")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 12
Physical and Emotional Burden of Rheumatoid Arthritis in Saudi Arabia: An Exploratory Cross-Sectional Study
Authors Omair MA , Erdogan A, Tietz N , Alten R
Received 20 October 2020
Accepted for publication 9 December 2020
Published 24 December 2020 Volume 2020:12 Pages 337—345
DOI https://doi.org/10.2147/OARRR.S284734
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Mohammed A Omair,1 Alper Erdogan,2 Nicole Tietz,3 Rieke Alten4
1Division of Rheumatology, Department of Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2Medical Affairs Department, Eli Lilly and Company, Riyadh, Saudi Arabia; 3Eli Lilly and Company, Indianapolis, IN, USA; 4Schlosspark-Klinik University Medicine, Berlin, Germany
Correspondence: Rieke Alten
Schlosspark-Klinik University Medicine, Heubnerweg 2, Berlin 14059, Germany
Tel +49 30 3264-1325
Fax +49 30 3264-1324
Email [email protected]
Purpose: The aim of this study was to better understand the physical and emotional impacts of rheumatoid arthritis (RA) on the lives of patients in Saudi Arabia, and to determine whether there are any discrepancies between how healthcare providers (HCPs) perceive the feelings of patients with RA and how patients actually feel.
Patients and Methods: An online survey of adults with RA and HCPs was conducted in Saudi Arabia between January and June 2018. The survey used closed-ended questions with nominal and interval scales to cover relationships with others, ability to work and career progression, ability to perform normal activities, and aspirations for the future.
Results: In total, 85 patients and 24 HCPs were surveyed. Patients were more likely than HCPs to feel that the people around them understood the emotional and physical impacts of RA (emotional impact understood: 67% of patients vs 42% of HCPs; physical impact understood: 61% vs 38%, respectively). Additionally, a larger proportion of younger (aged < 40 years) than older patients (aged 40– 59 and ≥ 60 years) felt that these impacts were not understood by others. For patients, the greatest barrier to working was difficulty using hands (52% vs 41% of HCPs), whereas HCPs considered pain the greatest barrier (50% vs 38% of patients). Both patients (59%) and HCPs (81%) considered pain to be a common barrier to undertaking everyday activities. Regarding future aspirations, 40% of patients wished to accept their RA despite the barriers it caused.
Conclusion: Discrepancies between how HCPs perceived the feelings of patients with RA and how patients actually felt suggest that HCP–patient communication could be improved. This is the first study of its kind in Saudi Arabia and should help increase awareness of the difficulties and concerns of patients with RA in the Arabic world.
Keywords: burden of illness, surveys, rheumatologists, health personnel, patients, quality of life
Introduction
Rheumatoid arthritis (RA) is estimated to affect between 0.3% and 1% of the global population.1 Prevalence usually increases with age, and the disease is more common in women and developed countries.1,2 Information regarding the prevalence of RA in Saudi Arabia is limited. In a study of 5891 subjects in the Qassim region of the country in 1998, the prevalence of RA was 2.2 per 1000 people and, as in other countries, the disease was more common in women and with older age.3 However, as no recent or nationwide RA prevalence studies in Saudi Arabia have been published, the current prevalence of RA in the country is unknown. Globally, the age-standardized prevalence and incidence rates of RA are increasing each year.4
RA is a disabling disease that has both physical and psychological impacts on patients, leading to reduced health-related quality of life and a negative effect on the course of the disease.5,6 Despite this impact on the quality of life, a survey of rheumatologists in Saudi Arabia found that only 41% of respondents used tools to measure patient physical function and quality of life in daily clinical practice.7
Recent studies have highlighted the importance of understanding how the burden of disease affects each individual patient.8 Patient-reported outcomes (PROs) are important tools for healthcare providers (HCPs) as they aid in assessing a patient’s response to treatment8,9 and provide a more patient-centered approach to treatment.10 The importance of understanding patients’ perceptions was highlighted in a recent real-world study that found that three-quarters of patients with RA were unhappy with their treatment despite the majority having received biologic disease-modifying antirheumatic drugs.11 It is also important to obtain the views of both patients with RA and HCPs, as previous observations have shown that there can be discordance between rheumatologists and patients on disease severity and how to manage it.12,13
The majority of studies assessing PROs in patients with RA have been carried out in Western populations, and no published studies have yet explored the burden of RA in patients from Saudi Arabia. Therefore, we conducted a survey of patients with RA and HCPs in Saudi Arabia to better understand how the disease affects the lives of patients in this country from the perception of both patients and HCPs.
Patients and Methods
Survey Development and Survey Population
An online survey of adult patients (aged ≥18 years) with a diagnosis of RA and rheumatologists or HCPs involved in managing patients with the disease was conducted in Saudi Arabia between January 24 and June 4, 2018. The survey was developed by Weber Shandwick, a global public relations company, and Eli Lilly and Company with guidance from KRC Research, a global public opinion research consultancy commissioned by Eli Lilly and Company. The survey was carried out by KRC Research.
The survey design was informed by an exploratory survey among patients prior to the full survey. The full survey used closed-ended questions with nominal and interval scales comparable to those in a similar survey conducted among patients with RA and HCPs in selected European countries and Canada14 in 2017 as a part of Eli Lilly and Company’s RA Matters campaign. The current survey sample was procured through several channels, including social media, RA support groups, and the RA Matters website (https://www.ramatters.eu/). Patients were invited to participate through an RA support group, the Charitable Association of Rheumatic Diseases, and HCPs were contacted directly by KRC Research.
Respondents were screened prior to the full survey using a screener questionnaire, and only adults diagnosed with RA by a rheumatologist or HCP with experience in the management of RA were included in the study. Demographic information was also collected in the screening questionnaire. Patients and HCPs were not required to be directly paired. Patients and HCPs were provided with nearly identical surveys, except that HCPs were asked how they believed their patients were affected by RA. Both English and Arabic versions of questionnaires were available.
The study was conducted according to the Declaration of Helsinki as revised in Brazil in 2013 and was approved by the Institutional Review Board at King Saud University (Research Project no. E-20-5013). All subjects signed an electronic consent form prior to study participation.
Survey Details
The survey contained 41 questions and took respondents an average of 11 minutes to complete. It explored four aspects of patients’ lives: (i) relationships with others, (ii) ability to work and career progression, (iii) ability to perform normal activities, and (iv) aspirations for the future. We also examined the differences between patient and HCP perceptions of how RA affects patients and the relationship between social support structures for patients and their outlook on living with RA.
The impact of RA on patients’ relationships with others included aspects such as effect on personal relationships (children, colleagues, friends, spouse/partner, other family), ability to interact with their children, trust in others, ability to relate to others, quality of time spent with their children, inclusion in family or social events, and intimacy with a partner. Patients’ career progression and level of support in the workplace were explored by questions about the flexibility of and physical and emotional support from work colleagues. The questionnaire also examined the obstacles and difficulties patients experienced in the workplace, including difficulty using hands, pain, fatigue, stress, reliance on others, fluctuation and unpredictability of disease, and ability to get to and from work.
The effects of RA on, and barriers to undertaking, normal activities were examined using questions about difficulties in exercising, carrying out housework, socializing, washing/personal grooming, and sex and intimacy. The impact of RA on patients’ perspectives for the future was examined with regards to how people around them viewed their disease and which activities were more important for patients, including going out with friends, everyday activities in the home, taking a holiday, exercising, and having an intimate relationship.
Analyses
Not all patients and HCPs answered all of the questions. Categorical data were therefore presented as percentages of participants, calculated using the number of observations with non-missing values as the denominator (unless noted otherwise). All analyses were descriptive; no formal statistical comparisons were performed. The study is reported according to Strengthening the Reporting of Observational studies in Epidemiology (STROBE) recommendations for the reporting of observational studies.15
Results
Respondent Demographics
A total of 85 patients and 24 HCPs participated in the survey. Of the 85 patients, 51 were female (60%), and the mean patient age (± standard deviation) was 46.0 ± 10.0 years; 68 patients (80%) were aged >40 years. The mean time since diagnosis of RA was 7.7 ± 7.5 years, and the time since diagnosis was <5 years for 42 patients (49%). For HCPs, the sex ratio was 50:50 female to male, and the mean age was 45.6 ± 10.0 years (Table 1).
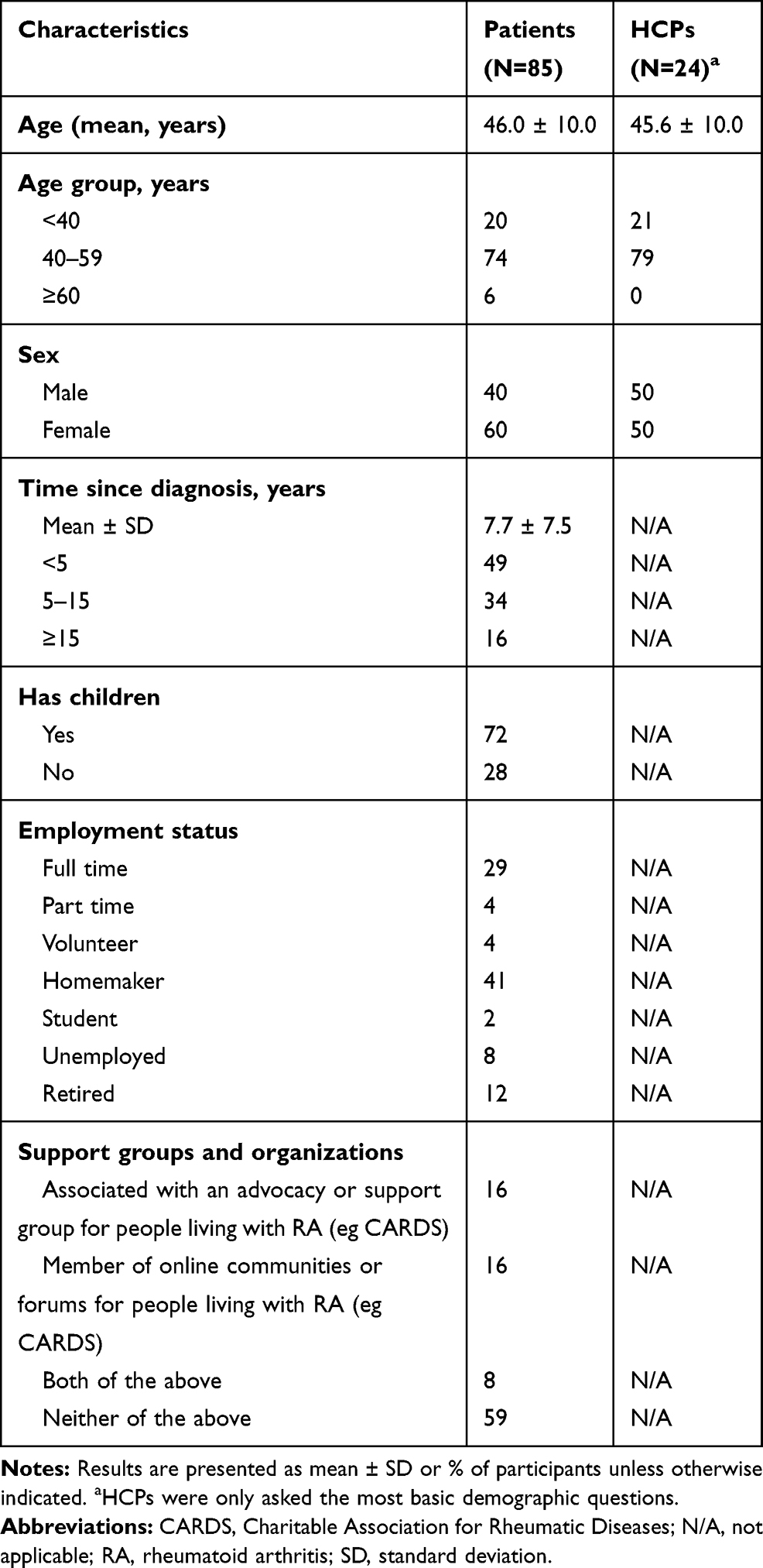 |
Table 1 Demographic Characteristics of Survey Participants |
Effect of RA on Relationships
Of participating patients, 57 (67%) felt that the people around them understood the emotional impact of RA, compared with 10 HCPs (42%) (Figure 1A). For patients aged <40 years, 41% considered the emotional impact of RA on their lives to be understood, compared with 71% of those aged 40–59 years and 100% of those aged ≥60 years (Figure 1B). In total, 52 patients (61%) and 9 HCPs (38%) felt the people around them understood the physical impact of RA (Figure 1A). As with emotional impact, younger patients were more likely than older patients to perceive that the physical impact of RA was not understood by others (Figure 1B).
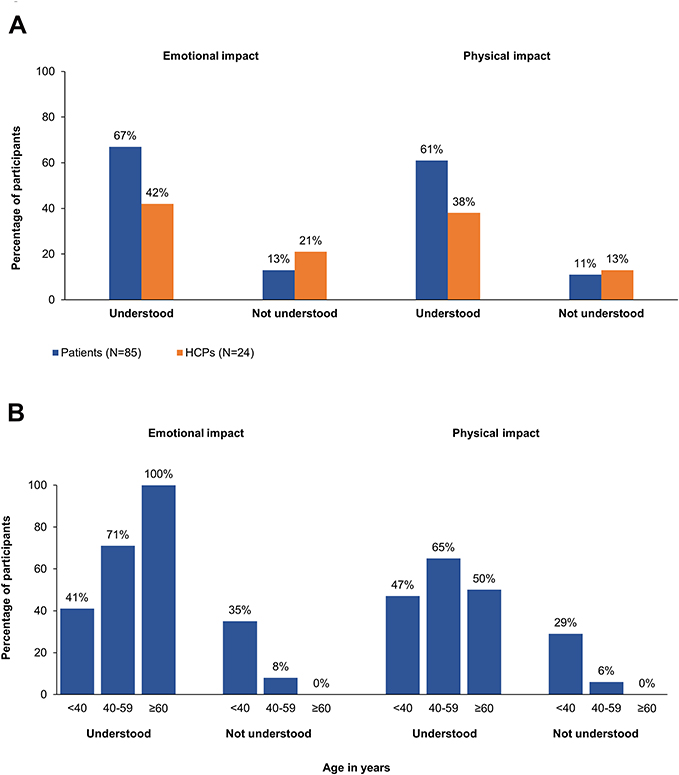 |
Figure 1 Perceived understanding of the impact of rheumatoid arthritis (RA) by others according to (A) patients and healthcare providers (HCPs) and (B) patient age group based on answers to the following survey questions: (Q14) How well do you think people in your life understand the emotional impact that RA has on your life? (Q27) How well do you think people understand the emotional impact that RA has on patients’ lives? (Q15) How well do you think people in your life understand the physical impact that RA has on your life? (Q28) How well do you think people understand the physical impact that RA has on patients’ lives?. |
There were no clear trends towards a perceived positive or negative impact of RA on personal relationships, including the ability to interact with their children, trust in others, ability to relate to others, and quality of time spent with others. However, responses from HCPs and patients differed regarding the effect of RA on inclusion in family or social events and intimacy with a partner: a majority of HCPs (12/22 [55%] and 9/22 [41%], respectively) felt that RA had a positive effect (as opposed to a neutral or negative effect) on these aspects, whereas lower proportions of patients considered this to be the case (31/83 [37%] and 29/84 [35%], respectively) (Supplementary Figure 1).
Effect of RA on Work
In total, 36 (42%) patients reported that they did not work, and two patients (2%) reported that their RA had forced them to take long-term leave or to retire (Figure 2). RA was perceived to have led to a slowing of career progression by 22 patients (26%), equivalent to 45% (22/49) of all working patients. The majority of patients felt they were getting adequate physical and emotional support in the workplace (24/32 [75%] and 22/32 [69%] patients, respectively), whereas physicians were more neutral regarding adequate physical and emotional support in the workplace (9/20 [45%] and 8/20 [40%] HCPs, respectively) (Supplementary Figure 2).
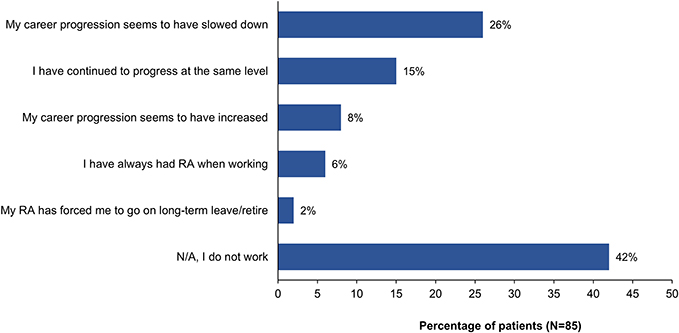 |
Figure 2 Perceived effect of rheumatoid arthritis (RA) on work according to patients based on their answer to question 16 of the survey: In what way has your career progression changed since being diagnosed with RA? N/A, not applicable. |
In total, 43 of 82 patients (52%) described difficulty in using their hands as the greatest barrier to work, followed by emotional stress (39 [48%]), pain (31 [38%]), and fatigue (31 [38%]). Conversely, HCPs felt pain was the greatest obstacle to work (11/22 [50%]), followed by emotional stress (10/22 [45%]), fluctuation of the disease (10/22 [45%]), difficulty using hands (9/22 [41%]), and ability to get to and from work (9/22 [41%]) (Supplementary Figure 3). Difficulty using hands was the greatest obstacle to working among females (67%) but not among males (30%); for males, the most frequently reported obstacle to working was emotional stress (70 vs 33% for females) (Supplementary Figure 4).
Effect of RA on Everyday Activities
Pain was considered one of the most common barriers to undertaking everyday activities, by 50/85 patients (59%) and 17/21 HCPs (81%). Fatigue and aching/stiff joints were also commonly perceived as a barrier. Difficulty using hands was considered almost equally important by patients and HCPs, whereas emotional stress related to RA and lack of self-confidence were more commonly reported as a barrier by patients (Figure 3).
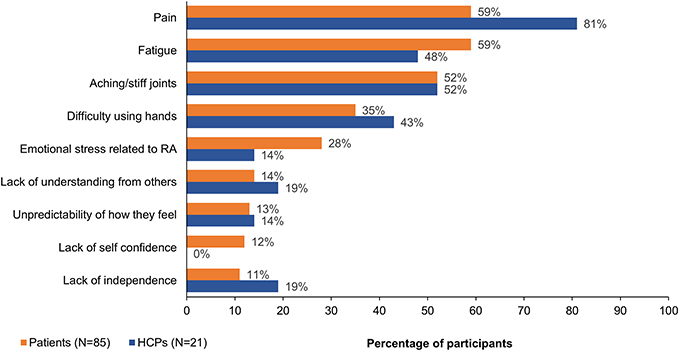 |
Figure 3 Barriers to undertaking everyday activities from the perspective of patients with rheumatoid arthritis (RA) and healthcare providers (HCPs) based on answers to the following questions: (Q20) Which aspects of your RA create the biggest barriers to your undertaking these activities? (Q33) Which aspects of living with RA create the biggest barriers to undertaking these activities for your patients?. |
The most common everyday activities cited as difficult to perform were exercise (35/83 patients [42%]; 6/21 HCPs [29%]) and housework (19/83 [23%]; 13/22 [59%], respectively). The impact of RA was perceived as greater by HCPs than patients on sex and intimacy (8/20 [40%] vs 10/81 [12%], respectively) and washing/personal grooming (8/21 [38%] vs 8/82 [10%], respectively) (Supplementary Figure 5). Patients most commonly reported feeling anxious (50/85 [59%]) or frustrated (27/85 [32%]) about being unable to accomplish tasks because of RA, whereas HCPs cited anxiety (9/22 [41%]), isolation (9/22 [41%]), and frustration (8/22 [36%]) as being the most likely feelings.
Effect of RA on Aspirations
When asked how they would like to feel about RA in the future, 34 of 85 patients (40%) responded that they would like to accept their RA despite the barriers it caused, whereas 17 (20%) felt that RA was part of who they were, and 17 (20%) hoped to live their lives in the same way as those without RA. A further 14 patients (16%) recognized that RA hindered their lives but accepted it, and only 3 (4%) could not accept having the disease.
Patients most commonly reported hoping that people in their lives would better understand the emotional impact of RA (41/83 [49%]), but this was highlighted by only 6/23 HCPs (26%) (Figure 4). HCPs considered the aspiration most likely to be chosen by patients was that people in their lives would better understand the physical impact of RA (14/23 [61%]), but only 28/83 patients (34%) cited this aspiration. In addition, 13/23 HCPs (57%) believed that patients hoped their doctor would take more interest in what they considered to be important with respect to their treatment, whereas only 21/83 patients (25%) reported this aspiration.
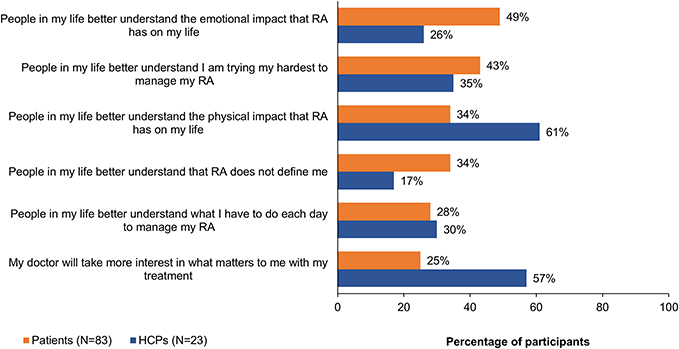 |
Figure 4 Patient aspirations for the future from the perspective of patients with rheumatoid arthritis (RA) and healthcare providers (HCPs) based on answers to the following survey questions: (Q23) In the future, I wish that …. (Q36) Which of the following do you believe is most important to people living with RA for the future? (Respondents were directed to select up to three options.). |
The most important activity for patients was being able to go out with friends (54/81 patients [67%] vs 10/22 HCPs [45%]), whereas HCPs considered taking a holiday to be most important (15/21 HCPs [71%] vs 49/80 patients [61%]). The greatest discordance between patients and HCPs was for performing everyday activities in the home (52/83 [63%] vs 7/23 [30%], respectively) and having an intimate relationship (45/83 [54%] vs 3/20 [15%], respectively).
Discussion
Results of this survey in Saudi Arabia indicate that RA has a considerable impact on many aspects of patients’ lives, including relationships, ability to work and career progression, and daily activities. Both patients and HCPs perceived that people without RA have an understanding of the emotional and physical impact of the disease on patients. However, this perception was less common among younger patients. Nearly half of the patients did not work. Many working patients noted a slowing of career progression, despite patients and—to some extent—HCPs reporting that patients felt supported by colleagues in the workplace. Outside of employment, exercising and housework were the most difficult everyday activities to perform. Patients experienced considerable anxiety as a result of RA hindering their ability to perform everyday activities. Aspirations for a future with RA were modest, with patients hoping that the people in their lives would better understand the emotional impact of the disease on their lives.
To understand how RA impacts on patient relationships, the RA Matters survey included questions about how interactions between patients and the people in their lives had changed since their RA diagnosis. In the current study, there were no clear trends towards a perceived positive or negative impact of RA on personal relationships. Indeed, the negative impact of RA on intimacy with a partner appeared less pronounced in the current study than in the European/Canadian survey,14 in which 48% of patients and 78% of HCPs felt the disease had a negative impact on this aspect of relationships (compared with 31% and 14%, respectively, in the current study). A similar proportion of patients in both surveys (44% in the European/Canadian survey, 45% in the current study) felt that RA had a negative impact on inclusion in family and social events, whereas a larger proportion of HCPs in the European/Canadian study (68%) felt this to be the case (compared with 32% in the current study).
It is well documented that many patients with RA have difficulty in continuing to work due to complications from the disease, with 27%–47% of patients unable to stay in full-time employment due to RA within approximately 20 years of disease onset.16 In this study, we sought to quantify how RA impacts on the ability of patients to work in Saudi Arabia. Almost half of the patients were not working at the time of completing the questionnaire, and more than one-quarter felt that RA had slowed their career progression; this is slightly higher than career progression results in the European/Canadian survey,14 in which 23% of patients felt that their careers had slowed since their RA diagnosis. This could be partially explained by cultural differences between Arabic and Western countries in terms of attitudes towards women who work. The high proportion of patients who did not work in the current survey is of note, as the ability to work is recognized as an important treatment target in Saudi Arabia.17
In our study, both patients and HCPs felt that colleagues were fairly accommodating in the workplace. These results contrast with the perceived lack of adequate physical or emotional support from colleagues by patients in Europe and Canada.14 The most common obstacles to working for patients with RA in Saudi Arabia were difficulty using hands (52%) and emotional stress (48%). Similar to the current study, the European/Canadian study14 found that difficulty using hands was also the greatest barrier, but pain and the unpredictability of how well patients would feel were also important (44%, 43%, and 34% of patients, respectively). Interestingly, responses from HCPs in the present study indicated that they considered pain, emotional stress, and disease fluctuation as the greatest barriers in the workplace, which is similar to the views of patients in the European/Canadian study.14
The burden of RA on patients is not limited to physical impacts. The psychological impact of the disease is also important as it has a negative effect on the course of the disease.18 However, physician–patient communications have traditionally focused on symptoms and treatment rather than on impact on the quality of life.10,19 Furthermore, two patient surveys conducted in the USA, Canada, and Europe found that patients with RA felt unable to effectively communicate with their HCP about their condition and treatment goals.20
The physical and emotional challenges of living with RA can make everyday activities difficult, so our study also explored these challenges. Similar to findings in the European/Canadian study,14 the physical effects of RA, such as pain, fatigue, and aching/stiff joints, were perceived by patients and HCPs as the primary barriers to undertaking activities, particularly exercising. Interestingly, the perception of how RA affects the ability to carry out housework differed greatly between patients and HCPs, with 59% of HCPs and only 23% of patients considering this activity difficult. As previously reported,14 inability to undertake or complete activities led to patients feeling anxious and frustrated.
Patients’ feelings about the future can offer insight into the deeper impact of living with RA. Our study showed that patients had only modest aspirations for a future with RA. In total, 40% of patients felt that they would like to accept their RA despite the barriers it caused, and 20% would like to live their lives in the same way as people without RA. Similarly, in the European/Canadian study,14 57% of patients reported that they would like to accept their life with RA and be able to cope with it in the future.
Despite a large proportion of patients feeling that the people around them understood the emotional impact of RA, nearly half hoped that this understanding would improve. This discrepancy may be due to a low patient expectation of the level of understanding of the impact of RA by the people around them. In contrast, HCPs more commonly believed that patients hoped for a better understanding of the physical impact of RA and that their physician would show more interest in their treatment. Understanding the physical impact of RA was perceived as an important aspiration by 61% of HCPs but only 34% of patients; this compared with 43% for patients in the European/Canadian study.14 Being able to go out with friends and accomplish everyday activities at home were important for patients, whereas HCPs perceived taking a holiday as a major aspiration, which is in line with patient results in the European/Canadian study.14 A recent multinational survey highlighted discrepancies between the views of patients with RA and HCPs, reporting that 90% of physicians were satisfied with their treatment-related communications with their patients but that 61% of patients were uncomfortable raising concerns or fears with their physician. Inadequate HCP–patient communication may explain the discrepancies between the views of patients and HCPs in our study, suggesting that improved communication could lead to improved management of RA.21
It is important to emphasize the relevance of the location of this study. Currently available PRO data for RA come from studies performed in Western populations; little is known about the impact of RA on patients’ lives in Saudi Arabia, yet patients’ perception of disease can be influenced by cultural differences. For example, in a cross-cultural study of pain intensity in patients with RA, Egyptian women reported worse pain, disease activity and physical function than Dutch women, despite having similar disease severity according to clinical measurements.22 The COMORA study, which evaluated patients with RA from 17 different countries, found that levels of fatigue varied between countries, and the proportion of patients with severe fatigue ranged from 14% in Venezuela to 65% in Egypt. This variation was partly explained by subjective outcomes but not by objective disease outcomes.23 Furthermore, work outcomes varied between countries, with patients in Morocco having the lowest odds of being employed (vs German patients) and the highest odds of absenteeism (vs Japanese patients).24 These studies highlight that patients from different cultures may assess the importance of specific health domains and their impact on the quality of life in different ways.
This study is limited by the small number of participants, particularly HCPs. Survey participants had to be literate (both with computers and in general) and available to participate in the survey; therefore, the survey may not be fully representative of patients with RA in Saudi Arabia. A previous study of patients with RA in Saudi Arabia found that 30% (53/185) of patients were illiterate.25 The current study was descriptive and did not include any formal statistical comparisons. Additionally, no information was collected on disease severity or patient comorbidities, which could have affected the results. In general, surveys are limited by the subjective nature of participants’ answers and by the possibility that participants may not necessarily have provided honest answers.
In conclusion, this survey of patients with RA and HCPs in Saudi Arabia found that patients and HCPs perceived that people without RA understand the emotional and physical impacts of RA. Most patients either did not work or had experienced a slowing of career progression due to the disease. Ability to perform everyday activities was also affected, which caused patients anxiety. Patients had modest aspirations for the future, their greatest hope being that the emotional impact of RA would be better understood. This study is the first of its kind in Saudi Arabia and should help to increase awareness of the difficulties and concerns of those living with RA in the Arabic world. There is a clear discrepancy in how HCPs in Saudi Arabia perceive patients’ feelings and how patients actually feel, indicating that HCP–patient communication could be improved. The findings of the survey require confirmation in a larger patient population and need to be evaluated in relation to disease activity and disability.
Abbreviations
HCP, healthcare provider; PRO, patient-reported outcome; RA, rheumatoid arthritis; STROBE, Strengthening the Reporting of Observational studies in Epidemiology.
Acknowledgments
The authors thank the patients and HCPs who participated in this survey, the Charitable Association for Rheumatic Diseases for its role in recruiting patients, and the personnel from KRC Research for conducting the survey. The authors also acknowledge Dr Lizeth Lacharme and Dr Sue Chambers (Rx Communications, Mold, UK) for medical writing assistance with the preparation of this manuscript, funded by Eli Lilly and Company. This study was funded by Eli Lilly and Company (Indianapolis, IN, USA).
Author Contributions
All authors made substantial contributions to the conception and design of the study, acquisition of data, or analysis and interpretation of data; participated in drafting the article or critically revising it for important intellectual content; agreed on submission to the current journal; gave final approval for the current version to be published; and agree to be accountable for all aspects of the work.
Disclosure
Mohammed A. Omair has received speaker’s fees/grants from Abbvie, Actelion, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, GlaxoSmithKline, Hekma, Janssen, New Bridge, Novartis, Pfizer, and Roche. Alper Erdogan is an employee and shareholder of Eli Lilly and Company, Riyadh, Saudi Arabia. Nicole Tietz is an employee and shareholder of Eli Lilly and Company, Indianapolis, IN, USA. Rieke Alten has received research grants and consultancy fees from Abbvie, BMS, Eli Lilly and Company, Gilead, Galapagos, Janssen, Pfizer and UCB. The authors report no other conflicts of interest in this work.
References
1. World Health Organization [internet]. Chronic rheumatic conditions; 2020. Available from: https://www.who.int/chp/topics/rheumatic/en/.
2. Hunter TM, Boytsov NN, Zhang X, et al. Prevalence of rheumatoid arthritis in the United States adult population in healthcare claims databases, 2004–2014. Rheumatol Int. 2017;37(9):1551–1557. doi:10.1007/s00296-017-3726-1
3. Al-Dalaan A, Al Ballaa S, Bahabri S, et al. The prevalence of rheumatoid arthritis in the Qassim region of Saudi Arabia. Ann Saudi Med. 1998;18(5):396–397. doi:10.5144/0256-4947.1998.396
4. Safiri S, Kolahi AA, Hoy D, et al. Global, regional and national burden of rheumatoid arthritis 1990–2017: a systematic analysis of the Global Burden of Disease study 2017. Ann Rheum Dis. 2019;78(11):1463–1471. doi:10.1136/annrheumdis-2019-215920
5. Bertin P, Fagnani F, Duburcq A, et al. Impact of rheumatoid arthritis on career progression, productivity, and employability: the PRET Study. Joint Bone Spine. 2016;83(1):47–52. doi:10.1016/j.jbspin.2015.05.001
6. Malm K, Bergman S, Andersson MLE, et al. Quality of life in patients with established rheumatoid arthritis: a phenomenographic study. SAGE Open Med. 2017;5:2050312117713647. doi:10.1177/2050312117713647
7. Omair MA, Omair MA, Halabi H. Survey on management strategies of rheumatoid arthritis in Saudi Arabia: a Saudi Society for Rheumatology initiative. Int J Rheum Dis. 2017;20(9):1185–1192. doi:10.1111/1756-185X.12735
8. Her M, Kavanaugh A. Patient-reported outcomes in rheumatoid arthritis. Curr Opin Rheumatol. 2012;24(3):327–334. doi:10.1097/BOR.0b013e3283521c64
9. van Tuyl LHD, Michaud K. Patient-reported outcomes in rheumatoid arthritis. Rheum Dis Clin North Am. 2016;42(2):219–237. doi:10.1016/j.rdc.2016.01.010
10. Fautrel B, Alten R, Kirkham B, et al. Call for action: how to improve use of patient-reported outcomes to guide clinical decision making in rheumatoid arthritis. Rheumatol Int. 2018;38:935–947.
11. Radawski C, Genovese MC, Hauber B, et al. Patient perceptions of unmet medical need in rheumatoid arthritis: a cross-sectional survey in the USA. Rheumatol Ther. 2019;6(3):461–471. doi:10.1007/s40744-019-00168-5
12. Nash N, Nicholls D. Perceptions of methotrexate use in rheumatoid arthritis by rheumatologists and their patients: an Australian survey study. Int J Rheum Dis. 2013;16:652–661.
13. Khan NA, Spencer HJ, Abda E, et al. Determinants of discordance in patients’ and physicians’ rating of rheumatoid arthritis disease activity. Arthritis Care Res. 2012;64(2):206–214. doi:10.1002/acr.20685
14. Alten R, van de Laar M, De Leonardis F, et al. Physical and emotional burden of rheumatoid arthritis: data from RA Matters, a web-based survey of patients and healthcare professionals. Rheumatol Ther. 2019;6:587–597.
15. von Elm E, Altman DG, Egger M, et al, STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
16. Nikiphorou E, Guh D, Bansback N, et al. Work disability rates in RA. Results from an inception cohort with 24 years follow-up. Rheumatology. 2012;51(2):385–392. doi:10.1093/rheumatology/ker401
17. Almoallim HM, Alharbi LA. Rheumatoid arthritis in Saudi Arabia. Saudi Med J. 2014;35:1442–1454.
18. Yilmaz V, Umay E, Gündoğdu I, et al. Rheumatoid arthritis: are psychological factors effective in disease flare? Eur J Rheumatol. 2017;4(2):127–132. doi:10.5152/eurjrheum.2017.16100
19. McInnes I, Combe B, Burmester G. Understanding the patient perspective – results of the Rheumatoid Arthritis: Insights, Strategies & Expectations (RAISE) patient needs survey. Clin Exp Rheumatol. 2013;31:350–357.
20. Strand V, Wright GC, Bergman MJ, et al. Patient expectations and perceptions of goal-setting strategies for disease management in rheumatoid arthritis. J Rheumatol. 2015;42(11):2046–2054. doi:10.3899/jrheum.140976
21. Gibofsky A, Galloway J, Kekow J, et al. Comparison of patient and physician perspectives in the management of rheumatoid arthritis: results from global physician- and patient-based surveys. Health Qual Life Outcomes. 2018;16(1):211. doi:10.1186/s12955-018-1035-3
22. Vlaar APJ, Ten Klooster PM, Taal E, et al. A cross-cultural study of pain intensity in Egyptian and Dutch women with rheumatoid arthritis. J Pain. 2007;8(9):730–736. doi:10.1016/j.jpain.2007.05.003
23. Hifinger M, Putrik P, Ramiro S, et al. In rheumatoid arthritis, country of residence has an important influence on fatigue: results from the multinational COMORA study. Rheumatology. 2016;55:735–744.
24. van der Zee-neuen A, Putrik P, Ramiro S, et al. Large country differences in work outcomes in patients with RA – an analysis in the multinational study COMORA. Arthritis Res Ther. 2017;19(1):216. doi:10.1186/s13075-017-1421-y
25. Albaqami J, Alshalhoub R, Almalag H, et al. Prevalence of methotrexate intolerance among patients with rheumatoid arthritis using the Arabic version of the methotrexate intolerance severity score. Int J Rheum Dis. 2019;22(8):1572–1577. doi:10.1111/1756-185X.13637
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.