")
Back to Journals » Drug Design, Development and Therapy » Volume 16
Pharmacokinetic Drug Interaction Between Amlodipine and Tadalafil: An Open-Label, Randomized, Multiple-Dose Crossover Study in Healthy Male Volunteers
Authors Kim H , Lee SH , Jung J , Hong S , Lim HS
Received 18 November 2021
Accepted for publication 26 January 2022
Published 19 February 2022 Volume 2022:16 Pages 425—433
DOI https://doi.org/10.2147/DDDT.S348897
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Hyungsub Kim,1 Shi Hyang Lee,2 Jina Jung,3 Sunghee Hong,3 Hyeong-Seok Lim2
1Department of Emergency Medical Services, College of Health Sciences, Eulji University, Seongnam, Republic of Korea; 2Department of Clinical Pharmacology and Therapeutics, Asan Medical Center, University of Ulsan, Seoul, Republic of Korea; 3Hanmi Pharmaceutical Co. Ltd., Seoul, Republic of Korea
Correspondence: Hyeong-Seok Lim, Tel +82-2-3010-4613, Fax +82-2-3010-4623, Email [email protected]
Purpose: The combined administration of tadalafil, a phosphodiesterase-5 inhibitor, and amlodipine, a calcium channel blocker, can be a promising therapeutic option for hypertension patients with erectile dysfunction. This study aimed to examine the pharmacokinetic drug interaction between tadalafil and amlodipine and the tolerability of their combined administration in healthy male subjects.
Subjects and Methods: Healthy volunteers (N = 24) were randomly assigned to one of the six sequences that consisted of three treatments: tadalafil (5 mg) alone, amlodipine (10 mg) alone, and tadalafil plus amlodipine. The study drugs were administered orally for 9 d, and the collected serial blood samples were analyzed up to 72 h after the last dosing. Pharmacokinetic parameters were calculated using non-compartmental analysis.
Results: For tadalafil, geometric mean ratios (GMRs) (90% confidence interval (CI)) of the combined therapy over the monotherapy were 1.57 (1.46– 1.68) for AUCτ,ss and 1.34 (1.24– 1.45) for Cmax,ss. For amlodipine, the GMRs (90% CI) of AUCτ,ss and Cmax,ss were 0.93 (0.90– 0.97) and 0.95 (0.91– 0.99), respectively. The severity of all observed adverse events (AEs) related to the study drugs was mild, and the frequency of AEs of the combined administration was not significantly different from the monotherapy.
Conclusion: A substantial pharmacokinetic drug interaction between tadalafil and amlodipine was observed with respect to the concentration of tadalafil when administered concomitantly. However, the dose range of the combined administration of tadalafil and amlodipine in the present study was well tolerated by the subjects.
Keywords: drug interaction, tadalafil, amlodipine, pharmacokinetics, tolerability
Introduction
Erectile dysfunction (ED) is characterized by the consistent inability to attain or keep an erection sufficient for satisfactory sexual intercourse. The prevalence of ED has been increasing persistently, and diabetes mellitus, hypertension and dyslipidemia are known to be risk factors of ED.1,2 In particular, based on patient questionnaire and the International Index of Erectile Function, Giuliano et al reported that the overall prevalence of ED in hypertension patients was 61% and 67%, respectively.1 In patients with chronic hypertension, the need for co-administration of a phosphodiesterase (PDE)-5 inhibitor such as tadalafil for ED is increasing.
At present, phosphodiesterase (PDE)-5 inhibitors such as sildenafil, tadalafil, vardenafil and avanafil are marketed globally. ED drugs inhibit the activity of PDE-5 in the corpus cavernosum, which prevents the breakdown of cyclic guanosine monophosphate (cGMP), leading to improvement of penile blood flow.3 Among the PDE-5 inhibitors, tadalafil is predominantly metabolized by cytochrome P450 (CYP) 3A4 with a relatively long half-life of 17.5 h.4,5
Amlodipine is one of the most extensively used oral dihydropyridine calcium channel blocker (CCB), which particularly reduced blood pressure variability and was effective for protecting stroke and myocardial infarction.6 It is slowly absorbed with Tmax of 5.0–6.0 h after oral administration and is eliminated via a biphasic mode with a half-life of 40–60 h.7 In terms of metabolism, it is known as a substrate and a weak inhibitor of CYP3A4.8,9
Considering that both drugs are common substrates of CYP3A4 and that amlodipine is a potent inhibitor of CYP3A4, the possibility of a drug interaction cannot be ruled out. No study has examined the pharmacokinetic (PK) interaction between tadalafil and amlodipine in healthy subjects. The primary aim of this study was to evaluate PK interaction and tolerability of tadalafil and amlodipine administered to healthy male volunteers at steady state.
Methods
Study Information
The study protocol was approved by the Korean Ministry of Food and Drug Safety and by the Institutional Review Board (IRB) of Asan Medical Center (AMC, Seoul, Republic of Korea) (IRB Approval Number 2014-0711). All subjects provided written informed consent before undergoing screening tests. The trial was registered at ClinicalTrials.gov (identifier number NCT02243319). All the procedures were conducted according to the guidelines of Good Clinical Practice and the principles of the Declaration of Helsinki.
Subjects
Healthy male volunteers aged 19–45 years with a body mass index (BMI) of 19–28 kg/m2 were eligible for the study. All subjects were considered to be in good health based on medical history, physical examinations, vital signs (blood pressure, heart rate and body temperature), 12-lead electrocardiogram (ECG), clinical laboratory tests, serology, and urine drug screening within 4 weeks before the first administration of the study drug. Subjects with a known allergic or hypersensitivity reaction to tadalafil or amlodipine, or with a history of drug abuse, were excluded from the study.
Study Design
The study was designed as an open-label, randomized, multiple-dose, three-treatment, three-period, six-sequence, and crossover clinical trial. All subjects were randomly assigned to one of the six sequences and received one of the three different treatments every 24 h for 9 consecutive days:10 tadalafil 5 mg (Treatment A), amlodipine 10 mg (Treatment B), or tadalafil 5 mg plus amlodipine 10 mg (Treatment C) (Figure 1). All treatments were administered under fasting conditions along with 240 mL of water. After the administration of the study drug(s), subjects were required to fast for 4 h. Following a 15-d washout interval, subjects received one of the other treatment regimens. This was repeated until they had received all three treatments. Subjects were admitted to the Clinical Trial Center (CTC) at AMC from Day 8 to Day 10 (24 h after the last dose) during each treatment period. On Days 11 and 12, all subjects visited the CTC for tolerability and PK interaction assessments of tadalafil and amlodipine. The schedule for the second and third treatment periods was the same as that for the first period. Follow-up visit was performed 2 weeks after the last dosing.
 |
Figure 1 Study design (open-label, multiple-dose, three-treatment, three-period, six-sequence crossover study). (A) Tadalafil 5 mg; (B) amlodipine 10 mg; (C) tadalafil 5 mg + amlodipine 10 mg. Abbreviation: SEQ, sequence. |
Sampling and Measurement of Concentration
For PK analysis, sequential blood samples were collected prior to dosing on Day 1, Day 8 and Day 9 and 0.5, 1, 1.5, 2, 3, 4, 6, 8, 10, 12, 24, 48, and 72 h after the Day 9 dosing.11 Samplings prior to dosing on Day 8 and Day 9 were to confirm the steady state by comparing trough concentrations. All the blood samples used to determine the concentration of tadalafil and amlodipine were drawn into ethylenediaminetetraacetic acid-K2 tubes and separated via centrifugation at 1800 g for 8 minutes at 4 °C. Samples were then stored at – 70 °C until analysis.
The plasma concentrations of tadalafil and amlodipine were measured using a validated liquid chromatography-tandem mass spectrometric (LC-MS/MS) method after solid-phase extraction from plasma. Calibration curves covered the range of 1.0 ~ 2000.0 ng/mL tadalafil and 0.05 ~ 50.0 ng/mL amlodipine. All plasma analyses were performed at BIOINFRA Life Science Inc. (Seoul, Republic of Korea).
PK Assessment and Statistical Analysis
The PK of tadalafil and amlodipine in each subject was analyzed using a non-compartmental method with Phoenix WinNonlin® software (version 6.4, Pharsight, CA, USA) and R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria). All analyses were based on actual sampling time. The peak plasma concentration at steady state (Cmax,ss) and the time taken to reach Cmax,ss (Tmax,ss) were determined from observed values. Terminal elimination rate constant (λz) was estimated using linear regression of the terminal log-linear portion of the plasma concentration–time curves. The t1/2β for each participant was calculated as ln(2)/λz.
Demographic data and PK parameters were summarized using descriptive statistics. To compare PK characteristics between tadalafil, amlodipine or combined administration of tadalafil and amlodipine, Cmax,ss, AUCτ,ss and AUC0~∞ were log-transformed and tested using analysis of variance model. The mean differences and 90% confidence interval (CI) were back-transformed to obtain geometric mean ratio (GMR) and CI for those ratios. In addition, paired t-test was used to compare the pharmacokinetic parameters. A P-value <0.05 was deemed significant.
Tolerability Assessments
Tolerability was assessed by measuring vital signs, 12-lead ECGs, clinical laboratory tests (hematology, blood chemistry, and urinalysis), physical examinations, and monitoring of adverse events (AEs). AEs were recorded based on symptoms and signs, duration, intensity, relationship to the study drug, action taken, outcome, and seriousness. All AEs were coded using the Medical Dictionary for Regulatory Activities (MedDRA® version 17.0).
Result
Study Participants
Of the 24 participants that received the study drug at least once, 22 subjects completed the study. Two out of the 24 subjects administered the study drug in the first period were excluded from the study due to AEs (fever for the tadalafil-treated subject and increased aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels for the amlodipine-treated subject).
All subjects were included in the tolerability assessment. Demographics of participants such as age, height, weight, and BMI are summarized as follows: Mean (SD) age was 29.54 (5.70) years, mean height was 173.73 (4.16) cm, mean weight was 69.68 (8.05) kg, and mean BMI was 23.05 (2.23) kg/m2, respectively. There were no statistical differences across the sequence groups in terms of demographic distribution.
PK Analysis
To evaluate the PK drug interactions between tadalafil and amlodipine, the PK profiles of tadalafil (Figure 2A) and amlodipine (Figure 2B) were separately assessed. Since two subjects were excluded from the study due to AEs, 22 subjects were included in the PK analysis of the present study.
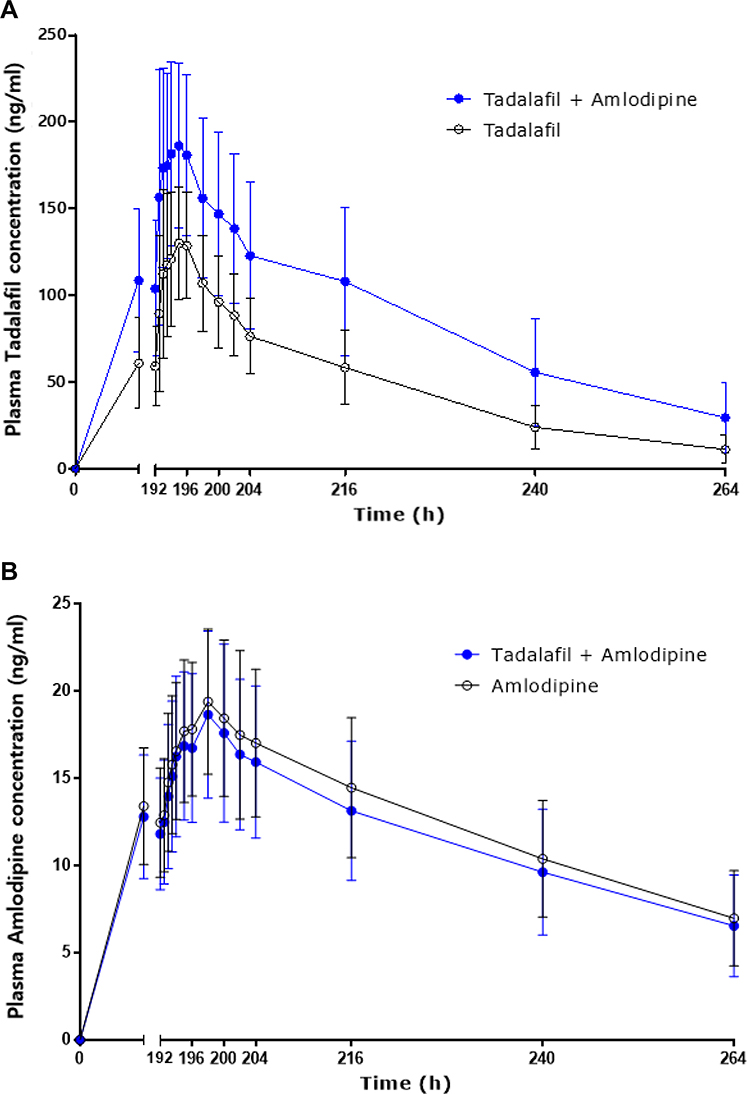 |
Figure 2 Mean (SD) plasma concentration–time curves of tadalafil (A) and amlodipine (B) after oral administration of 5 mg tadalafil with or without 10 mg amlodipine at steady state (n = 22). |
The PK parameters of tadalafil and amlodipine are shown in Table 1. The steady-state mean ratios (90% CI) of co-administration of tadalafil and amlodipine over a single dose of tadalafil were 1.57 (1.46–1.68) for AUCτ,ss and 1.34 (1.24–1.45) for Cmax,ss, respectively. The GMRs (90% CI) of co-administration of tadalafil and amlodipine over a single dose of amlodipine were 0.93 (0.90–0.97) and 0.95 (0.91–0.99) for AUCτ,ss and Cmax,ss, respectively (Table 2).
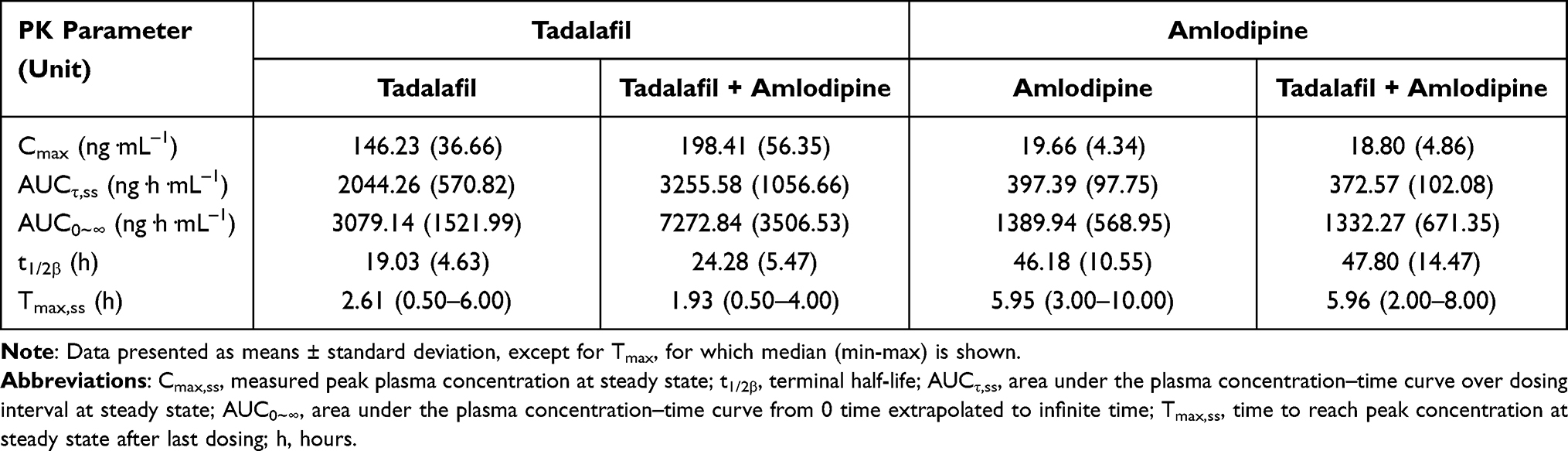 |
Table 1 Pharmacokinetic Parameters of Tadalafil and Amlodipine in Healthy Subjects (n = 22) |
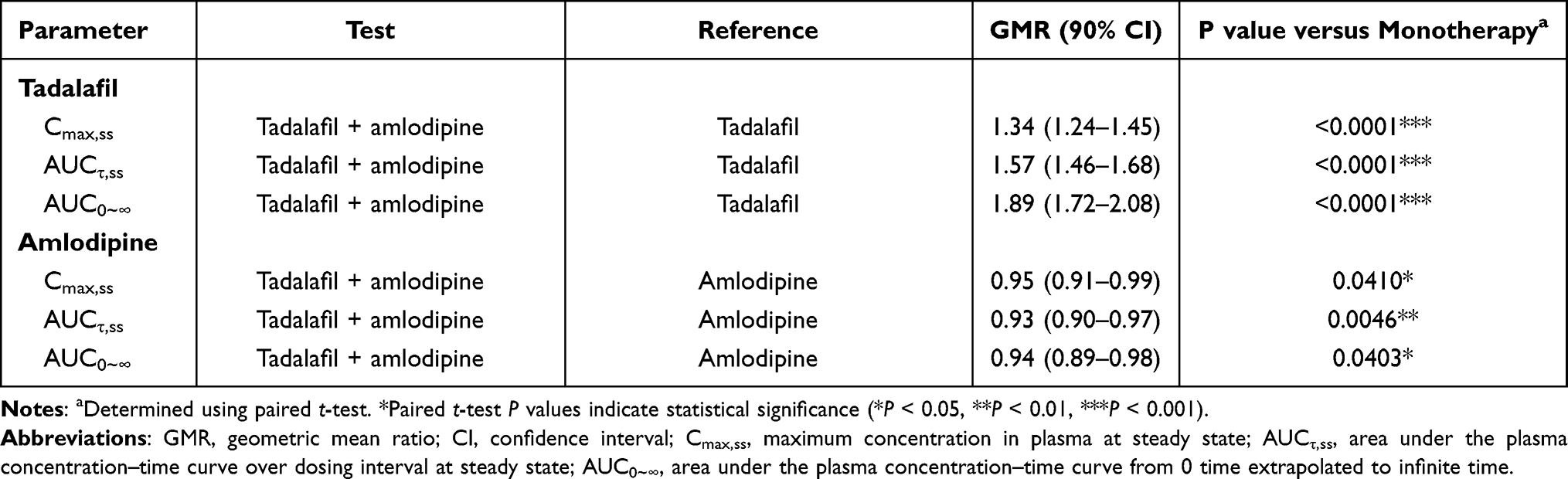 |
Table 2 Geometric Mean Ratio of Pharmacokinetic Parameters of Tadalafil and Amlodipine When Given Alone and in Combination at Steady State in Healthy Subjects (n = 22) |
Tolerability Assessment
Thirteen subjects showed a total of 37 AEs, of which 29 were considered to be “related” to the study drugs. The most common AE in the groups of tadalafil single administration and co-administration (amlodipine plus tadalafil) was headache (seven subjects, ten events) (Table 3). Laboratory tests revealed an increase in AST, ALT, and triglyceride and a decrease in absolute neutrophil count. No clinically significant abnormality in 12-lead ECGs and physical examination was found. After 9-day consecutive administration of tadalafil, amlodipine and tadalafil plus amlodipine, the greatest decreases in mean (SD) SBP were 13.9 (7.5), 13.7 (7.3) and 18.8 (6.9) mmHg, respectively, and DBP, 16.0 (6.4), 14.7 (6.6) and 19.2 (6.5) mmHg (Figure 3). No serious AEs occurred throughout the entire study. All AEs were mild in severity and resolved without any sequelae.
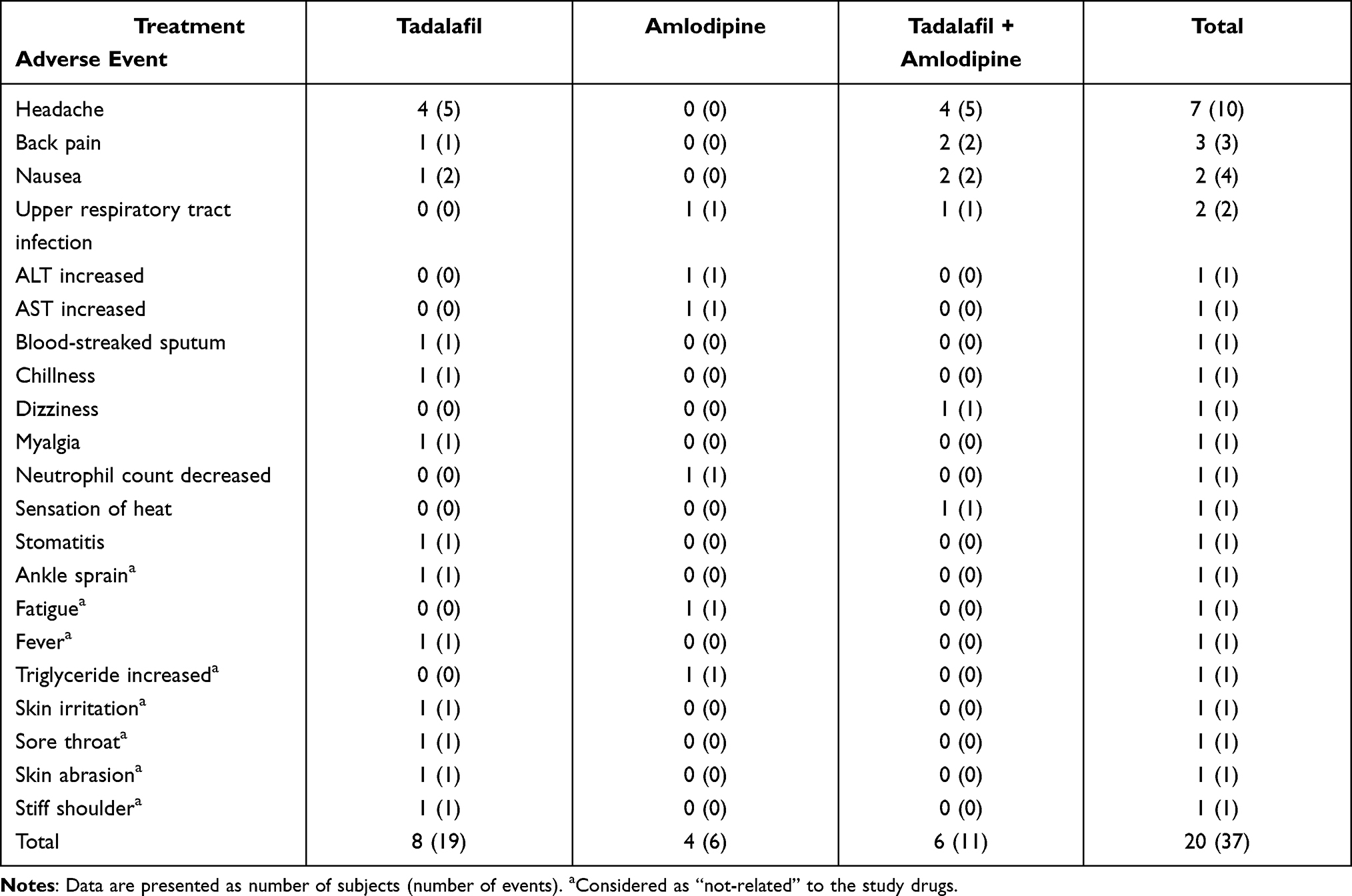 |
Table 3 Summary of Adverse Event After the Study Drug Administration |
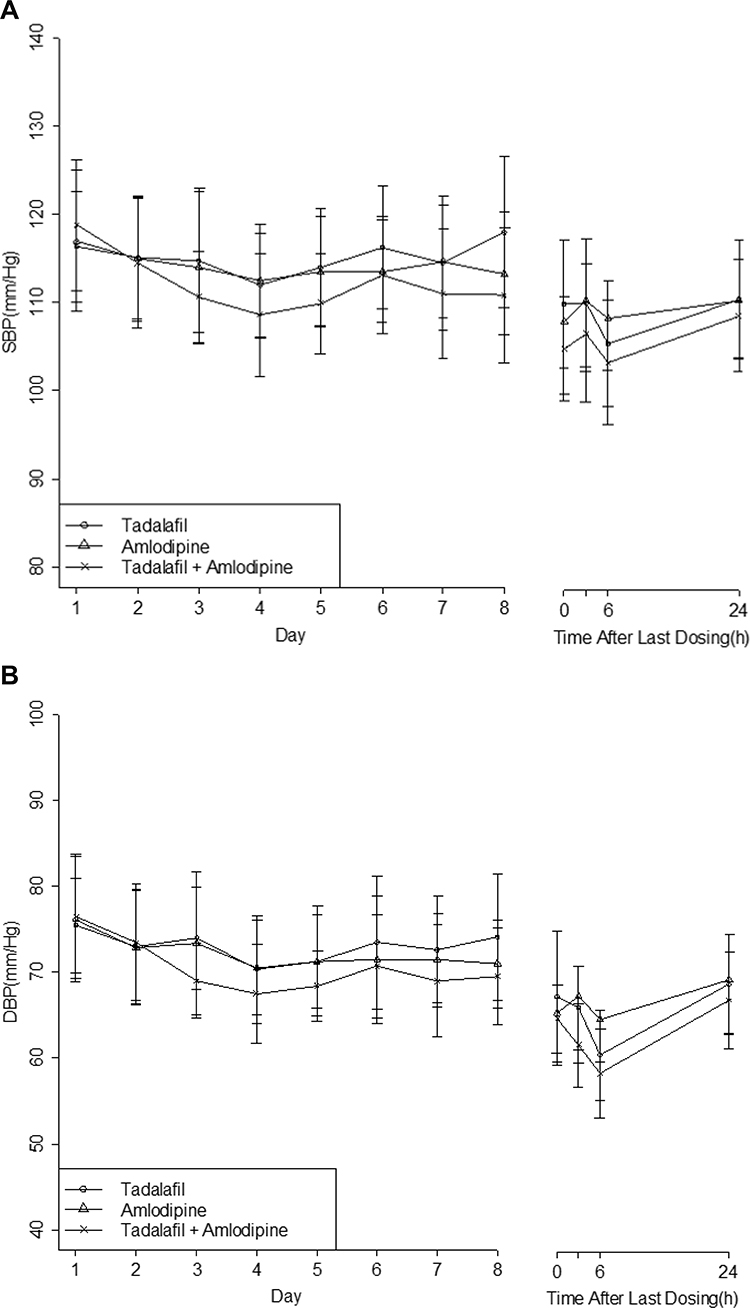 |
Figure 3 Mean (SD) (A) systolic and (B) diastolic blood pressure (SBP and DBP, respectively) over 9 days of administration of tadalafil and amlodipine administered as monotherapy and combined therapy in healthy subjects (n = 22). |
Discussion
This study investigated the potential PK interaction between tadalafil and amlodipine in healthy subjects at steady state. Based on the results of the present study, the half-life of amlodipine, which was approximately 46 h, was larger than that of tadalafil (19 h). Washout period was set up at 15 d, which was 7 times higher than the half-life, allowing both study drugs to be excreted to the lowest level of quantification before the next period. Moreover, the AUCτ,ss/AUCinf,ss of both tadalafil and amlodipine were over 80% (data not shown). Blood sampling was performed for up to 72 h after the last dosing to estimate the exposures of tadalafil and amlodipine sufficiently.
Recently, Kim et al reported that the Cmax and Tmax of amlodipine were 18.4 ng/mL and 6.0 h in subjects administered 10 mg amlodipine for 10 d, respectively.12 Their results are consistent with the results presented in this study (19.6 ng/mL and 5.95 h). The AUC of tadalafil increased proportionally with dose in healthy subjects administered 2.5 to 20 mg of tadalafil. Steady-state plasma concentrations were attained within 5 d of administering the drug once per day, and exposure was approximately 1.6-fold greater after a single dose, similar to the profile in this study.
In this study, the primary PK parameters were Cmax,ss and AUCτ,ss of tadalafil and amlodipine. The administration of tadalafil alone increased both Cmax,ss and AUCτ,ss significantly compared with the co-administration of tadalafil and amlodipine; 90% CIs for the GMRs of Cmax,ss and AUCτ,ss were all out of the range of 0.80–1.25. However, the 90% CIs for the GMRs of combined administration versus monotherapy of amlodipine were within the range of 0.80–1.25 for Cmax,ss and AUCτ,ss.
Tadalafil is predominantly metabolized by CYP3A4, and CCBs such as amlodipine, diltiazem, and verapamil are known to be a potent CYP3A4 inhibitor.8,9 These facts could explain why the Cmax,ss and AUCτ,ss of tadalafil were remarkably increased in the group of tadalafil plus amlodipine in the present study. Although the plasma level of tadalafil concentration in co-administration treatment was greater than monotherapy treatment, and the frequency of AEs such as a remarked decrease in blood pressure was not significantly different. Sildenafil, other PDE-5 inhibitor, and antihypertensive dihydropyridines such as amlodipine were metabolized by CYP3A4. However, administration of sildenafil and amlodipine did not exhibit a synergistic blood pressure-lowering action.13,14
The most common AE was headache in the treatment group of tadalafil alone and tadalafil with amlodipine, which was a well-known AE of tadalafil. As shown in Table 2 and Figure 2, tadalafil was absorbed rapidly (Tmax,ss= 2.61 h) and decreased to the approximate baseline by 24 h after dosing. Likewise, the AE, which started at least 3 h late after drug administration, was almost resolved within 2 d.
The limitation of the present study is that the subjects that participated in the study were all healthy volunteers who have different pathophysiological environments from the hypertension patients. Further studies, to continue drug development, should be carried out on hypertension patients to confirm the PK drug interaction between tadalafil and amlodipine.
Conclusion
This study demonstrated that multiple oral co-administration of 5 mg tadalafil and 10 mg amlodipine showed significant PK drug interactions at steady state. In addition, within the dose range studied here, it was well tolerated in the healthy male subjects.
Data Sharing Statement
The raw data of this study will not be shared because of confidentiality.
Acknowledgments
We thank Dr. Joon Seo Lim from the Scientific Publications Team at Asan Medical Center for his editorial assistance in preparing this manuscript.
Funding
This study was sponsored by Hanmi Pharmaceutical Co. Ltd. (Seoul, Republic of Korea).
Disclosure
Jina Jung and Junghee Hong are employees of Hanmi Pharmaceutical Co. Ltd. Prof. Dr. Hyeong-Seok Lim reports grants from Hanmi Pharmaceutical Company, outside the submitted work. The other authors report no conflicts of interest in this work.
References
1. Giuliano FA, Leriche A, Jaudinot EO, De Gendre AS. Prevalence of erectile dysfunction among 7689 patients with diabetes or hypertension, or both. Urology. 2004;64(6):1196–1201. doi:10.1016/j.urology.2004.08.059
2. Terentes-Printzois D, Ioakeimidis N, Rokkas K, Vlachopoulos C. Interactions between erectile dysfunction, cardiovascular disease and cardiovascular drugs. Nat Rev Cardiol. 2022;19(1):59–74. doi:10.1038/s41569-021-00593-6
3. Rajfer J, Aliotta PJ, Steidle CP, Fitch WP
4. Zhu Y, Wang F, Li Q, et al. Amlodipine metabolism in human liver microsomes and roles of CYP3A4/5 in the dihydropyridine dehydrogenation. Drug Metab Dispos. 2014;42(2):245–249. doi:10.1124/dmd.113.055400
5. Cialis (Tadalafil tablet) [package insert]. Indianapolis IN: Eli Lilly and Company; February, 2018.
6. Iyengar SS, Mohan JC, Ray S, et al. Effect of amlodipine in stroke and myocardial infarction: a systematic review and meta-analysis. Cardiol Ther. 2021;10(2):429–444. doi:10.1007/s40119-021-00239-1
7. Shirley M, McCormack PL. Perindopril/amlodipine (Prestalia®): a review in hypertension. Am J Cardiovasc Drugs. 2015;15(5):363–370. doi:10.1007/s40256-015-0144-1
8. Kirigaya Y, Shiramoto M, Ishizuka T, et al. Pharmacokinetic interaction of esaxerenone with amlodipine and digoxin in healthy Japanese subjects. BMC Pharmacol Toxicol. 2020;21:55. doi:10.1186/s40360-020-00423-4
9. Wang Y-C, Hsieh T-C, Chou C-L, Wu J-L, Fang T-C. Risks of adverse event following coprescription of statins and calcium channel blockers: a nationwide population-based study. Medicine. 2016;95(2):e2487. doi:10.1097/MD.0000000000002487
10. Noh YH, Lim HS, Kim MJ, et al. Pharmacokinetic interaction of telmisartan with S-amlodipine: an open-label, two period crossover study in healthy male volunteers. Clin Ther. 2012;34(7):1625–1634. doi:10.1016/j.clinthera.2012.05.010
11. Seong SJ, Ohk B, Kang WY, et al. Pharmacokinetic drug interactions between amlodipine, valsartan, and rosuvastatin in healthy volunteers. Adv Ther. 2019;36(7):1642–1656. doi:10.1007/s12325-019-00976-9
12. Kim JR, Kim S, Huh W, Ko JW. No pharmacokinetic interaction between candesartan and amlodipine following multiple oral administrations in healthy subjects. Drug Des Devel Ther. 2018;12:2475–2483. doi:10.2147/DDDT.S172568
13. Robert A, Kloner RA, Mitchell M, Emmick JT. Cardiovascular effects of tadalafil in patients on common antihypertensive therapies. Am J Cardiol. 2003;92(suppl):47M–57M. doi:10.1016/S0002-9149(03)00075-4
14. Simonsen U. Interaction between drugs for erectile dysfunction and drugs for cardiovascular disease. Int J Impot Res. 2002;14:178–188. doi:10.1038/sj.ijir.3900846
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.