")
Back to Journals » Local and Regional Anesthesia » Volume 13
Peripheral Neuropathic Pain and Pain Related to Complex Regional Pain Syndrome with and without Fixed Dystonia – Efficient Therapeutic Approach with Local Anesthetics
Authors Michels T
Received 30 August 2019
Accepted for publication 17 December 2019
Published 31 January 2020 Volume 2020:13 Pages 11—16
DOI https://doi.org/10.2147/LRA.S229315
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Stefan Wirz
Thomas Michels
Internal Medicine, Hematology, Radiology, Natural Cure, Cologne (Köln) 50968, Germany
Correspondence: Thomas Michels
Internal Medicine, Hematology, Radiology, Natural Cure, Pferdmengesstr.8, Cologne (Köln) 50968, Germany
Email [email protected]
Abstract: Peripheral Neuropathic Pain (PNP) as well as the Complex Regional Pain Syndrome (CRPS), also known as “Reflex Sympathetic Dystrophy”, or “Sudeck Dystrophy”, all of them have a poor prognosis. The numerous therapeutic offers are rarely accompanied by convincing success over a long duration of time. Even worse is the prognosis of a fixed dystonia which may develop in the extremities of PNP or CRPS patients. In literature a few cases are reported in which the often unbearable pain of those patients with or without a disabling dystonia disappeared immediately after the injection of local anesthetics (LAs) into the scars of a preceding trauma. This review evaluates publications concerning the neuropathological characteristics of fixed dystonia in PNP/CRPS patients and the electrophysiological processes of scar neuromas. The results of these evaluations support the understanding of the therapeutic successes and their immediate results reported above by the injection of LAs into triggering scars. Therapeutic options are discussed.
Keywords: peripheral neuropathic pain, complex regional pain syndrome, fixed dystonia, scar neuroma, local anesthetics, subthreshold membrane potential oscillations
Definition and History of Peripheral Neuropathic Pain Conditions
In 1864 the term “causalgia” was introduced, describing terrible and long lasting pain of burning quality following nerve injuries of the limbs during the American Civil War.1
In 1902 the “Sudeck atrophy” of bones and muscles following traumas of the limbs accompanied by vasomotoric disturbances and edema was described.2
In 1916 the discussion of a sympathetic influence in causalgia was opened.3
In 1946 the term “reflex sympathetic dystrophy” was introduced to give the impression that a prolonged bombardment of pain impulses set up a vicious circle of reflexes in the spinal cord that generated efferent activity in the sympathetic system leading to spasms in the peripheral blood vessels and dystrophic changes in the periphery of the limbs.4
In 1986 and 8 years later in 1994, the International Association for the Study of Pain (IASP) introduced the term “complex regional pain syndrome” (CRPS):
Type I, synonym with reflex sympathetic dystrophy, “usually develops after an initiating noxious event, is not limited to the distribution of a single peripheral nerve, and is apparently disproportionate to the inciting event. It is associated at some point with evidence of edema, changes in skin blood flow, abnormal sudomotor activity in the region of pain, or allodynia or hyperalgesia.”
Type II is “associated with nerve injury, ‘causalgia’ (burning pain), and sometimes edema, plus changes in skin and blood flow and abnormal sudomotor activity in the region of pain”.5
In 2003 the “Budapest Criteria” (Table 1) improved the poor specificity (0.41) of the IASP criteria to a higher specificity (0.79) retaining the exceptional sensitivity of the IASP criteria (0.99).6
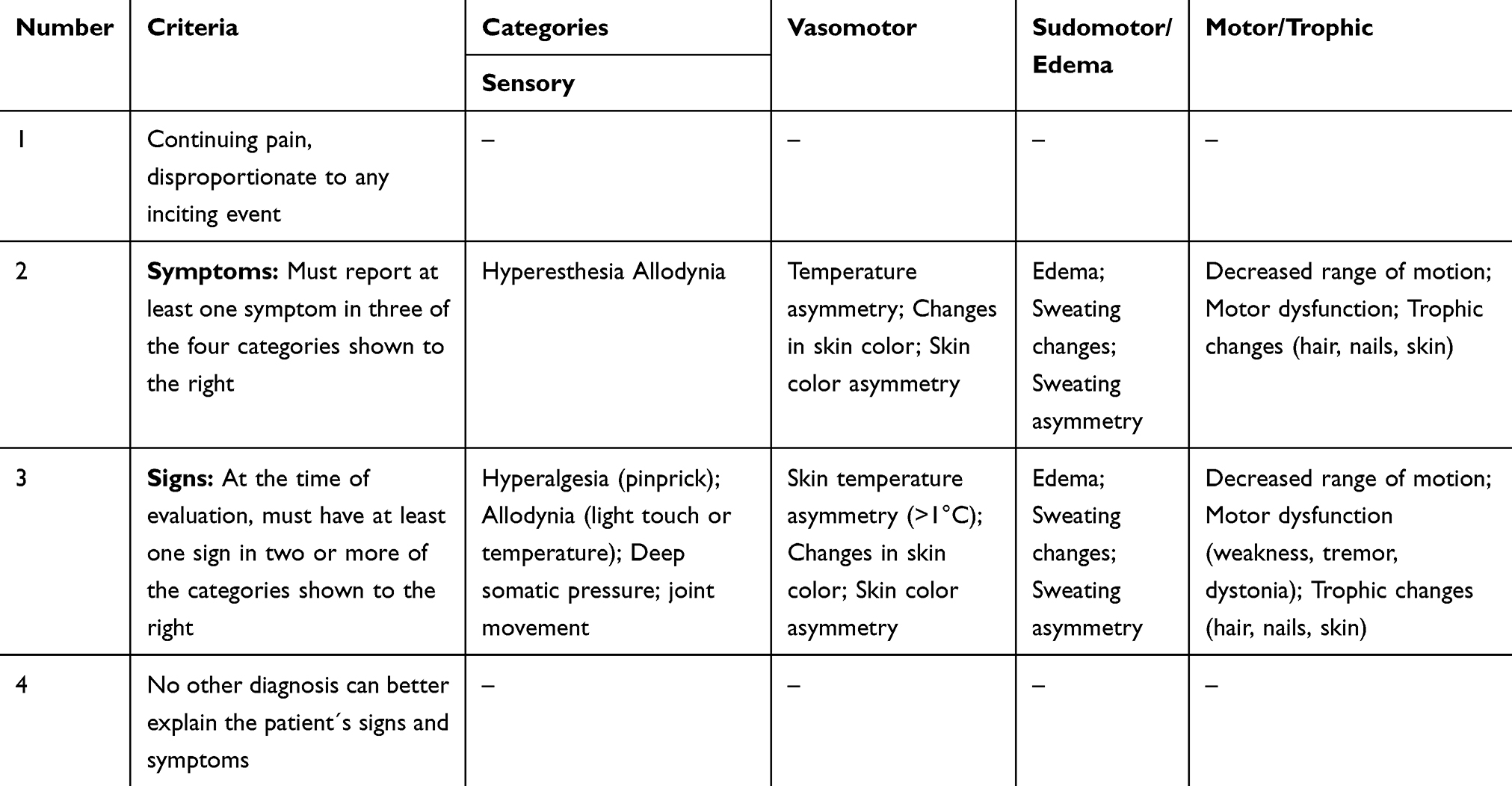 |
Table 1 The Budapest Criteria: 4 Criteria Must Be Met for the Clinical Diagnosis of CRPS |
About 20% of CRPS patients develop “fixed dystonia” characterized by fixed flexion postures of the fingers, wrists and feet (rarely extensions).7
Methods
Medline, PubMed, Livivo database was searched using the following terms: scar neuromas, local anesthetics, peripheral neuropathic pain, complex regional pain syndrome, fixed dystonia.
Prognosis
In spite of the fact that over decades local anesthetic sympathetic blockades have been undertaken in many patients very often they were not accompanied by convincing success of long duration as shown in a review evaluation of 12 studies with 461 cases of CRPS.8 Even if the sympathetic system does not initiate PNP/CRPS it is still assumed to contribute to its maintenance.9 Fixed dystonia in PNP/CRPS does not even improve after sympathetic blockades and its prognosis is typically poor.10,11
Therapeutic Approach via Scar Neuromas
A few authors described that the application of a local anesthetic (LA) into a scar which preceded PNP or a CRPS is immediately followed by the disappearance of the pain and of the fixed dystonia even if they had existed for years (Table 2).
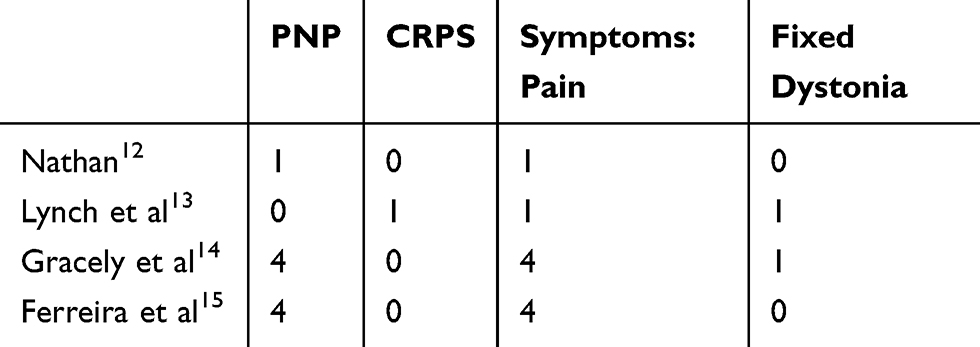 |
Table 2 LA Injections into Scars |
Nathan PW, 1960,12 reports that a burning pain in the right leg of a patient for a period of 18 months following an operation of a prolapsed intervertebral disc between the 2nd and 3rd lumbar vertebra had gone within 2 mins after an injection of lignocaine into the midline scar of the operation.
Lynch et al, 1991,13 presents a patient with reflex sympathetic dystrophy and severe contractures of the toes of the right foot over a duration of 24 months. Toes 2–5 were tightly flexed and the hallux was locked in flexion and curled beneath the sole. The patient was unable to move the toes. Immediately after the injection of lidocaine subcutaneously into two scars outside the area of motor abnormality the toes uncurled and the patient was then able to move them normally.
Gracely et al, 1992,14 published that in 1 of 4 cases with PNP “during the infiltration of lidocaine 1.5% along the trauma scar the contracted toes opened; the patient was able to move them normally. All spontaneous pain disappeared”. Lumbar sympathetic blocks had no effect on motor symptoms and were followed only by a relief of pain for a few hours.
Ferreira et al, 2012,15 reports that severe headaches presumably due to scar neuromas after craniotomy improved considerably after repeated injections of lidocaine 2% into the scar (2 cases) or vanished completely (2 cases, a follow-up of 2 years).
A similar case has also been observed in our office:
A 32 year old lady with CRPS and fixed dystonia of both hands and arms following a scalding of her right wrist with boiling water 4 years before was able to move her hands and fingers without any pain or movement disorder immediately after the injection of 0.4 mL of Procaine 0.5% into the 2 mm long scar on the volar side of her wrist. This condition lasted 21 hrs, returning to the original painfully fixed dystonia of both hands and disappeared in the same way after the next scar injections which were repeated by different doctors in different towns and were always followed by the same phenomena but with an increasing length of remission of up to 5 days during the following 3 months (unpublished).
In this case the spreading of pain, the development of the fixed dystonia and of its spreading to the opposite side followed a typical pattern as shown by the evaluation of 185 CRPS patients.15,16
Most impressive in these observations is that in PNP as well as in CRPS the pain improves or disappeares immediately after the application of LAs into the triggering scars. Also the movement disorders (fixed dystonia) which may develop in these pain conditions disappear completely and simultaneously with the accompanying pain.
Neurophysiological Findings in PNP/CRPS and Dystonia
One of the former master experts in pain research assumed already in 1989 that “the abnormalities of movements go off when the pain is relieved”.17
In a systematic review of “motor consequences of experimentally induced limb pain” it is stated, that “pain may induce immediate changes at all levels of motor control, irrespective to the source of pain” and that "cutaneous pain causes amplification of the nociceptive withdrawal reflex, most often seen in fixed dystonia with inward flexion of fingers an toes and the fixed inward flexion of the wrist and ankle."18
The immediate restoration of movement abnormalities (fixed dystonia) corresponds to the observation of a normal cortical activity during motor performances in 9 patients with CRPS and fixed dystonia as well as to the statement that “in line with earlier reports and regardless of the pain source there is no evidence of muscle hyperactivity”.18,19 Furthermore it was shown by EMG in 15 CRPS patients with abnormal postures and 15 healthy control persons that the deviant joint postures were not characterized by sustained muscle contractions or excessive muscle activity, which would have been typical of dystonia with a different origin than PNP/CRPS.20
In 10 patients with CRPS and fixed dystonia in the right upper limb the sensory motor plasticity was comparable to that of 10 healthy control persons and the CRPS patients showed a preserved topographic specificity.21
In a placebo-controlled study on the time-dependent relation between pain and motor function in affected arms of 29 CRPS patients it was found, that “motor function changes were mediated by, or occurred simultaneously with, changes in pain intensity” and it was concluded, that “pain relief may be an important factor in the treatment of motor disturbances in this condition”.22
Finally in a study with 33 patients with CRPS and dystonia and 19 healthy controls somatosensory-evoked potentials after spatially or temporally separated stimulation revealed that the “central sensory integration of proprioceptive afferent input is normal in patients with CRPS-related dystonia”.23
On the other hand in a one case presentation it was shown recently by magnetoencephalographic recordings in conjunction with somatosensory tactile stimulation that “the evolvement and spreading of the clinical symptoms in a CRPS patient was associated with major changes in the primary somatosensory cortical representation”.24
But an investigation in 19 female CRPS patients and 19 age- and sex-matched controls of healthy persons did not show differences of MRI data in brain structure or function.25
A recent review concerning neuropathic pain concludes that “clinical evidence demonstrates the essential role of peripheral mechanisms” and that “clinical evidence for autonomic central mechanisms remains relatively limited”.26
These observations make it very probable that the fixed dystonia in CRPS patients or in patients with PNP is due to the pain factor and is dissolved as soon as the pain disappears in accordance with our own observations and those of others.12–14
Electrophysiology of Pain Treatment in PNP or CRPS via Neuromas
The extinction of nociceptive afferent activity in neuromas by LAs has been long known in animals where “Na+ channel blockers consistently quenched neuroma firing. They did so by suppressing the process of impulse initiation. Only rarely was propagation block the dominant process.27 Meanwhile the suppression of impulse initiation by suppression of subthreshold membrane potential oscillations is well described. This suppression lasts much longer than a conduction block. It is induced by LAs in much lower concentration and quantity than necessary for conduction blocks and is followed by long lasting extinction of the connected pain.28–30
In a scar there are countless cut skin nerves, i.e. neuromas with an increased number of Na+ channels at their demyelinated blind end. This raises the latent excitability.31–34,36
It remains unclear so far, why most often scar neuromas remain passive and by which mechanism they start their pain inducing nociceptive afferent activity even after years of passiveness. It is assumed however, that the nociceptive afferent activity of a new trauma activates scar neuromas which had been passive so far via sympathetic efferent activity. It may happen in a similar way in which the rare diagonal spreading of a fixed dystonia in CRPS patients is preceeded by a second new nerve trauma in 91%.16
Therapeutic Options
To influence the pain in patients with PNP and in CRPS patients is commonly regarded as being extremely difficult. To influence the CRPS connected dystonia is even more so.10,11,37,38
Given this background it is suggested to begin the treatment in PNP or in CRPS with subcutaneous injections of low-dose LAs in and along the triggering scar especially when they are accompanied by a fixed dystonia. To prolong the duration of remissions it is recommended to repeat this procedure up to 20–30 times (1–2 times per week) and also to supplement it with sympathetic blockades even in a very reduced form by periosteal application.9,14,35,39
It is especially advisable to check for neuropathic pain due to postoperative nerve damage. Patients with those pains “are often misinterpreted and met with suspicion of malingering”.40
In 185 CRPS patients surgery as the preceding trauma was observed in 24.3%, and also corresponding in 123 CRPS patients the same origin was reported in 23.7%. The same percentage is reported with a laceration (and probable scars) of the preceding trauma.38 This means that in about 50% of all CRPS patients a triggering scar could be expected as a possible therapeutic access.
If the therapeutic interventions prove to be insufficient there are numerous other options for therapy. But the majority of patients does not receive satisfactory relief.37
A rather unnatural therapy is the excision of the scar neuroma which results in the creation of a new scar. But the belief that the operating of pain will only result in more pain may not apply. In a comparative meta-analysis comprising 54 articles “a meaningful reduction of pain was found in 77% of patients and no significant differences were seen between different surgical techniques”.41 In accordance with other studies the surgical intervention remains recommended only for patients with painful neuromas who are not responsive to medical or other treatments.42,43 It seems that the surgical procedure could at least partially dissolve the pain triggering mechanisms of the old scar neuromas, whereas the new scar neuromas created by this surgical procedure may follow new and different rules. This could support the suspicion that operating on a pain condition with a wrong assumption of its origin could still solve the pain problem at least partially.
Outlook
Finally it should be emphasized that “CRPS patients generally report a poorer quality of life than patients with other chronic pain conditions” (including cancer) as shown by an evaluation of 975 CRPS patients.44
Further studies to prove, to investigate, and to develop the role of scar neuromas in PNP and CRPS with and without dystonia seem to be desirable and worthwhile.
Ethics
A written informed consent for the publication of the case report has been obtained.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Mitchell SW. Gunshot Wounds and Other Injuries of Nerves. Philadelphia: J. B. Lippincott & Co; 1864.
2. Sudeck P. Ueber die akute (trophoneurotische) Knochenatrophie nach Entzündungen und Traumen der Extremitäten1). DMW. 1902;28(19):336–338. doi:10.1055/s-0029-1203535
3. Leriche R. La Chirurgie de La Douleur. Paris: Masson; 1937.
4. Evans JA. Reflex sympathetic dystrophy. Surg Gynecol Obstet. 1946;82:36–43.
5. Merskey H, Bogduk N. International association for the study of pain. In: Classification of Chronic Pain: Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms.
6. Harden RN, Bruehl S, Perez RSGM, et al. Validation of proposed diagnostic criteria (the “Budapest criteria”) for complex regional pain syndrome. Pain. 2010;150(2):268–274. doi:10.1016/j.pain.2010.04.030
7. van Hilten JJ. Movement disorders in complex regional pain syndrome. Pain Med Malden Mass. 2010;11(8):1274–1277. doi:10.1111/j.1526-4637.2010.00916.x
8. O’Connell NE, Wand BM, Gibson W, Carr DB, Birklein F, Stanton TR. Local anaesthetic sympathetic blockade for complex regional pain syndrome. Cochrane Database Syst Rev. 2016;(7). doi:10.1002/14651858.CD004598.pub4
9. Melis M, Zawawi K, al-Badawi E, Lobo LS, Mehta N. Complex regional pain syndrome in the head and neck: a review of the literature. J Orofac Pain. 2002;16(2):93–104.
10. Schott G. Peripherally-triggered CRPS and dystonia. Pain. 2007;130(3):203–207. doi:10.1016/j.pain.2007.04.013
11. Schrag A, Trimble M, Quinn N, Bhatia K. The syndrome of fixed dystonia: an evaluation of 103 patients. Brain J Neurol. 2004;127(Pt10):2360–2372. doi:10.1093/brain/awh262
12. Nathan PW. Improvement in cutaneous sensibility associated with relief of pain. J Neurol Neurosurg Psychiatry. 1960;23:202–206. doi:10.1136/jnnp.23.3.202
13. Lynch S, Gracely R H, Bennett G J. Contractures in a Patient With Reflex Sympathetic Dystrophy Reversibly Eliminated by Ischemic Block and Local Anethetic Infusion into a Putative Focus of Nociceptor Discharge. The Clinical Journal of Pain. 1991;7(1):48.
14. Gracely RH, Lynch SA, Bennett GJ. Painful neuropathy: altered central processing maintained dynamically by peripheral input. Pain. 1992;51(2):175–194. doi:10.1016/0304-3959(92)90259-E
15. Ferreira KDS, Dach F, Speciali JG. Scar neuromas as triggers for headache after craniotomy: clinical evidence. Arq Neuropsiquiatr. 2012;70(3):206–209. doi:10.1590/S0004-282X2012000300010
16. van Rijn MA, Marinus J, Putter H, Bosselaar SRJ, Moseley GL, van Hilten JJ. Spreading of complex regional pain syndrome: not a random process. J Neural Transm Vienna Austria 1996. 2011;118(9):1301–1309. doi:10.1007/s00702-011-0601-1
17. Nathan PW. The sympathetic system and pain. Funct Neurol. 1989;4(1):11–15.
18. Bank PJM, Peper CE, Marinus J, Beek PJ, van Hilten JJ. Motor consequences of experimentally induced limb pain: a systematic review. Eur J Pain Lond Engl. 2013;17(2):145–157. doi:10.1002/j.1532-2149.2012.00186.x
19. van Velzen GAJ, Marinus J, van Dijk JG, van Zwet EW, Schipper IB, van Hilten JJ. Motor cortical activity during motor tasks is normal in patients with complex regional pain syndrome. J Pain off J Am Pain Soc. 2015;16(1):87–94. doi:10.1016/j.jpain.2014.10.010
20. Bank PJM, Peper CLE, Marinus J, Beek PJ, van Hilten JJ. Deficient muscle activation in patients with complex regional pain syndrome and abnormal hand postures: an electromyographic evaluation. Clin Neurophysiol off J Int Fed Clin Neurophysiol. 2013;124(10):2025–2035. doi:10.1016/j.clinph.2013.03.029
21. Morgante F, Naro A, Terranova C, et al. Normal sensorimotor plasticity in complex regional pain syndrome with fixed posture of the hand. Mov Disord off J Mov Disord Soc. 2017;32(1):149–157. doi:10.1002/mds.26836
22. Schilder JCM, Sigtermans MJ, Schouten AC, et al. Pain relief is associated with improvement in motor function in complex regional pain syndrome type 1: secondary analysis of a placebo-controlled study on the effects of ketamine. J Pain off J Am Pain Soc. 2013;14(11):1514–1521. doi:10.1016/j.jpain.2013.07.013
23. van Rijn MA, van Hilten JJ, van Dijk JG. Spatiotemporal integration of sensory stimuli in complex regional pain syndrome and dystonia. J Neural Transm Vienna Austria 1996. 2009;116(5):559–565. doi:10.1007/s00702-009-0220-2
24. Büntjen L, Hopf J-M, Merkel C, et al. Somatosensory misrepresentation associated with chronic pain: spatiotemporal correlates of sensory perception in a patient following a complex regional pain syndrome spread. Front Neurol. 2017;8:142. doi:10.3389/fneur.2017.00142
25. van Velzen GAJ, Rombouts SARB, van Buchem MA, Marinus J, van Hilten JJ. Is the brain of complex regional pain syndrome patients truly different? Eur J Pain Lond Engl. 2016;20(10):1622–1633. doi:10.1002/ejp.882
26. Meacham K, Shepherd A, Mohapatra DP, Haroutounian S. Neuropathic pain: central vs. peripheral mechanisms. Curr Pain Headache Rep. 2017;21(6):28. doi:10.1007/s11916-017-0629-5
27. Matzner O, Devor M. Hyperexcitability at sites of nerve injury depends on voltage-sensitive Na+ channels. J Neurophysiol. 1994;72(1):349–359. doi:10.1152/jn.1994.72.1.349
28. Amir R, Michaelis M, Devor M. Membrane potential oscillations in dorsal root ganglion neurons: role in normal electrogenesis and neuropathic pain. J Neurosci off J Soc Neurosci. 1999;19(19):8589–8596. doi:10.1523/JNEUROSCI.19-19-08589.1999
29. Sukhotinsky I, Ben-Dor E, Raber P, Devor M. Key role of the dorsal root ganglion in neuropathic tactile hypersensibility. Eur J Pain. 2004;8(2):135–143. doi:10.1016/S1090-3801(03)00086-7
30. Amir R, Michaelis M, Devor M. Burst discharge in primary sensory neurons: triggered by subthreshold oscillations, maintained by depolarizing afterpotentials. J Neurosci off J Soc Neurosci. 2002;22(3):1187–1198. doi:10.1523/JNEUROSCI.22-03-01187.2002
31. Hilliges M, Wang L, Johansson O. Ultrastructural evidence for nerve fibers within all vital layers of the human epidermis. J Invest Dermatol. 1995;104(1):134–137. doi:10.1111/1523-1747.ep12613631
32. Ali Z, Ringkamp M, Hartke TV, et al. Uninjured C-fiber nociceptors develop spontaneous activity and alpha-adrenergic sensitivity following L6 spinal nerve ligation in monkey. J Neurophysiol. 1999;81(2):455–466. doi:10.1152/jn.1999.81.2.455
33. England JD, Gamboni F, Ferguson MA, Levinson SR. Sodium channels accumulate at the tips of injured axons. Muscle Nerve. 1994;17(6):593–598. doi:10.1002/mus.880170605
34. England JD, Happel LT, Kline DG, et al. Sodium channel accumulation in humans with painful neuromas. Neurology. 1996;47(1):272–276. doi:10.1212/WNL.47.1.272
35. Omana-Zapata I, Khabbaz MA, Hunter JC, Clarke DE, Bley KR. Tetrodotoxin inhibits neuropathic ectopic activity in neuromas, dorsal root ganglia and dorsal horn neurons. Pain. 1997;72(1–2):41–49. doi:10.1016/S0304-3959(97)00012-2
36. Michels T, Ahmadi S, Graf N. Treatment of peripheral pain with low-dose local anesthetics by epidermal, epithelial and periosteal application. Local Reg Anesth. 2018;11:129–136. doi:10.2147/LRA.S151316
37. Hegarty D. Abstracts from proceedings cork CRPS 2017: IASP special interest group in Complex Regional Pain Syndrome (CRPS). Pain Rep. 2018;3(1):e635. doi:10.1097/PR9.0000000000000635
38. Harden RN, Bruehl S, Galer BS, et al. Complex regional pain syndrome: are the IASP diagnostic criteria valid and sufficiently comprehensive? Pain. 1999;83(2):211–219. doi:10.1016/S0304-3959(99)00104-9
39. Loh L, Nathan PW. Painful peripheral states and sympathetic blocks. J Neurol Neurosurg Psychiatry. 1978;41(7):664–671. doi:10.1136/jnnp.41.7.664
40. Paltved CV, Kamp-Jensen M, Højsted J, Eriksen J. [Diagnosis and treatment of postoperative nerve damage. Chronic neuropathic pain]. Ugeskr Laeger. 1999;161(12):1739–1743.
41. Poppler L, Parikh R, Bichanich M, et al. Surgical interventions for the treatment of painful neuroma: a comparative meta-analysis. Pain. 2018;159(2):214–223. doi:10.1097/j.pain.0000000000001101
42. Domeshek LF, Krauss EM, Snyder-Warwick AK, et al. Surgical treatment of neuromas improves patient-reported pain, depression, and quality of life. Plast Reconstr Surg. 2017;139(2):407–418. doi:10.1097/PRS.0000000000003018
43. Wolvetang NH, Lans J, Verhiel SHW, Notermans BJ, Chen N, Eberlin K. Surgery for symptomatic neuroma: anatomic distribution and predictors of secondary surgery. Plast Reconstr Surg. 2019;143(6):1762–1771. doi:10.1097/PRS.0000000000005664
44. van Velzen GAJ, Perez RSGM, van Gestel MA, et al. Health-related quality of life in 975 patients with complex regional pain syndrome type 1. Pain. 2014;155(3):629–634. doi:10.1016/j.pain.2013.12.017
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.