")
Back to Journals » Patient Preference and Adherence » Volume 14
Polish Adaptation of the Self-Care of Diabetes Inventory (SCODI)
Authors Uchmanowicz I , Krzemińska S , Ausili D , Luciani M , Lisiak M
Received 11 March 2020
Accepted for publication 26 June 2020
Published 31 July 2020 Volume 2020:14 Pages 1341—1350
DOI https://doi.org/10.2147/PPA.S253444
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Izabella Uchmanowicz,1 Sylwia Krzemińska,1 Davide Ausili,2 Michela Luciani,2,3 Magdalena Lisiak1
1Department of Clinical Nursing, Faculty of Health Sciences, Wroclaw Medical University, Wroclaw, Poland; 2Department of Medicine and Surgery, University of Milano-Bicocca, Monza, Italy; 3Department of Public Health and Pediatrics, University of Turin, Torino, Italy
Correspondence: Izabella Uchmanowicz
Department of Clinical Nursing, Faculty of Health Sciences, Wroclaw Medical University, Wroclaw, Poland
Tel +48 71 784 18 05
Fax +48 71 345 93 24
Email [email protected]
Purpose: As the guidelines indicate, education and self-care in diabetic patients are essential elements in the treatment process. The efficient evaluation of the level of self-care will enable the patient’s needs to be identified and education and care to be optimised. The Self-Care of Diabetes Inventory (SCODI) is a valid and reliable tool which can measure self-care behaviours among patients with diabetes. The purpose of this study was to assess the reliability of the Polish version of the SCODI.
Methods: The World Health Organization (WHO) translation protocol was used for the translation and cultural adaptation of the English version of the SCODI into Polish. The study included 276 Polish patients with type 2 diabetes (mean age 61.28± 12.02 years). There were 145 men and 131 women in the study. The internal consistency of the SCODI was evaluated using Cronbach’s Alpha.
Results: The original four actor tool structure was confirmed. The mean overall levels of self-care in the four SCODI scales in the study group were self-care maintenance (67.66 pts; SD=18.55), self-care monitoring (61.81 pts; SD=24.94), self-care management (54.65 pts; SD=22.98) and self-care confidence (62.86 pts; SD=20.87). The item-total correlations were positive, so there is no need to change the scales of any of the questions. The overall consistencies for individual scales were assessed using Cronbach’s Alpha: self-care maintenance (0.759), self-care monitoring (0.741), self-care management (0.695) and self-care confidence (0.932). Exploratory factor analysis and item factor loadings of the individual items ranged from 0.137 to 0.886 and, with two exceptions (questions number 23 and 32), were statistically significant (p< 0.05).
Conclusion: The SCODI questionnaire has acceptable internal consistency and reliability in assessing self-care among diabetic patients in the Polish population. This reliable research tool can be managed in planned studies of Polish patients with diabetes.
Keywords: Self-Care of Diabetes Inventory, reliability, self-care, diabetes
Introduction
Although diabetes is a non-communicable disease, it has been recognized by the United Nations as an epidemic due to its rapid spread.1 In the 21st century, there has been a rapid increase in the incidence of diabetes. According to estimates from the World Health Organization (WHO), diabetes, cancer and respiratory and circulatory diseases are responsible for 82% of all non-communicable disease deaths worldwide. As reported by the International Diabetes Federation (IDF) Diabetes Atlas data, diabetes affects 463 million people, which represents 9.3% of the world’s population between 20 and 79 years of age. This disease changes the functioning of patients and their families in everyday life. It should be noted that there will be an increase in the number of patients living with diabetes to 578 million in 2030 and up to 700 million in 2045.2
The latest IDF estimates indicate that there are currently 52 million adults in Europe (20–79 years old) with diabetes mellitus, which means that type 2 diabetes mellitus (T2DM) is the most common form of diabetes. The prevalence of diabetes is 7.9%. Almost half of the patients with diabetes are of working age (under 60), and over 17 million are not aware of their illness. Poland has two million adults with diabetes, which places it among the countries that have an average prevalence of diabetes (7.1%). More than half of the patients in Poland are elderly people between the ages of 60 and 79.3
Modern diabetes therapy goes beyond the traditional understanding of chronic disease treatment. It includes early prevention, identification and monitoring of risk factors and education. A conscious patient who understands his or her role in the therapeutic process becomes an active participant in the fight against the disease.4
The IDF Clinical Practice Recommendations for Managing Type 2 Diabetes in Primary Care guidelines of 2017 emphasise that diabetes education and self-care are the pillars of diabetes administration.5 Nowadays, patient-centred care with self-care is an international problem which needs multidisciplinary team collaboration. Self-care is an important issue for prevention and management of T2DM.6 Self-care of a diabetic patient is defined as a continuous process of knowledge and skills based on the patient’s awareness to be an active and knowledgeable participant in the treatment process. Self-care in diabetes assumes that the patient will practise behaviours that include an appropriate diet, avoidance of high fat intake, increased physical activity, glycaemic monitoring and regular foot evaluation.7 A high level of preparedness for self-care and decision-making by the patient and/or his family will be beneficial in reducing the number of hospitalisations.8 Good self-care in diabetes patients can improve their quality of life.9
Diabetes education, which increases the competence of patients and their families in the fight against the disease, also aims to prepare them for cooperation in the process of treatment, care and self-care. Proper education increases the patient’s mental resilience to stress, builds his independence, motivates him to take on the difficulties associated with therapy, eliminates fear of the future and prevents anxiety, loss and depression.10 The outcome of effective diabetes education is that the patient takes responsibility for the treatment of his illness and makes appropriate therapeutic decisions.11 Patient education can be conducted individually, as an integral part of his contacts with members of the therapeutic team, or in groups. Small and, if possible, homogeneous groups are preferable, and the content and methods should be individually adjusted to the patient’s needs and abilities.12
Diabetes education also increases the patient’s readiness to take pro-health actions13 and is connected with improved compliance with medical recommendations concerning regular drug intake, proper diet and physical activity, implementation of foot self-care, glycaemic measurement, blood pressure, body mass and blood laboratory parameters. It also contributes to better collaboration with the physician.14,15 Therefore, we may conclude that diabetes education is important, but it must be transferred into action, which means into self-care activities, to be fully beneficial for the patient. Self-care activities refer to certain behaviours, such as following a diet plan, avoiding high fat foods, increasing physical activity, self-monitoring of blood glucose, taking medications and solving problems as they occur.16
Good health behaviour with regard to self-care influences adequate self-care practices and reduces cardiovascular risk, hospitalisations and disease-related complications, while also improving quality of life.17,18
In recent years, it has been shown that there are many single and multidimensional tools for the assessment of self-care behaviour in people with T2DM. It is worth noting that studies on the evaluation of psychometric profiles for self-care tools still need to be evaluated for their usefulness and effectiveness of implementation in everyday clinical practice.19,20
It is important to have a tool that measures self-care behaviours of diabetic patients because the assessment of self-care in this group of patients is essential. Therefore, we chose the Self-Care of Diabetes Inventory (SCODI), which was developed based on the Middle-Range Theory Of Self-Care Of Chronic Illness,21 for adaptation into Polish. We decided to use this tool because, based on the development process, it is up to date clinically, was proven to be a valid and reliable tool to measure self-care in diabetic patients and can be useful for both clinicians and researchers.22 The last multicentre cross-sectional study which concerned the test invariance of the SCODI questionnaire between Italy and the United States showed that this tool can be used in other countries because it appears to be psychometrically reliable.23 We decided to carry out a systematic evaluation of the SCODI instrument to assess its psychometric properties. Therefore, the purpose of this study was to adapt the language of the SCODI questionnaire and assess its psychometric performance in the Polish population.
Methods
Settings and Participants
The study was conducted between March 2018 and March 2019 in the Wroclaw University Hospital in Poland. The sample of 276 patients with type 2 diabetes (mean age 61.28 years) was recruited from 373 eligible patients and enrolled in the study, as shown in the flow diagram (Figure 1). Based on data provided by the Polish National Health Fund and the Diabetes Coalition, it is believed that there are approximately 3.5 million people living with diabetes in Poland, which represents 9% of the total population. T2DM has been diagnosed in two million people with diabetes, which is 6% of the total population. Considering that 6% of the population in Poland suffers from T2DM (assuming that the maximum error is 3% and the confidence interval is 90), the minimum sample size was estimated to be 163 people. Therefore, the sample size used in the study was considered sufficient.
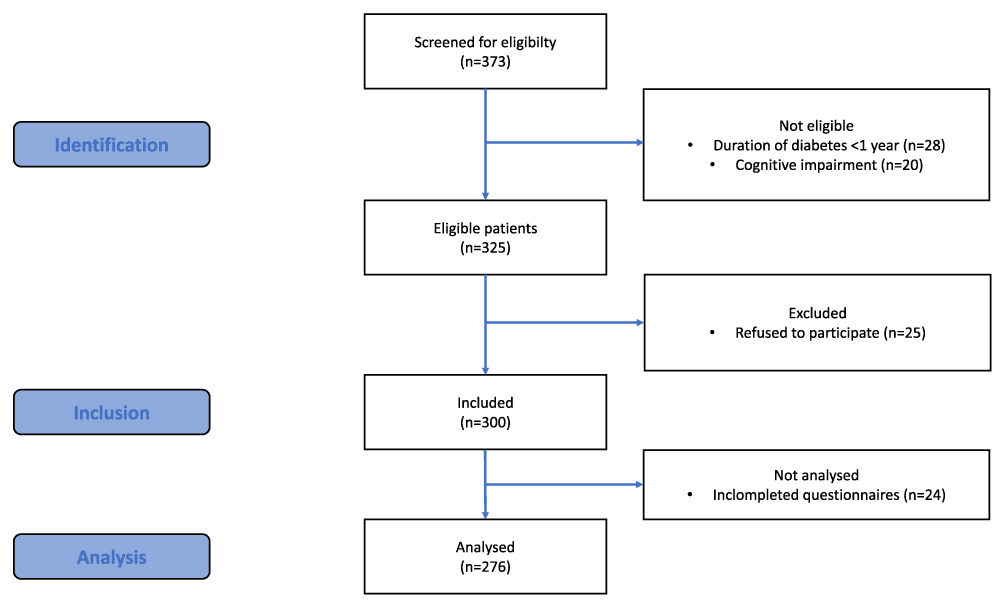 |
Figure 1 Flow diagram of the selection of study population. |
Eligibility Criteria
The criteria for inclusion in the study were: consent to participate in the study, confirmed diagnosis of type 2 diabetes according to guideline criteria, age >18 years. Exclusion criteria were as follow: time from the diagnosis of diabetes < 1 year; documented cognitive impairment, lack of consent to participate in the study.
Ethical Considerations
The study was approved by the Bioethics Committee of the Wroclaw Medical University, Poland (approval no. KB–621/2018). All patients provided informed consent, and were informed that they could withdraw from the study at any time. The study protocol was carried out in accordance with the tenets of the Declaration of Helsinki and Good Clinical Practice guidelines.
Translation Protocol
We followed the WHO24 translation protocol, which has a number of steps that include a forward translation, a panel of experts, a back translation, pretesting and creation of the final version. In the present study, forward translation of the SCODI was performed independently by two bilingual persons. Then a panel of experts (one nursing educator in diabetology, one nurse from a diabetology ward and one medical doctor) reviewed the translation. This group work was moderated by the authors of this adaptation. The team discussed the discrepancies between the original version of the questionnaire and the back translation, and they reached a consensus.
Pretesting was performed by a focus group using interviews. Finally, the back translation was conducted by a bilingual person whose native language was English. Therefore, the expert panel with a translator discussed the discrepancies between the original version and the back translation until consensus was reached.
Research Instrument
The SCODI was developed according to the Middle-Range Theory of Self-Care of Chronic Illness.22 It has proven itself to be valid by the use of external indicators, such as glycated haemoglobin and the presence of diabetes complications.22 It was also tested for the invariance of the measurement model cross-nationally between Italy and the USA.23 The SCODI is composed of four scales measuring self-care maintenance, self-care monitoring, self-care management and self-care confidence.22 Each scale has a 5-point Likert structure and scores 0–100, where higher scores represent better self-care. Each scale measures a specific part of the self-care process with good or high reliability.22 In the original version, self-care maintenance comprises health promoting exercise behaviours, disease prevention behaviours, health promoting behaviours and illness related behaviours. Self-care monitoring comprises body listening and symptom recognition. Self-care management comprises autonomous self-care management behaviours and consultative self-care management behaviours. Self-care confidence comprises task-specific self-care confidence and persistence of self-care confidence.22 A cut-off score of 70 for each scale (ie self-care maintenance, monitoring, management and confidence) has been used by previous studies to discriminate between adequate or inadequate self-care.25
Data Analysis
Internal consistency was assessed using Cronbach’s Alpha, teem-total correlation and confirmatory factor analysis (CFA). In the latter, the double indicator method of Hu and Bentler was used to assess the model fit. Since SCODI items are expressed on an ordinal scale and not on a continuous scale, the parameters were estimated using the Diagonally Weighted Least Squares weighted method. In the analysis, the significance level of 0.05 was assumed. Therefore, all p values below 0.05 were interpreted as indicating significant dependencies. The analysis was performed in the R program, version 3.6.0.
Results
Characteristics of the Study Group
The characteristics of the participants are presented in Table 1. The study group included 145 (52.54%) men and 131 (47.46%) women for a total of 276 participants. The mean age was 61.28±12.02 years, and the mean disease duration was 10.95±8.47 years. The majority of the participants had a middle school (37.68%) or high school education (35.51%) and were in a relationship (64.13%). The evaluation of body mass index (BMI) found that the most common BMI was in the 25.0–29.99 (38.77%) range, and the percentages in the 18.5–24.99 (30.80%) and ≥ 30.0 (30.43%) ranges were comparable.
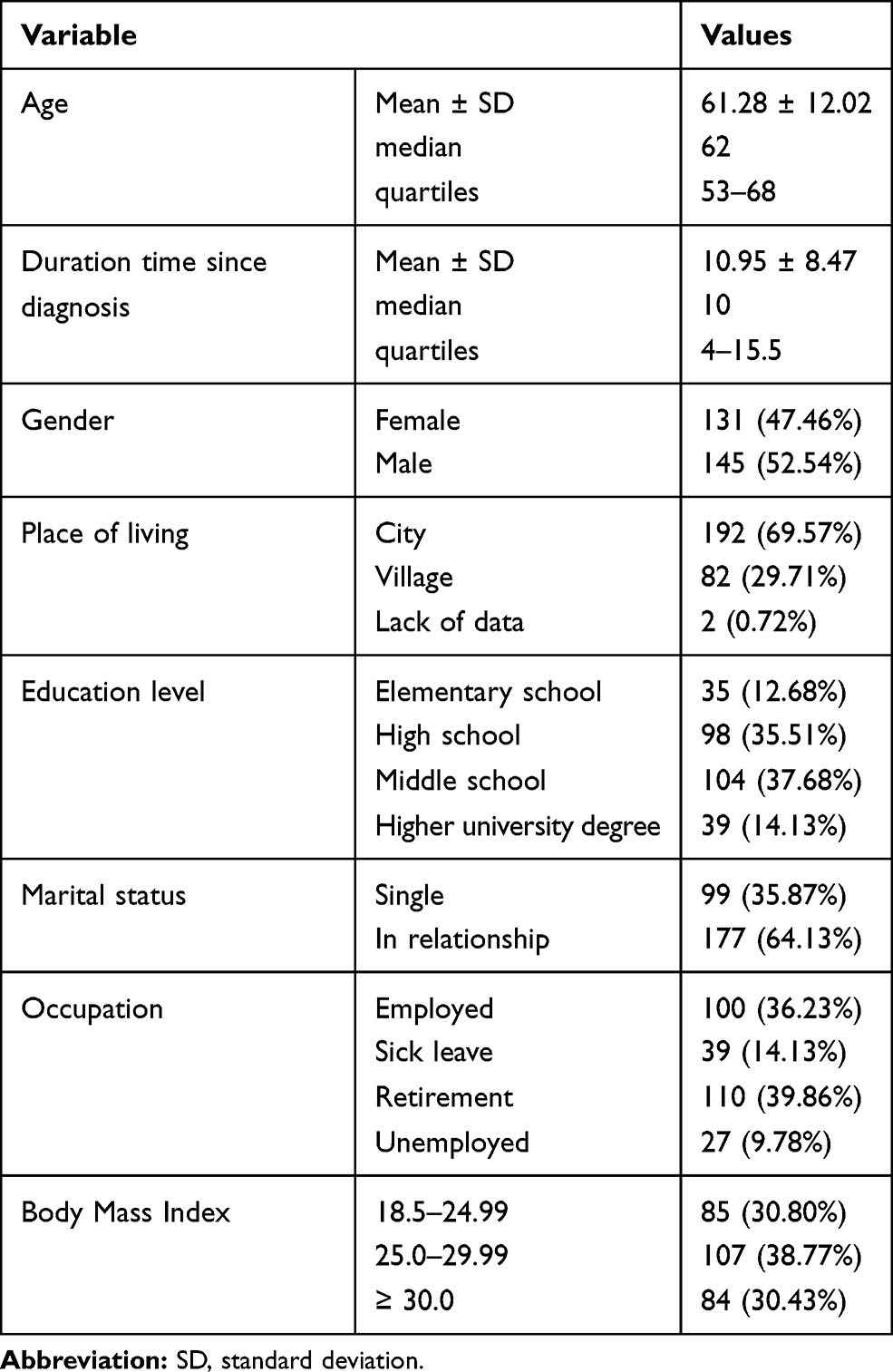 |
Table 1 Socio-Demographic and Clinical Characteristic of the Study Group |
SCODI Questionnaire
The SCODI questionnaire allows the self-care of a diabetic patient to be assessed in four scales (self-care maintenance, self-care monitoring, self-care management and self-care confidence). The result for each area is a number in the range of 0–100, and larger numbers mean better self-care. However, there are no standards to say what results mean high or low self-care. However, since all areas are scored on the same scale, self-care in different areas can be compared to identify potential problems in self-care.
The respondents were best at self-care maintenance (67.66 points; SD=18.55), while they were most likely to have difficulty controlling self-care management (54.65 points; SD=22.98). The detailed SCODI scales characteristics of the Polish version questionnaire are presented in Table 2.
 |
Table 2 SCODI Scales Characteristics |
Cronbach’s Alpha and Discriminatory Powers
Cronbach’s alpha for the individual scales were: self-care maintenance – 0.759, self-care monitoring – 0.741, self-care management – 0.695 and self-care confidence – 0.932
Table 3 includes discriminating powers (item-total correlations) that are positive, so there is no need to change the scales of any of the questions. The individual’s reliability of alpha in the self-care scales of the SCODI questionnaire are presented in Table 3.
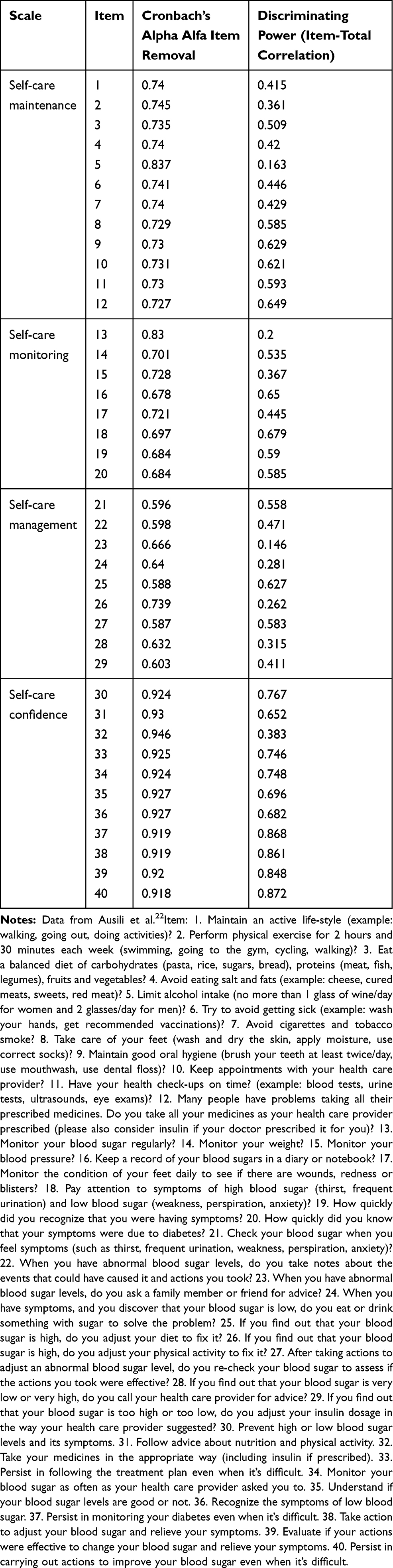 |
Table 3 Reliability Analysis for the SCODI Questionnaire |
Confirmation Factor Analysis (CFA)
Items of our questionnaire are expressed on an orderly scale and not on a continuous scale, so the weighted method Diagonally Weighted Least Squares was used (Table 4).
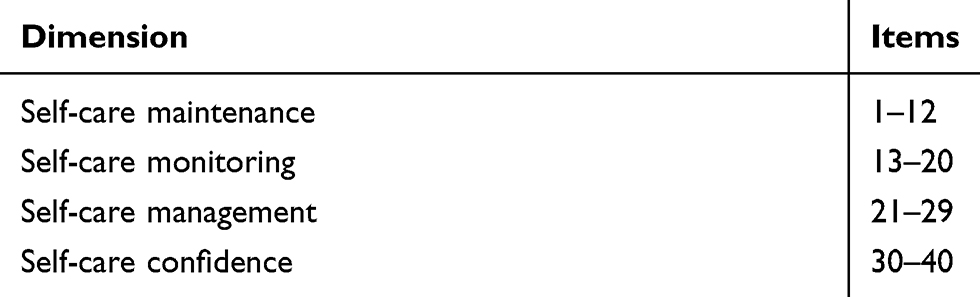 |
Table 4 The Original Structure of SCODI (4 Factorial) |
For this structure, satisfactory values of the fit indices of standardized root mean square residual (SRMR), root mean square error of approximation (RMSEA), confirmatory fit index (CFI) and Tucker–Lewis index (TLI) were obtained. This allowed us to confirm the original four factor tool structure. The results are presented in Table 5.
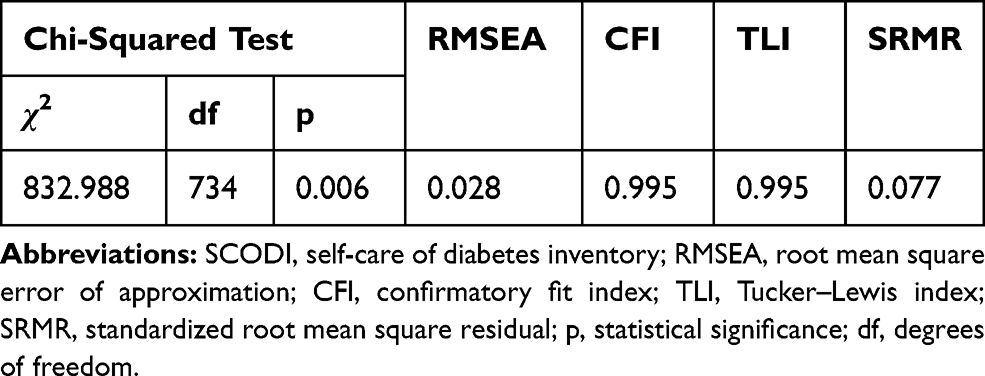 |
Table 5 Fit Indices for the 4 SCODI Scales for the Polish Version |
The loadings of the individual items ranged from 0.137 to 0.886 and, with two exceptions, were statistically significant (p<0.05). The detailed characteristics are presented in Table 6.
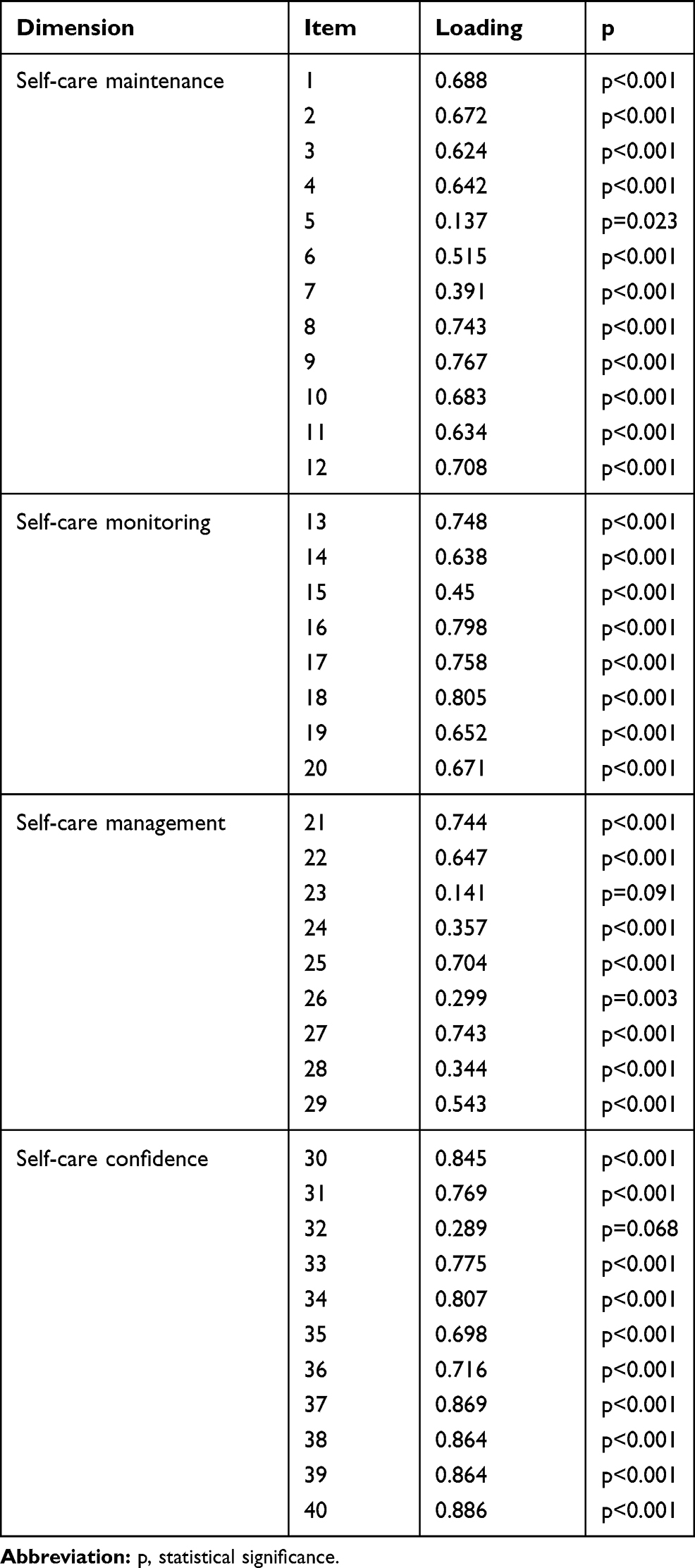 |
Table 6 Exploratory Factor Analysis and Item Factor Loadings for the Self-Care Maintenance, Self-Care Monitoring, Self-Care Management and Self-Care Confidence Scales |
The statistical structure of each SCODI question is presented in Table 7. It shows the frequency of answers to each question.
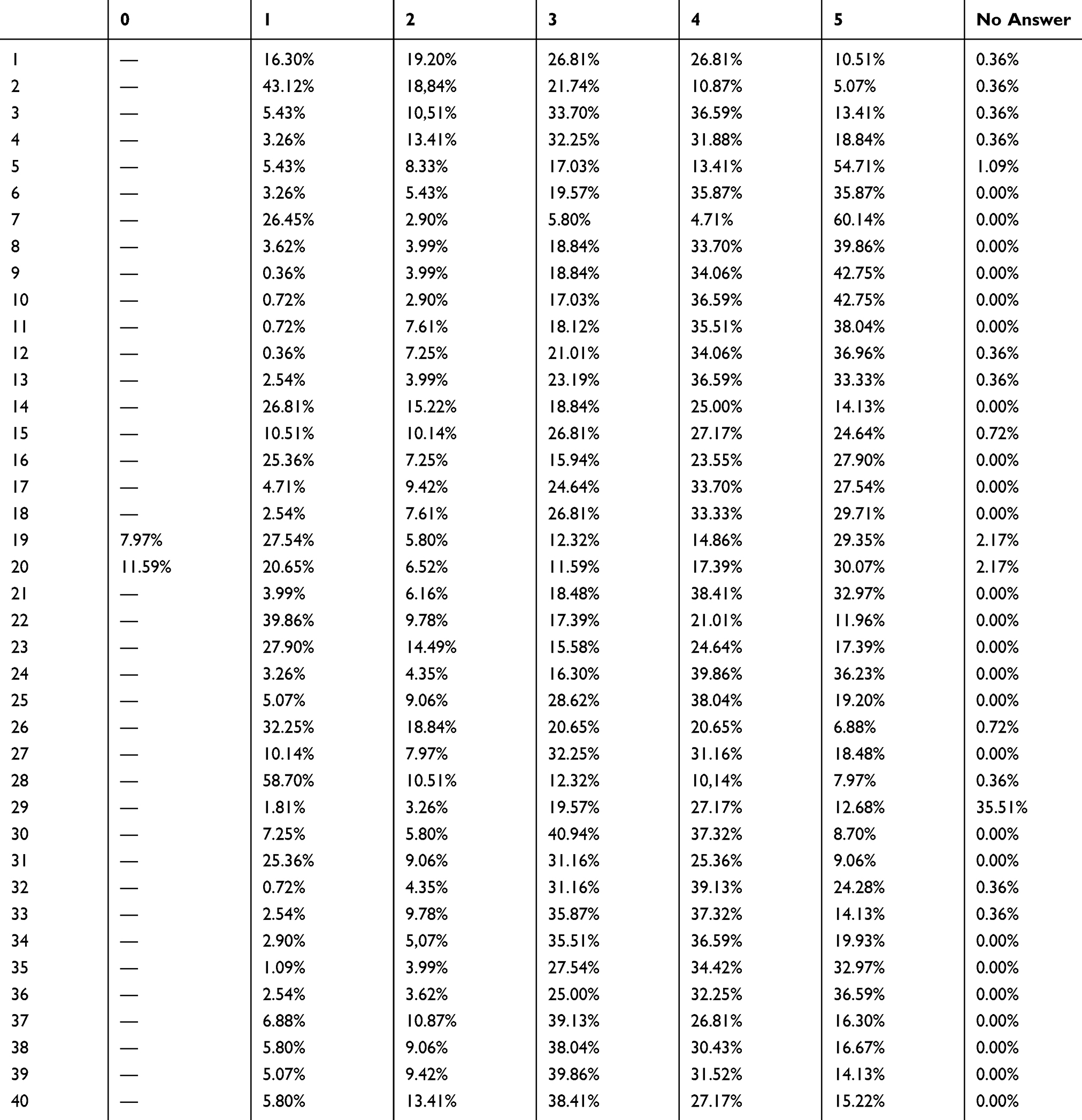 |
Table 7 Answers to Specific SCODI Questions |
Discussion
The purpose of this study was to adapt and test the psychometric properties of a Polish version of the SCODI questionnaire for patients with diabetes. This questionnaire was developed based on the Middle-Range Theory Of Chronic Illness, and this instrument measures self-care maintenance, self-care monitoring, self-care management and self-care confidence. Its original version demonstrated content validity, reliability and construct validity. It was also shown to have generalisability of the measurement model.22 It should be noted that a recently published study has shown good validity and reliability in measuring self-care using a Farsi version of the SCODI.26
Nowadays, due to the rising prevalence of diabetes, the importance of self-care has become more relevant to good disease management. Moreover, the main principle of self-care in diabetes is patient-centred care. A good relationship between the patient and the therapeutic team must be maintained to achieve the goals of self-care management. Appropriate preparation for self-care behaviours, such as healthy eating, physical activity, blood glucose monitoring, adherence with medications, satisfactory problem-solving skills, healthy coping skills and reducing risky behaviours, can predict greater patient involvement in the therapy process and better outcomes.27 However, in Poland, studies that would clearly demonstrate the impact of self-care on management in diabetes patients are still lacking. The studies that have been conducted concern the assessment of only selected variables which play a role in disease management, such as self-monitoring of blood glucose, blood pressure and foot self-care.28,29
The Polish adaptation of the SCODI may increase the research area in the evaluation of self-care in patients living with diabetes. This is significant due to the fact that a lack of systematic self-care assessment may contribute to a passive attitude in patients and thus cause low effectiveness of disease management. The implementation of a multi-faceted level of self-care is particularly difficult in patients with diabetes and comorbidities. Another notable aspect is that diabetic patients are exposed to polypharmacy as a result of multimorbidity, age-related pharmacokinetic variability, cognitive impairment, use of over-the-counter medications or inability to control their diseases.30 The complexity of the problem makes it essential to intensify efforts to identify elderly patients who may not follow the recommendations and require more attention. Innovative and intensive self-care should be implemented in the daily treatment practice process to improve diabetes patients’ outcomes and quality of life.31
Good management and implementation of self-care offers a number of benefits, such as improved well-being and decreased morbidity, mortality and health care expenditures.32 Due to every country having its own cultural and social behaviour, there can be an impact on perception of self-care practices. In many cultures, a holistic approach is practised, but there can also be some cultural differences which may have an influence on specific self-care activities.33 Nowadays, there is still a need to conduct research and recognise the burden of cultural differences in self-care. It should be remarked that both the Polish and Italian versions have the same factor loading as self-care. It may indicate that both of these populations have comparable views and approaches to self-care.
The SCODI proved to be a valid measure of self-care in our reference sample, which consisted of 276 patients with type 2 diabetes. When adapting the tool, it was checked whether the original scales matched the Polish language version. CFA was performed. The original SCODI structure has four factors, and for this structure, satisfactory values of the fit indices of SRMR, RMSEA, CFI and TLI were obtained. In the Polish study, we also confirmed that this structure was as satisfactory as it was in the Italian and American versions. The loadings of the individual items ranged from 0.137 to 0.886 and, with two exceptions, were statistically significant (p<0.05).
We interpreted the loads as correlations of the items with the subscale to which they belong. Their significance means that all the items significantly correlated with the result of the subscale tested (CFA-implied item-total correlations), which means that good results of the original scale were confirmed. Therefore, we may assume that the SCODI is characterised by good construct validity, reliability and acceptable internal consistency. The internal consistency of the adapted version of the scale was determined by means of Cronbach’s alpha. Some studies have suggested that the internal consistency of items should be classified as follows: values ≥ 0.9 as excellent, ≥ 0.8 as good, ≥ 0.7 as acceptable, ≥ 0.6 as questionable, ≥ 0.5 as poor, and <0.5 as unacceptable. However, there is actually no lower limit to the coefficient.34 In the group of 276 patients, Cronbach’s alpha for the individual scales were: self-care maintenance – 0.759, self-care monitoring – 0.741, self-care management – 0.695 and self-care confidence – 0.932. These values are similar to those documented in the original SCODI version. In the original validation, Cronbach’s alpha for the individual scales were, respectively: 0.81, 0.84, 0.86 and 0.89.22 The reliability of the Polish version is good, which is evidenced by strong chance-corrected item agreement and adequate internal consistency of the SCODI scores.
Conclusions
Our study revealed that the instrument tested is valid and reproducible for the assessment of self-care in Polish patients with type 2 diabetes and could be useful to both clinicians and researchers. The SCODI is a simple research tool which can be used in standardised daily clinical practice to assess the self-care behaviour of patients with diabetes mellitus. The evaluation of self-care will allow care to be optimised and will support tailored educational interventions. The outcome obtained using this questionnaire may be helpful in identifying negative determinants while planning the self-care process. Moreover, using this instrument in everyday practice may improve patients’ self-care and their quality of life.
Implications for Practice
The SCODI is a simple research tool that can be used in clinical practice or in research to evaluate the self-care capabilities of the diabetes population. The translation of this tool into 10 languages may be crucial for comparing how self-care maintenance, monitoring, management and confidence are measured in other cultures. The SCODI questionnaire can improve the effectiveness of educational activities undertaken by multidisciplinary teams in cross-cultural research.
Abbreviations
CFA, confirmatory factor analysis; CFI, confirmatory fit index; IDF, International Diabetes Federation; RMSEA, root mean square error of approximation; SCODI, self-care of diabetes inventory; SRMR, standardized root mean square residual; T2DM, type 2 diabetes mellitus; TLI, Tucker–Lewis index (TLI); WHO, World Health Organization.
Acknowledgments
There were no other contributors to the article than the Authors as well as there was no writing assistance required. The certificated English language services were provided by an academic highly qualified native speaker.
Disclosure
No conflict of interest has been declared by the authors regarding this work.
References
1. Unnikrishnan R, Pradeepa R, Joshi SR, Mohan V. Type 2 diabetes: demystifying the global epidemic. Diabetes. 2017;66(6):1432–1442. doi:10.2337/db16-0766
2. Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. 2019;157:107843. doi:10.1016/j.diabres.2019.107843
3. Topor-Madry R, Wojtyniak B, Strojek K, et al. Prevalence of diabetes in Poland: a combined analysis of national databases. Diabet Med. 2019;36(10):1209–1216. doi:10.1111/dme.13949
4. Masupe TK, Ndayi K, Tsolekile L, Delobelle P, Puoane T. Redefining diabetes and the concept of self-management from a patient’s perspective: implications for disease risk factor management. Health Educ Res. 2018;33(1):40–54. doi:10.1093/her/cyx077
5. Aschner P. New IDF clinical practice recommendations for managing type 2 diabetes in primary care. Diabetes Res Clin Pract. 2017;132:169–170. doi:10.1016/j.diabres.2017.09.002
6. Eva JJ, Kassab YW, Neoh CF, et al. Self-care and self-management among adolescent T2DM patients: a review. Front Endocrinol (Lausanne). 2018;9. doi:10.3389/fendo.2018.00489
7. Shrivastava SR, Shrivastava PS, Ramasamy J. Role of self-care in management of diabetes mellitus. J Diabetes Metab Disord. 2013;12(1):14. doi:10.1186/2251-6581-12-14
8. Song M, Ratcliffe SJ, Tkacs NC, Riegel B. Self-care and health outcomes of diabetes mellitus. Clin Nurs Res. 2012;21(3):309–326. doi:10.1177/1054773811422604
9. Dickson VV, Clark RA, Rabelo-Silva ER, Buck HG. Self-care and chronic disease. Nurs Res Pract. 2013;2013:827409. doi:10.1155/2013/827409
10. Powers MA, Bardsley J, Cypress M, et al. Diabetes self-management education and support in type 2 diabetes: a joint position statement of the American Diabetes Association, the American Association of Diabetes Educators, and the Academy of Nutrition and Dietetics. Clin Diabetes. 2016;34(2):70–80. doi:10.2337/diaclin.34.2.70
11. Burke SD, Sherr D, Lipman RD. Partnering with diabetes educators to improve patient outcomes. Diabetes Metab Syndr Obes. 2014;7:45–53. doi:10.2147/DMSO.S40036
12. Jones H, Berard LD, MacNeill G, Whitham D, Yu C; Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Self-management education. Can J Diabetes. 2013;37(Suppl 1):S26–30. doi:10.1016/j.jcjd.2013.01.015
13. Powell CK, Hill EG, Clancy DE. The relationship between health literacy and diabetes knowledge and readiness to take health actions. Diabetes Educ. 2007;33(1):144–151. doi:10.1177/0145721706297452
14. Toobert DJ, Glasgow RE, Strycker LA, et al. Biologic and quality-of-life outcomes from the Mediterranean lifestyle program: a randomized clinical trial. Diabetes Care. 2003;26(8):2288–2293. doi:10.2337/diacare.26.8.2288
15. Toobert DJ, Glasgow RE, Strycker LA, Barrera M, Ritzwoller DP, Weidner G. Long-term effects of the Mediterranean lifestyle program: a randomized clinical trial for postmenopausal women with type 2 diabetes. Int J Behav Nutr Phys Act. 2007;4:1. doi:10.1186/1479-5868-4-1
16. Glasgow RE, Strycker LA. Preventive care practices for diabetes management in two primary care samples. Am J Prev Med. 2000;19(1):9–14. doi:10.1016/s0749-3797(00)00157-4
17. Yuan C, Lai CWK, Chan LWC, Chow M, Law HKW, Ying M. The effect of diabetes self-management education on body weight, glycemic control, and other metabolic markers in patients with type 2 diabetes mellitus. J Diabetes Res. 2014;2014:789761. doi:10.1155/2014/789761
18. Sicuro J, Charrier L, Berchialla P, et al. Self-management education by group care reduces cardiovascular risk in patients with type 2 diabetes: analysis of the ROMEO clinical trial. Diabetes Care. 2014;37(9):e192–193. doi:10.2337/dc14-1054
19. Lu Y, Xu J, Zhao W, Han H-R. Measuring self-care in persons with type 2 diabetes: a systematic review. Eval Health Prof. 2016;39(2):131–184. doi:10.1177/0163278715588927
20. Caro-Bautista J, Martín-Santos FJ, Morales-Asencio JM. Systematic review of the psychometric properties and theoretical grounding of instruments evaluating self-care in people with type 2 diabetes mellitus. J Adv Nurs. 2014;70(6):1209–1227. doi:10.1111/jan.12298
21. Riegel B, Jaarsma T, Strömberg A. A middle-range theory of self-care of chronic illness. ANS Adv Nurs Sci. 2012;35(3):194–204. doi:10.1097/ANS.0b013e318261b1ba
22. Ausili D, Barbaranelli C, Rossi E, et al. Development and psychometric testing of a theory-based tool to measure self-care in diabetes patients: the self-care of diabetes inventory. BMC Endocr Disord. 2017;17(1):66. doi:10.1186/s12902-017-0218-y
23. Ausili D, Barbaranelli C, Riegel B. Generalizability of the self-care of diabetes inventory across cultures and languages: Italy and the United States. Eval Health Prof. 2020;43(1):41–49. doi:10.1177/0163278719840689
24. World Health Organization. WHO collaborative study on substitution therapy of opioid dependence and HIV/AIDS. Geneva, Switzerland; 2003. https://www.who.int/substance_abuse/activities/substituion_therapy_opioid_dependence_general_protocol%20_v2.pdf?ua=1.
25. Caruso R, Rebora P, Dellafiore F, et al. Clinical and socio-demographic determinants of inadequate self-care in adults with type 1 diabetes mellitus: the leading role of self-care confidence. Acta Diabetol. 2019;56(2):151–161. doi:10.1007/s00592-018-1259-z
26. Ebadi A, Ausili D, Albatineh AN, Salarvand S, Ghanei Ghashlagh R. Psychometric evaluation of the Farsi version of the self-care of diabetes inventory in Iranian patients with diabetes. Diabetes Metab Syndr Obes. 2019;12:2775–2784. doi:10.2147/DMSO.S235436
27. American Association of Diabetes Educators. An effective model of diabetes care and education: revising the AADE7 self-care behaviors®. Diabetes Educ. 2020;46(2):139–160. doi:10.1177/0145721719894903.
28. Szymborska-Kajanek A, Psurek A, Hese R, Strojek K. Self-monitoring of blood glucose in treatment of type 2 diabetes. Diabetes Res Clin Pract. 2009;86(Suppl1):S49–S52. doi:10.1016/S0168-8227(09)70009-97
29. Malec K, Moleda P, Homa K, Stefański A, Raczyński A, Majkowska L. Diabetes care and self-monitoring of type 2 diabetic patients in a rural district of West-Pomeranian Province. Pol Arch Med Wewn. 2008;118(1–2):29–34.
30. Dobrică EC, Găman MA, Cozma MA, Bratu OG, Pantea Stoian A, Diaconu CC. Polypharmacy in type 2 diabetes mellitus: insights from an internal medicine department. Medicina (Kaunas). 2019;55(8):436. doi:10.3390/medicina55080436
31. MinKyoung S. Diabetes mellitus and the importance of self-care. J Cardiovasc Nurs. 2010;25(2):93–98. doi:10.1097/JCN.0b013e3181c5a364
32. Tol A, Alhani F, Shojaeazadeh D, Sharifirad G, Moazam N. An empowering approach to promote the quality of life and self-management among type 2 diabetic patients. J Educ Health Promot. 2015;4:13. doi:10.4103/2277-9531.154022
33. Riegel B, Dunbar SB, Fitzsimons D, et al. Self-care research: where are we now? Where are we going? Int J Nurs Stud. 2019:103402. doi:10.1016/j.ijnurstu.2019.103402.
34. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi:10.1097/00007632-200012150-00014
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.