")
Back to Journals » Clinical Optometry » Volume 11
Polarized glasses may help in symptomatic cases of intraocular lens glistenings
Authors Borkenstein AF , Borkenstein EM
Received 24 January 2019
Accepted for publication 16 April 2019
Published 6 May 2019 Volume 2019:11 Pages 57—62
DOI https://doi.org/10.2147/OPTO.S202796
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Andreas F Borkenstein, Eva-Maria Borkenstein
Borkenstein & Borkenstein, Privatklinik der Kreuzschwestern, Graz, Austria
Abstract: Intraocular lens (IOL) glistening is a relatively common phenomenon. Although most of the patients remain asymptomatic, a small percentage of patients can develop unwanted optical side effects. We report 6 symptomatic patients with IOL glistening. All patients underwent an implantation of a hydrophobic acrylic mononofocal, multifocal or toric IOL in external clinics for visually significant cataract at least 6 months prior. Patients had very reasonable corrected visual acuity (0.8–1.0 decimal), but significantly had reduced contrast sensitivity and modulation transfer function, complained of visual phenomena and expressed dissatisfaction with their visual status. Patients indicated the symptoms were not present immediately after surgery, but gradually developed postoperatively. Slit-lamp examination revealed moderate-to-severe glistening in all cases. No other pathology that would be responsible for the visual symptoms was present. Patients reported improvement in side effects with the use of edge filter (blue-light blocking) eyeglasses and polarized sunglasses with an increase in contrast sensitivity by aproximately 1 line on Pelli–Robson chart. The use of specific eyewear seems to be a promising alternative to avoid explant of an IOL in symptomatic patients with glistenings and very good visual acuity. In conclusion, we believe that long-term optical clarity is crucial for the choice of an IOL.
Keywords: glistenings, intraocular lenses, quality of vision
Introduction
Glistening is described as the formation of fluid-filled microvacuoles within an intraocular lens (IOL) optic when the IOL is in an aqueous environment.1 Although glistening can appear in various IOL biomaterials, hydrophobic acrylic lenses are more susceptible to this phenomenon.2,3 There are ongoing disputes in ophthalmic community about the effect of glistening on visual function with contradictory outcomes in the literature.4 The aim of this article is to present symptoms and optical side effects of small case series of symptomatic patients, propose options to improve their visual functioning as well as raise awareness of this phenomenon among optometrists.
Case reports
Six patients (4 female, 2 male) aged between 58 and 76 years presented in our clinic in 2017. Phacoemulsification with lens implantation for age-related cataracts was performed in external clinics at least 6 months prior. Patients reported problems with nocturnal car driving as well as gradual worsening of the symptoms in rainy weather since surgery. Glare from headlights of oncoming cars, straylight effects in street lamps and various billboards were mentioned. A taxi driver could not work anymore in twilight or darkness. Two patients described their complaints with a general dissatisfaction with vision and a “blurred vision”, difficulty in reading newspapers with light book print and subjective color perception disorders (choice/distinction of matching black, grey, blue and brown socks).
Patients reported uneventful standard cataract procedures with no adverse events in the postoperative course. All patients stated the symptoms were not present immediately after the cataract procedure, but gradually developed postoperatively.
Clinical findings
The data of all 6 cases are presented in Table 1. Five patients achieved best-corrected distance visual acuity (BCDVA) of 0.9–1.0 (decimal) and 1 patient 0.8 (decimal). Patient records from external clinics as well as clinical evaluation of the lens implants revealed IOL models of the company Alcon (Forth Worth, TX, USA); 4 monofocal IOLs Acrysof IQ, one astigmatism correcting Acrysof IQ Toric and one multifocal Acrysof IQ ReSTOR. Biomicroscopy and photo documentation showed well-centered IOLs with no apparent tilt. In addition, Scheimpflug measurement confirmed the correct position of the IOLs. No primary posterior capsular fibrosis or shrinkage was detected. In 2 cases, a slightly superior/nasally decentered, asymmetric capsulorrhexis with small diameter (<4,5 mm) was found.
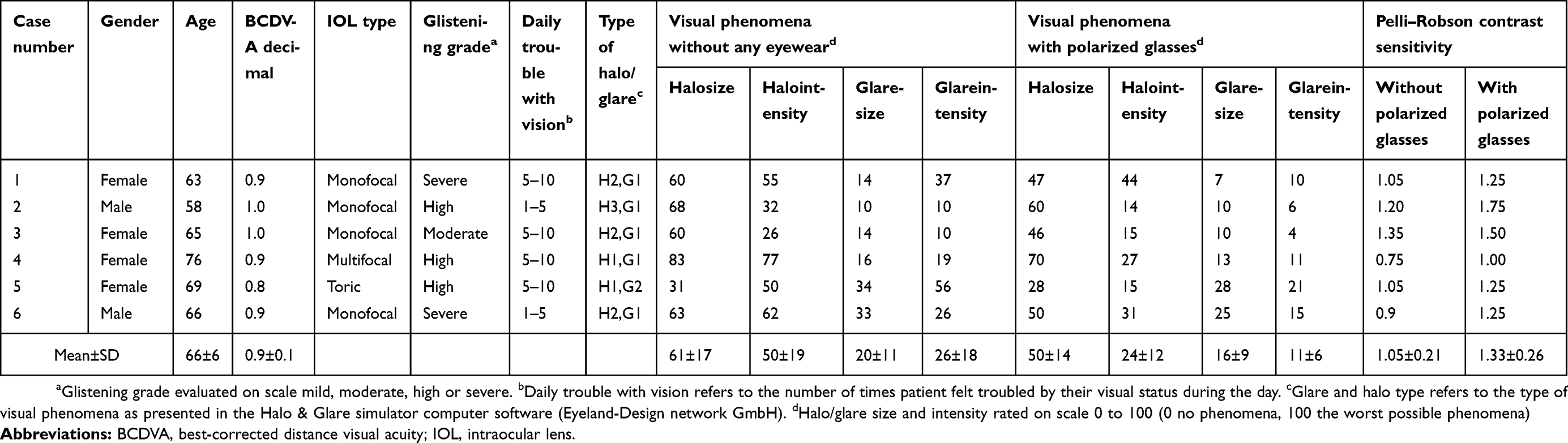 | Table 1 Case reports with glistening |
Examination of the IOLs showed the presence of glistenings in all cases (Figures 1 and 2). A grading system on the scale 1–4 (mild, moderate, high and severe) was used to grade the severity of glistening. In the area of 2×2 mm, mild glistening referred to the total coverage of scattered area ≤0.50%, with the number of glistenings up to 50 and the size of microvacuoles 20 μ. The same parameters for the other categories were as follows: moderate: coverage ≤2%, number 51–250, size 20 μ; high: coverage ≤10%, number 251–2,500, size 20 μ; severe: coverage >10%, number >2,500, size 10 μ. One case in our report had moderate glistening, 3 cases high and 2 cases severe.
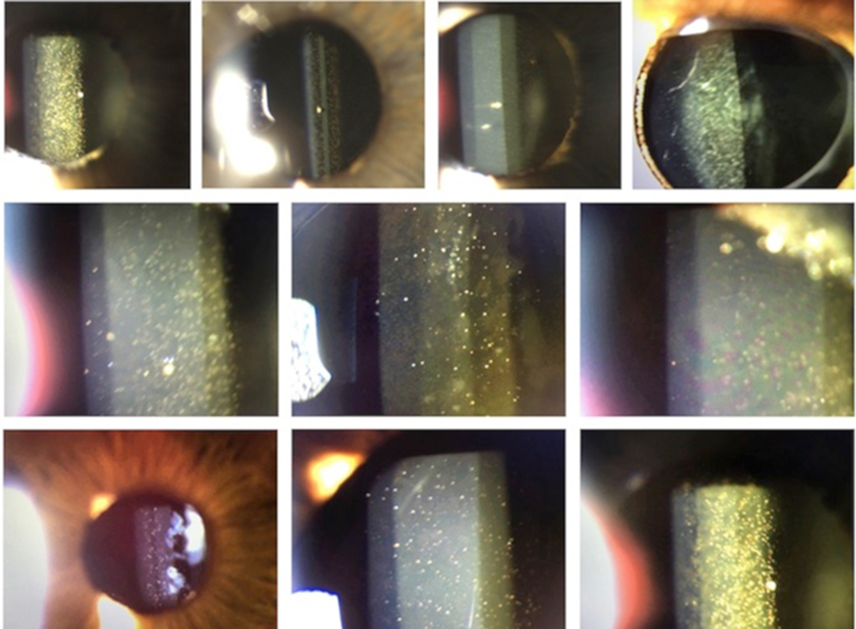 | Figure 1 Slit-lamp images of glistening. |
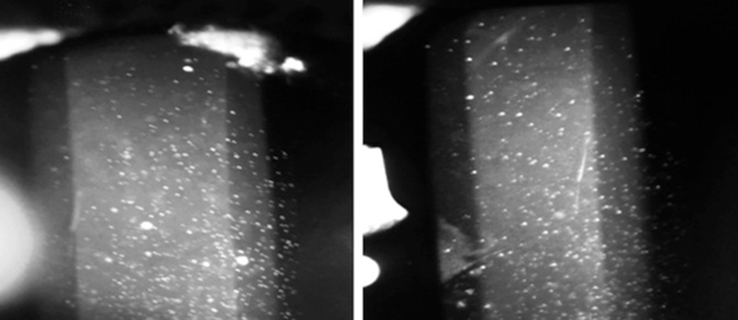 | Figure 2 High-contrast black–white image (slit-lamp photograph) of glistenings. |
Wavefront analysis revealed a reduced modulation transfer function (MTF) as a measure of image quality. Pelli–Robson contrast sensitivity testing revealed a mean value of 1.05±0.21 logCS (from 0.75 to 1.35). In the Halo & Glare simulator computer software (Eyeland-Design network GmbH), patients rated their halo/glare size and intensity on the scale from 0 (no symptoms) to 100 (worst possible symptoms) and the scores are presented in Table 1. Patients had to describe their overall visual function in daily routine. Five patients rated their visual status as “very unsatisfactory” and one patient as “unsatisfactory”. It is noteworthy that in no case – despite the good visual performance – the condition was rated as “satisfactory” or even “very satisfactory”.
All 6 cases were regularly followed in our clinic for at least 12 months, and the presence of other pathologies that could be associated with the symptoms was excluded. In one case, posterior capsule opacification (PCO) was treated by Nd:YAG laser capsulotomy. Patients continued reporting disturbing glare in their daily lives. In a written survey to determine how often patients would ponder about glare or diminished contrasts, 4 patients answered to actively trouble over problems 5–10 times a day, one patient 1–5 times a day and one patient 1–5 times a week.
Therapy
In all cases, the well-being was significantly improved by fitting edge filter blue-light blocking eyeglasses (L500-H) and the consistent wearing of polarized sunglasses outdoors. With this eyewear, the contrast sensitivity improved on average by 0.28 log units (aproximately 1 line on Pelli–Robson chart). Figure 3 shows the simulation of halo and glare in vision simulator without polarized glasses and with polarized glasses. Patients noted slight improvement in the size of halo (from 61±17 to 50±14, Table 1) and glare (from 20±11 to 16±9), but considerable improvement was seen in the intensity, which reduced by approximately 50% (halo intensity reduced from 50±19 to 24±12 and glare intensity from 26±18 to 11±6).
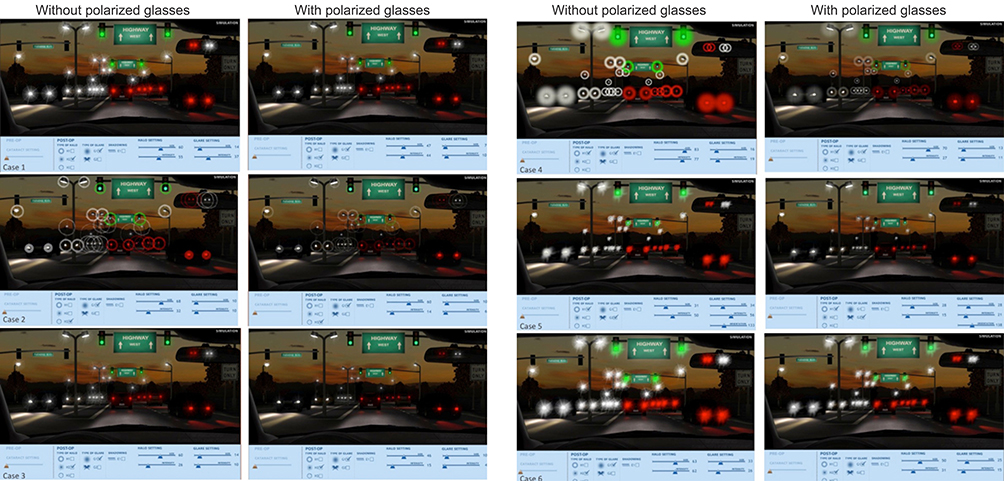 | Figure 3 Halo & Glare simulator in the 6 cases without the use of polarized glasses and with polarized glasses. |
In two cases, the explantation of the IOL was considered, but with good visual acuity, patients were discouraged due to the risks associated with the lens exchange.
Discussion
The first reports of glistening emmerged in 1990s5,6 and referred to reflective, “glittering” points over the entire body of the IOL causing retinal straylight. Although glistenings have been described in various materials, in the majority of cases, it is associated with hydrophobic acrylic lenses.2 The development of glistening is not yet fully understood,1,4 but one hypothesis is commonly referred to: polymers (IOL material) absorb water when immersed in an aqueous environment. Even hydrophobic acrylic IOLs are capable of absorbing small amount of water (generally <1%).1 If the IOL is placed in warm water and the temperature is then lowered, the water inside the polymer becomes oversaturated and, consequently, it separates into phases, collects in a void and forms a visible water droplet.4 The onset of glistening is usually a few months after IOL implantation.4 Although many studies argue glistening has no effect on vision,4 David J. Apple postulated in his legendary “IOL Safety Report” (referring to a database of >19,000 eyes) that glistenings may have clinical significance.7 It was then thought that at least 1% of the cases would contribute to disorders in contrast perception and increased glare. If fibrosis or PCO occurs, performing Nd:YAG capsulotomy may be more difficult due to the glittering deposits in the lens. In these cases, Nd:YAG shots (pitting) may further degrade the optical quality of the lens.
Unfortunately, glistening still remains relatively common more than 20 years since the first report.1,4,7 Although most of the patients remain asymptomatic, with increasing life expectancy and the raising number of pseudophakic patients, practitioners will encounter patients with significant symptoms, even if clinically significant problems were to develop only in a small percentage of patients.
Management of such patients is not always straightforward. Follow-up time seems to be a significant factor in glistening formation and intensity.8,9 Reports of lens exchange as far as 6–15 years postcataract surgery have been presented in the literature.10 Experimental laboratory studies with 20 years simulation of accelerated aging showed a significant deterioration of some IOL materials, possibly attributed to glistening.11 Although explant of an IOL would be the only permanent solution to the problem, surgical intervention at such late postoperative stage can be extremely challenging and might lead to further complications (eg, surgical induced astigmatism, Irvine–Gass syndrome). Conservative approach of managing the symptoms in patients with reasonable corrected visual acuity is often preferred.
In our case report, we presented symptomatic patients who showed improvement in contrast sensitivity and reduction of halo and glare intensity with the use of polarized lenses. This is likely because the light is filtered before it enters IOL affected by glistening, and therefore the amount of optical side effects is generally reduced. However, we believe that the best solution to the problem would be prevention with the choice of glistening-free biomaterials. Patients who opt for premium IOLs often expect spectacle independence. Having to rely on eyewear to relieve unwanted symptoms is, therefore, an inconvenience. Considering our way of life with increased activity in higher age (driving, sports and hobbies), image quality of IOLs plays a high role. Glistenings in monofocal and especially multifocal or toric IOLs, together with the physiological decrease in contrast sensitivity, can be considered to be particularly problematic with increasing age. Affected individuals may be subjectively dissatisfied despite the very good visual acuity due to the sensation of dazzling, halo, starburst or diminished contrasts.
A few studies agree with findings presented in this article.4 Quite recently, Luo et al12 showed that IOLs with glistening implanted at least 5 years prior had decreased contrast sensitivity, point spread function, MTF, increase in spherical aberration and higher straylight value compared to controls with no glistening. The problem can be even more pronounced in patients with multifocal IOLs where quality of vision is potentially compromised due to the nature of the multifocal design. For example, DeHoog and Doraswamy,13 using mathematical modeling, demonstrated substantial reduction of MTF in multifocal IOLs with glistening. The loss of MTF was more significant compared to monofocal IOL. In our case series, we report one patient with a multifocal IOL, where a combination of IOL design and significant glistening has led to severely impaired visual quality. The fact that the patient did not have the symptoms initially but were developed over the months suggests that optical side effects were caused by glistening rather than the multifocality of the lens.
Conclusion
In conclusion, we believe that long-term optical clarity is crucial for the choice of an IOL. Various biomaterials have been extensively researched, and their long-term biocompatibility has been published.7 The choice of IOL should not be based on subjective preference or economic aspects, but on well-founded scientific evidence. Practitioners should provide long-term care to their patients to be able to assess the performance of IOLs, because many aspects of the IOL (such as glistening, centration or PCO susceptibility) are not obvious at early postoperative aftercare visits. In our small case reports, the polarized or edge filter (blue-light blocking) glasses alleviated symptoms associated with glistening, but further studies should be conducted to find options to relieve symptoms in these patients as it is not a rare condition. Although this is only a small case report study, we aimed to improve the understanding of the issue and describe symptoms patients may experience in daily life. Opticians and ophthalmologists should work in collaboration when managing such patients. Corrective eyewear in patients with good visual acuity is the first step, and a referral for an explant should be reserved only for severe cases.
Ethics
This retrospective study was performed in accordance with the ethical standards of the institutional research committee and of the Declaration of Helsinki and its later amendments or comparable ethical standards and used only de-identified patient data. All patients signed an informed consent document. For this type of study, using de-identified data and without clinical intervention, no ethical approval is required in our institution.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Werner L. Glistenings and surface light scattering in intraocular lenses. J Cataract Refract Surg. 2010;36(8):1398–1420. doi:10.1016/j.jcrs.2010.06.003
2. Labuz G, Knebel D, Auffarth GU, et al. Glistening formation and light scattering in six hydrophobic-acrylic intraocular lenses. Am J Ophthalmol. 2018;196:112–120. doi:10.1016/j.ajo.2018.08.032
3. Oshika T, Ando H, Inoue Y, et al. Influence of surface light scattering and glistenings of intraocular lenses on visual function 15 to 20 years after surgery. J Cataract Refract Surg. 2018;44(2):219–225. doi:10.1016/j.jcrs.2017.12.014
4. Pérez-Vives C. Biomaterial influence on intraocular lens performance: an overview. J Ophthalmol. 2018;2018, Article ID 2687385. doi:10.1155/2018/2687385
5. Omar O, Pirayesh A, Mamalis N, Olson RJ. In vitro analysis of Acrysof intraocular lens glistenings in Acrypak and Wagon wheel packaging. J Cataract Refract Surg. 1998;24(1):107–113.
6. Dhaliwal DK, Mamalis N, Olson RJ, et al. Visual significance of glistenings seen in the AcrySof intraocular lens. J Cataract Refract Surg. 1996;22(4):452–457.
7. Apple DJ, Escobar-Gomez M, Zaugg B, Kleinmann G, Borkenstein AF. Modern cataract surgery: unfinished business and unanswered questions. Surv Ophthalmol. 2011;56(6 Suppl):S3–S53. doi:10.1016/j.survophthal.2011.10.001
8. Henriksen BS, Kinard K, Olson RJ. Effect of intraocular lens glistening size on visual quality. J Cataract Refract Surg. 2015;41(6):1190–1198. doi:10.1016/j.jcrs.2014.09.051
9. Colin J, Praud D, Touboul D, Schweitzer C. Incidence of glistenings with the latest generation of yellow-tinted hydrophobic acrylic intraocular lenses. J Cataract Refract Surg. 2012;38(7):1140–1146. doi:10.1016/j.jcrs.2012.01.031
10. Matsushima H, Nagata M, Katsuki Y, et al. Decreased visual acuity resulting from glistening and sub-surface nano-glistening formation in intraocular lenses: a retrospective analysis of 5 cases. Saudi J Ophthalmol. 2015;29(4):259–263. doi:10.1016/j.sjopt.2015.07.001
11. Kawai K, Hayakawa K, Suzuki T. Simulation of 20-year deterioration of acrylic IOLs using severe accelerated deterioration tests. Tokai J Exp Clin Med. 2012;37(3):62–65.
12. Luo F, Bao X, Qin Y, Hou M, Wu M. Subjective visual performance and objective optical quality with intraocular lens glistening and surface light scattering. J Refract Surg. 2018;34(6):372–378. doi:10.3928/1081597X-20180406-01
13. DeHoog E, Doraiswamy A. Evaluation of loss in optical quality of multifocal intraocular lenses with glistenings. J Cataract Refract Surg. 2016;42(4):606–612. doi:10.1016/j.jcrs.2015.10.071
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.