")
Back to Journals » Vascular Health and Risk Management » Volume 16
Platelet-Derived Microparticles (MPs) and Thrombin Generation Velocity in Deep Vein Thrombosis (DVT): Results of a Case–Control Study
Authors Signorelli SS , Oliveri Conti G , Fiore M, Cangiano F, Zuccarello P, Gaudio A , Ferrante M
Received 27 October 2019
Accepted for publication 15 June 2020
Published 26 November 2020 Volume 2020:16 Pages 489—495
DOI https://doi.org/10.2147/VHRM.S236286
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Harry Struijker-Boudier
Salvatore Santo Signorelli,1 Gea Oliveri Conti,2 Maria Fiore,2 Federica Cangiano,2 Pietro Zuccarello,2 Agostino Gaudio,1 Margherita Ferrante2
1Department of Clinical and Experimental Medicine, University of Catania, Catania, Italy; 2Department of Medical, Surgical Sciences and Advanced Technologies, G.F. Ingrassia, University of Catania, Catania, Italy
Correspondence: Salvatore Santo Signorelli
Department of Clinical and Experimental Medicine, University of Catania, via S.Sofia, Catania I-95123, Italy
Tel +39 0953782545
Fax +39 0953782376
Email [email protected]
Introduction: The role of platelets (Ps) and platelet-derived microparticles (MPs) in venous thromboembolism (VTE) is still being debated.
Methods: We measured MPs, velocity of thrombin formation (PiCT) and phospholipid generation (PLPs) in 40 patients with unprovoked deep vein thrombosis (DVT), who were compared with 40 healthy controls.
Results: MPs were higher in DVT (7.12 nM; 25th– 75th percentile 5.26– 9.12) than in controls (5.45 nM; 25th– 75th percentile 1.67– 8.96) (p = 0.19). PiCT velocity was lower in DVT (1.87 sec; 25th– 75th percentile 1.75– 1.93 sec) compared with controls (1.95 sec; 25th– 75th percentile 1.84– 2.24 sec) (p = 0.04). PLPs were higher in DVT (77.03 μg/mL; 25th– 75th percentile 72.12– 103.59 μg/mL) compared with controls (68.65 μg/mL, 25th– 75th percentile 55.31– 78.20 μg/mL) (p = 0.02).
Discussion: We hypothesize that MPs could be integrated with the lab network assay in evaluating Ps’ role as an activated procoagulative condition. We encourage research on Ps and P-derived microvesicle pathways in patients with unprovoked DVT and not only in patients with cancer-induced DVT.
Keywords: deep vein thrombosis, microparticles, platelet, extracellular vesicles, biomarkers
Plain Language Summary
The intent of the study was to draw attention to platelet-derived microparticles and thrombin generation in deep vein thrombosis because a favourable role for platelets in venous thromboembolism is still being debated. In unprovoked deep vein thrombosis, the authors found a high release of platelet-derived microparticles and raised thrombin generation. These results raise awareness of the role of platelets, platelet-derived microparticles in unprovoked deep vein thrombosis, as well as evaluating the clot-activated conditions leading to thromboembolism in the venous circulation.
Introduction
Deep vein thrombosis (DVT) is a venous thromboembolic disease1 that occurs in patients with favourable conditions (ie, cardiac, cerebral or inflammatory diseases, recent trauma or surgical procedures, etc.). DVT frequently affects patients suffering from cancer, those prescribed anti-cancer drugs or those with central venous catheter implants.2–5 DVT mainly occurs in individuals with genetic or acquired thrombophilia.6 A high level of awareness has been drawn to coagulative cascade factors in DVT, whereas there is little awareness of platelets as agents which induce clotting in DVT patients. The results of clinical trials7,8 have pointed to the efficacy of low doses of acetylsalicylic acid in reducing the risk of venous thromboembolism. However, the efficacy of platelets (Ps) antagonism in venous thromboembolism has not been clearly demonstrated, whereas its role in arterial thrombosis has been demonstrated. Interestingly, platelets are a primary source of microparticles (MPs), which are phospholipid vesicles (0.1–1.0 µm) with procoagulative activity linked to tissue factor (TF) and phospholipids (PLPs).9,10 To investigate the MPs released in the bloodstream and in thrombin generation in patients suffering from DVT of the lower limbs, we performed a case–control study focusing on platelet-derived MPs in 40 patients diagnosed with DVT.
Materials and Methods
Study Subjects (Table 1)
We enrolled forty patients (mean age 57.8 ± 7.2 years old), of which 21 were male (mean age 57.9 ± 6.9 years) and 19 were female (mean age 58.8 ± 7.3 years) affected with unprovoked DVT who had been referred to the Vascular Medicine Laboratory of the Internal Medicine Unit at the “G. Rodolico” University Hospital (Catania, Italy). The patients were matched to a similar number of individuals that attended the vascular laboratory and were not diagnosed with an illness. They were considered as controls. None of the DVT patients had suffered from recent cardiac ischemic events (myocardial infarction, cerebral stroke, bowel ischemia), chronic renal failure, active liver diseases or cancer. None of the DVT patients were smokers at the time of enrolment. Patients were informed of the research, consented to blood sampling and provided verbal consent to the research. Verbal consent was approved by the ethics committee. To diagnose DVT of the lower limbs, patients received a non-invasive ultrasound test (US) using a MyLab Twice instrument (Esaote Ind. Genova, Italy) equipped with a linear probe. The diagnosis of DVT of the lower limb was carried out non-compressing one or more deep lower limb veins by doppler probe (positive CUS test), and/or evidence of echogenic patterns in one or more deep lower limb veins. The present study was previously approved by the Ethics committee Study of the Hospital Garibaldi (Catania, Italy; resolution n.23/2016/CECT2) and was conducted in accordance with the Declaration of Helsinki.
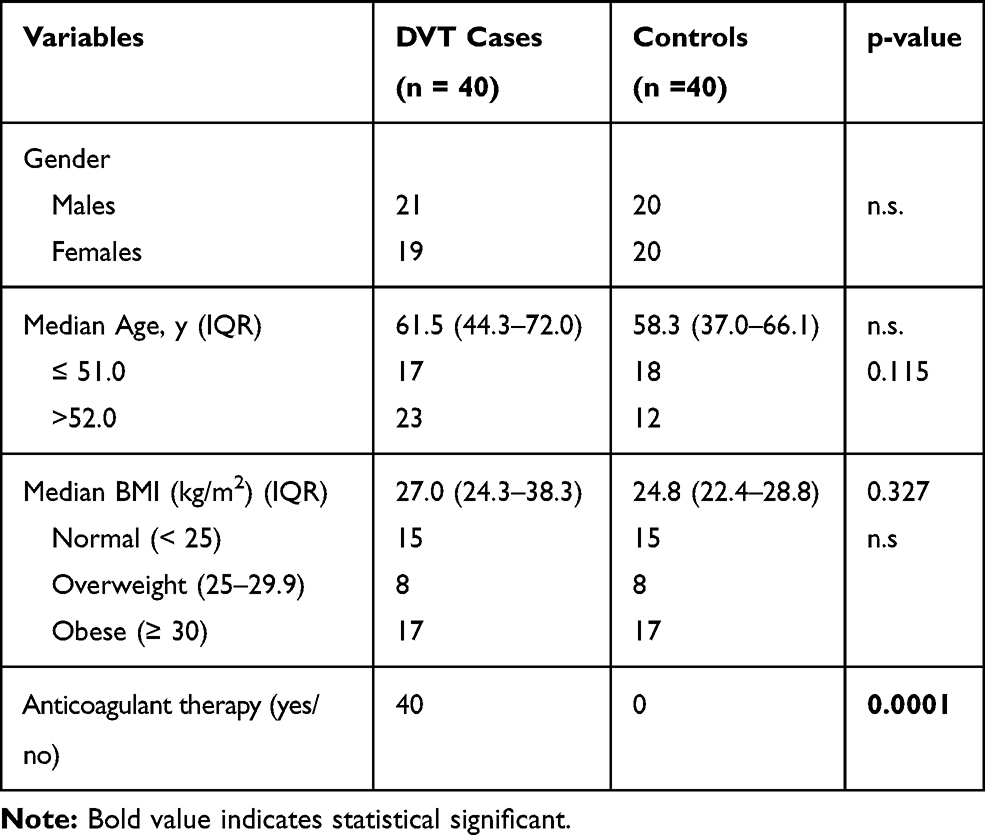 |
Table 1 Characteristics of Controls and DVT Cases |
Microparticle (MP) Detection
The blood samples were drawn quickly and early in the morning. Venous blood samples were drowned in citrate vacuum tubes and treated rapidly by centrifugation (1500 rpm for 15 minutes with an Eppendorf Centrifuge 5417 C/R) to obtain platelet-poor plasma. A second centrifugation step was carried out on plasma (13,400 rpm for 2 minutes). Platelet-free plasma samples were stored at −80 °C to ensure sufficient microparticles, which were then captured by immobilized annexin V. In brief, biotinylated annexin V (annexin VBi; Roche Diagnostics, Mannheim, Germany) was insolubilized onto streptavidin-coated 96-well micro-titration plates (Roche Diagnostics, Mannheim, Germany). After washing the plates three times with TBS–Ca2+ (50 mM Tris buffer, pH 7.5 containing 120 mM NaCl, 2.7 mM KCl, and 1 mM CaCl2), 300 μL aliquots of platelet-free plasma was thawed and thrombin inhibitor, and factor Xa inhibitor (Merck, Darmstadt, Germany) were added. A 100 μL aliquot of platelet-free plasma per well was incubated for 30 min at 37 °C (duplicate wells). After four washing steps, the anionic phospholipid content was determined by a classic prothrombinase assay. The results were reported as nM phosphatidylserine equivalents (nM PS) according to Pigault et al.11
Prothrombinase-Induced Clotting Time Assay (PiCT)
The immobilized MPs were incubated in a final volume of 150 μL with factor Va (250 pM), Xa (9.3 pM), prothrombin (0.7 μM) and CaCl2 (saturated solution) for 15 min at 37 °C (all reagents from Sigma Aldrich, USA). Then, 1.5 mM Chromozym TH (Roche Diagnostics, Mannheim, Germany) was added as a chromogenic substrate for thrombin, and the solution was incubated for another 4 min. The chromogenic substrate was cleaved by thrombin. The colour change was measured photometrically (405 nm) using a micro-titration plate reader (Thermo Fisher Scientific Inc, Canada) equipped with kinetic software. The colour development reaction followed a Michaelis–Menten kinetic and was stopped after 4 min by the addition of EDTA (5 mM, Sigma Aldrich, USA). Velocity was reported in seconds (sec).
Phospholipid Detection (PLPs)
Phospholipids were quantified according to a modified Stewart assay (only 100 µL of platelet-free plasma). The Stewart assay is based on the ability of phospholipids to form a complex with ammonium ferrothiocyanate. Quantities of 13.52 g of ferric chloride hexahydrate and 15.2 g of ammonium thiocyanate (both from Sigma Aldrich) were dissolved in 0.5 L Milli-Q water. The solution is stable at room temperature for several months. A PLP (Sigma Aldrich) calibration standard of 0.1 mg/mL was prepared in chloroform. A six-point calibration curve was performed using chloroform as solvent, bringing the final volume to 2 mL (0–1 mL of PhPs standard in 2 mL of chloroform). Finally, 2 mL of ferrothiocyanate solution was added to all six standards prepared in glass tubes. The tubes were vortexed for 20 seconds and then centrifuged for 5 minutes at 1000 r.p.m., the lower layer then being removed using Pasteur pipettes. Test samples were similarly prepared. The optical density of the standards and samples was read at 485 nm in a Shimadzu Recording Spectrophotometer UV-2401PC. Test-sample concentrations were found by comparing them with the standard curve.
Statistical Analysis
Descriptive statistics used medians (IQR) for quantitative variables, and frequencies and percentages for categorical variables. Distribution differences were calculated using the Mann–Whitney U-test for continuous variables and the Chi-Square Test or Fisher’s Exact Test, depending on the number of subjects in each subgroup of categorical variables. The level of significance was p ≤ 0.05. All the calculations were performed using the Statistical Package for Social Sciences (SPSS), version 21.0 for Windows (SPSS Inc., Chicago, IL, USA).
Results
P-Derived Microparticle (MPs) Levels
The median value (interquartile 25th–75th percentile) of the MPs was 7.12 (5.26–9.12) phosphatidyl-serine equivalent (nM) in DVT patients, and in controls, it was 5.45 (1.67–8.96) phosphatidyl-serine equivalent. The difference between the medians was not significant (p = 0.19) (Figure 1).
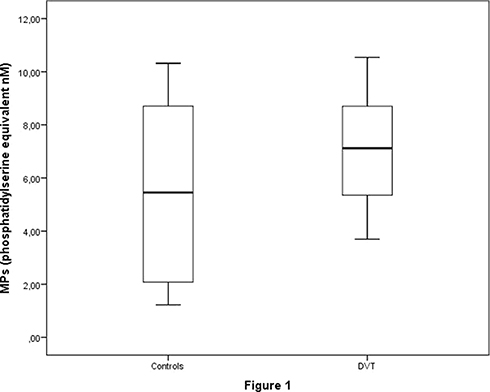 |
Figure 1 Box-plot showing the distribution of microparticle (MP) quantification by controls and DVT cases. |
Prothrombinase-Induced Clotting Time Assay (PiCT) Velocity
The median value (interquartile 25th–75th percentile) of the PiCT was 1.87 sec (1.75–1.93) in DVT patients and 1.95 sec (1.84–2.24) in controls (Figure 2). This difference was statistically significant (p = 0.04).
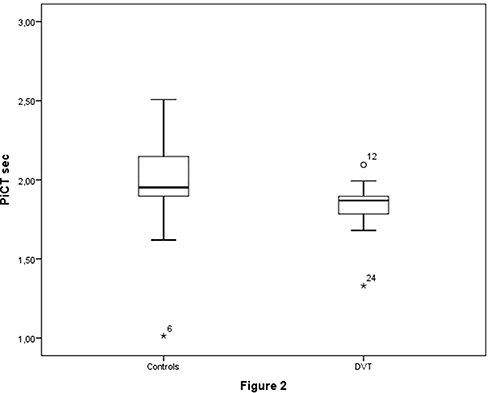 |
Figure 2 Box-plot showing the distribution of prothrombinase-induced clotting time assay (PiCT) velocity by controls and DVT cases. The asterisks are outliers, and the dots are extreme values. The numbers identify the sample to which the asterisk or dot refers. |
Phospholipids (PLPs)
The median value (interquartile 25th–75th percentile) of PLPs was 77.03 µg/mL (72.12–103.59) in DVT patients and 68.65 µg/mL (55.31–78.20) in controls (Figure 3). This difference was statistically significant (p = 0.02).
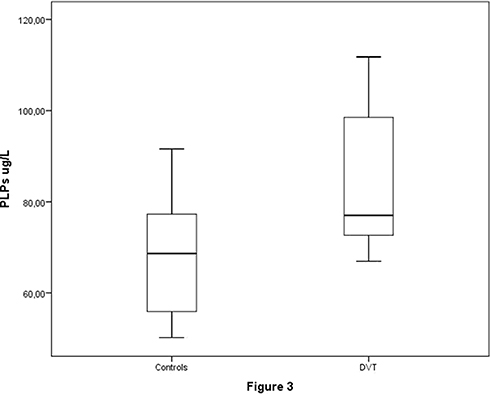 |
Figure 3 Box-plot showing the distribution of phospholipid (PLP) quantification by controls and DVT cases. |
Discussion
Procoagulative disorders play a key role in venous thromboembolic diseases such as DVT, even when they occur as asymptomatic or poorly symptomatic. However, there is a close tie-in between DVT and pulmonary embolism,1,6 for which it is widely accepted that combined coagulative markers (ie, D-dimer) and ultrasound examination (ie, ultrasound) have improved the diagnosis of DVT. From the abundant evidence on the role of coagulative factors and disorders in provoking DVT, the latest anticoagulant drugs are the first line of treatment for DVT.12–15 All these drugs focus on inhibiting the activation of components in the coagulative cascade to counteract prothrombotic event drama in the venous circulation. The role of Ps as active cells in venous thromboembolism has been less contested or almost unknown, whereas the role of Ps aggregation is considered as crucial both in starting and in determining arterial thrombosis. Study results and meta-analyses have commented on the effectiveness of acetylsalicylic acid in reducing VTE recurrence.7,8 These studies compared acetylsalicylic acid favourably to dicumarolics in the secondary prevention of venous thromboembolisms including lower limb DVT. However, to date, there has not been any consensus on the efficacy of platelet antagonism in treating or reducing VTE.15 Microparticles favour clots by increasing the assembly of procoagulative factors, which gives them high procoagulant capability. It is known that the surfaces of microparticles have both clot proteins and phosphatidylserine. In turn, the presence of gamma-carboxyglutamic acid in clot proteins greatly increases the activated complex of procoagulative factors such as activated factors VIII/IX and V/X.16 Additionally, it is known that microparticles release tissue factor (TF), a transmembrane glycoprotein, and it is a potent initiator of procoagulant activity in vitro. TF increases procoagulant activity dramatically, and it has been demonstrated in different diseases showing a high frequency or risk for thromboembolic events. Platelet-derived microparticles are closely linked to activated coagulative factor complexes; therefore, these particles play a key role in thrombin generation.17,18
Our study shows that MPs plasma levels and thrombin generation increase in DVT patients compared with controls. To explain these results, it is necessary to consider the close relationship between pro-inflammatory mediators like lipopolysaccharides,19 the complementary activation of platelet-leukocyte complexes and cytokines,20 and soluble CD40 ligands on platelet stimulation.21 We know that soluble CD40 ligands induce thrombin-receptor activating peptides.22 It is accepted that platelets carry, transfer and internalize tissue factor (TF), leading to the TF-rich P-derived microparticles.22,23 MPs increase the velocity of thrombin generation and promote clot propagation following TF.24 Furthermore, MPs are also rich in anionic PLPs and are capable of supporting and stimulating coagulation. The adhering platelets degranulate and release several components, including calcium ions, which bind to phospholipids and provide a surface for various coagulation factors to assemble.25 In normal haemostasis, free-ionized calcium needs to start platelet plug formation, but it also facilitates several steps in the coagulative cascade. Calcium also mediates the binding of prothrombin complexes through terminal gamma-carboxy residues to the PLP surfaces expressed by activated platelets, as well as acting on the procoagulant MPs shed from them (this particular role of calcium ions also acts on the PLP of MPs shed from them). It is noteworthy that we decided to modify the PiCT assay methodology to reveal the possible differences in thrombin generation and in its velocity of generation in the two groups of samples. We want to draw attention to the role of Ca2+ by using a saturated Ca2+ solution for a modified prothrombinase test on blood samples from both groups. The test showed a greater velocity of thrombin generation in DVT patients. We know that annexin is one essential protein for activating factors V and VII of the coagulative cascade as well as Ca2+ regulation of phospholipid-binding proteins.25,26 Our laboratory methodology for assaying PiCT included equal Ca2+ saturation in blood samples drawn from DVT patients and from controls. The PiCT results were independent of thrombin-mediated FV activation.
It should be noted that the activation of coagulation by the whole prothrombinase complex containing pre-activated factor V is between 30,000 and 300,000 times faster than that by FXa alone and 1000 times faster than the activation stimulated by FXa together with calcium ions and phospholipids. Our modified PiCT test with saturated Ca2+ solution increased prothrombin activation velocity, improved test reproducibility and linearity and reduced result variability. Therefore, this methodology may obtain more accessible and reproducible results as suggested by other authors.24–27 The P-derived MPs add a procoagulative surface to the P-derived phospholipids by an enzymatic catalytic process, actively promoting procoagulative imbalance, thus improving thrombin generation and binding fibrinogen and, finally, increasing Ps aggregation. It is also interesting to note that MPs promote the release of TF, which is the most active clotting factor in venous thrombosis. It should also be noted that the PiCT assay is a sensitive, specific laboratory test in measuring both the activation of thrombin-dependent and anti-thrombin-independent FXa inhibition.
To discuss P and MPs in venous thromboembolism, we would like to cite our findings on oxidative stress in DVT. We have demonstrated that oxidative stress occurs in DVT patients from the high plasma levels of oxidative stress surrogate biomarkers (malondialdehyde, thiobarbituric acid-reactivity, 4-hydroxynonenal assay) in DVT patients.28 Note that oxidative stress is closely related to the generation of platelet agonist agents (ie, thromboxane), which promote platelet activation, leading to conditions that favour thrombosis. Malondialdehyde-lipid adducts have the ability to activate coagulation.29 Among the pathophysiological roles that both P and MPs may play in venous thrombotic diseases, we should note that the two mentioned above are closely linked to TF, which is crucial in promoting VTE events both in cancer patients and in those showing no prothrombotic conditions.3–9 Mixed research results were found for MPs in patients suffering from venous thrombotic events (eg, lower limb DVT). Chrinos et al did not find high levels of microparticles in acute VTE patients, and no association was found between P microparticles and VTE.29 Chirinos and Thaler found that elevated plasma levels of MPs were also associated with TF in unprovoked DVT patients compared with non-DVTs.29–31 In contrast, in patients with antiphospholipid syndrome, P microparticles were considered key to a pathophysiological mechanism, and these particles were also cited as able to cause thrombotic complications in those types of patients.32 Based on our results, we could conclude that in non-cancer DVT patients there is a P-mediated procoagulative condition. In DVT patients compared with controls, there were higher plasma levels of P-derived microparticles by PiCT assay and finally by increased levels of PLPs, which agrees with Pabineger.33 So, MPs cannot be used as a single indicator in the laboratory of the possible risk of VTE. Rather, we would like to suggest considering a network of laboratory markers including MPs, modified PiCT assays and PLPs to elicit the role played by Ps and to screen for activated prothrombotic conditions favourable to DVT. We would like to draw attention to the fact that the enrolled patients were affected by unprovoked lower limb DVT. None of the enrolled patients was affected by cancer. We know that P and derived micro-vesicles are key players in venous thromboembolism associated cancer.34–36 In conclusion, the results of this study could increase awareness of Ps in the pathophysiology of venous thromboembolism as well as in DVT patients.
Our study has limitations. Firstly, the number of enrolled patients with lower limb DVT was limited. The present paper shows the results of an observational monocentre institutional study enrolling patients affected from DVT of the lower limbs. We are aware of the low incidence of DVT; it ranges from 20 to 24 cases young individuals to 80–84 in older adults per 10,000 per year.37 Based on the abovementioned epidemiological data, it is therefore understandably difficult for a single clinical centre to enrol a large number of cases of patients that suffer from DVT of the lower limbs alone. Furthermore, the present study was planned to evaluate the plasma levels of platelet-derived microparticles in patients suffering from unprovoked DVT of the lower limbs who did not have cancer. Our study was planned to enrol cancer-free patients diagnosed for DVT of lower limbs, since cancer represents both a dramatic risk factor for venous thromboembolic events, including DVT of the lower limbs, and also because cancer per se seriously alters haemostatic balance. Additionally, cancer causes high release of TF, which is closely linked to elevated production of platelet-derived microparticles. Therefore, we planned a case–control study to help achieve the study objectives. The strengths of the study are that we measured MPs, PiCTs and PLPs from patients suffering from unprovoked DVT of the lower limbs but none from patients having cancer as the most favourable prothrombotic condition. In conclusion, we would like to promote more awareness of platelets and their derived microparticles as important components in venous, as well as arterial, thrombogenesis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest.
References
1. Writing Group M, Mozaffarian D, Benjamin EJ, et al. Heart disease and stroke statistics-2016 update: a report from the American Heart Association. Circulation. 2016;133:e38–e360.
2. Mahajan A, Brunson A, White R, et al. The epidemiology of cancer-associated venous thromboembolism: an update. Semin Thromb Hemost. 2019;45(4):321–325. doi:10.1055/s-0039-1688494
3. Jara-Palomares L, van Es N, Praena-Fernandez JM, et al. Relationship between type of unprovoked venous thromboembolism and cancer location: an individual patient data meta-analysis. Thromb Res. 2019;176:79–84. doi:10.1016/j.thromres.2019.02.011
4. Figueroa A, Alfonso A, Lopez-Picazo J, et al. Insights into venous thromboembolism prevention in hospitalized cancer patients: lessons from a prospective study. PLoS One. 2018;13(8):e0200220. doi:10.1371/journal.pone.0200220
5. Di Nisio M, Candeloro M, Rutjes AWS, et al. Venous thromboembolism in cancer patients receiving neoadjuvant chemotherapy: a systematic review and meta-analysis. J Thromb Haemost. 2018;16(7):1336–1346. doi:10.1111/jth.14149
6. Simioni P, Tormene D, Spiezia L, et al. Inherited thrombophilia and venous thromboembolism. Semin Thromb Hemost. 2006;32:700. doi:10.1055/s-2006-951298
7. Campello E, Spiezia L, Radu CM, et al. Endothelial, platelet, and tissue factor-bearing microparticles in cancer patients with and without thromboembolism. Thromb Res. 2011;127:437. doi:10.1016/j.thromres.2011.01.002
8. Beccattini C, Agnelli G, Schenone A, et al. WARFASA Investigators. Aspirin for preventing the recurrence of venous thromboembolism. N Engl J Med. 2012;366:1959. doi:10.1056/NEJMoa1114238
9. Brighton TA, Eikelboom JW, Mann K, et al. The ASPIRE investigators. Low-dose aspirin for preventing recurrent venous thromboembolism. N Engl J Med. 2012;367:1979–1987. doi:10.1056/NEJMoa1210384
10. Rautou P, Mackman N. Microvesicles as risk markers for venous thrombosis. Expert Rev Hematol. 2013;6(1):91–101. doi:10.1586/ehm.12.74
11. Pigault C, Folleniuswund A, Schmutz M, et al. Formation of two-dimensional arrays of annexin V on phosphatidylserine-containing liposomes. J Mol Biol. 1994;236:199. doi:10.1006/jmbi.1994.1129
12. Fricke A, Ullrich P, Cimniak AFV, et al. Levels of activated platelet-derived microvesicles in patients with soft tissue sarcoma correlate with an increased risk of venous thromboembolism. BMC Cancer. 2017;17:527. doi:10.1186/s12885-017-3515-y
13. Stewart JC. Colorimetric determination of phospholipids with ammonium ferrothiocyanate. Anal Biochem. 1980;104I:10. doi:10.1016/0003-2697(80)90269-9
14. Kearon C, Akl EA, Ornelas J, et al. Antithrombotic therapy for VTE disease. Chest. 2016;149(2):315–352. doi:10.1016/j.chest.2015.11.026
15. Castellucci LA, Cameron C, Le Gal G, et al. Efficacy and safety outcomes of oral anticoagulants and antiplatelet drugs in the secondary prevention of venous thromboembolism: systematic review and network meta-analysis. BMJ. 2013;347:f5133. doi:10.1136/bmj.f5133
16. Morel O, Toti F, Hugel B. Procoagulant microparticles: disrupting the vascular equation? Arterioscler Thromb Vasc Biol. 2006;26(12):2594–2604. doi:10.1161/01.ATV.0000246775.14471.26
17. Ståhl AL, Sartz L, Karpman D. Complement activation on platelet-leukocyte complexes and microparticles in enterohaemorrhagic Escherichia coli-induced haemolytic uremic syndrome. Blood. 2011;117(20):5503–5513. doi:10.1182/blood-2010-09-309161
18. Nomura S, Nakamura T, Cone J, et al. Cytometric analysis of high shear-induced platelet microparticles and effect of cytokines on microparticle generation. Cytometry. 2000;40(3):173–181. doi:10.1002/1097-0320(20000701)40:3<173::AID-CYTO1>3.0.CO;2-L
19. Prasad KS, Andre P, He M, et al. Soluble CD40 ligand induces beta3 integrin tyrosine phosphorylation and triggers platelet activation by outside-in signalling. Proc Natl Acad Sci U S A. 2003;100(21):12367–12371.
20. Tschuor C, Asmis LM, Lenzlinger PM, et al. In vitro norepinephrine significantly activates isolated platelets from healthy volunteers and critically ill patients following severe traumatic brain injury. Crit Care. 2008;12(3):R80. doi:10.1186/cc6931
21. Camera M, Brambilla M, Toschi V, et al. Tissue factor expression on platelets is a dynamic event. Blood. 2010;116:5076–5077. doi:10.1182/blood-2010-09-307306
22. Escolar G, Lopez-Vilchez I, Diaz-Ricart M, et al. Internalization of tissue factor by platelets. Thromb Res. 2008;122(Suppl. 1):S37–S41. doi:10.1016/S0049-3848(08)70017-3
23. Lopez-Vilchez I, Escolar G, Diaz-Ricart M, et al. Tissue factor-enriched vesicles are taken up by platelets and induce platelet aggregation in the presence of factor VIIa. Thromb Haemost. 2007;97(2):202–211. doi:10.1160/TH06-04-0216
24. Lim W, Le Gal G, Bates SM, et al. American Society of Haematology 2018 guidelines for management of venous thromboembolism: diagnosis of venous thromboembolism. Blood Adv. 2018;2:3226–3325.
25. Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur Respir J. 2019;54(3):1901647.
26. Collaborative overview of randomized trials of antiplatelet therapy-III: reduction in venous thrombosis and pulmonary embolism by antiplatelet prophylaxis among surgical and medical patients. Antiplatelet Trialists’ Collaboration. BMJ. 1994;308:235. doi:10.1136/bmj.308.6923.235
27. Korte W, Jovic R, Hollenstein M, et al. The uncalibrated prothrombinase-induced clotting time test. Equally convenient but more precise than the aPTT for monitoring of unfractionated heparin. Hamostaseologie. 2010;30:212. doi:10.1055/s-0037-1619058
28. Ferrante M, Fiore M, Oliveri Conti G, et al. Transition and heavy metals compared to oxidative parameter balance in patients with deep vein thrombosis: a case-control study. Mol Med Rep. 2017;15:3438. doi:10.3892/mmr.2017.6394
29. Balasubramanian K, Bevers EM, Willems GM, et al. Binding of Annexin V to membrane products of lipid peroxidation. Biochemistry. 2001;40:8672. doi:10.1021/bi010841y
30. Chirinos JA, Heresi GA, Velasquez H, et al. Elevation of endothelial microparticles, platelets, and leukocyte activation in patients with venous thromboembolism. J Am Coll Cardiol. 2005;45:1467. doi:10.1016/j.jacc.2004.12.075
31. Thaler J, Koppensteiner R, Pabinger I, et al. Microparticle-associated tissue factor activity in patients with acute unprovoked deep vein thrombosis and during the course of one year. Thromb Res. 2014;134:1093. doi:10.1016/j.thromres.2014.07.041
32. Dignat GF, Camoin JL, Sabatier F, et al. Endothelial microparticles: a potential contribution to the thrombotic complications of antiphospholipid syndrome. Thromb Haemost. 2004;91:667.
33. Pabinger I, Thaler J, Ay C. Biomarkers for prediction of venous thromboembolism in cancer. Blood. 2013;122:2011. doi:10.1182/blood-2013-04-460147
34. Mege D, Aubert M, Lacroix R, et al. Involvement of platelets in cancers. Semin Thromb Hemost. 2019;45(6):569–575. doi:10.1055/s-0039-1693475
35. Mahajan A, Wun T. Biomarkers of cancer-associated thromboembolism. Cancer Treat Res. 2019;179:69–85.
36. Falanga A, Schieppati F, Russo L. Pathophysiology 1. Mechanisms of thrombosis in cancer patients. Cancer Treat Res. 2019;179:11–36.
37. Cushman M. Epidemiology and risk factors for venous thrombosis. Semin Hematol. 2007;44(2):62–69. doi:10.1053/j.seminhematol.2007.02.004
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.