")
Back to Journals » Clinical Ophthalmology » Volume 9
Polymerase chain reaction in unilateral cases of presumed viral anterior uveitis
Authors Shoughy S , Alkatan H , Al-Abdullah A, El-Khani A, de Groot-Mijnes J, Tabbara K
Received 3 August 2015
Accepted for publication 23 October 2015
Published 14 December 2015 Volume 2015:9 Pages 2325—2328
DOI https://doi.org/10.2147/OPTH.S93655
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Samir S Shoughy,1 Hind M Alkatan,2,4 Abdulelah A Al-Abdullah,2 Albarah El-Khani,2 Jolanda DF de Groot-Mijnes,3 Khalid F Tabbara1,4,5
1Department of Ophthalmology, The Eye Center and The Eye Foundation for Research in Ophthalmology, 2Department of Pathology & Laboratory Medicine and Uveitis Division, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia; 3Department of Virology and Ophthalmology, University Medical Center Utrecht, Utrecht, the Netherlands; 4Department of Ophthalmology, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 5The Wilmer Ophthalmological Institute of The Johns Hopkins University School of Medicine, Baltimore, MD, USA
Background and objectives: Anterior uveitis is the most common form of intraocular inflammation. The main aim of this study was to determine the viral etiology in patients with unilateral cases of anterior uveitis.
Patients and methods: A total of 12 consecutive patients with the diagnosis of idiopathic unilateral anterior uveitis were included prospectively. Aqueous specimens were obtained from each patient by anterior chamber paracentesis and subjected to the detection of viral DNA/RNA genome by polymerase chain reaction assay for herpes simplex virus, varicella zoster virus, cytomegalovirus, Epstein–Barr virus, and rubella virus.
Results: There were six male and six female patients. The mean age was 43 years, with an age range of 11–82 years. All 12 cases presented with unilateral anterior uveitis. In four (33%) patients, polymerase chain reaction was positive for viral genome. Two patients were positive for herpes simplex virus type 1, one patient was positive for cytomegalovirus and one for Epstein–Barr virus.
Conclusion: Recent molecular diagnostic assays would help in the identification of the causative agent in patients with unilateral anterior uveitis.
Keywords: viral anterior uveitis, PCR, herpes simplex virus, cytomegalovirus, diffuse keratic precipitates, anterior chamber paracentesis
Introduction
Anterior uveitis is the most common form of intraocular inflammation.1–3 The disease is caused by immune-mediated, infectious and undetermined disorders. Forty-eight percent of new cases of uveitis were idiopathic in a recent large epidemiological study.4 With improvements in molecular diagnostic techniques, viruses are increasingly being identified as a cause of anterior uveitis. Viral anterior uveitis is the most common form of infectious anterior uveitis and accounts for more than 10% of cases of anterior uveitis.5 Viral etiology should be suspected in patients with unilateral anterior uveitis and signs of diffuse, fine, stellate or dendritic keratic precipitates (KPs), ocular hypertension, and iris atrophy.6
Viral anterior uveitis is caused mainly by viruses from the Herpesviridae family. Herpes viruses are commonly encountered causes of infections in both immunocompetent and immunocompromised individuals. This family includes herpes simplex virus (HSV) types 1 and 2, varicella zoster virus, cytomegalovirus (CMV), Epstein–Barr virus (EBV), and human herpes virus types 6, 7, and 8. The main viruses responsible for ocular inflammation are HSV type 1, varicella zoster virus, and CMV. EBV and HSV type 2 have also been detected in ocular fluids of patients with anterior uveitis, though less frequently.7 The rubella virus may induce a distinct clinical spectrum of ocular symptoms similar to the Fuchs heterochromic iridocyclitis.8,9 The chikungunya virus and parechoviruses have also been associated with anterior uveitis.10–12 However, EBV is frequently found in ocular fluids from patients with another uveitis entity, for example, toxoplasmosis, or without intraocular inflammation.13,14 EBV was also detected in ocular fluids without evidence of concurrent intraocular antibody production.12 Accordingly, polymerase chain reaction (PCR) detection of EBV in ocular fluids should be interpreted with caution.
In order to effectively manage patients with anterior uveitis, clear distinction between infectious and noninfectious causes should be done. Two types of tests are most commonly performed to detect the causative viral agent. The first one is detection of specific antibody production in ocular fluids (Goldmann-Witmer coefficient [GWC]) and the second method is to detect viral genome by using qualitative or quantitative PCR methods. The main objective of this study is to determine the viral etiology in unilateral cases of anterior uveitis by PCR assay.
Patients and methods
A total of 12 consecutive immunocompetent patients with the diagnosis of idiopathic unilateral anterior uveitis were included. The patients presented with signs suggestive of viral etiology including: unilateral anterior uveitis, diffuse stellate KPs, ocular hypertension, and/or iris atrophy. Inflammation was acute in ten patients and chronic in two patients. All other causes of uveitis were excluded, including HLA-B27-related uveitis. Each patient underwent complete ophthalmic examination, medical evaluation, and laboratory investigations whenever indicated. The determination of antiviral antibodies in the serum was done for the selected patients. Ophthalmic evaluation included determination of visual acuity, applanation tonometry, slit-lamp biomicroscopy, and ophthalmoscopy. All patients underwent a tailored laboratory screening approach, which included complete blood counts, erythrocyte sedimentation rate, and chest X-ray. Tuberculin skin test was done for all patients. HLA-B27 typing was performed if the patients had an acute attack of unilateral uveitis.
Aqueous specimens were obtained from each patient by anterior chamber paracentesis. The aqueous samples were stored at -70°C prior to analysis at the Clinical Virology of the Medical Microbiology department of the University Medical Center Utrecht, Utrecht, the Netherlands. Aqueous was subjected to PCR analysis for the detection of viral nucleic acid of HSV, varicella zoster virus, CMV, EBV, and rubella virus. The last three patients (Table 1) were not tested for EBV or rubella virus due mainly to insufficient sample. All PCR analyses were performed essentially as described previously.7,12 Institutional review board approval from The Eye Center and King Khalid Eye Specialist Hospital Review Boards and written consent from each patient were obtained. The study was adherent to the tenets of the Declaration of Helsinki.
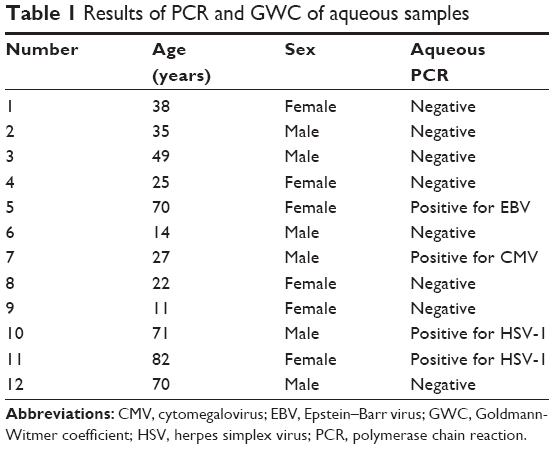 | Table 1 Results of PCR and GWC of aqueous samples |
Results
A total of 12 consecutive immunocompetent patients with the diagnosis of idiopathic unilateral anterior uveitis were included. There were six male and six female patients. The mean age was 43 years, with an age range of 11–82 years. All the 12 cases presented with unilateral anterior uveitis. Four (33%) out of the 12 patients showed positive results for viral etiology (Table 1). Two patients were positive for HSV-1, one patient was positive for CMV and one for EBV. Ten (82%) out of the 12 cases had elevated intraocular pressure. Five cases showed fine diffuse KPs, three cases showed medium-sized KPs, two cases showed inferior KPs, and one showed mutton-fat KPs. Five had posterior synechiae and three cases showed iris atrophy. There was no different pattern of clinical features in the patients with a viral etiology compared with those with a negative PCR outcome.
Discussion
Effective management of patients with anterior uveitis requires clear differentiation between infectious and noninfectious causes. Every effort should be made to identify the cause of uveitis. This depends mainly on the clinical picture, and in cases of uncertainty, laboratory investigations should be considered. For the diagnosis of infectious uveitis, the obtained sample is usually an anterior chamber paracentesis or a vitreous tap.15 In cases of viral anterior uveitis, two types of tests are most commonly performed to detect the causative viral agent including specific antibody detection and PCR analysis in the ocular tissues or fluids.
Antibodies that are found in the eye during an attack of uveitis can be derived from the blood due to either disruption of the blood–aqueous barrier or intraocular synthesis by plasma cells.16 GWC analysis is applied to determine actual intraocular production of antibodies. The second method is to detect viral genome by using qualitative or quantitative PCR.
The PCR is a powerful molecular biological tool that involves enzymatic amplification of nucleic acid sequences in repeated cycles of denaturation, oligonucleotide annealing, and DNA polymerase extension. PCR has revolutionized much of molecular biology and has greatly accelerated the development of molecular diagnostics. However, the use of PCR to determine the viral genome in the aqueous can lead to a diagnosis of viral uveitis if it is positive, but cannot exclude a viral etiology if it is negative.
Studies have shown that combining these two techniques will generally increase the diagnostic yield.7,17 However, in certain cases, such as immunocompromised states, antibody testing may be less reliable, most likely due to aberrant antibody synthesis.18 In these cases, PCR is preferred. On the other hand, in chronic infectious uveitis, such as rubella virus-associated ocular disease, the GWC analysis is superior.9,19
Viruses have long been suspected as causative agents in unilateral cases of anterior uveitis. Indeed, studies have shown that viral infection is a major cause of anterior uveitis. Viral uveitis determined by either real-time PCR and/or GWC was documented in 20 out of 30 patients (67%).20 In our series, only four (33%) out of 12 patients showed positive results for viral etiology using PCR. In another series including larger numbers of patients, positive results for microbial causes were obtained in 54 (23%) out of 230 patients suspected of infectious uveitis.7
The discrepancy between the clinically presumed viral etiology of anterior uveitis and the low rate of actual identification of the viral genome could be explained in different ways. Not all patients may be analyzed by both diagnostic assays as in our patients. Moreover, the negative results may be due to anterior uveitis caused by a nonviral disease or by a virus that was not tested for in the aqueous samples.17 In addition, PCR may show false-negative results due to a short-lived release of the virus into the aqueous humor.7 PCR may also be positive only after repeated taps, resulting from a low viral load in combination with a limited volume of aqueous sample or depending on the time of sampling after onset of disease.7,13 The limitations of our study are low number of patients and the aqueous samples were not subjected to detect viral antibodies.
Studies have shown that combining PCR and GWC will generally increase the diagnostic yield.7,17 However, in certain cases, such as immunocompromised states, antibody testing may be less reliable, most likely due to aberrant antibody synthesis.18 In these cases, PCR is preferred. On the other hand, in chronic infectious uveitis, such as rubella virus-associated ocular disease, the GWC analysis is superior.9,19
A high index of suspicion toward an intraocular infection should be kept in mind in cases of unilateral anterior uveitis. The clinician should bear in mind the possibility of viral etiology. However, according to our series, only 33% of the clinically suspected cases of viral etiology are proven by PCR.
Acknowledgments
Financial/proprietary interests: The authors do not have any financial and proprietary interests in this study.
Support: This study was supported in part by a Special Fund from The Eye Center and The Eye Foundation for Research in Ophthalmology, Riyadh, Saudi Arabia.
This paper was presented in part at the Saudi Ophthalmology 2014 annual meeting held in the period of March 2–5, 2014, King Fahd Cultural Center, Riyadh, Saudi Arabia.
Disclosure
The authors report no conflicts of interest in this work.
References
Islam SM, Tabbara KF. Causes of uveitis at The Eye Center in Saudi Arabia: a retrospective review. Ophthalmic Epidemiol. 2002;9:239–249. | ||
Yang P, Zhang Z, Zhou H, et al. Clinical patterns and characteristics of uveitis in a tertiary center for uveitis in China. Curr Eye Res. 2005;30:943–948. | ||
Khairallah M, Yahia SB, Ladjimi A, et al. Pattern of uveitis in a referral centre in Tunisia, North Africa. Eye. 2007;21:33–39. | ||
Kim EC, Margolis TP. Hypertensive iridocyclitis. Br J Ophthalmol. 2006;90(7):812–813. | ||
Garweg JG. Diagnostics of virus-induced anterior uveitis. Acta Ophthalmol. 2011;89:0. doi:10.1111/j.1755-3768.2011.4445.x | ||
Tugal-Tutkun I, Otük-Yasar B, Altinkurt E. Clinical features and prognosis of herpetic anterior uveitis: a retrospective study of 111 cases. Int Ophthalmol. 2010;30:559–565. | ||
De Groot-Mijnes JD, Rothova A, Van Loon AM, et al. Polymerase chain reaction and Goldmann-Witmer coefficient analysis are complimentary for the diagnosis of infectious uveitis. Am J Ophthalmol. 2006;141(2):313–318. | ||
de Visser L, Braakenburg A, Rothova A, de Boer JH. Rubella virus-associated uveitis: clinical manifestations and visual prognosis. Am J Ophthalmol. 2008;146(2):292–297. | ||
Suzuki J, Goto H, Komase K, et al. Rubella virus as a possible etiological agent of Fuchs heterochromic iridocyclitis. Graefes Arch Clin Exp Ophthalmol. 2010;248(10):1487–1491. | ||
Mahendradas P, Ranganna SK, Shetty R, et al. Ocular manifestations associated with chikungunya. Ophthalmology. 2008;115(2):287–291. | ||
Mahendradas P, Shetty R, Malathi J, Madhavan HN. Chikungunya virus iridocyclitis in Fuchs’ heterochromic iridocyclitis. Indian J Ophthalmol. 2010;58(6):545–547. | ||
de Groot-Mijnes JD, de Visser L, Zuurveen S, et al. Identification of new pathogens in the intraocular fluid of patients with uveitis. Am J Ophthalmol. 2010;150(5):628–636. | ||
Matos K, Muccioli C, Belfort Junior R, Rizzo LV. Correlation between clinical diagnosis and PCR analysis of serum, aqueous, and vitreous samples in patients with inflammatory eye disease. Arq Bras Oftalmol. 2007;70(1):109–114. | ||
Sugita S, Shimizu N, Watanabe K, et al. Use of multiplex PCR and real-time PCR to detect human herpes virus genome in ocular fluids of patients with uveitis. Br J Ophthalmol. 2008;92(7):928–932. | ||
Nandi K, Ranjan P, Therese L, Biswas J. Polymerase chain reaction in intraocular inflammation. Open Ophthalmol. 2008;2:141–145. | ||
de Boer JH, Luyendijk L, Rothova A, Kijlstra A. Analysis of ocular fluids for local antibody production in uveitis. Br J Ophthalmol. 1995;79:610–616. | ||
Kongyai N, Sirirungsi W, Pathanapitoon K, et al. Viral causes of unexplained anterior uveitis in Thailand. Eye (Lond). 2012;26(4):529–534. | ||
Westeneng AC, Rothova A, de Boer JH, de Groot-Mijnes JD. Infectious uveitis in immunocompromised patients and the diagnostic value of polymerase chain reaction and Goldmann-Witmer coefficient in aqueous analysis. Am J Ophthalmol. 2007;144(5):781–785. | ||
Quentin CD, Reiber H. Fuchs heterochromic cyclitis: rubella virus antibodies and genome in aqueous humor. Am J Ophthalmol. 2004;138(1):46–54. | ||
Tan WJ, Poh EW, Wong PY, Ho SL, Lim WK, Teoh SC. Trends in patterns of anterior uveitis in a tertiary institution in Singapore. Ocul Immunol Inflamm. 2013;21(4):270–275. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.