")
Back to Journals » Journal of Inflammation Research » Volume 16
Perinatal Infection with Listeria monocytogenes: A 10-Year Hospital-Based Study in Western China
Authors Zhan Y, Xu T, Liu H, Wang X, Yu H
Received 12 December 2022
Accepted for publication 16 March 2023
Published 22 March 2023 Volume 2023:16 Pages 1243—1254
DOI https://doi.org/10.2147/JIR.S401171
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Adam D Bachstetter
Yongchi Zhan,1,2 Tingting Xu,1,2 Hongyan Liu,1,2 Xiaodong Wang,1,2 Haiyan Yu1,2
1Department of Obstetrics and Gynecology, West China Second University Hospital, Sichuan University, Chengdu, People’s Republic of China; 2Key Laboratory of Birth Defects and Related Diseases of Women and Children (Sichuan University), Ministry of Education, Chengdu, People’s Republic of China
Correspondence: Haiyan Yu; Xiaodong Wang, Department of Obstetrics and Gynecology, West China Second University Hospital; Key Laboratory of Birth Defects and Related Diseases of Women and Children, Sichuan University, No. 20, 3rd Section, South Renmin Road, Chengdu, Sichuan, 610041, People’s Republic of China, Email [email protected]; [email protected]
Objective: Listeriosis is a rare but severe foodborne disease that is contracted by the consumption of food contaminated with Listeria, and perinatal listeriosis can cause major adverse pregnancy outcomes. In the current study, we sought to retrospectively analyze 10 years of perinatal outcomes due to listeriosis in western China.
Methods: Based on the isolation of Listeria monocytogenes (L. monocytogenes), we retrospectively reviewed the pregnancy-associated cases of listeriosis from June 2010 to February 2022 at our hospital. We investigated the crude incidence, clinical manifestations, perinatal management, and outcomes of perinatal listeriosis cases.
Results: We diagnosed a total of 28 cases of perinatal listeriosis during the study period at our hospital, including four cases of twin pregnancies. Of the 28 cases, 32.14% (9/28) were infected in the second trimester and 67.86% (19/28) in the third trimester. The fetal or neonatal mortality rate for perinatal listeriosis was high, with a crude fetal mortality rate of 46.88% (15/32) in the 32 offspring and a neonatal mortality rate of 47.06% (8/17) in the 17 live births.
Conclusion: Perinatal listeriosis exhibits high fetal or neonatal mortality. We recommend that appropriate antibiotics be administered in cases of perinatal listeriosis.
Keywords: Listeria monocytogenes, bacteremia, perinatal listeriosis, perinatal outcomes
Introduction
Listeria monocytogenes (L. monocytogenes) is a Gram-positive, facultative intracellular pathogen that causes listeriosis, a rare but severe foodborne disease.1 L. monocytogenes can be found in a wide range of natural environments and contaminates many types of foods, even the processed foods found in refrigerators.2 Pregnant women, neonates, elderly individuals, and the immune-compromised population are more susceptible to listeriosis.1 During gestation, the high levels of estradiol and progesterone affect the immune system significantly, reducing T lymphocyte numbers and enhancing or maintaining innate immunity and increasing susceptibility to listeriosis.3
The estimated incidence of perinatal listeriosis varies by region. The crude incidence of perinatal listeriosis is 2.27–8.90 cases per 100,000 births in the American population,4 with a crude incidence of 12.3 cases per 100,000 births in New Zealand.5 According to published reports, perinatal cases in China account for 41–68% of listeriosis cases nationwide.6–10 However, the proven incidence of perinatal listeriosis in the general population remains unknown. One recent study showed the incidence of perinatal listeriosis at 13.7 per 100,000 deliveries at a maternity hospital in Beijing, China.11
Invasive listeriosis can be divided into three forms: Listeria bacteremia, neurolisteriosis, and perinatal listeriosis.1 Perinatal listeriosis exhibits clinical manifestations that are quite different from the general population, and is pernicious with respect to perinatal outcomes. While maternal symptoms can be non-specific with a mostly uneventful prognosis, the affected fetuses and neonates show a significantly increased risk of miscarriage, stillbirth, intrauterine demise, preterm birth, and long-term complications after birth, with a fetal and neonatal fatality rate as high as 20–35%.12 However, there are few reports on perinatal listeriosis, particularly in developing countries. Due to the lack of an adequate understanding and attention to this disease, there is an urgent need for further study regarding the gestational outcomes and management of perinatal listeriosis. We therefore conducted this retrospective, 10-year hospital-based study at West China Second University Hospital to analyze the clinical characteristics and outcomes of perinatal listeriosis.
Methods
Study Design and Data Collection
We retrospectively scrutinized the pregnancy-associated cases of L. monocytogenes infection from June of 2010 to February of 2022 at our hospital, a tertiary referral center for maternal and children’s health in western China. The study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board of West China Second University Hospital (no. 2022–148). Written informed consent was obtained for all material and clinical data from each patient.
Based on the data of laboratory-confirmed L. monocytogenes-positive cultured samples, we collected and reviewed the medical records of patients, including the maternal cases during the entire gestational period and related neonatal cases between birth and their first 28 days of life.13 Maternal information included demographic characteristics, obstetric history, clinical presentation, perinatal complications, laboratory findings, types of antimicrobial therapy, perinatal management, placental pathology, and perinatal outcomes. Neonatal data included neonatal symptoms at onset, sample cultures, neonatal complications, neonatal antibiotic exposure, early-onset listeriosis (1–6 days after birth), late-onset listeriosis (7–28 days after birth), and neonatal follow-up.12
The diagnosis of perinatal listeriosis is based on microbiologic evidence that includes the isolation of L. monocytogenes 1) from a normally sterile site from mothers and neonates, such as blood or cerebrospinal fluid (CSF); 2) from the products of conception by swabbing the placenta, uterus, and cervix; and 3) from neonatal sputum, or by swabbing the ear or pharynx.1,11
Listeria bacteremia is defined as the positive isolation of L. monocytogenes from blood cultures without neurolisteriosis. Neurolisteriosis, the central nervous system (CNS) infection with L. monocytogenes, is defined as 1) the isolation of L. monocytogenes from the CSF; and 2) CSF that was microbiologically negative, but where the patients manifested unexplained neurological symptoms such as altered consciousness, seizures, nuchal rigidity, or focal neurological symptoms with elevated white blood cell (WBC) count in the CSF and positive blood cultures for L. monocytogenes.1
We executed culture, isolation, identification, and drug-susceptibility testing of L. monocytogenes. The normally sterile samples (blood and CSF) were then added to blood culture bottles and cultured automatically in a BACTEC FX system (Becton Dickinson, USA). The traditional blood agar plating method was used for the pure growth of blood and CSF cultures and for other types of samples, followed by automated confirmation (VITEK-MS and VITEK2-COMPACT, Bio Merieux, France) of visible colonies.
Statistical Analysis
We conducted statistical analyses using SPSS 27.0 (IBM, USA), and adopted descriptive statistical methods for this study. Normally distributed data are presented as mean and standard deviations, while data that did not follow a normal distribution are presented as medians and ranges. Frequencies were used to describe the participants and outcomes.
Results
Between June 2010 and February 2022, we identified 28 cases of perinatal listeriosis, including 24 singleton pregnancies and four twin pregnancies (14.29%), the latter consisting of four dichorionic diamniotic (DCDA) twin pregnancies. The median maternal age was 29 years (range, 19–42 years) with a median hospital stay of 8.5 days (range, 3–23 days). Nine of the 28 patients (32.14%) were primiparous and four cases (14.29%) were conceived by in vitro fertilization and embryo transfer (IVF-ET). Among the 28 cases with listeriosis, nine (32.14%) were infected in the second trimester (range, 17 weeks 5 days to 27 weeks 6 days), while the other cases (67.86%) were infected in the third trimester (range, 28 weeks 1 day to 38 weeks 3 days). Detailed information is provided in Table 1.
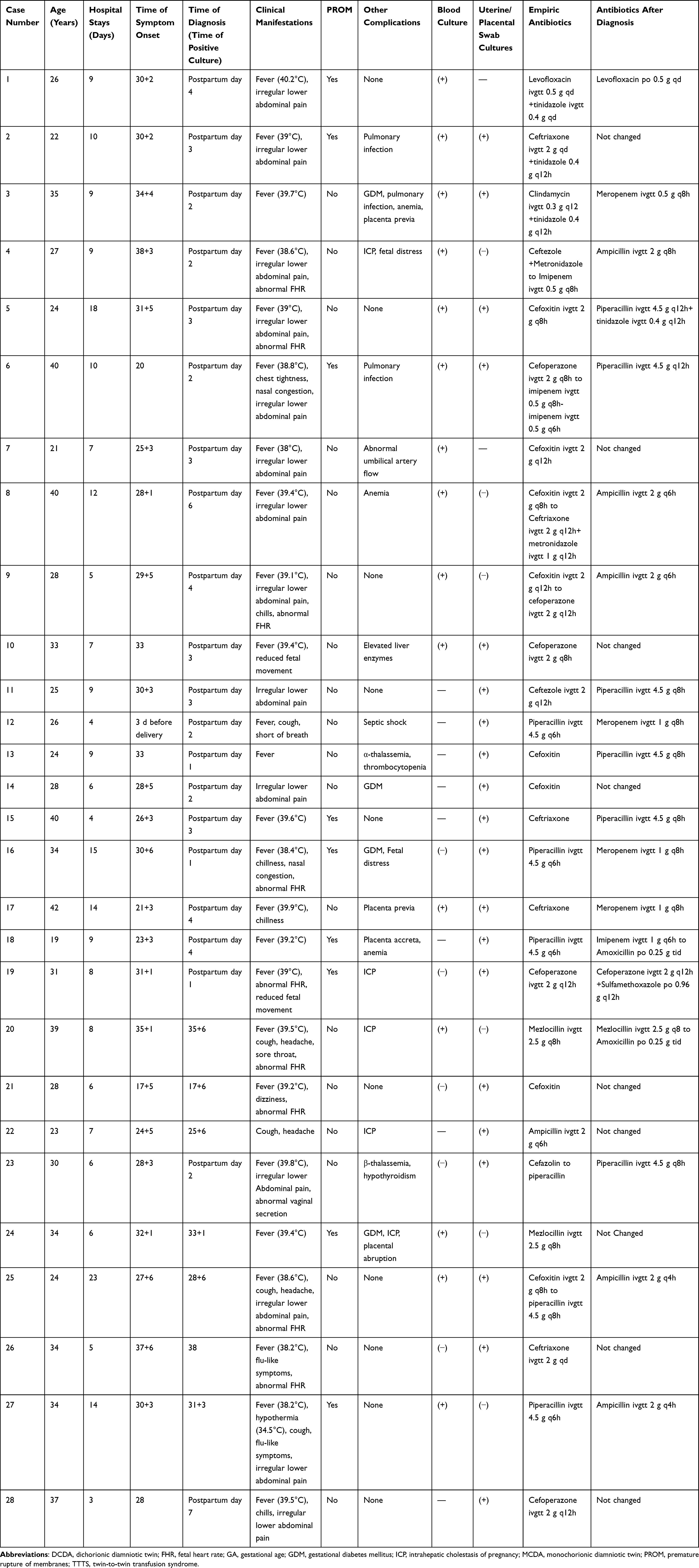 |
Table 1 Clinical Characteristics of Maternal Listeriosis |
The major prenatal maternal symptoms we noted were fever (25/28, 89.29%, 38–40.2°C), irregular abdominal pain (14/28, 50.0%), and flu-like symptoms (12/28, 42.86%). Moreover, in one case, the patient experienced hypothermia (34.5°C). Most of the non-specific symptoms were relieved after birth or with the appropriate use of antibiotics. Maternal complications were as follows: nine of 28 patients (32.14%) were found with premature rupture of membranes (PROM), nine cases (32.14%) with abnormal fetal heart rate (FHR), four cases (14.29%) with gestational diabetes mellitus (GDM), five cases (17.86%) with intrahepatic cholestasis of pregnancy (ICP), two cases (7.14%) with placenta previa, and one case (3.57%) with placental abruption.
Serial laboratory testing in cases of maternal listeriosis showed a maximal peripheral WBC count of (18.76±8.73)×109/L, of which 84.3% were neutrophil granulocytes (range, 60.7–99.6%), and a mononuclear cell count of 0.91±0.47×109/L. Assay of serum C-reactive protein (CRP) and procalcitonin (PCT) revealed an elevated level of serum CRP in 23 cases and augmented serum PCT in 19 cases.
Peripheral maternal blood cultures were collected and cultures were also obtained by swabbing other sites that included uterus, cervix, and placenta in 28 cases.
The 28 pregnant patients in our study all showed positive cultures for L. monocytogenes: eight women (28.57%) were positive for blood cultures; 13 women (46.43%) were positive for uterine, placental, or cervical swab cultures; and seven women (25.0%) were positive for both types of culture samples. The diagnosis of maternal Listeria bacteremia was established in 15 patients (53.57%). Three patients (cases 12, 18, and 25) were transferred to the intensive care unit (ICU), and one of these (case 12) experienced septic shock. None of the 28 maternal patients exhibited neurolisteriosis, and there was no case of perinatal maternal death related to listeriosis.
Empiric intravenous antibiotic treatment was administered to all cases prior to receiving the culture results for L. monocytogenes. Sixteen patients (16/28, 57.14%) received cephalosporins or cephamycin. Antibiotics were then adjusted according to the confirmation of L. monocytogenes and antibiotic sensitivity testing of the cultures.
Among the 28 women with perinatal listeriosis, there were 16 cases (57.14%) of preterm births, 7 (25.0%) with miscarriages before 28 completed weeks of gestation, and five (17.86%) cases with full-term births. Regarding delivery mode, 21 cases (75.0%) experienced a vaginal delivery and seven (25.0%) underwent cesarean sections. We observed meconium staining of amniotic fluid during labor or cesarean in 13 cases (46.43%).
The outcomes of the 32 fetuses in this study were as follows: 12 premature infants (37.5%), 15 fetal deaths (46.88%), and five full-term babies (15.63%). The crude neonatal mortality rate was 47.06% (8/17) in the 17 live births. In cases with maternal L. monocytogenes infection in the second trimester, the overall case-fatality rate among the offspring was 92.31% (12/13), while in the third trimester the overall case-fatality rate among the offspring was 52.63% (10/19) (detailed information is provided in Table 2). The median gestational age of the 17 live births was 31 weeks 2 days (range, 28 weeks 2 days to 39 weeks 3 days) with a median birth weight of 1585 g (range, 1240–3650 g).
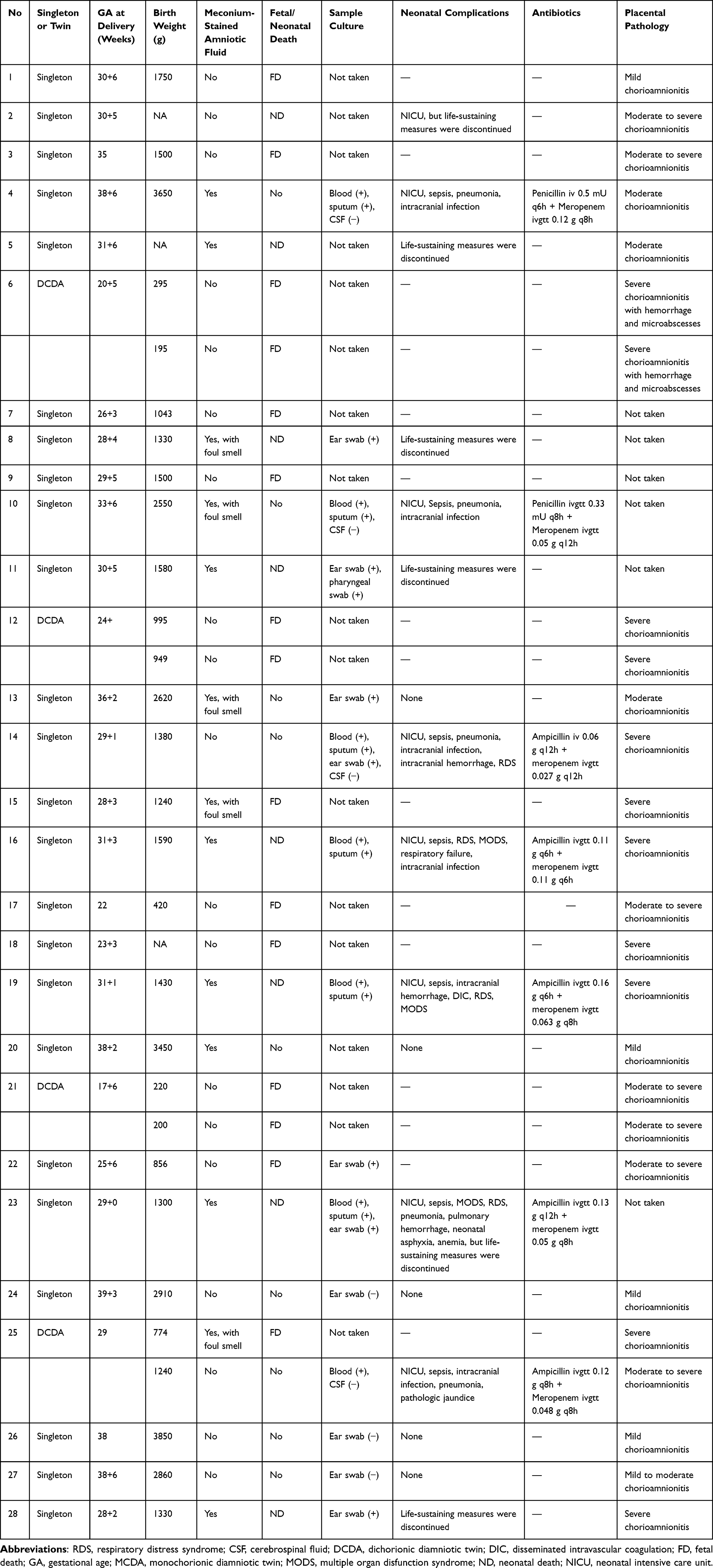 |
Table 2 Fetal and Neonatal Outcomes of 25 Cases |
Of the 17 live births, eight neonates exhibited Apgar scores lower than 8 at one minute. Eleven of the 17 live births (64.71%) had positive cultures for L. monocytogenes, including seven neonates (41.18%) diagnosed with Listeria bacteremia by positive blood culture. Four neonates (28.57%; cases 4, 10, 14, and 25) suffered seizures with elevated WBCs and protein in CSF, and their blood cultures were positive for L. monocytogenes. The diagnosis of CNS infection was established, whereas the microbiologic CSF cultures were negative for these four neonates. All of the neonatal patients manifested early-onset listeriosis, with the onset of symptoms and isolation of L. monocytogenes noted in the first seven days after birth.
Three cases (cases 20, 24, and 27) with maternal Listeria bacteremia received timely and effective antibiotic treatment, and this resulted in the prolongation of gestation and the delivery of healthy babies at term. In case 25, the outcomes for the twins were discordant, as follows: one twin underwent intrauterine demise while the co-twin was transferred to the neonatal intensive care unit (NICU) after vaginal delivery and survived. Eight of the 17 babies born alive died postnatally due to the severity of their illness and life-sustaining measures were discontinued. None of the other nine neonate survivors exhibited neurologic or neurodevelopmental sequelae during postpartum follow-up upon assistance from the Department of Children Healthcare and Department of Pediatric Neurology at our hospital.
Discussion
Pregnant women have a much higher susceptibility to infection with L. monocytogenes, which may be attributed to suppressed cellular immunity during gestation;3 multiple pregnancies are at greater risk for perinatal listeriosis than singleton pregnancies because of greater immunosuppression.14 We herein retrospectively reviewed the perinatal listeriosis cases over the past 10 years, and identified and analyzed 28 cases of perinatal listeriosis. The incidence of perinatal listeriosis is estimated to be 4–10/100,000 births in Europe and North America,15 while in Li’s study the estimated incidence of perinatal listeriosis was 13.7/100,000 at a maternity hospital in Beijing, China.11
The maternal symptoms of perinatal listeriosis are usually non-specific and this generates difficulty and delays in accurate prenatal diagnosis. Twenty-two of the 28 cases (78.57%) in our study were diagnosed with listeriosis in the postpartum period. Fever, mild flu-like symptoms, and non-specific obstetric signs (such as irregular uterine contractions, labor, and abnormal FHR) are the most frequent clinical manifestations of perinatal listeriosis,12,16 and infectious disease of the respiratory system or intrauterine infection is initially considered. In addition, not every maternal listeriosis patient is febrile; in fact, approximately 29% of maternal patients were asymptomatic in a previous case review, making the identification of perinatal listeriosis more difficult.17 The diagnosis of perinatal listeriosis relies on the isolation of L. monocytogenes from blood, CSF, or other bodily fluid. Maternal blood cultures were positive in only 55% of samples in a large national prospective cohort study in France, consistent with our study (53.57%), with placental and neonatal gastric fluid samples (positive in 78%) the most sensitive tissues for the isolation of L. monocytogenes, while neonatal CSF samples cultured positive in only 18% of samples.1 It is impossible to retrieve placental samples or neonatal bodily fluid prenatally, and thus the prenatal diagnosis of perinatal listeriosis is very problematic. Pathologic examinations of the placenta can provide us with characteristic findings that can reveal significant chorioamnionitis, macroabscesses, or microabscesses with focal necrosis and hemorrhage in the placenta infected with listeriosis.18 Although stool cultures used for the diagnosis of listeriosis are more controversial due to their low sensitivity,19 we postulate that they can be valuable for the prenatal diagnosis of listeriosis because they comprise an available diagnostic test that can be completed prenatally.
Maternal listeriosis is typically associated with uneventful prognosis and maternal death is rare. There was no neurolisteriosis or maternal death in our study and only one of our patients (case 12) experienced septic shock with no other underlying disease. However, infection with L. monocytogenes can cause severe fetal and neonatal outcomes, including spontaneous abortion, intrauterine fetal demise, stillbirth, preterm birth, and neonatal complications.12,16 In Charlier’s study, only 5% of the infected mothers experienced a normal delivery and a normal postpartum period, with 21% of cases enduring fetal loss.1 In another large cohort study published recently, the fetal loss rate was 46% among pregnant patients,20 while in our study the crude fetal fatality rate was 46.88% (15/32) of the 32 offspring; the neonatal fatality rate was 47.06% (8/17) in the 17 live births, with an overall case-fatality rate as high as 71.88% among the 32 offspring. This latter rate was much higher than the fatality rate reported previously, which may be attributed to the difficulty in prepartum diagnosis of perinatal listeriosis, as it is challenging to deliver appropriate antibiotics before the microbiologic isolation of L. monocytogenes.
A majority of listeriosis cases do not receive appropriate empiric antibiotics before microbiologic confirmation of L. monocytogenes, which is sensitive to numerous antibiotics, including ampicillin and penicillin, but is naturally resistant to cephalosporins.21 The American College of Obstetrics and Gynecology advises high-dose intravenous ampicillin (at least 6 g/d) for the treatment of symptomatic and febrile perinatal listeriosis patients.22 While all of the samples in our study underwent drug-resistance tests, none showed resistance to ampicillin or penicillin. In Li’s study, 66.67% of the maternal patients initially received cephalosporins,11 and in our study, 57.14% of patients initially received only cephalosporin or cephamycin antibiotics. Difficulties in both prepartum diagnosis of perinatal listeriosis and in administering appropriate antibiotics prior to the microbiologic isolation of L. monocytogenes precipitated an unexpectedly high fetal and neonatal fatality rate in our study. Anti-Listeria empiric therapy may be beneficial to undifferentiated febrile patients during pregnancy, which could prevent the development of and deterioration associated with perinatal listeriosis. However, most of the undifferentiated fever during pregnancy is attributed to viral infection, and perinatal listeriosis is uncommon.23 Whether empiric anti-Listeria antibiotics should be recommended for undifferentiated febrile pregnant women requires further investigation.
The gestational age at infection with L. monocytogenes is also related to fetal and neonatal survival rate.24 Charlier et al ascertained that fetal death was minimized when infection occurred after 29 weeks of gestation. According to Elinav’s study, each additional gestational week increased fetal survival by 33%.13
Infection with L. monocytogenes is not an indication for immediate delivery or emergency cesarean section. If the diagnosis of perinatal listeriosis can be established prenatally, appropriate and timely antibiotic therapy for listeriosis can improve fetal and neonatal outcomes. Three of our patients (cases 20, 24, and 27) initially received intravenous mezlocillin or piperacillin when they were febrile, but before the microbiologic diagnosis had been established. After the isolation of L. monocytogenes, cases 20 and 24 maintained and completed the mezlocillin therapy, and the antibiotics for case 27 were changed to ampicillin; they subsequently all went on to deliver healthy babies at full-term. Even infection with L. monocytogenes in the first trimester can achieve a favorable perinatal outcome after anti-Listeria therapy. Chan et al reported and reviewed their cases of maternal listeriosis in the first trimester, and seven of nine women underwent successful treatment with intravenous ampicillin and gentamicin, and only two women aborted.25
Perinatal listeriosis of twins can be discordant, such that one twin can be infected with L. monocytogenes with the co-twin remaining healthy.26 One of the patients in the present study (case 25) experienced the intrauterine demise of one twin, with the woman then delivering the co-twin vaginally and the baby surviving after transfer to the NICU. We hypothesize that chorionicity in twin pregnancies may explain such discordancy in neonatal outcomes.
Conclusions
In the present study, we identified and comprehensively summarized and analyzed a total of 28 cases of perinatal listeriosis over 10 years at a tertiary referral center for maternal and children’s health in western China. Listeriosis is a rare but severe foodborne disease that occurs due to the consumption of food contaminated with Listeria, and the prevalence of perinatal listeriosis may be underestimated in China. The consequences of L. monocytogenes infection during pregnancy and in neonates are often severe, and significantly adverse perinatal outcomes were revealed in our study; for example, the fetal and neonatal mortality rate was as high as 71.88% (23/32). We stress that appropriate antibiotics be administered in maternal and neonatal listeriosis as it constitutes a major public health concern, and we acknowledge the great challenges conferred in the management of perinatal listeriosis. In addition, there is an urgent need for a comprehensive Listeria surveillance system for pregnant women in China.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board of West China Second University Hospital (no. 2022-148), and informed consent was obtained from each patient.
Funding
This study was supported by the Natural Science Foundation of Sichuan (2022NSFSC0659), the Academic and Technical Leader’s Foundation of Sichuan Province (no. 2017-919-25), and the Science Foundation of Chengdu (no. 2021-YF05-01532-SN).
Disclosure
The authors report no conflicts of interest for this work.
References
1. Charlier C, Perrodeau É, Leclercq A, et al. Clinical features and prognostic factors of listeriosis: the MONALISA national prospective cohort study. Lancet Infect Dis. 2017;17:510–519. doi:10.1016/S1473-3099(16)30521-7
2. Moran LJ, Verwiel Y, Bahri Khomami M, et al. Nutrition and listeriosis during pregnancy: a systematic review. J Nutr Sci. 2018;7. doi:10.1017/jns.2018.16
3. Kourtis AP, Read JS, Jamieson DJ. Pregnancy and infection. N Engl J Med. 2014;370:2211–2218. doi:10.1056/NEJMra1213566
4. Silk BJ, Date KA, Jackson KA, et al. Invasive listeriosis in the Foodborne Diseases Active Surveillance Network (FoodNet), 2004–2009: further targeted prevention needed for higher-risk groups. Clin Infect Dis. 2012;54(Suppl 5):S396–404. doi:10.1093/cid/cis268
5. Jeffs E, Williman J, Brunton C, et al. The epidemiology of listeriosis in pregnant women and children in New Zealand from 1997 to 2016: an observational study. BMC Public Health. 2020;20:116. doi:10.1186/s12889-020-8221-z
6. Feng Y, Wu S, Varma JK, et al. Systematic review of human listeriosis in China, 1964–2010. Trop Med Int Health. 2013;18(10):1248–1256. doi:10.1111/tmi.12173
7. Li W, Bai L, Fu P, et al. The Epidemiology of Listeria monocytogenes in China. Foodborne Pathog Dis. 2018;15:459–466. doi:10.1089/fpd.2017.2409
8. Li W, Bai L, Ma X, et al. Sentinel listeriosis surveillance in selected hospitals, China, 2013–2017. Emerg Infect Dis. 2019;25:2274–2277. doi:10.3201/eid2512.180892
9. Fan Z, Xie J, Li Y, et al. Listeriosis in mainland China: a systematic review. Int J Infect Dis. 2019;81:17–24. doi:10.1016/j.ijid.2019.01.007
10. Chen S, Meng F, Sun X, et al. Epidemiology of human listeriosis in china during 2008–2017. Foodborne Pathog Dis. 2020;17:119–125. doi:10.1089/fpd.2019.2683
11. Li C, Zeng H, Ding X, et al. Perinatal listeriosis patients treated at a maternity hospital in Beijing, China, from 2013–2018. BMC Infect Dis. 2020;20:601. doi:10.1186/s12879-020-05327-6
12. Madjunkov M, Chaudhry S, Ito S. Listeriosis during pregnancy. Arch Gynecol Obstet. 2017;296:143–152. doi:10.1007/s00404-017-4401-1
13. Elinav H, Hershko-Klement A, Valinsky L, et al. Pregnancy-associated listeriosis: clinical characteristics and geospatial analysis of a 10-year period in Israel. Clin Infect Dis. 2014;59:953–961. doi:10.1093/cid/ciu504
14. Mascola L, Ewert DP, Eller A. Listeriosis: a previously unreported medical complication in women with multiple gestations. Am J Obstet Gynecol. 1994;170:1328–1332. doi:10.1016/S0002-9378(94)70151-2
15. Charlier C, Disson O, Lecuit M. Maternal-neonatal listeriosis. Virulence. 2020;11:391–397. doi:10.1080/21505594.2020.1759287
16. Lamont RF, Sobel J, Mazaki-Tovi S, et al. Listeriosis in human pregnancy: a systematic review. J Perinat Med. 2011;39:227–236. doi:10.1515/jpm.2011.035
17. Mylonakis E, Paliou M, Hohmann EL, et al. Listeriosis during pregnancy: a case series and review of 222 cases. Medicine. 2002;81(4):260–269. doi:10.1097/00005792-200207000-00002
18. Park JH, Ahn JH, Seo KJ, et al. Challenging management of chorioamnionitis with placental listeriosis: lessons from 2 cases. Obstet Gynecol Sci. 2018;61:688–692. doi:10.5468/ogs.2018.61.6.688
19. Elinav H, Hershko-Klement A, Solt I, et al. Pregnancy-associated listeriosis: many beliefs, few facts. Lancet Infect Dis. 2015;15(10):1128–1130. doi:10.1016/S1473-3099(15)00302-3
20. Thomas J, Govender N, McCarthy KM, et al. Outbreak of listeriosis in South Africa associated with processed meat. N Engl J Med. 2020;382:632–643. doi:10.1056/NEJMoa1907462
21. Swaminathan B, Gerner-Smidt P. The epidemiology of human listeriosis. Microbes Infect. 2007;9:1236–1243. doi:10.1016/j.micinf.2007.05.011
22. Committee on Obstetric Practice, American College of Obstetricians and Gynecologists. Committee Opinion No. 614: management of pregnant women with presumptive exposure to Listeria monocytogenes. Obstet Gynecol. 2014;124:1241–1244. doi:10.1097/01.AOG.0000457501.73326.6c
23. Charlier C, Perrodeau E, Levallois C, et al. Causes of fever in pregnant women with acute undifferentiated fever: a prospective multicentric study. Eur J Clin Microbiol Infect Dis. 2020;39:999–1002. doi:10.1007/s10096-019-03809-3
24. Tai YL, Chi H, Chiu NC, et al. Clinical features of neonatal listeriosis in Taiwan: a hospital-based study. J Microbiol Immunol Infect. 2019;53(6):866–874. doi:10.1016/j.jmii.2019.08.001
25. Chan LM, Lin HH, Hsiao SM. Successful treatment of maternal Listeria monocytogenes bacteremia in the first trimester of pregnancy: a case report and literature review. Taiwan J Obstet Gynecol. 2018;57:462–463. doi:10.1016/j.tjog.2018.04.025
26. Joshi MS. Intrauterine infection of non-presenting twin: a rare occurrence. J Obstet Gynaecol. 2006;26:565–569. doi:10.1080/01443610600821663
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.