")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Plasma Adipsin as a Biomarker and Its Implication in Type 2 Diabetes Mellitus
Authors Tafere GG , Wondafrash DZ , Zewdie KA , Assefa BT , Ayza MA
Received 14 March 2020
Accepted for publication 1 May 2020
Published 28 May 2020 Volume 2020:13 Pages 1855—1861
DOI https://doi.org/10.2147/DMSO.S253967
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Gebrehiwot Gebremedhin Tafere, Dawit Zewdu Wondafrash, Kaleab Alemayehu Zewdie, Brhane Teklebrhan Assefa, Muluken Altaye Ayza
Department of Pharmacology and Toxicology, School of Pharmacy, Mekelle University, Mekelle, Ethiopia
Correspondence: Gebrehiwot Gebremedhin Tafere
Department of Pharmacology and Toxicology,School of Pharmacy, Mekelle University, P.O. Box: 1871, Mekelle, Ethiopia
Tel +251 908822323
Email [email protected]
Abstract: Diabetes mellitus (DM) is a worldwide health threat affecting millions of people, which is associated with different micro- and macro-vascular complications. Type 2 diabetes mellitus (T2DM) is one of the different types of DM caused by insulin resistance and/or reduced secretion of insulin from the pancreas. A validated novel biomarker is required to enhance the accuracy of disease prediction, provide novel insights into pathophysiology and contribute to future prevention of T2DM. Various newer diagnostic methods have been developed by targeting endogenous proteins among which Adipsin is one of the promising target. Therefore, this review discusses Adipsin as a potential biomarker and its implication in T2DM. Adipsin is one of the adipokines secreted by adipose tissues which is involved in maintaining adipose tissue homeostasis and increasing insulin secretion in response to glucose. According to different experimental and clinical studies, plasma Adipsin concentrations are low in animals and patients with DM which support its use as a biomarker in combination to the other diagnostic modalities for DM. Additionally, the existence of Adipsin could be important in improving hyperglycemia by preserving β-cell mass through improving β-cell survival and maintaining their transcriptional identity.
Keywords: adipsin, type 2 diabetes mellitus, biomarker
Introduction
Diabetes mellitus is one of the most common metabolic disorders characterized by hyperglycemia.1 It occurs due to absolute or partial lack of insulin and/or insulin resistance.2 Diabetes mellitus is a common public health threat affecting millions of people in the world of all ages, gender, race and ethnic groups.3 The burden of DM is increasing throughout the world, and around 80% of diabetes deaths occur mainly in low and middle-income countries.4 Based on the pathogenesis of hyperglycemia, most patients with DM are either Type 1 (insulin dependent) or Type 2 (non-insulin dependent).5 Among which, T2DM has been most commonly reported (90–95% of cases).6
According to World Health Organization (WHO) report in 2019, DM affects around 422 million adults in the world.2 In 2013, DM was the seventh leading cause of death (causing 74.9 thousand deaths) and it is the eighth leading cause of disability (causing 1.85 million years living with disability).7 It is also estimated that diabetes will affect 642 million in 2040.8 Even though the prevalence of DM diagnosed patients is high, nearly half of them are unaware of their disease.9 On the other hand, according to the International Diabetes Federation, T2DM contributes for the sufferings of about 415 million people in the world; and it is becoming increasing in its prevalence.10
The pathologic hallmarks of T2DM are mainly abnormal insulin secretion and increased insulin resistance. There is also a decrease in the functional pancreatic β-cell mass over time upon the progression of the disease condition.11 T2DM is associated mainly with obesity, which results in impaired insulin mediated glucose uptake due to intracellular impairment of insulin signaling. There is also a significant reduction in glucagon-like peptide-1 secretion, which is secreted after food ingestion and increases insulin secretion, in patients with T2DM.12
If left untreated, DM is associated with devastating short-term (diabetic ketoacidosis and hyperosmolar hyperglycemic state) and long-term (retinopathy, nephropathy, neuropathy and lower limp amputation) complications.5,13,14 Moreover, different cardiovascular and endocrine abnormalities are associated with DM, which can affect the quality of life of patients.8,15
The diagnosis of DM has been varied from time to time. However, recurrent or persistent hyperglycemia is used to characterize DM. Different diagnostic parameters were used to assess patients with DM including, fasting plasma glucose (FPG), oral glucose tolerance test (OGTT) and Hemoglobin Alc (HgA1c).16,17 However, these diagnostic tools are associated with reduced sensitivity and/or specificity to detect diabetes in its early stage.18 To overcome such problems different newer diagnostic methods were developed by targeting endogenous proteins such as Leptin, TNF-alpha, C-reactive protein (CRP),19 Netrin,20 Thioredoxin-interacting protein (TXNIP).3 But, these novel methods have been also associated with increased cost.21 Hence, the present review is used to assess the role of Adipsin as a novel diagnostic parameter and its implication in T2DM.
Overview of Adipsin
Adipose tissue is no longer regarded as a passive site for energy accumulation in the form of triacylglycerols. Nevertheless, it is also a vital endocrine gland that secretes many bioactive molecules.22,23 Adipokines (or adipocytokines) can be defined as a group of more than 600 bioactive molecules made from adipose tissue that acts as paracrine and endocrine hormones.23,24 Adipokines are involved in maintaining varieties of processes such as, appetite and satiety, energy expenditure activity, endothelial function, blood pressure, hemostasis, adipogenesis, insulin sensitivity, energy metabolism in insulin-sensitive tissues, fat distribution and insulin secretion in pancreatic β-cells.25–27 Adipsin, also termed as complement factor D, is one of the adipokines which was the first described adipokine.28 Adipsin is a member of the serine protease family with a 28-kilo Dalton protein found in 3T3 adipocytes.29 Adipsin maintain adipose tissue homeostasis and increases insulin secretion in response to glucose. Additionally, it catalyzes C3a (an active form of component 3, C3) production by controlling the alternative complement pathway causing an increase in insulin secretion from the pancreas.30,31
Adipsin is important in the formation of the C5–C9 membrane attack complex and in the generation of various signaling molecules, comprising the anaphylatoxins, complement 3a (C3a) and C5a.30 In the synthesis, these signaling molecules, first complement factor B is cleaved by Adipsin and these catalyze the formation of C3 convertase and it leads to the hydrolysis cascade that produces different complement fragments including C3a, C3b, C5a and C5b.32 It was reported that familial C3 deficiency is associated with obesity and metabolic diseases, and C3a levels are risk factors for DM.33 The overall effect of Adipsin on insulin secretion is summarized in Figure 1.
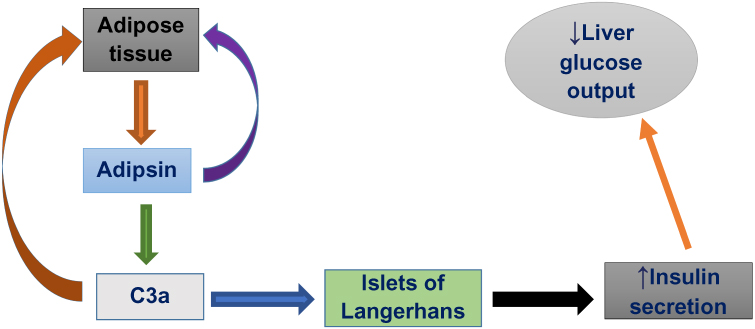 |
Figure 1 Effect of adipsin on insulin secretion. |
Preclinical and Clinical Studies on the Serum Levels of Adipsin in Type 2 Diabetes Mellitus
Circulating Adipsin levels are negatively correlated with T2DM. Various experimental and clinical studies showed that plasma concentrations of Adipsin is decreased in humans and animals with DM compared to the normal control group as indicated in the table below (Table 1).
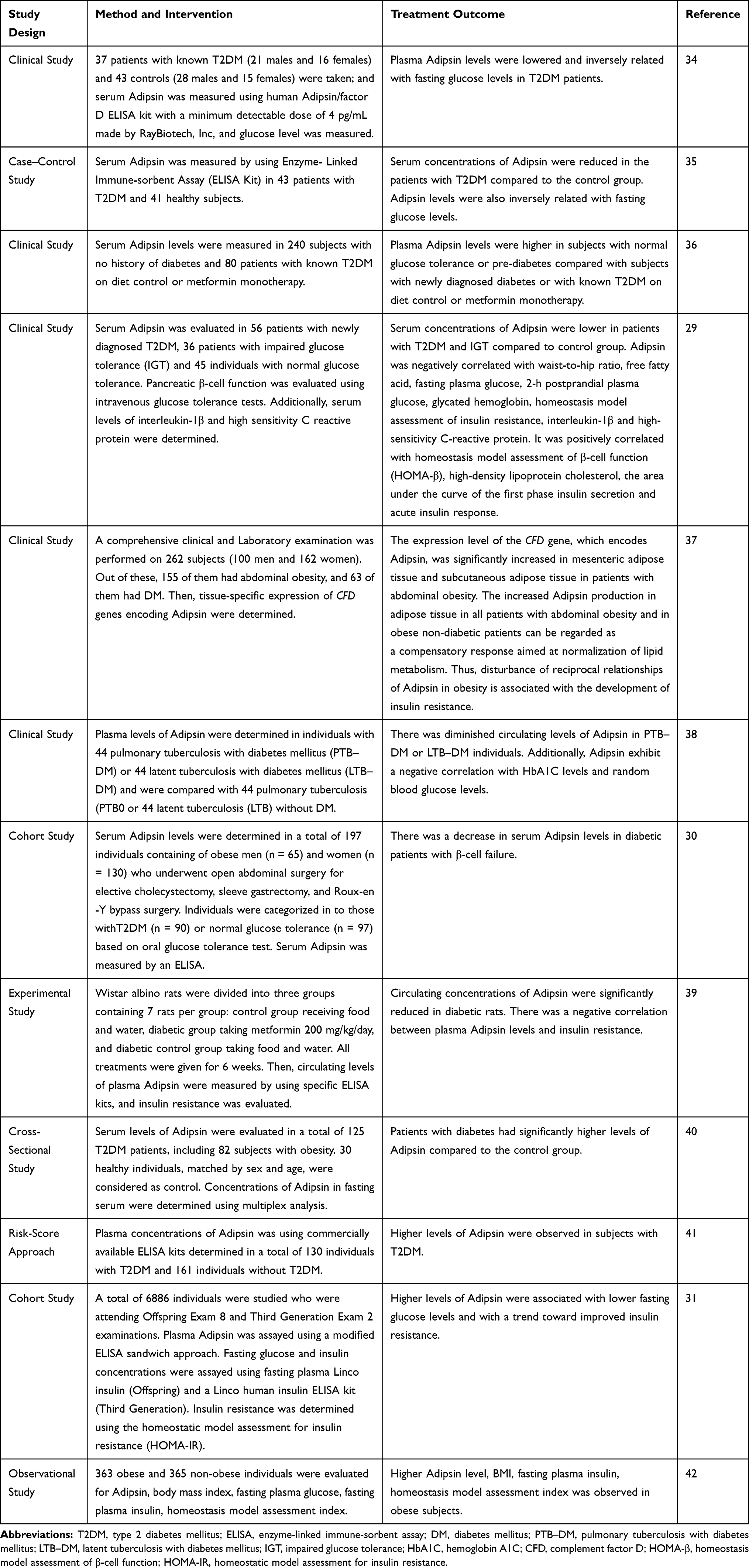 |
Table 1 Serum Levels of Adipsin in Type 2 Diabetes Mellitus |
Implications of Adipsin in Type 2 Diabetes Mellitus
Type 2 diabetes mellitus is characterized by an increase in blood glucose level caused by pancreatic β-cell failure and/or insulin resistance.43 Adipsin is reported to maintain β-cell function, which is important to boost insulin secretion.30 According to a study by Gómez-Banoy et al31, restoration of Adipsin in diabetic mice did not merely improve hyperglycemia, rather it also preserves β-cell mass by improving β-cell survival and maintaining β-cell transcriptional identity. Additionally, increased Adipsin level is associated with lower risk of diabetes in humans.31
Patients with newly diagnosed diabetes and known T2DM show a decreased levels of Adipsin; and there is an independent negative association between Adipsin and HOMA-IR. It was concluded that the negative association might be due to the expression of inflammatory cytokines like IL-17 in T2DM.36 The plasma concentrations of Adipsin were reduced in T2DM patients with impaired glucose tolerance; which is associated with the first‐phase insulin secretion of pancreatic β‐cells and glucose metabolism. This was evidenced by the positive correlation between serum Adipsin and HOMA‐β.29
In obesity complicated with T2DM, there is a disturbance in the relationship between Adipsin and leptin. An increase in Adipsin production in obesity can be regarded as a compensatory response for normalizing the parameters of the lipid and carbohydrate metabolism.37
Unlike other insulin secretagogues, various preclinical studies showed that Adipsin replenishment in diabetic mice reduces hyperglycemia, and raises insulin levels while maintaining β-cells by stopping dedifferentiation and death. In recent times, Adipsin has been found capable of promoting insulin secretion and stabilizing plasma glucose levels. In addition, diabetic mice treated with Adipsin showed significant reductions in fasting plasma glucose and increased glucose clearance, while fasting and glucose-induced insulin levels were also improved.27,30 Adipsin could also stimulate glucose transport for triglyceride accumulation in adipose tissue and inhibits lipolysis. It is justified that free fatty acids could exacerbate pancreatic β-cell failure and insulin resistance.37
On the other hand, the negative correlation between Adipsin and insulin resistance in diabetic rats implies that Adipsin might increase insulin sensitivity and reduce glucose intolerance in T2DM.39 As explained by Lo et al, the possible mechanism by which Adipsin increases insulin secretion is via generating C3a. C3a acts on islets of the pancreas by augmenting its receptor (C3aR1) and inhibiting ATP sensitive K+ channel, thus, increasing intracellular Ca2+ concentrations.30
Klimontov et al40 reported that the serum concentrations of Adipsin were increased in patients with T2DM by which they did not confirm the inverse relationship of Adipsin with T2DM. The possible reasons for these inconsistencies could be that the authors used small sample size of patients, a large number of patients receiving insulin therapy, and unable to differentiate subcutaneous and visceral fat depots as stated in their paper as a limitation of their study.
Conclusion and Future Perspective
Though there are different diagnostic and management modalities for DM, it is becoming a public health threat causing different micro and macro-complications in the world. To prevent these complications and to reduce mortality associated with DM, searching new promising diagnostic and therapeutic options are important. Adipsin, secreted by the adipocytes, has a crucial role in maintaining adipose tissue homeostasis and increases insulin secretion in response to glucose. It has the potential to become an early novel biomarker in patients with T2DM.
Various clinical and animal studies showed that there is a reduction in the plasma concentrations of Adipsin in animals/humans with DM. Additionally, Adipsin has varieties of effects in the pancreas including preserving β-cell mass by improving β-cell survival and maintaining β-cell transcriptional identity, and promoting insulin secretion from the β-cells of the pancreas. It also stimulates glucose transport for triglyceride accumulation in adipose tissue and inhibits lipolysis.
Further detailed animal and human studies will be required to confirm Adipsin as a novel biomarker for T2DM. Additionally, further investigations are in need to decide the mechanism by which Adipsin increases insulin secretion from β-cells of the pancreas. Adipsin has a biological function in in vivo studies and could be considered as a therapeutic option in the future.
Abbreviations
ADA, American Diabetes Association; CFD, complement factor D; CRP, C-reactive Protein; DM, diabetes mellitus; ELISA, enzyme linked immune-sorbent assay; FPG, fast plasma glucose; HgA1C, hemoglobin A1C; HOMA-IR, homeostasis model assessment–insulin resistance; IGT, impaired glucose tolerance; LTB, latent tuberculosis; OGTT, Oral Glucose Tolerance Test; PLB, pulmonary tuberculosis; T2DM, type 2 diabetes mellitus; TNF, tumor necrosis factor; TXNIP, thioredoxin interacting protein; WHO, World Health Organization.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Oguntibeju O. Pathophysiology and Complications of Diabetes Mellitus. BoD–Books on Demand; 2012.
2. WHO. Classification of Diabetes Mellitus. World Health Organization; 2019:1–40. Licence: CC BY-NC-SA 3.0 IGO 2019.
3. Wondafrash DZ, Nire’a AT, Tafere GG, Desta DM, Berhe DA, Zewdie KA. Thioredoxin-interacting protein as a novel potential therapeutic target in diabetes mellitus and its underlying complications. Diabetes Metab Syndr Obes. 2020;13:43. doi:10.2147/DMSO.S232221
4. Afroz A, Ali L, Karim MN, et al. Glycaemic control for people with type 2 diabetes mellitus in Bangladesh-an urgent need for optimization of management plan. Sci Rep. 2019;9(1):1–10. doi:10.1038/s41598-019-46766-9
5. Baynes HW. Classification, pathophysiology, diagnosis and management of diabetes mellitus. J Diabetes Metab. 2015;6(5):1–9.
6. ADA. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Supplement 1):S81–S90. doi:10.2337/dc14-S081
7. Asmelash D, Asmelash Y. The burden of undiagnosed diabetes mellitus in adult African population: a systematic review and meta-analysis. J Diabetes Res. 2019;2019:1–8. doi:10.1155/2019/4134937
8. Fan W. Epidemiology in diabetes mellitus and cardiovascular disease. Cardiovasc Endocrinol. 2017;6(1):8–16. doi:10.1097/XCE.0000000000000116
9. Piero M, Nzaro G, Njagi J. Diabetes mellitus-a devastating metabolic disorder. Asian J Biomed Pharm Sci. 2015;5(40):1.
10. Elekofehinti OO, Ejelonu OC, Kamdem JP, Akinlosotu OB, Adanlawo IG. Saponins as adipokines modulator: a possible therapeutic intervention for type 2 diabetes. World J Diabetes. 2017;8(7):337. doi:10.4239/wjd.v8.i7.337
11. Kohei K. Pathophysiology of type 2 diabetes and its treatment policy. Jpn Med Assoc J. 2010;53(1):41–46.
12. Zaccardi F, Webb DR, Yates T, Davies MJ. Pathophysiology of type 1 and type 2 diabetes mellitus: a 90-year perspective. Postgrad Med J. 2016;92(1084):63–69. doi:10.1136/postgradmedj-2015-133281
13. Heng L, Comyn O, Peto T, et al. Diabetic retinopathy: pathogenesis, clinical grading, management and future developments. Diabet Med. 2013;30(6):640–650. doi:10.1111/dme.12089
14. Wang W, Lo AC. Diabetic retinopathy: pathophysiology and treatments. Int J Mol Sci. 2018;19(6):1–14.
15. Skyler JS, Bakris GL, Bonifacio E, et al. Differentiation of diabetes by pathophysiology, natural history, and prognosis. Diabetes. 2017;66(2):241–255. doi:10.2337/db16-0806
16. Lyons TJ, Basu A. Biomarkers in diabetes: hemoglobin A1c, vascular and tissue markers. Transl Res. 2012;159(4):303–312. doi:10.1016/j.trsl.2012.01.009
17. Diwaker A, Kishore D, Singh V, Mahapatra SP. The novel biomarkers in diabetes. J Assoc Physicians India. 2019;67(7):65–69.
18. Punthakee Z, Goldenberg R, Katz P. Définition, classification et diagnostic du diabète, du prédiabète et du syndrome métabolique. Can J Diabetes. 2018;42:S10–S15. doi:10.1016/j.jcjd.2017.10.003
19. Riaz S. Study of protein biomarkers of diabetes mellitus type 2 and therapy with vitamin B1. J Diabetes Res. 2015;2015:1–10. doi:10.1155/2015/150176
20. Yimer EM, Zewdie KA, Hishe HZ. Netrin as a novel biomarker and its therapeutic implications in diabetes mellitus and diabetes-associated complications. J Diabetes Res. 2018;2018:1–20. doi:10.1155/2018/8250521
21. Laakso M. Biomarkers for type 2 diabetes. Mol Metab. 2019;27:S139–S146. doi:10.1016/j.molmet.2019.06.016
22. Lu B, Zhao M, Jiang W, et al. Independent association of circulating level of chemerin with functional and early morphological vascular changes in newly diagnosed type 2 diabetic patients. Medicine. 2015;94(47):1–8. doi:10.1097/MD.0000000000001990
23. Mamdouh M, Shaban S, Ibrahim Abushouk A, Zaki MMM, Ahmed OM, Abdel-Daim MM. Adipokines: potential therapeutic targets for vascular dysfunction in type II diabetes mellitus and obesity. J Diabetes Res. 2017;2017:1–11.
24. Blüher M. Adipokines–removing road blocks to obesity and diabetes therapy. Mol Metab. 2014;3(3):230–240. doi:10.1016/j.molmet.2014.01.005
25. Tilg H, Moschen AR. Adipocytokines: mediators linking adipose tissue, inflammation and immunity. Nat Rev Immunol. 2006;6(10):772–783. doi:10.1038/nri1937
26. Blüher M. Clinical relevance of adipokines. Diabetes Metab J. 2012;36(5):317–327. doi:10.4093/dmj.2012.36.5.317
27. Freitas Lima LC, Braga V, Do Socorro de França Silva M, et al. Adipokines, diabetes and atherosclerosis: an inflammatory association. Front Physiol. 2015;6:304. doi:10.3389/fphys.2015.00304
28. Cook KS, Groves DL, Min HY, Spiegelman BM. A developmentally regulated mRNA from 3T3 adipocytes encodes a novel serine protease homologue. Proc Natl Acad Sci. 1985;82(19):6480–6484. doi:10.1073/pnas.82.19.6480
29. Zhou Q, Ge Q, Ding Y, et al. Relationship between serum adipsin and the first phase of glucose‐stimulated insulin secretion in individuals with different glucose tolerance. J Diabetes Investig. 2018;9(5):1128–1134. doi:10.1111/jdi.12819
30. Lo JC, Ljubicic S, Leibiger B, et al. Adipsin is an adipokine that improves β cell function in diabetes. Cell. 2014;158(1):41–53. doi:10.1016/j.cell.2014.06.005
31. Gómez-Banoy N, Guseh JS, Li G, et al. Adipsin preserves beta cells in diabetic mice and associates with protection from type 2 diabetes in humans. Nat Med. 2019;25(11):1739–1747. doi:10.1038/s41591-019-0610-4
32. Baas T. Adipsin meets β cells. Sci Bus Exch. 2014;7(30):883–886. doi:10.1038/scibx.2014.883
33. Song N-J, Kim S, Jang B-H, et al. Small molecule-induced complement factor D (Adipsin) promotes lipid accumulation and adipocyte differentiation. PLoS One. 2016;11(9):e0162228. doi:10.1371/journal.pone.0162228
34. Legakis I, Mantzouridis T, Bouboulis G, Chrousos GP. Reciprocal changes of serum adispin and visfatin levels in patients with type 2 diabetes after an overnight fast. Arch Endocrinol Metab. 2016;60(1):76–78. doi:10.1590/2359-3997000000147
35. Karajibani M, Montazerifar F, Sadeghi MB, Keikhaie MA, Dashipour A. Serum fetuin-A and adipsin levels in type II diabetes patients. Int J High Risk Behav Addict. 2019;1–6.
36. Wang J-S, Lee W-J, Lee I-T, et al. Association between serum Adipsin levels and insulin resistance in subjects with various degrees of glucose intolerance. J Endocr Soc. 2019;3(2):403–410. doi:10.1210/js.2018-00359
37. Vasilenko MA, Kirienkova EV, Skuratovskaia DA, et al., editors. The role of production of adipsin and leptin in the development of insulin resistance in patients with abdominal obesity. Dokl Biochem Biophys. 2017;475:271–276. doi:10.1134/S160767291704010X
38. Kumar NP, Nair D, Banurekha V, et al. Type 2 diabetes mellitus coincident with pulmonary or latent tuberculosis results in modulation of adipocytokines. Cytokine. 2016;79:74–81. doi:10.1016/j.cyto.2015.12.026
39. Taşdemir E, Şermet A. The relationship between plasma adipsin, adiponectin, vaspin, visfatin, and leptin levels with glucose metabolism and diabetes parameters. Haydarpasa Numune Med J. 2019;59(2):95–103.
40. Klimontov VV, Bulumbaeva DM, Bgatova NP, et al. Serum adipokine concentrations in patients with type 2 diabetes: the relationships with distribution, hypertrophy and vascularization of subcutaneous adipose tissue. Diabetes mellitus. 2019;22(4):336–347. doi:10.14341/DM10129
41. Cox AJ, Zhang P, Bowden DW, et al. Enteroendocrine and adipokine associations with type 2 diabetes: phenotypic risk scoring approaches. J Gastroenterol Hepatol. 2018;33(7):1357–1364. doi:10.1111/jgh.14057
42. Derosa G, Fogari E, D’Angelo A, et al. Adipocytokine levels in obese and non-obese subjects: an observational study. Inflammation. 2013;36(4):914–920. doi:10.1007/s10753-013-9620-4
43. Azizi M, Tadibi V, Behpour N. The effect of aerobic exercise training on β-cell function and circulating levels of adipsin in community of obese women with type 2 diabetes mellitus. Int J Diabetes Dev Ctries. 2017;37(3):298–304. doi:10.1007/s13410-016-0504-7
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.