")
Back to Journals » Clinical Interventions in Aging » Volume 16
Plasma Amyloid-β Oligomerization Tendency Predicts Amyloid PET Positivity
Authors Pyun JM, Ryu JS, Lee R, Shim KH, Youn YC , Ryoo N, Han SW, Park YH, Kang S, An SS , Kim SY
Received 23 March 2021
Accepted for publication 17 April 2021
Published 30 April 2021 Volume 2021:16 Pages 749—755
DOI https://doi.org/10.2147/CIA.S312473
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Jung-Min Pyun,1 Ji Sun Ryu,2 Ryan Lee,2 Kyu Hawn Shim,3 Young Chul Youn,4 Nayoung Ryoo,5 Sang-Won Han,5 Young Ho Park,5 Sungmin Kang,2 Seong Soo A An,6 SangYun Kim5
1Department of Neurology, Uijeongbu Eulji Medical Center, Eulji University, Uijeongbu-si, Gyeonggi-do, Republic of Korea; 2Research and Development, PeopleBio Inc., Seongnam-si, Gyeonggi-do, Republic of Korea; 3Department of Neurology, Veterans Medical Research Institute, Veterans Health Service Medical Center, Seoul, Republic of Korea; 4Department of Neurology, Chung-Ang University College of Medicine, Seoul, Republic of Korea; 5Department of Neurology, Seoul National University College of Medicine and Seoul National University Bundang Hospital, Seongnam-si, Gyeonggi-do, Republic of Korea; 6Department of Bionanotechnology, Gachon University, Seongnam-si, Gyeonggi-do, Republic of Korea
Correspondence: SangYun Kim
Department of Neurology, Seoul National University Bundang Hospital, 82, Gumi-ro 173 Beon-gil, Bundang-gu, Seongnam-si, Gyeonggi-do, 13620, Republic of Korea
Tel +82 31 787 7462 Fax +82 31 787 4059
Email [email protected]
Purpose: Among other emerging amyloid-targeting blood-based biomarkers, Multimer Detection System-Oligomeric Amyloid-β (MDS-OAβ) measures dynamic changes in concentration of oligomeric amyloid-β (OAβ), which is considered the main pathogenic culprit of Alzheimer’s disease (AD), in plasma after spiking with synthetic amyloid-β (Aβ). We aimed to investigate the predictability of MDS-OAβ on amyloid positron emission tomography (PET) positivity.
Patients and Methods: A total of 96 subjects who visited Seoul National University Bundang Hospital for medical check-up complaining of cognitive decline and had undergone extensive medical assessment were recruited. Amyloid statuses were dichotomized into positive or negative based on visual assessment of amyloid PET. Plasma OAβ concentration was measured by MDS-OAβ. In the previous validation study, 0.78ng/mL was established as the cut-off value and the plasma OAβ concentration higher than or equal to the cut-off value was defined as MDS-OAβ positive.
Results: MDS-OAβ positivity could discriminate amyloid PET positivity with the AUC value of 0.855 (95% CI 0.776– 0.933). Adding MDS-OAβ positivity to prediction models including age, MMSE score, and APOE ϵ4 status improved performance up to the AUC value of 0.926 (95% CI 0.871– 0.980).
Conclusion: The Aβ oligomerization tendency in plasma could predict amyloid PET positivity with high performance, and, when it is combined with age, MMSE score, and APOE ϵ4 status, predictability was improved substantially. This suggests the potential of MDS-OAβ as a useful initial stage test in the clinical and research fields of AD.
Keywords: multimer detection system-oligomeric amyloid-β, Aβ oligomer, predictability, amyloidopathy, blood-based biomarker
Introduction
Brain amyloidopathy is a hallmark of Alzheimer’s disease (AD) and pathologic changes associated with amyloid-β (Aβ) are known to start 10–20 years prior to clinical manifestation.1,2 Due to such a long period of progressive pathological changes without symptoms, prediction of disease progression has always been a challenge. Also, as clinical trials on disease-modifying treatment have not shown satisfactory results, the necessity of making the early AD stage the therapeutic target population has been emphasized, as well as the importance of early detection of amyloidopathy.
Currently, brain amyloidopathy is assessed by amyloid positron emission tomography (PET) and the cerebrospinal fluid (CSF) biomarker test.3 However, their high cost and invasiveness limit their utility in spite of increased need and, hence, the development of an AD biomarker which could overcome such limitations has been long anticipated. There have been efforts to develop an amyloid-targeting blood-based biomarker in order to provide better accessibility in the research and primary care fields, and blood-based biomarkers have shown promising potential in their utility in the prediction of amyloidopathy.4
Multimer Detection System-Oligomeric Amyloid-β (MDS-OAβ) is a modified atypical sandwich immunoassay for measuring Aβ oligomerization in plasma.5 MDS was originally developed as a means to detect prion oligomers in the blood of scrapie-infected animals, which selectively detect oligomers over monomers. The technique was further modified by spiking synthetic Aβ into plasma prior to the antigen–antibody reaction to measure the oligomerization tendency of plasma Aβ. It measures the dynamic change of plasma oligomeric Aβ concentration, which is higher in AD patients compared to normal healthy controls.5,6 In previous studies, MDS-OAβ could differentiate AD from a normal control group with high sensitivity and specificity.5,6
In this study, we aimed to evaluate the predictability of plasma Aβ oligomerization tendency measured by MDS-OAβ on brain amyloidopathy.
Patients and Methods
Subjects
An observational cross-sectional study was conducted. We included subjects who visited the Neurocognitive Behavior Center of the Seoul National University Bundang Hospital, Republic of Korea for medical check-up regarding complaints about cognitive decline and had undergone extensive evaluation of cognitive function, including: physical, neurological, neuropsychological, genetic (APOE genotyping), and biomarker analyses such as brain magnetic resonance imaging, amyloid PET, and MDS-OAβ. Diagnostic work-ups except MDS-OAβ were performed partially in other medical centers and those patients were then referred to our medical center for further evaluation. Patients who had not undergone amyloid PET or MDS-OAβ were excluded from this study. Subjects consisted of 54 probable AD dementia patients according to the National Institute on Aging–Alzheimer’s Association criteria,7 27 mild cognitive impairment (MCI) patients according to the National Institute on Aging–Alzheimer’s Association criteria,8 7 subjective cognitive decline (SCD) patients according to the guideline by Jessen et al,9 and 8 other neurodegenerative diseases as a disease control group: 4 frontotemporal dementia (FTD) patients,10,11 1 corticobasal syndrome (CBS) patient,12 1 Parkinson’s disease dementia (PDD) patient,13 and 2 progressive supranuclear palsy (PSP) patients.14 Written informed consent was obtained from all subjects or their caregivers. This study was approved by the institutional review board of the Seoul National University Bundang Hospital (B-2004-604-305). This study was conducted in accordance with the Declaration of Helsinki.
Blood Sampling and MDS-OAβ Measurement
Blood was collected in 10-mL sodium heparin-containing tubes (BD-367874; BD Bioscience, San Jose, CA, USA) and centrifuged at 1500×g for 10 minutes at room temperature. The time interval between the blood sampling and centrifugation was a maximal 3 hours. The plasma supernatant was aliquoted and stored in screw cap microtubes (polypropylene, SARSTEDT, Ref. number: 72.690) at −80°C until further analysis.
The MDS-OAβ measurement was performed using the inBloodTM OAβ test (PeopleBio Inc., Gyeonggi-do, Republic of Korea) with heparin-treated plasma samples. The OAβ test is a modified sandwich Enzyme-Linked Immunosorbent Assay (ELISA) for measuring oligomerization tendency using two epitope-overlapping antibodies specific for the N-terminus of Aβ. The antibodies used are mouse monoclonal 6E10 (BioLegend, San Diego, CA, USA) and WO-2-HRP (Absolute Antibody Ltd, Oxford, UK) and the epitopes for these antibodies overlap at the N-terminus of Aβ. 6E10, the capturing antibodies, are coated on the wells of the 96-well plate to initially capture heterogenous forms of Aβ. WO-2-HRP, the detection antibodies, are added after the first antigen–antibody reaction and three rounds of washing to detect oligomeric forms of Aβ and produce signal via chemiluminescence.
Prior to the assay, plasma samples were thawed at 37°C for 15 min. PBR-1 (synthetic Aβ made by PeopleBio Inc.) was then spiked into plasma and the mixture was incubated at 37°C for 48 hours. The incubated plasma sample mixture and serially diluted standard samples were added to respective wells, and the plates were incubated at room temperature for 1 hour. Afterwards, 100 µL/well of enhanced chemiluminescence substrate solution (Rockland Immunochemicals Inc., Limerick, PA, USA) was added, and the Relative Luminescence Unit (RLU) signal was detected using a Victor 3TM multi-spectrophotometer. Dilutions providing signal in the linear range of the standard curves were used for the conversion to RLU values to determine the concentration of oligomerized Aβ. All tests were completed in duplicate and the average was used. 0.78 ng/mL was established as the cut-off value in the previous validation study and the plasma OAβ concentration equal to or higher than the cut-off value was defined as MDS-OAβ positive.6 The MDS-OAβ tester was blinded to clinical information, including demographics and diagnosis.
Amyloid Status
Amyloid status was evaluated by amyloid PET. [18F]Florbetaben (n=82), [18F]Flutemetamol (n=6), [18F]Florbetapir (n=2), and [11C]Pittsburgh compound B (PiB; n=1) were used as ligands. Amyloid status was defined as positive (abnormal) or negative (normal) after visual assessment by nuclear medicine physicians and two neurologists.
Statistical Analysis
Baseline characteristics of the amyloid normal and abnormal groups were compared using chi-squared tests and Mann–Whitney U-tests, as appropriate. The predictive ability of MDS-OAβ and covariates on amyloid PET positivity was assessed by binary logistic regression models and presented as area under the curve (AUC) values by receiver operating characteristic (ROC) analysis. All statistical analyses were performed by R (version 4.0.0) and statistical significance was set at 0.05.
Results
Demographics and Clinical Characteristics
A total of 96 subjects were included in the study. The average age of total subjects was 71.50 ± 9.73 years old, and 42 subjects (43.8%) were male. Among the total cohort, 68 (70.8%) subjects presented as amyloid-positive and 28 subjects were amyloid-negative. Comparisons of baseline characteristics of the groups are shown in Table 1. There was no significant difference in age, sex, education level, or frequency of APOE ε4 carrier between groups. Amyloid-positive groups showed poor MMSE scores reflecting poor general cognitive function, and higher CDR and CDR-SOB indicating increased disease severity. Correspondingly, the amyloid-positive group contained more AD patients than the amyloid-negative group. The amyloid-positive group presented a significantly higher MDS-OAβ value with a plasma oligomeric Aβ concentration of 0.89 ng/mL than the amyloid-negative group with 0.67 ng/mL (Figure 1).
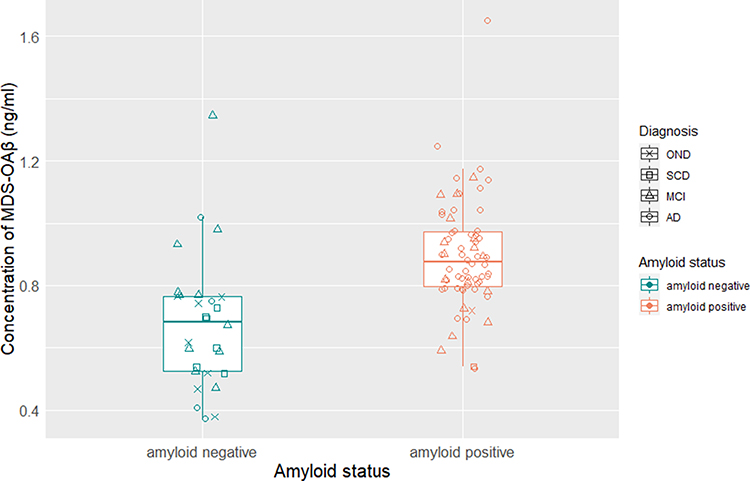 |
Figure 1 Concentration of plasma MDS-OAβ according to groups. Abbreviations: AD, Alzheimer’s disease; MCI, mild cognitive impairment; MDS-OAβ, Multimer Detection System-Oligomeric Amyloid-β; OND, other neurodegenerative disease; SCD, subjective cognitive decline. |
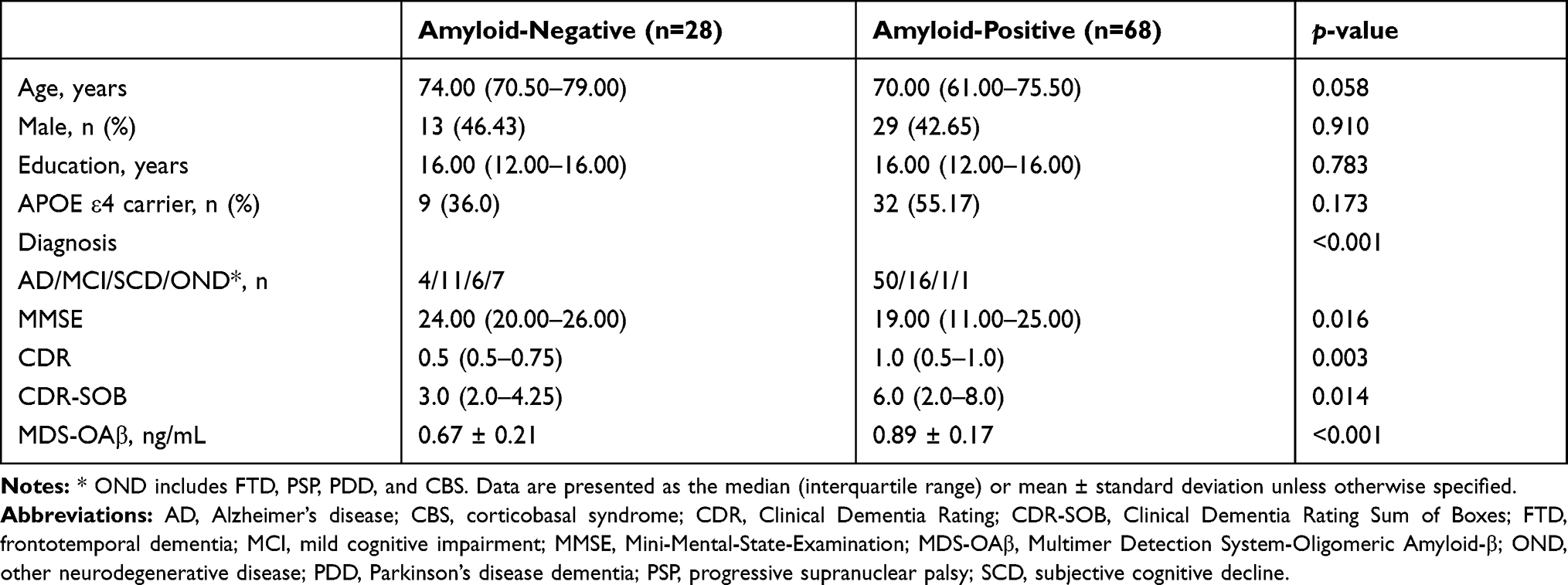 |
Table 1 Demographics and Clinical Characteristics of Subjects |
MDS-OAβ as a Predictor of Amyloid Status
MDS-OAβ positivity could differentiate amyloid-positive subjects from amyloid-negative subjects with a sensitivity of 85.3% and a specificity of 85.7% (AUC = 0.855, 95% CI = 0.776–0.933). Multivariate models with MDS-OAβ positivity and other covariates including age, MMSE score, and APOE ε4 status showed much better performance with AUC values between 0.892 and 0.926 than multivariate models without MDS-OAβ positivity (Table 2). Among various combinations of predictors, MDS-OAβ positivity combined with age, APOE ε4 status, and MMSE score demonstrated the highest AUC value, 0.926 (0.871–0.980).
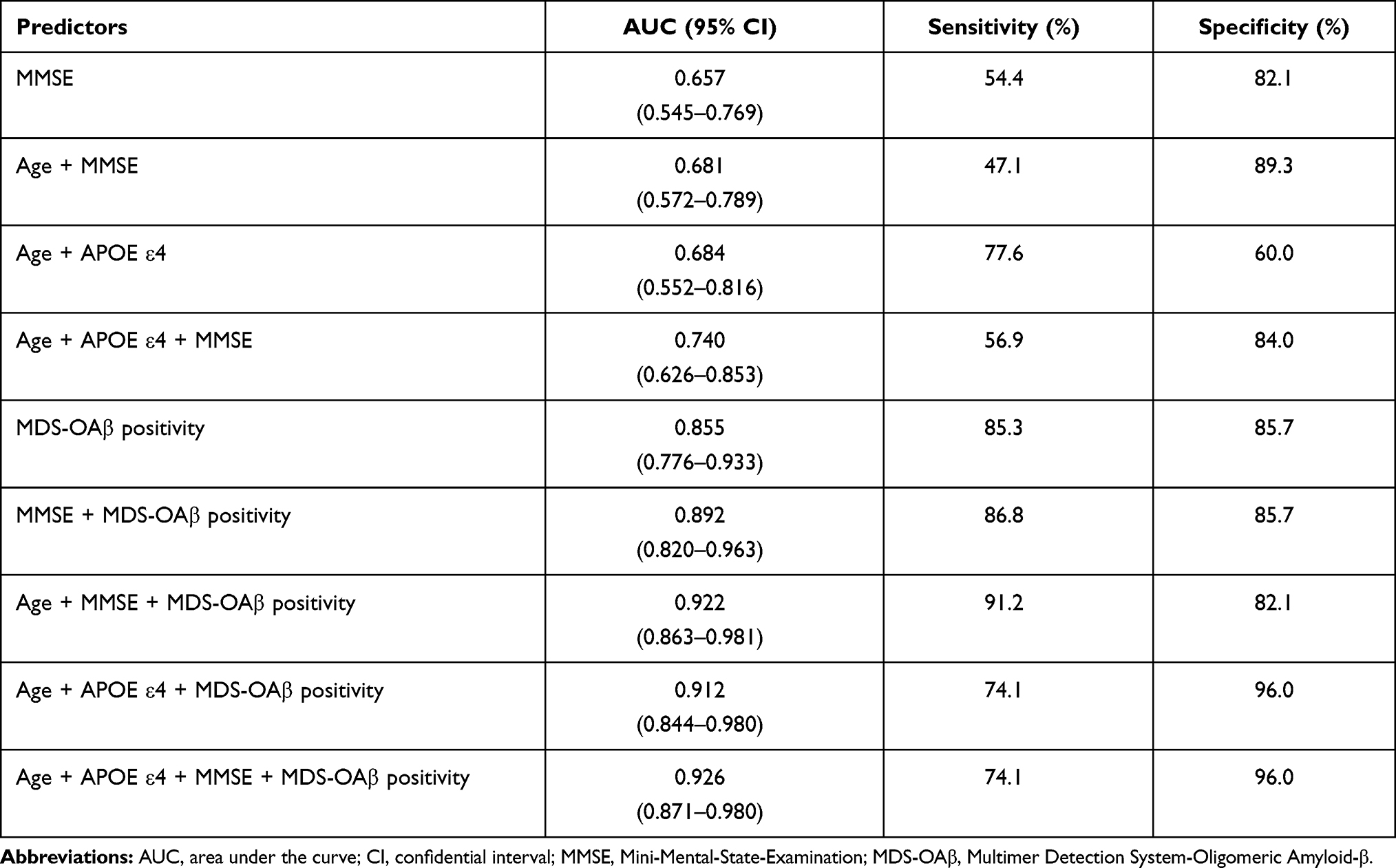 |
Table 2 Performance of Predictors for Amyloid PET Positivity with and without MDS-OAβ Positivity |
MDS-OAβ positivity alone presented better predictability than MMSE alone (AUC = 0.657, 95% CI = 0.545–0.769). Although, when combined with age and APOE ε4 status, the AUC value for MMSE increased to 0.740 (95% CI = 0.626–0.853), this was not statistically significant compared with MMSE alone. However, when the combination of predictors was added to MDS-OAβ positivity, predictive performance improved significantly (AUC = 0.926, 95% CI = 0.871–0.980) (Figure 2A). When the combination excluded MMSE and was inclusive of only objective factors such as age and APOE ε4 status, the predictability on amyloid PET positivity was 0.684 (0.552–0.816). Adding MDS-OAβ positivity to the combination strengthened the predictability to 0.912 (0.844–0.980) (Figure 2B).
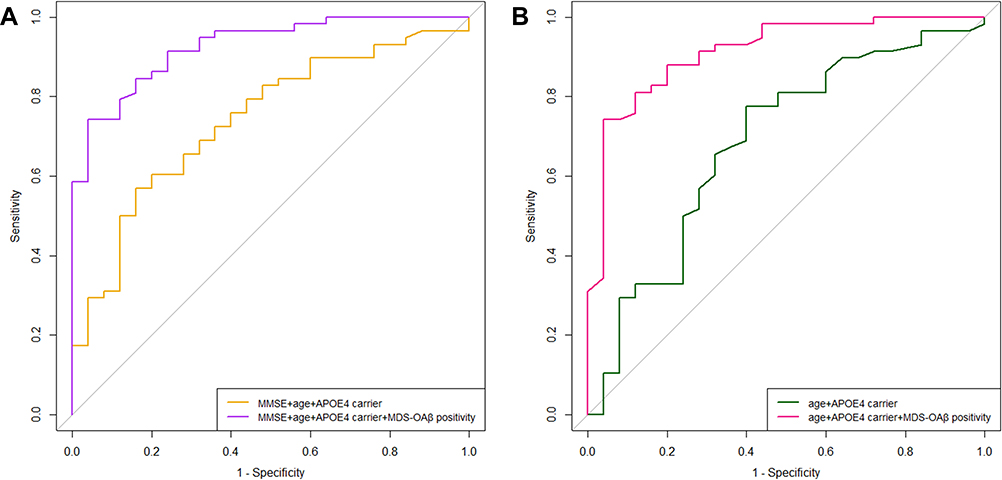 |
Figure 2 Receiver operating characteristic analysis of MDS-OAβ positivity with other predictors on amyloid PET positivity. (A) Added MDS-OAβ positivity to clinical information such as age, MMSE score, and APOE ε4 status, predictability for amyloid PET positivity improves. (B) Considered only objective factors such as age and APOE ε4 status, combining with MDS-OAβ positivity strengthened the predictability on amyloid PET positivity. Abbreviations: MDS-OAβ, Multimer Detection System-Oligomeric Amyloid-β; MMSE, Mini-Mental-State-Examination. |
Discussion
In this study, we found that MDS-OAβ positivity could discriminate amyloid PET positivity with the AUC value of 0.855. Furthermore, adding MDS-OAβ positivity to prediction models including age, MMSE score, and APOE ε4 status improved the performance significantly up to the AUC value of 0.926.
A substantial effort has been made to detect and measure amyloid-β in the blood and several assays were promising candidates for blood-based biomarkers.4 These assays principally aimed to quantify the concentration of Aβ42 and Aβ42/Aβ40. However, they have been employed in a limited capacity due to several unique characteristics of this protein, such as its scarcity in the blood15 and tendency to self-aggregate,16 as well as of the blood matrix such as the abundance of various Aβ-binding proteins in the blood,17 which interfere in the detection of Aβ.
MDS-OAβ, on the other hand, takes a distinct approach to possibly overcoming the said challenges. It measures the Aβ oligomerization tendency of plasma by implementing the spiking of synthetic Aβ,5 prior to selective detection of Aβ oligomers, reputedly the main pathogen of AD,18 over Aβ monomers using epitope-overlapping antibodies. It is highly anticipated that this technique shall bring an unprecedented solution to detection and monitoring of AD-related amyloid dynamics in the blood.
The discriminative performance of MDS-OAβ between AD and a normal control group has been demonstrated in previous studies. In the study by An et al, the MDS-OAβ assay mechanism and its diagnostic performance were evaluated. The AD group (n=27) was differentiated from the age-matched normal control group (n=144) with AUC of 0.896 (sensitivity 83.3%, specificity 90.0%).5 A recent validation study with AD (n=52) and normal control (n=52) confirmed the diagnostic accuracy with an AUC value of 0.999 (sensitivity 100%, specificity 92.31%).6 The current study was completed in a more heterogeneous population including individuals with AD, MCI, SCD, or other neurodegenerative diseases, and predictability on amyloid PET positivity was comparable (AUC 0.855). In various combinations with age, MMSE scores, and APOE ε4 status, AUC values increased between 0.892 and 0.926. These are also comparable with or even better than performance of other amyloid-targeting blood-based assays including immunoprecipitation followed by mass spectrometry,19,20 single-molecule arrays,21,22 and immune-infrared-sensor.23,24
Another interesting finding was that the predictability of amyloid PET positivity was considerably enhanced when combining MDS-OAβ positivity with age and MMSE scores, with the AUC increasing to 0.922, whereas the predictability of age and MMSE scores combined had only an AUC of 0.681 (95% CI 0.572–0.789). In clinical settings such as primary care, age and MMSE scores might be the only accessible information, and transfer of patients to specialized memory clinics for further work-up often relies on limited information based on MMSE score and age. A blood test such as the MDS-OAβ which has good predictability on amyloid PET positivity could be implemented as an early stage AD blood test to address such drawbacks and be utile in terms of screening the patients in advance of further diagnostic examination. A previous study showed that amyloid PET provided more diagnostic confidence for clinicians than a CSF biomarker test, and the concordance of amyloid positivity in amyloid PET and CSF in the study was moderate with an unweighted k value of 0.52 (95% CI 0.32–0.72).25 This could result from the fact that those two biomarkers detect different amyloid-β forms in different temporal dynamics.25 In our study, the concordance between amyloid PET and MDS-OAβ was substantial, with an unweighted k value of 0.67 (95% CI 0.51–0.83). Both biomarkers, each as a fluid and imaging biomarker, have different modalities, with different dynamics of action and target. In order to deepen understanding of MDS-OAβ, the influential factors of MDS-OAβ, such as interactive proteins in plasma, should be further investigated in the future.26
In this study, we could not analyze the association between MDS-OAβ and quantitative measures of amyloid PET due to partial absence of data for imaging analyses. Although we could not provide quantitative analyses of amyloid PET, use of visual rating just as a routine reading process could benefit in clinical practice.
Conclusion
In summary, Aβ oligomerization tendency in plasma measured by MDS-OAβ could predict amyloid PET positivity (AUC = 0.855, 95% CI = 0.776–0.933). Furthermore, when MDS-OAβ positivity is combined with clinical information such as age, MMSE score, and APOE ε4 status, predictability for amyloid PET positivity was improved (AUC = 0.926, 95% CI = 0.871–0.980). This suggests the potential of MDS-OAβ as a useful initial stage test in the clinical and research fields of AD.
Ethics Approval and Informed Consent
This study was approved by the institutional review board of the Seoul National University Bundang Hospital (B-2004-60-305). Written informed consent was obtained from all subjects or their caregivers.
Author Contributions
All authors met the following conditions:
- Made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas.
- Drafted or wrote, or substantially revised or critically reviewed, the article.
- Agreed on the journal to which the article will be submitted.
- Reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage.
- Agree to take responsibility and be accountable for the contents of the article.
Funding
This study was not funded.
Disclosure
All authors declare no competing interests.
References
1. Jack CR, Knopman DS, Jagust WJ, et al. Tracking pathophysiological processes in Alzheimer’s disease: an updated hypothetical model of dynamic biomarkers. Lancet Neurol. 2013;12:207–216.
2. Bateman RJ, Xiong C, Benzinger TLS, et al. Clinical and biomarker changes in dominantly inherited Alzheimer’s disease. N Engl J Med. 2012;367:795–804.
3. Jack CR, Bennett DA, Blennow K, et al. NIA-AA Research Framework: toward a biological definition of Alzheimer’s disease. Alzheimer’s Dement. 2018;14:535–562.
4. Pyun J-M, Kang MJ, Ryoo N, et al. Amyloid metabolism and amyloid-targeting blood-based biomarkers of Alzheimer’s Disease. J Alzheimer’s Dis. 2020;75:685–696.
5. An SSA, Lee BS, Yu JS, et al. Dynamic changes of oligomeric amyloid β levels in plasma induced by spiked synthetic Aβ42. Alzheimer’s Res Ther. 2017;9:86.
6. Youn YC, Lee BS, Kim GJ, et al. Blood Amyloid-β oligomerization as a biomarker of Alzheimer’s disease: a blinded validation study. J Alzheimer’s Dis. 2020;75:493–499.
7. McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011;7:263–269.
8. Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011;7:270–279.
9. Jessen F, Amariglio RE, Van Boxtel M, et al. A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimer’s Dement. 2014;10:844–852.
10. Rascovsky K, Hodges JR, Knopman D, et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain. 2011;134:2456–2477.
11. Gorno-Tempini ML, Hillis AE, Weintraub S, et al. Classification of primary progressive aphasia and its variants. Neurology. 2011;76:1006–1014.
12. Armstrong MJ, Litvan I, Lang AE, et al. Criteria for the diagnosis of corticobasal degeneration. Neurology. 2013;80:496–503.
13. Dubois B, Burn D, Goetz C, et al. Diagnostic procedures for Parkinson’s disease dementia: recommendations from the Movement Disorder Society Task Force. Mov Disord. 2007;22:2314–2324.
14. Litvan I, Agid Y, Calne D, et al. Clinical research criteria for the diagnosis of progressive supranuclear palsy (Steele-Richardson-Olszewski syndrome): report of the NINDS-SPSP International Workshop. Neurology. 1996;47:1–9.
15. Toledo JB, Vanderstichele H, Figurski M, et al. Factors affecting Aβ plasma levels and their utility as biomarkers in ADNI. Acta Neuropathol. 2011;122:401–413.
16. Serem WK, Bett CK, Ngunjiri JN, et al. Studies of the growth, evolution, and self-aggregation of β-amyloid fibrils using tapping-mode atomic force microscopy. Microsc Res Tech. Microsc Res Tech. 2011;74:699–708.
17. Kuo YM, Emmerling MR, Lampert HC, et al. High levels of circulating Aβ42 are sequestered by plasma proteins in Alzheimer’s disease. Biochem Biophys Res Commun. 1999;257:787–791.
18. Cline EN, Bicca MA, Viola KL, et al. The Amyloid-β oligomer hypothesis: beginning of the third decade. J Alzheimer’s Dis. 2018;64:S567–S610.
19. Ovod V, Ramsey KN, Mawuenyega KG, et al. Amyloid β concentrations and stable isotope labeling kinetics of human plasma specific to central nervous system amyloidosis. Alzheimer’s Dement. 2017;13:841–849.
20. Nakamura A, Kaneko N, Villemagne VL, et al. High performance plasma amyloid-β biomarkers for Alzheimer’s disease. Nature. 2018;554:249–254.
21. Verberk IMW, Slot RE, Verfaillie SCJ, et al. Plasma amyloid as prescreener for the earliest alzheimer pathological changes. Ann Neurol. 2018;84:648–658.
22. Vergallo A, Mégret L, Lista S, et al. Plasma amyloid β 40/42 ratio predicts cerebral amyloidosis in cognitively normal individuals at risk for Alzheimer’s disease. Alzheimer’s Dement. 2019;15:764–775.
23. Nabers A, Ollesch J, Schartner J, et al. Amyloid-β-Secondary structure distribution in cerebrospinal fluid and blood measured by an immuno-infrared-sensor: a biomarker candidate for Alzheimer’s disease. Anal Chem. 2016;88:2755–2762.
24. Güldenhaupt J, Brenner H, Janelidze S, et al. Amyloid blood biomarker detects Alzheimer’s disease. EMBO Mol Med. 2018;10:e8763.
25. Ramusino MC, Garibotto V, Bacchin R, et al. Incremental value of amyloid-PET versus CSF in the diagnosis of Alzheimer’s disease. Eur J Nucl Med Mol Imaging. 2020;47(2):270–280.
26. Choi Y, Joh Y, Ryu JS, et al. Endogenous Aβ peptide promote Aβ oligomerization tendency of spiked synthetic Aβ in Alzheimer’s disease plasma. Mol Cell Neurosci. 2021;111:103588.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.