")
Back to Journals » Journal of Pain Research » Volume 11
Personal experience and attitudes of pain medicine specialists in Israel regarding the medical use of cannabis for chronic pain
Authors Sharon H , Goldway N , Goor-Aryeh I , Eisenberg E, Brill S
Received 15 December 2017
Accepted for publication 2 March 2018
Published 31 July 2018 Volume 2018:11 Pages 1411—1419
DOI https://doi.org/10.2147/JPR.S159852
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Katherine Hanlon
Haggai Sharon,1–4 Noam Goldway,2 Itay Goor-Aryeh,5 Elon Eisenberg,6,7 Silviu Brill1,8
1Institute of Pain Medicine, Department of Anesthesiology and Critical Care Medicine, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel; 2Center for Brain Functions, Wohl Institute for Advanced Imaging, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel; 3Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel; 4Pain Management and Neuromodulation Centre, Guy’s and St Thomas’ Hospital, London, UK; 5Pain Center, Sheba Medical Center, Tel Hashomer, Israel; 6Institute for Pain Medicine, Rambam Health Care Campus, Haifa, Israel; 7Rappaport Faculty of Medicine, Technion Institute for Technology, Haifa, Israel; 8Goldman School of Medicine, Faculty of Health Sciences, Ben Gurion University of the Negev, Beer Sheva, Israel
Introduction: The scientific study of the role of cannabis in pain medicine still lags far behind the growing use driven by public approval. Accumulated clinical experience is therefore an important source of knowledge. However, no study to date has targeted physicians who actually use cannabis in their daily practice.
Methods: Registered, active, board-certified pain specialists in Israel (n=79) were asked to complete a Web-based survey. The survey was developed using the Qualtrics Online Survey Software. Questions were formulated as multiple-choice questions, and these addressed three areas of interest: 1) doctors’ personal experience; 2) the role of cannabis in pain medicine; and 3) cannabis medicalization and legalization.
Results: Sixty-four percent of all practicing pain specialists in Israel responded. Almost all prescribe cannabis. Among them, 63% find cannabis moderately to highly effective, 56% have encountered mild or no side effects, and only 5% perceive it as significantly harmful. Common indications are neuropathic pain (65%), oncological pain (50%), arthralgias (25%), and any intractable pain (29%). Leading contraindications are schizophrenia (76%), pregnancy/breastfeeding (65%), and age <18 years (59%). Only 12% rated cannabis as more hazardous than opiates. On a personal note, 45% prefer cannabis for themselves or a family member. Lastly, 54% would like to see cannabis legalized in Israel.
Conclusion: In this survey, pain clinicians experienced in prescribing cannabis over prolonged periods view it as an effective and relatively safe treatment for chronic pain, based on their own experience. Their responses suggest a possible change of paradigm from using cannabis as the last resort.
Keywords: cannabis, pain, survey
Introduction
The role of cannabis and cannabis-based pharmaceuticals in modern medicine is a topic of growing interest.1 This is especially true in clinical pain management, where standard treatments often fall short and there is an ongoing effort to find better and safer treatment options. Preliminary studies have so far provided only limited evidence to support the use of medical cannabis (MC) in the treatment of several chronic pain conditions,2 including neuropathic pain,3 visceral pain,4 arthritic pain,5,6 and headache.7 This is in part due to the considerable regulatory obstacles limiting clinical research on cannabis in most countries. At the same time, almost paradoxically, a growing number of countries permit the use of cannabis for medical purposes such as the control of pain. Nevertheless, even where there is some clinical use, making cannabis available for rigorous and widespread scientific research still lags behind clinical developments. This situation precludes establishing evidence-based professional guidelines and may in turn lead to much confusion among clinicians regarding basic practical issues related to MC. The accumulated clinical experience of physicians using cannabis in their daily practice is therefore of paramount importance. Only a few studies thus far have examined the attitude, beliefs, and knowledge of specialist physicians toward the clinical application of cannabis. Two older studies have explored the attitudes of US oncologists regarding the theoretical use of cannabis as an antiemetic, with only a minority supporting rescheduling of cannabis for this purpose8 and availability of cannabis on prescription.9 More recent studies attempted to address physician attitudes toward the general equations of medical use and legalization of cannabis10–12 or physicians’ educational gaps in the field.13 Of note, none of these studies has targeted physicians with actual experience in the clinical use of cannabis nor addressed practical questions relating to their accumulated experience.
Israel is one of the pioneers and world leaders in the study and application of cannabis for medical purposes. In accordance with the 1961 UN Convention on Narcotic Drugs, cannabis is still defined as a “dangerous substance” under Israeli law. However, in 2004, the Israeli Ministry of Health began issuing permits for compassionate use of cannabis in selected patients. Due to increased demand, the Ministry of Health formed a dedicated in-house government agency in 2011, the Medical Cannabis Unit (MCU), which authorizes and regulates cannabis growth, cultivation, distribution, medical use, and scientific research. In practice, a physician with a designated specialty relevant to the particular case at hand submits a licensure application to the MCU. If approved, the individual patient receives a prespecified monthly amount of cannabis (either as plant flowers or as cannabis oil) for 6–12 months. Follow-up appointments and scheduled renewals are mandatory. Of note, the prescribing physicians do not specify the exact composition of cannabis dispensed to the patient. These are determined by trial and error by the dispensing authority. This process is currently being revised with the formation of distinct preapproved strains, pharmacological grade analyses for growers, and so on.
Out of >30,000 licensed patients, the most common indication for MC use in Israel is chronic intractable pain, with figures steadily increasing. Accordingly, a considerable number of pain specialists in Israel have gained substantial, long-lasting experience following and monitoring patients on MC. Nevertheless, only two small surveys to date have evaluated Israeli physicians’ attitudes toward MC. In one study, 72 practitioners comprising a heterogeneous group with very limited experience with cannabis have voiced partial acceptance of MC for therapeutic use with concern for mental health implications.14 However, as mentioned, the overwhelming majority of their responders had no direct personal experience with cannabis at all as clinicians. The other study consisted of a very small sample of rheumatologists who supported some potential role for cannabinoids in the management of rheumatoid disease.15 It is therefore intriguing to examine the attitudes, beliefs, and personal experience of pain specialists in Israel regarding the medicinal use of cannabis, as they represent one of the largest potential reservoirs of clinicians who see and manage cannabis patients in their daily practice.
Materials and methods
In April–May 2017, all registered, active, board-certified pain specialists in Israel (n=79) were invited by email to complete a Web-based survey. The email included a short explanation about the survey, its structure, and the intended publication of the data. Therefore, completing and returning the survey was considered as informed consent.
Of note, a major limitation is the fact that after deliberating over the issue, we decided not to collect personal or demographic details regarding study participants. The community of pain specialists in Israel is a very small one and it would have been possible in principle to identify responders even based on basic demographic variables. Therefore, we have decided, despite the clear added value, to avoid collecting such data. Review and approval by an institutional review board (IRB) was not deemed necessary due to the following considerations: 1) it was a Web-based study targeting a healthy population, with no questions regarding the individual’s personal medical condition, no direct measurement of biological properties, and not involving any medical interventions; 2) responses were completely anonymized, and no personal data regarding the responders were collected in any data base.
The survey was developed using the Qualtrics Online Survey Software (Qualtrics, Provo, UT, USA). Server space and access to the Qualtrics application was provided by the Center for Brain Functions, Tel Aviv Sourasky Medical Center, as well as by Tel Aviv University. Questions were formulated as multiple-choice questions.
The survey consisted of 18 questions relating to three major areas of interest:
- Doctors’ personal experience with patients under their care
- The number of new cannabis permit requests issued per year
- Observed treatment efficacy and safety
- Whether they feel they received adequate education on MC during their fellowship training
- Views and beliefs regarding the role of cannabis in pain medicine
- The most suitable indications and contraindications, as well as estimated rates of addiction in pain patients
- A comparison of MC and opiates in terms of potential hazard, which should be attempted first, and their personal preference if they were patients themselves.
- Personal view regarding cannabis medicalization and legalization
- The need for a specialized government agency for MC approval and their view regarding its current professional framework
- Their view regarding legalizing the recreational use of cannabis
Statistical analyses
Statistical analyses were performed with IBM SPSS Statistics version 20 (IBM Corporation, Armonk, NY, USA). For all questions but two (Item numbers 1 and 2 in Section 2), we calculated the percentage of detectors that selected a certain answer out of the total pool of responders. For Questions 1 and 2 in Section 2, we calculated the percentage of “yes” responders for each item. We used the chi-square or independent samples t-test to examine our hypotheses.
Results
Fifty pain specialists responded to the survey, which represents 64% of all practicing pain specialists in Israel.
Doctors’ personal experience
Most responders (95%) prescribe cannabis in their pain practice: more than a half (54%) request cannabis for >20 patients per year, and a third issue >50 requests per year. Only 5% of specialists never prescribe cannabis for chronic pain (Figure 1A). Nearly two-thirds of responders (63%) find cannabis to be moderately to highly effective in treating patients with intractable chronic pain. An additional 20% find it marginally effective, and only 5% find it ineffective (Figure 1B). In terms of general safety, only three responders (7%) find cannabis marginally harmful; two (5%) perceive it as significantly harmful.
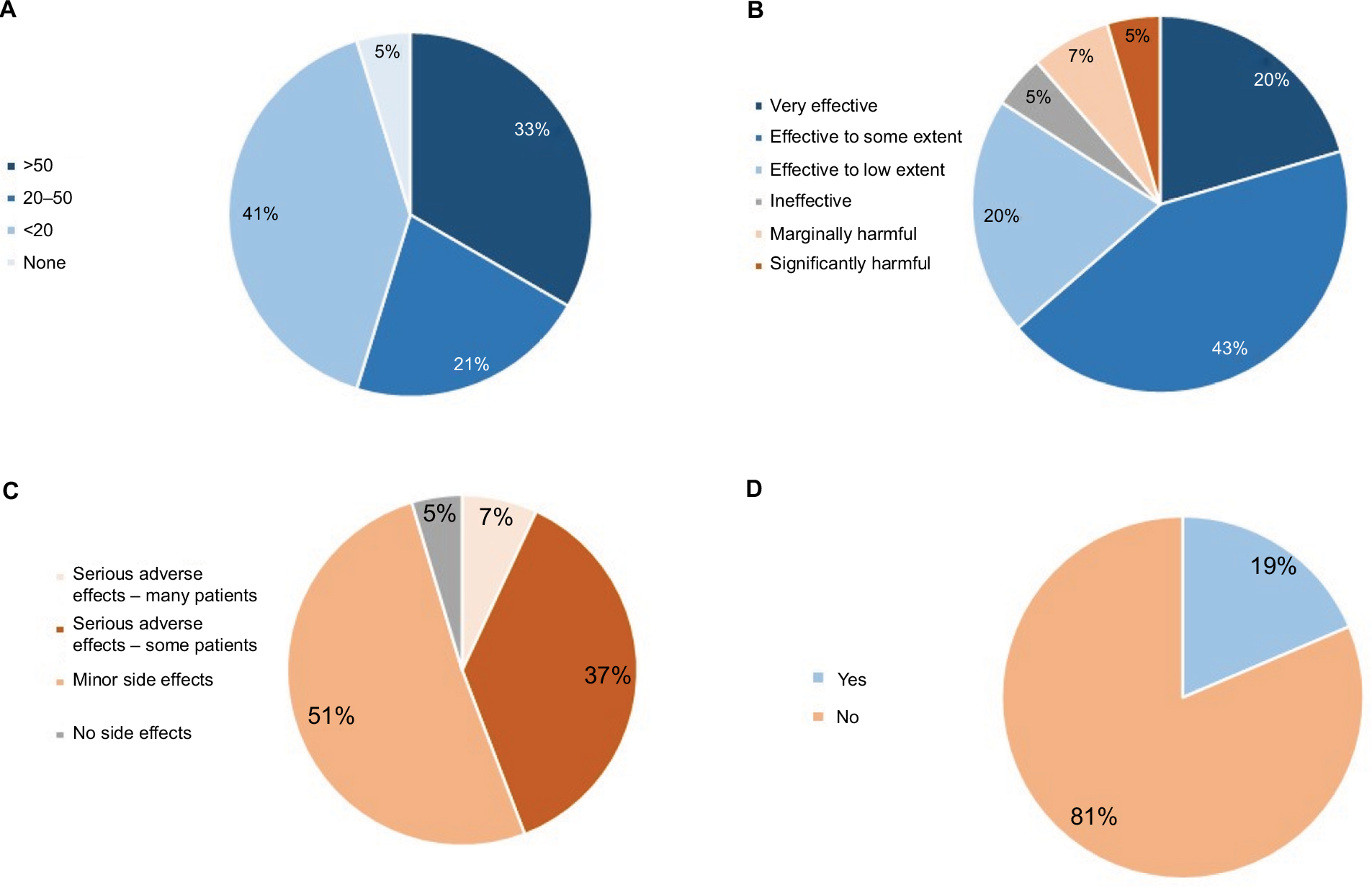 | Figure 1 Doctors’ personal experience with MC and patients under their care. Notes: (A) The number of new cannabis permit requests issued per year; (B) perceived treatment efficacy; (C) observed treatment safety; (D) do you feel that you received adequate education on MC during your fellowship training? Abbreviation: MC, medical cannabis. |
In terms of side effects, 25 responders (56%) state that they have encountered only mild or no side effects, and an additional 16 (37%) report observing serious adverse effects in few patients (Figure 1C).
Of note, 81% of pain clinicians feel that they have not received adequate education regarding the medical use of cannabis during their specialty training (Figure 1D).
Views and beliefs regarding the role of cannabis in pain medicine
The indications judged most suitable for starting cannabis treatment in patients were neuropathic pain, supported by nearly two-thirds (65%) of responders, followed by oncological pain supported by exactly half (50%), arthralgias related to rheumatic diseases by a quarter (25%), and any pain after failing previous conventional treatments by 29%. The least suitable were chronic low back pain (15%), visceral pain (12%), and chronic postoperative pain (8%). Fibromyalgia was considered an appropriate indication by 21% of responders (Figure 2A).
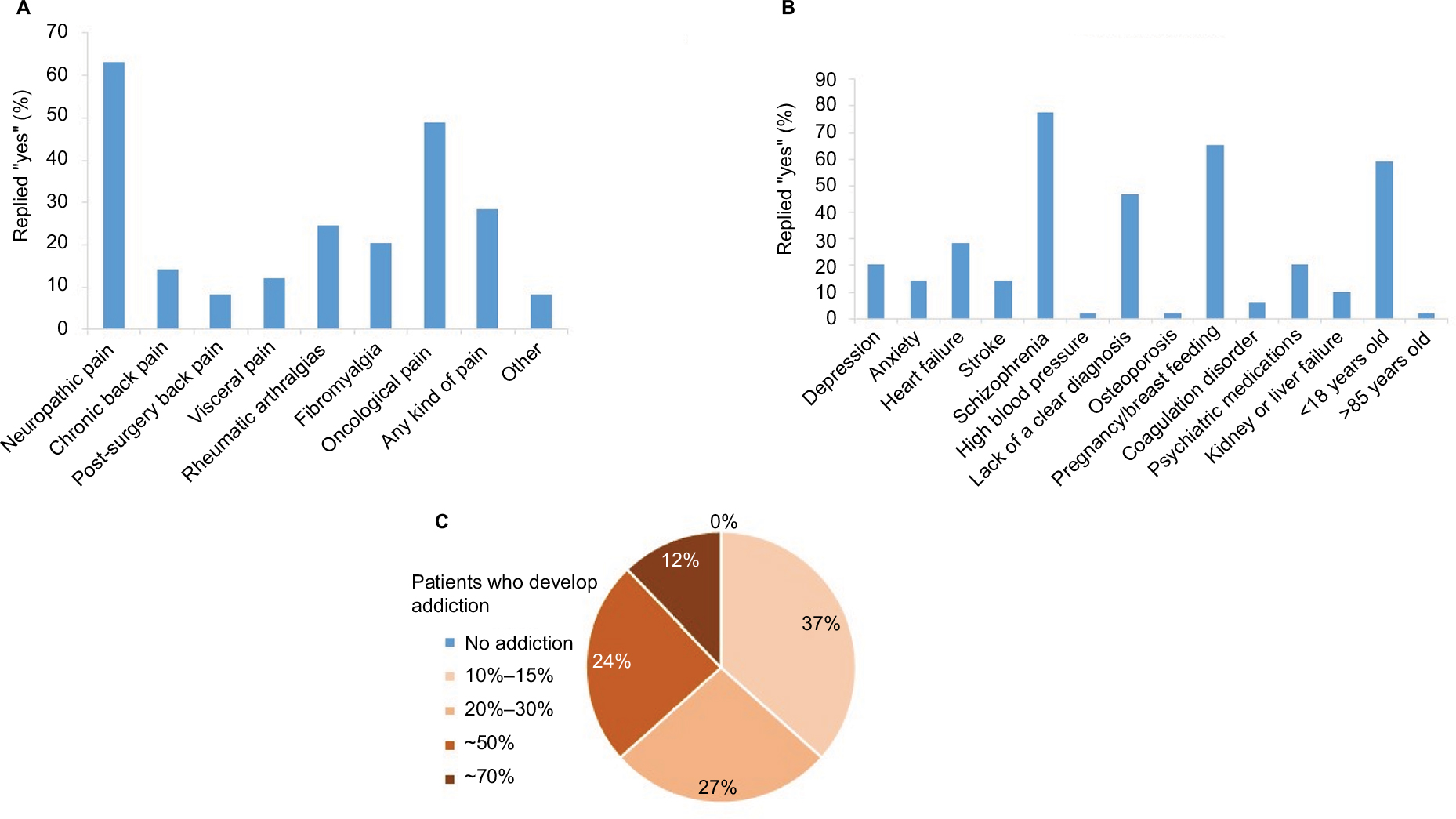 | Figure 2 Views and beliefs regarding the role of cannabis in pain medicine. Notes: (A) Most suitable indications; (B) contraindications; (C) rates of addiction. |
The most relevant contraindications were schizophrenia and previous psychosis (76% of the responders), followed by pregnancy/breastfeeding (65%) and age <18 years (59%). Lack of a clear diagnosis was considered a contraindication by 47%. Interestingly, despite growing evidence implicating cannabis use in adverse cardiovascular events,16,17 significant cardiovascular disease was only rated as a contraindication by 29% of responders and age >85 years was only considered a contraindication by one responder (2%) (Figure 2B). In terms of rates of addiction to cannabis in the context of medical use, 37% of the responders estimated that 10%–15% of patients develop addiction. However, the majority (63.4%) estimated it to be higher than that (Figure 2C).
Only 12% rated cannabis as more hazardous than opiates, whereas 43% felt that opiates are more hazardous than cannabis and 45% found them equally hazardous (Figure 3A). Nevertheless, 60% replied that opiate therapy should be exhausted prior to commencing cannabis treatment, with 40% opting for cannabis treatment prior to initiation of opiates (Figure 3B). On a personal note, when asked whether they would personally prefer for themselves or a family member to be treated with cannabis or opiates in case the need arises, 55% opted for opiate treatment, with 45% preferring treatment with cannabis (Figure 3C).
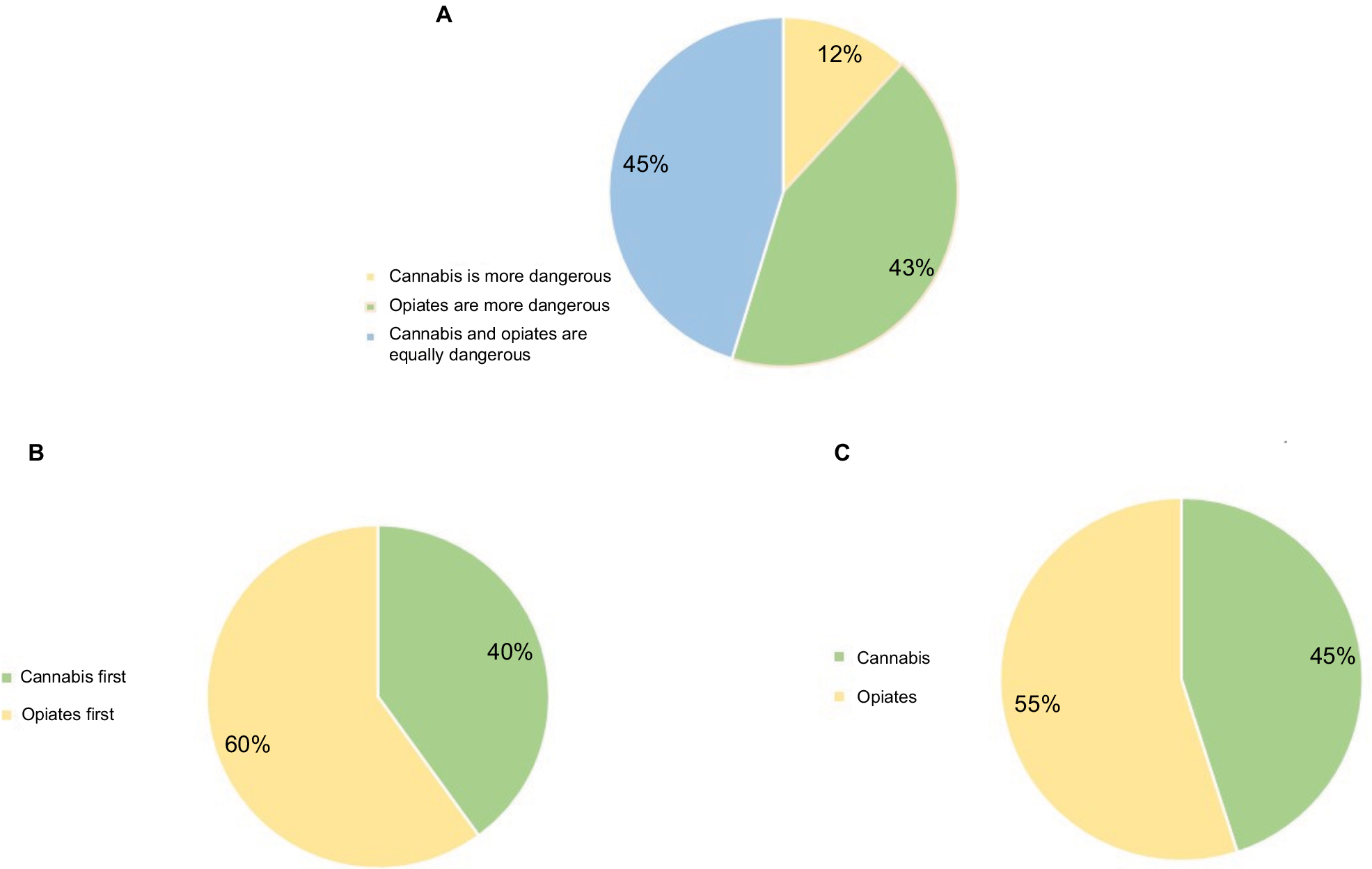 | Figure 3 Views and beliefs on the comparison of cannabis and opiates. Notes: (A) Is cannabis more or less hazardous to patients than opiates? (B) Which should be attempted first in pain patients? (C) Personal preference if you were patient yourself. |
Personal view regarding cannabis medicalization and legalization
Responders present divided views on the need for a specialized government agency that reviews and issues cannabis permits following the recommendation of a specialist: (51%) feel that such an agency is needed, compared with 49% who regard it redundant. When asked about the application process, 37% think that cannabis should be handled by specialists requested to complete prescriptions similar to those of other controlled medications (such as opiates or amphetamines). Additional 10% think that regular prescriptions completed by a specialist should suffice, and only one feels that any registered medical doctor should be able to directly prescribe cannabis (Figure 4A).
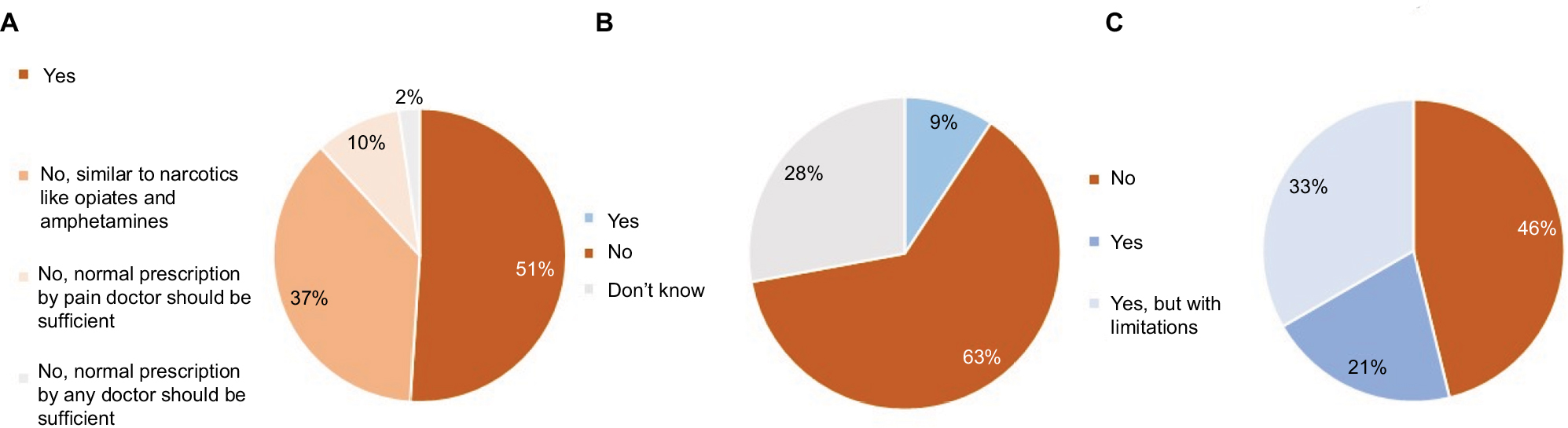 | Figure 4 Personal views regarding cannabis medicalization and legalization. Notes: (A) Should MC be prescribed via an MCU? (B) Does a valid professional framework underlie the MCU decisions? (C) Legalization (recreational use). Abbreviation: MC, medical cannabis; MCU, Medical Cannabis Unit. |
Nevertheless, the majority of all responders (63%) feel that the doctors reviewing applications on behalf of the MCU approve or decline them not based on clear criteria or a solid professional knowledge. Only 9% feel the opposite, while the remaining 28% respond that they do not know (Figure 4B). Notably, doctors with more experience in prescribing cannabis were more likely to feel there was no sound professional basis for these decisions (χ2=7.5, p<0.05).
Lastly, a little over a half of the responding pain specialists in Israel (54%) state that based on their experience in treating patients with cannabis for prolonged periods of time, they would like to see cannabis legalized in Israel, under an age limit (Figure 4C).
Interestingly, an informative approach was to divide responders based on whether they would personally prefer to be treated with cannabis rather than opiates. Responders who preferred cannabis (n=17), in comparison with those who preferred to be treated with opiates (n=22), apply for more cannabis permits per year (χ2=6.8, p<0.01) and would treat their patients with cannabis before using opiates (χ2=16.84, p<0.00005) (Figure 5A and B). Furthermore, all the doctors who prefer to be treated with cannabis are in favor of legalization and vice versa (χ2=37, p<0.0000001) (Figure 5C). Finally, this group rated cannabis as more effective (t(41) =2.75, p<0.01), and less addictive (t(39)=2.33, p<0.05) (Figure 5D and E).
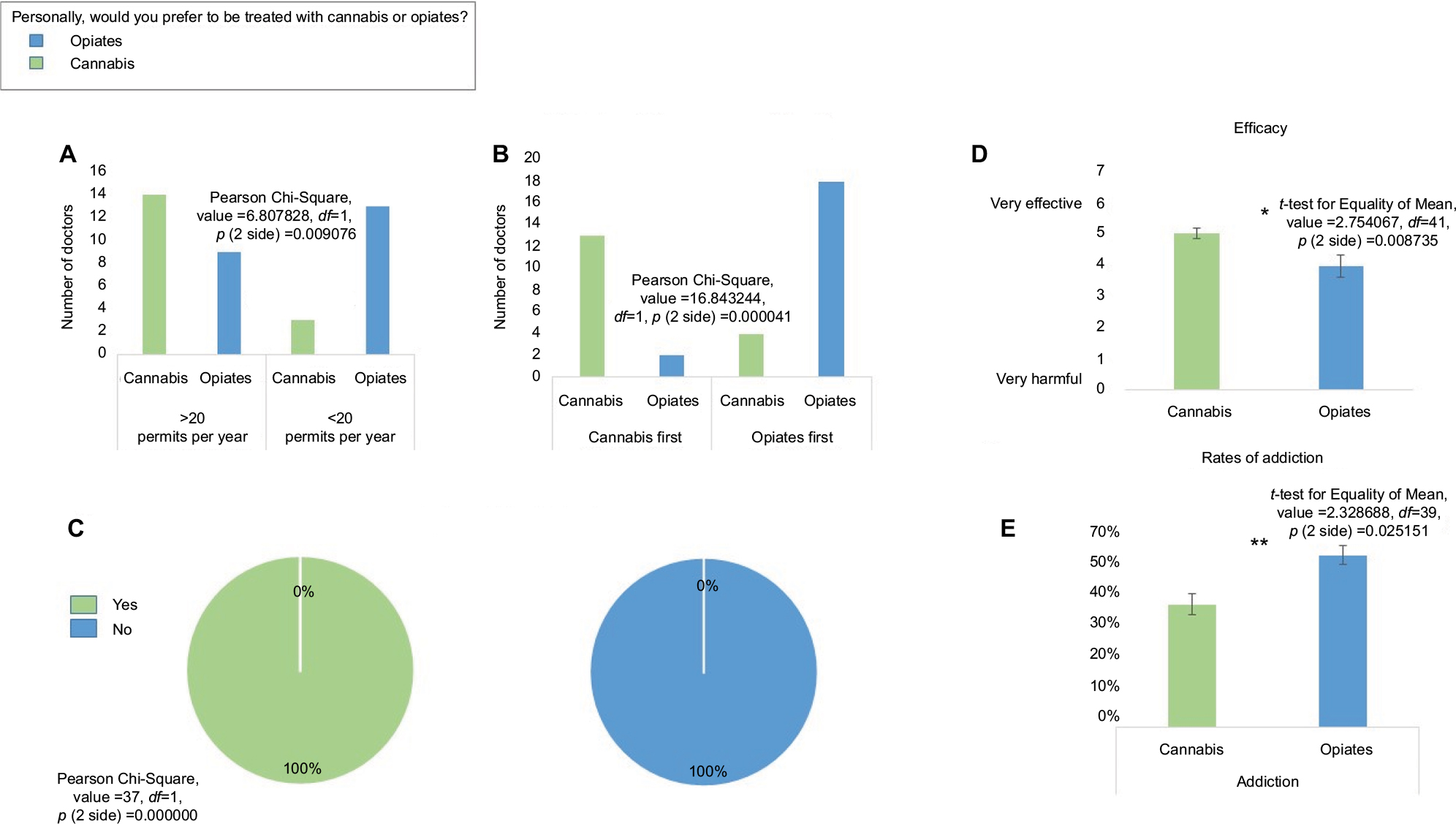 | Figure 5 Responses divided according to personal preference (cannabis or opiates) in case of personal need. Notes: (A) Number of new cannabis permits applied for per year. (B) Which should be attempted first? (C) Are you in favor of legalization? (D) Efficacy. (E) Rates of addiction. *p<0.05; **p<0.005. Error bars show standard error. |
Discussion
There is an obvious need to explore the potential role of cannabis as a part of the armamentarium for chronic pain management. Unfortunately, scientific evidence still lags far behind the growing use driven by public approval.18 Accumulated clinical experience is, therefore, in the meantime, a major source of knowledge that is important in guiding current practice. To date, this is the first survey examining attitudes toward the medical use of cannabis among a cohort of experienced pain specialists who actually use cannabis in their daily practice.
Of note, this survey has had impressive response rates – 50 out of 79 board-certified, active pain specialists have provided their inputs. The first emerging fact from this survey is that a majority of Israeli pain specialists are actively involved in the process leading to the use of cannabis by their patients. More than 90% of those involved in this process do so in their daily practice, with a third of the responders using it quite often. Similarly, a majority finds MC to be moderately to highly effective. This, by itself, is a significant finding, especially when considering the fact that patients treated with MC are, by definition, refractory to most existing therapeutic avenues. Moreover, it is generally agreed that the side effect profile is relatively favorable, with most pain specialists encountering only mild adverse effects in most patients and rare serious side effects.
Expanding evidence indicates that herbal cannabis has analgesic effects in both neuropathic and nonneuropathic pain.19 In terms of clinical indications, doctors in this survey tend to favor chronic pain states with a clear etiology or diagnosis, such as neuropathic pain, cancer-related pain, or rheumatic diseases. Accordingly, these are indeed three of the better-described indications in literature. The most robust evidence exists for neuropathic pain, and there are several high-quality randomized controlled clinical trials establishing the analgesic efficacy of smoked cannabis.3,20–22 Cancer-related pain has also been explored and has yielded similar supporting evidence for cannabis-induced analgesia.23,24 Similar data exist for pain associated with rheumatoid arthritis.25,26 For a more exhaustive recent review, refer the study by Hauser et al.27
Notably, all these leading indications are conditions that are amenable to objective diagnosis. Some (29%) also considered pain that is unresponsive to several acceptable lines of treatment as a possible indication, and a similar proportion also noted fibromyalgia as a considerable indication. This may reflect the helplessness that many pain specialists feel when dealing with these two patient populations, given the limited available effective treatment options for them.
Interestingly, low back pain and chronic postoperative pain, among the most common types of chronic pain syndromes seen in primary care and in pain clinics, were not considered to be good indications for MC treatment. This may reflect the basic distinction many physicians make between neuropathic and nociceptive pain syndromes (with these two conditions usually ascribed to the last, although this, of course, is not always the case). It may also stem from the fact that both conditions have many treatment options, a large body of literature to support current treatments, as well as updated and useful clinical guidelines.28,29
Most pain specialists view psychiatric morbidity, breastfeeding, and a young age as the leading contraindications. All these have indeed been implicated as potential contraindications,30–32 although there is still no clear consensus as to their scope and validity, as well as to the factors contributing to individual patient vulnerability to neuropsychiatric adverse effects.33 Medical conditions that have been suggested to be exacerbated by the use of cannabis, on the other hand, such as heart failure, arrhythmias, and excessive blood pressure,16,17,34 were not viewed as such by most pain specialists. This is surprising and may be due to gaps in knowledge rather than a well-informed stance. Similarly, when asked to estimate addiction rates, only 37% correctly estimated it to be 10%–15%, as we have recently reported in a prevalence study in two large tertiary pain clinics.35 Most have assumed higher rates of addiction, which is in accordance with the literature dealing mostly with addiction rates in recreational users, often adolescents, and does not relate to specific compositions of the cannabinoids used or to specific cannabis strains. The exact scope of addiction with cannabis is still largely debated. Some have claimed cumulative incidence as high as 37% after 3 years,36 while others have documented lower rates of a lifetime risk of 17% in those initiating cannabis use in early adolescence37 and still others have estimated the risk for users to develop dependence of 9% for cannabis, compared to 67.5% for nicotine and 22.7% for alcohol.38 As far as we are aware, there is no literature specifically evaluating cannabis misuse among patients with prescription-medical grade cannabis, except for our observation of 10%–15% addiction rates. The question of the addictive potential of cannabis across different life stages and psychosocial contexts therefore remains largely unresolved.
Such misconceptions regarding contraindications and addiction rates reflect a clear gap in knowledge. Indeed, >80% of responders feel that they had not received adequate training regarding cannabis use during their pain medicine training. It is interesting to note that while >90% of respondents do use cannabis, the vast majority still feel they were inadequately trained to do so. It may be seen as somewhat worrying that pain specialists are comfortable prescribing what they consider themselves untrained to use. This may reflect the fact that they are being pressured to use cannabis by public opinion rather than by medicinal considerations. Otherwise, it may reflect the difficulty in managing intractable pain patients, where often one turns to less-proven therapies and interventions in the face of ongoing suffering and dwindling options. Lastly, it may signify that pain specialists are not well trained in the use of cannabis but become aware and experienced during their posttraining medical practice. In any case, there is obviously a clear need for improvement in formal education on MC, since physicians practically use it in their clinics.
The comparison between MC and opiate therapy is intriguing for obvious reasons. Approximately 90% of pain specialists regard opiates as more than – or as hazardous – as cannabis, with only a small minority rating cannabis to be more hazardous than opiates. Most also feel that cannabis is moderately to highly effective (and this relates mostly to patients who have already failed opiate therapy, as this is a preliminary requirement for MC approval). However, only 40% feel that cannabis should be attempted before prescribing opiates, while most pain specialists still prefer exhausting opiate therapy prior to prescribing cannabis. This apparent discrepancy may stem from lingering biases but may also reflect the fact that doctors are more comfortable prescribing medications they have extensive literature on and that are properly manufactured, rather than using an unstandardized herbal product that is relatively unsupported, despite their own good experience with it. Lastly, this may represent a feeling that opiates are nevertheless more powerful analgesics than cannabis and therefore more efficacious.
Crucially, 45% of Israeli pain specialists state that they themselves would prefer to be treated with cannabis rather than opiates in case of chronic pain. While there still is a small opposing majority (55%), this can be seen as an overall vote of confidence in cannabis treatment.
In regards to legal and procedural issues concerning cannabis treatment, a small majority of responders feel that currently, there is a need for a specialized government agency for reviewing and handling cannabis permits. However, a large majority feels that, currently, this agency does not operate under any clear criteria or sound scientific knowledge. This view may change soon with the publication of Medical Grade Cannabis – Clinical Guide (Landschaft et al, unpublished data, 2017), nicknamed “The Green Book”, detailing current evidence and the guidelines they are operating under.
Lastly, a majority of Israeli pain specialists personally support the legalization of cannabis, provided there is an age restriction. This is extremely interesting since, as far as we know, this is the first survey of medical professionals reported thus far that shows such support. This may stem from the fact that these are pain specialists with actual experience with prescribing cannabis to a variety of patients under different conditions, who have had the chance to assess its overall and lasting effects, and have found them to be less daunting than assumed. Otherwise, it may also reflect the view that legalization may solve many problems and dilemmas that accompany medicalization, which in turn is often seen as a step toward cannabis legalization in the long run.
Interestingly, the question that was found to be most predictive of other favorable views on MC was whether the doctors preferred cannabis to opiates for themselves or a close family member in case of need. These doctors also prescribed more cannabis to their patients and thought it should be attempted prior to opiates. This may indeed reflect an independent personally held view. However, in light of the fact that these appear to be the doctors with more experience in prescribing cannabis, it may also suggest that more clinicians are experienced with the use of cannabis, and that there is a movement away from regarding cannabis as a dangerous substance in the same category as other class I drugs. If so, it may very well be that the role of cannabis in pain medicine may soon change, as more and more clinicians become experienced with its use. As their replies suggest, it may play a more central, as well as earlier, role in clinical pain management.
Conclusion
In the current survey, which probed the attitudes, beliefs, knowledge, and collected experience of pain specialists using cannabis in their daily practice, cannabis emerges as an effective treatment option for many patients with chronic pain who have failed previous treatments. Moreover, their responses arguably present a possible change of paradigm and the possibility to consider cannabis earlier in the course of the disease, and not as a last resort. In terms of side effect profile, it seems to be an acceptable option, although large population-based databases are required to address this issue in a more comprehensive manner. In light of the large gaps in knowledge, further research is needed to support or refute this practice. In the meantime, there is a clear need for better education on existing evidence and on practical issues pertaining to the use of MC in pain medicine.
Acknowledgment
This work was not funded by outside sources.
Author contributions
HS, SB, and IGA conceptualized and designed the study. HS and NG acquired the data and performed statistical analysis. All authors interpreted the data. HS, SB, and EE drafted the manuscript. All authors critically revised the manuscript and agreed to the final version.
Disclosure
The authors report no conflicts of interest in this work.
References
Hill KP. Medical marijuana for treatment of chronic pain and other medical and psychiatric problems: a clinical review. JAMA. 2015;313(24):2474–2483. | ||
Whiting PF, Wolff RF, Deshpande S, et al. Cannabinoids for medical use: a systematic review and meta-analysis. JAMA. 2015;313(24):2456–2473. | ||
Andreae MH, Carter GM, Shaparin N, et al. Inhaled cannabis for chronic neuropathic pain: a meta-analysis of individual patient data. J Pain. 2015;16(12):1221–1232. | ||
Goyal H, Singla U, Gupta U, May E. Role of cannabis in digestive disorders. Eur J Gastroenterol Hepatol. 2017;29(2):135–143. | ||
Barrie N, Kuruppu V, Manolios E, Ali M, Moghaddam M, Manolios N. Endocannabinoids in arthritis: current views and perspective. Int J Rheum Dis. 2017;20(7):789–797. | ||
Romero-Sandoval EA, Kolano AL, Alvarado-Vazquez PA. Cannabis and cannabinoids for chronic pain. Curr Rheumatol Rep. 2017;19(11):67. | ||
Kim PS, Fishman MA. Cannabis for pain and headaches: primer. Curr Pain Headache Rep. 2017;21(4):19. | ||
Schwartz RH, Voth EA, Sheridan MJ. Marijuana to prevent nausea and vomiting in cancer patients: a survey of clinical oncologists. South Med J. 1997;90(2):167–172. | ||
Doblin RE, Kleiman MA. Marijuana as antiemetic medicine: a survey of oncologists’ experiences and attitudes. J Clin Oncol. 1991;9(7):1314–1319. | ||
Charuvastra A, Friedmann PD, Stein MD. Physician attitudes regarding the prescription of medical marijuana. J Addict Dis. 2005;24(3):87–93. | ||
Kondrad E, Reid A. Colorado family physicians’ attitudes toward medical marijuana. J Am Board Fam Med. 2013;26(1):52–60. | ||
Crowley D, Collins C, Delargy I, Laird E, Van Hout MC. Irish general practitioner attitudes toward decriminalisation and medical use of cannabis: results from a national survey. Harm Reduct J. 2017;14(1):4. | ||
Ziemianski D, Capler R, Tekanoff R, Lacasse A, Luconi F, Ware MA. Cannabis in medicine: a national educational needs assessment among Canadian physicians. BMC Med Educ. 2015;15:52. | ||
Ebert T, Zolotov Y, Eliav S, Ginzburg O, Shapira I, Magnezi R. Assessment of Israeli physicians’ knowledge, experience and attitudes towards medical cannabis: a Pilot Study. Isr Med Assoc J. 2015;17(7):437–441. | ||
Ablin JN, Elkayam O, Fitzcharles MA. Attitudes of Israeli rheumatologists to the use of medical cannabis as therapy for rheumatic disorders. Rambam Maimonides Med J. 2016;7(2). | ||
Thomas G, Kloner RA, Rezkalla S. Adverse cardiovascular, cerebrovascular, and peripheral vascular effects of marijuana inhalation: what cardiologists need to know. Am J Cardiol. 2014;113(1):187–190. | ||
Franz CA, Frishman WH. Marijuana use and cardiovascular disease. Cardiol Rev. 2016;24(4):158–162. | ||
Bostwick JM. Blurred boundaries: the therapeutics and politics of medical marijuana. Mayo Clinic Proc. 2012;87(2):172–186. | ||
Lynch ME, Ware MA. Cannabinoids for the treatment of chronic non-cancer pain: an updated systematic review of randomized controlled trials. J Neuroimmune Pharmacol. 2015;10(2):293–301. | ||
Abrams DI, Jay CA, Shade SB, et al. Cannabis in painful HIV-associated sensory neuropathy: a randomized placebo-controlled trial. Neurology. 2007;68(7):515–521. | ||
Wallace MS, Marcotte TD, Umlauf A, Gouaux B, Atkinson JH. Efficacy of inhaled cannabis on painful diabetic neuropathy. J Pain. 2015;16(7):616–627. | ||
Ware MA, Wang T, Shapiro S, et al. Smoked cannabis for chronic neuropathic pain: a randomized controlled trial. CMAJ. 2010;182(14): E694–E701. | ||
Blake A, Wan BA, Malek L, et al. A selective review of medical cannabis in cancer pain management. Ann Palliat Med. 2017;6(suppl 2): S215–S222. | ||
Hauser W, Fitzcharles MA, Radbruch L, Petzke F. Cannabinoids in pain management and palliative medicine. Dtsch Arztebl Int. 2017;114(38):627–634. | ||
Lynch ME, Campbell F. Cannabinoids for treatment of chronic non-cancer pain; a systematic review of randomized trials. Br J Clin Pharmacol. 2011;72(5):735–744. | ||
Blake DR, Robson P, Ho M, Jubb RW, McCabe CS. Preliminary assessment of the efficacy, tolerability and safety of a cannabis-based medicine (Sativex) in the treatment of pain caused by rheumatoid arthritis. Rheumatology (Oxford). 2006;45(1):50–52. | ||
Hauser W, Petzke F, Fitzcharles MA. Efficacy, tolerability and safety of cannabis-based medicines for chronic pain management – an overview of systematic reviews. Eur J Pain. 2018;22(3):455–470. | ||
National Institute for Health and Care Excellence: Clinical Guidelines. Low Back Pain and Sciatica in Over 16s: Assessment and Management. London: NICE; 2016. | ||
Chou R, Gordon DB, de Leon-Casasola OA, et al. Management of postoperative pain: a clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016;17(2):131–157. | ||
Garry A, Rigourd V, Amirouche A, Fauroux V, Aubry S, Serreau R. Cannabis and breastfeeding. J Toxicol. 2009;2009:596149. | ||
Manrique-Garcia E, Zammit S, Dalman C, Hemmingsson T, Andreasson S, Allebeck P. Prognosis of schizophrenia in persons with and without a history of cannabis use. Psychol Med. 2014;44(12):2513–2521. | ||
Hadland SE, Knight JR, Harris SK. Medical marijuana: review of the science and implications for developmental-behavioral pediatric practice. J Dev Behav Pediatr. 2015;36(2):115–123. | ||
Curran HV, Freeman TP, Mokrysz C, Lewis DA, Morgan CJ, Parsons LH. Keep off the grass? Cannabis, cognition and addiction. Nat Rev Neurosci. 2016;17(5):293–306. | ||
Goyal H, Awad HH, Ghali JK. Role of cannabis in cardiovascular disorders. J Thorac Dis. 2017;9(7):2079–2092. | ||
Feingold D, Goor-Aryeh I, Bril S, Delayahu Y, Lev-Ran S. Problematic use of prescription opiates and medicinal cannabis among patients suffering from chronic pain. Pain Med. 2017;18(2):294–306. | ||
van der Pol P, Liebregts N, de Graaf R, Korf DJ, van den Brink W, van Laar M. Predicting the transition from frequent cannabis use to cannabis dependence: a three-year prospective study. Drug Alcohol Depend. 2013;133(2):352–359. | ||
Vsevolozhskaya OA, Anthony JC. Estimated probability of becoming a case of drug dependence in relation to duration of drug-taking experience: a functional analysis approach. Int J Methods Psychiatr Res. Epub 2017 Jun 29. | ||
Lopez-Quintero C, Perez de los Cobos J, Hasin DS, et al. Probability and predictors of transition from first use to dependence on nicotine, alcohol, cannabis, and cocaine: results of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Drug Alcohol Depend. 2011;115(1–2):120–130. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.