")
Back to Journals » Journal of Pain Research » Volume 15
Perspectives of Healthcare Professionals Towards Combination Use of Oral Paracetamol and Topical Non-Steroidal Inflammatory Drugs in Managing Mild-to-Moderate Pain for Osteoarthritis in a Clinical Setting: An Exploratory Study
Authors Sethi V , Van der Laan L , Gupta S, Piros KC
Received 4 May 2022
Accepted for publication 30 July 2022
Published 6 August 2022 Volume 2022:15 Pages 2263—2272
DOI https://doi.org/10.2147/JPR.S373382
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Twillman
Vidhu Sethi,1 Luke Van der Laan,2 Sanjeev Gupta,3 K Cornelius Piros4
1GlaxoSmithKline Consumer Healthcare, Singapore; 2Faculty of Business, Education, Law & Arts, University of Southern Queensland, Queensland, Australia; 3Department of Orthopaedic Surgery, Royal Prince Alfred Hospital, Sydney, Australia; 4Regena Healthcare, Selangor, Malaysia
Correspondence: Vidhu Sethi, GlaxoSmithKline Consumer Healthcare, Singapore, GSK Asia House, 23 Rochester Park, 139234, Singapore, Tel +65 96447203, Email [email protected]
Purpose: To seek indicative evidence on clinical prescription practice and perspectives regarding combined oral paracetamol (APAP) and/or topical non-steroidal anti-inflammatory drugs (NSAIDs) therapy for managing mild-to-moderate osteoarthritis (OA) pain.
Participants and Methods: An exploratory qualitative study to investigate the perspectives towards using APAP and/or topical NSAIDs for OA pain management and whether current clinical practices are aligned with OA guidelines was conducted using a two-round modified Delphi methodology among three general practitioners, three orthopedists, and two pharmacists from Australia, Malaysia, and Sweden during January–June 2021. In the first round, 60-minute virtual in-depth interviews were conducted individually; in the second round, summary of the key findings was shared with the panel to seek clarity on the level of consensus (≥ 70% unanimity) and disagreement.
Results: The healthcare professionals (HCPs) agreed that APAP was considered as a universally accepted pharmacologic for most OA patients except those with contraindications or allergies. Consensus was achieved towards APAP combination with topical NSAIDs being a safer alternative than with oral NSAIDs. However, prescription uptake of combined therapy APAP with topical NSAIDs was low among the panel due to lack of strong scientific evidence on efficacy and awareness. Differences in clinical practice across and within countries could be due to different reference sources for OA pain – clinical practice experience or local/international guidelines/medical products handbooks.
Conclusion: The study suggests an opportunity to raise awareness of the suitability and potential benefits for adjuvant topical NSAIDs to APAP for effective OA pain management as well as a need for universal OA guidelines.
Keywords: combination therapy, pain relief, Delphi methodology, consensus, prescription uptake
Introduction
Approximately 20% of chronic pain globally has been attributed to osteoarthritis (OA).1 The global prevalence and incidence of OA in 2019 was estimated at 6,348.3 per 100,000 population and 492.2 per 100,000 population, respectively.2 Pain resulting from OA was associated with functional impairment, negative effects on mental health as well as significant avoidance of social activities, decline in work productivity, and activity impairment.3–5
Pharmacological options recommended by various clinical guidelines for managing OA pain and improving function include oral analgesics, topicals, and intra-articular therapies.6–9 Oral analgesics such as oral paracetamol (hereafter APAP) and oral non-steroidal anti-inflammatory drugs (NSAIDs) were recommended for nociceptive OA pain. In events where oral analgesics may not provide clinically meaningful pain relief, opioids were considered as the next line of treatment for OA pain management and are often associated with risks of dependency and/or drug abuse.7,9
In recent years, there had been discussions on the suitability of APAP being used as a first-line analgesic for OA due to small clinical effect size. This prompted a shift of many OA guidelines from recommending APAP monotherapy as a first-line pharmacologic to recommending adding adjuvant options, eg, topical/oral NSAIDs, or intra-articular injections of corticosteroids or hyaluronic acid.9,10 For instance, the Royal Australian College of General Practitioners (RACGP) OA guidelines 2018 reflected a neutral stance towards using APAP monotherapy for managing OA pain.11
The emerging evidence on the efficacy of topical NSAIDs in clinical studies led to the approval of topical NSAIDs as first-line analgesic therapy or adjuvant treatment to APAP monotherapy for effective OA pain management.10,12 The National Institute for Health and Care Excellence (NICE) OA guidelines6 as well as OA guidelines by the Ministry of Health, Malaysia (MOHM)13 recommended topical NSAIDs to be used with APAP ahead of oral NSAIDs for mild-to-moderate OA pain management.
While previous studies found APAP monotherapy a common prescription by clinicians for managing pain in OA patients,14 there is a paucity of information about recent clinical practice in managing OA pain since the updates in the clinical guidelines. Therefore, this study sought to explore and gather the perspectives and clinical practices of a panel consisting of different healthcare professionals (HCPs) – general practitioners (GPs), orthopedists, and pharmacists, towards APAP as a monotherapy and in combination with topical NSAIDs as well as the impact of OA guideline changes on clinical practices in Australia, Malaysia, and Sweden. The study aims to seek indicative evidence of APAP and topical NSAIDs combination therapy practice and perspectives on its effectiveness in relieving OA pain among HCPs. Findings from this study would provide insights and inform further research towards the clinical practice habits of different types of HCPs and diverse geographical perspectives for managing mild-to-moderate OA pain in their community.
Materials and Methods
Study Design
This exploratory qualitative study, conducted between January and June 2021, investigated the perspectives towards using APAP and/or topical NSAIDs in clinical practices and if current prescription practices were aligned with changes in OA pain management guidelines. A Delphi method was adopted whereby successive rounds of enquiry amongst panel members were conducted. The Delphi methodology, involving the opinions or recommendations from a group of experts to potentially ISO9001-standard quality management plans for healthcare systems,15 was deemed appropriate as it gave panel members equal voice, anonymity from other panel members and the ability to change their perspectives based on the results of the previous round.15 While a level of consensus was sought regarding the responses of panel members as evidence of practice perspectives, the method allows for the exploration of non-consensual responses and reasons for disagreement.
The practice perspectives were gathered from a panel of HCPs comprising GPs, orthopedists, and pharmacists from Australia, Malaysia, and Sweden, using a modified Delphi technique consisting of two rounds (Figure 1). The HCPs were blinded to the study sponsor and each other. The first round of the Delphi method comprised 60-minute virtual in-depth interviews with individual HCPs, wherein scientific evidence on the topic of using combination therapy of APAP with ketoprofen (topical) for pain reduction16 and a review of OA treatment guidelines addressing concomitant and/or sequential use of APAP with topical NSAIDs7,11,17,18 were shared with the HCPs. Items discussed during the open interviews in the first round of Delphi method explored the HCPs’ perspectives towards 1) current clinical and treatment practices for managing mild-to-moderate OA pain; 2) combination use of APAP with NSAIDs (oral and topical; short-term and long-term use); 3) clinical guidelines (NICE, European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases [ESCEO], and European Alliance of Associations for Rheumatology [EULAR]) regarding use of APAP for OA pain management; and 4) awareness of recent updates in OA clinical guidelines (NICE, Osteoarthritis Research Society International [OARSI], RACGP, American College of Rheumatology [ACR]) and the potential impact of the guideline changes on their future clinical practice; as well as their perspectives on the impact of the scientific evidence supporting the interview items.
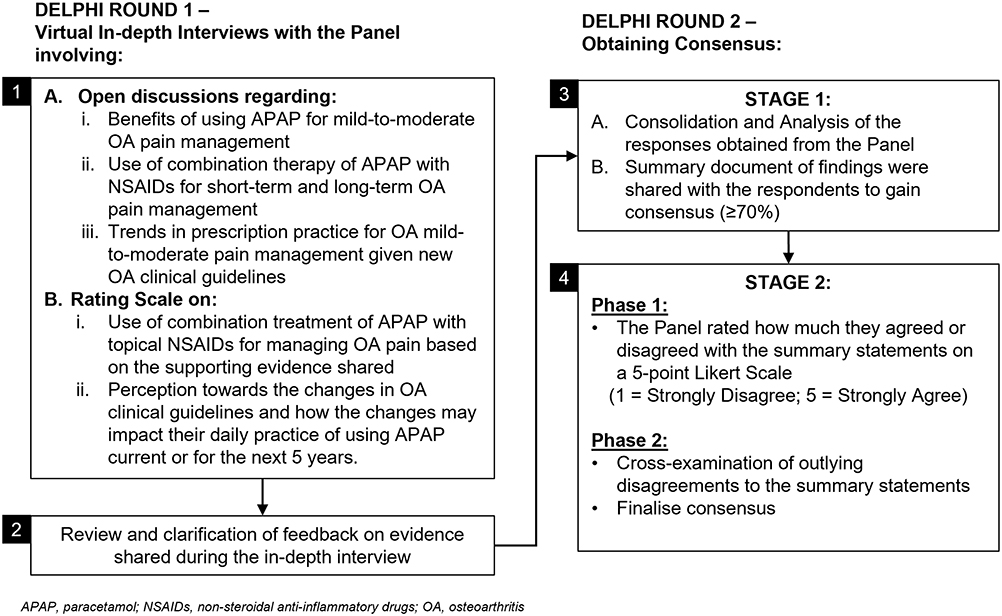 |
Figure 1 Study design. |
The key findings from the first round of the Delphi technique were summarized and shared with the HCPs in the second round to seek additional clarity on their responses. The level of consensus and disagreement towards statements derived from the key findings and clarifications (Figures 2 and 3) were then sought from the panel members. Consensus was achieved when there was ≥70% unanimity within the panel determined with a quantitative 5-point Likert Scale (“1” being “strongly disagree” and “5” being “strongly agree”) response to the key findings from round one. Outlying disagreements were further examined to gain a deeper insight to the rationale for continued disagreement at the second phase of round two.
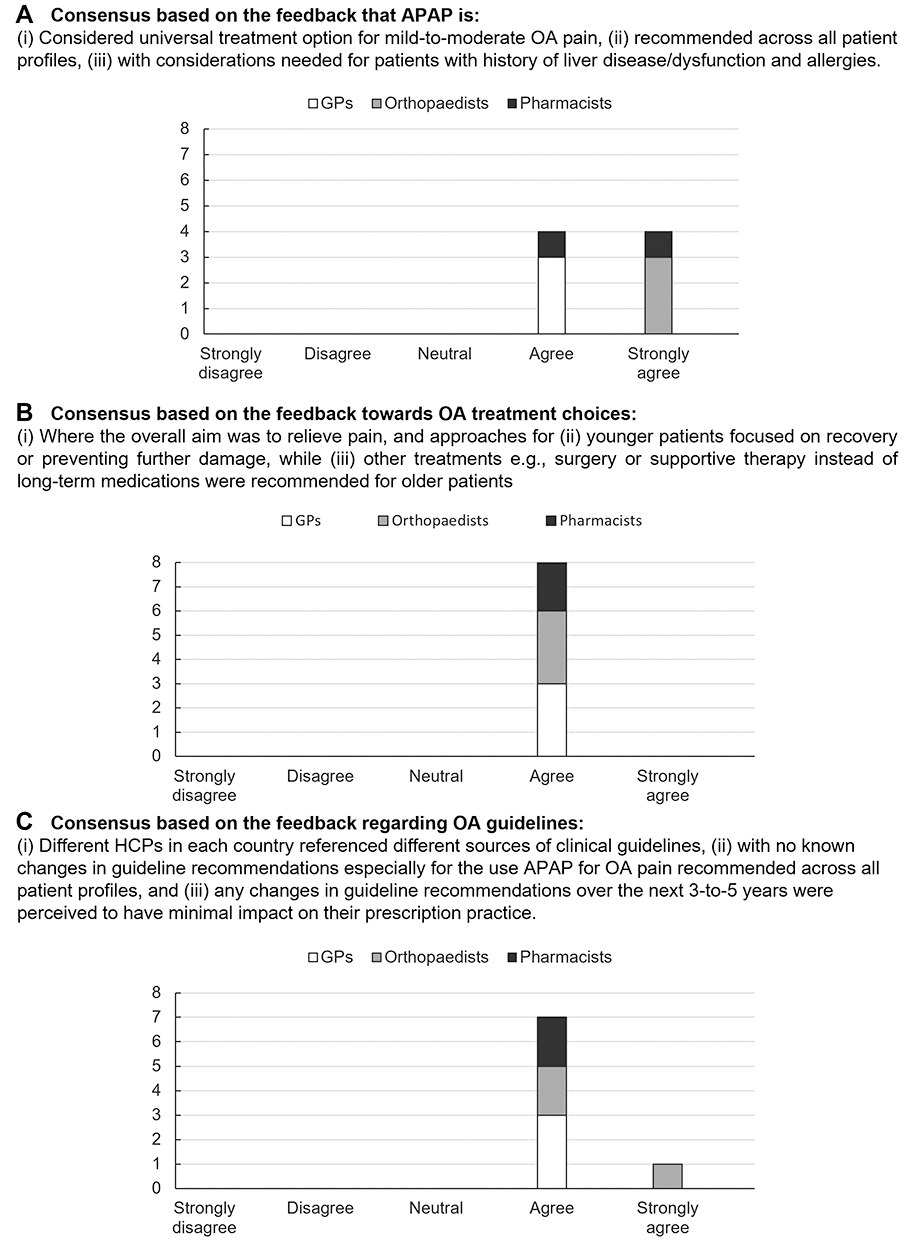 |
Figure 2 Consensus of the key findings pertaining to paracetamol (APAP), treatment choices, osteoarthritis (OA) guidelines among the panel of general practitioners (GPs) (n=3), orthopedists (n=3), and pharmacists (n=2). Proportion of panel members’ level of agreement or disagreement towards the feedback on (A) the relevance of APAP monotherapy for patients with mild-to-moderate OA pain, (B) relevance and AIM of different OA treatment options, and (C) awareness of OA guidelines and guideline updates. |
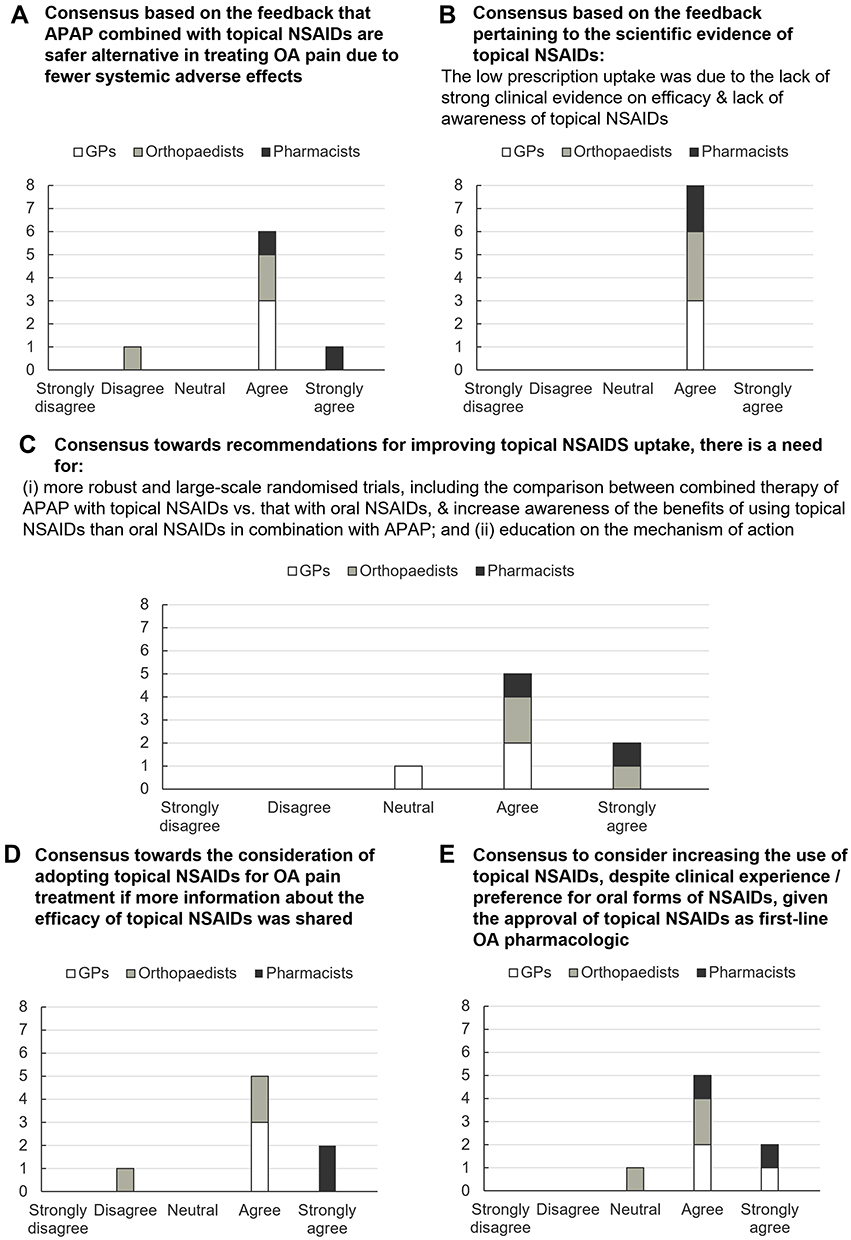 |
Figure 3 Consensus of the key findings pertaining to use of topical non-steroidal anti-inflammatory drugs (NSAIDs) as an adjuvant therapy with paracetamol (APAP) among the panel of general practitioners (GPs) (n=3), orthopedists (n=3), and pharmacists (n=2). Proportion of panel members’ level of agreement or disagreement towards feedback on (A) combined APAP therapy and topical NSAIDs as safer alternatives in OA management, (B) availability of strong scientific evidence on combined therapy of APAP with topical NSAIDs versus APAP with oral NSAIDs predisposed low prescription uptake of APAP combination therapy with topical NSAIDs efficacy, (C) recommendations for improving topical NSAIDs, (D) considerations to adopting topical NSAIDs for OA pain if more information was available, and (E) considerations to increasing use of topical NSAIDs based on clinical guidelines regardless of clinical experience/preference. |
HCP Panel Members Recruitment
Eligible GPs and orthopedists with ≥10 years of clinical experience and spent ≥60% of their time in direct patient care were invited to participate in this study. Preliminary screening criteria of eligible HCPs comprised having experience in treating mild-to-moderate OA or joint pain; have attended conferences or are members of medical societies, eg, pain societies; and have had relevant publications in pain management in peer-reviewed journals. Additional inclusion criteria included if GPs and orthopedists consulted ≥30 patients suffering from mild-to-moderate OA pain per month and treated ≥30% and ≥10% of these patients with APAP and combination treatment (including APAP with topical NSAIDs), respectively. Eligible pharmacists with ≥10 years’ senior pharmacist experience, who had permanent employment and spent ≥5 hours daily in direct patient contact were invited to participate. Additional inclusion criteria included monthly interactions with ≥30 patients with mild-to-moderate OA pain and having dispensed ≥30% and ≥10% of their patients with APAP and combination treatments (including APAP with topical NSAIDs), respectively. The profiles of the HCPs are detailed in Table 1.
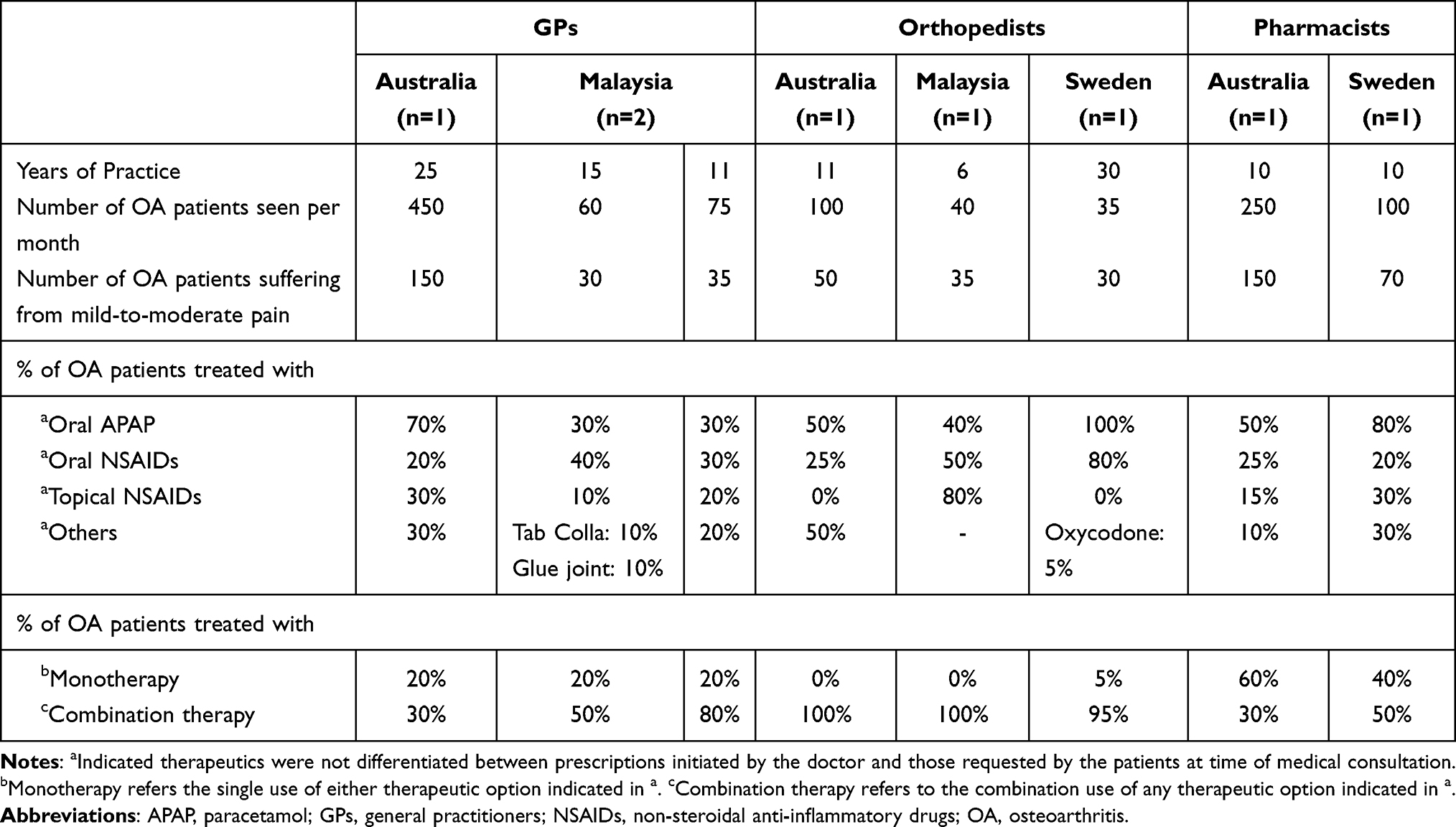 |
Table 1 Clinical Experience, Patient Load and Prescription Practice of General Practitioners (GPs), Orthopedists, and (Senior) Pharmacists in Australia, Malaysia, and Sweden |
Results
Prescribed Pharmacologic Treatment Pattern
The use of pharmacologic treatment options for managing mild-to-moderate pain in OA patients varied across different types of HCPs (Table 1). The GPs reported treating 30–70% of their patients with APAP, 10–20% with topical NSAIDs, and 30–80% with combination therapy, whereas orthopedists treated 40–100% of their patients with APAP, and 95–100% with combination treatment. Only one orthopedist prescribed topical NSAIDs to 80% of OA patients. The pharmacists had dispensed APAP and topical NSAIDs to 50–80% and 15–30% of their patients, respectively. Only 30–50% of their patients were dispensed with combination therapy.
Paracetamol for Mild-to-Moderate Osteoarthritis Pain Management
All panel members agreed or strongly agreed and regarded APAP as a universal pharmacologic option for most patient profiles, except for patients with contraindications or allergies (Figure 2A, Supplementary Table S1). Variations in the duration of prescription usage of APAP for OA pain management were observed across the three countries (Supplementary Table S1).
Treatment Choice for Mild-to-Moderate Osteoarthritis Pain Management
The overall aim for all HCPs was to relieve OA pain across all age groups, with different practices adopted to relieve OA pain in younger and older (aged >60 years) patients (Figure 2B).
Therapy regimens for younger patients often included recovery or preventing further damage through physiotherapy or exercise, while long-term medication prescription/dispensing, eg, oral NSAIDs were avoided for older patients or patients with comorbidities, preferring other supportive treatment regimens such as surgery depending on patient profile (Figure 2A, Supplementary Table S2).
In scenarios where OA pain was not effectively managed by APAP, all HCPs would add oral NSAIDs as an adjuvant to APAP due to better efficacy for relieving OA pain. However, cautionary use of this combination therapy was advised for patients with prior gastrointestinal (GI) issues, on comedications, prior liver dysfunction, or older age (≥65 years) (Supplementary Table S2).
Impact of Prescription Practice Towards Using Paracetamol Based on Osteoarthritis Guidelines
Regarding changes in OA guidelines towards use of APAP for managing pain, the panel members indicated a lack of awareness towards such changes in the guidelines’ recommendations. Additionally, any changes in guideline recommendations in the next 3-to-5 years were perceived to have minimal impact on their prescription practice (100% consensus) (Figure 2C, Supplementary Table S3).
Combination Therapy of Paracetamol and Topical Non-Steroidal Anti-Inflammatory Drugs for Mild-to-Moderate Osteoarthritis Pain
The panel (87.5% consensus) agreed that combination APAP therapy with topical NSAIDs was a safer alternative for managing OA than with oral NSAIDs (Figure 3A). One panel member disagreed on the safety profile of topical NSAIDs due to prior observations of patients presenting with adverse events, eg, skin blistering upon prior long-term usage of topical NSAIDs (Supplementary Table S4).
There was a lack of confidence in the combination use of APAP with topical NSAIDs among the panel members. All panel members agreed that the low prescription uptake of combination therapy of APAP with topical NSAIDs was due to lack of strong scientific evidence on the efficacy of combined therapy of APAP with topical NSAIDs versus APAP with oral NSAIDs (Figure 3B). There was also a perceived lack of awareness of the benefits and mechanism of action of topical NSAIDs (Figure 3C and D). The panel member with a neutral stance advised for additional investigations in scientific evidence to be conducted by independently and not by the manufacturing companies to add credibility of the evidence (Supplementary Table S4).
The majority (87.5%) agreed to consider increasing topical NSAIDs use in OA pain treatment, given the approval and use of topical NSAIDs as a first-line agent in OA treatment guidelines despite their preference for oral NSAIDs (Figure 3E). The panel member who disagreed would conditionally reconsider prescribing topical NSAIDs should more robust and convincing scientific evidence demonstrating the efficacy of topical NSAIDs in OA pain treatment be available (Supplementary Table S4).
Discussion
This study explored the perspectives of different types of HCPs towards using combination therapy of APAP and topical NSAIDs for managing mild-to-moderate OA pain based on their clinical expertise and with considerations to clinical OA guidelines update.
Emerging evidence on the small effect size of APAP for OA pain in clinical trials could be attributed to the high placebo effect.19 Despite initial indications APAP monotherapy may not provide clinically meaningful pain relief in all patients with OA, APAP remains universally accepted by physicians in real-life for managing mild-to-moderate OA pain. This was supported by all panel members, with considerations needed for patients with liver or GI comorbidities.12 Notably, the prescribing rate for combination therapy was highest among orthopedists (95–100%), followed by GPs (30–80%) and pharmacists (30–50%). This could be attributed to the severity of OA symptoms, where patients consulting with orthopedists may have more severe OA pain than those consulting with GPs or pharmacists.20 It is interesting to note that real-life practice indicates strong use of combination therapy with paucity of supporting scientific evidence.
Although the panel members were receptive towards the use of combination therapy of APAP with NSAIDs, there was a preference towards oral NSAIDs instead of topical NSAIDs. The most common reason for the low uptake of topical NSAIDs among the HCP panel in this study was due to the lack of awareness towards scientific evidence demonstrating the efficacy of topical NSAIDs. Furthermore, the available evidence comparing the efficacy of oral vs topical NSAIDs were perceived to be limited as the panel suggested the need for additional large-scale efficacy studies comparing NSAIDs delivered perorally and subcutaneously for OA pain.
Several studies demonstrating and comparing the efficacy and safety of topical NSAIDs with other forms of pharmacologics21–25 supported the shift of European- and US-based OA guidelines to include topical NSAIDs as first-line agents.10,23 Of note, the panel members were unaware of changes in guidelines’ recommendations for managing OA pain, which could be attributed to different OA guidelines with different therapeutic recommendations being referenced within the respective countries. For instance, two different guidelines, the American Academy of Orthopedic Surgeons (AAOS) and the MOHM OA guidelines were referenced in Malaysia; AAOS guideline recommended APAP monotherapy to improve pain and function in treating knee OA when it is not contraindicated,8 while MOHM recommended adjuvant use of topical NSAIDs with APAP.13 This suggests a need for standardizing guidelines for managing OA pain.
The findings found that the low prescription uptake of topical NSAIDs among the panel HCPs in this study could be associated with the lack of awareness and understanding towards how delivery of NSAIDs topically could effectively relieve OA pain. Topical NSAIDs play a role in antinociception and anti-inflammation. They inhibit cyclooxygenase enzymes (COX-1 and COX-2) and block arachidonic acid conversion to prostaglandin H2, the precursor of prostaglandins, prostacyclin, and thromboxanes which mediate inflammatory pain.26 This compliments APAP’s analgesic activity that is mediated by activation of serotonergic pathways which increases pain threshold.27 Additionally, studies not only pointed towards equivalent efficacy of topical over oral NSAIDs in rheumatic diseases21–24 but also an association with fewer risks of GI-related adverse effects than oral NSAIDs as they are absorbed via the skin into local tissues with minimal systemic exposure.21 Combination pharmacological effect of analgesics and anti-inflammatory with minimal GI side effects could meet the treatment needs of managing pain and inflammation associated with OA,26 reinforcing the need to educate HCPs on the suitability of the different forms of topical agents.
Overall, the findings suggest an opportunity to increase awareness of the suitability and potential benefit of adding topical NSAIDs to APAP for managing mild-to-moderate OA pain through education and alignment of OA clinical guidelines across different clinical practices/specialties and the mechanism of action of the combined use of topical NSAIDs with APAP.
Strengths of this study included using the Delphi technique to explore an aggregation of perspectives and indication of current clinical prescription practices towards using pharmacologic treatments such as APAP with or without adjuvant topical NSAIDs collected from a panel of different types of HCPs from different countries.
One limitation of this technique is associated with the sampling size of experts wherein a minimal criterion of having one expert for each HCP type was attempted to be fulfilled in each country. Whilst the diversity of experts in the panel could provide for a broader perspective of current clinical practice towards using pharmacologic treatments, the small sample size of each HCP type imposes a challenge to generalize the findings (including the prescribing rate of different OA treatment options as well as the awareness rate of the efficacy and available scientific evidence of combined APAP and topical NSAIDs) to a wider clinician population both locally and globally. As this is an exploratory study, the findings could only serve as an indication on the justification for further research into this line of enquiry with larger sample size of each HCP type.
Within the context of the scarcity of research as to treatment practices for mild-to-moderate OA pain, the study identified themes describing behavior in clinical practice for future modelling of behavioral studies. However, additional studies with a larger HCP sample size are warranted to evidence suggestions or recommendations for potential changes in clinical practice.
Conclusion
This study explored the receptiveness and current clinical practices among different types of healthcare professionals in various geographies towards using APAP monotherapy and combined therapy of APAP and topical NSAIDs for managing mild-to-moderate pain.
Oral paracetamol remains perceived by the panel as a gold standard for managing mild-to-moderate pain due to observations in real-world clinical settings despite scientific evidence demonstrating APAP high placebo effect. The perceived observed lack of awareness towards scientific evidence supporting the efficacy of topical NSAIDs as well as understanding of the mechanism of action could have hindered uptake of this treatment option. This is notwithstanding the updated recommendations in OA clinical guidelines for using topical NSAIDs in combination with APAP.
The findings suggest indications justifying the need for increasing the awareness of the suitability and potential benefits of using adjuvant topical NSAIDs to APAP for effectively managing mild-to-moderate OA pain. Further investigations are needed with larger datasets and more robust evidence on combination therapy of APAP with topical NSAIDs to validate this study’s findings.
Abbreviations
AAOS, American Academy of Orthopedic Surgeons; ACR, American College of Rheumatology; APAP, oral paracetamol; COX, cyclooxygenase enzymes; ESCEO, European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases; EULAR, European Alliance of Associations for Rheumatology; GPs, general practitioners; GI, gastrointestinal; HCPs, healthcare professionals; MOHM, Ministry of Health, Malaysia; NICE, National Institute for Health and Care Excellence; NSAIDs, non-steroidal anti-inflammatory drugs; OA, osteoarthritis; OARSI, Osteoarthritis Research Society International.
Ethics Approval and Declaration
No patients were involved in this study. The research team invited experts to participate in the research. All participants voluntarily participated in the research without coercion or reward. Only experts who had provided informed consent to participate in this study were included to complete the Delphi interviews and questionnaire. As agreed with the experts, the data was analyzed anonymously while respecting confidentiality and privacy and has not been shared with other parties. The content of the interview questions and questionnaire do not concern medical scientific research and there is no infringement of the participant’s physical and/or psychological integrity of the subject. This research was conducted as a market research survey to understand the perspectives of healthcare professionals towards the use of a fast-dissolving paracetamol formulation for managing pain relief. Therefore, no ethical approval from an Ethical Review Board was required as per the guidelines of the British Healthcare Business Intelligence Association (BHBIA) and the European Pharmaceutical Market Research Association (EphMRA).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by GlaxoSmithKline (GSK); the study sponsor (GSK) provided valuable support in project execution. Cerner Enviza received funding from GSK to conduct the study. The authors acknowledge the team from Cerner Enviza for supporting the development of the study (Mr James McManus and Dr Shikha Singh) and providing medical writing and editorial support (Dr Amanda Woo).
Disclosure
VS Sethi is an employee of GlaxoSmithKline (GSK). L Van der Laan, S Gupta, and KC Piros declare no conflict of interests.
References
1. Perrot S. Osteoarthritis pain: pathophysiology, diagnosis, and management. International Association for the Study of Pain; 2016. Available from: https://s3.amazonaws.com/rdcms-iasp/files/production/public/Content/ContentFolders/GlobalYearAgainstPain2/2016/FactSheets/English/13.%20Osteoarthritis%20Pain.pdf.
2. Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) results. Osteoarthritis —level 3 cause. Institute for Health Metrics and Evaluation; 2020Available from: https://www.healthdata.org/results/gbd_summaries/2019/osteoarthritis-level-3-cause.
3. Nakata K, Tsuji T, Vietri J, Jaffe DH. Work impairment, osteoarthritis, and health-related quality of life among employees in Japan. Health Qual Life Outcomes. 2018;16(64):1–11. doi:10.1186/s12955-018-0896-9
4. DiBonaventura M, da Costa GS, McDonald M, Sadosky A. Evaluating the health and economic impact of osteoarthritis pain in the workforce: results from the national health and wellness survey. BMC Musculoskelet Disord. 2011;12(83):1–9. doi:10.1186/1471-2474-12-83
5. Hawker GA. Osteoarthritis is a serious disease. Clin Exp Rheumatol. 2019;120(5):3–6.
6. National Institute for Health and Care Excellence. Osteoarthritis: care and management | clinical Guideline CG177; 2020.
7. Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, Hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27(11):1578–1589. doi:10.1016/j.joca.2019.06.011
8. American Academy of Orthopaedic Surgeons. Management of Osteoarthritis of the Knee (NonArthroplasty) Evidence-Based Clinical Practice Guideline; 2021. Available from: https://www.aaos.org/oak3cpg.
9. Primorac D, Molnar V, Matišić V, et al. Comprehensive review of knee osteoarthritis pharmacological treatment and the latest professional societies’ guidelines. Pharmaceuticals. 2021;14(3):205. doi:10.3390/ph14030205
10. Balmaceda CM. Evolving guidelines in the use of topical nonsteroidal anti-inflammatory drugs in the treatment of osteoarthritis. BMC Musculoskelet Disord. 2014;15(27):1–5. doi:10.1186/1471-2474-15-27
11. The Royal Australian College of General Practitioners. Guideline for the management of knee and Hip osteoarthritis (Second edition). East Melbourne, VIc: RACCP; 2018. Available from: https://www.racgp.org.au/FSDEDEV/media/documents/Clinical%20Resources/Guidelines/Joint%20replacement/Guideline-for-the-management-of-knee-and-hip-OA-2nd-edition.pdf.
12. Freo U, Ruocco C, Valerio A, Scagnol I, Paracetamol: NE. A review of guideline recommendations. J Clin Med. 2021;10(15):3420. doi:10.3390/jcm10153420
13. Malaysia Health Technology Assessment Section (MaHTAS). Management of osteoarthritis (Second Edition). Malaysia Health Technology Assessment Section (MaHTAS); 2013. Available from: https://www.moh.gov.my/moh/attachments/8933.pdf.
14. Jawad ASM. Analgesics and osteoarthritis: are treatment guidelines reflected in clinical practice? Am J Ther. 2005;12(1):98–103. doi:10.1097/00045391-200501000-00013
15. van den Heuvel J, Koning L, Bogers AJJC, Berg M, van Dijen MEM. An ISO 9001 quality management system in a hospital: bureaucracy or just benefits? Int J Health Care Qual Assur. 2005;18(5):361–369. doi:10.1108/09526860510612216
16. Yoo B, Choi SW, Lee MS, Moon HB. Treatment of knee osteoarthritis with Ketoprofen (Ketotop): a double-blind placebo-controlled randomized trial. J Korean Rheum Assoc. 2015;3(1):70–75.
17. Bruyère O, Honvo G, Veronese N, et al. An updated algorithm recommendation for the management of knee osteoarthritis from the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal diseases (ESCEO). Semin Arthritis Rheum. 2019;49(3):337–350. doi:10.1016/j.semarthrit.2019.04.008
18. Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/arthritis foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Rheumatol. 2020;72(2):220–233. doi:10.1002/art.41142
19. Zhang W. The powerful placebo effect in osteoarthritis. Clin Exp Rheumatol. 2019;120(5):118–123.
20. Musila N, Underwood M, McCaskie AW, Black N, Clarke A, van der Meulen JH. Referral recommendations for osteoarthritis of the knee incorporating patients’ preferences. Fam Pract. 2011;28(1):68–74. doi:10.1093/fampra/cmq066
21. Klinge SA, Sawyer GA. Effectiveness and safety of topical versus oral nonsteroidal anti-inflammatory drugs: a comprehensive review. Phys Sportsmed. 2013;41(2):64–74. doi:10.3810/psm.2013.05.2016
22. Zeng C, Doherty M, Persson MSM, et al. Comparative efficacy and safety of Acetaminophen, topical and oral non-steroidal anti-inflammatory drugs for knee osteoarthritis: evidence from a network meta-analysis of randomized controlled trials and real-world data. Osteoarthr Cartil. 2021;29(9):1242–1251. doi:10.1016/j.joca.2021.06.004
23. National Collaborating Centre for Chronic Conditions (UK). Osteoarthritis: national clinical guideline for care and management in adults. London: Royal College of Physicians (UK). National Institute for Health and Clinical Excellence: Guidance; 2008. Available from: http://www.ncbi.nlm.nih.gov/books/NBK48984/.
24. Rannou F, Pelletier JP, Martel-Pelletier J. Efficacy and safety of topical NSAIDs in the management of osteoarthritis: evidence from real-life setting trials and surveys. Semin Arthritis Rheum. 2016;45(4):S18–21. doi:10.1016/j.semarthrit.2015.11.007
25. Argoff CE, Gloth FM. Topical nonsteroidal anti-inflammatory drugs for management of osteoarthritis in long-term care patients. Ther Clin Risk Manag. 2011;7:393–399. doi:10.2147/TCRM.S24458
26. Altman RD. A rationale for combining Acetaminophen and NSAIDs for mild-to-moderate pain - PubMed. Clin Exp Rheumatol. 2004;22:110–117.
27. Anderson BJ. Paracetamol (Acetaminophen): mechanisms of action. Paediatr Anaesth. 2008;18(10):915–921. doi:10.1111/j.1460-9592.2008.02764.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.