")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 12
Perspective on the Budgetary Impact of FP/FORM pMDI on Treatment and Management of Exacerbation in Moderate-to-Severe Asthma Patients in Singapore
Authors Boisseau S, Qasuri M, Ho WT, Ghosh W, Hadjiat Y
Received 12 May 2020
Accepted for publication 2 September 2020
Published 6 October 2020 Volume 2020:12 Pages 567—577
DOI https://doi.org/10.2147/CEOR.S262267
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Giorgio Colombo
Sebastien Boisseau,1 Murtaza Qasuri,1 Weng Tong Ho,1 Wrik Ghosh,2 Yacine Hadjiat1
1Mundipharma Singapore Holding Pte Limited, Singapore; 2Costello Medical Singapore Pte Ltd, Singapore
Correspondence: Yacine Hadjiat
Mundipharma Singapore Holding Pte Limited, 12 Marina View, #22-01 Asia Square Tower 2, 018961, Singapore
Tel +65 65111165
Fax +65 65111167
Email [email protected]
Purpose: Reducing the risk of exacerbation is a long-term goal of managing moderate-to-severe asthma. The use of fluticasone propionate/formoterol fumarate dihydrate (FP/FORM) pressurized metered-dose (pMDI, Flutiform®), a type of inhaled corticosteroid (ICS) and long-acting β 2 agonist (LABA) fixed-dose combination, has been associated with lower oral corticosteroid-requiring exacerbation rates than other ICS/LABA fixed-dose combinations, fluticasone propionate/salmeterol xinafoate (FP/SAL) and budesonide/formoterol fumarate (BUD/FORM). This study presents the first budget impact analysis of drug and exacerbation management cost savings associated with the increased access to FP/FORM compared to the currently available ICS/LABAs for treating moderate-to-severe asthma in Singapore.
Patients and Methods: A budget impact model showed changes to annual drug and exacerbation costs over 5 years for patients with moderate-to-severe asthma in Singapore, following the inclusion of FP/FORM on a government subsidy list. The eligible patient population was identified based on national statistics data. Different treatment costs pertaining to the population were applied according to the usage data (IQVIA Singapore National Sales Data) for different scenarios. Drug costs were obtained from public-sector hospitals. Exacerbation management costs were obtained from literature searches.
Results: The analysis showed that increased access to FP/FORM as a result of switching from FP/SAL could help achieve drug (S$1,042,289) and exacerbation management (S$223,550) cost savings over 5 years. In the scenario where patients switched from BUD/FORM, greater drug (S$2,572,797) and exacerbation management (S$256,781) cost savings were observed over 5 years.
Conclusion: The analysis provides a perspective that the increased access to FP/FORM could help achieve drug and exacerbation cost savings for the treatment of moderate-to-severe asthma.
Keywords: ICS/LABA, asthma exacerbation, treatment cost, Flutiform®, Fluticasone/formoterol, reimbursement
Introduction
Asthma is a persistent global health issue. As of 2016, 339 million people were estimated to present with asthma, contributing to the global prevalence of 4.3% among younger adults aged 18–45 years.1,2 The Global Burden of Disease study reported that in 2016, asthma resulted in approximately 13 million years of life lived with disability and was ranked 16th leading cause of burden of disease globally.2 Furthermore, the age-standardized prevalence of asthma has been increasing since early 2000 and the number of patients with asthma is estimated to increase by 100 million by 2025, highlighting the increasing clinical burden of asthma.2,3
Currently, the long-term goal of asthma management is to reduce the risk of exacerbations.4 Frequent exacerbations have been reported to lead to increased risks of impaired quality of life, debilitation and mortality in asthma patients.5 Uncontrolled exacerbations pose a substantial economic burden, as exacerbations result in direct costs with physician visits, hospitalization and medications and indirect costs attributed to productivity loss. Previous economic evaluations in US and Europe have reported that compared with the mean annual direct and indirect costs per patient with controlled asthma (USD 178–USD 855), those of uncontrolled patients could go up to as high as USD 5,669.6–8 An economic evaluation in Spain has demonstrated that direct costs of managing exacerbations have been increasing over time, highlighting the urgent need for a more effective treatment at an affordable price.9
The Global Initiative for Asthma (GINA) currently recommends the use of inhaled corticosteroid (ICS) and long-acting β2 agonist (LABA) fixed-dose combination therapy to achieve optimal asthma control in patients with moderate-to-severe asthma.4 In clinical trials and real-world studies, fluticasone propionate/formoterol fumarate dihydrate (FP/FORM) pressurized metered-dose (pMDI) [Flutiform®, Mundipharma International Ltd, Cambridge, United Kingdom (UK)] has demonstrated comparable efficacy and safety with other ICS/LABA combinations including fluticasone propionate/salmeterol xinafoate (FP/SAL) pMDI (Seretide® Evohaler, GlaxoSmithKline, London, UK) and dry powder inhaler (DPI, Seretide® Accuhaler, GlaxoSmithKline, London, UK) and budesonide/formoterol fumarate (BUD/FORM) DPI (Symbicort®, AstraZeneca, Cambridge, UK).5,10–15 Notably, the use of FP/FORM is associated with a faster onset of bronchodilation, lower incidence of exacerbations and improved quality of life when compared with FP/SAL.11,12,16 In the absence of head-to-head trials, a pooled analysis comparing FP/FORM oral corticosteroid-requiring (OCS) exacerbation rates from two open-label trials and OCS exacerbation rates from similar cohorts for FP/SAL and BUD/FORM from three different meta-analyses demonstrated that the incidence of OCS exacerbations with FP/FORM was lower than FP/SAL and BUD/FORM (2.1% vs. 9.5% vs. 10.6%).5 This is further supported by real-world evidence from Europe showing that the use of FP/FORM results in a very low rate of severe exacerbation, improvements in lung function parameters, and overall improvements in physician- and patient-assessed satisfaction with efficacy of asthma control and tolerability from baseline.16,17 Furthermore, European studies reported that the use of FP/FORM was associated with a low asthma-related healthcare resource utilization and was shown to be cost-effective in clinical settings.17–19
Although these data imply the potential of FP/FORM in improving exacerbation control and subsequently reducing healthcare resource utilization in a clinical setting, widespread use of FP/FORM is limited by a lack of government reimbursement in many countries. Singapore has been ranked as an intermediate risk country for asthma prevalence.20 A pan-Asian survey including Singaporean patients reported that 73% of asthma patients experienced one or more exacerbations in the past year.21 Importantly, a substantial proportion of asthma patients in Singapore persistently present with poor prognosis including recurrent exacerbations, declining lung function and poor quality of life; this is reflected by the moderate-to-high mortality rate of asthma in Singapore, which is three times higher than that of other developed countries, suggesting that the currently available asthma medications fail to meet the need for effective prevention of exacerbations in Singapore.21 FP/FORM was approved for the treatment of asthma in individuals aged 12 years and above by the government agency for medical device and pharmaceutical regulations in Singapore, Health Science Authority (HSA) in 2014. There are two ICS/LABA combinations in the standard list of government-subsidized drugs as of 2019, and FP/FORM is not in that list yet.22,23 Recently, a budget impact analysis conducted from the Singapore payer perspective demonstrated that the inclusion of FP/FORM on a government subsidy list would potentially lead to significant drug cost savings if patients were switched over 5 years from the two ICS/LABA combinations currently subsidized in Singapore, FP/SAL or BUD/FORM.24 However, this model in 2018 did not consider the overall cost of treating exacerbations, and thus it is unknown if the inclusion of FP/FORM in the government subsidy list and subsequent improvements in exacerbation control would translate to a reduction in the financial burden of asthma management in a real-world setting.24
The objective of this study was therefore to conduct a budget impact analysis that takes into consideration the cost of FP/FORM and the listed ICS/LABAs in treating moderate-to-severe asthma exacerbation in Singapore.
Patients and Methods
Population
The population considered by the budget impact model was patients with moderate to severe asthma in Singapore. The eligible patient population was estimated using the Ministry of Health Statistics on the Singapore population and results from literature searches (Table 1). The model considered 2018 as Year 1 given that the complete data for 2019 were not currently available, and thus analyses utilized 2018 data as model inputs wherever possible. The expected annual growth rate of the eligible population was estimated using the IQVIA Singapore National Sales Data from 2016 to 2018.25 Hospital and polyclinic market growth rates were expected to be 5% and 20% per year, based on the 2016–2018 data. These rates were weighted according to units FP/SAL and BUD/FORM sold over 2018, to obtain an annual growth rate of 11% (Table S1). This growth rate was applied to each year in the model up to Year 5 (Table S2).
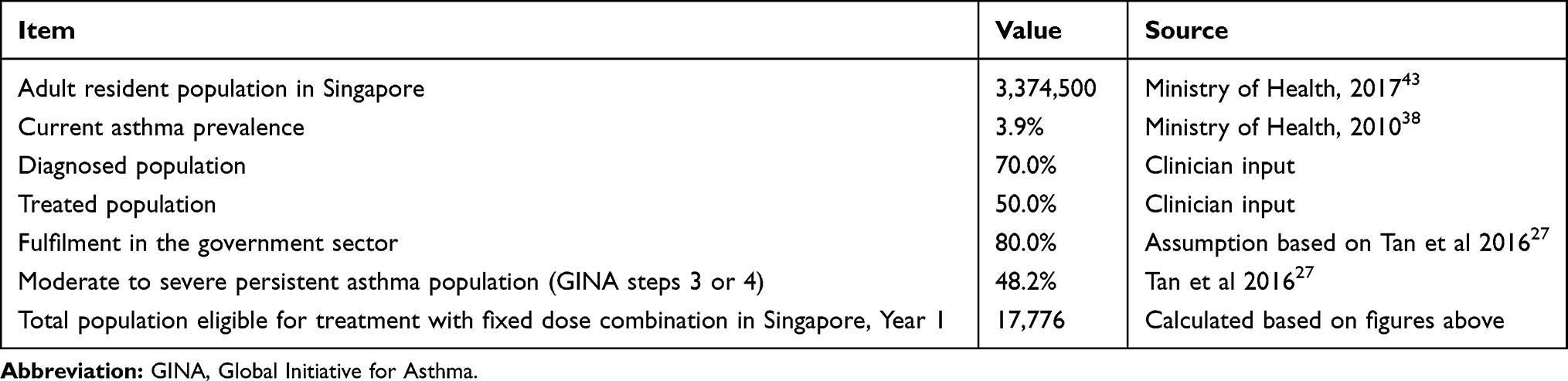 |
Table 1 Eligible Patient Population for Fixed Dose Combinations |
Comparators
In our model, the eligible patient population received ICS/LABA fixed dose combinations only, as per the GINA recommendations. The model considered ICS/LABA fixed dose combinations that are currently approved by the HSA and listed for a government subsidy, which were FP/SAL and BUD/FORM (Table 2). Currently, three doses of FP/FORM (low, medium and high) approved for the treatment of moderate-to-severe asthma in Singapore were included in the model. Similarly, three doses of FP/SAL pMDI and DPI that were approved and included on a government subsidy were considered as comparators in the model (Table 2). For BUD/FORM, three doses were approved for the treatment of asthma in Singapore.26 However, the low dose was not recommended for the treatment of severe asthma and the high dose was not recommended as a maintenance and reliever therapy regimen (ie treatment in response to symptoms).26 Therefore, a medium dose of BUD/FORM was selected as an appropriate comparator in the model. Fluticasone furoate/vilanterol was not considered as it is not currently included on a government subsidy.
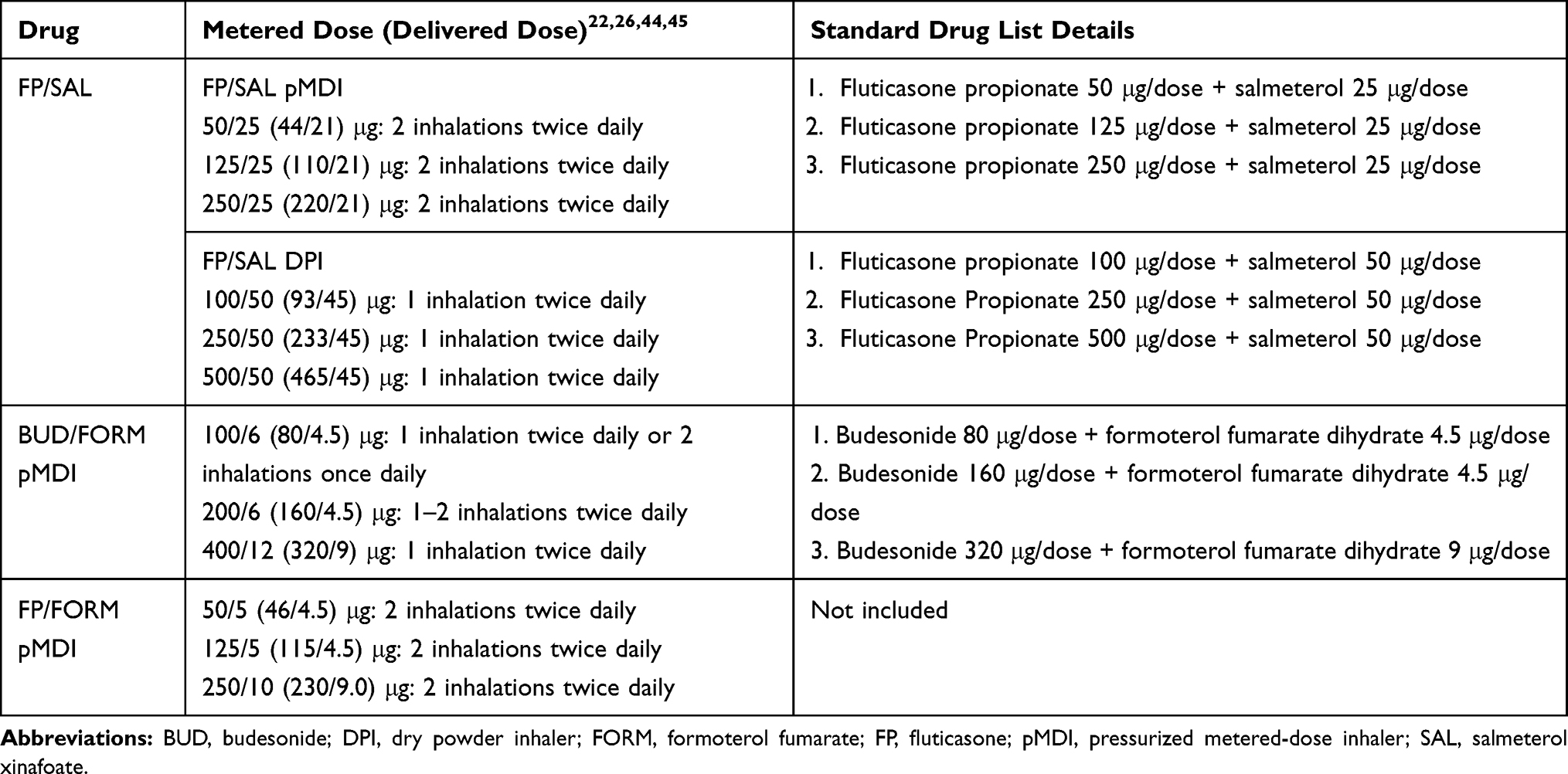 |
Table 2 List of ICS/LABA Fixed Combinations Included in the Model |
Analysis Approach
The model was built from a healthcare payer’s perspective, to demonstrate the change in drug and exacerbation costs over a time horizon of 5 years in the Singapore clinical setting. The time horizon of 5 years was chosen in line with what is recommended by the Agency for Care Effectiveness, which is Singapore’s national health technology assessment body. The base case predicted what would likely occur if there were no changes to access to FP/FORM as FP/FORM continued to be excluded from a government subsidy list. The base case usage data for FP/FORM, FP/SAL and BUD/FORM were projected based on the IQVIA sales data. There were two switch scenarios considered in the model, which were developed from the perspective that subsidy listing of FP/FORM would lead to its increased access resulting in patients with moderate-to-severe asthma switching from the comparators in Singapore. The first scenario predicted the change to drug and exacerbation costs if FP/FORM was included on a government subsidy list and its usage data subsequently increased as a result of patients switching from FP/SAL. The second scenario predicted the impact of a similar switch from BUD/FORM. The usage of FP/FORM, FP/SAL and BUD/FORM in the two switch scenarios are described in detail in the Usage Data section.
Model Inputs
Drug Costs
Unit costs for FP/FORM, FP/SAL, and BUD/FORM were calculated as the average of publicly available non-subsidized patient prices from public healthcare institutions in Singapore as of 2018 (Table 3). Annual drug costs were calculated assuming 100% adherence to the dosage approved by the HSA. Given that the units with 120 actuations require two inhalations twice daily, and the units with 60 actuations require one inhalation twice daily (Table 3), 12 units would be required in a year.
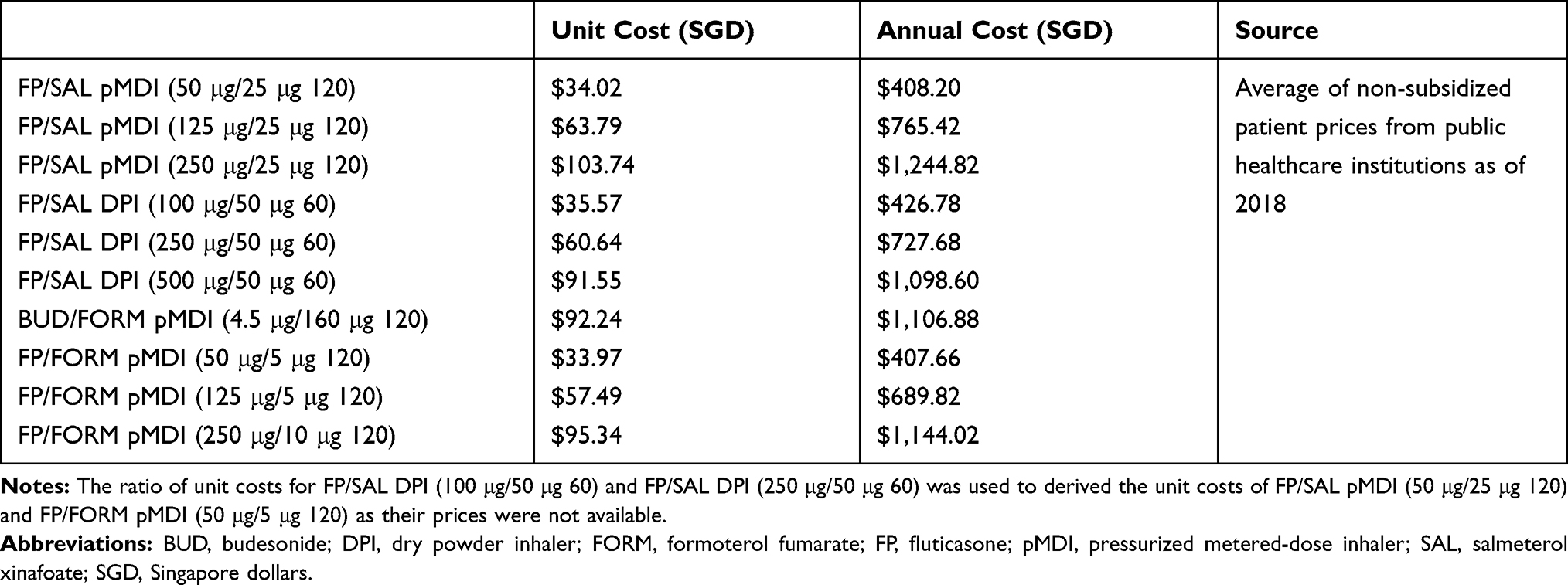 |
Table 3 Unit and Annual Costs of FP/SAL and BUD/FORM |
Exacerbation Management Costs
The proportion of patients with moderate to severe asthma with exacerbations was determined based on Tan et al 2016 which considered the GINA guidelines to categorize the asthma population in Singapore.27 Exacerbation management costs associated with FP/FORM, FP/SAL, and BUD/FORM were calculated by multiplying the incidence of OCS exacerbations with the number of patients with moderate-to-severe asthma who are uncontrolled on any ICS/LABA combinations, with the yearly costs associated with the management of these exacerbations in Singapore as of 2018 (Table 4). The rate of uncontrolled asthma among patients on any ICS/LABA was obtained from the Recognize Asthma and Link to Symptoms and Experience Asia (REALISE) study.28 The incidence of OCS exacerbations for FP/FORM, FP/SAL and BUD/FORM were taken from a meta-analysis (Figure 1), which compared the pooled incidence of OCS exacerbation rates from two open-label clinical trials of FP/FORM in adult and adolescent patients with asthma with rates of OCS exacerbation from similar cohorts for FP/SAL and BUD/FORM from three different Cochrane meta-analyses.5 Resource utilization for the following uncontrolled exacerbation implications were considered in the model: number of exacerbation-related hospitalizations, number of emergency department visits, number of visits to physicians in primary care, and number of specialist outpatient visits (Table 4).29 Based on clinician input, it was assumed in our model, that once a patient has had a visit to an emergency department or undergone hospitalization, the patient would likely be referred to an outpatient specialist. Healthcare costs associated with these implications were calculated as the average of costs reported by Singapore statistics, public institutions and polyclinics, and Nguyen et al 2017 (Table 4).29–35 Exacerbation costs were calculated per patient per year. The model assumed that asthma treatment using an ICS/LABA combination fixed-dose therapy would reduce the incidence of future OCS exacerbations thus lead to exacerbation cost savings across 5 years.
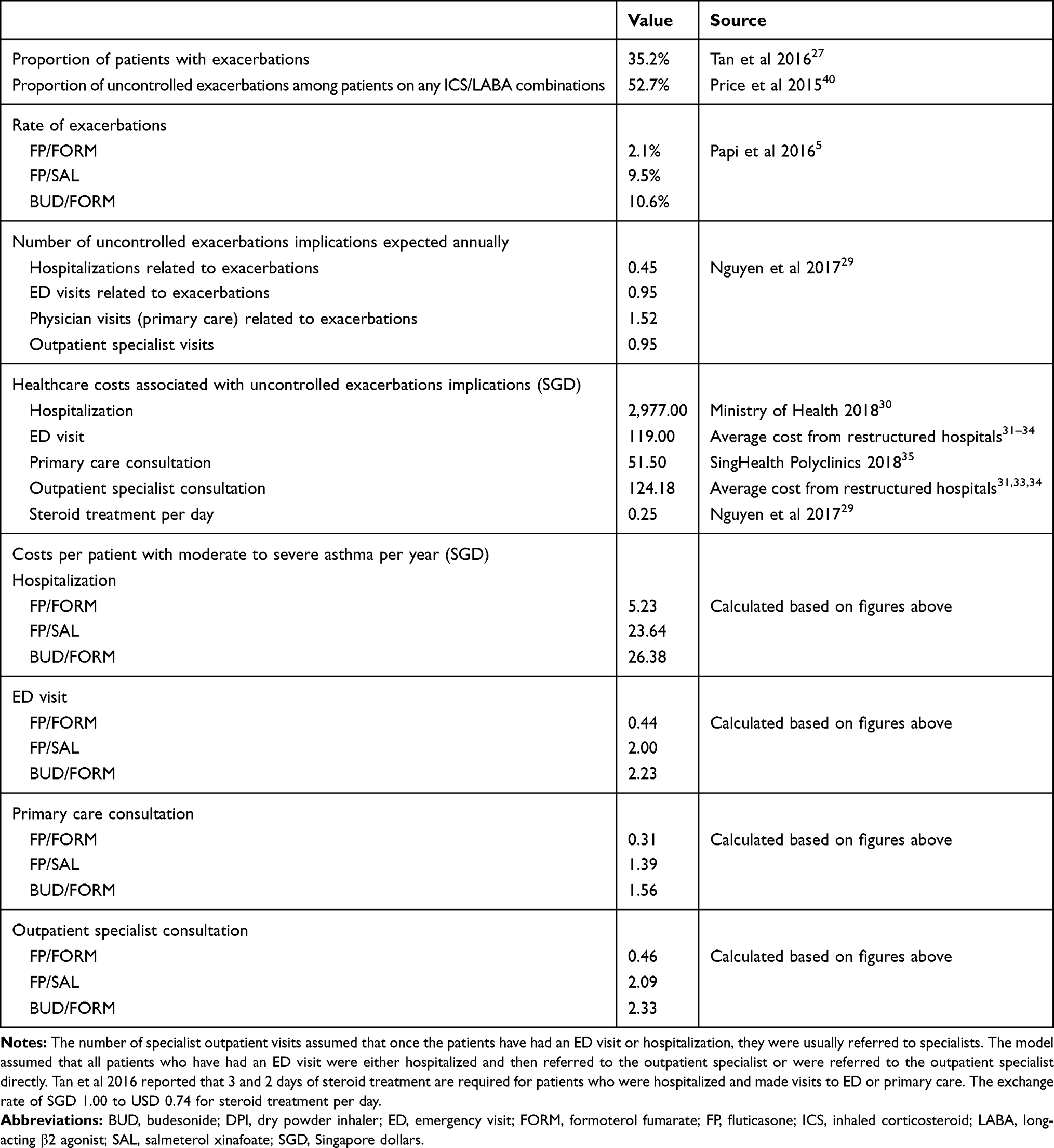 |
Table 4 Inputs for Exacerbation Management Costs |
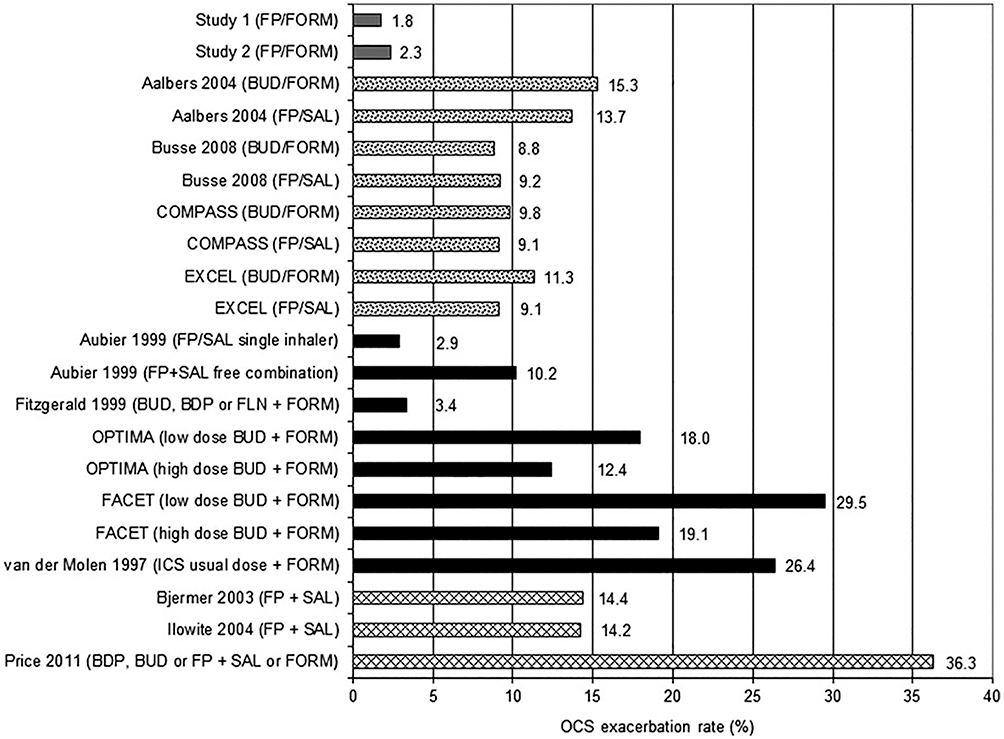 |
Figure 1 OCS exacerbation incidences for individual studies of ICS/LABA combinations. ICS/LABA OCS exacerbation rates are for studies 1 and 2, and in the individual studies as reported in the Cochrane by Lasserson et al, Mansur and Kaiser, Ducharme et al, and Chauhan and Ducharme. Notes: Grey bars represent the OCS exacerbation rates reported in open-label controlled trials of FP/FORM;46,47 white dotted bars represent the OCS exacerbation rates reported in studies from Lasserson et al 2011;48 black bars represent the OCS exacerbation rates reported in studies from Ducharme et al 2010;49 white checkered bars represent the OCS exacerbation rates reported in studies from Chauhan and Ducharme 2014.50 Reprinted with permission from Papi A, Mansur AH, Pertseva T et al. Long-Term Fluticasone Propionate/Formoterol Fumarate Combination Therapy Is Associated with a Low Incidence of Severe Asthma Exacerbations. J Aerosol Med Pulm Drug Deliv. 2016;29, 346–361. The publisher for this copyrighted material is Mary Ann Liebert, Inc. publishers.5Abbreviations: BDP, beclometasone; BUD, budesonide; FLN, flunisolide; FORM, formoterol fumarate; FP, fluticasone; ICS, inhaled corticosteroid; LABA, long-acting β2 agonist; OCS, oral corticosteroid; SAL, salmeterol xinafoate. |
Usage Data
For the base case, usage data for the comparators were determined using their IQVIA sales for asthma in Singapore from 2016 to 2018 (Table S3). The data presented sales from both private and public sectors, and it was assumed that the private sales of FP/SAL and BUD/FORM did not significantly affect the actual usage data in the public sector. The annual change in usage data was estimated based on the IQVIA data from 2016 to 2018. The usage data in 2018 were applied to Year 1 in the model. For the two switch scenarios, it was expected that the FP/FORM usage data would increase, as a result of being included for subsidy listing and subsequent increase its usage in the public sector (Table S4). The FP/SAL scenario assumed that the usage data of FP/FORM would increase as a direct result of a reduction in usage data of FP/SAL. Compared to FP/SAL, FP/FORM is associated with faster bronchodilation, reduced incidence of exacerbations and improved quality of life.5,11–14 These benefits would encourage patients to switch from FP/SAL to FP/FORM. Similarly, the BUD/FORM scenario assumed that the usage data of FP/FORM would increase as a result of decreasing BUD/FORM usage data. The BUD/FORM scenario assumed that a DPI would be displaced by a pMDI. The pMDI method has demonstrated a significantly higher drug deposition fraction to the central/peripheral airways compared with the DPI delivery method, which could support patients switching from BUD/FORM.36 In each scenario, it was assumed that the total usage data of FP/FORM and the comparator it was displacing would still match the usage data of the comparator it was displacing in the base case, for each of the years of the model. The expected usage data for FP/FORM in the switch scenarios were calculated based on projections of IQVIA sales data for the next 5 years (Table S4).
In order to evaluate the benefit of increased access to FP/FORM to the patient population in both scenarios, cost savings per patient was calculated by dividing the total drug and exacerbations costs by the number of eligible patients in each year.
Results
Base Case
The budget impact model estimated that in Year 1, 17,776 patients with moderate-to-severe asthma were estimated to be eligible for the treatment with ICS/LABA fixed-dose combinations.
Our model demonstrated that in the base case where access to FP/FORM remained unchanged, treatment of moderate-to-severe asthma per patient eligible for the fixed dose ICS/LABA combinations would cost $4,753 per patient over 5 years, and drug costs comprised 97% of the total cost savings (Tables 5 and 6).
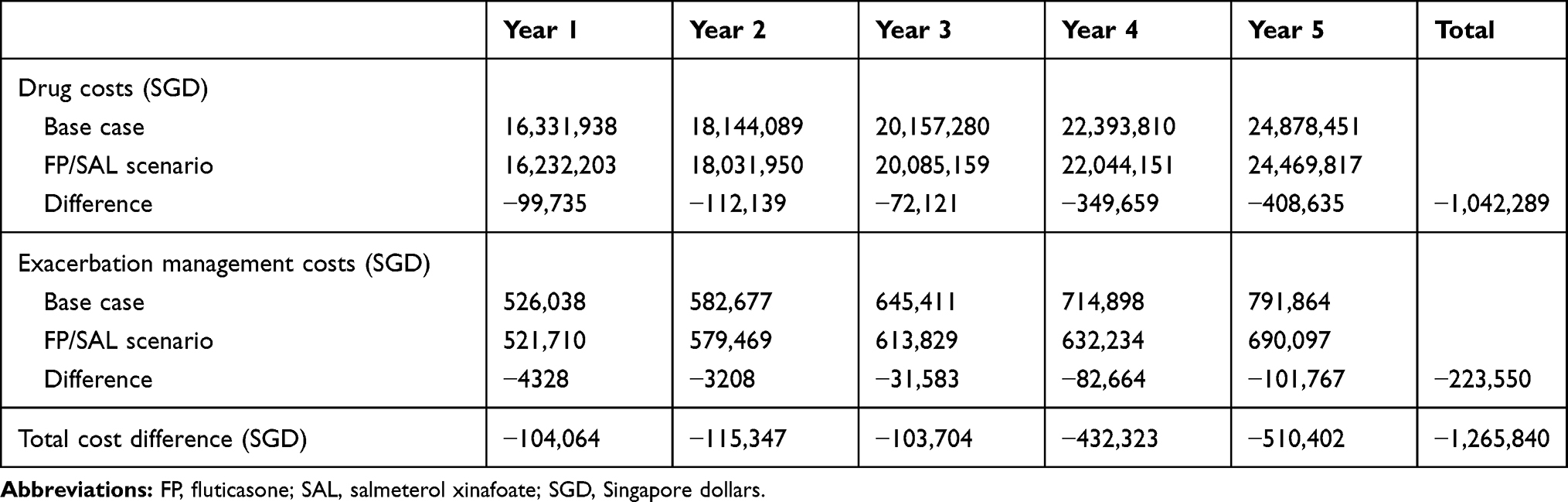 |
Table 5 Budget Impact Results Considering Switch from FP/SAL |
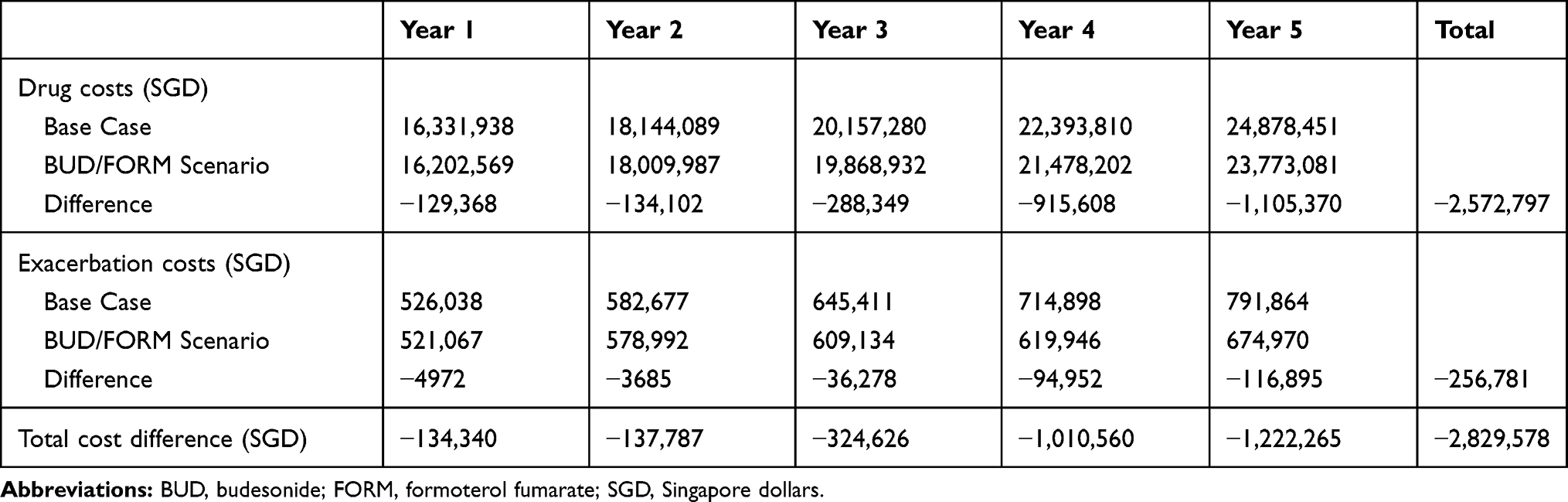 |
Table 6 Budget Impact Results Considering Switch from BUD/FORM |
Switch from FP/SAL and BUD/FORM
The switch scenarios were based on a perspective that recognized cost savings derived from increased access to FP/FORM for moderate-to-severe asthma patients in Singapore over a 5-year period, as a result of switching from the currently available treatment options in the standard list that were considered as comparators in the analysis. The model demonstrated that compared to the base case, increased access to FP/FORM upon patients switching from FP/SAL or BUD/FORM would lead to significant cost savings over 5 years (Tables 5 and 6). The greater cost savings per patient were achieved in the BUD/FORM scenario than in the FP/SAL scenario over 5 years ($116.36 vs. $53.19). In the model, drug cost savings comprised 82% and 91% of total cost savings in the FP/SAL and BUD/FORM scenarios, respectively (Tables 5 and 6).
The magnitude of both drug and exacerbation management cost savings increased over 5 years as an increased number of patients had access to FP/FORM over time in FP/SAL and BUD/FORM scenarios (Tables 5 and 6). In our model, total cost savings increased over 4-fold and 9-fold in FP/SAL and BUD/FORM scenarios over 5 years, respectively.
Over the 5-year period, the proportion of exacerbation management cost savings increased. In the FP/SAL scenario, exacerbation management cost comprised 4% of total cost savings in Year 1, which increased to 20% in Year 5. In the BUD/FORM scenario, the percentage of total cost difference due to a reduction in exacerbation management cost increased from 4% in Year 1 to 10% in Year 5.
Discussion
We present the first budget impact analysis of the drug and exacerbation management costs associated with the use of FP/FORM compared to the currently listed ICS/LABAs in the treatment of moderate-to-severe asthma in Singapore. In our study, the improved access to FP/FORM for patients with moderate-to-severe asthma resulted in significant drug and exacerbation management cost savings of $1.0–$2.6 million to the payer in the Singaporean clinical setting. These results can be explained by the established efficacy of FP/FORM in improving asthma control from baseline and low severe exacerbation rates associated with the use of this treatment. Indeed, exacerbation rates as low as 9.8% were reported in the largest real-world study of FP/FORM conducted in 2,539 asthma patients from 8 European countries.17 In our model, lower drug costs of FP/FORM compared to those of FP/SAL and BUD/FORM were the main drivers for cost savings. These tallied with the results of previous analyses in Spain and the UK, where the low drug cost of FP/FORM was the main driver for cost reductions.18,19 The impact of drug costs of FP/FORM was also reflected in the trends of cost savings upon increased access to FP/FORM in the switch scenarios. Our model predicted that there would be an increase in the use of the most expensive, high-dose FP/FORM in Year 3, explaining why the increase in the cost savings was not smooth over 5 years. The greater cost savings in the BUD/FORM scenario than that in the FP/SAL scenario were attributed to the higher drug costs of BUD/FORM than FP/SAL in Singapore. Furthermore, the total cost savings shown in the model was a conservative estimate, given that the usage data of FP/FORM increased to 20% only by Year 5 upon subsidy listing. This is in contrast to a small-cohort case study in Northern Ireland which reported that 88.3% of 53 patients successfully switched from FP/SAL to FP/FORM.37 A budget impact analysis in the UK also determined that FP/FORM share of 50% would be realistic usage data in a clinical setting.19
Apart from direct drug costs, our model demonstrated that the increased access to FP/FORM and subsequent improvements in exacerbation control would provide cost savings for the management of moderate-to-severe asthma in Singapore, further to previous evidence showing that the use of FP/FORM has been associated with a lower incidence of exacerbations compared to the use of FP/SAL or BUD/FORM.5 Similarly, previous real-world studies have shown that uncontrolled exacerbations were associated with increased healthcare resource use and subsequently an increase in healthcare costs.8,38–40 In Singapore, consultation fees were reported as one of the main drivers of asthma-related costs from 2004 to 2013.21,27 Our model therefore further emphasized the importance of FP/FORM’s enhanced control of exacerbation in improving the efficiency of healthcare resource utilization and reducing total costs of managing moderate-to-severe asthma. More real-world studies comparing the effect of FP/FORM on exacerbation control with other ICS/LABA combinations would help translate clinical benefits of FP/FORM into cost savings in clinical practice.
The model did not consider the potential indirect cost savings attributed to improved work productivity as a result of more effective exacerbation control with FP/FORM, suggesting that increased access to FP/FORM could result in additional cost savings generated from the quality of life in the real-world setting. In addition, FP/FORM is currently indicated for the treatment of asthma only, unlike FP/SAL and BUD/FORM which are indicated for the treatment of patients with severe chronic obstructive pulmonary disease and a history of repeated exacerbations. Therefore, the perspective of cost savings per patient as a result of increased access to FP/FORM was specific for the treatment of moderate-to-severe asthma only.
It is also worth noting that the exacerbation rates used in our analysis were derived from randomized controlled trials, which generally have more stringent eligibility criteria (e.g. exclusion of patients who smoke or have a history of smoking, or patients who have experienced an onset of exacerbations in the last 12 months prior to enrolment) than real-world studies. This might have resulted in seemingly lower exacerbation rates in patients receiving ICS/LABA combinations when compared with the rates reported in real-world studies.17,41 Also, in the real-world setting, confounding environmental factors such as suboptimal compliance could lead to less favorable exacerbation outcomes.
Our model has a number of limitations. Firstly, the estimation of the eligible population required several assumptions. Diagnosis and treatment rates of asthma were assumed due to a lack of evidence reporting these rates in the local clinical setting. Also, the entirety of the calculated eligible population was assumed to be treated with a fixed-dose combination treatment without any drop-out, and the annual growth rate of the population receiving the fixed-dose combinations was assumed to remain constant. These assumptions were validated by clinicians in Singapore through face-to-face discussions. Moreover, a few assumptions were made for usage data expectations upon including FP/FORM on government subsidy due to the nature of the IQVIA data. The IQVIA sales data used in the model were across all respiratory conditions without a further breakdown by disease, and thus, the model assumed that the disease-specific breakdown would not significantly change the results. Given that the IQVIA sales data were from both private and public sector sales, it was assumed that the inclusion of private sector sales would not significantly affect the usage data of FP/SAL and BUD/FORM. The usage data changes across 2016–2018 in the IQVIA data were used to derive the rate of annual usage data change in the model, and thus assumed that it would remain constant over 5 years, as there were insufficient data available to estimate the usage data changes. The percentages of switching from FP/SAL and BUD/FORM were assumed and validated by clinicians as there were insufficient local data available in Singapore. Lastly, the treatment pathway used in the model was based on the 2017 GINA guidelines, where an adjustment to steps 3 and 4 of treatment with low or medium-to-high dose of ICS/LABA fixed dose combinations was recommended for patients with moderate-to-severe asthma, whilst add-on treatment was recommended for step 5 of treatment.42 In the recently updated GINA guidelines, low-, medium- and high-dose ICS/LABA combinations were recommended for treatment steps 3, 4 and 5, respectively.4 Applying these changes to the GINA guidelines for the treatment of moderate-to-severe asthma will increase the number of patients prescribed with high-dose ICS/LABA combinations. Subsequently, more patients will switch to the most expensive, high-dose FP/FORM upon increased access to FP/FORM, and thus decrease the amount of cost savings that could be generated with the increased access to FP/FORM in Singapore due to higher drug costs. Our model had also excluded other treatments for moderate-to-severe asthma, such as biologics; future analyses including a wider range of treatment options may present a broader perspective of asthma management.
Conclusion
The budget impact model provided a perspective for the first time that increased access to FP/FORM would bring significant cost benefits for the treatment of moderate-to-severe asthma. With improved exacerbation control and lower drug costs, increased access to FP/FORM would provide a more effective and affordable treatment option for patients with moderate-to-severe asthma in Singapore. Based on the developed model and strong results, further research in other countries and health systems would help to substantiate findings on a larger scale.
Abbreviations
BUD, budesonide; DPI, dry powder inhaler; FORM, formoterol fumarate; FP, fluticasone; GINA, Global Initiative for Asthma; ICS, inhaled corticosteroid; HSA, Science Authority; LABA, long-acting β2 agonist; OCS, oral corticosteroid-requiring; pMDI, pressurized metered-dose inhaler; SAL, salmeterol xinafoate.
Data Sharing Statement
IQVIA Singapore National Sales 2016–2018 data were data on file and are not available for sharing.
Acknowledgments
The authors acknowledge support for third-party writing assistance for this article, provided by Min Hee Choi, PhD, Costello Medical Singapore Pte Ltd, Singapore, funded by Mundipharma Singapore Holding Pte Limited, Singapore in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3). The authors also acknowledge Dr Lim Hui Fang, National University of Singapore, Singapore, for providing and validating inputs required for the research. The authors thank Rohini Bose, PhD, from Costello Medical Singapore Pte Ltd, Singapore, for her guidance and support in the research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Mundipharma Singapore Holding Pte Limited.
Disclosure
Sebastien Boisseau, Murtaza Qasuri, Weng Tong Ho and Yacine Hadjiat are employees of Mundipharma Singapore Holding Pte Limited, Singapore. Wrik Ghosh was an employee of Costello Medical Singapore Pte Ltd, Singapore during the development of the model and manuscript. The authors report no other conflicts of interest in this work.
References
1. To T, Stanojevic S, Moores G, et al. Global asthma prevalence in adults: findings from the cross-sectional world health survey. BMC Public Health. 2012;12(1):204. doi:10.1186/1471-2458-12-204
2. Hay SI. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211–1259.
3. Masoli M, Fabian D, Holt S, Beasley R. The global burden of asthma: executive summary of the GINA dissemination committee report. Allergy. 2004;59(5):469–478. doi:10.1111/j.1398-9995.2004.00526.x
4. Global Strategy for Asthma Management and Prevention, 2019 [homepage on the Internet]. Global initiative for asthma; 2019. Available from: https://ginasthma.org/.
5. Papi A, Mansur AH, Pertseva T, et al. Long-term fluticasone propionate/formoterol fumarate combination therapy is associated with a low incidence of severe asthma exacerbations. J Aerosol Med Pulm Drug Deliv. 2016;29(4):346–361. doi:10.1089/jamp.2015.1255
6. Gold LS, Yeung K, Smith N, Allen-Ramey FC, Nathan RA, Sullivan SD. Asthma control, cost and race: results from a national survey. J Asthma. 2013;50(7):783–790. doi:10.3109/02770903.2013.795589
7. Accordini S, Corsico AG, Braggion M, et al. The cost of persistent asthma in Europe: an international population-based study in adults. Int Arch Allergy Immunol. 2013;160(1):93–101.
8. Doz M, Chouaid C, Com-Ruelle L, et al. The association between asthma control, health care costs, and quality of life in France and Spain. BMC Pulm Med. 2013;13(1):15. doi:10.1186/1471-2466-13-15
9. de Miguel-diez J, Jimenez-Garcia R, Hernandez-Barrera V, et al. National trends in hospital admissions for asthma exacerbations among pediatric and young adult population in Spain (2002–2010). Respir Med. 2014;108(7):983–991. doi:10.1016/j.rmed.2014.04.008
10. Bodzenta-Lukaszyk A, Buhl R, Balint B, Lomax M, Spooner K, Dissanayake S. Fluticasone/formoterol combination therapy versus budesonide/formoterol for the treatment of asthma: a randomized, controlled, non-inferiority trial of efficacy and safety. J Asthma. 2012;49(10):1060–1070. doi:10.3109/02770903.2012.719253
11. Bodzenta-Lukaszyk A, Dymek A, McAulay K, Mansikka H. Fluticasone/formoterol combination therapy is as effective as fluticasone/salmeterol in the treatment of asthma, but has a more rapid onset of action: an open-label, randomized study. BMC Pulm Med. 2011;11(1):28. doi:10.1186/1471-2466-11-28
12. Aalbers R, Brusselle G, McIver T, Grothe B, Bodzenta-Lukaszyk A. Onset of bronchodilation with fluticasone/formoterol combination versus fluticasone/salmeterol in an open-label, randomized study. Adv Ther. 2012;29(11):958–969. doi:10.1007/s12325-012-0058-0
13. Lim D, Small I, Wolfe S, et al. Real world effectiveness of changing fixed-dose combination therapy from seretide MDI to flutiform in UK asthma patients.
14. Lim D, Small I, Wolfe S, et al. Effectiveness of fluticasone-propionate/salmeterol vs fluticasone-propionate/formoterol in UK patients with asthma. Pragmat Obs Res. 2015;6:34–35.
15. Usmani OS, Kemppinen A, Gardener E, et al. A randomized pragmatic trial of changing to and stepping down fluticasone/formoterol in asthma. J Allergy Clin Immunol Pract. 2017;5(5):1378–1387.e1375. doi:10.1016/j.jaip.2017.02.006
16. Schmidt O, Petro W, Hoheisel G, Kanniess F, Oepen P, Langer-Brauburger B. Real-life effectiveness of asthma treatment with a fixed-dose fluticasone/formoterol pressurised metered-dose inhaler - results from a non-interventional study. Respir Med. 2017;131:166–174. doi:10.1016/j.rmed.2017.08.017
17. Backer V, Ellery A, Borzova S, et al. Non-interventional study of the safety and effectiveness of fluticasone propionate/formoterol fumarate in real-world asthma management. Ther Adv Respir Dis. 2018;12:1753466618796987. doi:10.1177/1753466618796987
18. Martínez-Moragón E, Delgado J, Ojeda P, et al. Economic evaluation of fluticasone propionate/formoterol fumarate (flutiform®) vs fluticasone/salmeterol and budesonide/formoterol in Spain. Value Health. 2015;18(7):A501. doi:10.1016/j.jval.2015.09.1417
19. Farrington E, Saunders A, Heron L, Dunlop W. FP/FORM versus FP/SAL within clinical practice: an updated budget impact analysis in asthma. Adv Ther. 2016;33(5):794–806. doi:10.1007/s12325-016-0317-6
20. The Global Asthma Report 2014 [homepage on the Internet]. The global asthma network; 2014. Available from: http://www.globalasthmareport.org/2014/about/executive.php.
21. Koh MS, Yii AC, Ong YY. Asthma in Singapore: past, present and future. Ann Acad Med Singapore. 2017;46(3):81–83.
22. Mundipharma Singapore Holding Pte Limited. Flutiform® Pressurised Inhalation, Suspension [Prescribing Information]. Singapore: Mundipharma Singapore Holding Pte Limited; 2014.
23. Drug Subsidies & Schemes [Homepage on the Internet]. Singapore: Ministry of Health; 2020. Available from: https://www.moh.gov.sg/cost-financing/healthcare-schemes-subsidies/drug-subsidies-schemes.
24. Boisseau S, Qasuri M, Ho WT, et al. Analysis of the inclusion of fluticasone propionate/formoterol on a government subsidy list in Singapore for the treatment of moderate-to-severe asthma. Value Health. 2018;21:S103–S104. doi:10.1016/j.jval.2018.07.785
25. IQVIA data on file. Singapore National Sales 2016–2018 (R03F); 2019.
26. AstraZeneca Pte Ltd. Symbicort® Turbuhaler® Inhalation Powder [Prescribing Information]. Singapore: AstraZeneca Pte Ltd; 2017.
27. Tan NC, Nguyen HV, Lye WK, Sankari U, Nadkarni NV. Trends and predictors of asthma costs: results from a 10-year longitudinal study. Eur Respir J. 2016;47(3):801–809. doi:10.1183/13993003.00188-2015
28. Price D, Fletcher M, van der Molen T. Asthma control and management in 8000 European patients: the REcognise Asthma and LInk to Symptoms and Experience (REALISE) survey. NPJ Prim Care Respir Med. 2014;24(1):14009. doi:10.1038/npjpcrm.2014.9
29. Nguyen HV, Bose S, Mital S, et al. Is bronchial thermoplasty cost-effective as treatment for problematic asthma patients? Singapore’s perspective on a global model. Respirology. 2017;22(6):1102–1109. doi:10.1111/resp.13027
30. Fee Benchmarks and Bill Amount Information [hompeage on the Internet]. Singapore: Ministry of Health; 2019. Available from: https://www.moh.gov.sg/cost-financing/fee-benchmarks-and-bill-amount-information.
31. Charges & Payment [homepage on the Internet]. Singapore: National University Hospital; 2019. Available from: https://www.nuh.com.sg/patients-visitors/Pages/Charges-Payment.aspx.
32. Hospital Charges [homepage on the Internet]. Singapore: Changi General Hospital; 2019. Available from: https://www.cgh.com.sg/patients-visitors/Pages/Hospital-Charges.aspx.
33. Outpatient Charges [homepage on the Internet]. Singapore: Singapore General Hospital: SingHealth; 2019. Available from: https://www.sgh.com.sg/patient-care/visiting-specialist/Pages/charges-payments.aspx.
34. Outpatient Charges [homepage on the Internet]. Singapore: Tan Tock Seng Hospital; 2019. Available from: https://www.ttsh.com.sg/Patients-and-Visitors/Your-Clinic-Visit/Pages/Outpatient-Charges.aspx.
35. Charges & Payment [hompage on the Internet]. Singapore: SingHealth Polyclinics; 2019. Available from: https://polyclinic.singhealth.com.sg/patient-care/charges-payment.
36. Iwanaga T, Kozuka T, Nakanishi J, et al. Aerosol deposition of inhaled corticosteroids/long-acting β2-agonists in the peripheral airways of patients with asthma using functional respiratory imaging, a novel imaging technology. Pulm Ther. 2017;3(1):219–231. doi:10.1007/s41030-017-0036-4
37. Hamill J, and Spyridon M. Real-world evidence on asthma review and change from fluticasone propionate/salmeterol to fluticasone propionate/formoterol.
38. National Health Survey 2010 [homepage on the Internet]. Singapore: Ministry of Health Epidemiology and Disease Control Division; 2011. Available from: https://www.moh.gov.sg/resources-statistics/reports/national-health-survey-2010.
39. Demoly P, Annunziata K, Gubba E, Adamek L. Repeated cross-sectional survey of patient-reported asthma control in Europe in the past 5 years. Eur Respir Rev. 2012;21(123):66–74. doi:10.1183/09059180.00008111
40. Price D, David-Wang A, Cho SH, et al. Time for a new language for asthma control: results from REALISE Asia. J Asthma Allergy. 2015;8:93–103.
41. Price D, Musgrave SD, Shepstone L, et al. Leukotriene antagonists as first-line or add-on asthma-controller therapy. N Engl J Med. 2011;364:1695–1707.
42. Global Strategy for Asthma Management and Prevention, 2017 [homepage on the Internet]. Global initiative for asthma; 2017. Available from: https://ginasthma.org/2017-gina/.
43. Annual Report 2017 [homepage on the Internet]. Singapore: Ministry of Health; 2017. Available from: https://www.moh.gov.sg/resources-statistics.
44. GlaxoSmithKline Pte Ltd. Seretide® Accuhaler® (salmeterol/fluticasone propionate) inhalation powder [prescribing information]. Singapore: GlaxoSmithKline Pte Ltd; 2016.
45. GlaxoSmithKline Pte Ltd. Seretide® Evohaler® (salmeterol/fluticasone propionate) inhalation aerosol [prescribing information]. Singapore: GlaxoSmithKline Pte Ltd; 2016.
46. Kaiser K. and Pertseva T. Long-term safety and efficacy of fluticasone propionate/formoterol fumarate combination therapy in patients with asthma. Prim Care Respir J. 2013;22:A1–A18.
47. Mansur AH, and Kaiser K. Long-term safety and efficacy of fluticasone/formoterol combination therapy in asthma. J Aerosol Med Pulm Drug Deliv. 2013;26(4):190–199. doi:10.1089/jamp.2012.0977
48. Lasserson TJ, Ferrara G, and Casali L. Combination fluticasone and salmeterol versus fixed dose combination budesonide and formoterol for chronic asthma in adults and children. Cochrane Database Syst Rev. 2011;12. doi:10.1002/14651858.CD004106
49. Ducharme FM, Ni Chroinin M, Greenstone I, and Lasserson TJ. Addition of long-acting beta2-agonists to inhaled steroids versus higher dose inhaled steroids in adults and children with persistent asthma. Cochrane Database Syst Rev. 2010;4. doi:10.1002/14651858.CD005533
50. Chauhan BF, and Ducharme FM. Addition to inhaled corticosteroids of long-acting beta2 agonists versus antileukotrienes for chronic asthma. Cochrane Database Syst Rev. 2014;1. doi:10.1002/14651858.CD003137.pub5
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.