")
Back to Journals » Journal of Inflammation Research » Volume 14
Plasma Neutrophil-to-Lymphocyte Ratio on the Third Day Postburn is Associated with 90-Day Mortality Among Patients with Burns Over 30% of Total Body Surface Area in Two Chinese Burns Centers
Authors Qiu L, Jin X, Wang JJ, Tang XD, Fang X, Li SJ, Wang F, Chen XL
Received 28 November 2020
Accepted for publication 3 February 2021
Published 24 February 2021 Volume 2021:14 Pages 519—526
DOI https://doi.org/10.2147/JIR.S294543
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Le Qiu,* Xu Jin,* Jun-Jie Wang,* Xu-Dong Tang,* Xiao Fang, Shi-Ji Li, Fei Wang, Xu-Lin Chen
Department of Burns, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xu-Lin Chen
Department of Burns, The First Affiliated Hospital of Anhui Medical University, 120 Wanshui Road, Hefei, Anhui, 230088, People’s Republic of China
Tel +86-551-65908495 Email [email protected]
Introduction: Neutrophil-to-lymphocyte ratio (NLR) is a marker of inflammation. This study aimed to evaluate the potential role of NLR to predict 90-day mortality.
Methods: Data of 577 patients with burns over 30% of total body surface area were collected and retrospectively analyzed. The risk factors for 90-day mortality were evaluated using logistic regression analyses. Receiver operating characteristic (ROC) curve analysis of the 3rd day NLR was performed and the optimal cut-off value was calculated. The 90-day mortality rates were compared between high and low NLR groups using Kaplan-Meier analysis.
Results: Age, mechanical ventilation, burn index, 3rd day NLR, and 7th day red blood cell and platelet (PLT) counts were found to be independent predictive values for 90-day mortality. In contrast, percentage of total body surface area burned, inhalation injury, 1st day white blood cell and neutrophil counts, the 3rd day lymphocytes and PLT counts, and 7th day hemoglobin level were not independently associated with 90-day mortality. The area under the ROC curve of the 3rd day NLR for severe burn–delayed death prediction was 0.665 (95% confidence interval, 0.591– 0.739), and the optimal cut-off value of the 3rd day NLR was 10.50. The 90-day mortality rates differed significantly between the NLR > 10.5 group and the NLR ≤ 10.5 group (17.03% vs 5.92%, respectively; P < 0.01).
Conclusion: These results suggested that the 3rd day NLR was associated with an increased risk of death in severely burned patients; thus, it can provide useful information to predict 90-day mortality.
Keywords: burns, neutrophil-to-lymphocyte ratio, 90-day mortality
Introduction
According to the World Health Organization, burns remains a serious global health problem, with over 195,000 burn-related deaths each year.1 Shock and cardiogenic injury can follow burn injury, resulting in death in the first week (“early death”).2 However, subsequent infections are a significant cause of late mortality associated with burn injury.3 Infections and their complications, such as sepsis, septic shock, and multiple organ dysfunction syndrome (MODS), play an important role in the late mortality of burn patients.4
The neutrophil-to-lymphocyte ratio (NLR) is calculated from the absolute neutrophil and lymphocyte counts, which are easily obtained from laboratory test data. NLR was found to be a simple and inexpensive marker of infection in clinical application.5 Numerous studies have documented NLR as an independent risk factor for several serious diseases, such as sepsis, cardiovascular disease and malignancies; NLR can also reflect changes in the systemic inflammatory response.6–9 Inflammation is a common early pathophysiologic characteristic for severe burn injured patients, including shock, and is frequently followed by sepsis and MODS.10,11 Nonetheless, the association between NLR and 90-day mortality in severe burn injuries has not been studied.
Therefore, we collected and retrospectively analyzed the data of patients with burns who were admitted to the First Affiliated Hospital of Anhui Medical University and Ruijin Hospital of Shanghai Jiao Tong University to investigate the predictive value of NLR for the mortality of burn patients.
Methods
Patients
This retrospective study included patients with severe burn injuries who were admitted to the First Affiliated Hospital of Anhui Medical University and Rui Jin Hospital of Shanghai Jiao Tong University between January 2008 and December 2015. All patients provided informed consent for the use of their data in research, and that this study was conducted in accordance with the Declaration of Helsinki. All procedures were approved by the Human Subjects Review Board of Anhui Medical University Hospital, Hefei, China. Patients with shock at admission were resuscitated with the Chinese formula that was adjusted according to the physiological response.12,13
The inclusion criteria were burn injury (including flame, scalding, electric, contact, or spark burn) patients aged ≥18 years, percentage of the total body surface area (%TBSA) ≥30%, and survival time ≥7 days. The exclusion criteria were age<18 years and known pre-existing cardiac disease, kidney disease, hemolytic anemia, bone marrow arrest, or other inflammatory diseases.
The China formula is as follows: 1.5 mL/kg/%TBSA + 5% dextrose solution 2000 mL, and 1.5 mL/kg/%TBSA = lactate Ringer’s solution 1.0 mL/kg/%TBSA + fresh-frozen plasma 0.5 mL/kg/% TBSA.12,13 Half of this volume was administered in the first 8 h, and the remaining half was administered during the next 16 h. Meanwhile, the rehydration is dynamically adjusted according to the blood pressure, central venous pressure and urine output.
A series of pathophysiological changes occur in a body after severe burn. Past studies have described early-stage postburn to range from 48 h to within 21 days of the burn.14–17 Early excision and autograft within one week are now considered standards of care in the treatment of severely burned patients.18 In this study, early stage was referred to 7 days postburn and late stage was referred to 7 days later. This definition is consistent with many previous studies.19–21
Data Collection
Each patient’s demographic, clinical, and laboratory data were obtained from the electronic medical records. The burn departments in Anhui Medical University Hospital and Ruijin Hospital are two major burn centers in east China. In these two centers, the laboratory examination was conducted at least every other day during the first week postburn for the major burn patients with burned area over 30% TBSA. Blood samples were analyzed by fully auto hemocyte analyzer in two different laboratories of the burn centers with the same national standards.
The primary outcome was 90-day mortality collected from the hospital medical records and telephone follow-up. All eligible patients were grouped as follows: (a) survivor group, which included patients who survived 90 days after severe burn injury; and (b) non-survivor group, which included patients who died between day 7 and day 90.
Statistical Analysis
Statistical analyses were performed using SPSS 22.0 (SPSS Inc., Chicago, IL, USA), and values of P < 0.05 were considered statistically significant. Continuous variables are described as mean ± SD, and categorical indicators were presented as frequency (%). Intergroup comparisons were performed using Student’s t-test or Pearson’s χ2 test.
Normal analysis was performed on these 577 patients by using histograms and descriptive statistics and the results showed that the data were close to normal distribution. It was reasonable to use t-test for continuous variables when the samples are sufficiently large.
Logistic proportional hazard regression was performed to examine the association between NLR and 90-day mortality, and 95% confidence intervals (CIs) were generated. The 3rd day NLR was used as a variable in the receiver operating characteristic (ROC) curve analysis to estimate the sensitivity, specificity, and areas under the ROC curves. The optimal cut-off value was obtained from the maximum value of Youden’s index (sensitivity + specificity - 1). The survival curves of the high and low NLR groups were calculated using the Kaplan–Meier method.
Results
Demographic and Clinical Data
There were 652 adult patients who sustained severe burns according to Chinese burn severity criteria (%TBSA burned ≥30%, or %TBSA of full-thickness burn ≥10%, or complicated with shock, moderate or severe inhalation injury, or combined injury)22 and admitted in these two centers during 2008–2015. Because 32 had a %TBSA < 30%, 8 patients’ hospital stays were less than 48h, 33 patients survived less than 7 days post-burn, and 2 patients’ data were incomplete, the data of 577 severe burn patients were ultimately analyzed.
The clinical data of patients included patients’ demographic data, inhalation injury, mechanical ventilation, surgery during the first week, %TBSA burned and burn index. The laboratory data were only collected from the results of blood routine test and the biochemical data were not retrieved in this study. The blood routine test included white blood cell count, Neutrophils, Lymphocytes, red blood cell count, platelet count, Eosinophil count, Basophil count, Monocyte count and so on. White blood cell count, Neutrophils, Lymphocytes, red blood cell count, and platelet count were analyzed. Eosinophil count, Basophil count, and Monocyte count were missed due to non-significant changes in the early postburn period.
Table 1 shows that 55 patients died during the late postburn period, with a mortality rate of 9.53%, a mean %TBSA of 67.49%, and a mean survival time of 17.95 days, while 522 patients survived the 90-day follow-up period. Age, inhalation injury, mechanical ventilation, %TBSA burned, and burn index (BI) were significantly higher in the non-survivor group (P < 0.05). The burn index (BI) was referred to formula BI=%TBSA of third-degree burns+½ %TBSA of second-degree burns.23 There were no significant differences in sex or need for surgery during the first week between the survivors and non-survivors.
 |
Table 1 Baseline Characteristics Comparing Severe Burn Survivors and Non-Survivors |
Significant differences were observed between severe burn injury survivors and non-survivors in the 1st day data (white blood cell and neutrophil counts), the 3rd day data (lymphocytes, NLR, platelets [PLT]), and the 7th day data (red blood cell and PLT counts, hemoglobin level) (P < 0.05; Table 2).
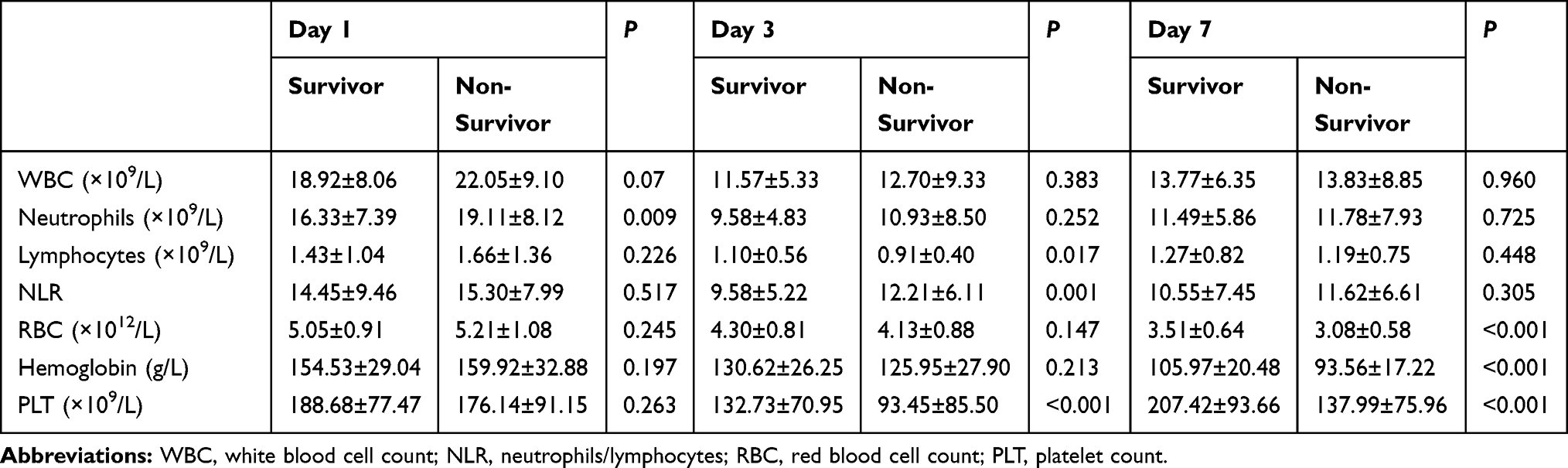 |
Table 2 Laboratory Parameters Comparing Severe Burn Survivors and Non-Survivors |
ROC Curves of Variables and 90-Day Mortality
The 3rd day NLR was used as a variable in the receiver operating characteristic (ROC) curve analysis to estimate the sensitivity, specificity, and areas under the ROC curves. The optimal cut-off value was obtained from the maximum value of Youden’s index (sensitivity + specificity - 1). As shown in Figure 1, the areas under the ROC curves of the 3rd day NLR for severe burn–delayed death prediction were 0.665 (95% CI, 0.591–0.739), and the optimal cut-off value of the 3rd day NLR was 10.50 (60.00% sensitivity,70.10% specificity). The 3rd day NLR was converted from a continuous variable to a categorical variable for the NLR >10.50 group and the NLR≤10.50 group according to the optimal cut-off value.
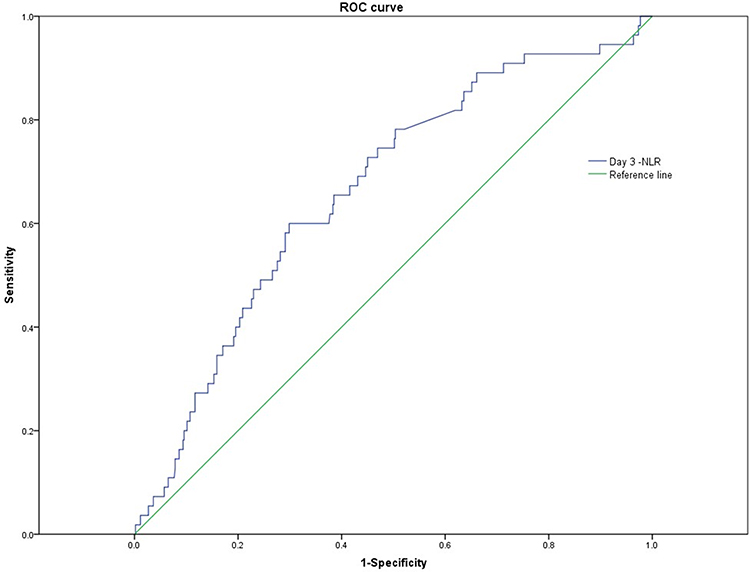 |
Figure 1 Receiver operating characteristic (ROC) curve analysis of preoperative neutrophil-to-lymphocyte ratio for the 90-day mortality in severely burned patients. |
Survival Analysis for Predicting 90-Day Mortality
All variables mentioned above were gathered into the Logistic regression analysis. Age, mechanical ventilation, BI, 3rd day NLR, and 7th day red blood cell and PLT counts provided independent predictive values for 90-day mortality. However, %TBSA burned, inhalation injury, 1st day white blood cell and neutrophil counts, 3rd day lymphocytes and PLT, and 7th day hemoglobin levels were not independently associated with 90-day mortality (Table 3).
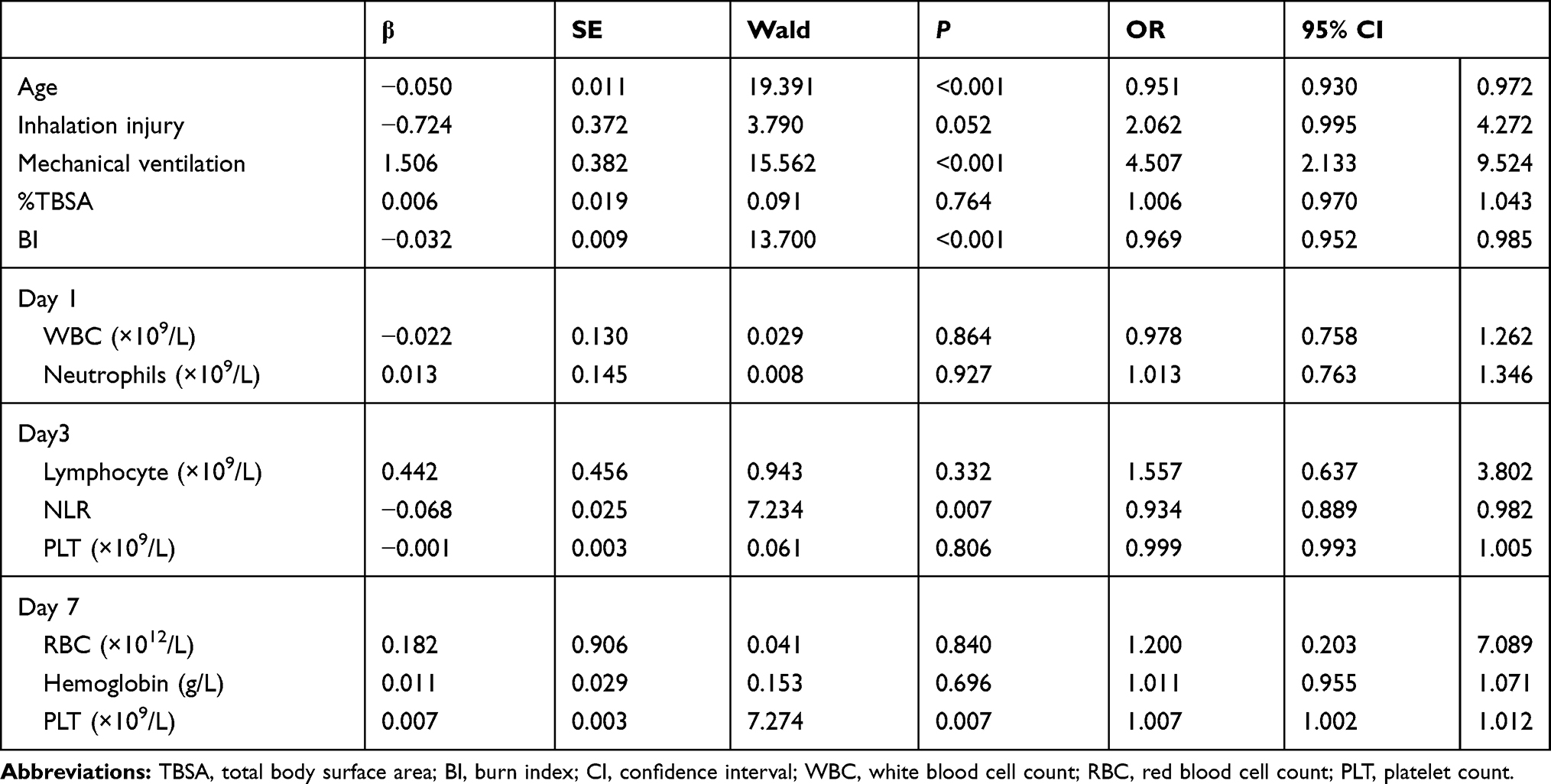 |
Table 3 Logistic Regression for the Later Postburn Period Mortality |
There was a significant difference in 90-day mortality between high and low NLR groups, with a 90-day overall survival rate of 82.97% for patients with severe burn injury and NLR > 10.50 versus 94.08% for patients with an NLR ≤ 10.50 (P = 0.003; Figure 2). The 90-day mortality rates differed significantly between the NLR >10.5 group and the NLR ≤ 10.5 group (17.03% vs 5.92%, respectively; P < 0.01).
 |
Figure 2 Kaplan–Meier curve of 90-day survival of severe burn injuries. The blue line indicates patients’ survival in the 3rd NLR ≤ 10.50 group. The green line indicates patient’ survival in the 3rd NLR >10.50 group. |
Discussion
Cardiac, lung, and renal dysfunction, followed by the overrelease of toxins and inflammatory mediators into the blood circulation and distributive shock, are the main causes of fatality in the early period of severe burn injury.24,25 However, the mortality rate is significantly reduced in the early period, which is attributed to the timely and effective progress in the treatment of burn injuries.26–28 The mortality rate among severely injured patients remains high in the late postburn period, in which the main causes of fatality are generalized infection, sepsis, and MODS.10,29 The diagnosis of infection, sepsis, and MODS in severely burned patients represents a major challenge, and a delayed diagnosis within a few hours has been shown to lead to increased mortality.30 Therefore, it is crucial to find a significant risk factor in the early period of severe burn injury that could predict the poor prognosis of fatal injuries in the late postburn period.
This study, in our opinion, was the first to investigate the value of NLR in predicting the 90-day mortality in severely burned patients. In the present study, we collected and retrospectively analyzed the data of 577 burn patients admitted to the First Affiliated Hospital of Anhui Medical University and Ruijin Hospital of Shanghai Jiao Tong University between 2008 and 2015. We found that age, mechanical ventilation, BI, and 7th day red blood cell and PLT counts were independent risk factors of mortality during the late postburn period as documented elsewhere.31 Furthermore, in this study, we found that the 3rd day NLR was associated with mortality during the late postburn period.
In our study, we found that the 3rd day NLR was a predictor of 90-day mortality in cases of severe burn injury. NLR was first confirmed as an indicator of inflammation in1967.5 Owing to its easy and quick calculation from clinical data and its predictive power for inflammation, NLR is used to predict the prognosis of several serious diseases, such as sepsis, cardiovascular disease and malignancies.6–8 In burn patients, preoperative NLR is useful for the early detection of postoperative acute kidney injury.32 The NLR, calculated from the NLR ratio, is elevated with an increase in neutrophil counts or decrease in lymphocyte counts that could reflect the immune response of the host and as the NLR value becomes above 10, the more specific and concerning it becomes.9,33
A previous study documented that NLR increases rapidly following acute physiologic stress within 6 hours,34 which is consistent with our study. We found that the 1st day NLR was high in the survivor and non-survivor groups, but the intergroup difference was insignificant, which could be explained by the excessive release of neutrophils followed by the intense stress of the burn.35–37 The NLR value remained high on the 7th day and the intergroup difference remained insignificant. Neutrophil count reflects the body’s response to external stimuli. Hampson showed that the circulating number of neutrophils was elevated within 24 hours of a burn injury, returned to normal levels on day 3, and elevated again at day 7.38 Studies have documented that the lymphocyte populations were diminished on the 3rd day postburn and the abnormal lymphocyte count at 72 hours postburn injury has been associated with adverse outcomes.39,40 The adverse outcomes contain infections, length of stay, intensive care unit length of stay, and ventilator days.39,40 As far as we know, there were few studies concerning the decline in early lymphocyte numbers with postburn 90d mortality. Since the lymphocyte count is related to the immunization activity of the body, a continuous decrease of lymphocytes may suggest a poor prognosis, which remains to be further studied.
The hemodynamics changed dramatically after severe burns for interfered by hypovolemic shock, fluid resuscitation and acute stress reaction in the first 48h after severe burn injury. With the presence of infection, inflammation and immunosuppression, the blood tests on 7th day are affected by clinical therapy. Therefore, we believe the blood tests count on 3rd day reflect the reaction of the body to the severe burn injury. The neutrophil count and lymphocyte count have dynamic changes on 3rd day postburn injury. Neither the association between neutrophil and acute stress reaction nor the correlation between lymphocyte and immune status can entirely explain the mortality and morbidity in severe burn injuries. Considering both parameters in the analysis can reflect the generalized health information after severe burn injury, the combination of these data may provide more meaningful results. Meanwhile, whether the 1st and 7th day NLRs are associated with burn mortality deserves further study with a larger sample size.
We found that the 3rd day NLR was 9.58 ± 5.22 in the survivor group versus 12.21 ± 6.11 in the non-survivor group, of which the difference was significant. The 3rd day NLR may reflect the immune response of the host and that an NLR >10.50 indicates a poor prognosis in the later period of burn injury.
The predictive accuracy of NLR has been already shown in other medical conditions. In Jin-Sun Park’s study, they reported that increased NLR was associated increased rate of all-cause mortality in 30-day survivors after index ST-elevation myocardial infarction (STEMI), who received a successful coronary intervention.41 In STEMI, baseline NLR can help to assess the prognosis and a more intensive treatment might be needed for patients with increased NLR. In Asuman Celikbilek’s research, NLR served as a simple inexpensive, and readily available marker of prognosis in acute ischemic stroke.42 Simona Lattanzi and his coworkers found that the NLR was associated with 30-day mortality after intracerebral hemorrhage (ICH), and improved the accuracy of outcome prediction when added to the Modified ICH score.43 That is why we described NLR as an independent risk factor for several serious diseases.
This study has several limitations. First, its retrospective nature was a disadvantage since the information was missing for many patients. Second, since only two burn centers participated in the study, patient numbers and distributions are limited. Thirdly, only severe burn injuries were analyzed in this study according to the inclusion and exclusion criteria. And finally, whether advances in therapeutic techniques and economics influenced the results and whether NLR has a prognostic role in minor burns require further investigations.
Affected by many factors, patients with burns over 30% of total body surface area will inevitably have wound infections or multiple infections throughout the treatment. Based on the results of bacterial culture of patients’ wound secretions, we found that the wound of the same patient could cultivate a variety of bacteria during the whole treatment. Therefore, the relationship between NLR and different bacterial infections is difficult to define in this retrospective study. Further studies are warranted to determine the relationship between NLR and different bacterial infections in wound.
The present study demonstrated that the 3rd day NLR was an independent prognostic factor for 90-day mortality in patients with severe burn injury. Further prospective studies are needed to determine the inherent relationship between neutrophil and lymphocyte counts and 90-day mortality in severely burned patients.
Ethic Statement
This study was approved by the Ethics Committee of Anhui Medical University (20131071).
Acknowledgments
We thank Dr. Feng Guo, Shanghai Jiao Tong University Hospital, for his valuable help in data collection. Le Qiu, Xu Jin, Jun-Jie Wang, and Xu-Dong Tang are co-first authors for this study.
Funding
This work was supported by the National Natural Science Foundation of China (Grant no. 81671877).
Disclosure
The authors declare no conflicts of interest in relationship to this study.
References
1. WHO burns. Available from: https://www.who.int/news-room/fact-sheets/detail/burns.
2. Rani M, Nicholson SE, Zhang Q, Schwacha MG. Damage-associated molecular patterns (DAMPs) released after burn are associated with inflammation and monocyte activation. Burns. 2017;43(2):297–303. doi:10.1016/j.burns.2016.10.001
3. Johnson BL
4. Zhang F, Qiu XC, Wang JJ, Hong XD, Wang GY, Xia ZF. Burn-related dysregulation of inflammation and immunity in experimental and clinical studies. J Burn Care Res. 2017;38(6):e892–e899. doi:10.1097/BCR.0000000000000511
5. Bobb GA, Fairchild EJ. Neutrophil-to-lymphocyte ratio as indicator of ozone exposure. Toxicol Appl Pharmacol. 1967;11(3):558–564. doi:10.1016/0041-008x(67)90056-7
6. Martins EC, Silveira LDF, Viegas K, et al. Neutrophil-lymphocyte ratio in the early diagnosis of sepsis in an intensive care unit: a case-control study. Rev Bras Ter Intensiva. 2019;31(1):64–70.
7. Cho JH, Cho HJ, Lee HY, et al. Neutrophil-lymphocyte ratio in patients with acute heart failure predicts in-hospital and long-term mortality. J Clin Med. 2020;9(2):557. doi:10.3390/jcm9020557
8. Russo A, Russano M, Franchina T, et al. Neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and outcomes with nivolumab in pretreated non-small cell lung cancer (NSCLC): a large retrospective multicenter study. Adv Ther. 2020;37(3):1145–1155. doi:10.1007/s12325-020-01229-w
9. Guthrie GJ, Charles KA, Roxburgh CS, Horgan PG, McMillan DC, Clarke SJ. The systemic inflammation-based neutrophil-lymphocyte ratio: experience in patients with cancer. Crit Rev Oncol Hematol. 2013;88(1):218–230. doi:10.1016/j.critrevonc.2013.03.010
10. Sharma BR. Delayed death in burns and the allegations of medical negligence. Burns. 2006;32(3):269–275. doi:10.1016/j.burns.2006.01.012
11. Gomez R, Murray CK, Hospenthal DR, et al. Causes of mortality by autopsy findings of combat casualties and civilian patients admitted to a burn unit. J Am Coll Surg. 2009;208(3):348–354. doi:10.1016/j.jamcollsurg.2008.11.012
12. Chen XL, Liang X, Sun L, Wang F, Liu S, Wang YJ. Microskin autografting in the treatment of burns over 70% of total body surface area: 14 years of clinical experience. Burns. 2011;37(6):973–980. doi:10.1016/j.burns.2011.03.022
13. Luo G, Peng Y, Yuan Z, et al. Fluid resuscitation for major burn patients with the TMMU protocol. Burns. 2009;35(8):1118–1123. doi:10.1016/j.burns.2009.02.020
14. Gong C, Zhang F, Li L, et al. The variation of hemodynamic parameters through PiCCO in the early stage after severe burns. J Burn Care Res. 2017;38(6):e966. doi:10.1097/BCR.0000000000000533
15. You B, Zhang YL, Luo GX, et al. Early application of continuous high-volume haemofiltration can reduce sepsis and improve the prognosis of patients with severe burns. Crit Care. 2018;22(1):173. doi:10.1186/s13054-018-2095-9
16. Gueugniaud PY, Bertin-Maghit M, Hirschauer C, Bouchard C, Petit P. In the early stage of major burns, is there a correlation between survival, interleukin-6 levels and oxygen delivery and consumption? Burns. 1997;23(5):426–431. doi:10.1016/S0305-4179(97)00036-3
17. Loncar Z, Bras M. Coping with severe burns in the early stage after burn injury. J Pain. 2007;8(4):S58–S58. doi:10.1016/j.jpain.2007.02.236
18. Gacto-Sanchez P. Surgical treatment and management of the severely burn patient: review and update. Med Intensiva. 2017. doi:10.1016/j.medin.2017.02.008
19. Xie X, Zhao J, Xie L, et al. Identification of differentially expressed proteins in the injured lung from zinc chloride smoke inhalation based on proteomics analysis. Respir Res. 2019;20(1). doi:10.1186/s12931-019-0995-0.
20. Zhang ZJ, Ding LT, Zou J, Lyu GZ. [Changes of helper T lymphocytes 17 and regulatory T lymphocytes in peripheral blood of patients with extensive burn at early stage in August 2nd Kunshan factory aluminum dust explosion accident and the significance]. Zhonghua Shao Shang Za Zhi. 2018;34(6):360–364. doi:10.3760/cma.j.issn.1009-2587.2018.06.009. Chinese.
21. Wang YB. [Emphasis on the exploration and research of the protective strategy of organs after burns in the early stage]. Zhonghua Shao Shang Za Zhi. 2019;35(3):161–162. doi:10.3760/cma.j.issn.1009-2587.2019.03.001. Chinese.
22. Fang ZY, Sheng ZY, Li N. Modern Treatment of Severe Burns. Springer Science & Business Media; 2012.
23. Yoshino Y, Ohtsuka M, Kawaguchi M, et al. The wound/burn guidelines–6: guidelines for the management of burns. J Dermatol. 2016;43(9):989–1010. doi:10.1111/1346-8138.13288
24. Bloemsma GC, Dokter J, Boxma H, Oen IM. Mortality and causes of death in a burn centre. Burns. 2008;34(8):1103–1107. doi:10.1016/j.burns.2008.02.010
25. Brusselaers N, Monstrey S, Vogelaers D, Hoste E, Blot S. Severe burn injury in Europe: a systematic review of the incidence, etiology, morbidity, and mortality. Crit Care. 2010;14(5):R188. doi:10.1186/cc9300
26. Janzekovic Z. A new concept in the early excision and immediate grafting of burns. J Trauma. 1970;10(12):1103–1108. doi:10.1097/00005373-197012000-00001
27. Rae L, Fidler P, Gibran N. The physiologic basis of burn shock and the need for aggressive fluid resuscitation. Crit Care Clin. 2016;32(4):491–505. doi:10.1016/j.ccc.2016.06.001
28. Suri MP, Dhingra VJ, Raibagkar SC, Mehta DR. Nutrition in burns: need for an aggressive dynamic approach. Burns. 2006;32(7):880–884. doi:10.1016/j.burns.2006.02.006
29. Jackson PC, Hardwicke J, Bamford A, et al. Revised estimates of mortality from the Birmingham Burn Centre, 2001–2010: a continuing analysis over 65 years. Ann Surg. 2014;259(5):979–984. doi:10.1097/SLA.0b013e31829160ca
30. Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34(6):1589–1596. doi:10.1097/01.Ccm.0000217961.75225.E9
31. Qiu L, Chen C, Li SJ, et al. Prognostic values of red blood cell distribution width, platelet count, and red cell distribution width-to-platelet ratio for severe burn injury. Sci Rep. 2017;7(1):13720. doi:10.1038/s41598-017-13151-3
32. Kim HY, Kong YG, Park JH, Kim YK. Acute kidney injury after burn surgery: preoperative neutrophil/lymphocyte ratio as a predictive factor. Acta Anaesthesiol Scand. 2019;63(2):240–247. doi:10.1111/aas.13255
33. Farkas JD. The complete blood count to diagnose septic shock. J Thorac Dis. 2020;12(Suppl 1):S16–S21. doi:10.21037/jtd.2019.12.63
34. Zahorec R. Ratio of neutrophil to lymphocyte counts–rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl Lek Listy. 2001;102(1):5–14.
35. Devine RA, Diltz Z, Hall MW, Thakkar RK. The systemic immune response to pediatric thermal injury. Int J Burns Trauma. 2018;8(1):6–16.
36. Sood RF, Gibran NS, Arnoldo BD, et al. Early leukocyte gene expression associated with age, burn size, and inhalation injury in severely burned adults. J Trauma Acute Care Surg. 2016;80(2):250–257. doi:10.1097/TA.0000000000000905
37. Fang X, Duan SF, Gong YZ, Wang F, Chen XL. Identification of key genes associated with changes in the host response to severe burn shock: a bioinformatics analysis with data from the gene expression omnibus (GEO) database. J Inflamm Res. 2020;13:1029–1041. doi:10.2147/JIR.S282722
38. Hampson P, Dinsdale RJ, Wearn CM, et al. Neutrophil dysfunction, immature granulocytes, and cell-free DNA are early biomarkers of sepsis in burn-injured patients: a prospective observational cohort study. Ann Surg. 2017;265(6):1241–1249. doi:10.1097/SLA.0000000000001807
39. Deveci M, Sengezer M, Bozkurt M, Eski M, Inal A. Comparison of lymphocyte populations in cutaneous and electrical burn patients: a clinical study. Burns. 2000;26(3):229–232. doi:10.1016/s0305-4179(99)00124-2
40. Thakkar RK, Diltz Z, Drews JD, et al. Abnormal lymphocyte response after pediatric thermal injury is associated with adverse outcomes. J Surg Res. 2018;228:221–227. doi:10.1016/j.jss.2018.03.039
41. Park J-S, Seo K-W, Choi B-J, et al. Importance of prognostic value of neutrophil to lymphocyte ratio in patients with ST-elevation myocardial infarction. Medicine. 2018;97(48):e13471. doi:10.1097/MD.0000000000013471
42. Celikbilek A, Ismailogullari S, Zararsiz G. Neutrophil to lymphocyte ratio predicts poor prognosis in ischemic cerebrovascular disease. J Clin Lab Anal. 2014;28(1):27–31. doi:10.1002/jcla.21639
43. Simona L, Francesco B, Eugen T, Claudia C, Mario DN, Mauro S. Neutrophil-to-lymphocyte ratio in acute cerebral hemorrhage: a system review. Transl Stroke Res. 2018:1–9.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.