")
Back to Journals » Patient Preference and Adherence » Volume 15
Personalized and Patient-Centered Strategies to Improve Positive Airway Pressure Adherence in Patients with Obstructive Sleep Apnea
Authors Watach AJ , Hwang D, Sawyer AM
Received 17 March 2021
Accepted for publication 23 June 2021
Published 12 July 2021 Volume 2021:15 Pages 1557—1570
DOI https://doi.org/10.2147/PPA.S264927
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Alexa J Watach,1,2 Dennis Hwang,3 Amy M Sawyer2,4
1Division of Sleep Medicine, Department of Medicine, University of Pennsylvania, Philadelphia, PA, USA; 2School of Nursing, University of Pennsylvania, Philadelphia, PA, USA; 3Kaiser Permanente Southern California, Sleep Medicine and Department of Research and Evaluation, Fontana, CA, USA; 4Corporal Michael J. Crescenz Veterans Affairs Medical Center, Philadelphia, PA, USA
Correspondence: Alexa J Watach
University of Pennsylvania, School of Nursing, Claire Fagin Hall, Rm 349, 418 Curie Blvd, Philadelphia, PA, 19104, USA
Tel +1-717-599-9908
Email [email protected]
Abstract: Obstructive sleep apnea (OSA), a common sleep disorder characterized by repeated pauses in breathing during sleep, is effectively treated with positive airway pressure (PAP) therapy. The magnitude of improvements in daily functioning and reduced negative health risks are dependent on maintaining PAP adherence, which is a significant challenge. Evidence-based interventions to improve PAP use are not easily translated to clinical practice because they are labor-intensive and require specialty expertise. Further, to date, individualized care, inclusive of personalized medicine and patient- and person-centered care have been marginally incorporated in the field’s understanding of OSA and PAP adherence. This integrative review describes current PAP adherence assessment processes, interventions to improve adherence, and outlines future opportunities to advance the field, particularly as it relates to individualizing care and the use of implementation science to apply evidence to practice.
Keywords: patient preference, patient-centered care, implementation science, precision health, health behavior
Introduction
Obstructive sleep apnea (OSA) is a common sleep disorder, characterized by repeated pauses in breathing during sleep. It is a chronic condition affecting nearly one billion adults worldwide, with nearly half requiring treatment based only on OSA severity.1 An OSA diagnosis is established using either a home sleep apnea test or in-laboratory sleep testing,2 providing an objective measure of obstructive breathing events. OSA is defined by the presence of at least five obstructive respiratory events per hour of sleep and the presence of symptoms such as daytime sleepiness, snoring, witnessed breathing interruptions, awakenings due to gasping or choking, resistant hypertension, or reduced sleep-related quality of life.2,3 Daytime sleepiness is often prioritized due to immediate safety risks, as individuals with untreated OSA are 243% more likely to have a motor vehicle accident than drivers without OSA.4–6 In addition to excessive daytime sleepiness7 and increased risk of motor vehicle accidents,5,8 untreated OSA is associated with additional adverse daytime symptoms including impaired cognitive performance,9–11 and mood disturbances.12–14 It is also associated with negative health consequences, including cardiovascular disease and hypertension,15,16 diabetes,17–19 stroke,20,21 and death.21–23
Positive airway pressure (PAP) therapy is an efficacious treatment for OSA.24 Various types of PAP devices include continuous positive airway pressure (CPAP), auto-titrating positive airway pressure (APAP), and bi-level positive airway pressure (bi-level PAP). The appropriate device type is selected based on a variety of OSA characteristics; however, the specifics of device selection are beyond the scope of this paper (see Brown & Javaheri, 2017).25 All types of PAP, however, deliver pressurized air into the airway to prevent the collapse or blockage of the airway, as caused by OSA. This requires the individual with OSA to wear a mask while asleep, during all sleep bouts, in order to prevent apneic episodes. Adherence to therapy is critical for improved patient reported outcomes including sleepiness24,26–28 and quality of life and function.24,29 Incidence of associated comorbidities such as hypertension,30–32 stroke,33,34 and insulin resistance,35,36 may also be reduced by PAP and a dose–response effect has been suggested for these improvements.27,37–39 The magnitude of these improvements and reduced risk are in part dependent on adherence to PAP. This has been a persistent obstacle for the sleep field.40
PAP treatment is behaviorally based and requires the individual with OSA to wear PAP every night. This is often a long-term commitment to treatment as no alternative OSA treatments have equivalent efficacy, particularly for moderate to severe disease.2,41 Therefore, PAP adherence and the operationalization of strategies to promote PAP adherence are critical. As both evidence-based strategies for promoting adherence and future recommendations from the sleep field are discussed herein, an integrative review approach is utilized to present the current state of the science.42 The objective of this integrative review is to describe PAP adherence assessment, adherence promotion strategies, and discuss future opportunities to advance the field, particularly as it relates to the application of personalized medicine, patient-centered care and implementation science.
Assessing PAP Adherence
Sleep medicine is at a major advantage when it comes to capabilities of tracking and monitoring treatment adherence. PAP efficacy (residual breathing events on treatment), hours of use, mask leaks, and a number of flow signals are captured and recorded by the PAP device.43 This data is downloaded from a smart card on the PAP device, or, more commonly with emerging technologies and newer devices, transferred to a cloud database via Wi-Fi or cellular connection.44 The objective, near real-time usage and effectiveness data is accessed remotely by both providers and patients. This affords patients the opportunity to track their own nightly usage on the device as well as on their smartphone, as many device manufacturers offer a companion app (eg, myAirTM [ResMed Corp., San Diego, CA, USA] or DreamMapper [Philips Respironics, Monroeville, PA, USA]). Patient engagement by self-monitoring, an influential factor for PAP adherence behavior,45–47 is presumably “standard” care with the availability of these apps, but patients must choose to utilize them. Further, remote monitoring capabilities are especially beneficial to providers and researchers, as information technology platforms are designed to risk-stratify individuals struggling to meet adherence thresholds.48,49 This has the potential to support cost-effective clinical care by enabling “management by exception” (MBE) follow-up processes. This process concentrates provider effort on patients most at need by allowing providers to passively observe successful users and actively intervene with PAP strugglers.49,50 Other interventions to promote adherence are discussed later in this review.
The ability to remotely and objectively monitor adherence is not without some negative consequence. Insurance coverage for PAP is commonly contingent upon meeting objective PAP adherence metrics set forth by the Centers for Medicare and Medicaid Services, defined as PAP usage at least 4 hours per night on at least 70% of nights within a 30-day period.51 A failure to meet this criteria within a 90-day trial period can result in loss of insurance coverage for PAP, necessitating out-of-pocket costs to continue treatment, requalification for a new PAP prescription by a healthcare provider, or treatment forfeiture. This strict and arbitrary criteria is problematic, as it results in patients not being treated at all rather than being partially treated.44 Though findings of dose–response studies are inconsistent in determining the exact amount of PAP required to reduce cardiovascular and metabolic comorbidities,52–55 evidence suggests that longer nightly use is associated with better functional outcomes such as daytime sleepiness and quality of life.27,39 A recent meta-analysis suggests that although large trials have failed to find significant associations between PAP therapy and improved cardiovascular outcomes, this is potentially a result of poor PAP use and adherence among trial participants.56 Post hoc analyses indicate that there are significant decreases in major cardiovascular events and all-cause mortality in patients wearing PAP for more than four hours per night.56 Assessment and monitoring of PAP use is but one step in the process of treating OSA with PAP. The bigger hurdle exists in the promotion, early uptake, and sustained use of PAP for individuals with OSA.
Promoting PAP Adherence
While predicting adherence to a behaviorally based treatment is complex, PAP use within the first week is robustly predictive of long-term PAP use.57–61 This importantly highlights the need for early intervention in order to potentiate adherence in the long term. Minimizing negative early experiences by addressing barriers and PAP intolerance may improve PAP acceptance and adherence, thereby avoiding abandonment or suboptimal adherence to PAP.43 Clinical guidelines suggest ensuring proper mask fit to reduce negative side effects such as air leak and discomfort and the use of humidification to reduce side effects such as dry mouth/throat or nasal congestion to improve comfort and improve adherence.2 In addition to these suggestions, there is a growing body of research investigating interventions to promote PAP adherence.24,28,62,63 These interventions have been categorized as educational, supportive, behavioral, or technological in nature, each supporting approximately one hour per night increases in PAP use within the short term (ie, 3–12 months; see Table 1).24,28,45,62 While these types of interventions are beneficial for increasing PAP use, this set of evidence has simultaneously been criticized for interventions that are not readily translatable to practice. Most interventions require substantial resources or specialized personnel not commonly available outside of a clinical trial environment and are therefore of less value for addressing PAP non-adherence clinically on a larger scale.64
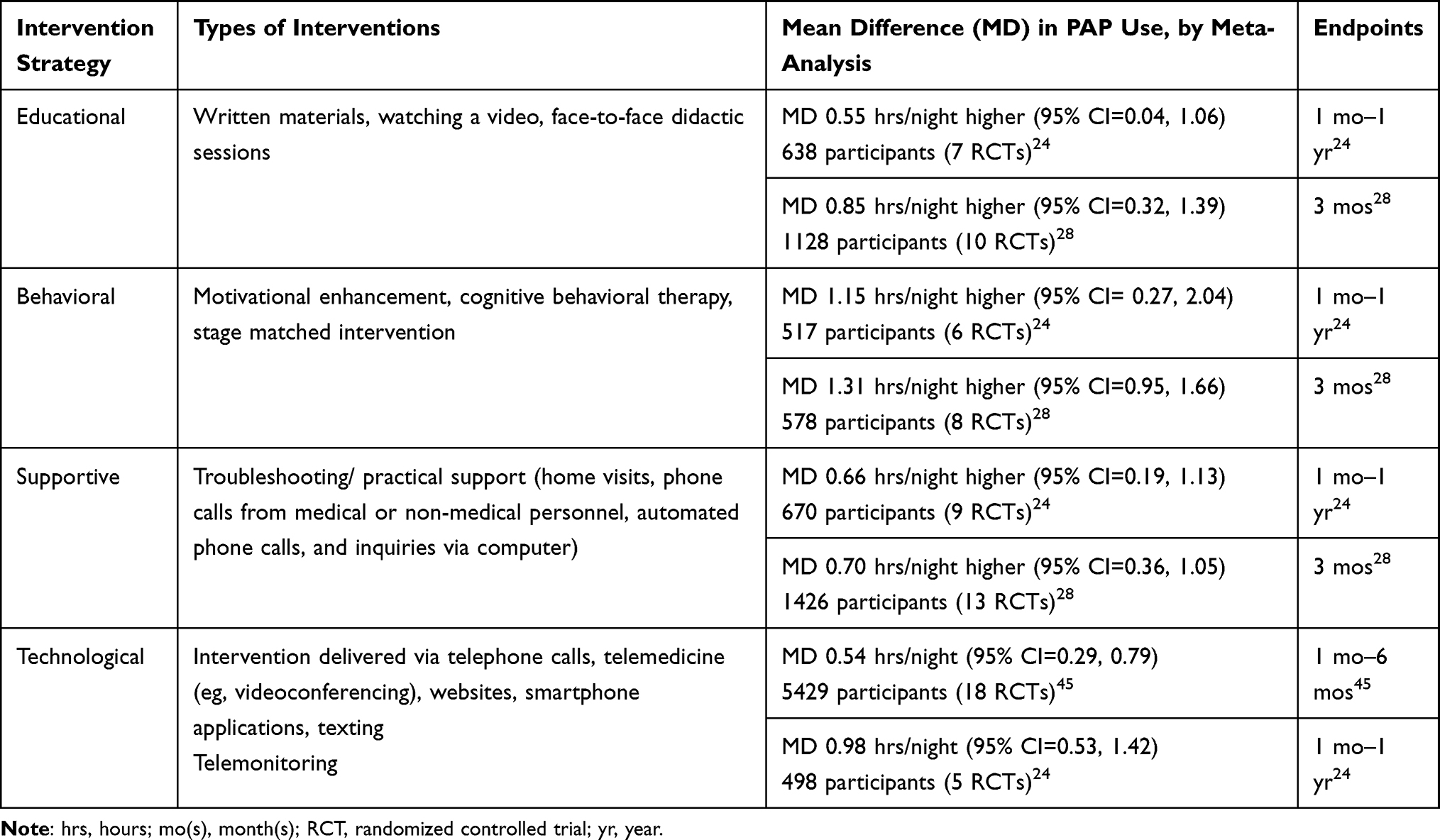 |
Table 1 Positive Airway Pressure (PAP) Adherence Interventions |
Many factors interact to predict PAP adherence,26,63,65 and many tested interventions have been designed and developed based on factors known to influence adherence such as experienced side effects (eg, skin irritation, dryness in the nose or mouth, and abdominal bloating)65 and psychosocial factors (eg, skills at coping with challenging situations, mental health, self-efficacy, and social support).26,63,65,66 However, some risk factors for nonadherence are non-modifiable, such as patient characteristics (eg, age, race, socioeconomic status),26,63,66 and disease characteristics (eg, symptom severity, OSA severity, mask type).63,67 To date, individualized care, inclusive of personalized medicine and patient- and person-centered care, has only marginally made its way into developing a deeper understanding of OSA and PAP adherence.44,48,68 Rather than pursuing a “one size fits all” approach to improving PAP adherence, further information on OSA risks, varied characteristics of OSA presentation, and patient preference could markedly enhance the availability of more individualized approaches that may be more promising with regard to effectiveness and scalability.69
Individualized Care
Personalized medicine and patient- and person-centered care are three care concepts seeking a similar goal—individualized health care for each patient.70–72 These individualized approaches place patients at the pinnacle of care, but differ in their core components and defining characteristics. Personalized medicine stems from a more biomedically based framework; determining who is at risk for disease, preventing disease, personalizing treatment, and involving patient participation. The goal of patient-centered care is focused on meeting patient’s needs by understanding patient values and preferences and promoting patient engagement and shared decision-making with an overall focus on functional life for the patient.70–72 Person-centered care broadens and extends the goals of patient-centered care to consider the whole life of the patient, beyond the impact of disease.70–72 See Table 2 for brief examples of how each of these individualized approaches to health care can be operationalized in OSA/PAP care. Implications for the use of personalized medicine and patient-centered care in sleep medicine have been previously published.44,48,68,69,73,74 This review brings into focus the opportunity to apply personalized medicine and patient-centered care to the promotion of PAP adherence.
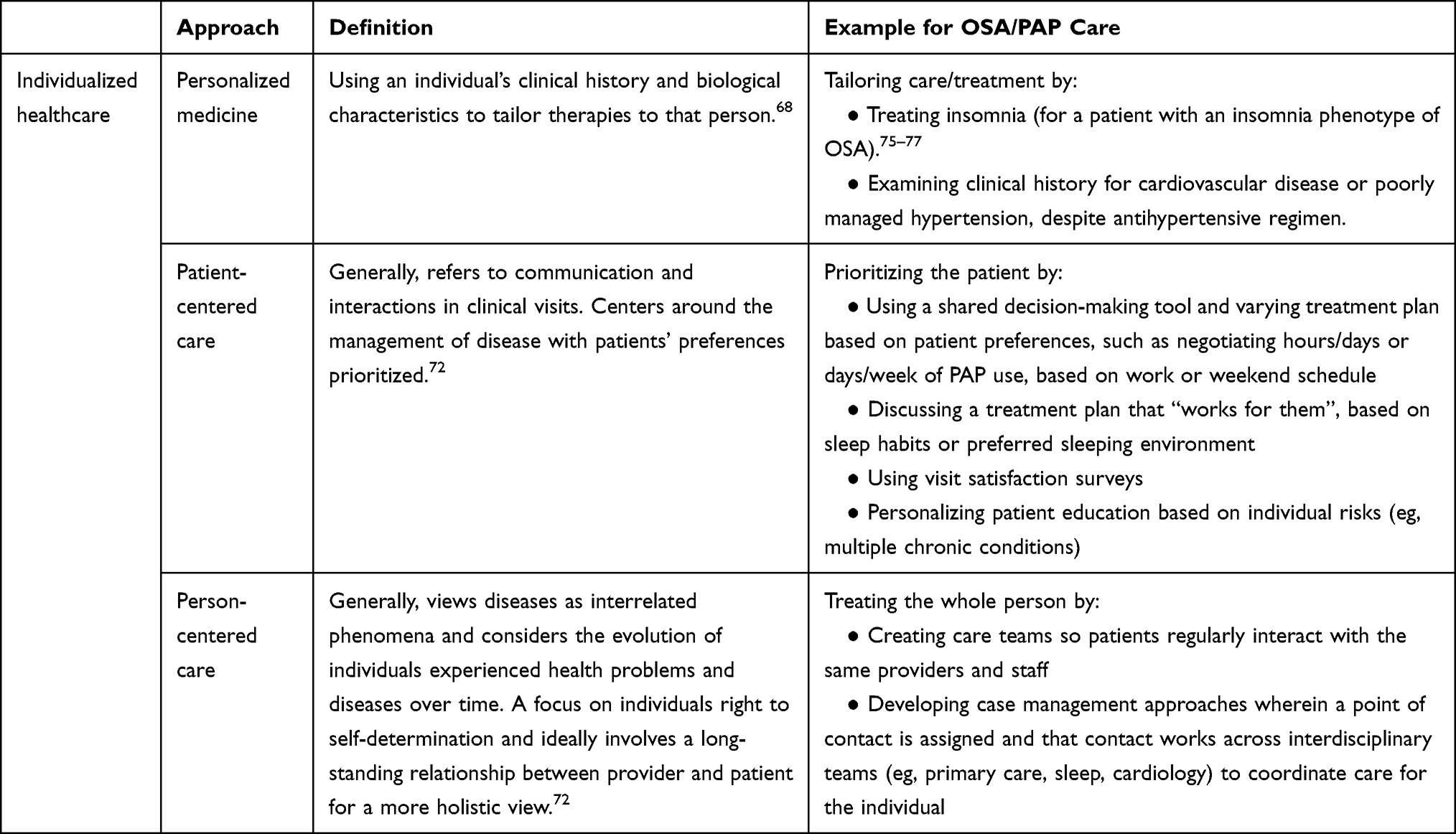 |
Table 2 Individualized Health Care Approaches and Applications |
Personalized Medicine
Personalized medicine approaches consider individual differences that are influential in the diagnosis and treatment of disease.68 “P4 medicine” is an approach to medicine that includes (1) predicting who will develop disease and comorbidities, (2) preventing disease rather than reacting, (3) personalizing diagnosis and treatment, and (4) patient participation in their own care.48,68,78,79 With regard to PAP adherence, personalization and patient participation are of particular relevance in this P4 medicine model.
OSA has historically been defined and treated according to disease severity based on the apnea hypopnea index.68 However, a shift in this approach may be necessary to promote adherence, as clinical subgroups of patients with OSA present with varied clinical phenotypes.68 Three distinct subgroups emerged to date, include (1) patients with insomnia complaints, (2) largely asymptomatic patients with cardiovascular comorbidities, and (3) excessive daytime sleepiness patients.48,80 Phenotypic presentations may result in patients having varied individual needs, preferences, and values that have important therapeutic implications in treatment decision-making. This variance may require different and individualized approaches to promoting adherence to therapy.
Not all patients with OSA will develop cardiovascular complications, and not all patients with OSA will be sleepy; this may potentiate varied intrinsic motivation by patients to treat their OSA and adhere to PAP therapy. For example, adhering to therapy may be obvious to an individual who experiences a dramatic improvement in their daytime sleepiness, thus serving as a motivating factor for continued use of PAP. However, patients that are asymptomatic but are “invisibly” developing cardiovascular risks may not be similarly motivated to use PAP therapy as there is no perceived immediate benefit or reward. In this case, it is imperative to understand what will motivate asymptomatic patients to adhere to therapy and how best to leverage that motivation to support adherence.
Individuals with an insomnia phenotype of OSA may experience worsened sleep quality as they adjust to sleeping with a PAP machine. Managing adherence in this group may require a substantially different approach than one used for individuals with a different clinical phenotype of OSA. “Lower and slower” adherence thresholds may be better aligned with the individual nature of the insomnia phenotype along with targeted cognitive behavioral intervention approaches. The identification of these clinical phenotypes is an important discovery to move the field of sleep medicine toward a personalized approach to OSA care, as patient-specific needs and patient-specific benefits of PAP therapy are identified.
An additional component of personalized medicine is patient participation. This participatory approach to medicine takes the patient from a passive receiver of care to actively managing and engaging in their own health and healthcare-related decisions.68,78 Patient engagement studies in other chronic diseases have highlighted improved clinical outcomes, increased engagement in healthy behaviors, reduced progression in disease burden, greater use of preventive healthcare, and reduced costs.81,82 Efforts to engage patients can be maximined with the use of new technologies for health (eg, eHealth and telehealth resources).83 PAP management is particularly well suited for engaging patients in their own health care. As previously highlighted, remote monitoring capabilities and apps support patients to monitor their own nightly PAP use and thus create accountability and awareness.
Patient-Centered Care to Enhance Patient Preference
A patient-centered care approach should be prioritized in order to enhance PAP acceptance and encourage PAP use.44,73 This is especially true as OSA affects individuals with varied needs, values and preferences. Men are two times as likely as women to have OSA,84 while women are less likely to adhere to PAP than men.85 Black, Hispanic, and Latino individuals are disproportionately affected by OSA,40,84,86,87 yet are less likely to be diagnosed and treated.88,89 Individuals from disadvantaged communities and of lower socioeconomic status are also at higher risk for OSA but less likely to adhere to PAP therapy.88,90,91 A “one size fits all” approach to managing PAP adherence is bound to fail when addressing a diverse OSA population. To individualize care and promote patient preference, patient-centered PAP care should include the following: (1) assessing and enhancing patient readiness, beliefs, and expectations about OSA and PAP, (2) employing health-literacy aligned patient education that is accessible to the diverse OSA population, (3) understanding patient values and preferences and collaborating on a plan for change (ie, shared decision-making), and (4) promoting patient engagement.
Assess and Enhance Patient Readiness, Beliefs, and Expectations
PAP therapy requires substantial behavior change. A new nightly routine must be adopted; daily, weekly, and monthly equipment maintenance and cleaning schedule must be established; and, additional clinical appointments for follow-up care are necessary. Patients feel most ready to adopt PAP when they perceive that PAP therapy is important and that they possess the skills to manage their care effectively.73 Understanding patients’ beliefs and expectations about PAP, as well as dismantling or enhancing preconceived notions and expectations, is critically important, as these factors may influence their decision to use PAP.67,92,93
Patient readiness and belief in their own abilities to use PAP can be clinically evaluated by one question: “On a scale of 1–10, how confident are you in your ability to use PAP from now until the next time we meet?”73 If this number is low, asking “What might make that number higher?” is a good strategy to identify patient-specific needs to increase confidence and perceived self-efficacy,73 as increased self-efficacy predicts improvements in PAP use.94,95 To improve confidence, increase self-efficacy, and address patient-specific needs, a variety of strategies can be used, including motivational enhancement therapy,96 teach-back methods,97 and allowing time for patients to “buy in” to therapy with gradual use/practice that increases their confidence and garners commitment.67 Promoting a discussion that leads to the identification of patient-specific beliefs, expectations, and confidence with PAP therapy can lead to an individualized treatment plan that is feasible and agreeable to the patient. A critical next step in following a patient-centered care model is to use these identified beliefs, expectations, and confidence in abilities to provide education that is tailored to meet and address personal needs.
Enhancing Patient Education
Risk perception is based on one’s beliefs, expectations, knowledge and awareness of a condition.98,99 This makes it critically important to dispel inaccurate notions and replace misperceptions with truths because misperceptions of health information can influence health-related decision-making. Misinformation can also lead to confusion, minimization of risk, frustration, care avoidance, nonadherence, and treatment abandonment.100 Standard education about OSA and PAP that is provided to patients commonly includes face-to-face communication with a provider, a brochure or handout, and occasionally educational videos often developed by medical device companies or professional practice organizations. Problematically, these common OSA and PAP education materials have high health literacy demands and provider communication is often too complex.101,102 Further, individuals that are at increased risk for OSA and PAP non-adherence, such as those of low socioeconomic status88,90,91 and African American, black, Hispanic, and Latino populations,40,63,84,86–88,103 are also populations that are more likely to have limited health literacy, which creates and extends inequities in care.104 Health literacy-aligned approaches to patient education are needed to empower patients to make informed decisions about their care and to ensure health information is accessible and usable by all OSA patients.
In addition to health literacy concerns related to established education practices, the current approach to patient education takes a “one size fits all” approach—everyone receives the same education on what OSA is, what PAP is, and how PAP can improve their health. In contrast, a patient-centered approach to educating patients will use dialogue about beliefs, expectations and readiness for change to guide and shape the education provided. For example, a patient expresses that they are concerned about OSA and their increased risk for diabetes because “everyone in my family is diabetic.” In this case, it may be important to focus education on the benefits of OSA treatment and diabetes risk that best aligns with the individual’s motivation to use PAP.
Another approach uses dialogue that first addresses patient concerns to promote a more productive and personalized education session. For example, if a patient is concerned that starting PAP therapy will increase their electric bill and jeopardize their finances, these concerns may distract the patient from absorbing additional important education. A patient-centered interaction that first explicitly addresses concerns and/or fears may result in a more positive, patient-centered experience and translate to enhanced use of PAP.93 Patient-centered dialogue that explicitly incorporates and prioritizes patient beliefs, expectations, and readiness will meet patients’ needs and is consistent with personalized education by being better aligned with the individual patient. As engaged participants in their own care, considerations should be given to patient preferences and autonomy in decisions to pursue treatment.
Patient Values, Preferences and Collaboration in a Plan for Change
Perhaps the most foundational component of patient-centered care is respect for patients’ values and preferences for their own health priorities. Patient-provider communication can be challenging. It is even more challenging in the context of specialty sleep care when patients meet a sleep provider for the first time and receive a diagnosis and treatment options in a single encounter. By design, this commonplace practice approach provides little opportunity to discuss patients’ preferences and establish care goals with the provider.105 Adherence “goals” are consistently pre-determined by insurance requirements,51 and patient preference in the context of treatment decisions is largely limited to selecting a PAP mask that “feels best”.67 Yet, the mask-fitting session does provide an opportunity to employ patient-centered principles by promoting patient engagement, providing education about advantages and disadvantages of varied mask types, ensuring understanding, and addressing individual questions.67 To improve the mask-fitting experience, three-dimensional face scanning is an innovative approach to individualize PAP care.106 This technology provides vital information on which masks may be best for a patient according to the patients’ facial anatomy.106 By reducing the complexity of mask selection by patients, novice to the treatment, patient decision-making is supported.67
Shared decision-making supports personalized PAP care and improves adherence to OSA treatment.107 As previously noted, adherence goals are often pre-determined; collaborating on how best to achieve that goal is an opportunity to use shared decision-making strategies. This two-way process of information sharing and mutual goal setting can be enhanced with the use of decision aids, tools that present options and help patients clarify their values.108 Decision aids can reduce decisional conflict related to feeling uninformed or unclear about treatment options and how the options align or misalign with their own values.108,109 OSA decision aides have proven beneficial for increasing disease-specific knowledge, reducing decisional conflict, are perceived as useful by patients, and increase preparedness for decision-making.110,111 Decision aids to date have rarely been developed with lower literacy populations in mind.112,113 Importantly, health literacy should also be considered during the development of decision aids, as a tool that cannot be readily understood or used is of little value.
A collaborative approach to care is associated with more self-management, care that is aligned with values, and increased patient satisfaction.114 Providers’ awareness of using patient-centered communication during PAP initiation can improve the care provided.115 By understanding patients’ beliefs and expectations, acknowledging and incorporating patient values and preferences, and collaborating on a plan for care, patients become more empowered to self-manage and act as “active care participants” rather than as “passive care recipients.”67 Promoting patient engagement is another patient-centered approach to care and also meets the needs of personalized medicine by promoting patient participation. Given objective measures of PAP use, and near real-time translation of this data, self-monitoring and telemonitoring is an opportunity for patients to further engage in their care.
Patient Engagement and Self-Monitoring
Research on improving PAP adherence and advancements in device technology have continued to evolve. Patients are increasingly interested in engaging in their own health management, as evidenced by the rapid growth in health apps and wearable devices, independently seeking medical information online, and the increased use of patient portals for electronic medical records.44,116 As previously noted, patient-facing apps are available from PAP device companies, affording patients the opportunity to self-monitor their nightly PAP use.117 Monitoring of one’s own PAP use is beneficial for increasing PAP adherence,45–47,118 however, patients must choose to actively engage with the apps to acquire this benefit. Research has demonstrated that interests and abilities to engage in patient portals are influenced by personal factors such as age, ethnicity, education level, health literacy, and health status.119 This further highlights the need for a variety of strategies for engagement to optimize individualized care approaches.119
Telemonitoring, including the use of automated messaging, coaching, reinforcement emails/texts/calls/patient portal messages, education, and videoconferencing, presents additional opportunity to employ patient engagement strategies to improve PAP use.49,64,117,120–122 Early engagement by telemonitoring and subsequent outreach can prevent PAP nonadherence.45 Trials have demonstrated telemonitoring encounters to be successful in improving PAP use49,122–124 and reducing the rate of long-term therapy termination.125 Though remote telemonitoring is standard care for PAP management, long-term telemonitoring of large volumes of patients and nightly data from entire clinics is often not sustainable.117 This clinical approach to telemonitoring relies on patients to engage, self-monitor and reach out to healthcare providers with problems. This last step may occur late in the cycle of behavior change126,127 and lead to treatment failure.59,128,129
To improve monitoring capacities, reduce staff burden, and extend telemonitoring beyond the typical 90-day window, the use of software and technology platforms that apply artificial intelligence technologies are warranted. Embedded algorithms and application of decision rules to identify poor adherence and automate alert messages may provide a feasible solution for managing large amounts of PAP data.117 Future studies are needed to determine the effects of continued, long-term engagement of patients via PAP telemonitoring, especially in context of clinical trials wherein adherence must be maintained in order to assess PAP effectiveness on various clinical endpoints/outcomes such as cardiovascular and metabolic risks.64
Clear OSA telehealth algorithms and pathways can support more individualized care by applying varied telehealth engagement strategies to specific populations. For example, as previously noted, varied OSA phenotypes or patient characteristics may influence responsiveness to telemonitoring engagement strategies or intrinsic motivation to self-monitor. These individualized differences are an important consideration for determining who will engage, and how best to target varied populations. This does not necessarily involve “reinventing the wheel”, per se, as telehealth/telemonitoring technologies provide the opportunity to deliver improved OSA care by more widely and efficiently distributing evidence-based interventions (EBIs) for PAP adherence, including behavioral, educational, and supportive interventions.130 There is, however, opportunity to examine who responds best to what type of intervention, while simultaneously examining the most effective way to implement the EBI to practice.
Implementation Science as a Way Forward
Practical implementation of EBIs into practice requires an understanding of the local context in which it will be applied. As previously noted, interventions developed to date are not readily translatable to clinical practice. While there is a growing set of evidence for interventions that improve PAP adherence, very few trials have sought to understand how interventions will function outside of a clinical trial environment, nor have they employed patient-centered approaches. Future patient-centered approaches should include engaging patient stakeholders at the outset of intervention development131 or, with testing interventions that are specifically tailored to meet individual’s needs.92 Studies that embed EBIs that are effective at improving PAP adherence for a wide variety of patients with varied needs are needed to inform clinical practice and move away from a “one size fits all” approach to managing PAP adherence.69 An implementation gap separates the scientific knowledge we have about PAP adherence and the implementation of such knowledge into effective interventions or clinical care.130 Implementation science methodologies and study designs provide a real opportunity to translate EBIs faster while also focusing on creating interventions that are acceptable, feasible, cost effective, and sustainable.
Implementation science is
the scientific study of methods to promote the systematic uptake of research findings and other evidence-based practices and interventions into routine practice, and, hence, to improve the quality and effectiveness of health services.132
In other words, implementation science research evaluates the process of implementing an evidence-based practice or EBI and how to do so most effectively. Implementation studies typically employ mixed quantitative-qualitative designs to identify specific factors that impact adoption or uptake across patient, provider, and organizational levels.132 The ability to systematically and strategically embed an EBI, while simultaneously collecting feedback from the patient makes implementation science a vehicle to incorporate patient-preferred, effective interventions for PAP adherence.
Further, implementation science focuses on facilitators and barriers to adoption of an EBI, measuring the ways people engage and respond to an intervention. This includes gaining an understanding of the context in which the intervention is to be applied at the patient, provider, and organizational level. In its most true fashion, implementation science research involves employing EBIs in “real world settings”, testing various strategies to promote the adoption and uptake of an EBI in a given setting. However, implementation science research priorities can also be applied in controlled implementation trials to examine barriers and facilitators of intervention adoption to prepare for scaling, larger trials, and wider dissemination. Many PAP trials to date have included interventions that are not readily translatable to practice.64 By adapting these interventions so they are adoptable and manageable in practice settings, the effectiveness and clinical utility of these PAP adherence interventions can be tested simultaneously, leading to a more efficient research process. A dual-focus approach to research (ie, assessing both effectiveness of implementation and the health impact of an EBI), coined hybrid implementation-effectiveness design, has the potential to identify effective interventions, while concurrently studying implementation strategies to promote uptake of the EBI.132,133
PAP adherence trials that use implementation science designs will better clarify effectiveness of various PAP interventions in real-world settings as well as determine effective implementation strategies for such interventions.130 PAP adherence interventions tested to date are mixed component approaches with a single predominant component (eg, educational plus supportive interventions; supportive plus behavioral interventions).28 Identifying the core versus adaptable components of interventions using implementation methods will aid in determining the most effective interventions. Additionally, implementation trials present the opportunity to test implementation strategies to optimize the uptake of interventions. Further, with the growth of personalized medicine and phenotyping of OSA, the field is well positioned to examine who responds best to what type of intervention using an implementation science approach. This can also incorporate patient preference, either directly by measuring acceptability and engaging stakeholders to understand preferences, barriers, and the overall context in which interventions are applied, or indirectly by examining reasons for failed adoption.
The sleep field currently has an abundance of early-stage efficacy research, but less later-stage implementation research to support practice translation. Recognizing this need, both the American Thoracic Society (ATS) and the Sleep Research Society (SRS) organized workshops to discuss how implementation science can be applied and adopted in sleep medicine and have released research statements.130,134 ATS and SRS have recognized this opportunity for growth in the sleep field, and with the support of other organizations and societies, implementation science in sleep medicine is a strategic and warranted approach to promote PAP adherence and best PAP care. We can move the field forward by linking sleep researchers, implementation scientists, industry and insurance partners, front-line clinicians, and patients to problem solve and propose feasible interventions to promote PAP adherence. Although efficacy trials are critically important, the field needs to utilize existing EBIs, adapt them to be practical and translatable with the help of stakeholder engagement, and deploy and test their implementation. Conducting such implementation trials that simultaneously evaluate efficacy, effectiveness, and implementation will begin to shorten the persistent 17-year gap of research to practice translation that plagues the field.
Conclusion
Individualized care, whether by a personalized medicine or patient-centered approach, places the patient and their individual characteristics, needs and preferences as a top priority. An individualized care approach with the patient at the pinnacle has the opportunity to improve patient-preferred outcomes, PAP care, and PAP adherence. This review highlights the work that is taking place to move toward individualized care in sleep medicine. Many effective PAP adherence interventions developed to date are in need to refinement in order to 1) be individualized to patients’ needs whether biological (ie, OSA phenotype) or psychosocial (ie, patient preference), and 2) to be readily applied to practice and tested on a clinical scale. This intervention development and refinement should consider leveraging previous qualitative research findings to encourage interventions that are designed based on patient identified needs.93,135–138 Further, prioritizing patient preference, engaging patient stakeholders, and collecting patient-centered outcomes should continue to be pursued to better understanding PAP adherence. The Patient-Centered Outcomes Research Institute (PCORI) has funded work in this area, including the Sleep Apnea Patient-Centered Outcomes Network (SAPCON), a collaborative group of patients, researchers and clinicians focused on generating patient-centered research,69 peer support programs to improve treatment satisfaction for adults with OSA,131 and engagement of patient, provider, professional organization, and medical equipment providers to help plan and design studies139 and understand PAP adherence barriers.140
Lastly, to begin to test PAP adherence interventions on a broader and more diverse scale, whether it be patient diversity, geographic diversity, or diversity related to clinic resources (ie, a large academic institution versus rural sleep clinic), sleep researchers should seek to collaborate to gain a better understanding of how EBIs function in various OSA populations and within varied settings. This endeavor is far too large to accomplish alone, but through strong scientific collaborations, PAP care can be optimized, patient care improved, and perhaps most importantly, patient health outcomes improved. Sleep medicine is on a promising path to develop individualized approaches to PAP care through the continued research on personalized medicine and patient-centered care, and implementation science can provide a critical vehicle to more rapidly move EBIs to practice for the benefit of all patients.
Acknowledgments
The authors acknowledge conceptualizing motivation for this work by the Penn Implementation Science Center (PISCE) and the innovators in sleep at Kaiser Permanente SBC Sleep Center, Kaiser Permanente Southern California. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Disclosure
Dr. Sawyer reports grants from VA HSR&D, grants from American Lung Association, grants from NIH/NHLBI, grants from University of Pennsylvania School of Nursing Faculty Senate Research, outside the submitted work. Dr. Watach reports support from the National Institutes of Health (T32 HL007953). Dr. Hwang reports relevant research grant support from National Institute of Health, American Academy of Sleep Medicine Foundation Strategic Research Award 205-SR-19; Regional Research Committee of Kaiser Permanente Southern California, Grant Number: KP-RRC-KP-RRC-20190502.
References
1. Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687–698. doi:10.1016/s2213-2600(19)30198-5
2. Patil SP, Ayappa IA, Caples SM, Kimoff RJ, Patel SR, Harrod CG. Treatment of adult obstructive sleep apnea with positive airway pressure: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2019;15(2):335–343. doi:10.5664/jcsm.7640
3. Epstein LJ, Kristo D, Strollo PJ, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(3):263–276.
4. Purtle MW, Renner CH, McCann DA, Mallen JC, Spilman SK, Sahr SM. Driving with undiagnosed obstructive sleep apnea (OSA): high prevalence of OSA risk in drivers who experienced a motor vehicle crash. Traffic Inj Prev. 2020;21(1):38–41. doi:10.1080/15389588.2019.1709175
5. Tregear S, Reston J, Schoelles K, Phillips B. Obstructive sleep apnea and risk of motor vehicle crash: systematic review and meta-analysis. J Clin Sleep Med. 2009;5(6):573–581. doi:10.5664/jcsm.27662
6. Gurubhagavatula I, Sullivan S, Meoli A, et al. Management of obstructive sleep apnea in commercial motor vehicle operators: recommendations of the AASM sleep and transportation safety awareness task force. J Clin Sleep Med. 2017;13(5):745–758. doi:10.5664/jcsm.6598
7. Gottlieb DJ, Whitney CW, Bonekat WH, et al. Relation of sleepiness to respiratory disturbance index: the Sleep Heart Health Study. Am J Respir Crit Care Med. 1999;159(2):502–507. doi:10.1164/ajrccm.159.2.9804051
8. Matsuo R, Tanigawa T, Tomooka K, et al. Sleep disordered breathing and subjective excessive daytime sleepiness in relation to the risk of motor vehicle crash: the Toon Health Study. Sci Rep. 2020;10(1):17050. doi:10.1038/s41598-020-74132-7
9. Stranks EK, Crowe SF. The cognitive effects of obstructive sleep apnea: an updated meta-analysis. Arch Clin Neuropsychol. 2016;31(2):186–193. doi:10.1093/arclin/acv087
10. Zhou J, Camacho M, Tang X, Kushida CA. A review of neurocognitive function and obstructive sleep apnea with or without daytime sleepiness. Sleep Med. 2016;23:99–108. doi:10.1016/j.sleep.2016.02.008
11. Olaithe M, Bucks RS, Hillman DR, Eastwood PR. Cognitive deficits in obstructive sleep apnea: insights from a meta-review and comparison with deficits observed in COPD, insomnia, and sleep deprivation. Sleep Med Rev. 2018;38:39–49. doi:10.1016/j.smrv.2017.03.005
12. Stubbs B, Vancampfort D, Veronese N, et al. The prevalence and predictors of obstructive sleep apnea in major depressive disorder, bipolar disorder and schizophrenia: a systematic review and meta-analysis. J Affect Disord. 2016;197:259–267. doi:10.1016/j.jad.2016.02.060
13. Gupta MA, Simpson FC. Obstructive sleep apnea and psychiatric disorders: a systematic review. J Clin Sleep Med. 2015;11(2):165–175. doi:10.5664/jcsm.4466
14. Peppard PE, Szklo-Coxe M, Hla KM, Young T. Longitudinal association of sleep-related breathing disorder and depression. Arch Intern Med. 2006;166(16):1709–1715. doi:10.1001/archinte.166.16.1709
15. Somers VK, White DP, Amin R, et al. Sleep apnea and cardiovascular disease: an American heart association/American college of cardiology foundation scientific statement from the American heart association council for high blood pressure research professional education committee, council on clinical cardiology, stroke council, and council on cardiovascular nursing in collaboration with the national heart, lung, and blood institute national center on sleep disorders research (national institutes of health). J Am Coll Cardiol. 2008;52(8):686–717.
16. Shahar E, Whitney CW, Redline S, et al. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J Respir Crit Care Med. 2001;163(1):19–25. doi:10.1164/ajrccm.163.1.2001008
17. Reutrakul S, Mokhlesi B. Obstructive sleep apnea and diabetes: a state of the art review. Chest. 2017;152(5):1070–1086. doi:10.1016/j.chest.2017.05.009
18. Punjabi NM, Sorkin JD, Katzel LI, Goldberg AP, Schwartz AR, Smith PL. Sleep-disordered breathing and insulin resistance in middle-aged and overweight men. Am J Respir Crit Care Med. 2002;165(5):677–682. doi:10.1164/ajrccm.165.5.2104087
19. Punjabi NM, Shahar E, Redline S, et al. Sleep-disordered breathing, glucose intolerance, and insulin resistance: the Sleep Heart Health Study. Am J Epidemiol. 2004;160(6):521–530. doi:10.1093/aje/kwh261
20. Redline S, Yenokyan G, Gottlieb DJ, et al. Obstructive sleep apnea-hypopnea and incident stroke: the sleep heart health study. Am J Respir Crit Care Med. 2010;182(2):269–277. doi:10.1164/rccm.200911-1746OC
21. Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353(19):2034–2041. doi:10.1056/NEJMoa043104
22. Punjabi NM, Caffo BS, Goodwin JL, et al. Sleep-disordered breathing and mortality: a prospective cohort study. PLoS Med. 2009;6(8):e1000132. doi:10.1371/journal.pmed.1000132
23. Fu Y, Xia Y, Yi H, Xu H, Guan J, Yin S. Meta-analysis of all-cause and cardiovascular mortality in obstructive sleep apnea with or without continuous positive airway pressure treatment. Sleep Breath. 2017;21(1):181–189. doi:10.1007/s11325-016-1393-1
24. Patil SP, Ayappa IA, Caples SM, Kimoff RJ, Patel SR, Harrod CG. Treatment of adult obstructive sleep apnea with positive airway pressure: an American academy of sleep medicine systematic review, meta-analysis, and GRADE assessment. J Clin Sleep Med. 2019;15(2):301–334. doi:10.5664/jcsm.7638
25. Brown LK, Javaheri S. Positive airway pressure device technology past and present: what’s in the “Black Box”? Sleep Med Clin. 2017;12(4):501–515. doi:10.1016/j.jsmc.2017.07.001
26. Weaver TE, Sawyer AM. Adherence to continuous positive airway pressure treatment for obstructive sleep apnoea: implications for future interventions. Indian J Med Res. 2010;131:245–258.
27. Antic NA, Catcheside P, Buchan C, et al. The effect of CPAP in normalizing daytime sleepiness, quality of life, and neurocognitive function in patients with moderate to severe OSA. Sleep. 2011;34(1):111–119. doi:10.1093/sleep/34.1.111
28. Askland K, Wright L, Wozniak DR, Emmanuel T, Caston J, Smith I. Educational, supportive and behavioural interventions to improve usage of continuous positive airway pressure machines in adults with obstructive sleep apnoea. Cochrane Database Syst Rev. 2020;4(4):Cd007736. doi:10.1002/14651858.CD007736.pub3
29. Kuhn E, Schwarz EI, Bratton DJ, Rossi VA, Kohler M. Effects of CPAP and mandibular advancement devices on health-related quality of life in OSA: a systematic review and meta-analysis. Chest. 2017;151(4):786–794. doi:10.1016/j.chest.2017.01.020
30. Gottlieb DJ, Punjabi NM, Mehra R, et al. CPAP versus oxygen in obstructive sleep apnea. N Engl J Med. 2014;370(24):2276–2285. doi:10.1056/NEJMoa1306766
31. Iftikhar IH, Valentine CW, Bittencourt LR, et al. Effects of continuous positive airway pressure on blood pressure in patients with resistant hypertension and obstructive sleep apnea: a meta-analysis. J Hypertens. 2014;32(12):2341–2350. doi:10.1097/hjh.0000000000000372
32. Martínez-García MA, Capote F, Campos-Rodríguez F, et al. Effect of CPAP on blood pressure in patients with obstructive sleep apnea and resistant hypertension: the HIPARCO randomized clinical trial. JAMA. 2013;310(22):2407–2415. doi:10.1001/jama.2013.281250
33. Bravata DM, Sico J, Vaz Fragoso CA, et al. Diagnosing and treating sleep apnea in patients with acute cerebrovascular disease. J Am Heart Assoc. 2018;7(16):e008841. doi:10.1161/jaha.118.008841
34. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046–1053. doi:10.1016/s0140-6736(05)71141-7
35. Mokhlesi B, Grimaldi D, Beccuti G, Van Cauter E. Effect of one week of CPAP treatment of obstructive sleep apnoea on 24-hour profiles of glucose, insulin and counter-regulatory hormones in type 2 diabetes. Diabetes Obes Metab. 2017;19(3):452–456. doi:10.1111/dom.12823
36. Iftikhar IH, Hoyos CM, Phillips CL, Magalang UJ. Meta-analyses of the association of sleep apnea with insulin resistance, and the effects of CPAP on HOMA-IR, adiponectin, and visceral adipose fat. J Clin Sleep Med. 2015;11(4):475–485. doi:10.5664/jcsm.4610
37. Krakow B, Ulibarri VA, Foley-Shea MR, Tidler A, McIver ND. Adherence and subthreshold adherence in sleep apnea subjects receiving positive airway pressure therapy: a retrospective study evaluating differences in adherence versus use. Respir Care. 2016;61(8):1023–1032. doi:10.4187/respcare.04538
38. Stepnowsky CJ, Moore PJ. Nasal CPAP treatment for obstructive sleep apnea: developing a new perspective on dosing strategies and compliance. J Psychosom Res. 2003;54(6):599–605. doi:10.1016/s0022-3999(03)00038-2
39. Weaver TE, Maislin G, Dinges DF, et al. Relationship between hours of CPAP use and achieving normal levels of sleepiness and daily functioning. Sleep. 2007;30(6):711–719. doi:10.1093/sleep/30.6.711
40. Parthasarathy S. The positive and negative about positive airway pressure therapy. Am J Respir Crit Care Med. 2016;194(5):535–537. doi:10.1164/rccm.201603-0484ED
41. Liu T, Li W, Zhou H, Wang Z. Verifying the relative efficacy between continuous positive airway pressure therapy and its alternatives for obstructive sleep apnea: a network meta-analysis. Front Neurol. 2017;8:289. doi:10.3389/fneur.2017.00289
42. Whittemore R, Knafl K. The integrative review: updated methodology. J Adv Nurs. 2005;52(5):546–553. doi:10.1111/j.1365-2648.2005.03621.x
43. Schwab RJ, Badr SM, Epstein LJ, et al. An official American Thoracic Society statement: continuous positive airway pressure adherence tracking systems. The optimal monitoring strategies and outcome measures in adults. Am J Respir Crit Care Med. 2013;188(5):613–620. doi:10.1164/rccm.201307-1282ST
44. Hilbert J, Yaggi HK. Patient-centered care in obstructive sleep apnea: a vision for the future. Sleep Med Rev. 2018;37:138–147. doi:10.1016/j.smrv.2017.02.004
45. Aardoom JJ, Loheide-Niesmann L, Ossebaard HC, Riper H. Effectiveness of eHealth interventions in improving treatment adherence for adults with obstructive sleep apnea: meta-analytic review. J Med Internet Res. 2020;22(2):e16972. doi:10.2196/16972
46. Malhotra A, Crocker ME, Willes L, Kelly C, Lynch S, Benjafield AV. Patient engagement using new technology to improve adherence to positive airway pressure therapy: a retrospective analysis. Chest. 2018;153(4):843–850. doi:10.1016/j.chest.2017.11.005
47. Shaughnessy GF, Morgenthaler TI. The effect of patient-facing applications on positive airway pressure therapy adherence: a systematic review. J Clin Sleep Med. 2019;15(5):769–777. doi:10.5664/jcsm.7772
48. Pack AI. Application of personalized, predictive, preventative, and participatory (P4) medicine to obstructive sleep apnea. A roadmap for improving care? Ann Am Thorac Soc. 2016;13(9):1456–1467. doi:10.1513/AnnalsATS.201604-235PS
49. Hwang D, Chang JW, Benjafield AV, et al. Effect of telemedicine education and telemonitoring on continuous positive airway pressure adherence. The tele-OSA randomized trial. Am J Respir Crit Care Med. 2018;197(1):117–126. doi:10.1164/rccm.201703-0582OC
50. Hwang D. Monitoring progress and adherence with positive airway pressure therapy for obstructive sleep apnea: the roles of telemedicine and mobile health applications. Sleep Med Clin. 2016;11(2):161–171. doi:10.1016/j.jsmc.2016.01.008
51. Centers for Medicare and Medicaid Services. Positive airway pressure (PAP) devices: complying with documentation & coverage requirements (2016).
52. Hoyos CM, Murugan SM, Melehan KL, et al. Dose-dependent effects of continuous positive airway pressure for sleep apnea on weight or metabolic function: individual patient-level clinical trial meta-analysis. J Sleep Res. 2019;28(5):e12788. doi:10.1111/jsr.12788
53. Shafazand S, Patel SR. Effect of CPAP on blood pressure in patients with obstructive sleep apnea and resistant hypertension. J Clin Sleep Med. 2014;10(3):341–343. doi:10.5664/jcsm.3554
54. McEvoy RD, Antic NA, Heeley E, et al. CPAP for prevention of cardiovascular events in obstructive sleep apnea. N Engl J Med. 2016;375(10):919–931. doi:10.1056/NEJMoa1606599
55. Yu J, Zhou Z, McEvoy RD, et al. Association of positive airway pressure with cardiovascular events and death in adults with sleep apnea: a systematic review and meta-analysis. JAMA. 2017;318(2):156–166. doi:10.1001/jama.2017.7967
56. Abuzaid AS, Al Ashry HS, Elbadawi A, et al. Meta-analysis of cardiovascular outcomes with continuous positive airway pressure therapy in patients with obstructive sleep apnea. Am J Cardiol. 2017;120(4):693–699. doi:10.1016/j.amjcard.2017.05.042
57. Van Ryswyk E, Anderson CS, Antic NA, et al. Predictors of long-term adherence to continuous positive airway pressure in patients with obstructive sleep apnea and cardiovascular disease. Sleep. 2019;42(10). doi:10.1093/sleep/zsz152
58. Chai-Coetzer CL, Luo YM, Antic NA, et al. Predictors of long-term adherence to continuous positive airway pressure therapy in patients with obstructive sleep apnea and cardiovascular disease in the SAVE study. Sleep. 2013;36(12):1929–1937. doi:10.5665/sleep.3232
59. Budhiraja R, Parthasarathy S, Drake CL, et al. Early CPAP use identifies subsequent adherence to CPAP therapy. Sleep. 2007;30(3):320–324.
60. Weaver TE, Kribbs NB, Pack AI, et al. Night-to-night variability in CPAP use over the first three months of treatment. Sleep. 1997;20(4):278–283. doi:10.1093/sleep/20.4.278
61. Aloia MS, Arnedt JT, Stanchina M, Millman RP. How early in treatment is PAP adherence established? Revisiting night-to-night variability. Behav Sleep Med. 2007;5(3):229–240. doi:10.1080/15402000701264005
62. Wozniak DR, Lasserson TJ, Smith I. Educational, supportive and behavioural interventions to improve usage of continuous positive airway pressure machines in adults with obstructive sleep apnoea. Cochrane Database Syst Rev. 2014;(1):Cd007736. doi:10.1002/14651858.CD007736.pub2
63. Sawyer AM, Gooneratne NS, Marcus CL, Ofer D, Richards KC, Weaver TE. A systematic review of CPAP adherence across age groups: clinical and empiric insights for developing CPAP adherence interventions. Sleep Med Rev. 2011;6:343–356. doi:10.1016/j.smrv.2011.01.003
64. Sawyer AM, Wallace DM, Buenaver LF, et al. Where to next for optimizing adherence in large-scale trials of continuous positive airway pressure? Sleep Med Clin. 2021;16(1):125–144. doi:10.1016/j.jsmc.2020.10.007
65. Crawford MR, Espie CA, Bartlett DJ, Grunstein RR. Integrating psychology and medicine in CPAP adherence--new concepts? Sleep Med Rev. 2014;18(2):123–139. doi:10.1016/j.smrv.2013.03.002
66. Mehrtash M, Bakker JP, Ayas N. Predictors of continuous positive airway pressure adherence in patients with obstructive sleep apnea. Lung. 2019;197(2):115–121. doi:10.1007/s00408-018-00193-1
67. Genta PR, Kaminska M, Edwards BA, et al. The importance of mask selection on continuous positive airway pressure outcomes for obstructive sleep Apnea. An official American thoracic society workshop report. Ann Am Thorac Soc. 2020;17(10):1177–1185. doi:10.1513/AnnalsATS.202007-864ST
68. Lim DC, Sutherland K, Cistulli PA, Pack AI. P4 medicine approach to obstructive sleep apnoea. Respirology. 2017;22(5):849–860. doi:10.1111/resp.13063
69. Redline S, Baker-Goodwin S, Bakker JP, et al. Patient partnerships transforming sleep medicine research and clinical care: perspectives from the sleep apnea patient-centered outcomes network. J Clin Sleep Med. 2016;12(7):1053–1058. doi:10.5664/jcsm.5948
70. El-Alti L, Sandman L, Munthe C. Person centered care and personalized medicine: irreconcilable opposites or potential companions? Health Care Anal. 2019;27(1):45–59. doi:10.1007/s10728-017-0347-5
71. Håkansson Eklund J, Holmström IK, Kumlin T, et al. “Same same or different?” A review of reviews of person-centered and patient-centered care. Patient Educ Couns. 2019;102(1):3–11. doi:10.1016/j.pec.2018.08.029
72. Starfield B. Is patient-centered care the same as person-focused care? Perm J. 2011;15(2):63–69. doi:10.7812/tpp/10-148
73. Wickwire EM, Lettieri CJ, Cairns AA, Collop NA. Maximizing positive airway pressure adherence in adults: a common-sense approach. Chest. 2013;144(2):680–693. doi:10.1378/chest.12-2681
74. Feemster LC, Saft HL, Bartlett SJ, et al. Patient-centered outcomes research in pulmonary, critical care, and sleep medicine. An official American thoracic society workshop report. Ann Am Thorac Soc. 2018;15(9):1005–1015. doi:10.1513/AnnalsATS.201806-406WS
75. Zinchuk AV, Gentry MJ, Concato J, Yaggi HK. Phenotypes in obstructive sleep apnea: a definition, examples and evolution of approaches. Sleep Med Rev. 2017;35:113–123. doi:10.1016/j.smrv.2016.10.002
76. Pien GW, Ye L, Keenan BT, et al. Changing faces of obstructive sleep apnea: treatment effects by cluster designation in the Icelandic Sleep Apnea Cohort. Sleep. 2018;41(3):zsx201. doi:10.1093/sleep/zsx201
77. Mazzotti DR, Keenan BT, Lim DC, Gottlieb DJ, Kim J, Pack AI. Symptom subtypes of obstructive sleep apnea predict incidence of cardiovascular outcomes. Am J Respir Crit Care Med. 2019;200(4):493–506. doi:10.1164/rccm.201808-1509OC
78. Hood L. Systems biology and p4 medicine: past, present, and future. Rambam Maimonides Med J. 2013;4(2):e0012. doi:10.5041/rmmj.10112
79. Flores M, Glusman G, Brogaard K, Price ND, Hood L. P4 medicine: how systems medicine will transform the healthcare sector and society. Per Med. 2013;10(6):565–576. doi:10.2217/pme.13.57
80. Ye L, Pien GW, Ratcliffe SJ, et al. The different clinical faces of obstructive sleep apnoea: a cluster analysis. Eur Respir J. 2014;44(6):1600–1607. doi:10.1183/09031936.00032314
81. Greene J, Hibbard JH, Sacks R, Overton V, Parrotta CD. When patient activation levels change, health outcomes and costs change, too. Health Aff. 2015;34(3):431–437. doi:10.1377/hlthaff.2014.0452
82. Hibbard JH, Greene J, Sacks RM, Overton V, Parrotta C. Improving population health management strategies: identifying patients who are more likely to be users of avoidable costly care and those more likely to develop a new chronic disease. Health Serv Res. 2017;52(4):1297–1309. doi:10.1111/1475-6773.12545
83. Barello S, Triberti S, Graffigna G, et al. eHealth for patient engagement: a systematic review. Front Psychol. 2015;6:2013. doi:10.3389/fpsyg.2015.02013
84. Punjabi NM. The epidemiology of adult obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):136–143. doi:10.1513/pats.200709-155MG
85. Patel SR, Bakker JP, Stitt CJ, Aloia MS, Nouraie SM. Age and sex disparities in adherence to CPAP. CHEST. 2021;159(1):382–389. doi:10.1016/j.chest.2020.07.017
86. Dudley KA, Patel SR. Disparities and genetic risk factors in obstructive sleep apnea. Sleep Med. 2016;18:96–102. doi:10.1016/j.sleep.2015.01.015
87. Adenekan B, Pandey A, McKenzie S, Zizi F, Casimir GJ, Jean-Louis G. Sleep in America: role of racial/ethnic differences. Sleep Med Rev. 2013;17(4):255–262. doi:10.1016/j.smrv.2012.07.002
88. Billings ME, Auckley D, Benca R, et al. Race and residential socioeconomics as predictors of CPAP adherence. Sleep. 2011;34(12):1653–1658. doi:10.5665/sleep.1428
89. Redline S, Sotres-Alvarez D, Loredo J, et al. Sleep-disordered breathing in Hispanic/Latino individuals of diverse backgrounds. The Hispanic Community Health Study/Study of Latinos. Am J Respir Crit Care Med. 2014;189(3):335–344. doi:10.1164/rccm.201309-1735OC
90. Pandey A, Mereddy S, Combs D, et al. Socioeconomic inequities in adherence to positive airway pressure therapy in population-level analysis. J Clin Med. 2020;9(2):442. doi:10.3390/jcm9020442
91. Platt AB, Field SH, Asch DA, et al. Neighborhood of residence is associated with daily adherence to CPAP therapy. Sleep. 2009;32(6):799–806. doi:10.1093/sleep/32.6.799
92. Sawyer AM, King TS, Weaver TE, et al. A tailored intervention for PAP adherence: the SCIP-PA trial. Behav Sleep Med. 2019;17(1):49–69. doi:10.1080/15402002.2016.1276018
93. Khan NNS, Olomu AB, Bottu S, Roller MR, Smith RC. Semistructured motivational interviews of patients and caregivers to improve CPAP adherence: a qualitative analysis. J Clin Sleep Med. 2019;15(12):1721–1730. doi:10.5664/jcsm.8070
94. Weaver TE, Maislin G, Dinges DF, et al. Self-efficacy in sleep apnea: instrument development and patient perceptions of obstructive sleep apnea risk, treatment benefit, and volition to use continuous positive airway pressure. Sleep. 2003;26(6):727–732. doi:10.1093/sleep/26.6.727
95. Baron KG, Berg CA, Czajkowski LA, Smith TW, Gunn HE, Jones CR. Self-efficacy contributes to individual differences in subjective improvements using CPAP. Sleep Breath. 2011;15(3):599–606. doi:10.1007/s11325-010-0409-5
96. Bakker JP, Wang R, Weng J, et al. Motivational enhancement for increasing adherence to CPAP: a randomized controlled trial. Chest. 2016;150(2):337–345. doi:10.1016/j.chest.2016.03.019
97. Brega A, Barnard J, Mabachi N, et al. AHRQ Health Literacy Universal Precautions Toolkit.
98. Ferrer R, Klein WM. Risk perceptions and health behavior. Curr Opin Psychol. 2015;5:85–89. doi:10.1016/j.copsyc.2015.03.012
99. Witte K. Putting the fear back into fear appeals: the extended parallel process model. Commun Monogr. 1992;59(4):329–349. doi:10.1080/03637759209376276
100. Hardavella G, Aamli-Gaagnat A, Frille A, Saad N, Niculescu A, Powell P. Top tips to deal with challenging situations: doctor-patient interactions. Breathe. 2017;13(2):129–135. doi:10.1183/20734735.006616
101. Dudley KA, Rovnak A, Bertisch SM, Bakker JP, Patel SR. High health literacy demands of patient education materials for obstructive sleep apnea. Am J Respir Crit Care Med. 2017;195:A6548.
102. Nouri SS, Rudd RE. Health literacy in the “oral exchange”: an important element of patient-provider communication. Patient Educ Couns. 2015;98(5):565–571. doi:10.1016/j.pec.2014.12.002
103. Guglielmi O, Lanteri P, Garbarino S. Association between socioeconomic status, belonging to an ethnic minority and obstructive sleep apnea: a systematic review of the literature. Sleep Med. 2019;57:100–106. doi:10.1016/j.sleep.2019.01.042
104. Kutner M, Greenberg E, Jin Y, Paulsen C. The health literacy of America’s adults: results from the 2003 national assessment of adult literacy. US Department of Education; 2006.
105. Fung CH, Alessi C, Truong C, et al. Patient-provider communication with older adults about sleep apnea diagnosis and treatment. Behav Sleep Med. 2017;15(6):423–437. doi:10.1080/15402002.2016.1150278
106. Ma Z, Drinnan M, Hyde P, Munguia J. Mask interface for continuous positive airway pressure therapy: selection and design considerations. Expert Rev Med Devices. 2018;15(10):725–733. doi:10.1080/17434440.2018.1525291
107. Broström A, Pakpour AH, Nilsen P, Hedberg B, Ulander M. Validation of CollaboRATE and SURE - two short questionnaires to measure shared decision making during CPAP initiation. J Sleep Res. 2019;28(5):e12808. doi:10.1111/jsr.12808
108. Stacey D, Légaré F, Col NF, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2014;1:Cd001431. doi:10.1002/14651858.CD001431.pub4
109. Pelletier-Fleury N, Gafni A, Krucien N, Fleury B. The development and testing of a new communication tool to help clinicians inform patients with obstructive sleep apnoea syndrome about treatment options. J Sleep Res. 2012;21(5):577–583. doi:10.1111/j.1365-2869.2012.01015.x
110. Fung CH, Martin JL, Liang LJ, et al. Efficacy of a patient decision aid for improving person-centered decision-making by older adults with obstructive sleep apnea. J Clin Sleep Med. 2021;17(2):121–128. doi:10.5664/jcsm.8798
111. Trenaman L, Munro S, Almeida F, Ayas N, Hicklin J, Bansback N. Development of a patient decision aid prototype for adults with obstructive sleep apnea. Sleep Breath. 2016;20(2):653–661. doi:10.1007/s11325-015-1269-9
112. McCaffery KJ, Holmes-Rovner M, Smith SK, et al. Addressing health literacy in patient decision aids. BMC Med Inform Decis Mak. 2013;13(Suppl2):S10. doi:10.1186/1472-6947-13-s2-s10
113. Muscat DM, Shepherd HL, Nutbeam D, Trevena L, McCaffery KJ. Health literacy and shared decision-making: exploring the relationship to enable meaningful patient engagement in healthcare. J Gen Intern Med. 2021;36(2):521–524. doi:10.1007/s11606-020-05912-0
114. Rathert C, Wyrwich MD, Boren SA. Patient-centered care and outcomes: a systematic review of the literature. Med Care Res Rev. 2013;70(4):351–379. doi:10.1177/1077558712465774
115. Broström A, Fridlund B, Fossum B, Pakpour A, Nilsen P, Ulander M. Communication during the initial visit to a CPAP clinic Practitioners’ experiences of facilitators and barriers when talking to patients with obstructive sleep apnea. J Sleep Res. 2020;e13244. doi:10.1111/jsr.13244
116. Bombard Y, Baker GR, Orlando E, et al. Engaging patients to improve quality of care: a systematic review. Implement Sci. 2018;13(1):98. doi:10.1186/s13012-018-0784-z
117. Schutte-Rodin S. Telehealth, telemedicine, and obstructive sleep apnea. Sleep Med Clin. 2020;15(3):359–375. doi:10.1016/j.jsmc.2020.05.003
118. Kuna ST, Shuttleworth D, Chi L, et al. Web-based access to positive airway pressure usage with or without an initial financial incentive improves treatment use in patients with obstructive sleep apnea. Sleep. 2015;38(8):1229–1236. doi:10.5665/sleep.4898
119. Irizarry T, DeVito Dabbs A, Curran CR. Patient portals and patient engagement: a state of the science review. J Med Internet Res. 2015;17(6):e148. doi:10.2196/jmir.4255
120. Graffigna G, Barello S. Spotlight on the patient health engagement model (PHE model): a psychosocial theory to understand people’s meaningful engagement in their own health care. Patient Prefer Adherence. 2018;12:1261–1271. doi:10.2147/ppa.s145646
121. Woehrle H, Arzt M, Graml A, et al. Effect of a patient engagement tool on positive airway pressure adherence: analysis of a German healthcare provider database. Sleep Med. 2018;41:20–26. doi:10.1016/j.sleep.2017.07.026
122. Chen C, Wang J, Pang L, Wang Y, Ma G, Liao W. Telemonitor care helps CPAP compliance in patients with obstructive sleep apnea: a systemic review and meta-analysis of randomized controlled trials. Ther Adv Chronic Dis. 2020;11:2040622320901625. doi:10.1177/2040622320901625
123. Fox N, Hirsch-Allen AJ, Goodfellow E, et al. The impact of a telemedicine monitoring system on positive airway pressure adherence in patients with obstructive sleep apnea: a randomized controlled trial. Sleep. 2012;35(4):477–481. doi:10.5665/sleep.1728
124. Nilius G, Schroeder M, Domanski U, Tietze A, Schäfer T, Franke KJ. Telemedicine improves continuous positive airway pressure adherence in stroke patients with obstructive sleep apnea in a randomized trial. Respiration. 2019;98(5):410–420. doi:10.1159/000501656
125. Woehrle H, Ficker JH, Graml A, et al. Telemedicine-based proactive patient management during positive airway pressure therapy: impact on therapy termination rate. Somnologie. 2017;21(2):121–127. doi:10.1007/s11818-016-0098-9
126. Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward an integrative model of change. J Consult Clin Psychol. 1983;51(3):390–395. doi:10.1037//0022-006x.51.3.390
127. Prochaska JO, Norcross JC, DiClemente CC. Applying the Stages of Change. Vol. 19. PsychOz Publications & Human Condition Bookstore; 2013:10–15.
128. Sawyer AM, Deatrick JA, Kuna ST, Weaver TE. Differences in perceptions of the diagnosis and treatment of obstructive sleep apnea and continuous positive airway pressure therapy among adherers and nonadherers. Qual Health Res. 2010;20(7):873–892. doi:10.1177/1049732310365502
129. Broström A, Nilsen P, Johansson P, et al. Putative facilitators and barriers for adherence to CPAP treatment in patients with obstructive sleep apnea syndrome: a qualitative content analysis. Sleep Med. 2010;11(2):126–130. doi:10.1016/j.sleep.2009.04.010
130. Parthasarathy S, Carskadon MA, Jean-Louis G, et al. Implementation of sleep and circadian science: recommendations from the sleep research society and national institutes of health workshop. Sleep. 2016;39(12):2061–2075. doi:10.5665/sleep.6300
131. Parthasarathy S, Guerra S, Quan S, Grandner M, Haynes P. Does a peer support program improve satisfaction with treatment among patients with obstructive sleep apnea? PCORI. 2020. doi:10.25302/04.2020.IHS.130602505
132. Bauer MS, Damschroder L, Hagedorn H, Smith J, Kilbourne AM. An introduction to implementation science for the non-specialist. BMC Psychol. 2015;3(1):32. doi:10.1186/s40359-015-0089-9
133. Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C. Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med Care. 2012;50(3):217–226. doi:10.1097/MLR.0b013e3182408812
134. Weiss CH, Krishnan JA, Au DH, et al. An official American thoracic society research statement: implementation science in pulmonary, critical care, and sleep medicine. Am J Respir Crit Care Med. 2016;194(8):1015–1025. doi:10.1164/rccm.201608-1690ST
135. Almeida FR, Henrich N, Marra C, et al. Patient preferences and experiences of CPAP and oral appliances for the treatment of obstructive sleep apnea: a qualitative analysis. Sleep Breath. 2013;17(2):659–666. doi:10.1007/s11325-012-0739-6
136. Luyster FS, Dunbar-Jacob J, Aloia MS, Martire LM, Buysse DJ, Strollo PJ. Patient and partner experiences with obstructive sleep apnea and CPAP treatment: a qualitative analysis. Behav Sleep Med. 2016;14(1):67–84. doi:10.1080/15402002.2014.946597
137. Waldman LT, Parthasarathy S, Villa KF, Bron M, Bujanover S, Brod M. Understanding the burden of illness of excessive daytime sleepiness associated with obstructive sleep apnea: a qualitative study. Health Qual Life Outcomes. 2020;18(1):128. doi:10.1186/s12955-020-01382-4
138. Zarhin D, Oksenberg A. Ambivalent adherence and nonadherence to continuous positive airway pressure devices: a qualitative study. J Clin Sleep Med. 2017;13(12):1375–1384. doi:10.5664/jcsm.6828
139. Stepnowsky C. Comparing two ways to improve adherence to continuous positive airway pressure therapy in patients with chronic obstructive pulmonary disease and obstructive sleep apnea: the O2VERLAP study patient-centered outcomes research institute (PCORI). 2020. Available from: https://www.pcori.org/research-results/2016/comparing-two-ways-improve-adherence-continuous-positive-airway-pressure.
140. Mou J. Positive airway pressure intervention on patients with moderate-to-severe obstructive sleep apnea and resistant hypertension: engaging key stakeholders to understand what matters most. patient-centered outcomes research institute (PCORI). 2020. Available from: https://www.pcori.org/research-results/2017/positive-airway-pressure-intervention-patients-moderate-severe-obstructive.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.