")
Back to Journals » Advances in Medical Education and Practice » Volume 13
Polarity Based Model for Guiding Medical School Strategy During Crisis – A Cross Sectional Qualitative Study
Authors Ahmed SA , Kumar AP, Wasfy NF , Hegazy NN , Abouzeid E , Hassanien MA , Shehata MH , Kayser III WC, Mostafa RM, Khan YH, Hamdy H
Received 1 September 2021
Accepted for publication 22 November 2021
Published 11 January 2022 Volume 2022:13 Pages 11—25
DOI https://doi.org/10.2147/AMEP.S337127
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Samar A Ahmed,1 Archana P Kumar,2,3 Nourhan F Wasfy,4 Nagwa N Hegazy,5 Enjy Abouzeid,4 Mohammed A Hassanien,6,7 Mohamed H Shehata,8,9 W Cliff Kayser III,10 Randa M Mostafa,11 Yawar H Khan,12 Hossam Hamdy13
1Forensic Medicine and Clinical Toxicology Department, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 2Medical Education Unit, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain; 3Department of Physiology, Sri Ramachandra Medical College and Research Institute, SRIHER, Chennai, Tamil Nadu, India; 4Medical Education Department, Faculty of Medicine, Suez Canal University, Ismailia, Egypt; 5Family Medicine Department, Faculty of Medicine, Menoufia University, Menoufia, Egypt; 6Educational Affairs, College of Pharmacy, King Abdulaziz University, Jeddah, Saudi Arabia; 7College of Medicine, Tanta University, Tanta, Egypt; 8Family and community medicine department, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Kingdom of Bahrain; 9Faculty of Medicine, Helwan University, Helwan, Egypt; 10Six SEED Partners, Washington, DC, USA; 11Department of Physiology, Faculty of Medicine, Benha University, Benha, Egypt; 12Riphah International University, Islamabad, Pakistan; 13Gulf Medical University, Ajman, United Arab Emirates
Correspondence: Samar A Ahmed
Forensic Medicine and Clinical Toxicology Department, Faculty of Medicine, Ain Shams University, Cairo, Egypt
Email [email protected]
Background: Crises in academia can best be dealt with as a polarity that needs to be leveraged rather than a problem that needs to be solved. This work aimed at utilizing the Polarity Approach for Continuity and Transformation (PACT)™ to establish a guide for medical schools during times of crisis to minimize the effect of crisis-driven decisions on strategic growth.
Subjects and Methods: A qualitative study following the 5-Steps of the PACT process was conducted. A virtual mapping session was held with 108 medical educators from 22 countries to determine the upsides and downsides of strategic orientation and crisis management subsequently.
Results: Four polarity maps were generated identifying four tension areas; University reputation, mission, teams, and individuals followed by a 72-item assessment and another mapping session to map the warning signs and action steps. A comparison between private school scores and the whole cohort of respondents showed that private schools had the least problems in team-oriented work.
Conclusion: This study highlighted the importance of taking measures to communicate the mission and supporting team functions inside universities either by enhancing resources or utilizing time and effort-saving strategies.
Keywords: polarity, strategy, planning, crisis, medical, education
Background
The COVID-19 pandemic shook the world of academia to extremes.1 Medical schools were worst affected, due to the innate requirements of medical training that commands close communication and physical interaction among doctors, patients, family members, healthcare teams, support staff, etc. This event demonstrated without doubt the transcultural impact of the crisis.2,3
Nevertheless, medical schools across the world navigated through this unprecedented situation through crisis management by introducing drastic changes in methods of teaching and assessment.4,5 The magnitude of this change was huge and automatically most health care institutions shifted to online mode to ensure continuous transfer of knowledge and skills to their students.6–9 The crisis response was very efficient in most situations and students were successfully examined to be promoted to the next year.10–12 However, many of these solutions seemed to be temporary and experts recommended focusing on the strategic plan as well, to achieve long-term sustainability.13
In addition, the reality of pandemics extending over the span of a new academic year drew attention to the fact that the solutions to educational problems needed to be more concrete and permanent.14 Another realization was that the schools functioning in reactive mode to the crisis were more focused on technical needs rather than student engagement, which might disrupt many strategically designed activities directed towards the overall growth and accreditation of the organization.15
The hypothesis is that while extended crises like the COVID pandemic are bound to end at one point, the situation can best be dealt with as a polarity that needs to be strategically managed rather than a problem that needs to be solved.16 This approach has been used to leverage strategic planning in many institutes and is currently being addressed in education.
In health care, crisis and strategic management approaches should be considered as interdependent processes and managed as “both/and” practices instead of “either/or” judgments.17 If schools can successfully manage the shift from crisis mode to a strategy-oriented mindset, they can ensure that their development is minimally affected by the crisis interruption.
Polarity Approach for Continuity and Transformation (PACT)™ is an instrument which that enables an individual, team, or organization to analyze and manage opposing dilemmas in a rapidly changing ecosystem. Many authors have applied (PACT)™ in health care to navigate the conflicts while leveraging the strengths and it is available for purchase.15,17–19
This work aims at utilizing the (PACT)™ model to establish a guide for medical schools that is usable during times of crisis to minimize the effect of crisis-driven decisions on the strategic growth and development of the schools.
Methodology
This study is based on a qualitative approach using content evaluation for deductive analysis. The study followed all the five steps of the (PACT)™ model as shown in Figure 1. The five steps are Seeing, Mapping, Assessing, Learning, and Leveraging.20 All the experiment protocol for involving humans was in accordance to guidelines of Declaration of Helsinki.
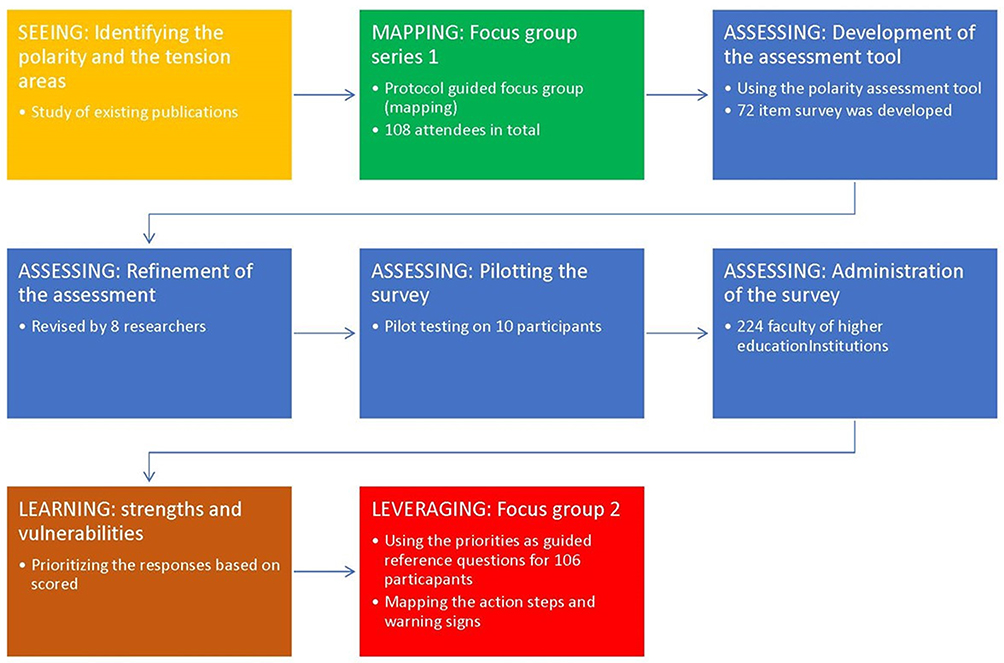 |
Figure 1 Flow chart showing study design and steps of implementation. |
Participants
The participants in this study are medical educators from all over the world belonging to different levels of management. for every stage of the data collection. Purposive sampling was applied in each stage using official invitations sent via email. For the focus group a purposeful sample was selected to represent the medical faculty who are involved in education development at the level of the school, or the country were included in the focus group discussion (FGD). Additionally, the assessment tool was sent to all faculty of various medical colleges.
The Five Steps of the (PACT)™ Model
Step 1, Seeing
The research team recognized the tension in the shift from the pole of growth strategy implementation and the embrace of the pole of crisis management. This was identified through a focus on outcomes of previous post-COVID studies and publications.13
Step 2, Mapping
Polarity was assessed in detail by mapping the key elements of the tension as expressed by key stakeholders. 108 medical educators from 22 countries, with diverse expertise in education and leadership, participated in this study. 30% of them were active decision-makers. The polarity was mapped using (PACT)™ through series of virtual meetings based on the following protocol:
A brief introduction was given to all participants about the study concept and a narrative of one school shifting from the conventional strategic imperatives to adopt the crisis response mode post- COVID-19 strike. Then, they were oriented to the concept of polarities, mapping of vital dimensions of tension areas, and their interdependency utilizing a Polarity Map. They were then divided into four groups, each with one investigator, employing the “breakout room” function of ZOOM. Each group was provided with a unique question from the Polarity Map, to contemplate and respond to.
The Guiding Question
(Group 1) What are the benefits which emerged from the use of short-term responsiveness (crisis management) in the COVID-19 pandemic (reflect on the impact on individuals (students, faculty), teams (working groups), organization mission, University reputation to those from the outside)?
(Group 2) What are the benefits of the university using a strategic orientation (long term/future needs) that are realized during the COVID-19 social distancing (reflect on the impact on individuals (students, faculty), teams (working groups), organization mission, University reputation to those from the outside)?
(Group 3) When short term responsiveness (crisis management) in the COVID-19 pandemic is used to the neglect of strategic orientation (long term/future needs), what are the limitations (reflect on the impact on individuals to the neglect of (students, faculty), teams (working groups), organization mission, University reputation to those from the outside)?
(Group 4) When strategic orientation (long term/future needs) is used to the neglect of short-term responsiveness (crisis management) in COVID-19 pandemic, what are the limitations (reflect on the impact on individuals (students, faculty), teams (working groups), organization mission, University reputation to those from the outside)?
Data Analysis
The ZOOM recording was transcribed by the researchers and coded accordingly. Results were analyzed and grouped thematically. Then the key themes were assigned to each of the map’s quadrants, based on the predetermined categories namely University reputation, mission, teams, and individuals. Two independent investigators verified the accuracy and minor differences were addressed through discussion. Items were identified and mapped in four different polarity maps.
Step 3, Assessing
Seventy-two assessment statements were derived using the (PACT)™ language, developed by Polarity Partnerships (https://assessmypolarities.com/).
An independent group of researchers (NW, EA, AK, NN) revised the assessment items to match with the chosen outcomes. The assessment was piloted among 10 respondents and language refinements were performed accordingly. The final assessment tool was then administered online to faculty and staff of various universities (Appendix).
Step 4, Learning
The results were analyzed and represented in the (PACT)™ web tool, in which each quadrant was coded based on the frequency of its appearance. For each quadrant, the highest-scoring item was identified as a priority strength or vulnerability.
Results were then color-coded based on the frequency into three groups namely, mild, moderate, and severe (http://assessmypolarities.com/). Items belonging to moderate and severe groups were placed as priorities for leveraging.
Step 5, Leveraging
This is the final step in which the Action Steps (to optimize benefits) and Early Warning Signs (to minimize failure) are identified. The participants were split into four groups, during FGD conducted via ZOOM and each was allocated with one question specific for each polarity.
(Group 1) What are the actions/measures you and/or your organization can or could take to gain or retain the benefits which emerged from the FGD on short-term responsiveness (crisis management) in the COVID-19 pandemic (who is going to do what by when?)
(Group 2) What are the actions/measures you and/or your organization can or could (imagine what could be in addition to what is) be doing take to gain or retain the benefits which emerged from the FGD on strategy (long term orientation) in COVID-19 pandemic (who is going to do what by when?)
(Group 3) What are the things you can quantify (measurable indicators) that will guide you to know that you are moving towards the downside of using short-term (tactical) responsiveness? (Reflect on individuals (students, faculty), teams (working groups), organization mission, University reputation to those from the outside)? Focus on Why things are happening … comments/ complaints.
(Group 4) What are the things you can quantify (measurable indicators) that will guide you to know that you are moving towards the downside of using strategic orientation (long term) (imagine what could be in addition to what is)? (Reflect on individuals (students, faculty), teams (working groups), organization mission, University reputation to those from the outside)? Focus on Why things are happening … comments/ complaints.
Ethical Considerations
Prior to starting the study, Ethics approval was obtained from Ain Shams University Research Ethics committee. The consent number is (R 01/2021). An informed oral/ written consent was obtained from all the participants.
Results
Findings from the assessment were mapped into the online polarity assessment system and the results were extracted. 214 participants responded to the assessment. Participants were from 22 countries all over the world with participation from four continents (Africa, Asia, Europe & North America as shown in Table 1).
 |
Table 1 The Distribution of the Participants Among 22 Countries |
140 participants were teachers, 30 participants were first line management, 28 participants were Middle management, and 14 participants were representing the top management with 6 in other positions. Public and private schools were included in the sample. 110 of the participants were affiliated to public school and 104 of the participants were affiliated to private school. Findings from the assessment were documented on four polarity maps highlighting scores of individual items and the prioritized strengths and vulnerability of each map (Figures 2–Figure 5). The results of the assessment reveal that the four tension areas appeared to be well leveraged (Figure 6).
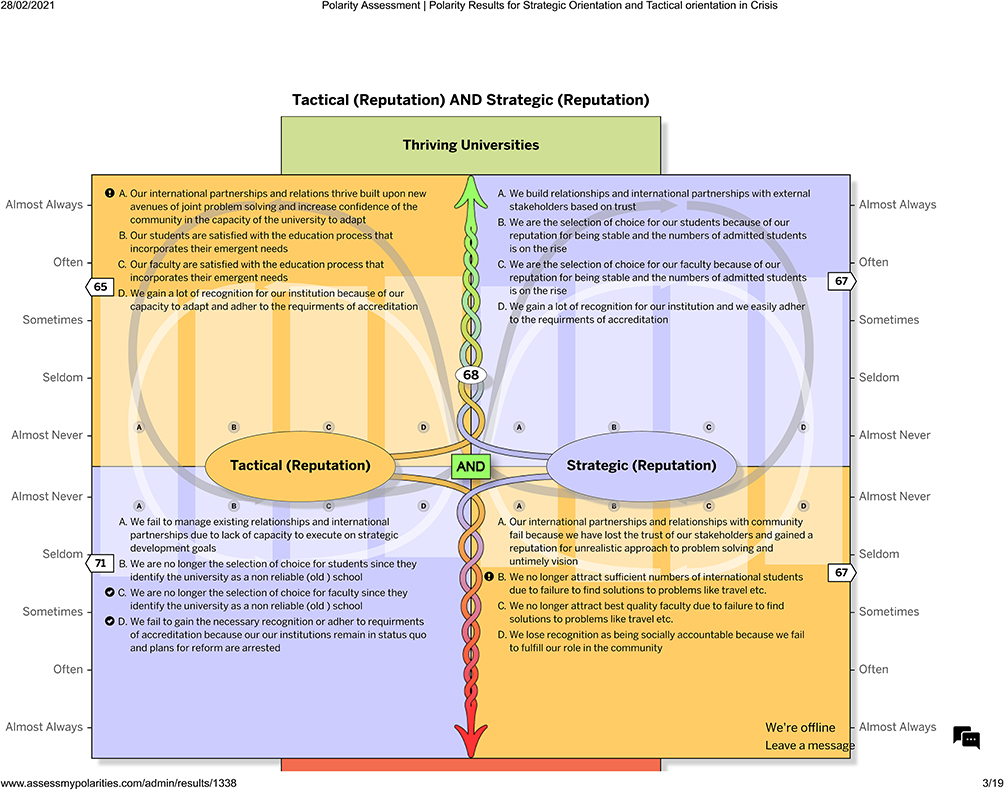 |
Figure 2 Mapping of the tension; University reputation. Notes: Figure adapted from: Polarity Map® (https://www.assessmypolarities.com/).48 Polarity Map® is a registered trademark of Barry Johnson & Polarity Partnerships, LLC. Commercial use encouraged with permission. |
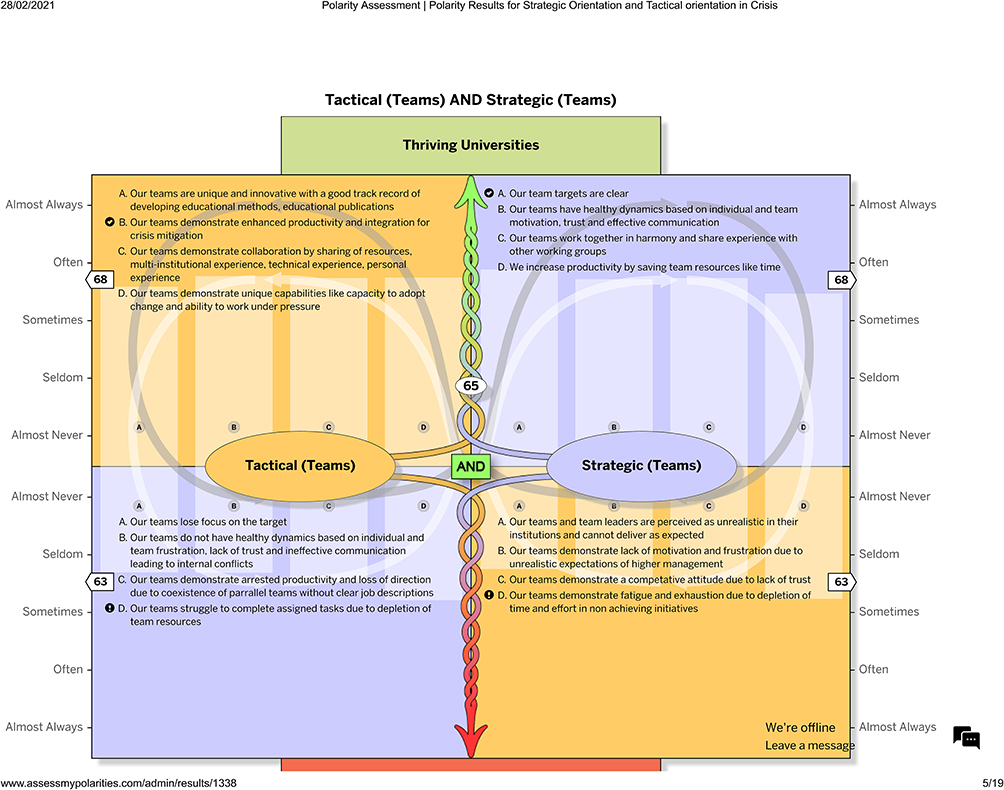 |
Figure 3 Mapping of the tension; Teams. Notes: Figure adapted from: Polarity Map® (https://www.assessmypolarities.com/).48 Polarity Map® is a registered trademark of Barry Johnson & Polarity Partnerships, LLC. Commercial use encouraged with permission. |
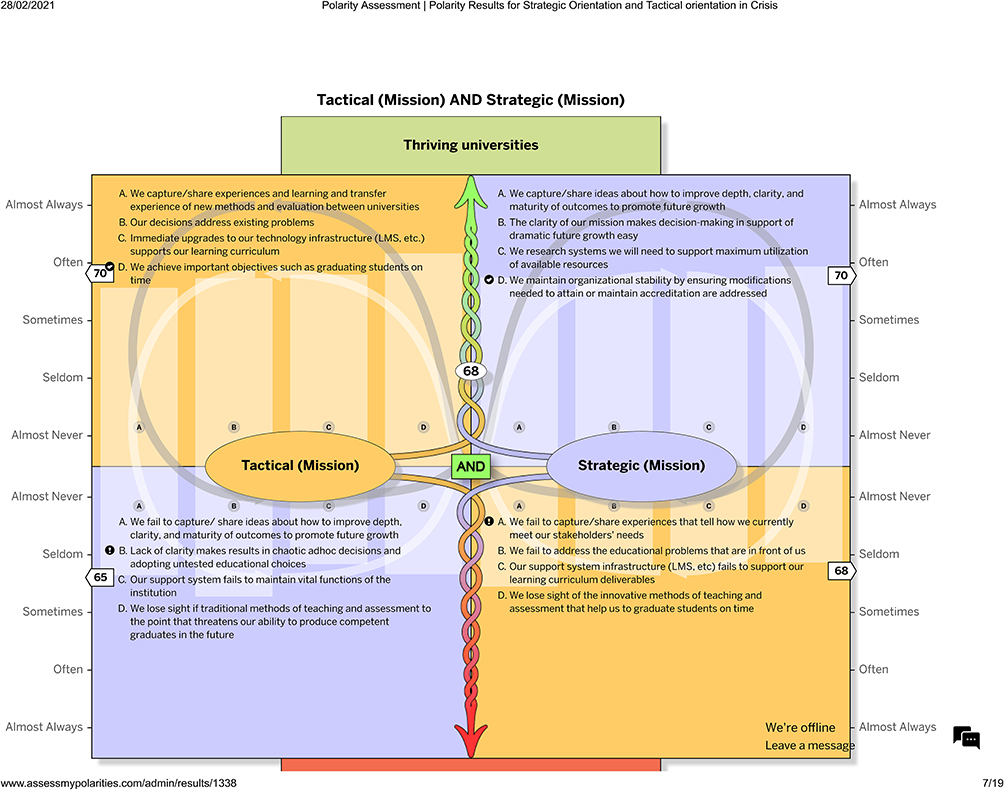 |
Figure 4 Mapping of the tension; University mission. Notes: Figure adapted from: Polarity Map® (https://www.assessmypolarities.com/).48 Polarity Map® is a registered trademark of Barry Johnson & Polarity Partnerships, LLC. Commercial use encouraged with permission. |
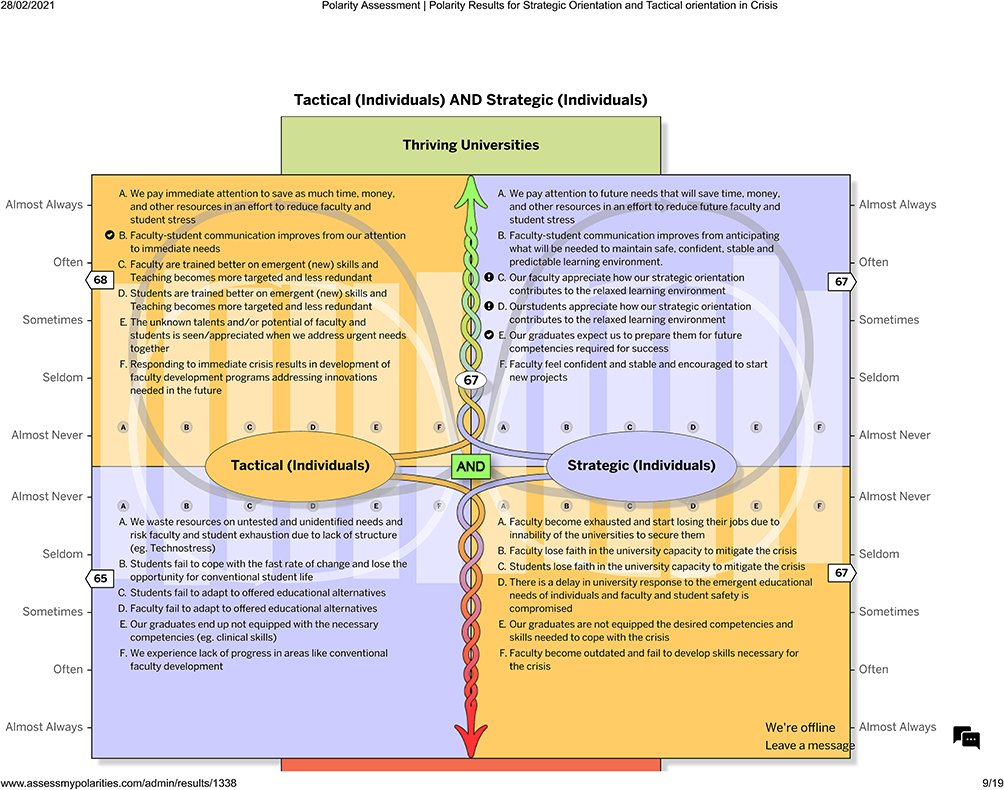 |
Figure 5 Mapping of the tension; Individuals. Notes: Figure adapted from: Polarity Map® (https://www.assessmypolarities.com/).48 Polarity Map® is a registered trademark of Barry Johnson & Polarity Partnerships, LLC. Commercial use encouraged with permission. |
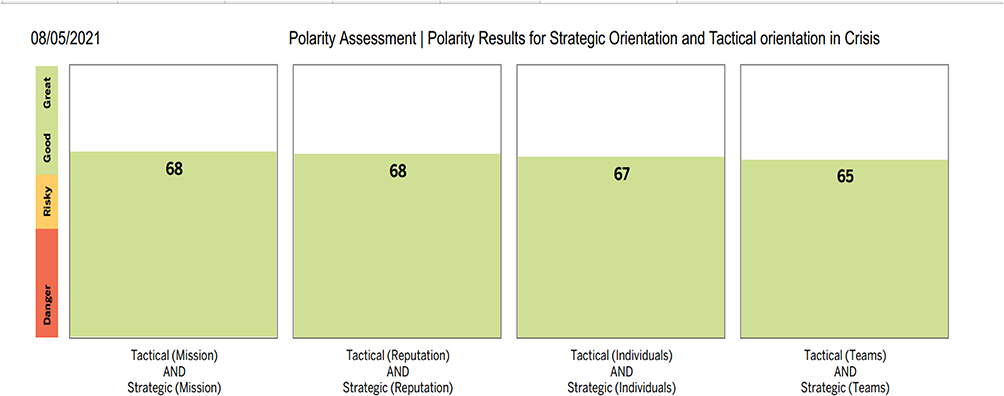 |
Figure 6 Overall mapping of the four tension areas. Notes: Figure adapted from: Polarity Map® (https://www.assessmypolarities.com/).48 Polarity Map® is a registered trademark of Barry Johnson & Polarity Partnerships, LLC. Commercial use encouraged with permission. |
Action Steps and Warning Signs
Findings from the second FGD were identified and mapped on the relevant sections of the maps considering the prioritized strengths and vulnerabilities. These action steps and warning signs are to become the recommendations of this study (Tables 2–3).
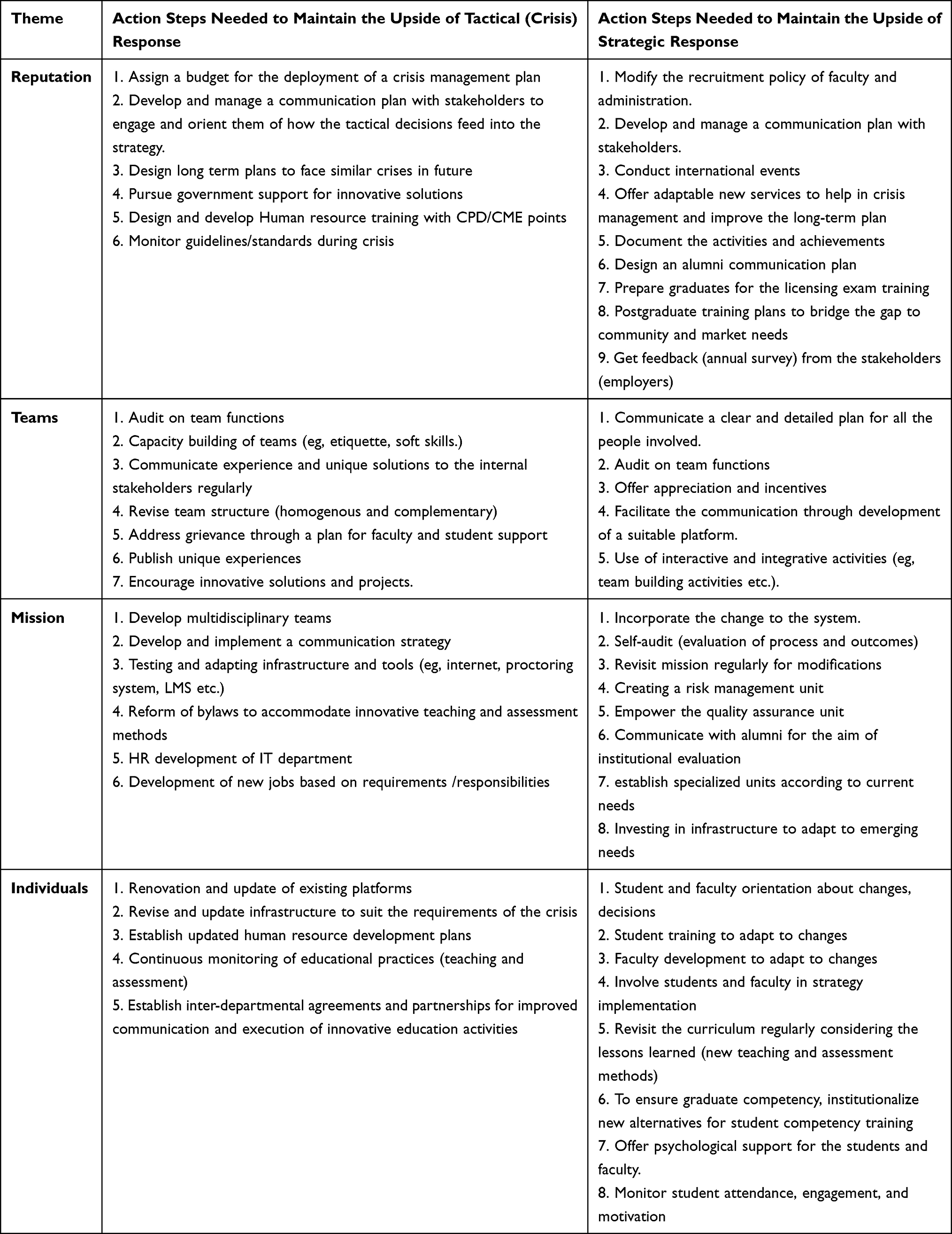 |
Table 2 Action Steps Required to Maintain Upside of Each Pole in the Tested Polarity (Tactical and Strategic Response) |
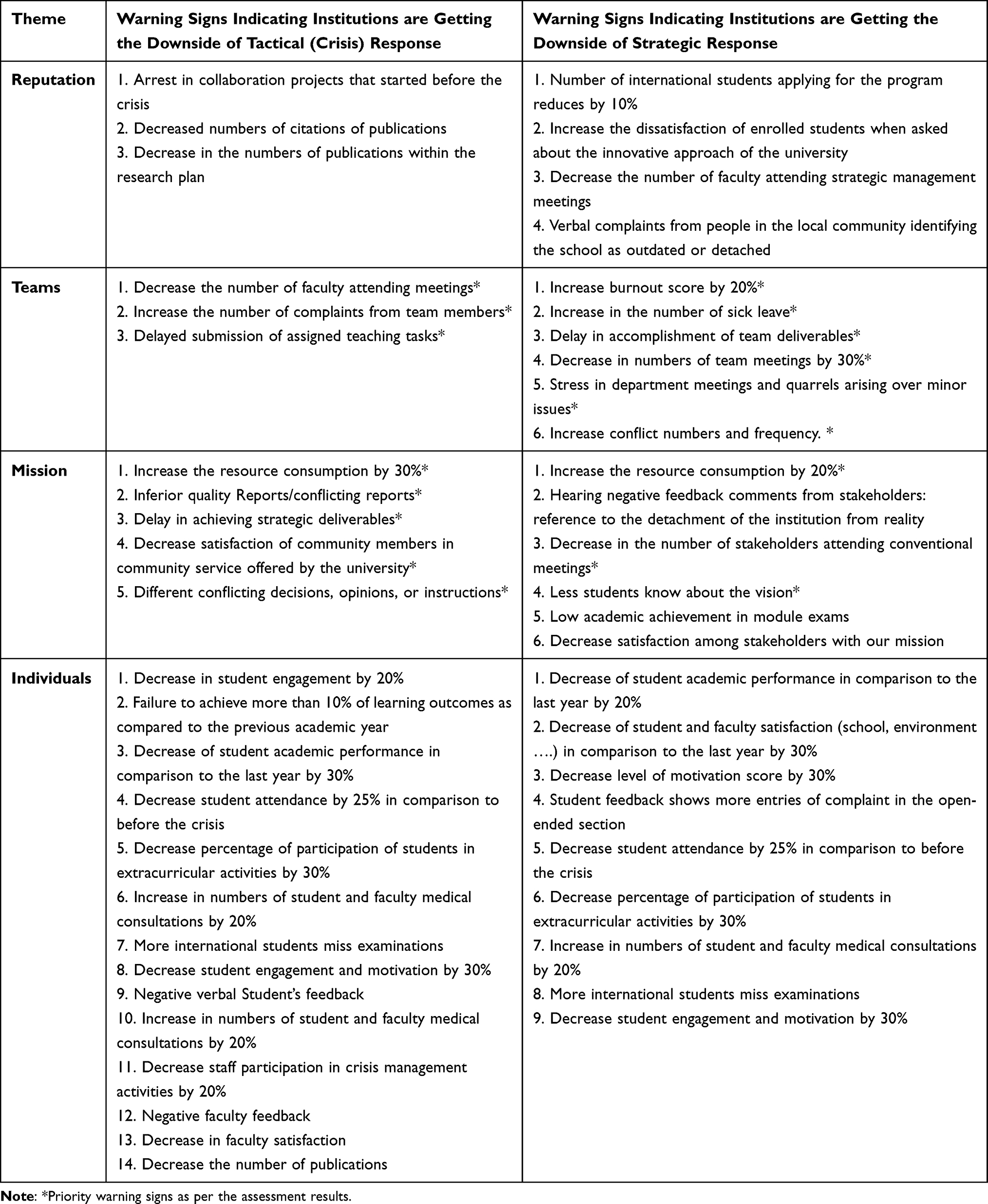 |
Table 3 Warning Signs Indicating Institutions are Getting the Downside of Each Pole in the Tested Polarity (Tactical and Strategic Response) |
Regarding important areas that were identified in the study, a comparison was done between public (governmental schools) and private sector schools. Making the baseline of the study the governmental schools. It was evident that there was a change in the categorization of important aspects upside and downside of the poles in a number of tension areas (Table 4). This was evident in the area of team dynamics where the tension in private schools appeared considerably low.
Discussion
Polarity thinking employs “AND” to link the two poles while problem-solving habitually applies “OR”. It is about Leveraging Polarities to maximize the upsides and minimize the downsides. The Polarity Assessment™ tool offers an accurate measurement of the dynamics of complex and interdependent systems as it focuses on “both/and” Polarity Thinking facilitating the leverage creation for the complex and critical challenges that all leaders, teams, and organizational systems face.21–23
Thematic Representation of Data
The authors recognize that the responses of the participants in the polarity mapping should be considered under four themes namely “individuals”, “teams”, “mission”, and “reputation”. The success of an organization cannot be viewed as a separate entity away from the individuals who constitute it. Researchers in the recent past have recognized the importance of individuals in the performance of any organization.24,25
Concurrently, individuals should also work in teams for prudent allocation of the healthcare workforce and judicious utilization of resources during unprecedented challenges.26 It is well known that all members can individually and collectively participate in developing innovative solutions for complex problems.27 Usually, individuals working in teams choose to adopt ingenious behaviors that may result in enhanced performance, by displaying extra-role behavior, citizenship behavior, social exchange, and reciprocation.26
The mission of a medical school or health care organization serves as the fundamental philosophy that guides all its activities including patient care, research, education, and health promotion.28 The success of educational institutions is assured when their daily existence and culture are in alignment with their organizational values and mission.29 It also reflects their culture, good practices, and precise decision-making while handling an extraordinary situation.30
Reputation is defined as collective beliefs, views, opinions, anticipation, and cognition about an organization.31 Organized and timely responses in change management add value to the judgments about an institutions’ trustworthiness and reliability built over a period of time.32 Therefore, how an institute responds to a challenge or catastrophe will have significant consequences on its reputation, regionally and globally. In summary the dynamics between the individuals, teams, institutional mission and reputation, influence the actions and outcomes of an institution.
Value of Team Support in Crisis
The current study results confirm the value of the team on either pole. It is considered one of the important tension areas to consider either in the tactical or strategic modes. King G (2002) suggests that corporations should have well-organized crisis management teams that are capable of responding collectively during a crisis.33 As suggested by medical educators who participated in the FGD, King emphasized that an institution should have proper guidelines and procedures for communication to effectively manage crises. In agreement with the findings of this research, effective communication between teams allows facilitation and exchanging ideas among diverse departments.
Sommer et al highlighted another critical area that markedly affects the outcomes of teams during a crisis which is the leadership style in an organization.34 Transformational leadership seems to be associated with better performance while inverse effects were found to be associated with passive leadership.
In healthcare, Rice (2014) proves that successful teams can solve challenges in sophisticated organizations such as healthcare as the success of teams and teamwork can lead to better outcomes for patients and staff.35
Clarity of Mission
The mission statement is recognized as an effective tool for regulating and guiding the organization. The importance of mission clarity roots in goal-setting theory36 which explains that when employees understand the institutional goals, they are more motivated to perform better. Moreover, they need to understand how their work may contribute to the overall institutional mission.37
It brings in a sense of belonging, motivation, and inspiration among employees.38 Additionally, the clarity of the mission will reflect transparency that may invest in the public view of the institution.39 It also serves as an instrument of communication for stakeholders.40
Kim et al provided evidence regarding the effect of the strategic alignment in the form of clarity of goals and process and their significantly positive relationship with employee’s engagement and in turn the organization’s performance and sustainability.41 Another study proposes that organizations should possess insightful vision and mission statements for achieving strategic goals.30
Project Indicators
In the current study and based on the data analysis, one of the most prominent warning signs that the polarity is not leveraged and that teams are not functioning their best is the delay in project indicator achievements.
Project success has two integral components, which are management success and product success.42 The success of project management is closely directed to the process of project management, in relation to time, cost, and quality. In other words, these three dimensions reflect what is called “efficiency of project execution”.43 Product success is closely directed to the accomplishment of projects outputs or end products as proposed in the project plan.43
Product success which reflects the success of the achievement of project deliverables and outputs could be considered the success of the project plan or strategy. The indicators for strategy success should include measures that reflect and relate to project outputs. These indicators or measures are related to the project outputs’ deliverable itself for example its alignment to goals, beliefs, and satisfaction.44
Comparing Public Universities and Private Universities
In this study, the comparison between private school scores and the whole cohort of respondents showed that private schools had higher scores in all tension areas but still showed the least score for the “teams” tension.
Comparing private school scores also showed that elements of risk in the whole cohort like the clarity of the mission, the capacity of teams to perform due to lack of resources, and team fatigue and exhaustion were not risky within the private school scores. This is in agreement with many studies comparing capacities to adapt within higher education systems. The augmentation of the digital infrastructure would benefit more blended learning which in turn facilitates online mobility for students and faculty.45
When public schools were considered the baseline and compared to the rest of the cohort, it was clear that there was no increase in the overall scores of each tension area but there were elements within the tension areas that showed a degree of risk compared to the main cohort. These elements include:
International partnerships that are built on confidence in the school to adapt
This is mostly due to the long chain of command in public universities. Public universities usually adopt the “Traditional Hierarchy” or “Hierarchical Structure”. This model supports bureaucracy from top to bottom. The people at the top control the better brains at the bottom resulting in dissatisfaction of lower employees.46
This is in agreement with the findings of the international UNESCO study conducted post-COVID which demonstrated that half of the partnerships were affected or weakened by COVID19.45
Faculty and student satisfaction with the response of the university to their emergent needs and training
The presence of unmet training needs for faculty and students is especially a finding that haunts public universities with a higher student load and lower capacity to adapt timely to the needs. This is in accordance with the same UNESCO study.45
The capacity to attract on international students
This was highlighted as a risky area for public universities. This finding acknowledges the fact that there existed little, or in-school adapted contingency plans for student mobility issues.45
The capacity to save time and effort and arrested productivity and loss of direction due to the coexistence of parallel teams without clear job descriptions.
The presence of parallel teams with the same job description is an element of failure in planning and execution. This usually happens in large institutions that have extensive structures. This duplication tends to happen in times of crisis.47 It usually results in a waste of time and effort that results in fatigue and loss of drive in the workplace. The same hierarchy allows for a large amount of bureaucracy. This is the obstacle that faces public universities when trying to adopt practices that save time and effort.46
Recommendations
The results of this study identify a need to involve teams in extensive preparation for crisis management in anticipation of future crises. Several action steps need to be taken by institutions to maintain the upside of both poles when they are preparing for or anticipating the educational crisis (Table 2). There are also identified indicators that raise flags for institutions when preparing for anticipated crises (Table 3). It is recommended that institutions maintain close observation of these indicators and incorporate them in their strategy’s tested indicators.
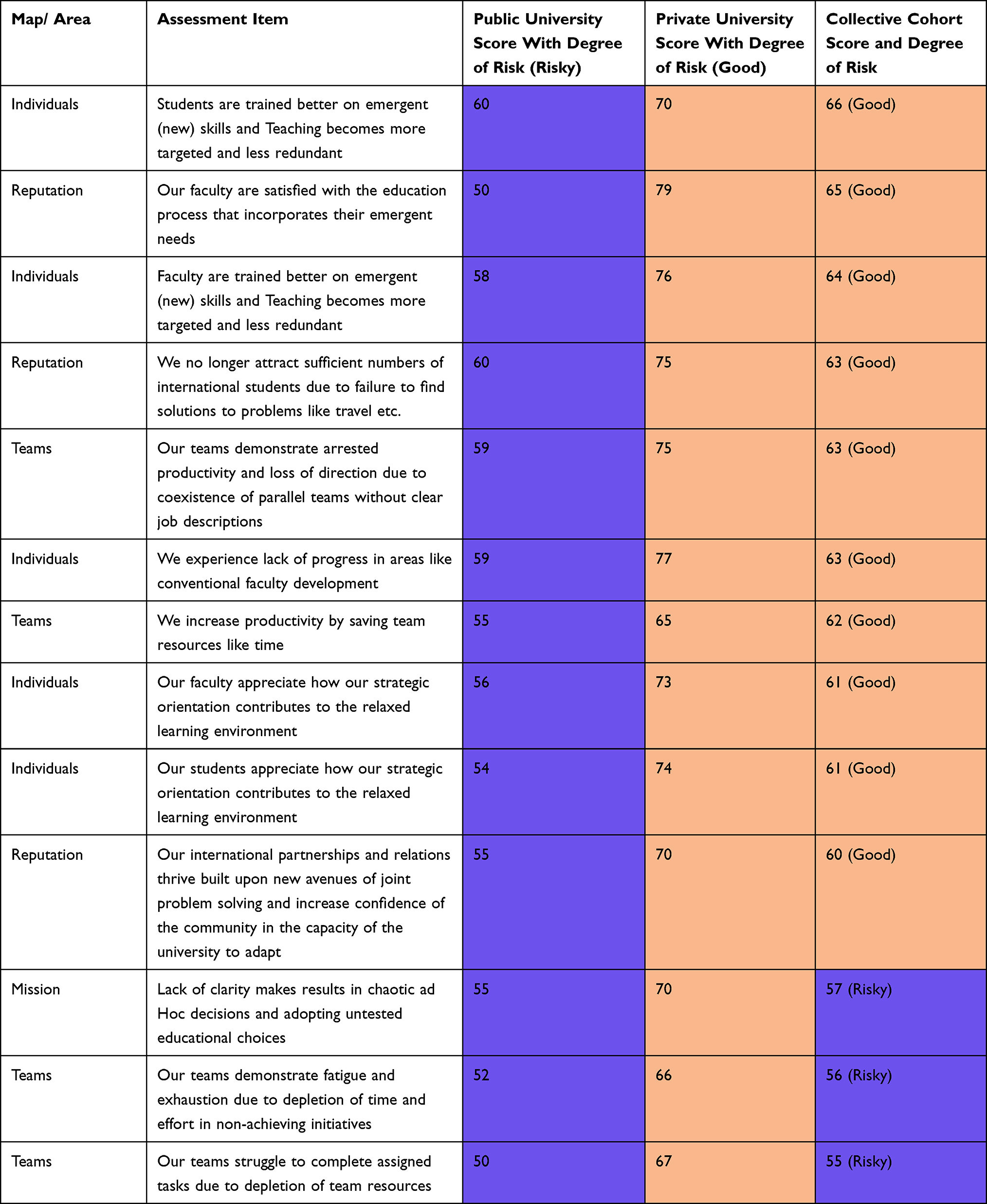 |
Table 4 Comparison Between Assessment Scores of Private Universities and Public Universities |
Limitations
This study shares some limitations of qualitative research. (1) Participating educators are either responders to the sent invitation or nominated by their educational leaders. This nonsystematic sampling approach might exclude educators who are less motivated to participate or who have more serious organizational issues that might reflect contradicting perspectives. (2) Another limitation is dividing participants into four different groups where each group had a specific question to stimulate discussions. This approach might provide some biased inputs from groups as views of participants from other groups were not considered. (3) Biased responses can be another limitation because of peer pressure where participants gave the appropriate responses discussing educational strategies and not responses that reflect reality. (4) Some facilitators might also have influence, or some direction of the opinions and views discussed among their groups.
Conclusion
Using the (PACT)TM model for polarity mapping allows for a novel view of decision-making during a crisis. Managing educational crises needs to be approached as polarity rather than either/or decision-making process. In order to be able to accomplish this, it is recommended to engage in a mapping process and anticipate warning signs attributed to the over-focus on one of the poles. This work offers a guide for universities based on informed inputs of faculty and decision-makers to help with strategic decision-making during times of crisis. The focus of this work sheds light on the importance of taking all measures to communicate the mission and clarify it to internal and external stakeholders. It also draws attention to the importance of support of team functions inside universities either by enhancing resources or utilizing time and effort-saving strategies. These are the priority strategies that need to be deployed during times of crisis.
Data Sharing Statement
“Model for Guiding Medical School Strategy during Crisis Using (PACT)™ a Cross Sectional Qualitative Study” data set are available at Harvard Dataverse: doi: https://doi.org/10.7910/DVN/QWLRGP.
Ethics Approval and Consent to Participate
Ethics approval was obtained from Ain Shams University Research Ethics committee. The consent number is (R 01/2021). An informed oral/written consent was obtained from all the participants that was approved by Ain Shams University Research Ethics committee.
Consent for Publication
All authors have read the manuscript and have given consent for publication of this manuscript.
Acknowledgments
The authors would like to thank the medical educators who participated in the study. Additionally, acknowledging their special contribution to the mapping process.
Samar A Ahmed is currently affiliated with the Delta University, Faculty of Medicine, Dakahlia, Egypt.
Author Contributions
1. All the authors have made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas.
2. All the authors have drafted or written, or substantially revised or critically reviewed the article.
3. All the authors have agreed on the journal to which the article was submitted.
4. All the authors have reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage.
5. All the authors agree to take responsibility and be accountable for the contents of the article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mustafa N. Impact of the 2019–20 coronavirus pandemic on education. Int J Health Serv. 2020;7:1–12.
2. Goh P-S, Sandars J. A vision of the use of technology in medical education after the COVID-19 pandemic. MedEdPublish. 2020;9:1–8.
3. Liang ZC, Ooi SBS, Wang W. Pandemics and their impact on medical training: lessons from Singapore. Acad Med. 2020;95(9):1359–1361. doi:10.1097/ACM.0000000000003441
4. Hall AK, Nousiainen MT, Campisi P, et al. Training disrupted: practical tips for supporting competency-based medical education during the COVID-19 pandemic. Med Teach. 2020;42(7):756–761. doi:10.1080/0142159X.2020.1766669
5. Rose S. Medical student education in the time of COVID-19. JAMA. 2020;323(21):2131–2132. doi:10.1001/jama.2020.5227
6. Bezerra IMP. State of the art of nursing education and the challenges to use remote technologies in the time of Corona virus pandemic. J Hum Growth Dev. 2020;30(1):141–147. doi:10.7322/jhgd.v30.10087
7. Dewart G, Corcoran L, Thirsk L, Petrovic K. Nursing education in a pandemic: academic challenges in response to COVID-19. Nurse Educ Today. 2020;92:104471. doi:10.1016/j.nedt.2020.104471
8. Alexander L, Ashcroft J, Byrne MHV, Wan J. All hands on deck: early graduation of senior medical students in the COVID-19 pandemic. MedEdPublish. 2020;9. doi:10.15694/mep.2020.000096.1
9. Ting ASJ, Ho CLT. Outbreak measures taken by medical schools during the coronavirus pandemic in London, United Kingdom: a qualitative study; 2020.
10. Amin HA, Shehata MHK, Ahmed SA. Step-by-step guide to create competency-based assignments as an alternative for traditional summative assessment. MedEdPublish. 2020;9:120.
11. Shehata MHK, Abouzeid E, Wasfy NF, Abdelaziz A, Wells RL, Ahmed SA. Medical education adaptations post COVID-19: an Egyptian reflection. J Med Educ Curric Dev. 2020;7:2382120520951819. doi:10.1177/2382120520951819
12. Kumar AP, Al Ansari AM, Shehata MHK, et al. Evaluation of curricular adaptations using digital transformation in a medical school in Arabian gulf during the COVID-19 pandemic. J Microsc Ultrastruct. 2020;8(4):186. doi:10.4103/jmau.jmau_87_20
13. Ehrlich H, McKenney M, Elkbuli A. Strategic planning and recommendations for healthcare workers during the COVID-19 pandemic. Am J Emerg Med. 2020;38(7):1446–1447. doi:10.1016/j.ajem.2020.03.057
14. Macdougall C, Dangerfield P, Katz D, Strain WD. The impact of COVID-19 on medical education and medical students. How and when can they return to placements? MedEdPublish. 2020;9:1–9.
15. Ahmed SA, Hegazy NN, Malak HWA, et al. Model for utilizing distance learning post COVID-19 using (PACT)™ a cross sectional qualitative study. BMC Med Educ. 2020;20(1):1–13. doi:10.1186/s12909-020-02311-1
16. Preble JF. Integrating the crisis management perspective into the strategic management process. J Manag Stud. 1997;34(5):769–791. doi:10.1111/1467-6486.00071
17. Monrad SU, Mangrulkar RS, Woolliscroft JO, et al. Competency committees in undergraduate medical education: approaching tensions using a polarity management framework. Acad Med. 2019;94(12):1865–1872. doi:10.1097/ACM.0000000000002816
18. Holcombe RF. Improving health care quality: a polarity management perspective. Acad Med. 2015;90(2):259. doi:10.1097/ACM.0000000000000595
19. Keenan MJ, Hurst JB, Olnhausen K. Polarity management for quality care: self-direction and manager direction. Nurs Adm Q. 1993;18(1):23–29. doi:10.1097/00006216-199301810-00007
20. Johnson B. And: Making a Difference by Leveraging Polarity, Paradox, or Dilemma. Volume One: Foundations. HRD Press; 2020.
21. Yarime M, Tanaka Y. The issues and methodologies in sustainability assessment tools for higher education institutions: a review of recent trends and future challenges. J Educ Sustain Dev. 2012;6(1):63–77. doi:10.1177/097340821100600113
22. Baker MN. Organization use of self: a new symbol of leadership. Leader to Leader. 2016;2016(81):47–52. doi:10.1002/ltl.20245
23. Johnson B. Reflections: a perspective on paradox and its application to modern management. J Appl Behav Sci. 2014;50(2):206–212. doi:10.1177/0021886314524909
24. Mustafa M, Gavin F, Hughes M. Contextual determinants of employee entrepreneurial behavior in support of corporate entrepreneurship: a systematic review and research agenda. J Enterp Cult. 2018;26(3):285–326. doi:10.1142/S0218495818500115
25. Kraus S, Breier M, Jones P, Hughes M. Individual entrepreneurial orientation and intrapreneurship in the public sector. Int Entrepreneurship Manag J. 2019;15(4):1247–1268. doi:10.1007/s11365-019-00593-6
26. Covin JG, Rigtering JPC, Hughes M, Kraus S, Cheng C-F, Bouncken RB. Individual and team entrepreneurial orientation: scale development and configurations for success. J Bus Res. 2020;112:1–12. doi:10.1016/j.jbusres.2020.02.023
27. Hughes M, Rigtering JPC, Covin JG, Bouncken RB, Kraus S. Innovative behaviour, trust and perceived workplace performance. Br J Manag. 2018;29(4):750–768. doi:10.1111/1467-8551.12305
28. Lahey T, Nelson W. A dashboard to improve the alignment of healthcare organization decision making to core values and mission statement. Camb Q Healthc Ethics. 2020;29(1):156–162. doi:10.1017/S0963180119000884
29. Darr KJ. Management education in public health: further considerations: comment on “management matters: a leverage point for health systems strengthening in Global Health”. Int J Health Policy Manag. 2015;4(12):861. doi:10.15171/ijhpm.2015.158
30. Taiwo AA, Lawal FA, Agwu PE. Vision and mission in organization: myth or heuristic device? Int J Bus Manag. 2016;4(3):1–8.
31. Walker K. A systematic review of the corporate reputation literature: definition, measurement, and theory. Corp Reput Rev. 2010;12(4):357–387. doi:10.1057/crr.2009.26
32. Clardy A. Organizational reputation: issues in conceptualization and measurement. Corp Reput Rev. 2012;15(4):285–303. doi:10.1057/crr.2012.17
33. King G. Crisis management & team effectiveness: a closer examination. J Bus Ethics. 2002;41(3):235–249. doi:10.1023/A:1021200514323
34. Sommer SA, Howell JM, Hadley CN. Keeping positive and building strength: the role of affect and team leadership in developing resilience during an organizational crisis. Group Org Manag. 2016;41(2):172–202. doi:10.1177/1059601115578027
35. Rice MM. Strategies for clinical team building: the importance of teams in medicine. In: Emergency Department Leadership and Management: Best Principles and Practice. 2014:47.
36. Locke EA. Guest editor’s introduction: goal-setting theory and its applications to the world of business. Acad Manag Perspect. 2004;18(4):124–125. doi:10.5465/ame.2004.15268720
37. Desmidt S, Prinzie A. Establishing a mission-based culture: analyzing the relation between intra-organizational socialization agents, mission valence, public service motivation, goal clarity and work impact. Int Public Manag J. 2019;22(4):664–690. doi:10.1080/10967494.2018.1428253
38. Alawneh AA. The impact of mission statement on performance: an exploratory study in the Jordanian banking industry. J Manag Policy Pract. 2015;16(4):73.
39. Norman SM, Avolio BJ, Luthans F. The impact of positivity and transparency on trust in leaders and their perceived effectiveness. Leadersh Q. 2010;21(3):350–364. doi:10.1016/j.leaqua.2010.03.002
40. Darbi WPK. Of mission and vision statements and their potential impact on employee behaviour and attitudes: the case of a public but profit-oriented tertiary institution. Int J Bus Soc Sci. 2012;3:14.
41. Kim J, Kim H, Kwon H. The impact of employees’ perceptions of strategic alignment on sustainability: an empirical investigation of Korean firms. Sustainability. 2020;12(10):4180. doi:10.3390/su12104180
42. Baccarini D. The logical framework method for defining project success. Proj Manag J. 1999;30(4):25–32. doi:10.1177/875697289903000405
43. Pinkerton W. Project Management: Achieving Project Bottom-Line Succe. McGraw Hill Professional; 2003.
44. Bannerman PL. Defining project success: a multilevel framework. In
45. Marinoni G, Van’t Land H, Jensen T. The impact of Covid-19 on higher education around the world. IAU Global Survey Report; 2020.
46. Asita MP, Alasomuka VA. Chain of command in higher education. Int J Inst Leadersh Policy Manag. 2019;1(1):92–105.
47. Ahmed SA, Shehata MHK, Wells RL, Amin HAA, Atwa HSM. Step-by-step guide to managing the educational crisis: lessons learned from COVID-19 pandemic. J Microsc Ultrastruct. 2020;8(4):193. doi:10.4103/jmau.jmau_79_20
48. Barry Johnson & Polarity Partnerships, LLC. Polarity Map®; 2021. Available from: https://www.assessmypolarities.com/.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.