")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Performance of the Arabic Population on the Adolescent-Adult Sensory Profile: An Observational Study
Authors Al-Momani F , Alghadir AH, Al-Momani MO, Alharethy S , Al-Sharman A, Al-Dibii R, Anwer S
Received 22 September 2019
Accepted for publication 13 November 2019
Published 7 January 2020 Volume 2020:16 Pages 35—42
DOI https://doi.org/10.2147/NDT.S232059
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Fidaa Al-Momani, 1 Ahmad H Alghadir, 2 Murad O Al-Momani, 3 Sami Alharethy, 3 Alham Al-Sharman, 1 Roya Al-Dibii, 4 Shahnawaz Anwer 2, 5
1Department of Rehabilitation Sciences, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Amman, Jordan; 2Rehabilitation Research Chair, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia; 3ENT Department, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 4Department of Statistics, Faculty of Science, Yarmouk University, Irbid, Jordan; 5Department of Building and Real Estate, Hong Kong Polytechnic University, Kowloon, Hong Kong Special Administrative Region, People’s Republic of China
Correspondence: Shahnawaz Anwer
Rehabilitation Research Chair, Cams, King Saud University, Riyadh 11433, Saudi Arabia
Email [email protected]
Background: The Adult-Adolescent Sensory Profile (AASP) is a questionnaire developed to measure the way in which people in different age groups respond to different sensory stimuli. These sensory stimuli may uncover different behavioral problems that may affect activities of daily living. This observational study aimed to validate the Arabic version of the AASP used to assess the sensory processing abilities of healthy individuals.
Methods: Participants comprised 560 Jordanians aged 11 years and older. Participants were recruited from different community centers in Amman, Jordan during 10th March 2017 to 10th September 2017. The English version of the AASP was translated into Arabic and all participants were instructed to complete this version of the scale.
Results: Internal consistency was 0.78 and 0.79 for the Arabic and the English version, respectively. The ranges of cut-off scores in the Arabic version were higher than the English version for all the quadrants of the scale. The biggest differences were found in the sensation seeking and sensory sensitivity quadrants. In certain age groups (11– 17 and 18– 64 years), women were more sensitive compared with men.
Conclusion: The Arabic version of the AASP showed good internal consistency and can be used to assess the sensory processing abilities of healthy individuals.
Keywords: adolescent/adult sensory profile, translation, reliability, arabic, sensory processing
Corrigendum for this paper has been published
Introduction
Sensory Profiles are commonly used outcome measures among occupational therapists in the United States1 and are used to evaluate sensory processing difficulties in clients from birth to advanced age.2,3 The standardization, reliability, and validity of Sensory Profiles have been reported in previous studies.4,5 There are currently four Sensory Profile versions: the Sensory Profile Caregiver questionnaire, Infant-Toddler Sensory Profile, Adult-Adolescent Sensory Profile, and the School Companion Sensory Profile.
The Adult-Adolescent Sensory Profile (AASP) is a questionnaire developed to measure the way in which people in different age groups respond to different sensory stimuli. These sensory stimuli may uncover different behavioral problems that may affect activities of daily living (ADL). This questionnaire was designed by Dunn and standardized in the United States of America for individuals aged 12 years and above.6 This instrument includes 6 sections: taste and smell processing section, movement processing, visual processing, touch processing, activity level, and auditory processing. The total scale comprises 60 items in three main areas. The first area assesses modulation or the ability to regulate sensory inputs that affect ADL. The second area assesses sensory processing or the ability to interpret different sensory inputs related to different sensory systems. The third area assesses behavioral and emotional responses or the ability to process sensory stimulation and respond to it.6
Problems in sensory processing may result from the emotional burden that people may experience such as in anxiety and depression.7,8 Previous research has indicated that problems in sensory processing may present in adulthood and affect functional performance and participation in ADL,3 mental health problems, social participation, and quality of life.9–11 Therefore, it is necessary to study sensory processing difficulties among different age groups and their impact on daily functioning.
In the last century, occupational therapy (OT) has spread across the world including Arabic speaking countries. There are many schools of OT distributed all over the Arabic countries (e.g., Jordan, Kuwait, Saudi Arabia) and most of these schools (e.g., Jordan University of Science and Technology, Jordan University, Hashemait University) are accredited by the World Federation of Occupational Therapy (WFOT). In addition, there are many Arabic associations of OT and most are approved by the WFOT. However, there are some barriers faced by occupational therapists in Arabic countries. First, there is a lack of published literature to provide evidence-based practice in areas related to OT. Second, although in some Arabic countries OT practice is well-established, in other countries the OT program is either just starting or has not yet developed as a profession. Third, most OT literature is available in the English language and evidence (literature/research) written in the Arabic language may not be available in English.
Translation of an instrument from one language to another is a complex procedure that must consider both cultural and language differences.7,9,11–16 The lack of standardized instruments in Arabic is considered one of the most common barriers as it limits the ability to perform research. However, translating instruments from English to Arabic is becoming a very common procedure today for health professions in Arabic-speaking countries.17–21
The present study aimed to: (a) validate the Arabic version of the AASP (b) investigate sensory processing abilities among a group of healthy Jordanian adolescents, adults, and older adults, and (c) examine the relationship between age and gender with sensory processing performance.
Methods
A cross sectional questionnaire-based survey was used to assess the sensory processing abilities of healthy adolescents, adults, and older adults. Based on age and gender, the sample was stratified and compared to determine the relationship between age and gender with sensory processing performance.
Instruments
First, a demographic questionnaire was used in this study which included items regarding age, gender, academic level, area of residence, and annual family income. Second, AASP, which is a 60-item questionnaire that assesses the way in which individuals respond to different sensory stimuli, was used. Brown et al3 developed this instrument based on the sensory profile6 to obtain the profile for adolescents and adults aged 11 years and older.
The AASP includes four subscales: sensory sensitivity, sensation avoiding, low registration, and sensation seeking. Individuals with a high neurological threshold are not able to detect sensation and use of passive behavior indicates low registration. These individuals were found to be quiet, obedient, and unable to recognize or express emotions.22 Individuals with a high neurological threshold who typically look for a rich sensory environment refers to sensation seeking. These individuals may engage in activities with increased motor behaviors, and seek strong stimuli such as spicy food, stimulating noises, and visuals.22 Sensory sensitivity refers to people with a low neurological threshold who are diverted by and feel uneasiness with sensations, yet do not constrain their exposure to uncomfortable sensations. They are easily diverted from various stimuli, for example, smells, sounds, clothing tags, or certain textures.2 Individuals with a low neurological threshold who usually limit their exposure to sensory stimuli refers to sensation avoiding behavior. They avoid distracting settings and make day-by-day schedules to reduce unpredictable situations.3
Translation Procedure
After obtaining permission from the copyright holder, the AASP was translated into Arabic using the published guidelines.23–25 Four bilingual occupational therapists made the forward translation of AASP items into Arabic. The differences among the translators were discussed and a final agreement was determined by consensus. A revision of this version was made after pilot testing with 40 participants. A backward translation was done by a bilingual translator who is a native English speaker born in the United States who also speaks Arabic fluently and lives in Jordan.
A group of 10 researchers evaluated and discussed the original and the back-translated items to investigate the degree of similarity between the back-translated items and the items of the original version. To determine the adequacy of the Arabic translation, a cut-off score of 0.8 or higher was selected (score range, 0 = not similar, 1 = similar). This cut-off score suggested that no less than 80% of the evaluators concurred that the back-translated item was similar to the original sensory profile item. A score below 0.8 suggested a possible issue with the interpretation.
Reliability Procedure
A total of 87 participants aged 11 years and older (mean age = 38.6 years, SD = 3.4) participated in this cross-sectional study to determine the reliability of the AASP. The sample was selected randomly from different community centres in Amman, Jordan during 10th March 2017 to 10 September 2017, with differing socioeconomic status representing the normal distribution of the population. Based on age, the sample was divided into three groups: adolescent (11–17 years, n=20), adult (18–64 years, n=33), and older adult (65 years and more, n=34). All participants were requested to sign an informed consent form approved by Institutional Review Board (IRB) of Dean of faculty of applied medical sciences, Jordan University of Science & Technology, Jordan (Ref.: 8/103/2017). Additionally, parental informed consent was also obtained for the minor participants. Individuals were eligible to participate in the study if they had a good knowledge of Arabic and English languages and had lived at least four years in each of the United States and Jordan. Each participant was requested to fill out the English and Arabic copies of AASP, separately over a period of two weeks. This study was conducted in accordance with the Declaration of Helsinki.
Standardization of Arabic Version
The final Arabic version of the AASP was completed by a sample of 560 adolescents and adults. The sample was selected randomly from different geographic areas in Jordan with participants of differing socioeconomic status representing the normal distribution of the population. Based on age, the sample was divided into three groups: adolescent, adult, and older adult.
Statistical Analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS) software version 11.0 (SPSS®: Inc., Chicago, IL, USA). The classification system for the AASP scale was derived by examining the frequency distribution of scores in the standardization sample. The scores were approximately normally distributed. Different cut-off scores were established for adolescents, adults, and older adults for each quadrant/subscale. Cut-off scores for the classification system were established as follows: much less than most people = less than 2% of the study population, less than most people = between 2% and below 16% of the study population, similar to most people = between 16% to 84% of the study population, more than most people = between greater than 84% and 98% of the study population, much more than most people = greater than 98% of the study population. To determine internal consistency, Cronbach’s alpha coefficient was calculated. Moreover, the difference between genders on AASP scores [Mean (SD)] in each age group were calculated. Independent t-tests were used for comparison between genders on sensory profile subset scores. A P ≤ 0.05 was selected for the level of significance.
Results
A total of 560 Jordanian adults (18–64 years and ≥ 65 years) and adolescents (11–17 years) completed the Arabic questionnaire. Demographics details of the participants are presented in Table 1. Internal consistency, cut-off scores for the Arabic version, and the relationship between gender and sensory processing in the different age groups are reported.
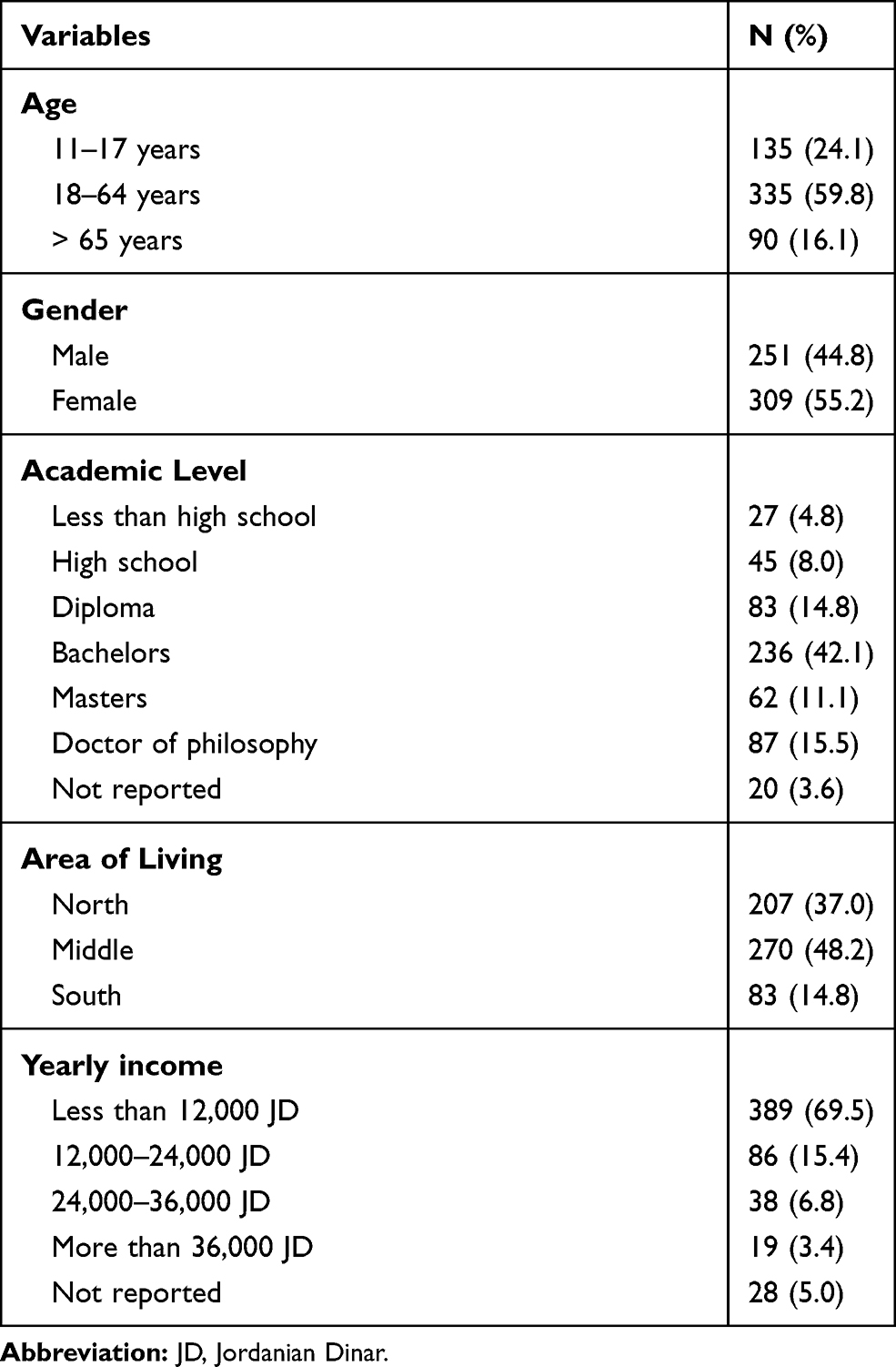 |
Table 1 Characteristics of Participants (N = 560) |
Internal Consistency
To identify whether the alpha coefficient for the Arabic version was different from the alpha coefficient for the English version, the internal consistency was calculated for each quadrant of the AASP for the Arabic and English versions separately for the total sample, collapsed across gender and age. Given that most bilingual subjects were Jordan natives and Arabic was their first language, it was anticipated that the alpha value would be higher than in the English version, or similar in value. The alpha values for the Arabic and English version for the low registration quadrant were 0.79 and 0.81, sensory sensitivity quadrant = 0.72 and 0.79, sensation seeking quadrant = 0.76 and 0.78, and for the sensory avoiding quadrant = 0.70 and 0.69, respectively. The alpha value for the total score was 0.74 and 0.77 for the Arabic and the English versions, respectively.
Table 2 summarizes Cronbach’s alpha coefficients for the quadrants by age groups. The coefficients ranged from 0.62 to 0.85. The highest coefficients were among the elderly age group for all quadrants and ranged from 0.72 to 0.85. The lowest score being for “sensation avoiding” among the 18–64 years old group and the highest coefficients was being for “low registration” among the elderly age group.
 |
Table 2 Internal Consistency of Each Quadrant According to Age Groups |
Cut-off Scores for Arabic Version
Table 3 provides the cut-off scores of each quadrant in the various age groups. Quadrant cut-off scores for the four quadrants for the adolescent group (11–17 years) are summarized for 135 normal participants in Table 3. For the low registration quadrant, individuals with scores of 15–18 have a moderate reduction in noticing and detection behaviors, whereas, adolescents with scores of 55–75 have a moderate increase in noticing and detection behaviors compared with others in the same age category. Similarly, for the sensation seeking quadrant, adolescents with scores of 15–34 have a moderate reduction in seeking additional stimuli behaviors, while adolescents with scores of 70–75 have a moderate increase in seeking additional stimuli when compared with others in the adolescent age category. For the sensory sensitivity quadrant, adolescents with scores of 15–23 have a moderate reduction in responding rapidly to sensory stimuli, and adolescents with scores of 61–75 have a moderate increase in responding rapidly to sensory stimuli. For the sensation avoiding quadrant, adolescents with scores of 15–25 have a moderate reduction in avoiding sensory stimuli, and adolescents with scores of 62–75 have a moderate increase in avoiding sensory stimuli when compared with others in the adolescent age category.
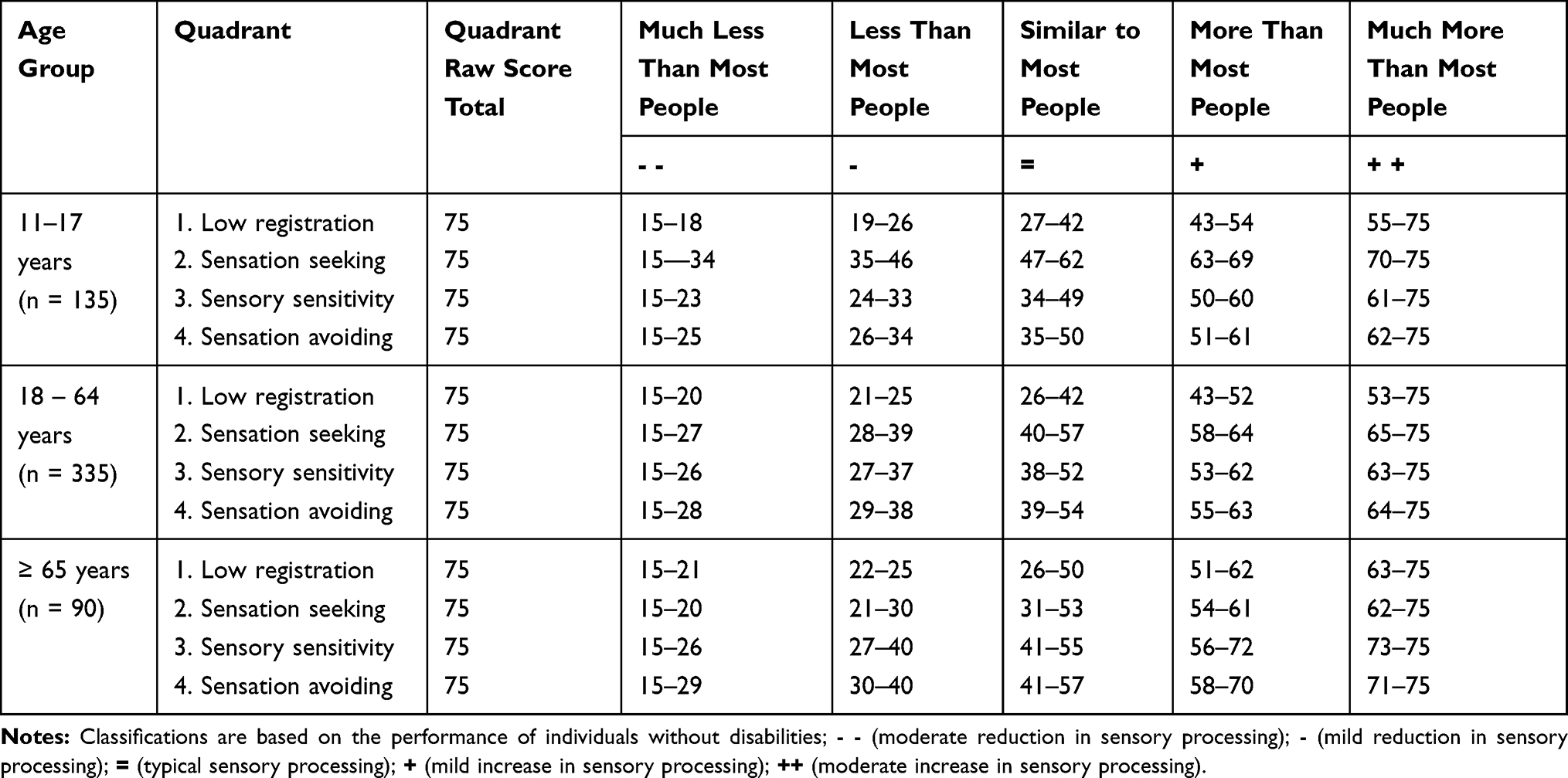 |
Table 3 Cut-off Scores for Each Quadrant in Different Age Groups |
Quadrant cut-off scores for the four quadrants for the adult group (18–64 years) are summarized for 335 normal participants in Table 3. For low registration quadrant, adults with scores of 15–20 have a moderate reduction in noticing and detection behaviors, while adults with scores of 53–75 have a moderate increase in noticing and detection behaviors compared with others in the same age group. For the sensation seeking quadrant, adults with scores of 15–27 showed a moderate reduction in seeking additional stimuli, whereas adults with scores of 65–75 showed a moderate increase in seeking additional stimuli when compared with others in the same age group. For the sensory sensitivity quadrant cut-off scores, adults with scores of 15–26 have a moderate reduction in responding rapidly to sensory stimuli, and adults with scores of 63–75 have a moderate increase in responding rapidly to sensory stimuli when compared with others in the adult age category. For the sensation avoiding quadrant cut-off scores, adults with scores of 15–28 have a moderate reduction in avoiding sensory stimuli, and adults with scores of 64–75 have a moderate increase in avoiding sensory stimuli when compared with others in the same age category.
Quadrant cut-off scores for the four quadrants for the elderly group (≥ 65 years) are summarized for 90 normal participants in Table 3. For low registration quadrant cut-off scores, elderly with scores of 15–21 have a moderate reduction in noticing and detection behaviors, and elderly with scores of 63–75 have a moderate increase in noticing and detection behaviors compared with others in the same age group. For the sensation seeking quadrant cut-off scores, elderly with scores of 15–20 have a moderate reduction in seeking additional stimuli, whereas elderly with scores of 62–75 have a moderate increase in seeking additional stimuli. For the sensory sensitivity quadrant cut-off scores, elderly with scores of 15–26 have a moderate reduction in responding rapidly to sensory stimuli, and elderly with scores of 73–75 have a moderate increase in responding rapidly to sensory stimuli. For the sensation avoiding quadrant cut-off scores, elderly with scores of 15–29 have a moderate reduction in avoiding sensory stimuli, and elderly with scores of 71–75 have a moderate increase in avoiding sensory stimuli.
Gender Effect on Sensory Processing in the Different Age Groups
Table 4 shows the differences between genders in AASP scores for each age group. Generally, females had relatively higher scores in comparison with males in all sensory profile scores among all age groups. Within the adolescent group (11–17 years), girls showed significantly higher scores compared with boys in sensory sensitivity (P = 0.009). Within the adult group (18–64 years), women showed significantly higher scores than men in sensation seeking (P = 0.006) and sensory sensitivity (P = 0.008). Within the elderly group (65 years and above), women had significantly higher scores than men in sensory sensitivity (P = 0.031).
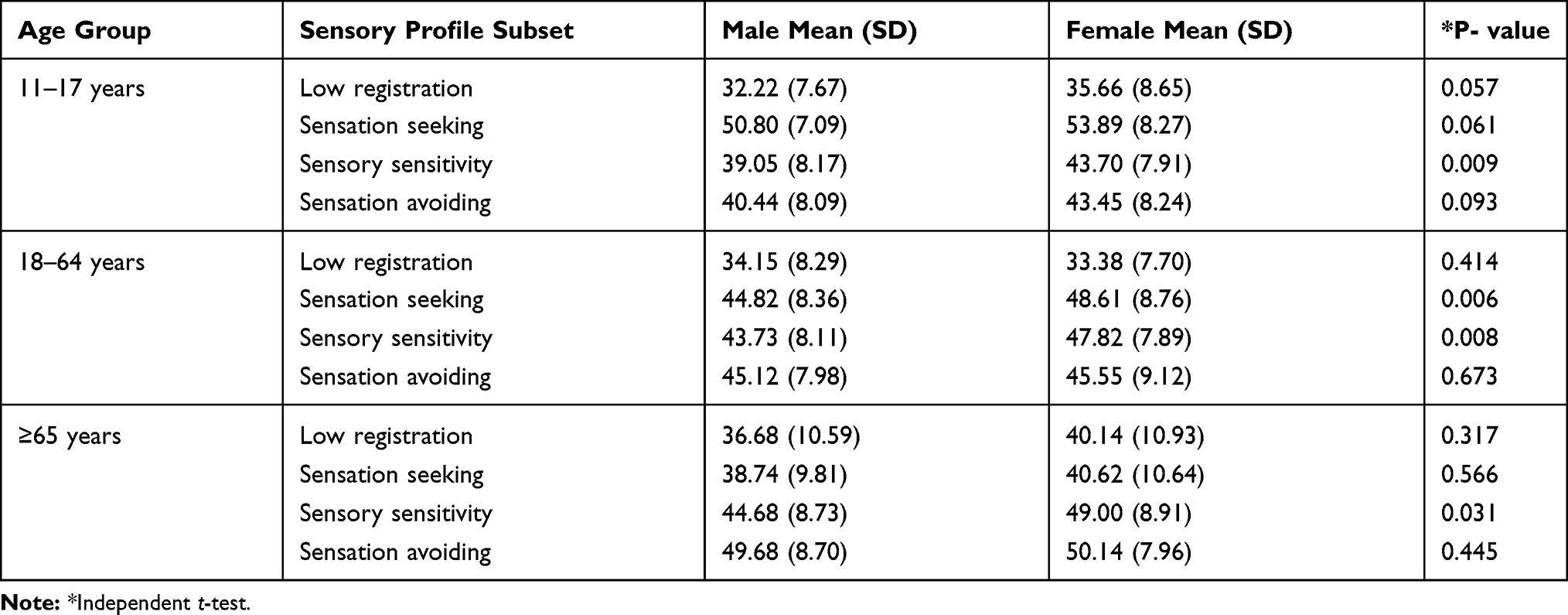 |
Table 4 Difference Between Genders in Adolescents /Adults Sensory Profile Scores, in Each Age Group |
Discussion
The Arabic AASP was found to be a reliable measure that can be used with confidence in Arab countries. The results of the present study indicated that the original English version and the Arabic AASP were comparable. However, there is a difference in the distribution of scores for the Arabic and English versions suggesting that the published English version cut-off scores should not be used for classifying Arabic clients to determine how their scores compare to a standardized sample.
The cut-off scores for the Arabic AASP were calculated so that the cut-off scores of the Arabic respondents could be compared to the cut-off scores of the published English version. In general, it was found that the ranges of the cut-off scores in the Arabic version were larger in the “less than” categories and that the cut-off scores were higher in the “more than” categories. These differences were most pronounced in the sensory sensitivity and sensation avoiding categories. The differences in the Arabic culture, traditions, communities, and religion may contribute to differences in these cut-off scores. For example, spicy food is not common in Arabic culture (item #7) and people prefer to eat traditional meals (item#5). Arabic homes are bigger (because of extended families) and could be more organized (because of non-working mothers) than homes in other societies (item #20), therefore Arabic people tend to keep their homes particularly tidy. Elevators and escalators are not common in Arabic countries and most of the time have a lot of problems, therefore, people avoid them as much as possible. In addition, small stores (item #24) are more common than big malls, parade, and carnivals (item #25) and Arabic cities tend to be quieter and less busy than the Western ones (items #51, 54, 60). Therefore, Arabic people may be more likely to be frustrated or bothered by crowds, noises, and busy places.
Religious factors may also affect the responses of people to different sensory stimuli. For example, people may prefer to keep the shades/curtains down in their homes for privacy issues related to religion (item # 18); women should be covered and should not be exposed to strangers according to Islamic rules. Also, because of religious reasons, it is not acceptable to be close when talking with another person, especially a person of a different gender (items #35, 38, 46). Arabic people often prefer quiet places because they need to pray in a quiet place five times a day (items # 53, 56, 57).
These results and explanations indicate that Arabic speakers living in Arabic communities tend to be more sensory sensitive and sensation avoiding and less sensation seeking than English speakers who live in the US. Therefore, the cut-off scores of the original English version of AASP should not be used when administering the measure to Arabic speaking individuals living in Arabic countries. In such situations, the cut-off scores from this study can provide a more reliable gauge until a larger sample from different countries can be established.
In the present study, adolescent, adult, and older adult males showed less sensory sensitivity compared to females in the comparable age groups. Many previous studies have identified higher sensory sensitivity in females than males. For instance, Engel-Yeger and Dunn (2011) had investigated 290 healthy adults aged 18–50 years, and their results concluded that females reported significantly higher sensory sensitivity scores than males.26 In another study, Engel-Yeger (2012) reported significantly higher scores of sensation seeking, sensory sensitivity, and sensation avoiding in females than males in the age group of 11–17 and 18–64 years, but there was no gender differences noted in the elderly aged 65 years or older.27 In contrast, another study reported a strong association between a low registration pattern and higher trait anxiety for males than females.28 While, other studies also reported increased sensory sensitivity among older females, and they explained this sensitivity due to hormonal changes occurring in older females.7,11,29 Similarly, a few studies have also investigated this issue among children and found that boys are less sensitive compared to girls in the various sensory domains.5,9,22
The present study has several limitations. The unequal number of participants in different age groups (men versus women, age groups) may result in sampling bias. In addition, the present study included only healthy individuals. Therefore, additional studies on clinical populations are warranted in order to strengthen the discriminant validity. Furthermore, the lack of field testing for the translated Arabic version may limit the validity of the results. Future research should use a larger standardization sample from different Arabic communities and cultures to create more representative ranges of the cut-off scores. Moreover, the ability to use a common instrument such as the AASP enables the comparison of the sensory processing patterns of typical individuals as well as individuals with disabilities, hailing from different cultural backgrounds and across different ages.
In conclusion, the internal consistency of the Arabic version of AASP was good and succeeded in profiling the sensory processing abilities of healthy Jordanians. The AASP is a self-administered questionnaire with which occupational therapists interpret the responses into meaningful information pertaining to sensory processing patterns in normal individuals. The applicability of the sensory profile can, therefore, be extended beyond Arabic speaking countries into western communities in normal individuals with Arabic as their first language.
Acknowledgments
The authors are grateful to the Deanship of Scientific Research, King Saud University for funding through Vice Deanship of Scientific Research Chairs.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alotaibi NM, Reed K, Nadar MS. Assessments used in occupational therapy practice: an exploratory study. Occup Ther Health Care. 2009;23:302–318. doi:10.3109/07380570903222583
2. Dunn W. The sensation of everyday life: empirical, theoretical, and pragmatic considerations. Am J Occup Ther. 2001;55:608–620. doi:10.5014/ajot.55.6.608
3. Brown C, Tollefson N, Dunn W, Cromwell R, Filion D. The adult sensory profile: measuring patterns of sensory processing. Am J Occup Ther. 2001;55:75–82. doi:10.5014/ajot.55.1.75
4. Eeles AL, Spittle AJ, Anderson PJ, et al. Assessments of sensory processing in infants: a systematic review. Dev Med Child Neurol. 2013;55:314–326. doi:10.1111/j.1469-8749.2012.04434.x
5. Brown T, Leo M, Austin DW. Discriminant validity of the sensory profile in Australian children with autism spectrum disorder. Phys Occup Ther Pediatr. 2008;28:253–266. doi:10.1080/01942630802224983
6. Dunn W. Sensory Profile: User’s Manual. San Antonio, TX: Psychological Corporation; 1999.
7. Engel-Yeger B, Muzio C, Rinosi G, et al. Extreme sensory processing patterns and their relation with clinical conditions among individuals with major affective disorders. Psychiatry Res. 2016;236:112–118. doi:10.1016/j.psychres.2015.12.022
8. Pfeiffer B, Kinnealey M, Reed C, Herzberg G. Sensory modulation and affective disorders in children and adolescents with asperger’s disorder. Am J Occup Ther. 2005;59:335–345. doi:10.5014/ajot.59.3.335
9. Abu-Dahab SM, Malkawi SH, Nadar MS, Al Momani F, Holm MB. The validity and reliability of the Arabic infant/toddler sensory profile. Phys Occup Ther Pediatr. 2014;34:300–312. doi:10.3109/01942638.2013.823474
10. Kinnealey M, Koenig KP, Smith S. Relationships between sensory modulation and social supports and health-related quality of life. Am J Occup Ther. 2011;65:320–327. doi:10.5014/ajot.2011.001370
11. Chung JC. Measuring sensory processing patterns of older Chinese people: psychometric validation of the adult sensory profile. Aging Ment Health. 2006;10:648–655. doi:10.1080/13607860600648080
12. Butcher JN. Translation and adaptation of the MMPI-2 for international use. In: Butcher JN, editor. International Adaptations of MMPI-2: Research and Clinical Applications. Minneapolis: University of Minnesota Press; 1996:26–43.
13. Hachey R, Jumoorty J, Mercier C. Methodology for validating the translation of test measurements applied to occupational therapy. Occup Ther Int. 1995;2:190–203. doi:10.1002/oti.v2.3
14. Ben-Porath YS, Almagor M, Hoffman-Chemi A, Tellegen A. A cross-cultural study of personality with the multidimensional personality questionnaire. J Cross Cult Psychol. 1995;26:360–373. doi:10.1177/0022022195264002
15. Geisinger KF. Cross-cultural normative assessment: translation and adaptation issues influencing the normative interpretation of assessment instruments. Psychol Assess. 1994;6:304–312. doi:10.1037/1040-3590.6.4.304
16. Ortar G. Some principals for adaptation of psychological tests. In: Cronbach LJ, Drenth PJD, editors. Mental Tests and Cultural Adaptation. The Hague, Netherlands: Mouton; 1972:111–120.
17. Al-Rajeh S, Ogunniyi A, Awada A, Daif A, Zaidan R. Preliminary assessment of an Arabic version of the mini-mental state examination. Ann Saudi Med. 1999;19:150–152. doi:10.5144/0256-4947.1999.150
18. Rahman TT, El Gaafary MM. Montreal cognitive assessment Arabic version: reliability and validity prevalence of mild cognitive impairment among elderly attending geriatric clubs in Cairo. Geriatr Gerontol Int. 2009;9:54–61. doi:10.1111/j.1447-0594.2008.00509.x
19. Alotaibi NM, Aljadi SH, Alrowayeh HN. Reliability, validity and responsiveness of the Arabic version of the Disability of Arm, Shoulder and Hand (DASH-Arabic). Disabil Rehabil. 2016;38:2469–2478. doi:10.3109/09638288.2015.1136846
20. Alghadir A, Anwer S, Iqbal ZA, Alsanawi HA. Cross-cultural adaptation, reliability and validity of the Arabic version of the reduced Western ontario and McMaster universities osteoarthritis index in patients with knee osteoarthritis. Disabil Rehabil. 2016;38:689–694. doi:10.3109/09638288.2015.1055380
21. Alsanawi HA, Alghadir A, Anwer S, Roach KE, Alawaji A. Cross-cultural adaptation and psychometric properties of an Arabic version of the shoulder pain and disability index. Int J Rehabil Res. 2015;38:270–275. doi:10.1097/MRR.0000000000000118
22. Dunn W, Westman K. The sensory profile: the performance of a national sample of children without disabilities. Am J Occup Ther. 1997;51:25–34. doi:10.5014/ajot.51.1.25
23. Sperber AD, Devellis RF, Boehlecke B. Cross-cultural translation: methodology and validation. J Cross Cult Psychol. 1994;25:501–524. doi:10.1177/0022022194254006
24. Brislin RW. The wording and translation of research instruments. In: Lonner WJ, Berry JW, editors. Field Methods in Cross-Cultural Research (Cross-Cultural Research and Methodology Series. Vol. 8. Thousand Oaks, CA: Sage; 1986:137–164.
25. Brislin RW. Translation and content analysis of oral and written material. In: Triandis HC, Berry JW, editors. Handbook of Cross-Cultural Psychology: Methodology. Boston: Allyn & Bacon; 1980:389–444.
26. Engel-Yeger B, Dunn W. Relationship between pain catastrophizing level and sensory processing patterns in typical adults. Am J Occup Ther. 2011;65(1):e1–0.
27. Engel-Yeger B. Validating the Adolescent/Adult Sensory Profile and examining its ability to screen sensory processing difficulties among Israeli people. Br J Occup Ther. 2012;75(7):321–9.
28. Engel-Yeger B, Dunn W. The relationship between sensory processing difficulties and anxiety level of healthy adults. British Journal of Occupational Therapy. 2011;74(5):210–6.
29. Guimaraes P, Frisina ST, Mapes F, Tadros SF, Frisina DR, Frisina RD. Progestin negatively affects hearing in aged women. Proc Natl Acad Sci U S A. 2006;103:14246–14249. doi:10.1073/pnas.0606891103
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.