")
Back to Journals » Drug Design, Development and Therapy » Volume 10
Pharmacokinetics of the evogliptin/metformin extended-release (5/1,000 mg) fixed-dose combination formulation compared to the corresponding loose combination, and food effect in healthy subjects
Authors Rhee S, Lee S , Yoon SH, Cho J , Jang I , Yu K
Received 14 December 2015
Accepted for publication 1 March 2016
Published 13 April 2016 Volume 2016:10 Pages 1411—1418
DOI https://doi.org/10.2147/DDDT.S102459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Wei Duan
Su-jin Rhee,1,* SeungHwan Lee,1,2,* Seo Hyun Yoon,1 Joo-Youn Cho,1 In-Jin Jang,1 Kyung-Sang Yu1
1Department of Clinical Pharmacology and Therapeutics, Seoul National University College of Medicine and Hospital, 2Clinical Trials Center, Seoul National University Hospital, Seoul, Republic of Korea
*These authors contributed equally to this work
Abstract: A new fixed-dose combination formulation of evogliptin 5 mg and metformin extended-release (XR) 1,000 mg (FDC_EVO5/MET1000) was developed to improve medication adherence for type 2 diabetes mellitus. The pharmacokinetics of FDC_EVO5/MET1000 was compared to the corresponding loose combination in a randomized, open-label, crossover study in 36 healthy male subjects (Part 1), and the food effect on FDC_EVO5/MET1000 was assessed (under fasted or fed conditions) in a randomized, open-label, crossover study in 28 healthy male subjects (Part 2). Serial blood samples for pharmacokinetic analysis were collected up to 72 hours, and pharmacokinetic parameters of evogliptin and metformin were calculated using non-compartmental methods. The geometric mean ratios (fixed-dose combination to loose combination) and 90% confidence intervals of pharmacokinetic parameters for evogliptin and metformin were all within 0.800–1.250, suggesting bioequivalent pharmacokinetic. After a single oral dose of FDC_EVO5/MET1000, food did not significantly affect evogliptin pharmacokinetic while systemic exposure of metformin was increased about 47.5% under the fed condition, which is consistent with the already established food effect on metformin XR. FDC_EVO5/MET1000 was generally well tolerated without any drug-related serious adverse events. In conclusion, FDC_EVO5/MET1000 can be substituted for the loose combination of FDC_EVO5/MET1000, providing better compliance with convenient administration.
Keywords: pharmacokinetics, bioequivalence, food effect, fixed-dose combination, evogliptin, metformin XR
Introduction
Type 2 diabetes, which is also referred to as non-insulin-dependent diabetes, accounts for more than 90% of patients with diabetes.1 The treatment guidelines for type 2 diabetes recommend metformin as the first-line therapy, followed by adding second-line agents to metformin for patients with insufficient control of hyperglycemia.2,3 Among the add-on agents, DPP-4 inhibitors are a relatively new and expanding class of treatment option.
DPP-4 inhibitors improve glycemic control mainly via stimulation of glucose-mediated incretin secretion, resulting in increased insulin secretion and decreased glucagon release.4 This glucose-dependent mechanism of DPP-4 inhibitor suggests a lower risk for hypoglycemia. Furthermore, DPP-4 inhibitor has been reported to positively affect metabolic abnormalities such as obesity, hypertension, and dyslipidemia, which are associated with type 2 diabetes.5 Currently, several DPP-4 inhibitors, including sitagliptin, vildagliptin, and saxagliptin, are used for treatment of type 2 diabetes.
Evogliptin, a novel oral DPP-4 inhibitor, was recently developed for treatment of type 2 diabetes. Following a single administration in healthy volunteers, evogliptin showed a long half-life (≥30 hours), and the pharmacokinetics of evogliptin was not affected by food.6 In a multiple-dosing study, evogliptin exhibited linear pharmacokinetics within the 5–20 mg dose range, and the inhibitory effect on DPP-4 activity was sustained over 24 hours in healthy volunteers.7 In patients with type 2 diabetes mellitus, once-daily administration of evogliptin 5 mg for 12 weeks showed significant glucose-lowering effects, resulting in the reduction of the mean HbA1c by 0.57% compared with the placebo, which is comparable to results with other DPP-4 inhibitors such as sitagliptin 100 mg (0.55%) and vildagliptin 100 mg (0.53%).8
Evogliptin is expected to be used as the add-on agent to metformin; therefore, the fixed-dose combination (FDC) formulation of evogliptin and metformin might increase therapeutic success by improving medication adherence compared with taking two individual component tablets. Indeed, the use of FDC formulations of two or more therapeutic agents with complementary mechanisms of action has been increasing in the clinical setting, and some studies have shown that FDCs are more effective than concomitant administration of individual components.9–11
Based on this understanding, a novel FDC formulation of evogliptin 5 mg and metformin extended-release (XR) 1,000 mg (FDC_EVO5/MET1000) has been developed with the expectation of improving patient adherence through once daily, one-pill dosing. This study aimed to compare the pharmacokinetics of evogliptin and metformin, administered as FDC_EVO5/MET1000 (evogliptin 5 mg/metformin XR 1,000 mg FDC formulation) or administered in corresponding doses as individual tablets. In addition, this study also aimed to evaluate the effect of food on the pharmacokinetics of FDC_EVO5/MET1000.
Materials and methods
Subjects and treatments
The study protocol was approved by the Institutional Review Board of Seoul National University Hospital (ClinicalTrials.gov registry no.: NCT02167061). Written informed consent was obtained before any study-related procedure was performed, and the study was conducted in accordance with the major ethical principles stipulated in the Declaration of Helsinki and Good Clinical Practice guidelines.
This clinical trial consisted of two independent studies, one a comparative pharmacokinetic study (Part 1), and the other a food effect study (Part 2). Each study had a randomized, open-label, single dose, two-period, two-sequence, two-treatment crossover design. Healthy male subjects were included who were 20–45 years of age, weighed at least 55 kg, and had a body mass index (BMI) of 18–27 kg/m2, with a fasting plasma glucose concentration of 60–125 mg/dL at screening. Subjects had to present no clinically significant abnormalities based on medical history, physical examination, and clinical laboratory tests, performed within 3 weeks before the first administration of the study drugs. A total of 64 subjects who met the screening criteria were admitted to the Clinical Trials Center at Seoul National University Hospital for 5 days in each period, with a 14-day washout between the two adjacent periods. The washout period was over seven-fold longer than the previously reported terminal half-lives for both evogliptin and metformin XR.6,9
In Part 1, a total of 36 subjects were randomized to two treatment sequences, in which the treatments consisted of a single oral dose of FDC_EVO5/MET1000 or a co-administration of the individual products of evogliptin 5 mg and metformin XR 1,000 mg (EVO+MET): Sequence A, FDC_EVO5/MET1000 followed by EVO+MET; and Sequence B, EVO+MET followed by FDC_EVO5/MET1000 (Figure 1). Each study drug, according to the assigned sequence, was administered under fasting conditions along with 240 mL of water. Food was restricted from 10 hours pre-dose until 4 hours post-dose, and water was not permitted from 1 hour before dosing until 2 hours following dosing.
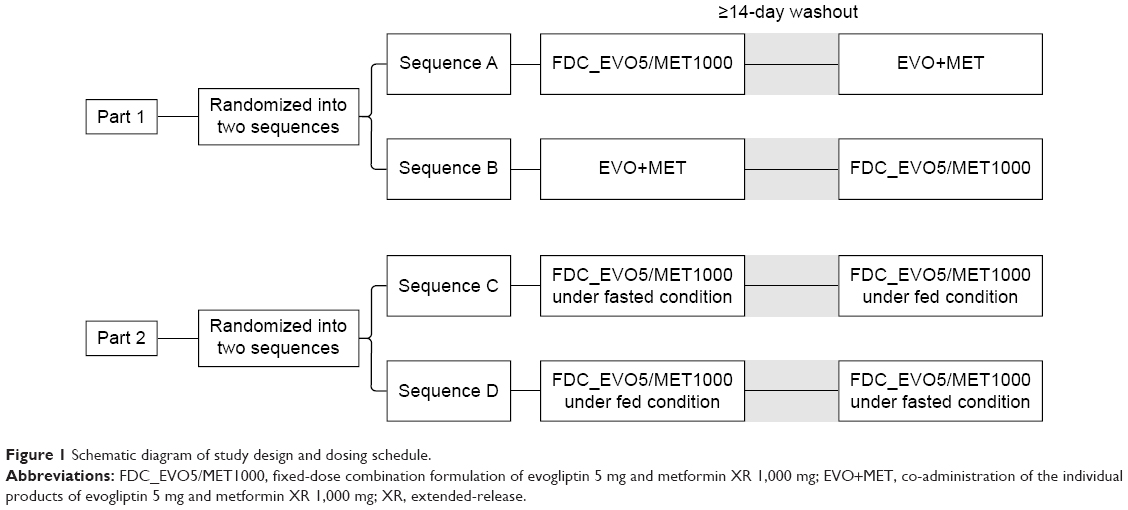 | Figure 1 Schematic diagram of study design and dosing schedule. |
In Part 2, a total of 28 subjects were randomly assigned to two treatment sequences and received a single oral dose of FDC_EVO5/MET1000 under fasted or fed conditions: sequence C, fasted condition followed by fed condition; and Sequence D, fed condition followed by fasted condition (Figure 1). For the treatment under the fasted condition, subjects fasted for 10 hours before the dose and until 4 hours after the dose. For treatment under the fed condition, subjects consumed a high-fat breakfast containing ≥900 kcal with ≥35% of calories from fat 30 minutes prior to study drug administration, according to Korean Ministry of Food and Drug Safety (MFDS) guidelines regarding food effect bioavailability of a sustained-release drug.12 The study drug was administered with 240 mL water in both treatments. No food or water was allowed for 2 hours after drug administration. Furthermore, subjects were prohibited from consuming any food.
Blood sample collection
Blood samples for determining the plasma concentration of evogliptin and metformin were collected up to 72 hours after the dose in each period: 0 (pre-dose) and 1, 2, 3, 4, 5, 6, 7, 8, 10, 12, 15, 24, 36, 48, 60, and 72 hours post-dose. The collected samples were centrifuged at 3,000 rpm and 4°C for 10 minutes, and the obtained plasma samples were frozen at below −70°C until assayed.
Determination of plasma drug concentration
Plasma concentrations of evogliptin and metformin were determined by a validated liquid chromatography (Agilent 1260 series; Agilent Technologies, Santa Clara, CA, USA) coupled with a tandem mass spectrometry method (Agilent 6490 Quadrupole for evogliptin and Agilent 6460 Quadrupole for metformin, Agilent Technologies). Chromatographic separation was performed under gradient conditions using a Venusil ASB C8 column (50.0×2.1 mm, 3 μm; Agela, Wilmington, DE, USA) for evogliptin and using a Kinetex HILIC 100 Å column (hydrophilic interaction liquid chromatography column; 100.0×2.1 mm, 2.6 μm; Phenomenex, Torrance, CA, USA) for metformin. The calibration curves were linear over the range of 0.5–50 μg/L for evogliptin and 10–3,000 μg/L for metformin (r2≥0.9957 and r2≥0.9982, respectively). The accuracy range was 97.81%–104.30% for evogliptin and 90.13%–105.30% for metformin. The precision coefficients of variation were ≤7.004% for evogliptin and ≤5.036% for metformin.
Pharmacokinetic analysis
The following pharmacokinetic parameters were calculated by non-compartmental methods using Phoenix WinNonlin software version 6.3 (Certara, St Louis, MO, USA). The maximum concentration (Cmax) and the time to reach Cmax (tmax) were obtained directly from the observed values. The area under the concentration-time curve (AUC) was determined using the linear trapezoidal method for ascending concentrations and the log trapezoidal method for descending concentration. The AUC from the last dosing time extrapolated to infinity (AUCinf) was calculated as:
AUClast + Clast/λz, | (1) |
where AUClast is the AUC from the time of last dosing to the last measurable concentration, Clast is the last measurable concentration, and λz is the terminal elimination rate constant estimated from a regression line of log-transformed plasma concentrations versus time over the terminal log-linear portion. The apparent clearance (CL/F) was calculated as a single dose divided by AUCinf. The terminal elimination half-life (t1/2) was calculated as the natural logarithm of 2 divided by λz.
Safety assessment
Tolerability and safety were evaluated throughout the study based on physical examinations, vital signs, 12-lead electrocardiograms, and clinical laboratory tests, including hematology, serum chemistry, and urinalysis. Subjects were instructed to inform the study physician and/or nurses of any adverse events (AEs) that occurred during the study. Any AE reported by the subjects was recorded throughout the entire period, and the investigators determined its relationship to the treatment.
Statistical analysis
The sample size for this study was determined by assuming the highest intrasubject variability of 23% for both evogliptin and metformin.6,9 A sample size ≥32 was estimated to have power ≥90%, and a sample size ≥24 was estimated to have power ≥80% at a 5% significance level to detect a 20% difference in the pharmacokinetic parameters (Cmax and AUCs) of evogliptin and metformin. Therefore, the sample sizes of 36 for Part 1 and 28 for Part 2 were chosen to account for possible dropouts.
Descriptive statistics were used to summarize baseline demographics, safety data, and pharmacokinetic parameters. All of the pharmacokinetic parameters are presented as mean ± standard deviation except for Tmax, for which median and range are displayed. Between-treatment comparison was performed using analyses of variance on log-transformed Cmax, AUClast, and AUCinf. The geometric mean ratio (GMR) and the 90% confidence interval (90% CI) were calculated from the analyses of variance model, including sequence, period, and treatment as fixed effects, and subject nested within sequence as a random effect. If the 90% CI was contained in the conventional bioequivalence range of 0.800–1.250, the conclusion was that there was no significant difference between two treatments. All statistical analyses were performed using the IBM SPSS Statistics software version 21.0 (SPSS Incorporated, Chicago, IL, USA).
Results
Demographics
Part 1 included 36 subjects with a mean (range) age of 26.8 years (22.0–38.0), height of 176.0 cm (167.3–185.3), weight of 69.5 kg (58.9–85.2), and mean BMI of 22.4 kg/m2 (18.9–26.3). In Part 2, the means (ranges) of age, height, weight, and BMI were 29.5 years (22.0–40.0), 174.3 cm (162.0–182.8), 68.6 kg (55.4–79.5), and 22.6 kg/m2 (18.3–25.9), respectively. Baseline demographics were similar and showed no statistical difference between sequence groups (Table 1).
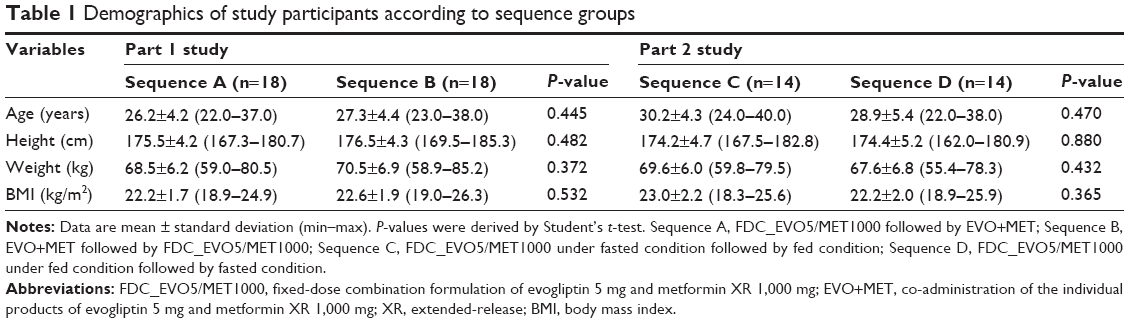 | Table 1 Demographics of study participants according to sequence groups |
Of the 64 subjects in total (36 for Part 1 and 28 for Part 2), one in Part 1 withdrew consent during the washout period for a personal reason, and one in Part 2 did not complete high-fat meal consumption in the period of treatment under the fed condition. Therefore, the 35 subjects in Part 1 and the 27 subjects in Part 2 who completed the study as planned were included in the pharmacokinetic analyses, and all of the enrolled subjects were included in the safety assessment.
Pharmacokinetics
In Part 1, the mean plasma concentration-time profile of evogliptin following a single oral administration of FDC_EVO5/MET1000 was almost superimposed on that of EVO+MET. Likewise, metformin showed a similar pharmacokinetic profile between the two treatments (Figure 2). These similar plasma concentration-time profiles for both evogliptin and metformin resulted in GMRs (FDC_EVO5/MET1000 to EVO+MET) for the pharmacokinetic parameters of evogliptin and metformin close to unity. Furthermore, 90% CIs of the GMRs fell entirely within the conventional bioequivalence range of 0.800–1.250 (Table 2). Other pharmacokinetic parameters of evogliptin and metformin, including Tmax, CL/F, and t1/2, were also comparable between the two treatments.
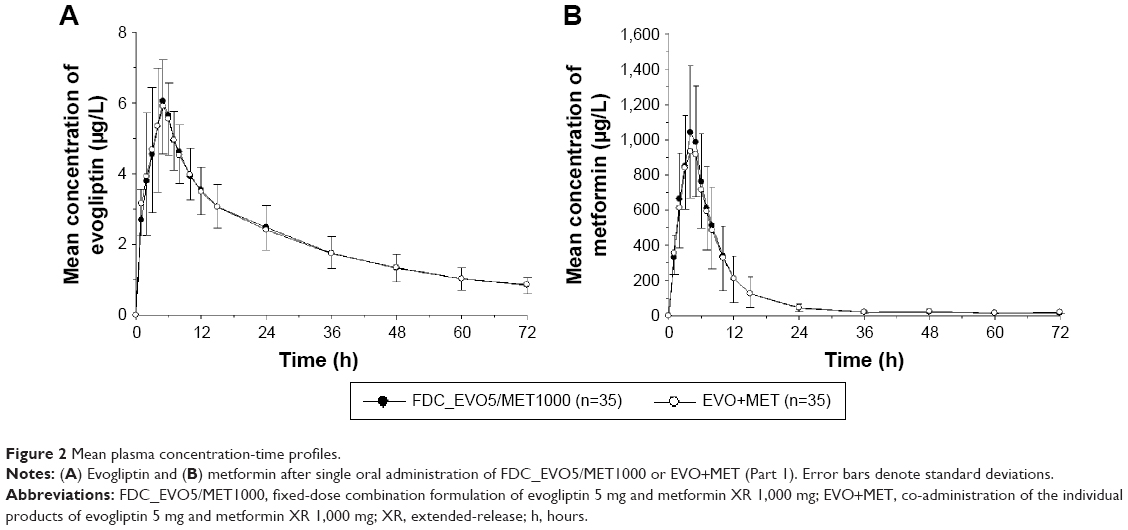 | Figure 2 Mean plasma concentration-time profiles. |
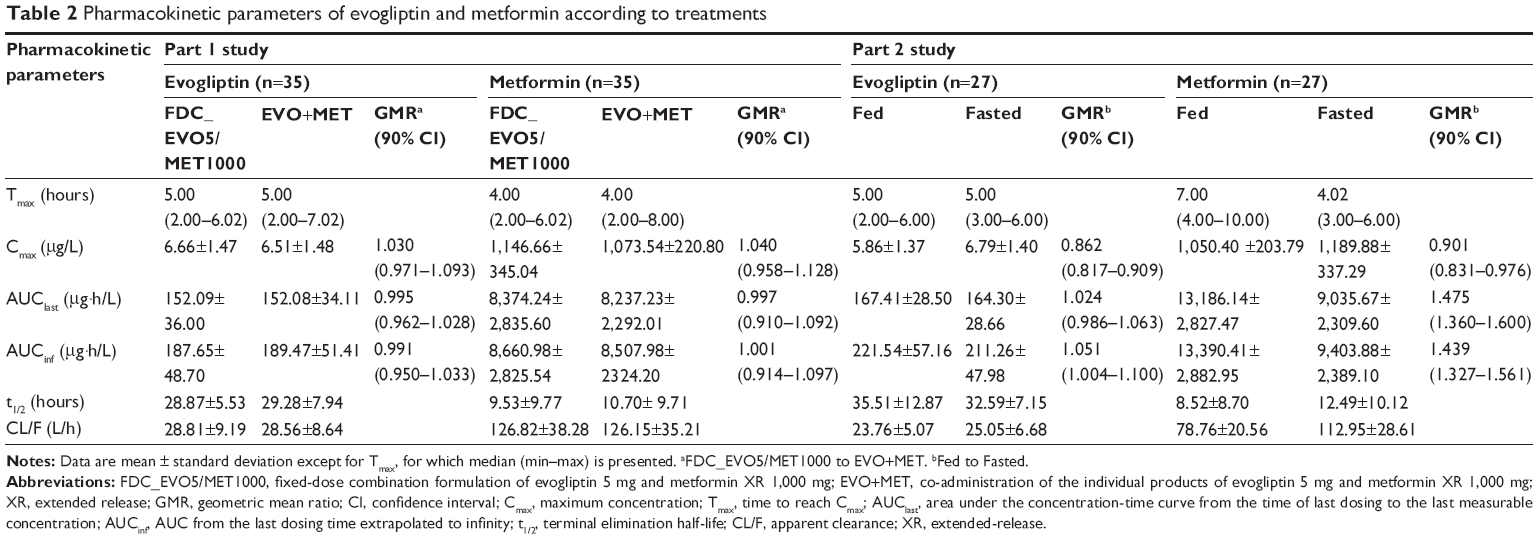 | Table 2 Pharmacokinetic parameters of evogliptin and metformin according to treatments |
In Part 2, a single dose of FDC_EVO5/MET1000 under the fed condition had a pharmacokinetic profile of evogliptin comparable with that of FDC_EVO5/MET1000 administered under the fasted condition (Figure 3). In terms of total systemic exposure, the pharmacokinetic parameters of evogliptin under the fed condition were similar to those under the fasted condition, leading to GMRs and 90% CI values that satisfied bioequivalence criteria (Table 2). On the other hand, the Tmax of metformin was slightly delayed, and systemic exposure (AUCs) increased under the fed condition compared to the fasted condition (Figure 3, Table 2). Especially, AUClast of metformin under the fed condition increased by 36%–60% compared to the fasted condition. However, the fed condition did not significantly affect Cmax of metformin, resulting in GMR and 90% CI values within the bioequivalence range.
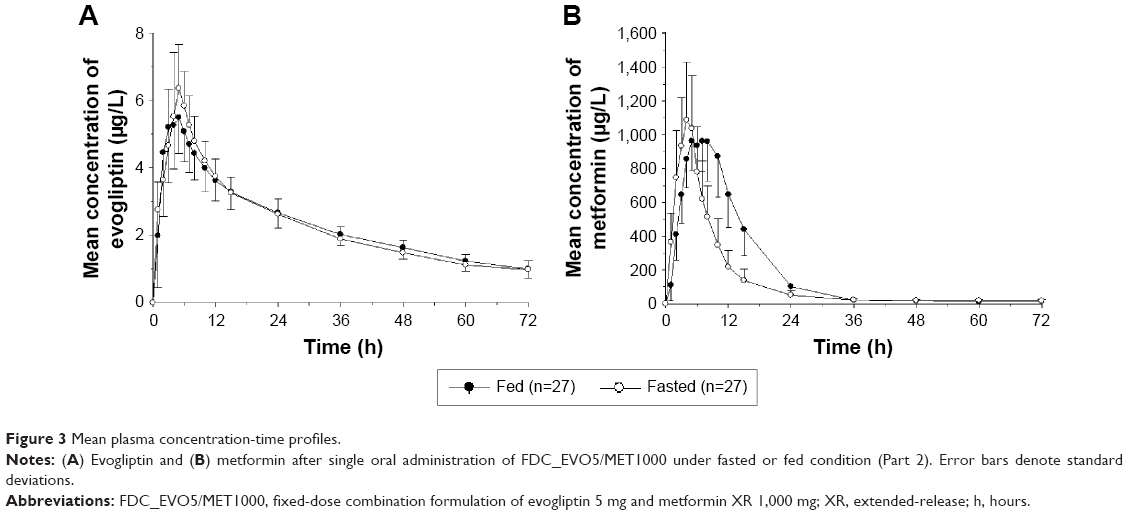 | Figure 3 Mean plasma concentration-time profiles. |
Safety results
In Part 1, four subjects (11.1%) experienced a total of five AEs that were considered possibly treatment-related; four AEs (two incidents of headache, and one incident each of diarrhea and mouth ulceration) occurred after FDC_EVO5/MET1000 administration, whereas only one AE (mouth ulceration) occurred after treatment with EVO+MET. In Part 2, seven subjects (25.0%) experienced at least one of eleven treatment-related AEs, among which four AEs (one incident each of headache, dizziness, nausea, and myalgia) occurred after treatment under fasted condition, and seven AEs (two incidents of headache, and one incident each of myalgia, abdominal discomfort, dry lips, oral mucosa erosion, and ear pain) occurred after treatment under the fed condition. All AEs were mild in intensity and resolved spontaneously without any intervention. Likewise, no clinically significant changes were noted on clinical laboratory tests, vital signs monitoring, electrocardiograms, or physical examinations throughout the entire study period of Part 1 or Part 2.
Discussion
For patients with type 2 diabetes, metformin-based combination therapy is recommended when monotherapy is insufficient.3 As a result, most type 2 diabetes patients receive more than two medications for appropriate glycemic control. The complexity of the treatment regimen and polypharmacy are known to be determinants of poor medication adherence, and FDCs have the potential to improve adherence by reducing the pill burden (polypharmacy).10 Indeed, a meta-analysis study showed that FDCs reduce the risk of medication non-compliance by 24%–26%.11 Therefore, the FDC formulation of evogliptin and metformin XR would be helpful to improve adherence, further reducing the practice–outcome gap, in which clinical guidelines are implemented but expected benefits are not realized.
According to the World Health Organization guidelines for registration of FDC medicinal products, the data requirements for marketing authorization of FDC depend broadly on the scenario into which the application falls.12 As FDC_EVO5/MET1000 contains a new chemical entity, evogliptin, this new FDC corresponds to scenario 4. For marketing approval of a new FDC in scenario 4, comparative bioavailability data for a new dosage form are required as well as clinical safety and efficacy data.12 Consequently, the present study was designed to compare bioavailability and demonstrated bioequivalent pharmacokinetics between FDC_EVO5/MET1000 and the corresponding loose combination. It was verified that all pharmacokinetic parameters for both evogliptin and metformin were similar between FDC_EVO5/MET1000 and the loose combination, leading to GMR and 90% CI values falling entirely within the conventional bioequivalence range of 0.800–1.250 for both Cmax and AUClast.
Because FDC_EVO5/MET1000 includes an XR dosage formulation, metformin XR, a food effect study was also conducted in accordance with Korean Ministry of Food and Drug Safety guidelines.13 According to the US Food and Drug Administration labeling of the metformin XR product, the extent of metformin absorption, as measured by AUC, increases by approximately 50% when given with food, although there is no effect of food on Cmax and Tmax of metformin.14 Consistently, in the present study, food increased the bioavailability of metformin by about 47.5% while Cmax was not significantly affected following administration of FDC_EVO5/MET1000. Practically, metformin is recommended to be taken with food to minimize gastrointestinal side effects.15 As the pharmacokinetics of metformin from FDC_EVO5/MET1000 with food was similar to that of metformin XR, the change in pharmacokinetics of metformin by food would not be clinically meaningful. On the other hand, the pharmacokinetics of evogliptin from FDC_EVO5/MET1000 was consistent regardless of food intake. Consequently, the results of the food effect study suggest that FDC_EVO5/MET1000 can be used according to the instructions for metformin XR regarding administration with food.
In bioavailability and bioequivalence studies, blood sampling is recommended to continue for at least three or more t1/2s of the drug to capture at least 80% of the relevant AUC.16 However, the current study was designed to characterize the pharmacokinetics of FDC_EVO5/MET1000 up to 72 hours, which covers only about two terminal half-lives of evogliptin. This time frame was chosen because most regulatory agencies accept the assessment of bioequivalence using truncated AUC (AUC0-72 h) for drugs with an elimination half-life of longer than 24 hours and low intrasubject variability in distribution and clearance.16,17 In the present study, the terminal half-life of evogliptin was longer than 24 hours, and intrasubject variability in the CL/F of evogliptin was low (around 10.0%). Therefore, truncated AUC at 72 hours for evogliptin is reasonable to use in a bioequivalence and food effect study for FDC_EVO5/MET1000.
In the present study, subjects did not experience any serious AEs, and the AEs observed were mild to moderate in nature and resolved without sequelae. Furthermore, there was no clinically meaningful difference in frequency and occurrence of AEs relative to treatments, and safety profiles were not altered to any clinically meaningful extent by treatment. Based on these safety outcomes, FDC_EVO5/MET1000 seems to be well tolerated and is expected to be used safely. However, it should be considered that the safety assessment was not a primary objective of the study, which also was conducted in only a few dozen healthy subjects.
In conclusion, FDC_EVO5/MET1000 is expected to be a substitute for the loose combination of evogliptin 5 mg and metformin XR 1,000 mg, providing better adherence with convenient administration. Furthermore, FDC_EVO5/MET1000 can be administered with food, which is recommended for metformin XR.
Acknowledgment
This study was sponsored by Dong-A ST Co., Ltd., Seoul, Republic of Korea.
Author contributions
All the authors significantly contributed to the conception, design, execution, and/or analysis and interpretation of data in this study. Furthermore, they participated in drafting, reviewing, and/or revising the manuscript for important intellectual content.
Disclosure
The authors have no conflicts of interest to disclose.
References
American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37 Suppl 1:S81–S90. | ||
Garber AJ, Abrahamson MJ, Barzilay JI, et al. AACE comprehensive diabetes management algorithm 2013. Endocr Pract. 2013;19(2):327–336. | ||
Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015;38(1):140–149. | ||
Drucker DJ, Nauck MA. The incretin system: glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. Lancet. 2006;368(9548):1696–1705. | ||
Rodbard HW, Jellinger PS, Davidson JA, et al. Statement by an American Association of Clinical Endocrinologists/American College of Endocrinology consensus panel on type 2 diabetes mellitus: an algorithm for glycemic control. Endocr Pract. 2009;15(6):540–559. | ||
Kim TE, Lim KS, Park MK, et al. Evaluation of the pharmacokinetics, food effect, pharmacodynamics, and tolerability of DA-1229, a dipeptidyl peptidase IV inhibitor, in healthy volunteers: first-in-human study. Clin Ther. 2012;34(9):1986–1998. | ||
Gu N, Park MK, Kim TE, et al. Multiple-dose pharmacokinetics and pharmacodynamics of evogliptin (DA-1229), a novel dipeptidyl peptidase IV inhibitor, in healthy volunteers. Drug Des Devel Ther. 2014;8:1709–1721. | ||
Jung CH, Park CY, Ahn KJ, et al. A randomized, double-blind, placebo-controlled, phase II clinical trial to investigate the efficacy and safety of oral DA-1229 in patients with type 2 diabetes mellitus who have inadequate glycaemic control with diet and exercise. Diabetes Metab Res Rev. 2015;31(3):295–306. | ||
Boulton DW, Smith CH, Li L, Huang J, Tang A, LaCreta FP. Bioequivalence of saxagliptin/metformin extended-release (XR) fixed-dose combination tablets and single-component saxagliptin and metformin XR tablets in healthy adult subjects. Clin Drug Investig. 2011;31(9):619–630. | ||
Blonde L, Wogen J, Kreilick C, Seymour AA. Greater reductions in A1C in type 2 diabetic patients new to therapy with glyburide/metformin tablets as compared to glyburide co-administered with metformin. Diabetes Obes Metab. 2003;5(6):424–431. | ||
Bangalore S, Kamalakkannan G, Parkar S, Messerli FH. Fixed-dose combinations improve medication compliance: a meta-analysis. Am J Med. 2007;120(8):713–719. | ||
World Health Organization. Guidelines for registration of fixed-dose combination medicinal products. WHO Technical Report Series; 2005. Available from: http://apps.who.int/prequal/info_general/documents/TRS929/WHO_TRS_929_annex5FDCs.pdf. Accessed March 5, 2016. | ||
National Institute of Toxicology Research. Guideline on food-effect bioavailability and fed bioequivalence studies. Ministry of Food and Drug Safety (MFDS); 2005. Available from: http://www.mfds.go.kr/index.do?mid=695&pageNo=81&seq=714&cmd=v. Accessed March 5, 2016. | ||
US Food and Drug Administration. Drug label information: GLUCOPHAGE XR. FDA; 2008. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2008/020357s031,021202s016lbl.pdf. Accessed March 5, 2016. | ||
Graham GG, Punt J, Arora M, et al. Clinical pharmacokinetics of metformin. Clin Pharmacokinet. 2011;50(2):81–98. | ||
US Food and Drug Administration. Guidance for industry: bioavailability and bioequivalence studies submitted in NDAs or INDs – General Considerations. FDA; 2014. Available from: http://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm389370.pdf. Accessed March 5, 2016. | ||
Committee for Medicinal Products for Human Use and European Medicines Agency. Guideline on the investigation of bioequivalence. EMA; 2010. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2010/01/WC500070039.pdf. Accessed March 5, 2016. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.