy » Volume 9
Polymorphisms in pre-miRNA genes and cooking oil fume exposure as well as their interaction on the risk of lung cancer in a Chinese nonsmoking female population
Authors Yin Z , Li H, Cui Z, Ren Y, Li X, Wu W, Guan P, Qian B, Rothman N, Lan Q, Zhou B
Received 22 September 2015
Accepted for publication 30 November 2015
Published 19 January 2016 Volume 2016:9 Pages 395—401
DOI https://doi.org/10.2147/OTT.S96870
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jianmin Xu
Zhihua Yin,1,2 Hang Li,1,2 Zhigang Cui,3 Yangwu Ren,1,2 Xuelian Li,1,2 Wei Wu,1,2 Peng Guan,1,2 Biyun Qian,4 Nathaniel Rothman,5 Qing Lan,5 Baosen Zhou1,2
1Department of Epidemiology, School of Public Health, China Medical University, 2Key Laboratory of Cancer Etiology and Intervention, University of Liaoning Province, 3China Medical University, Shenyang, 4Department of Epidemiology, School of Public Health, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 5Division of Cancer Epidemiology and Genetics, National Cancer Institute, Bethesda, MD, USA
Background: MicroRNAs (miRNAs) are suggested to be very important in the development of lung cancer. This study assesses the association between polymorphisms in miRNA-related (miR)-26a-1, miR-605, and miR-16-1 genes and risk of lung cancer, as well as the effect of gene–environment interaction between miRNA polymorphisms and cooking fume exposure on lung cancer.
Methods: A case–control study including 268 diagnosed nonsmoking female lung cancer patients and 266 nonsmoking female controls was carried out. Three miRNA polymorphisms (miR-26a-1 rs7372209, miR-605 rs2043556, and miR-16-1 rs1022960) were analyzed. Both additive and multiplicative interactions were assessed.
Results: MiR-16-1 rs1022960 may be associated with the risk of lung cancer. Carriers with TT genotype of miR-16-1 rs1022960 were observed to have a decreased risk of lung cancer compared with CC and CT genotype carriers (odds ratio =0.550, 95% confidence interval =0.308–0.983, P=0.044). MiR-26a-1 rs7372209 and miR-605 rs2043556 showed no statistically significant associations with lung cancer risk. There were no significant associations between the three single nucleotide polymorphisms and lung adenocarcinoma. People with exposure to both risk genotypes of miR-26a-1 rs7372209 and cooking oil fumes were more likely to develop lung cancer than those with only genetic risk factor or cooking oil fumes (odds ratios were 2.136, 1.255, and 1.730, respectively). The measures of biological interaction and logistic models indicate that gene–environment interactions were not statistically significant on additive scale or multiplicative scale.
Conclusion: MiR-16-1 rs1022960 may be associated with the risk of lung cancer in a Chinese nonsmoking female population. The interactions between miRNA polymorphisms (miR-26a-1 rs7372209, miR-605 rs2043556, and miR-16-1 rs1022960) and cooking oil fumes were not statistically significant.
Keywords: lung cancer, microRNA, single nucleotide polymorphism, cooking oil fume, interaction
Background
Among all kinds of malignancies, lung cancer has the highest morbidity and is the first leading cause of cancer-related death, which is a severe problem threatening people’s health all around the world. Although accumulating epidemiological studies have shown that exposure to environmental factors such as tobacco smoking, air pollution, and toxic chemical compounds may significantly increase one’s risk of developing lung cancer, there still exists a considerable proportion of lung cancer patients who had not been exposed to such factors. In addition, it was observed that only a small fraction of smokers eventually develop lung cancer and ~53% of females with lung cancer are nonsmokers globally,1 which suggest that not only environmental exposure factors play an important role in the development of lung cancer but genetic factors also contribute most to the susceptibility to lung malignancy.
MicroRNA (miRNA), a class of small, endogenous noncoding RNA, which is 18–25 nucleotides in length, can affect gene expression by binding to the 3′-untranslated region of the target messenger RNA (mRNA), leading to translation repression or cleavage of the target mRNA in the posttranscription stage.2 Using bioinformatics tools, it was speculated that miRNAs can regulate almost >60% of human protein-coding genes among which some are cancer-related genes, and it was further demonstrated that miRNA is involved in central cellular processes, including cell proliferation, differentiation, and apoptosis. In addition, dysregulation of these biological processes is considered to be associated with the induction and progression of cancer pathogenesis, and several miRNAs were observed to act as tumor suppressors or oncogenes, depending on the target gene.3–5 More established findings elucidated that one miRNA could regulate hundreds of target genes and one gene could be regulated by various miRNAs, functional mutations in human genome such as single nucleotide polymorphisms (SNPs) located in the miRNA-related region (miR-SNP). miR-SNP can exert its effect on mature miRNA processing or the binding activity of miRNA to target mRNA, so that it may play an extensively regulatory role in the expression of target gene,6 thus affecting many molecular pathways that may be associated with tumorigenesis. Accumulating evidence shows that miR-SNPs are associated with cancer susceptibility. It was reported that the A allele of miR-605 rs2043556 may decrease the risk of breast cancer in Asian population.7 Yang et al observed that TT genotype of miR-26a-1 rs7372209 decreased the susceptibility to bladder cancer compared with the CC/CT genotype.8 However, the associations between the three SNPs (miR-26a-1 rs7372209, miR-605 rs2043556, and miR-16-1 rs1022960) and lung cancer risk are seldom studied. We conduct this molecular epidemiological study to validate the potential association between miR-SNPs and lung cancer risk in nonsmoking females.
Methods
Study subjects
This case–control study was carried out in Shenyang City, which is located in the northeast of the People’s Republic of China. A total of 268 nonsmoking female patients diagnosed with lung cancer, who were recruited from the First Affiliated Hospital of China Medical University, the Liaoning Cancer Hospital and Institute, and others, were included in the case group. Patients with a previous history of metastasized cancer and those who had undergone radiotherapy or chemotherapy were excluded. The control group consisted of 266 cancer-free patients who were recruited from the medical examination centers during the same period. All controls were unrelated ethnic Han Chinese nonsmoking women. A written informed consent was obtained from each participant. This study was approved by the Institutional Review Board of China Medical University.
Every participant was interviewed to obtain demographic data and cooking oil fume exposure when they were admitted in the hospital, and 10 mL of venous blood was collected from each participant. Nonsmokers were defined as people who smoked not >100 cigarettes in their lifetime. The study subjects were asked about the frequency of cooking and types of oils to define cooking oil fume exposure. Participants were asked, “How often did the air in your kitchen become filled with oily ‘smoke’ during cooking?” There were four possible responses ranging from “never”, “seldom”, and “sometimes”, to “frequently”. Exposure to cooking oil fume was defined as an indicator variable equal to 0 if participants reported seldom or never and equal to 1 if participants reported frequently or sometimes.
SNP detecting
Genomic DNA sample of each subject was obtained from venous blood samples using phenol–chloroform method. The SNP detecting method was described in our previous study.9
Statistical analysis
Student’s t-test and χ2-test were used to evaluate the distribution of demographic variables and SNP genotypes among cases and controls. The relationship between SNPs and cooking oil fumes in patients with lung cancer was assessed by odds ratios (ORs) and their 95% confidence intervals (CIs), which were calculated by unconditional logistic regression analysis. Additive interactions were explored according to Tomas Andersson’s report.10 Relative excess risk due to interaction, attributable proportion due to interaction, and synergy index (S), including their 95% CIs, were computed to measure biological interaction. Logistic regression models were carried out to evaluate the multiplicative gene–environment interaction. All statistical analyses were carried out by IBM SPSS Statistics 20.0 (IBM SPSS, Inc. Chicago, IL, USA). All the tests were two sided, and the statistical significance was defined as P<0.05.
Results
Subject characteristics
A total of 268 cases and 266 controls, who were nonsmoking females, were included in this study. The mean ages for cases and controls were 55.30±11.85 and 56.71±11.69 years, respectively (mean ± standard deviation), with no statistically significant difference (t=1.382, P=0.167). Among the cases, 197 subjects had adenocarcinoma, 44 subjects had squamous cell lung cancer, and 27 subjects had other types. A total of 100 and 66 individuals had exposure to cooking oil fumes among the cases and controls, respectively, with a statistically significant difference (χ2=9.739, P=0.002). Individuals with exposure to cooking oil fumes were at an increased 1.804-fold risk of lung cancer (Table 1).
 | Table 1 The association between cooking oil exposure and lung cancer in a Chinese nonsmoking female population |
SNP frequencies and association with lung cancer and lung adenocarcinoma
The distributions of the three miR-SNPs (miR-26a-1 rs7372209, miR-605 rs2043556, and miR-16-1 rs1022960) in cases and controls as well as their associations with lung cancer and lung adenocarcinoma risk are shown in Tables 2 and 3. Carriers with TT genotype of miR-16-1 rs1022960 were observed to have a decreased risk of lung cancer compared with CC and CT genotype carriers (OR =0.550, 95% CI =0.308–0.983, P=0.044), and the remaining SNPs showed no statistically significant associations with lung cancer risk. As shown in Table 3, no significant associations between the three SNPs and lung adenocarcinoma were observed.
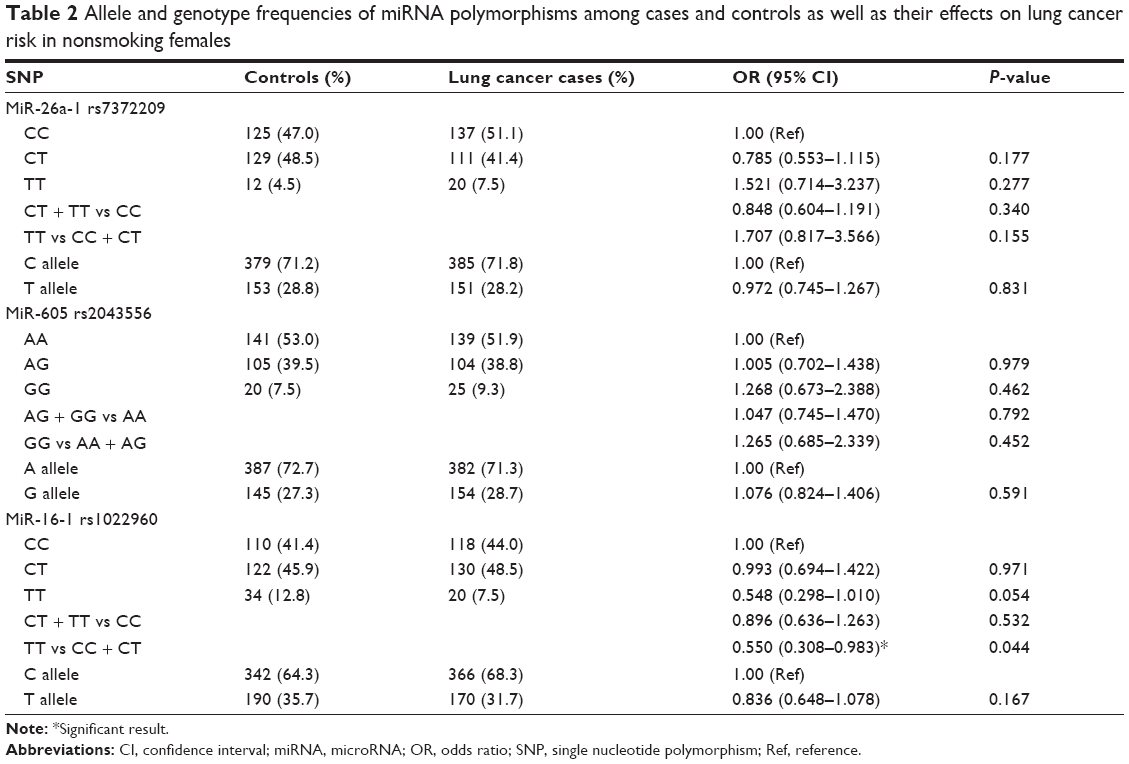 | Table 2 Allele and genotype frequencies of miRNA polymorphisms among cases and controls as well as their effects on lung cancer risk in nonsmoking females |
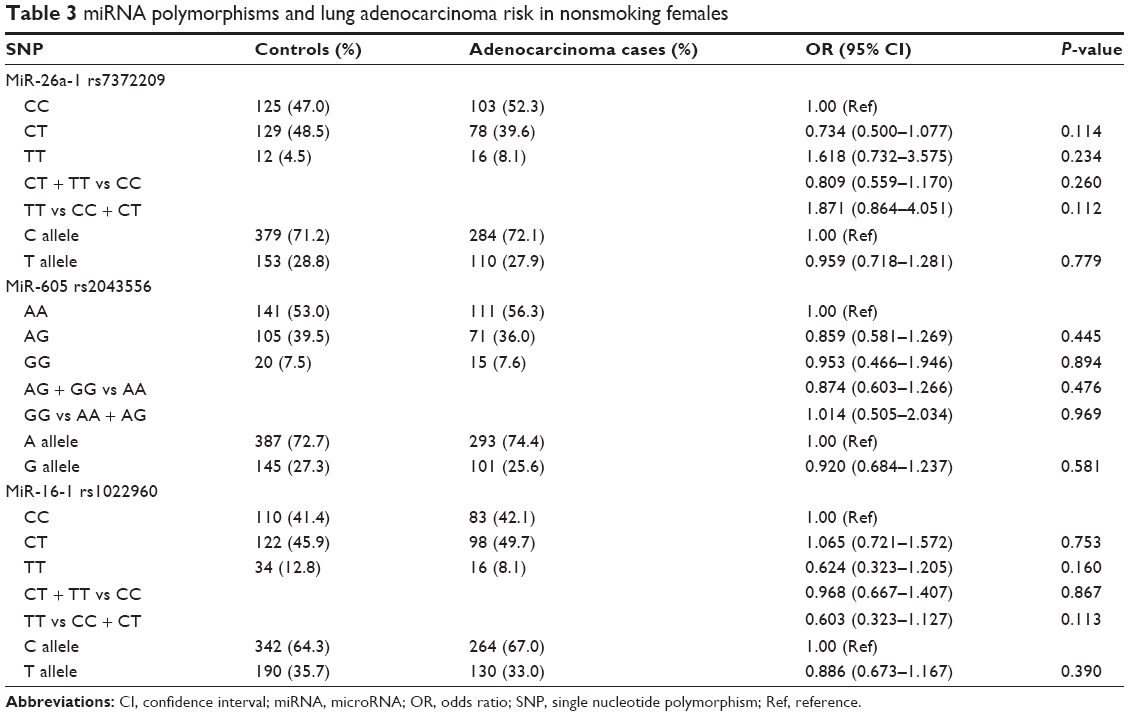 | Table 3 miRNA polymorphisms and lung adenocarcinoma risk in nonsmoking females |
Interaction between oil fume exposure and SNPs
We also conducted a crossover analysis to investigate the interaction of the three SNPs with exposure to oil fumes. The results are shown in Tables 4 and 5, which indicate that exposure to oil fumes can increase the risk of lung cancer in CT and TT genotype carriers of miR-26a-1 rs7372209 compared with the nonexposure CT and TT genotype carriers (OR =1.743, 95% CI =1.038–2.926, P=0.036). CC genotype carriers exposed to cooking oil fumes also had an increased risk of lung cancer (OR =2.177, 95% CI =1.274–3.719, P=0.004). AG and GG genotype carriers of miR-605 rs2043556 with exposure to cooking oil fumes had an elevated risk of lung cancer compared with AA genotype carriers who had no exposure to cooking oil fumes (OR =2.194, 95% CI =1.277–3.767, P=0.004). CT and TT genotype carriers of miR-16-1 rs1022960 with exposure to cooking oil fumes had higher risk of lung cancer compared with CT and TT genotype carriers who had no exposure to cooking oil fumes (OR =2.326, 95% CI =1.409–3.843, P=0.001), and CC genotype carriers who were exposed to cooking oil fumes also showed an elevated risk of lung cancer (OR =1.718, 95% CI =1.005–2.936, P=0.048).
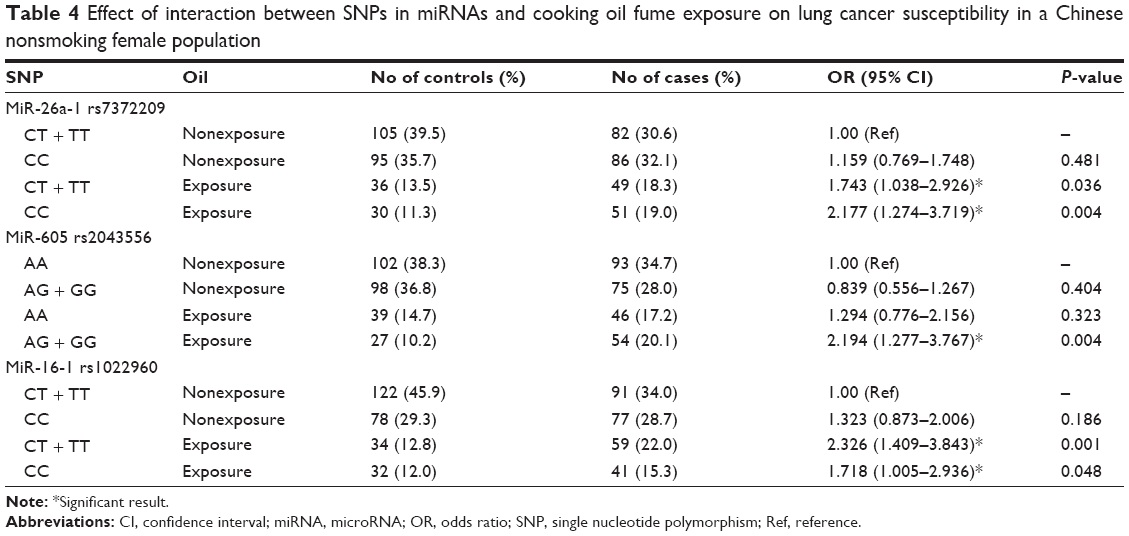 | Table 4 Effect of interaction between SNPs in miRNAs and cooking oil fume exposure on lung cancer susceptibility in a Chinese nonsmoking female population |
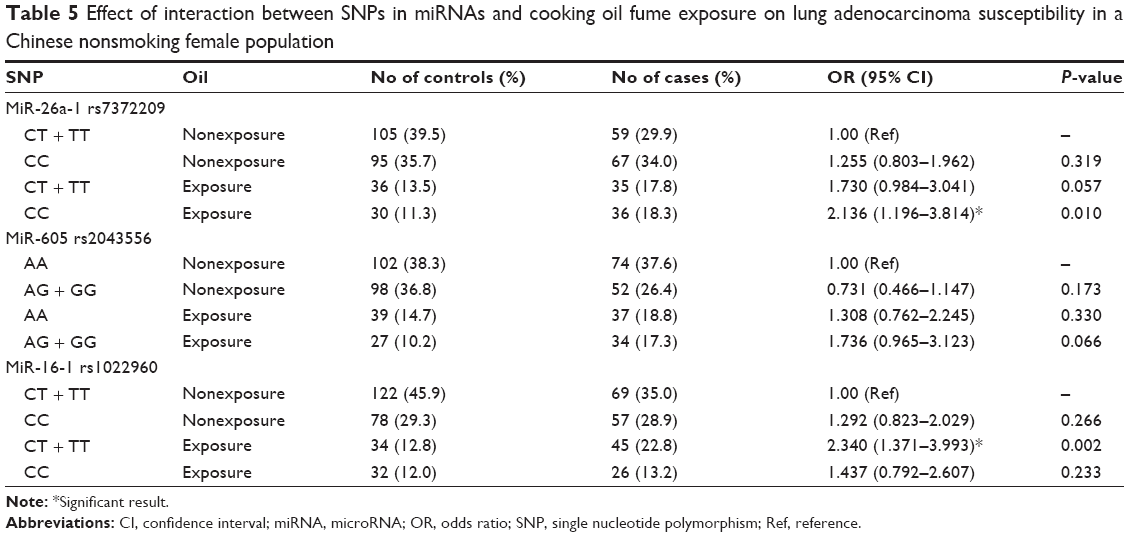 | Table 5 Effect of interaction between SNPs in miRNAs and cooking oil fume exposure on lung adenocarcinoma susceptibility in a Chinese nonsmoking female population |
In the lung adenocarcinoma subgroup shown in Table 5, we found that CC genotype carriers of miR-26a-1 rs7372209 with exposure to cooking oil fumes were more likely to develop lung adenocarcinoma than those with CT and TT genotype carriers (OR =2.136, 95% CI =1.196–3.814, P=0.010). Among the CT and TT genotype carriers of miR-16-1 rs1022960, we observed that exposure to cooking oil fumes increased the risk of lung adenocarcinoma in nonsmoking females (OR =2.340, 95% CI =1.371–3.993, P=0.002). No further statistically significant associations were found for the remaining miRNA SNPs.
The abovementioned crossover results suggested that there may be an interaction between miRNA SNPs and exposure to cooking oil fumes, and hence, the statistically significant tests were explored to assess the interaction on both additive scale and multiplicative scale. Table 6 shows the interaction results of an additive scale, including three measures of interaction, and their 95% CIs to suggest the biological interaction. The results indicate that interactions between miRNA SNPs and exposure to cooking oil fumes were not significant on an additive scale. The interactions on the multiplicative scale calculated by logistic models were not statistically significant. In the logistic analyses of lung cancer, ORs (95% CIs) and P-values of interaction terms were 1.077 (0.511–2.273) and 0.845 for oil*rs7372209, 2.020 (0.953–4.283) and 0.067 for oil*rs2043556, and 0.558 (0.263–1.183) and 0.128 for oil*rs1022960, respectively. In adenocarcinoma, ORs (95% CIs) and P-values of interaction terms were 0.983 (0.439–2.203) and 0.968 for oil*rs7372209, 1.815 (0.805–4.090) and 0.151 for oil*rs2043556, and 0.475 (0.210–1.077) and 0.075 for oil*rs1022960, respectively.
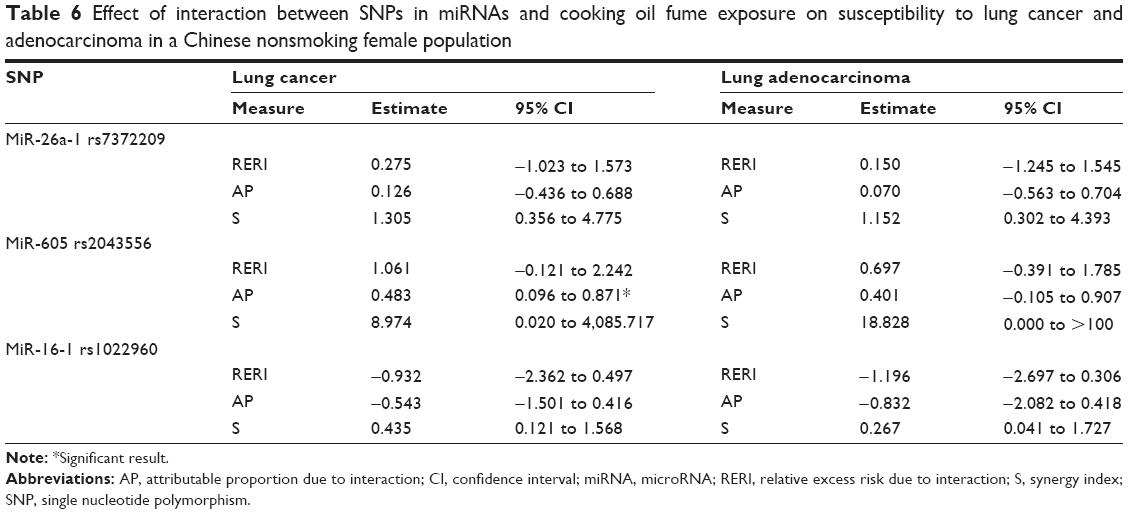 | Table 6 Effect of interaction between SNPs in miRNAs and cooking oil fume exposure on susceptibility to lung cancer and adenocarcinoma in a Chinese nonsmoking female population |
Discussion
Tumorigenesis is a complicated multistep process in which many factors such as environmental factors and genetic mutations play indispensable roles. Many established findings of genetic mutations in carcinogenesis are helpful biomarkers for evaluating cancer susceptibility and predicting prognosis as well as the development of targeting therapy. Ectopic expression levels of miRNAs in cancer cells compared with adjacent normal tissues were reported in many previous studies. Since miRNAs were observed to act as oncogenes or tumor suppressors in various malignancies, genomic mutations in the miRNA coding region such as SNPs may inactivate tumor suppressors or activate oncogenes in different contexts. Traditional Chinese-style cooking often involves heating oil to high temperature with stir frying and deep frying and therefore generates large amount of cooking oil fumes that contain a variety of toxic agents, which are classified as accepted or probable human carcinogens. Exposure to cooking oil fumes is common among Chinese females, and several studies have demonstrated that cooking oil fume is an important environmental risk factor.11,12 Therefore, in the present study, we also evaluated the risk of exposure to cooking oil fumes conferred to the development of lung cancer.
Previous studies have demonstrated that the roles of miR-26a in the tumorigenesis of different tumors and tissue types are not consistent. MiR-26a was reported to suppress cell proliferation in breast cancer, nasopharyngeal carcinoma, and liver cancer,13–15 whereas some studies observed that miR-26a may facilitate the proliferation of cancer cells in glioma.16,17 A study conducted by Liu et al18 aiming to validate the function of miR-26a in lung cancer found that miR-26a enhances the metastatic potential of lung cancer cells by directly targeting phosphatase and tensin homolog (PTEN). For miR-26a-1 rs7372209, a study conducted by Boni et al19 observed that C allele was a favorable factor to predict a relatively better prognosis in the treatment of colon cancer. In the present study, subjects with both cooking oil fume exposure and risk genotype showed a higher risk to develop lung cancer than the reference group. However, it was just a statistical association, and the underlying molecular mechanism needs to be validated.
Association of miR-605 rs2043556 polymorphism with cancer risk has been reported in other cancers. For example, Zhang et al reported an increased risk of gastric cancer in miR-605 AG/GG genotype carriers who engaged in smoke inhalation.20 However, there is a lack of studies focusing on the association between miR-605 rs2043556 polymorphisms and lung cancer risk. Zhang et al reported a marginal significance in elevated susceptibility of miR-605 AG/GG genotype carriers to develop lung cancer than AA carriers;21 however, we did not achieve a statistically significant result, which is consistent with the conclusion of Zhang et al in the overall association analysis of SNPs and risk of lung cancer. Subsequent analysis of gene–environment interactions in the present study showed that carriers with AG/GG genotype who were exposed to cooking oil fumes had a 2.19-fold increased risk than AA carriers without cooking oil fume exposure (OR =2.194, 95% CI =1.277–3.767).
For miR-16-1 rs1022960, CT or TT genotype carriers with exposure to cooking oil fumes showed a significantly elevated risk of lung cancer compared with those with no exposure to cooking oil fumes, consistent with the hypothesis that cooking oil fume is a risk factor of lung cancer. Ectopic expression of miR-16 was commonly observed, and it often exerts its effect of tumor suppression on various kinds of malignancies. In breast cancer model, Mobarra et al showed that upregulation of miR-16 can reduce mRNA of cyclin D1 and B-cell lymphoma-2 (BCL2) and protein levels in Michigan Cancer Foundation-7 (MCF-7) cell line thus decrease cell growth and proliferation and induce apoptosis in MCF-7 cells.22 Jiang et al reported that miR-16 inhibits the proliferation of bladder cancer cells by negatively regulating the expression of cyclin D1.23 The tumor suppressor role of miR-16 was also reported in colorectal cancer, glioma, and nasopharyngeal carcinoma.24–27 However, the expression of miR-16 has never been reported in lung cancer; we presume that miR-16-1 rs1022960 polymorphism may affect the expression level of miR-16 and thus may affect the susceptibility to lung cancer, which needs to be validated in future studies.
The cause of cancer is accepted to be a complex gene–environment interaction. Previous studies seldom investigated the associations between the gene and environment. To the best of our knowledge, this is the first study to comprehensively explore the additive interaction and multiplicative interaction between SNPs in miR-26a-1, miR-605, and miR-16-1 with cooking oil fumes and lung cancer. Results indicated that there were no statistically significant associations between combinations of the three miR-SNPs with cooking oil fumes and lung cancer risk, which we attribute to the limitation of the relatively small sample size. The validation of gene–environment interaction needs to be set in future studies with larger sample sizes.
Some limitations in our study should be taken into account. First, the present study is a hospital-based case–control study, and we enrolled the controls from the medical examination centers of the hospitals. These cancer-free controls may not be appropriate representatives for the overall population, which may result in selection bias in the study. Therefore, we should be cautious when we reach a conclusion. Second, the sample size may be a major obstacle for us to evaluate the gene–environment interaction; therefore, the sample size should be enlarged in a further study.
Conclusion
The present case–control study demonstrated the relationships between the SNPs in three miRNAs and the susceptibility to lung cancer; however, the gene–environment interaction between miRNA SNPs and cooking oil fume exposure was not statistically significant.
Acknowledgments
The authors would like to thank all the patients for their participation and the personnel at the hospitals. This study was supported by the National Natural Science Foundation of People’s Republic of China (No 81102194).
Disclosure
The authors report no conflicts of interest in this work.
References
Parkin DM, Bray F, Ferlay J, et al. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. | ||
Bartel DP. MicroRNAs: target recognition and regulatory functions. Cell. 2009;136:215–233. | ||
Ryan BM, Robles AI, Harris CC. Genetic variation in microRNA networks: the implications for cancer research. Nat Rev Cancer. 2010;10:389–402. | ||
Kumar MS, Lu J, Mercer KL, et al. Impaired microRNA processing enhances cellular transformation and tumorigenesis. Nat Genet. 2007;39:673–677. | ||
Hwang HW, Mendell JT. MicroRNAs in cell proliferation, cell death, and tumorigenesis. Br J Cancer. 2007;96(suppl):R40–R44. | ||
Bartel DP. MicroRNAs: genomics, biogenesis, mechanism, and function. Cell. 2004;116:281–297. | ||
Chen QH, Wang QB, Zhang B. Ethnicity modifies the association between functional microRNA polymorphisms and breast cancer risk: a HuGE meta-analysis. Tumour Biol. 2014;35:529–543. | ||
Yang H, Dinney CP, Ye Y, et al. Evaluation of genetic variants in microRNA-related genes and risk of bladder cancer. Cancer Res. 2008;68:2530–2537. | ||
Lan Q, Hsiung CA, Matsuo K, et al. Genome-wide association analysis identifies new lung cancer susceptibility loci in never-smoking women in Asia. Nat Genet. 2012;44:1330–1335. | ||
Andersson T, Alfredsson L, Kallberg H, et al. Calculating measures of biological interaction. Eur J Epidemiol. 2005;20:575–579. | ||
Yu IT, Chiu YL, Au JS, et al. Dose-response relationship between cooking fumes exposures and lung cancer among Chinese nonsmoking women. Cancer Res. 2006;66:4961–4967. | ||
Zhong L, Goldberg MS, Gao YT, et al. Lung cancer and indoor air pollution arising from Chinese-style cooking among nonsmoking women living in Shanghai, China. Epidemiology. 1999;10:488–494. | ||
Yu L, Lu J, Zhang B, et al. miR-26a inhibits invasion and metastasis of nasopharyngeal cancer by targeting EZH2. Oncol Lett. 2013;5:1223–1228. | ||
Zhang B, Liu XX, He JR, et al. Pathologically decreased miR-26a antagonizes apoptosis and facilitates carcinogenesis by targeting MTDH and EZH2 in breast cancer. Carcinogenesis. 2011;32:2–9. | ||
Lu J, He ML, Wang L, et al. MiR-26a inhibits cell growth and tumorigenesis of nasopharyngeal carcinoma through repression of EZH2. Cancer Res. 2011;71:225–233. | ||
Kim H, Huang W, Jiang X, et al. Integrative genome analysis reveals an oncomir/oncogene cluster regulating glioblastoma survivorship. Proc Natl Acad Sci U S A. 2010;107:2183–2188. | ||
Huse JT, Brennan C, Hambardzumyan D, et al. The PTEN-regulating microRNA miR-26a is amplified in high-grade glioma and facilitates gliomagenesis in vivo. Genes Dev. 2009;23:1327–1337. | ||
Liu B, Wu X, Liu B, et al. MiR-26a enhances metastasis potential of lung cancer cells via AKT pathway by targeting PTEN. Biochim Biophys Acta. 2012;1822(11):1692–1704. | ||
Boni V, Zarate R, Villa JC, et al. Role of primary miRNA polymorphic variants in metastatic colon cancer patients treated with 5-fluorouracil and irinotecan. Pharmacogenomics J. 2011;11(6):429–436. | ||
Zhang MW, Jin MJ, Yu YX, et al. Associations of lifestyle-related factors, hsa-miR-149 and hsa-miR-605 gene polymorphisms with gastrointestinal cancer risk. Mol Carcinog. 2012;51(suppl 1):E21–E31. | ||
Zhang MW, Yu YX, Jin MJ, et al. miR-605和miR-149基因多态性以及相关因素与肺癌易感性的关联研究 [Association of miR-605 and miR-149 genetic polymorphisms with related risk factors of lung cancer susceptibility]. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2011;40:265–271. Chinese. | ||
Mobarra N, Shafiee A, Rad SM, et al. Overexpression of microRNA-16 declines cellular growth, proliferation and induces apoptosis in human breast cancer cells. In Vitro Cell Dev Biol Anim. 2015;51(6):604–611. | ||
Jiang QQ, Liu B, Yuan T. MicroRNA-16 inhibits bladder cancer proliferation by targeting Cyclin D1. Asian Pac J Cancer Prev. 2013;14:4127–4130. | ||
Ma Q, Wang X, Li Z, et al. microRNA-16 represses colorectal cancer cell growth in vitro by regulating the p53/survivin signaling pathway. Oncol Rep. 2013;29:1652–1658. | ||
Yang TQ, Lu XJ, Wu TF, et al. MicroRNA-16 inhibits glioma cell growth and invasion through suppression of BCL2 and the nuclear factor-kappaB1/MMP9 signaling pathway. Cancer Sci. 2014;105:265–271. | ||
Zhang C, Fang X, Li W, et al. Influence of recombinant lentiviral vector encoding miR-15a/16-1 in biological features of human nasopharyngeal carcinoma CNE-2Z cells. Cancer Biother Radiopharm. 2014;29: 422–427. | ||
Xiao G, Tang H, Wei W, et al. Aberrant expression of microRNA-15a and microRNA-16 synergistically associates with tumor progression and prognosis in patients with colorectal cancer. Gastroenterol Res Pract. 2014;2014:364549. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.