")
Back to Journals » Orthopedic Research and Reviews » Volume 11
Platelet-rich plasma (PRP) treatment of noninsertional Achilles tendinopathy in a two case series: no significant difference in effect between leukocyte-rich and leukocyte-poor PRP
Authors Hanisch K , Wedderkopp N
Received 14 September 2018
Accepted for publication 24 January 2019
Published 8 April 2019 Volume 2019:11 Pages 55—60
DOI https://doi.org/10.2147/ORR.S187638
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Klaus Hanisch,1 Niels Wedderkopp1,2
1Orthopedic Department, Hospital of Southwestern Jutland, Esbjerg, Denmark; 2Department of Regional Health Research, University of Southern Denmark, Odense, Denmark
Background: There is a theoretical basis for the treatment of chronic tendinopathies by platelet-rich plasma (PRP), and it can, therefore, be considered a possible treatment of chronic Achilles tendinopathies (CATs), even though the clinical evidence for the use is not clear and, in addition, there is a lack of treatment algorithms and it is unclear which type of PRP is most effective. The objective of this study was through the comparison of two case series to assess: 1) the effect of PRP on CAT and 2) if there is any difference in effect between leukocyte-rich PRP (LR-PRP) and leukocyte-poor PRP (LP-PRP) in the treatment of CAT.
Patients and methods: Two separate series of achilles tenodinopathies treated with either LR-PRP or LP-PRP were evaluated with a natural experiment/quasi-experimental study design, with a short-term (2 months) and long-term (8–42 months) follow-up to assess the effect and stability of the treatment. In total, 84 patients with failed basic treatment for CAT for at least 6 months were treated with either Biomet’s GPS III recovery kit with LR-PRP (36 patients) or with Arthrex ACP LP-PRP (48 patients).
Results: The overall probability of reaching a minimal clinically important change (MCIC) of at least 30% reduction in visual analog scale (VAS) was in activity (63%) and during rest (81%), and for Victorian Institute of Sport Assessment Scale (VISA-A), it was 61%. There was no statistical difference in change of VISA-A score or VAS between the patients treated with LP-PRP and LR-PRP.
Conclusion: PRP seems to be a possible treatment when all other treatment regimens have failed, with a reasonably high probability of reaching MCIC. The choice of either LR-PRP or LP-PRP seems to be up to personal preference as there were no significant differences between patients treated with LR-PRP and LP-PRP.
Keywords: platelet-rich plasma, leukocyte-rich PRP, leukocyte-poor PRP, Achilles tendinopathy
Introduction
Chronic Achilles tendinopathy (CAT) can be difficult to treat. Several treatments have been reported to have a positive effect,1,2 but some cases seem to be resistant to all treatments. In these, platelet-rich plasma (PRP) could be a treatment option.3,4
Glucocorticoid injections are widely used, but there is no clear evidence showing this to be a good treatment and, in addition, there is a risk of serious side effects such as tendon rupture.5 PRP is, in contrast to glucocorticoid, usually extracted from the patient’s own blood and the risk of side effects with this treatment is probably considerably lower compared to glucocorticoid injections. Therefore the use of PRP has increased since Goosen et al reported good results treating tendinopathy of the tendon-insertion of wrist extensors on the lateral humerus epicondyle ten years ago (tennis elbow). There is evidence suggesting an induction of healing through an increase in immunoreactivity for types I and III collagen and promotes differentiation of tendon stem cells into active tenocytes.6–8 Although both leukocyte-rich PRP (LR-PRP) and leukocyte-poor PRP (LP-PRP) have been used and appear to be “safe” in inducing tendon stem/progenitor cells into active tenocytes, LR-PRP could have a detrimental effect on healing of injured tendons due to the induction of a catabolic and inflammatory effect on tendon cells which could prolong the healing process. Consequently, when LR-PRP is used to treat acutely injured tendons, it could result in the formation of excessive scar tissue, as LR-PRP seems to induce an excessive cellular anabolic effect.9,10 In addition, it is commonly accepted that the induction of inflammation by the LR-PRP causes posttreatment pain, for which reason patients are often in need of opioids the first few days after the treatment.
Hence, PRP has a theoretical basis and can, therefore, be considered a possible treatment of CAT, even though the clinical evidence for the use is not clear,11 and in addition, there is a lack of treatment algorithms and it is unclear which type of PRP is most effective.
The objectives of this study were to assess
- the apparent “effect” of PRP on CAT and
- if there is any difference in outcome between LR-PRP and LP-PRP in the treatment of CAT.
Study design
The study is a natural experiment/has a quasi-experimental study design, with a short-term (2 months) and long-term (8–42 months) follow-up to assess the outcome and stability of the treatment.
Patients and methods
From mid-2012 to July 2015, 84 patients who had failed to show progress with the “normal” treatment for CAT for at least 6 months were treated with either Biomet’s GPS III recovery kit (LR-group, 36 patients) or with Arthrex ACP (LP-group, 48 patients).
In the LR-group, 54 mL of patients’ own blood was buffered with 6 mL bicarbonate and centrifuged for 15 minutes at 3,200 U/min. About 5–6 mL of L-PRP was injected with ultrasound control in five different areas of the lesion. According to Biomet, this method results in a thrombocyte concentration that is 9.4 times and a leukocyte concentration that is five times above the basal level.
In the LP-group, 15 mL of blood was drawn in a double syringe, centrifuged for 5 minutes at 1,500 U/min. This produces about 5 mL of plasma, containing thrombocyte concentrations twice above the baseline. The injection technique was the same.
All patients were asked to stop any nonsteroidal anti-inflammatory drug treatment from 1 week before until 2 months after treatment. Paracetamol and morphine were tolerated. Nonweight bearing was prescribed for 2 weeks, but free ankle movement was encouraged.
Pain intensity was assessed using a visual analog scale (VAS) score (0–10) at rest and during activity. We measured CAT severity with the Victorian Institute of Sport Assessment Scale (VISA-A). These self-reported outcomes were completed at baseline and 2 months from the start of treatment. Patients were mailed the above questionnaires to assess the long-term follow-up.
If patients did not return the answers within 2 weeks, a telephone call was made to retrieve the missing information through a structured interview.
Ethics statement
In Denmark, ethical approval is not necessary for patient-reported outcome and questionnaire studies, as per the national guidelines, and the law is as follows: “Notification of questionnaire surveys and medical database research projects to the system of research ethics committee system is only required if the project involves human biological material.”12
Analyses
Continuous data are reported as means with SDs. Categorical data are reported as counts and percentages. The changes in the VAS pain and VISA-A score between treatments (LR- and LP-groups) were compared using 95% CIs; the change was considered significant if there was no overlap between the CIs. We analyzed the outcome in total and individually for both treatments, considering a 30% lowering of pain using the VAS score and a 30% increase in the VISA-A score to indicate a minimal clinically important change (MCIC). The difference between treatments was analyzed to determine if one of the treatments had more patients reaching the MCIC, using logistic regression with robust standard errors (SEs). Moreover, as a sensitivity analysis, we also explored how the application of 10-point increase in VISA-A impacted the proportion of patients achieving clinically important improvements in CAT severity.
Multivariate analyses were performed using multiple linear and logistic regression with robust SE. Multiple linear regression was used to assess the difference in VAS pain and VISA-A scores between treatments as the continuous variable. Multiple logistic regression was applied to assess the difference in probability of reaching an MCIC using the dichotomized variable of whether the patient reached an important clinical effect or not. In all multivariate analyses, sex and age were included as covariates.
Results
The LR-group consisted of 18 females with a median age of 51.9 (SD 11.6) and 18 males with a median age of 50.9 (SD 7.6). Five patients were treated bilaterally. In the LP-group, there were 27 females with a median age of 53.6 (SD 9.5) and 21 males with a median age of 49.7 (SD 11.7). Fifteen patients were treated bilaterally. A total of 104 Achilles tendons were treated with PRP.
In the LR-group, five patients and 5 of 41 tendons did not reach MCIC 8 weeks after treatment. Pain at rest showed a decline in VAS from 4.0 (95% CI =3.0, 5.5) to 1.1 (95% CI =0.5, 1.8), and pain under activity declined VAS from 7.3 (95% CI =6.7, 7.9) to 3.4 (95% CI =2.5, 4.4) and further to 1.8 (95% CI =1.0, 2.6) at the endpoint (median time 36.9 months, IQR 26–46). VISA-A increased from 45.4 (95% CI =28.6, 62.4) to 56.5 (95% CI =30.2, 82.8)
Nineteen were without pain and eight had recurrences. One had a complication (thrombosis), 27 were satisfied, and 26 replied that they would choose PRP treatment again in case of new tendinopathy. Nine received other treatments after PRP and one was operated. Eleven used morphine after the PRP treatment.
In the LP-group, 15 patients and 15 of 63 tendons did not reach MCID 8 weeks after treatment. Pain at rest according to the VAS scale declined from 4.2 (95% CI =4.0, 5.5) to 1.1 (95% CI =0.5, 1.8). Pain under activity declined from 7.8 (95% CI =7.3, 8.2) to 4.8 (95% CI =4.0, 5.6) and further to 3.6 (95% CI =2.3, 4.8) at the endpoint (median time 36.9 months, IQR 26–46). VISA-A increased from 29.7 (95% CI =24.0, 35.4) to 44.7. (95% CI =38.1, 51.2) and two patients reached a VISA-A score above 90.
Twelve were without pain and three had recurrence. No one had a complication, 19 were satisfied, and 11 replied that they would choose PRP treatment again in case of new tendinopathy. Five received other treatments after PRP and eight used morphine.
There was no statistical difference in change of the VAS or VISA-A scores between the patients treated with LP- and LR-PRP. There was a tendency for LR-PRP to have a better outcome, but this did not reach statistical significance (Table 1).
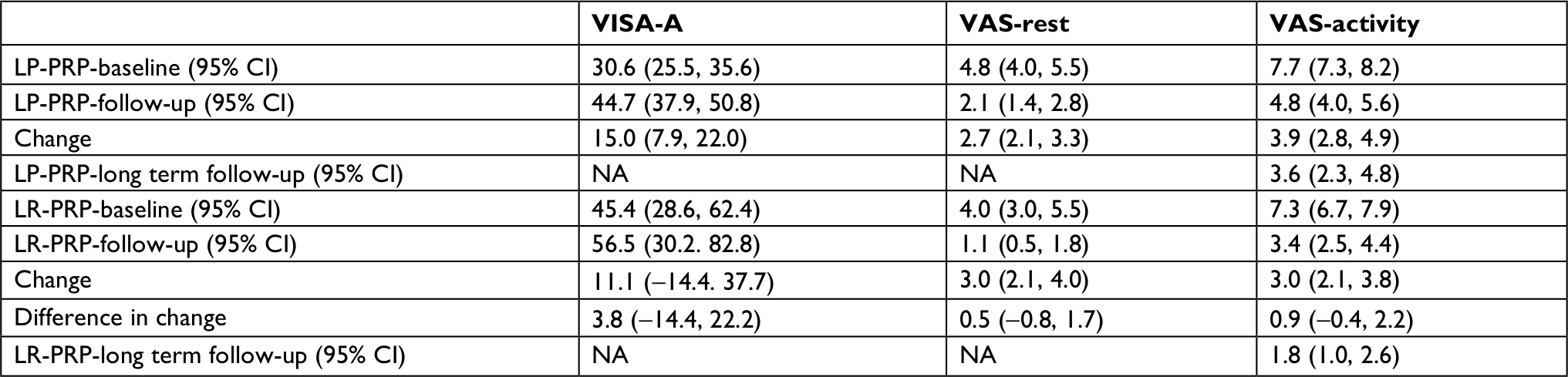 | Table 1 Mean VAS and VISA-A at baseline and follow-up with 95% CI Abbreviations: LP, leukocyte poor; LR, leukocyte rich; NA, not available; PRP, platelet-rich plasma; VAS, visual analog scale; VISA-A, Victorian Institute of Sport Assessment Scale. |
Minimal clinically important change
The overall probability of reaching an MCIC was 63% for VAS in activity (95% CI =54%, 73%) and 81% for VAS during rest (95% CI =73%, 88%). For VISA-A, it was 61% (95% CI =47%, 75%). The sensitivity analysis showed a probability of reaching MCIC of 59% (95% CI =46%, 73%). There was no significant difference in probability of reaching MCIC between the LR- and the LP-groups. The probability of reaching the MCIC for the LR-group was 68% for VAS in activity (95% CI =54%, 83%) and 88% for VAS during rest (95% CI =78%, 98%). For VISA-A, it was 62% (95% CI =28%, 96%). The corresponding results for LP were 60% (95% CI =54%, 83%), 76% (95% CI =66%, 87%), and 61% (95% CI =46%, 76%).
Discussion
We found that PRP may be a promising treatment for CAT when all other treatments have failed. Patients receiving PRP had an 81% probability of achieving an MCIC in pain intensity at rest and 61% probability of achieving an MCIC during activity. Moreover, 63% of patients experienced MCIC in CAT severity. There were no significant differences in pain intensity or CAT severity between patients treated with LR-PRP and LP-PRP. In addition, the sensitivity check showed no significant difference in the proportion of patients reaching the MCIC, but only two patients reached a VISA-A score of >90, which could be recognized as clinical resolution. These results inform future trials evaluating PRP for CAT and assist with effect size and sample size estimation. For example, when using the proportions of patients reaching the MCIC, the sample size calculation for the likelihood ratio test for the number needed to show a statistical difference gave 330 patients for resting pain intensity, 1,146 patients for pain during activity, and 74,336 for the VISA-A score. Thus, it might seem unrealistic to conduct a randomized controlled trial (RCT) when several thousand patients are required in each group to show a significant difference in one of the main outcomes.
We used a relatively conservative estimate for the MCIC as PRP treatment, in our opinion, remains experimental. Therefore, we only included patients with symptom duration greater than 6 months who had failed other therapies such as high-load strength training.13
Although PRP is used widely to treat chronic tendinopathies, it remains unclear which PRP technique is optimal. In particular, the comparative effectiveness of single vs multiple injections and the ideal time intervals between treatment sessions are unknown.
In one pilot study,14 PRP showed promising effects for epicondylitis. This is in line with two randomized clinical trials reporting the benefit of PRP.15,16 Mishra et al16 undertook a recent multicenter RCT on 230 patients with humerus epicondylitis with a follow-up of 3 and 6 months. They reported that 83.9% of patients benefited from PRP, and recommended that PRP should be given prior to surgery. They found PRP to be safe and less expensive than surgery, but the effect was often seen after >3 months. Long-term pain intensity and symptom severity outcomes at 4.5 years among patients with Achilles tendinopathy receiving LP-PRP are promising.17
The addition of exercise therapy to PRP may confer additional benefit. Boesen et al reported better outcomes when PRP was combined with eccentric exercises, compared to eccentric exercise alone.4 This is relevant to the current study results, as all patients underwent a trial eccentric exercise therapy prior to PRP, and we recommend they resume eccentric exercise 14 days after starting PRP treatment.
However, other studies have also found that PRP did not improve healing, pain, or function. Two previous double-blinded randomized clinical trials reported no differences in clinical outcome between LR-PRP and placebo18 or between LR-PRP and saline injections and steroid injections for Achilles tendinopathy.19
Dragoo et al compared LR- vs LP-PRP in an animal model using healthy rabbit patella tendons. They found greater acute inflammatory response 5 days after injection and hypothesized that leucocytes could increase the risk of pain and inflammation.20 However, it is unclear whether this reaction is harmful or beneficial for tendon healing.
Salini et al21 compared the VISA-A results of 29 younger and 15 older patients with Achilles tendinopathy and found PRP to be less effective in older patients. The average age of patients in the current study was 52 (range =34–71) in the LR-group and 49 (range =31–68) in the LP-group. Given such large variability, the role of age on treatment outcome in the current study is unclear. It is possible that important differences in tendinopathy exist between different age groups. For example, from a clinical perspective, it may not be reasonable to assume that tendinopathy in an active 30-year-old runner is similar to tendinopathy experienced by a sedentary 70-year-old patient. The impact of age on tendinopathy outcomes will be an important consideration for future research.
Pain with activity is commonly experienced by patients with chronic tendinopathy. In more severe cases, patients can also experience pain at rest. Consistent with our clinical experience, the current study results found the largest improvement in resting pain intensity at 2 months, while improvements in activity-related pain took longer. Additional injections may have accelerated the pain relief, and future studies should seek to identify optimal PRP dosage.
In the short term, 79% of patients benefited from PRP in the LR-group vs 73% in the LP-group. In the long term, 75% of patients in the LR-group vs 61% in the LP-group were satisfied. The proportion of satisfied patients was lower than the proportion of patients with clinically important change in rest; this suggests that it is the loss of activity due to pain rather than only being pain free in rest that is important for patient satisfaction. This could be interpreted as an advantage for LR-group, but it is not a statistically significant or clinically relevant difference. However, contrary to the above, the LR-group did appear to experience more pain (use of morphine 11 vs 8).
This study was not an RCT to identify the effect of treatment, and the study sample was small. However, we did identify the pain and function outcomes experienced by patients with CAT who underwent two forms of PRP. Further, we used cutoff points for an MCIC, which will inform future studies of PRP. Consequently, our work advances knowledge regarding the treatment of recalcitrant CAT.
Limitations
A limitation of the current study relates to the possibility of systematic error owing to the nonrandom sampling of patients. We recruited patients with recalcitrant Achilles tendinopathy referred to the orthopedic department, and patients were treated by one of two clinicians. Therefore, the external validity of these findings, beyond the study sample, is uncertain. Additionally, there is a risk of recall bias with respect to the outcome measures. Finally, these findings require replication, and the effectiveness of PRP should be further tested with robust clinical trials prior to confident clinical implementation.
Conclusion
We found that a clinically important effect of PRP treatment was achieved in 61%–81% of patients with recalcitrant CAT, depending on outcome. In addition, we compared two different PRP products, an LR-PRP and an LP-PRP, in the treatment of patients with chronic, recalcitrant Achilles tendinopathy. We found no statistically or clinically important differences in pain intensity or CAT severity between LR-PRP and LP-PRP.
Acknowledgments
The authors thank the Professors Charlotte Yde-Lebouef (University of Southern Denmark, Odense, Denmark) and Jeffery Hebert (University of New Brunswick, Fredericton, NB, Canada) for their vocabulary corrections.
Disclosure
The authors report no conflicts of interest in this work.
References
Mani-Babu S, Morrissey D, Waugh C, Screen H, Barton C. The effectiveness of extracorporeal shock wave therapy in lower limb tendinopathy: a systematic review. Am J Sports Med. 2015;43(3):752–761. | ||
Wasielewski NJ, Kotsko KM. Does eccentric exercise reduce pain and improve strength in physically active adults with symptomatic lower extremity tendinosis? A systematic review. J Athl Train. 2007;42(3):409–421. | ||
Andia I, Latorre PM, Gomez MC, Burgos-Alonso N, Abate M, Maffulli N. Platelet-rich plasma in the conservative treatment of painful tendinopathy: a systematic review and meta-analysis of controlled studies. Br Med Bull. 2014;110(1):99–115. | ||
Boesen AP, Hansen R, Boesen MI, Malliaras P, Langberg H. Effect of high-volume injection, platelet-rich plasma, and sham treatment in chronic midportion Achilles tendinopathy: a randomized double-blinded prospective study. Am J Sports Med. 2017;45(9):2034–2043. | ||
Shrier I, Matheson GO, Kohl HW. Achilles tendonitis: are corticosteroid injections useful or harmful? Clin J Sport Med. 1996;6(4):245–250. | ||
Kajikawa Y, Morihara T, Sakamoto H, et al. Platelet-rich plasma enhances the initial mobilization of circulation-derived cells for tendon healing. J Cell Physiol. 2008;215(3):837–845. | ||
Aspenberg P, Virchenko O. Platelet concentrate injection improves Achilles tendon repair in rats. Acta Orthop Scand. 2004;75(1):93–99. | ||
Zhang J, Wang JH. Platelet-rich plasma releasate promotes differentiation of tendon stem cells into active tenocytes. Am J Sports Med. 2010;38(12):2477–2486. | ||
Zhou Y, Zhang J, Wu H, Hogan MV, Wang JH. The differential effects of leukocyte-containing and pure platelet-rich plasma (PRP) on tendon stem/progenitor cells – implications of PRP application for the clinical treatment of tendon injuries. Stem Cell Res Ther. 2015;6(1):173. | ||
Mccarrel TM, Minas T, Fortier LA. Optimization of leukocyte concentration in platelet-rich plasma for the treatment of tendinopathy. J Bone Joint Surg Am. 2012;94(19):e143–148. | ||
Engebretsen L, Steffen K, Alsousou J, et al. IOC consensus paper on the use of platelet-rich plasma in sports medicine. Br J Sports Med. 2010;44(15):1072–1081. | ||
ETHICS TDNCOHR. Act on Research Ethics Review of Health Research Projects. Copenhagen: The Danish National Committee on Health Research Ethics; 2011. | ||
Rathleff MS, Mølgaard CM, Fredberg U, et al. High-load strength training improves outcome in patients with plantar fasciitis: a randomized controlled trial with 12-month follow-up. Scand J Med Sci Sports. 2015;25(3):e292–e300. | ||
Mishra A, Pavelko T. Treatment of chronic elbow tendinosis with buffered platelet-rich plasma. Am J Sports Med. 2006;34(11):1774–1778. | ||
Peerbooms JC, Sluimer J, Bruijn DJ, Gosens T. Positive effect of an autologous platelet concentrate in lateral epicondylitis in a double-blind randomized controlled trial: platelet-rich plasma versus corticosteroid injection with a 1-year follow-up. Am J Sports Med. 2010;38(2):255–262. | ||
Mishra AK, Skrepnik NV, Edwards SG, et al. Efficacy of platelet-rich plasma for chronic tennis elbow: a double-blind, prospective, multicenter, randomized controlled trial of 230 patients. Am J Sports Med. 2014;42(2):463–471. | ||
Filardo G, Kon E, Della Villa S, Vincentelli F, Fornasari PM, Marcacci M. Use of platelet-rich plasma for the treatment of refractory jumper’s knee. Int Orthop. 2010;34(6):909–915. | ||
de Jonge S, de Vos RJ, Weir A, et al. One-year follow-up of platelet-rich plasma treatment in chronic Achilles tendinopathy: a double-blind randomized placebo-controlled trial. Am J Sports Med. 2011;39(8):1623–1629. | ||
Krogh TP, Fredberg U, Stengaard-Pedersen K, Christensen R, Jensen P, Ellingsen T. Treatment of lateral epicondylitis with platelet-rich plasma, glucocorticoid, or saline: a randomized, double-blind, placebo-controlled trial. Am J Sports Med. 2013;41(3):625–635. | ||
Dragoo JL, Braun HJ, Durham JL, et al. Comparison of the acute inflammatory response of two commercial platelet-rich plasma systems in healthy rabbit tendons. Am J Sports Med. 2012;40(6):1274–1281. | ||
Salini V, Vanni D, Pantalone A, Abate M. Platelet rich plasma therapy in non-insertional Achilles tendinopathy: the efficacy is reduced in 60-years old people compared to young and middle-age individuals. Front Aging Neurosci. 2015;7(e37839):228. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.