")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Performance Evaluation of Combining with Medical and Old-Age Care in Pension Institutions of China: A Two-Stage Data Envelopment Analysis
Authors Du N, Wu P, Yuan M, Li Z
Received 18 August 2021
Accepted for publication 27 September 2021
Published 8 October 2021 Volume 2021:14 Pages 4211—4222
DOI https://doi.org/10.2147/RMHP.S332880
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Na Du,1 Peng Wu,2 Man Yuan,3 Zhiwu Li4
1Southern District of The Second Hospital of Shandong University, Jinan, People’s Republic of China; 2School of Economics and Management, Fuzhou University, Fuzhou, People’s Republic of China; 3The Third Affiliated Hospital of Soochow University, Changzhou, People’s Republic of China; 4The Institute of Systems Engineering, Macau University of Science and Technology, Macau, People’s Republic of China
Correspondence: Man Yuan Email [email protected]
Purpose: The aim of this paper was to build a performance evaluation index system for the combination of medical and old-age care services in pension institutions of China.
Methods: A two-stage data envelopment analysis (DEA) is used to evaluate the performance of 30 pension institutions in China.
Results: The results show that the two-stage DEA accounted for a relatively high affiance of medical and nursing care services, but resource allocation still needs to be further optimized. Institutions with ineffective DEA need to reduce the five factors of operations, management, fixed assets, technology and services in the input dimension.
Conclusion: In the output dimension, the service evaluation effect and safety management effect need to be improved. The performance of combined old-age care and medical care in old-age institutions can be improved in terms of investment in fixed assets, methods of capital subsidies, supervision and management, as well as standardized operations.
Keywords: medical and old-age care service, performance evaluation, two-stage DEA
Introduction
The elderly population of 65 years and above in China accounts for 10.8% of the total population.1 The proportion of the elderly aged 65 and above has increased for 21 consecutive years. However, the supply for various old-age beds in China is currently tight, with 30 beds for every 1000 elderly people. China’s aging population accounts for about one-fifth of the world’s aging population, and it is the country with the largest aging population and the fastest growth rate in the world. Providing proper health care for the elderly population is the focus of attention from all walks of life. As a new type of old-age care model, the combination of medical and nursing care combines medical services with old-age care services. On the basis of providing traditional old-age care services, it provides professional medical and rehabilitation services for the elderly. Judging from China’s current family development trend and the development trend of the elderly service industry, the combination of medical and nursing is an inevitable trend. Especially, the COVID-19 outbreak has not only caused a major impact on China’s economic and social sectors, but also posed a major challenge to China’s medical and health system. Thus, under the new circumstance, this paper attempts to evaluate index system for the combination of medical care and elderly care services in China. This study can not only provide a basis for China’s overall reasonable allocation and planning of medical resources, but also provide a reference for the high-quality development of regional health services.
There are still many difficulties in the implementation of the combination of medical and nursing. The main reasons are that China’s current social reality of getting old before getting rich and the combination of medical and nursing services lacks an effective performance evaluation mechanism. The most important thing to evaluate the performance of pension services is to determine the evaluation content and formulate scientific evaluation methods. Assessing the efficiency of a medical institution needs to consider the quality and quantity of services it provides rather than the resources it uses. In this multi-dimensional input/output environment, domestic and foreign researchers have used parametric statistics/metrics and non-parametric methods.2,3 Among these methods, Data envelopment analysis (DEA) is particularly popular in assessing the efficiency of health care units and has many applications in China, Europe, and other parts of the world.4–7 Athanassopoulos et al use constant and variable returns to measure technical efficiency and distribution efficiency in 98 Greek hospitals.8 Due to the excessive concentration of human and financial resources in large cities, suburban and rural hospitals are more efficient than large cities. Garcia and Martin find that Spanish hospitals are more efficient, while hospitals located in areas with low population-to-bed ratios are less efficient.9 Amado and Dyson review researches on the assessment of primary health care providers, especially those using non-parametric technical data envelopment analysis.10 Most researches focus on structure and output, without considering the ultimate measure of performance. Kontodimopoulos et al study balancing the efficiency of health services in remote areas of Greece with the fairness of access to services.11 Lindlbauer and Schreyögg compare different specialization measures for hospital specialization and technology use efficiency, including two novel methods based on the number of patients rather than the proportion of patients.12 Mitropoulos et al use two alternative conceptual models to evaluate the efficiency of public hospitals and regress the scores on explanatory variables related to hospital service performance to improve efficiency.13 Dimas et al evaluate the production performance, efficiency and technological changes of 22 Greek public general hospitals.14 Amiri et al combine differential methods and fuzzy preference programming methods for hospital performance evaluation.15 Liao et al propose a worst-best method for hesitant fuzzy language with inconsistent repair to evaluate hospital performance.16 Considering the existence of complex information in the evaluation process of cognitive hospitals, Breyer et al propose a multi-criteria decision method with hesitant fuzzy linguistic information.17 Chowdhury and Zelenyuk use a two-stage method to evaluate hospital performance.18 In the first stage, DEA is used to assess efficiency scores, and then truncated regression estimates are used to test the importance of explanatory variables. Based on the balanced scorecard and analytic hierarchy process, Mohammadi et al design a public hospital performance evaluation model.19 Singh and Prasher propose the integration of fuzzy set theory and SERVQUAL method to measure the service quality of four hospitals in India.20 Motevali and Torabi improve hospital operating performance from the perspective of mixed sustainability and resilience.21
The current domestic and international researches on the performance evaluation of pension services have achieved certain results, but there are still deficiencies. Most of the evaluation research on elderly care services focuses on home-based elderly care services, government-purchased elderly care services, and institutional elderly care services. There is a lack of performance evaluation research on the combination of medical and elderly care services. In addition, most of the researches focus on the construction of the indicator system, and lack of empirical analysis. Therefore, this paper summarizes the current status of the research on the evaluation of integrated care and elderly care services, based on the system theory and the theory of relevant stakeholders, and combined with the use of a two-stage DEA evaluation method to evaluate the performance of integrated care and medical services in China. This study takes the elderly care service agency as an example to conduct an empirical analysis, and proposes ways to improve the combination of medical and nursing care. This research can make up for the deficiencies of existing research, and promote the development of integrated medical and nursing care services.
Methods
Data envelopment analysis (DEA) is a non-parametric frontier analysis method especially suitable for complex systems with multiple inputs and multiple outputs.3,4 It uses mathematical programming models to evaluate the relative effectiveness of decision-making units (DMU). The traditional DEA model regards innovation activities as a black box. In order to deepen the analysis and analysis of the internal structure of the system, Kao establishes a two-stage DEA model with variable scale returns, which is suitable for comparison between enterprises of different sizes and is widely used in efficiency research. Therefore, this paper uses a two-stage DEA model to evaluate the efficiency of the combination of medical care and nursing.
In a two-stage DEA model, there are n decision-making units DMUs. In each DMUj (j=1,2, …,n), the first stage DEA has m input elements xij(i=1, 2, …, m) and d output elements zdj, d=1,2, …,d. At the same time, the output element of the first stage is regarded as the input element of the second stage, namely the intermediate element. The output factors of the second stage are yrj, r=1, 2, …, s. The two-stage model of the combination of medical care and elderly care service model is as follows:

where vi,  ,
,  and
and  are non-negative weight, when
are non-negative weight, when ,
, .
.
The proposed planning model is transformed into a linear programming model.











Descriptive Statistics of Inputs and Outputs
This study divides the operation process of the combination of medical and nursing into two stages. The first stage is the operation effect stage and the second stage is the service evaluation effect stage. The definition of the input and output indicators of the performance evaluation index system of integrated care and elderly care services takes into account the particularity of integrated care and elderly care services. In this paper, the performance level is measured from the two dimensions of effect and efficiency. In the efficiency-oriented medical and nursing performance evaluation, the DEA method is used for evaluation. Therefore, it is necessary to classify the theoretical indicator system for input and output, and integrate the resource input and service output dimensions in the initial theoretical indicator system into the input and output indicators. Essentially, an organization will only produce output if it is operating, so the internal organizational operating dimension is divided into input indicators.
The data of this study are obtained from the 2020 of National Health Commission of the People’s Republic of China (NHC). NHC data are freely available at http://www.nhc.gov.cn/. NHC is a nationally representative longitudinal survey of pension service combining with medical and old-age care in China. After the effective screening and processing of the data, effective data of 30 pension institutions are obtained. The service efficiency and related factors of combining medical and old-age care institutions are analyzed by binary logistic regression analysis, and the difference is statistically significant with P<0.05. Based on the research of references,4,18,20 the input and output indicators selected in this paper are shown in Tables 1 and 2.
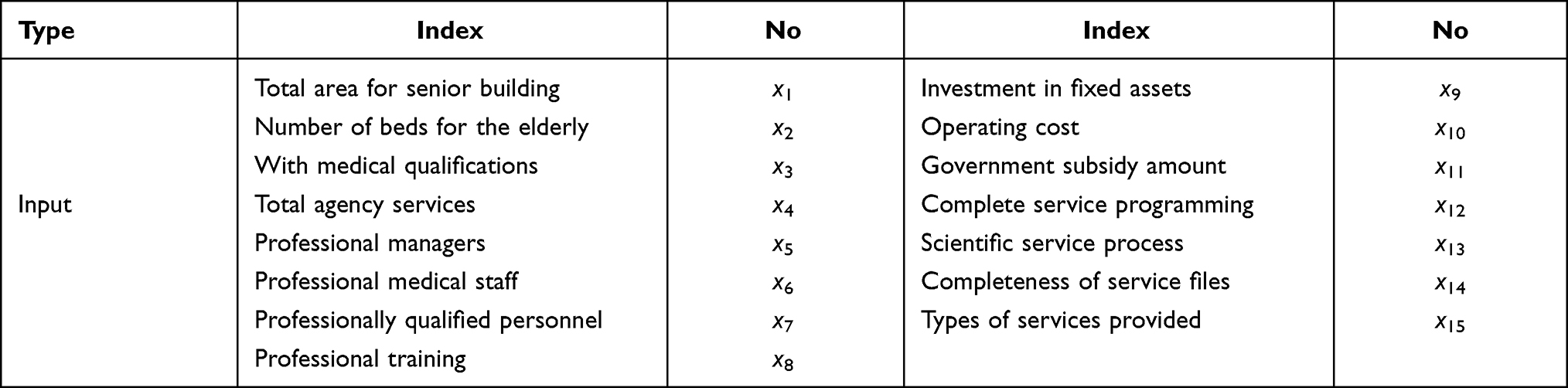 |
Table 1 Index System for Performance Evaluation of Medical and Nursing Care for the Elderly |
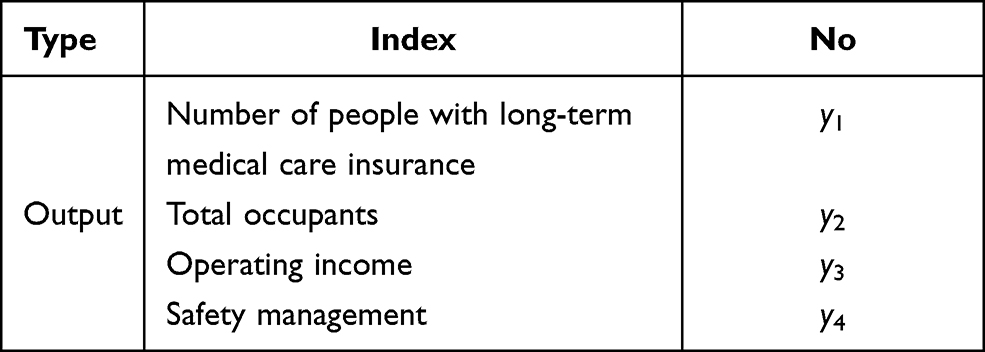 |
Table 2 Indicator System for Performance Evaluation and Output of Integrated Care and Elderly Care Services |
In the evaluation process, it is necessary to eliminate the correlation between the evaluation indicators and reduce the dimensionality. Based on the limited research time and the availability of data, this paper conducts factor analysis on the data of 30 medical and old-age care institutions, and reduces the evaluation index. In this paper, IBM SPSS software is used to reduce the dimensionality of the data. Before factor analysis, the reliability of the data of the survey scale is tested. The internal reliability value indicates whether each scale measures a single concept, that is, how the internal consistency is maintained between the items that make up the scale. If the intrinsic reliability coefficient is above 0.8, it can be considered that the scale has a high intrinsic consistency. The Cronbach coefficient of the data in this paper is 0.885, which proves that the survey scale designed in this paper has a high internal consistency. According to the results of factor analysis, the economic meaning of each public factor is defined, and 19 indicators are re-divided into 7 indicators. Among them, the indicators of the input side are five evaluation indicators: operational investment, management input, fixed asset input, technical input, and service development; the indicators of the output side are the operating effect and service evaluation effect indicators. The performance-oriented evaluation index is determined by two evaluation dimensions: operation effect and service evaluation effect, so as to determine the performance evaluation index system of the combination of medical care and elderly care services. As shown in Table 3.
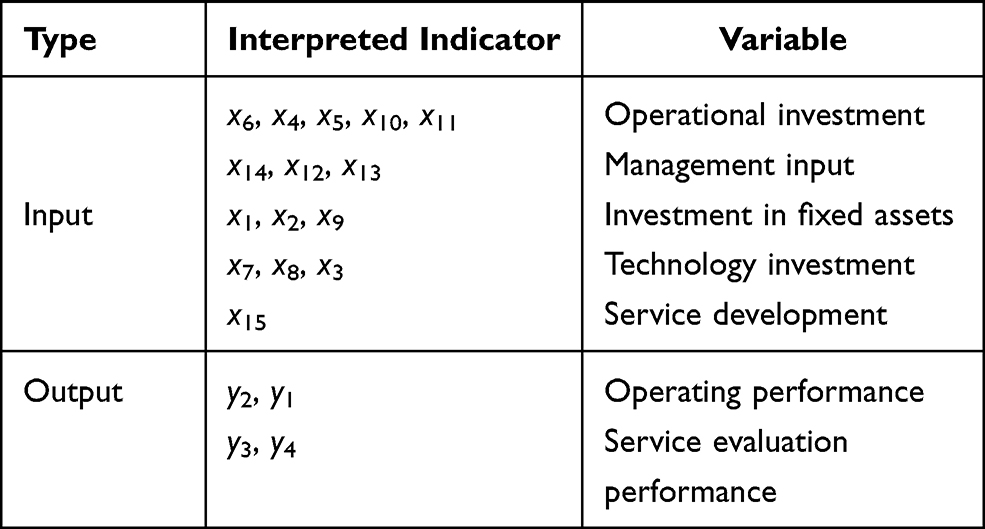 |
Table 3 Index System for Performance Evaluation of the Combination of Medical Care and Elderly Care |
Results and Discussions
This study estimates the changes in the overall efficiency E and staged efficiency indexes E1 and E2 of the combination of medical and nursing care of pension services in Qingdao of China. Using DEA to measure the service efficiency of 30 medical and nursing-type pension service institutions, we can obtain the results of the calculation, which are regarded as the comprehensive performance evaluation results as shown in Table 4 and Figure 1.
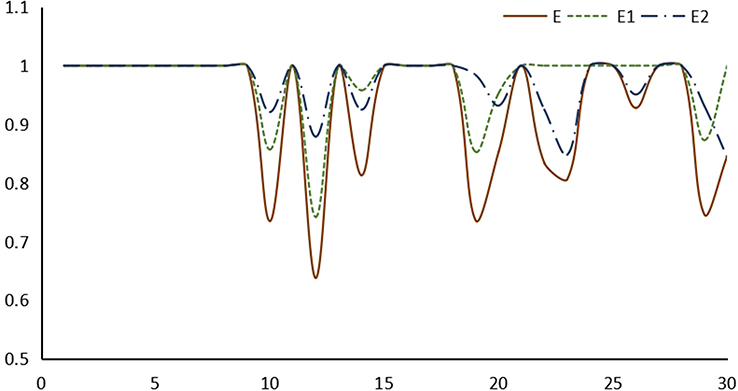 |
Figure 1 Comparison of efficiency between two stages. |
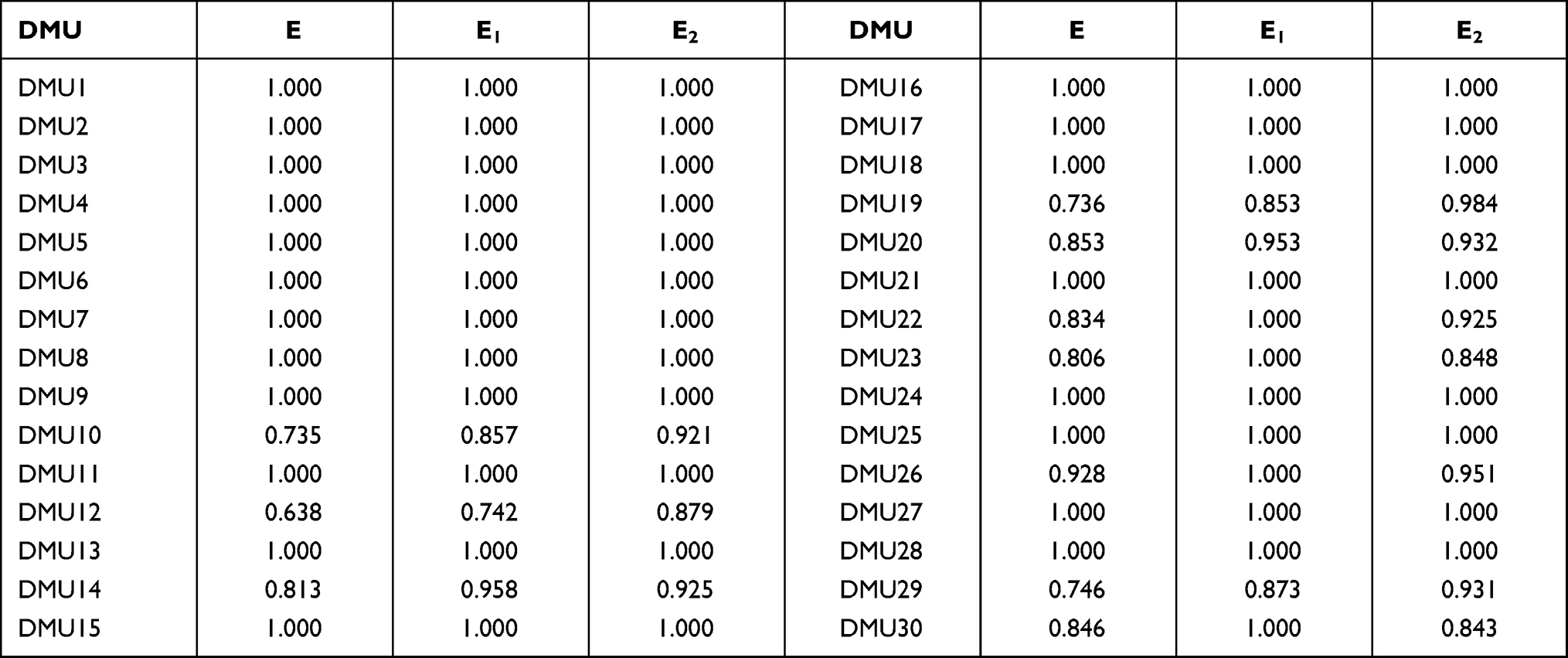 |
Table 4 Comprehensive Performance Evaluation Results of Pension Services |
It can be seen from Table 4 that the comprehensive efficiency value of 20 of the 30 medical and nursing-type pension institutions is 1, which is regarded as effective for DEA. The other 10 are in weak DEA, that is, they have not reached the optimal value in terms of scale efficiency or pure technical efficiency. Among them, the lowest is institution 12, whose comprehensive efficiency is only 0.638. In the case of variable returns to scale, there are 24 companies with a pure technical efficiency value of 1, accounting for 80%. From the perspective of scale efficiency, 20 of them have effective efficiency, and 10 is ineffective efficiency.
This study divides the reasons for the low efficiency of the input and output of the combination of medical care and old-age care services into two types. The first is the low scale efficiency, that is, the supply structure of pension services is unreasonable. The second is the low efficiency of pure technology, that is, the resource utilization rate of pension service institutions is not high, resulting in the input elements not being used most effectively. Therefore, it is necessary to further analyze the reasons for the inefficiency of the 10 DEA ineffective medical and elderly care services.
In these 10 DMUs with ineffective DEA, the pure medical efficiency of DMU22, DMU23, DMU26 and DMU30 is 1, and the scale efficiency value is less than 1, that is, the pure technology is effective but the scale is invalid. This means that the resource utilization technologies of these 4 DMUs match their service capabilities, and there is no problem that the input elements are not maximized. The reason for the inefficiency of its integrated medical and nursing services is that its supply structure is unreasonable and there is a problem of large or small operation scale. The remaining 6 DMU’s pure technical efficiency value and scale efficiency value are not 1, indicating that the service resource utilization technology is not good. There are input factors that are not used effectively and the organization’s service supply structure is unreasonable, and there are also problems of too large or too small an operation scale.
Performance score and ranking analysis is based on the super-efficiency CCR model. As can be seen from the foregoing, although the traditional input-oriented DEA model can measure the efficiency of DMU, it cannot measure all DMUs according to the efficiency value. The reason is that there are 20 DEA effective DMUs in the efficiency measurement results, and their efficiency values are all 1. Although the 10 DMUs can be sorted according to the size of the efficiency value, the efficiency cannot be sorted for the 20 DMUs with an efficiency value of 1. The government usually subsidizes or rewards them according to the ranking of institutions, and the managers of pension institutions pay more attention to the ranking of other pension institutions. In addition, by ranking, managers can learn from the top-ranked organizations to improve their service performance. Therefore, it is necessary to further calculate the super-efficiency CCR model of the input-output indicators in order to obtain rankings and further pick out the benchmarking pension institution.
It can be seen from Table 5 that each DMU has a different super efficiency value, so that the efficiency values of all DMUs can be sorted. Figure 2 is the efficiency ranking of 30 institutions. The top three institutions with super efficiency values are DMU27, DMU6 and DMU21, and their super efficiency values are 3.734, 3.643 and 2.953, respectively. For 10 invalid DMUs, a suitable benchmark learning object can be selected. The first is to choose the most efficient institution. Based on the super-efficiency calculation results, DMU27 ranked No. 1 can be selected as the learning benchmark. DMU27’s comprehensive efficiency, technical efficiency and scale efficiency are all 1, and its super efficiency has reached 3.734. Among the 30 medical and nursing-type pension service institutions, its efficiency is the highest. It is easier for 10 DEA invalid institutions to choose DMU27 with the highest efficiency value to stimulate their own enthusiasm. The second is to choose an institution that is closer. If there is a large gap between the DEA invalid institution and the most efficient DMU27, other DMUs with an overall efficiency value of 1 can be selected as a benchmark according to the similarity or similar principle of the region. These backward institutions can take advantage of geographical advantages to gradually approach the optimal efficiency.
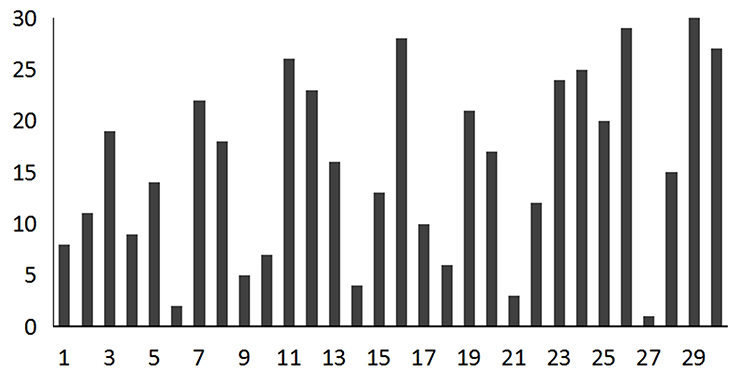 |
Figure 2 Histogram of 30 institutions’ efficiency ranking. |
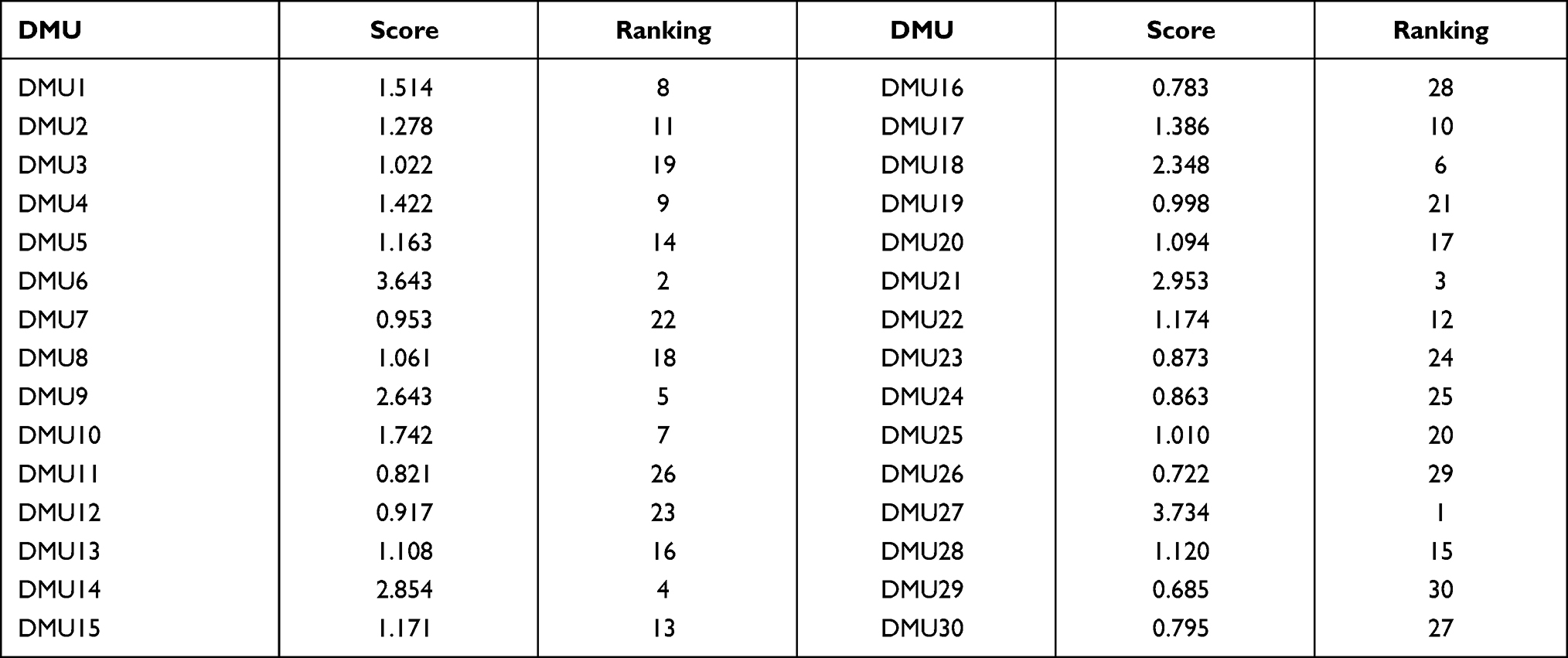 |
Table 5 Performance Score and Ranking Based on the Super-Efficient CCR Model |
If the amount of input is smaller and the amount of output is larger, it means that the utilization of medical care and elderly care services for the elderly care resources is higher and the input-output efficiency is higher. On the contrary, if the output is insufficient and the input is excessive, it means that there is a waste of resources and inefficiency of input and output in the pension institutions. The results of for the projection analysis of the input and output of pension services of 10 DEA invalid institutions are shown in Tables 6 and 7. AV and TV represent the actual value and target value respectively. Operating performance and service evaluation performance are show in Figures 3 and 4. The projection analysis of the DEA method is based on the optimal production frontier analysis of the degree of deviation between the integrated medical and nursing services and the projection point. If DMU is relatively effective to achieve DEA, there is room for adjustment in terms of input and output. If the 10 invalid DMUs are to be effective for DEA, they must increase output and reduce input. The adjustment target can be found based on the projection of the frontier of the benchmark of integrated medical and nursing services. Measure the gap between it and the leading edge of the benchmark to make it an effective DMU. The 20 DMUs effective by DEA have become the benchmark for the integration of medical care and elderly care services. The position of the 10 DMUs with invalid DEA in the multi-dimensional space of input and output deviates from the leading edge of the benchmark of integrated medical and nursing care services. It is very important to guide the research by deviating from the adjustable input-output structure, improving the level of resource allocation, and optimizing the efficiency of combined medical and nursing services.
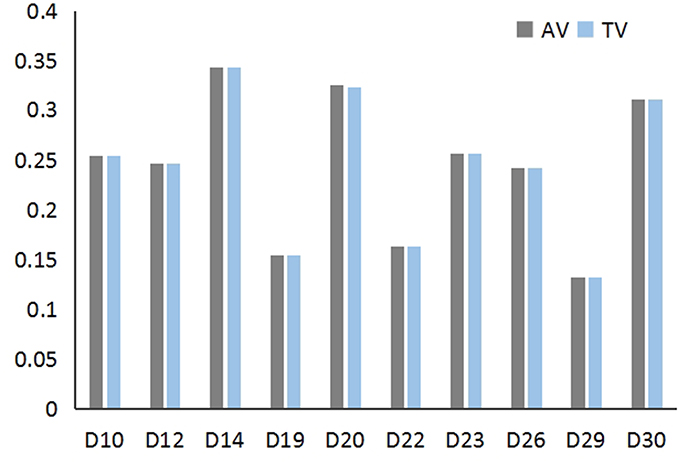 |
Figure 3 Operating performance. |
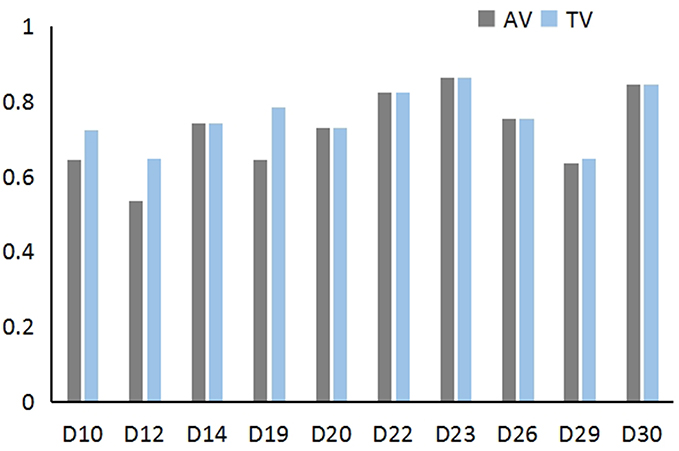 |
Figure 4 Service evaluation performance. |
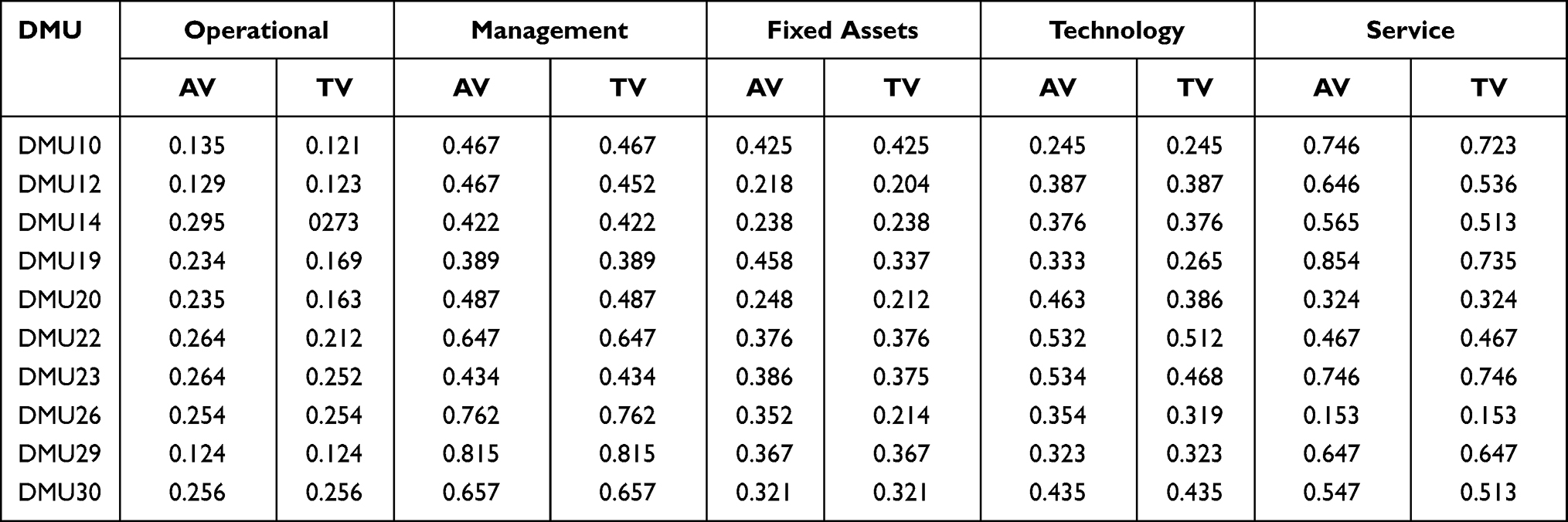 |
Table 6 Results of Impact Analysis of Inputs |
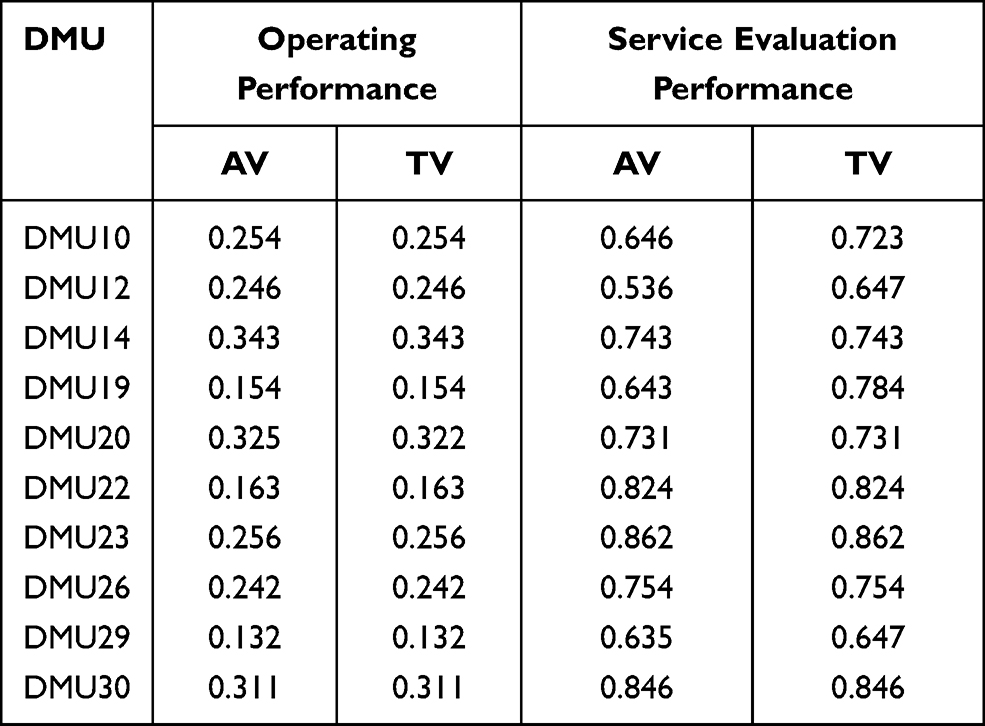 |
Table 7 Post-Projection Analysis Results |
It can be seen from the projection analysis results that ten DEA invalid DMUs can be divided into two categories. The first type is a DMU with a pure technical efficiency of 1. Its input and output have reached the ideal value, and there is no need to improve on input or output factors. It includes DMU22, DMU23, DMU26 and DMU30. If their input and output efficiency reaches DEA, it is only necessary to adjust the service supply structure of the institution and optimize the operation effect. The second category is the DMU with a pure technical efficiency of less than 1. Overall, there is a certain amount of input redundancy in the efficiency of the remaining six DMUs in the combination of medical care and elderly care services, and some DMUs have insufficient output.
Table 8 shows the DMU input and output improvement paths where DEA is invalid. Regarding operational investment, the operational input redundancy rate of DMU10, DMU22, and DMU30 all exceeded 10%. Among them, the highest redundancy rate of DMU30 is 14.38%, and the lowest redundancy rate of operation investment is DMU20 (6.95%). Regarding the investment in management elements, the operational input redundancy rate of DMU12, DMU20, and DMU22 all exceeded 10%, among which the highest is DMU12 (13.54%), and the lowest is DMU14 (8.25%). Regarding fixed asset inputs, those with a redundancy rate of more than 10% are DMU12, DMU20, and DMU30. Among them, the fixed asset investment rate of DMU20 and DMU30 is as high as 20%. The resource allocation level of these institutions is poor, and they only focus on the scale of investment, but not on the improvement of resource utilization technology. It is difficult to achieve comprehensive efficiency effectively. Regarding technology investment, there are still four pension service institutions whose technology investment redundancy rate is higher than 10%. Technical input represents the number of persons who have obtained professional qualification certificates, medical qualifications and training times. The higher redundancy rate in technology investment proves that although the investment in technical elements is relatively high, the best use effect has not been obtained. The investment in high-tech elements has not played a greater role. Regarding service development, the service deployment redundancy rate of DMU12, DMU14, and DMU20 is higher than 10%. Although more service projects have been carried out, they have not brought more output.
 |
Table 8 DEA Invalid DMU Input and Output Improvement Path |
Regarding output, only the service effect evaluation indicators have insufficient output, which is related to two aspects. On the one hand, the projection analysis in this paper is based on the super-efficiency DEA model from the input side, so the analysis is mainly from the input side. On the other hand, it may be related to the actual situation. Business performance is mainly related to the total number of occupants, the number of people receiving long-term medical care insurance, the number of disabled and semi-disabled, and operating income. Three of the four indicators are related to direct numbers. However, the number of elderly people admitted is an uncontrollable output, so pension service agencies cannot increase the output by increasing the number of elderly people admitted. For service evaluation, the main output shortages are DMU10, DMU12, DMU20, and DMU20 is as high as 20.35%. The output of them can be improved by improving the satisfaction of the elderly admitted and the effects of safety management. In summary, for an organization with a pure technical efficiency of less than 1 to achieve DEA effectiveness, it is necessary not only to reasonably adjust the organization’s service supply structure and operating scale, but also to improve its own resource utilization technology.
As mentioned above, we obtained evidence indicating that the efficiency of pension institutions is positively associated with operation, management, fixed assets, technology, and service. This finding is similar to previous studies,3,12,13 and they all found that operation, management, and fixed assets increased the inpatient service utilization. However, this finding is different from the finding of Sultan and Crispim4 who observed that service cannot promote pension institutions efficiency. Moreover, with the acceleration of global aging, pension institutions will continue to increase their demand for service quality, and there is an urgent need to establish a service evaluation and safety management system. This research is not only feasible for Chinese pension institutions, but also has reference value for foreign pension institutions, especially developing countries.
Conclusion
Through the DEA comparison analysis of 30 pension institutions, the following research conclusions can be drawn:
- The efficiency of the combination of medical care and elderly care services is relatively high, but the resource allocation still needs to be further optimized.
- Though the super-efficiency DEA evaluation Organizations are ranked a whole, the benchmark organizations can be established to be further optimized and improved. From the analysis of the projection structure of input and output, we can know that the improvement path can be set from the input and output elements.
- For the projection effect of input and output, the operational performance of each DMU is different, so the improvements of the indicators of each DMU are also different.
- The invalid DEA institutions need to reduce their input from five elements: operational input, management element input, fixed asset input, technical input and service development. The increase in output mainly depends on improving the service evaluation effect.
Based on the research results and the investigation on the combination of medical care and elderly care services, this study proposes the following countermeasures and suggestions.
Regarding the evaluation results, the average value of the fixed asset input redundancy rate is the highest among the input indicators. Fixed assets mainly cover four variables: building area, number of beds, investment amount, and service facility configuration. From the analysis results, it can be seen that the main variables leading to investment redundancy are the building area and the number of beds, which are also consistent with the actual situation. Pension institutions generally have large construction land, but the occupancy rate is less than 50%. At present, the main index for the government to subsidize the construction of pension institutions is the number of beds. The availability of pension land makes the construction area of pension institutions generally larger. The subsidy policy orientation has, to a certain extent, made pension institutions blindly pursue the number of beds. The government can adjust policies appropriately to favor aspects related to the results of operations.
The pension service institutions have poor operating capabilities, and depend on government operating subsidies. However, from the evaluation data, it can be seen that the pension service institutions have redundant operational inputs. In order to increase the utilization rate of operating subsidy funds, the government needs to build a hierarchical classification of capital allocation mechanism. In addition, government subsidies have no obvious impact on service performance. The government fund subsidies should be transformed to play the incentive role. According to the actual operation level, service level, and service efficiency of the medical care and elderly care service organization, the organizations can be divided into different levels. The amount of subsidies should be linked to the assessment level to reduce subsidies for underutilized operating capital resources. In order to encourage institutions with high operating efficiency and high service evaluation, the government may encourage them with appropriate operating funds. This can ensure that the investment of operating capital is maximized, so as to better improve the operating efficiency of the combination of medical care and elderly care services. Relevant departments should be aware of the various financial problems that arise in the process to improve the feasibility and practicality of subsidies.
From the analysis results, it can be seen that the medical care and elderly care service agencies have not made reasonable arrangements for the resources invested. In addition to the problems of the institutions’ own operation and management, they also lack effective government supervision and management. Among the existing management systems in various regions, there is no management system and evaluation standard specifically for pension institutions. As a result, the hardware facilities of the pension institutions and the configuration of service personnel have not reached the required standards. To a certain extent, this also puts the medical care and elderly care service institutions in a state of lack of supervision, which cannot guarantee that they will make reasonable plans and resources allocation during the operation process. In order to ensure the effective operation of medical care and elderly care service institutions, relevant government departments should establish a set of service operation specifications and standards including management, service, facility construction and other indicators as soon as possible. Relevant government departments irregularly supervise and inspect the medical and nursing care service agencies, and rank the evaluation results. Increased operational efficiency and improved service standard will encourage pension institutions to improve facility configuration, improve management and service levels.
According to the super-efficiency analysis ranking, DEA-invalid pension service agencies can choose benchmark companies based on two principles: choose the first-ranked pension service agency or choose an institution with a comprehensive efficiency value greater than 1 according to distance. The government should take the lead in evaluating the medical and nursing care service, and use the best-ranked institutions as industry benchmarks and formulate standards for various indicators in the operation of pension institutions. A perfect standardization system is conducive to the organization’s own standardized operation and improvement of operation quality.
Data Sharing Statement
The datasets used and/or analyzed in this study belong to our research team, and data does not involve any personal privacy information. The datasets are available from the corresponding author on reasonable request.
Ethical Approval
The ethics approval for this research was given by the medical ethics committee of Health Science Center of Shandong University (approval number 2016–375). The ethics committee approved the procedure for the verbal consent, which is allowed for social investigation not involving any biological or medical experiment. We confirmed that this study was conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from all individual participants included in the study. All procedures performed in the study were in accordance with the ethical standards. All methods were carried out in accordance with relevant guidelines and regulations in the manuscript.
Author Contributions
Man Yuan and Na Du contributed to Conceptualization, Methodology; Peng Wu contributed to Investigation, and Project administration; Na Du contributed to Writing- Original draft preparation and Formal analysis; Man Yuan contributed to Software and Validation; Zhiwu Li contributed to Supervision, Reviewing and Editing. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Funding
This work is supported in part by National Natural Science Foundation of China under Grant No. 61703322.
Disclosure
The authors declare no conflict of interests.
References
1. Fragkiadakis G, Doumpos M, Zopounidis C, Germain C. Operational and economic efficiency analysis of public hospitals in Greece. Ann Oper Res. 2014;247(2):787–806. doi:10.1007/s10479-014-1710-7
2. Hollingsworth B. Revolution, evolution, or status quo? Guidelines for efficiency measurement in health care. J Product Anal. 2011;37(1):1–5. doi:10.1007/s11123-011-0221-7
3. Worthington AC. Frontier efficiency measurement in health care: are view of empirical techniques and selected applications. Med Care Res Rev. 2004;61(2):135–170. doi:10.1177/1077558704263796
4. Sultan WIM, Crispim J. Measuring the efficiency of Palestinian public hospitals during 2010–2015: an application of a two-stage DEA method. BMC Health Serv Res. 2018;18(1):381. doi:10.1186/s12913-018-3228-1
5. Chang H, Chang W, Das S, Li S. Healthcare regulation and the operating efficiency of hospitals: evidence from Taiwan. J Account Public Policy. 2004;23(6):483–510. doi:10.1016/j.jaccpubpol.2004.10.004
6. Simoes P, Marques R. Performance and congestion analysis of the Portuguese hospital services. Cent Eur J Oper Res. 2011;19(1):39–63. doi:10.1007/s10100-009-0122-2
7. Sulku SN. The health sector reforms and the efficiency of public hospitals in Turkey: provincial markets. Eur J Public Health. 2012;22(5):634–638. doi:10.1093/eurpub/ckr163
8. Athanassopoulos A, Gounaris C, Sissouras A. A descriptive assessment of the production and cost efficiency of general hospitals of Greece. Health Care Manag Sci. 1999;2(2):97–106. doi:10.1023/A:1019023408924
9. Garcia-Lacalle J, Martin E. Rural vs urban hospital performance in a competitive public health service. Soc Sci Med. 2010;71(6):1131–1140. doi:10.1016/j.socscimed.2010.05.043
10. Amado CAF, Dyson RG. On comparing the performance of primary care providers. Eur J Oper Res. 2008;185(3):915–932. doi:10.1016/j.ejor.2006.02.052
11. Kontodimopoulos N, Nanos P, Niakas D. Balancing efficiency of health services and equity of access in remote areas in Greece. Health Policy (New York). 2006;76(1):49–57. doi:10.1016/j.healthpol.2005.04.006
12. Lindlbauer I, Schreyögg J. The relationship between hospital specialization and hospital efficiency: do different measures of specialization lead to different results? Health Care Manag Sci. 2004;17(4):365–378. doi:10.1007/s10729-014-9275-1
13. Mitropoulos P, Mitropoulos I, Sissouras A. Managing for efficiency in health care: the case of Greek public hospitals. Eur J Health Econ. 2013;14(6):929–938. doi:10.1007/s10198-012-0437-0
14. Dimas G, Goula A, Soulis S. Productive performance and its components in Greek public hospitals. Oper Res. 2012;12(1):15–27. doi:10.1007/s12351-010-0082-2
15. Amiri M, Hashemi TM, Ghahremanloo M, Keshavarz GM, Zavadskas EK, Antucheviciene J. A new fuzzy approach based on BWM and fuzzy preference programming for hospital performance evaluation: a case study. Appl Soft Comput. 2020;92:106279. doi:10.1016/j.asoc.2020.106279.
16. Liao H, Mi X, Yu Q, Luo L. Hospital performance evaluation by a hesitant fuzzy linguistic best worst method with inconsistency repairing. J Clean Prod. 2019;232(1):657–671. doi:10.1016/j.jclepro.2019.05.308
17. Breyer JZ, Giacomazzi J, Kuhmmer R, et al. Hospital quality indicators: a systematic review. Int J Health Care Qual Assur. 2019;32(2):474–487. doi:10.1108/IJHCQA-04-2018-0091
18. Chowdhury H, Zelenyuk V. Performance of hospital services in Ontario: DEA with truncated regression approach. Omega. 2016;63:111–122. doi:10.1016/j.omega.2015.10.007
19. Mohammadi A, Beheshti AR, Kamali K, et al. Introducing the evaluation tools for HSE management system performance using balanced score card model. J Hum Environ Health Promot. 2016;2(1):52–62. doi:10.29252/jhehp.2.1.52
20. Singh A, Prasher A. Measuring healthcare service quality from patients’ perspective: using fuzzy AHP application. Total Qual Manag Bus Excell. 2019;30(3–4):284–300. doi:10.1080/14783363.2017.1302794
21. Motevali HS, Torabi SA. A novel mixed sustainability-resilience framework for evaluating hospital information systems. Int J Med Inform. 2018;118:16–28. doi:10.1016/j.ijmedinf.2018.07.003
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.