")
Back to Journals » Advances in Medical Education and Practice » Volume 7
Point-of-care echocardiography in simulation-based education and assessment
Authors Amini R, Stolz L, Javedani P, Gaskin K, Baker N, Ng V, Adhikari S
Received 5 October 2015
Accepted for publication 10 March 2016
Published 31 May 2016 Volume 2016:7 Pages 325—328
DOI https://doi.org/10.2147/AMEP.S97658
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Richard Amini, Lori A Stolz, Parisa P Javedani, Kevin Gaskin, Nicola Baker, Vivienne Ng, Srikar Adhikari
Department of Emergency Medicine, University of Arizona Medical Center, Tucson, AZ, USA
Background: Emergency medicine milestones released by the Accreditation Council for Graduate Medical Education require residents to demonstrate competency in bedside ultrasound (US). The acquisition of these skills necessitates a combination of exposure to clinical pathology, hands-on US training, and feedback.
Objectives: We describe a novel simulation-based educational and assessment tool designed to evaluate emergency medicine residents’ competency in point-of-care echocardiography for evaluation of a hypotensive patient with chest pain using bedside US.
Methods: This was a cross-sectional study conducted at an academic medical center. A simulation-based module was developed to teach and assess the use of point-of-care echocardiography in the evaluation of the hypotensive patient. The focus of this module was sonographic imaging of cardiac pathology, and this focus was incorporated in all components of the session: asynchronous learning, didactic lecture, case-based learning, and hands-on stations.
Results: A total of 52 residents with varying US experience participated in this study. Questions focused on knowledge assessment demonstrated improvement across the postgraduate year (PGY) of training. Objective standardized clinical examination evaluation demonstrated improvement between PGY I and PGY III; however, it was noted that there was a small dip in hands-on scanning skills during the PGY II. Clinical diagnosis and management skills also demonstrated incremental improvement across the PGY of training.
Conclusion: The 1-day, simulation-based US workshop was an effective educational and assessment tool at our institution.
Keywords: point-of care ultrasound, simulation education
Introduction
Determining the etiology of undifferentiated hypotension is a common diagnostic and therapeutic dilemma encountered by emergency physicians. Use of other imaging modalities is precluded in the case of an unstable hypotensive patient, making bedside ultrasound (US) invaluable. Bedside US can assist the emergency physician quickly make critical decisions that can alter a patient’s clinical course and ultimate outcome.1–3 A number of protocols have been developed guiding the use of bedside US in patients with undifferentiated hypotension.1,4–6
The Accreditation Council for Graduate Medical Education (ACGME) requires the use of US for diagnostic evaluation as a core competency milestone for emergency medicine (EM) residency training programs. Most accredited residency programs incorporate US training into the resident curriculum, though specific components and clinical time devoted to US training are highly variable among programs.7,8 Proctored US hands-on instruction and training modules have been shown to positively impact US training; however, to our knowledge, US-focused simulation-based training has not been studied before.9,10 This study evaluated a novel simulation-based US educational and assessment workshop.
Methods
Study design and setting
This was a single-center cross-sectional study conducted at an academic medical center. This study was reviewed and approved by the University of Arizona institutional review board authority. Written informed consent from participants was not required as per IRB. The study participants were 52 EM residents (postgraduate year [PGY]-I to PGY-III) with varying US experience. Participation in the study was voluntary. Data were collected from December 2013 to January 2014.
Education
A 1-day educational and assessment workshop focusing on simulation-based US training was integrated into the scheduled education day for EM residents. The focus of this workshop was sonographic imaging of cardiac pathology, which was incorporated during all components of the session, including a pre-workshop survey, objective structured clinical examination (OSCE), hands-on education station, simulation-based diagnostic session, and simulation-based management station (Table 1). Simulation of real clinical scenarios relevant to management of the hypotensive patient with chest pain was integrated into the workshop. Instructors for this course were Department of Emergency Medicine faculty and fellows with expertise in bedside US.
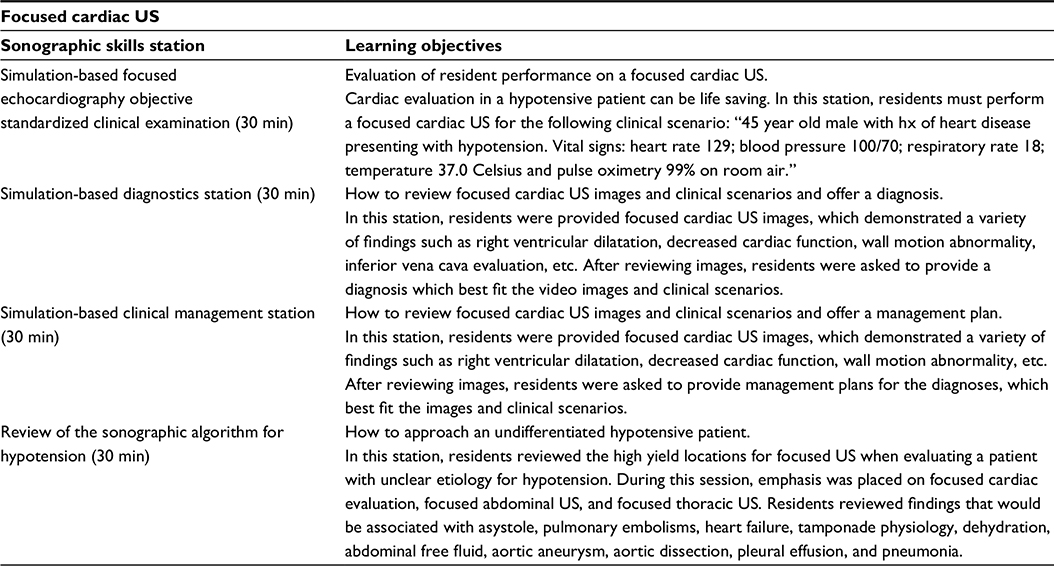 | Table 1 Skills station descriptions Abbreviations: US, ultrasound; min, minutes; hx, history. |
Assessment
Resident assessment of these sonographic skills consisted of a 29-question multiple-choice online survey, five-item simulated visual diagnosis survey, five-item simulated imaging-based clinical management survey, and a simulated hands-on point-of-care echocardiography OSCE.
Data analysis
All analyses were performed using Stata 11 (StataCorp LP, College Station, TX, USA). Data were presented as mean values and percentages with 95% confidence intervals. Continuous variables were compared between the two groups (posttest versus 3-month posttest) using Student’s t-test and Wilcoxon signed-rank test. The statistical level of significance was set at P<0.05.
Results
A total of 52 residents with varying US experience participated in this study. Questions focused on knowledge assessment demonstrated consistent improvements across PGY of training. The average scores on the online knowledge-based survey were PGY I: 63% (standard deviation [SD] =10), PGY II: 70% (SD =7), and PGY III: 72% (SD =5). Seventy-one percent of the residents completed the clinical diagnosis and clinical management survey. Similar to the knowledge-based survey, the residents’ clinical diagnostic skills and clinical management skills also revealed incremental improvement across PGY of training. The average scores on the clinical diagnosis survey were PGY I: 78% (SD =22), PGY II: 77% (SD =27), and PGY III: 93% (SD =10). The average scores on the clinical management survey were PGY I: 62% (SD =19), PGY II: 62% (SD =19), and PGY III: 91% (SD =13). All 52 residents participated in the cardiac US OSCE. Interestingly, the OSCE evaluation demonstrated improvement between PGY I and PGY III; however, there was a small decrease in hands-on scanning skills during the PGY II. The average scores on the OSCE were PGY I: 78% (SD =7), PGY II: 74% (SD =8), and PGY III: 82% (SD =9).
Discussion
Numerous underlying pathologies can contribute to hypotension in a patient with chest pain. While cardiac echocardiography can provide valuable information, a comprehensive echo often cannot be obtained in these situations. Bedside US can provide invaluable information about overall cardiac contractility and wall motion abnormalities and identify pathology, such as pericardial tamponade or pericardial effusion, that may benefit from immediate intervention. Resuscitation without understanding of the underlying pathology can lead to poor outcomes and patient demise.
Current literature has demonstrated that, in addition to improving clinical outcomes, simulation-based learning in medicine has positive impact on learner performance, knowledge, and confidence.11,12 Delivering high-quality patient care while simultaneously providing optimal physician training is rarely possible, and simulation has emerged as a tool to reconcile this gap.13,14 The ACGME mandates US training as a core competency milestone for EM residents. Proctored hands-on simulation has been shown to positively impact resident knowledge retention.9 While EM residency programs provide some form of US training, a standardized curriculum does not exist and educational training is highly variable.7,15 Furthermore, a gold standard for milestone training or assessment has not been established.8
In this study, we developed and implemented a unique training system merging simulation-based milestone education and assessment. The assessment component was integrated into each station of this 2-hour workshop: technical skills were assessed with the OSCE, clinical diagnostic skills were assessed with video clips in the diagnosis station, and clinical management skills were assessed with two-step reasoning questions following each clinical management station (Table 1). To our knowledge, this is the first workshop to integrate numerous components of assessment with a focus on the EM US milestone recommendations.16
Our results demonstrate improvement in resident scores across successive PGY on the online survey and the clinical diagnosis and clinical management survey, as evidenced by the absolute average and narrowing of SDs. PGY III residents had the highest performance on the cardiac US OSCE. This would be expected as a higher PGY correlates with greater clinical experience and increased US exposure. This is similar to previous studies, which demonstrated greater scores among the most senior residents.17 In our investigation, PGY I residents scored higher on the cardiac OSCE than PGY II residents; this difference may be attributable to proximity to US rotation (at our institution, the interns have a dedicated 2-week US rotation).
Management of complex patients in the emergency setting requires prompt yet thoughtful evaluation. Providers must quickly and effectively process information from multiple facets to appropriately manage patients. Simulating stressful, intense environments allows residents to learn how to treat and evaluate high-risk conditions without increasing risk of harm to live patients, making simulation a valuable component of residency training.18–21
Limitations
This study is limited by its small sample size. The education and assessment curriculum was not pilot-tested or validated prior to implementation. Lastly, this study was not designed to assess overall impact of this simulation-based US workshop.
Conclusion
The 1-day, simulation-based US educational event was an effective educational and assessment tool at our institution.
Disclosure
The authors report no conflicts of interest in this work.
References
Schmidt GA, Koenig S, Mayo PH. Shock: ultrasound to guide diagnosis and therapy. Chest. 2012;142(4):1042–1048. | ||
Jones AE, Tayal VS, Sullivan DM, Kline JA. Randomized, controlled trial of immediate versus delayed goal-directed ultrasound to identify the cause of nontraumatic hypotension in emergency department patients. Crit Care Med. 2004;32(8):1703–1708. | ||
Manno E, Navarra M, Faccio L, et al. Deep impact of ultrasound in the intensive care unit: the “ICU-sound” protocol. Anesthesiology. 2012;117(4):801–809. | ||
Rose JS, Bair AE, Mandavia D, Kinser DJ. The UHP ultrasound protocol: a novel ultrasound approach to the empiric evaluation of the undifferentiated hypotensive patient. Am J Emerg Med. 2001;19(4):299–302. | ||
Volpicelli G, Lamorte A, Tullio M, et al. Point-of-care multiorgan ultrasonography for the evaluation of undifferentiated hypotension in the emergency department. Intensive Care Med. 2013;39(7):1290–1298. | ||
Perera P, Mailhot T, Riley D, Mandavia D. The RUSH exam: Rapid Ultrasound in SHock in the evaluation of the critically III. Emerg Med Clin North Am. 2010;28(1):29–56, vii. | ||
Counselman FL, Sanders A, Slovis CM, Danzl D, Binder LS, Perina DG. The status of bedside ultrasonography training in emergency medicine residency programs. Acad Emerg Med. 2003;10(1):37–42. | ||
Amini R, Adhikari S, Fiorello A. Ultrasound competency assessment in emergency medicine residency programs. Acad Emerg Med. 2014;21(7):799–801. | ||
Noble VE, Nelson BP, Sutingco AN, Marill KA, Cranmer H. Assessment of knowledge retention and the value of proctored ultrasound exams after the introduction of an emergency ultrasound curriculum. BMC Med Educ. 2007;7:40. | ||
Kerwin C, Tommaso L, Kulstad E. A brief training module improves recognition of echocardiographic wall-motion abnormalities by emergency medicine physicians. Emerg Med Int. 2011;2011:483242. | ||
Ma IW, Brindle ME, Ronksley PE, Lorenzetti DL, Sauve RS, Ghali WA. Use of simulation-based education to improve outcomes of central venous catheterization: a systematic review and meta-analysis. Acad Med. 2011;86(9):1137–1147. | ||
Britt RC, Reed SF, Britt LD. Central line simulation: a new training algorithm. Am Surg. 2007;73(7):680–682. | ||
Gaba DM. The future vision of simulation in health care. Qual Saf Health Care. 2004;13(suppl 1):i2–i10. | ||
Reznek M, Harter P, Krummel T. Virtual reality and simulation: training the future emergency physician. Acad Emerg Med. 2002;9(1):78–87. | ||
Witting MD, Euerle BD, Butler KH. A comparison of emergency medicine ultrasound training with guidelines of the society for academic emergency medicine. Ann Emerg Med. 1999;34(5):604–609. | ||
Lewiss RE, Pearl M, Nomura JT, et al. CORD-AEUS: consensus document for the emergency ultrasound milestone project. Acad Emerg Med. 2013;20(7):740–745. | ||
Nicksa GA, Anderson C, Fidler R, Stewart L. Innovative approach using interprofessional simulation to educate surgical residents in technical and nontechnical skills in high-risk clinical scenarios. JAMA Surg. 2015;150(3):201–207. | ||
Ziv A, Wolpe PR, Small SD, Glick S. Simulation-based medical education: an ethical imperative. Acad Med. 2003;78(8):783–788. | ||
Hammond J. Simulation in critical care and trauma education and training. Curr Opin Crit Care. 2004;10(5):325–329. | ||
Lake CL. Simulation in cardiology and cardiothoracic and vascular surgery. Semin Cardiothorac Vasc Anesth. 2005;9(4):325–333. | ||
Binstadt ES, Walls RM, White BA, et al. A comprehensive medical simulation education curriculum for emergency medicine residents. Ann Emerg Med. 2007;49(4):495–504, 504.e1–e11. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.