")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Perceptions of Non-Communicable Disease and War Injury Management in the Palestinian Health System: A Qualitative Study of Healthcare Providers Perspectives
Authors Mosleh M, Aljeesh Y, Dalal K , Eriksson C, Carlerby H , Viitasara E
Received 10 March 2020
Accepted for publication 10 June 2020
Published 9 July 2020 Volume 2020:13 Pages 593—605
DOI https://doi.org/10.2147/JMDH.S253080
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Marwan Mosleh, 1, 2 Yousef Aljeesh, 3 Koustuv Dalal, 1, 4 Charli Eriksson, 5 Heidi Carlerby, 1 Eija Viitasara 1
1Department of Health Sciences (HLV), Public Health Science, Mid Sweden University, Sundsvall, Sweden; 2Ministry of Health, Gaza, Palestine; 3International Public Health Medicine, Islamic University, Gaza, Palestine; 4Department of Epidemiology, Biostatistics, and EBM; Faculty of Medicine and Health Care, Al-Farabi Kazakh National University, Almaty, Kazakhstan; 5Department of Public Health, Stockholm University, Stockholm, Sweden
Correspondence: Marwan Mosleh Tel +970599859122
Email [email protected]
Background: Palestine, like other low-income countries, is confronting an increasing epidemic of non-communicable disease (NCD) and trend of war injury. The management of health problems often presents a critical challenge to the Palestinian health system (PHS). Understanding the perceptions of healthcare providers is essential in exploring the gaps in the health system to develop an effective healthcare intervention. Unfortunately, health research on management of NCD and war injury has largely been neglected and received little attention. Therefore, the study aimed to explore the perspectives of healthcare providers regarding NCD and war injury management in the PHS in the Gaza Strip.
Methods: A qualitative study approach was used, based on four focus group discussions (FGDs) involving a purposive sampling strategy of 30 healthcare providers from three main public hospitals in Gaza Strip. A semi-structured topic guide was used, and the focus group interviews data were analyzed using manifest content analysis. The study was approved by the Palestinian Health Research Council (PHRC) for ethics approval.
Results: From the healthcare providers perspective, four main themes and several sub-themes have emerged from the descriptive manifest content analysis: functioning of healthcare system; system-related challenges; patients-related challenges; strategies and actions to navigating the challenges and improving care. Informants frequently discussed that despite some positive aspects in the system, fundamental changes and significant improvements are needed. Some expressed serious concerns that the healthcare system needs complete rebuilding to facilitate the management of NCD and war-related injury. They perceived important barriers to effective management of NCD and war injury such as poor hospital infrastructure and logistics, shortage of micro and sub-specialities and essential resources. Participants also expressed a dilemma and troubles in communication and interactions, especially during emergencies or crises. The informants stressed the unused of updated clinical management guidelines. There was a consensus regarding poor shared-care/task sharing, partnership, and cooperation among healthcare facilities.
Conclusion: Our findings suggest that fundamental changes and significant reforms are needed in the health system to make healthcare services more effective, timely, and efficient. The study disclosed the non-use of clinical guidelines as well as suboptimal sectorial task-sharing among different stakeholders and healthcare providers. A clear and comprehensive healthcare policy considering the gaps in the system must be adopted for the improvement and development of care in the PHS.
Keywords: NCD, management, Palestinian health system, perception, war injury
Introduction
NCD has emerged as a significant health problem around the world and is responsible for the main burden of morbidity, mortality, and disability in low–middle and high-income countries (LMHICs).1–3 It constitutes a great challenge to the global healthcare sector as evidenced by the prediction that, by 2020, NCD will represent 73% of all mortalities and nearly 60% of the overall burden of disease globally.4–7 The increasing burden of NCD affects the productivity and continuity of healthcare services in all countries.8 Despite this burden, their prevention and control are still neglected and are not given enough attention in health policy and planning in many developing countries nowadays.3 The management of NCD will be one of the most significant health challenges of the twenty-first century.9
Most cases of NCD could be better prevented or managed.10 The essential goal of NCD prevention and management is to prohibit disease occurrence, minimize the burden of epidemics, delay the incidence of disability, and optimize the quality of health and duration of life.11 In many low and middle-income countries (LMICs), healthcare systems are mainly constructed to manage acute illness and short-term management. Such systems primarily target acute care and need to be reformed to deal more effectively and efficiently with the growing burden of NCD.3
War-related injury is a substantial challenge to clinical medicine and public health globally.12,13 It accounts for most deaths currently experienced in countries affected by conflicts.14 War injury-related conditions also account for many of the healthcare needs and expenditures among those demanding attention in the immediate aftermath of such events. Appropriate health management of these injuries is a key element to improving survival and reducing subsequent functional impairment and disability.15 Current concepts in the management of war injuries have evolved over experiences acquired during numerous wars fought all over the world.16 It is important to take into consideration the whole management of the injured condition rather than the wounds in isolation. This is the key element to achieving optimum management and a successful outcome.17
In Palestine, healthcare for patients with chronic conditions and war injured survivors is problematic and poses a substantial challenge for the PHS, especially during and after the emergency circumstances.18 Besides, the progression of complications in war injured survivors following the initial management of war injury and discharge from hospitals is also of concern to the PHS.19 Care for the large numbers of war injured survivors remains a priority for the health system in this region.20 It was reported that, in 2013, NCD resulted in more than 50% of mortalities in Gaza Strip, where the health system suffers from extreme chronic resource shortage and the population has experienced long-lasting conflicts, resulting in a high economic and social burden on the healthcare sector, from chronic conditions. Managing the risk factors for NCD demands an effective health policy and multi-sectoral efforts and support. Unfortunately, such interventions in the Gaza Strip are still lacking. Policies to address lifestyle behaviors have not yet been advanced. The significant challenges to NCD management in Gaza Strip include unreliable provision of necessary medicines, particularly in the Ministry of Health (MOH) facilities. People may seek care from healthcare providers according to the availability of required treatment and medicines. These multiple challenges are a key concept of effective management for NCD disease.21
In spite of these challenges, the MOH, with the ongoing assistance of the United Nations as well as the international community, especially, the World Health Organization (WHO), has successfully managed the situation and prevented a PHS collapse.22 The WHO continues to support the PHS to enhance and strengthen care for people in the country.23
It is a fact that war and its impact cause extreme stress on targeted populations due to insecurity, instability, and direct reflection of the conflict on population and livelihoods. Disease patterns are not constant and vary over time, therefore, the need for healthcare increases rapidly.24
In Palestine, sufficient data are unavailable on the quantity and scope of NCDs and war injuries, and health research on the management of NCD and war injury has been largely neglected and received little attention.
Understanding the perceptions of healthcare providers is essential in exploring the gaps in the health system to develop an effective healthcare intervention and case management. Therefore, this study aims at exploring the perceptions of healthcare providers regarding NCD and war injury management in the PHS. Findings from this study are expected to provide essential and useful information to healthcare providers and policy makers to develop an appropriate and effective intervention for at least two million people in Gaza Strip and Palestine in general. Lessons learned from Palestine can be shared with other LMICs facing similar constraints and fragmentation in healthcare services to manage NCD and war injury.
Methods
Study Design
A qualitative research method was used at the main public health facilities in the Gaza strip, considering the diversity of specialities and geographical distribution, to provide a better understanding of the perceptions of healthcare providers of NCD and war injury management in the PHS. Qualitative methods are widely used in research and are best viewed as guidelines rather than instruments.25,26 By this research method, the previous experiences and practices of healthcare providers were considered, and generation of information and knowledge was interactive and collaborative.2,27
Study Population
A total of 30 participants in total (14 key physicians/surgeons and 16 head nurses), aged 38–55 were involved in the four FGDs in the targeted settings. Sex, age, location, and work experience were considered to ensure their representativeness in the study. The majority of participants were male. Each group of physicians/surgeons comprised seven participants (14 in total), whereas, each group of head nurses comprised eight participants (16 in total). The participants were purposely chosen, using a diversity of specialities and locations, to collect data that would better describe the topic about management issues in the public hospitals in Gaza Strip. Morgan recommends four to six focus groups as a common number for data collection in a qualitative study.28
Our sampling strategy was to invite participants who had enough knowledge and experience of NCD and war injury management. Therefore, we defined the target groups of healthcare providers that we intended to interview. The list of participants was recommended and recruited from their workplace/hospital’s administration which includes three main public hospitals (Al Shifa hospital, Nasser hospital, and Gaza European hospital).
The inclusion criteria were key physicians/surgeons and head nurses aged 38–55 years, who had work experience for at least 15 years at medical and surgical wards and were eager and willing to participate in the study. The four FGDs were distributed as follows: two focus groups addressed NCDs and war-injury management issues among key physicians/surgeons, whereas the other two focus groups addressed NCD and war-injury management issues among head nurses.
Data Collection
Data were gathered by the principal investigator and two assistant trained staff, using a semi-structured topic guide (Supplementary Appendix A1), and supported probes developed by the authors based on earliest literature, chronic care model (CCM),29 and after several discussions among authors. The study was conducted between September–December 2018.
To ensure the trustworthiness of a qualitative topic guide, the best method is a group review of the questions by a panel of experts from the same research field to minimize the complexity and clarity of the questions and to arrange questions according to their importance as: introductory questions, key questions, sensitive and stressful questions, etc.26 After developing the questions as a group based on themes we would like to study, we further refined the questions, and these were then critically reviewed and checked by the research experts’ team. Questions were then pre-tested with a small sample of individuals similar to those who would be investigated, and finally revised once more before they were performed. Each group of physicians/surgeons and head nurses was held separately in a calm, comfortable, and convenient environment in the targeted health facilities as preferred by the participants. The sessions were managed and led by the principal investigator. Each session was recorded in audio-tape format and supported with handwritten notes. Each session lasted between 1.5 and 2 hours. Participants were warmly welcomed and introduced to each other, a brief description of study purposes was given, and, after an introduction, a simple question on NCD and war injury issues was posed for physicians/surgeons and head nurses separately. All interviews were performed in the respective language (Arabic) and then translated to English language by expert fluent speakers. Quality was assured by two experts by further checking the translation. The topic guide included a series of open-ended questions on the aspects and issues of NCDs and war injuries management, with some themes further explored by subsequent questions.
Data Analysis
All FGD interviews data were transcribed verbatim, translated, and analyzed using manifest content analysis.30 The analysis process for the content of data emerged from interview sessions was performed at the manifest level to address the research questions and contribute to a better understanding of the topic.30,31 This method of analysis is widely used for summarizing and describing the content of data, as the elements are physically present and countable. Most importantly, it is more flexible for interpretation as well as a very useful guide for performing this kind of data analysis. One of the most basic things when using this kind of analysis is the ability to decide the unit of analysis.25,30,31
In our study, the unit of analysis was a focus group interviews texts about conceptions of NCD and war injury management. The initial step of data analysis was to frequently read and re-read the data generated from FGDs through several times to become familiar with the entire data as well as to gain a sense of the whole before proceeding to the next step. Our important interest was to gain a general understanding of what healthcare providers are talking about, their perspectives regarding NCDs and war injuries management. At this point, we obtained key points and ideas of what the informants were expressing. We further began dividing up the data texts into smaller sections or parts, namely, meaning units. We then condensed and abstracted the meaning units. While doing that, we were very careful about keeping the core meaning units without losing the essence of meaning. We then further labeled condensed meaning units by generating codes and sorting them in terms of similarities and differences.
Ethical Issues
This study complies with the regulations and principles of Helsinki Declaration Ethics. The study was approved by Palestinian Health Research Council for Ethics Approval (Ref: PHRC/HC/234/17). Permission and approval were also given by the Ministry of Health to conduct the study at different health facilities. Verbal and written informed consent were also obtained from the participants and approved by the Palestinian Health Research Council for Ethics Approval in Gaza. Before conducting the study, the purposes of the study were explained to all participants and they were informed that they had the right to refuse participation or withdrawal from the survey without any reasons. The anonymity and privacy were secured for all participants, no personal data were included.
Results
The qualitative manifest content analysis resulted in four themes/categories composed from the voices of the physicians/surgeons and head nurses. These will be described in Table 1 and the results will be substantiated by quotations from the healthcare professionals.
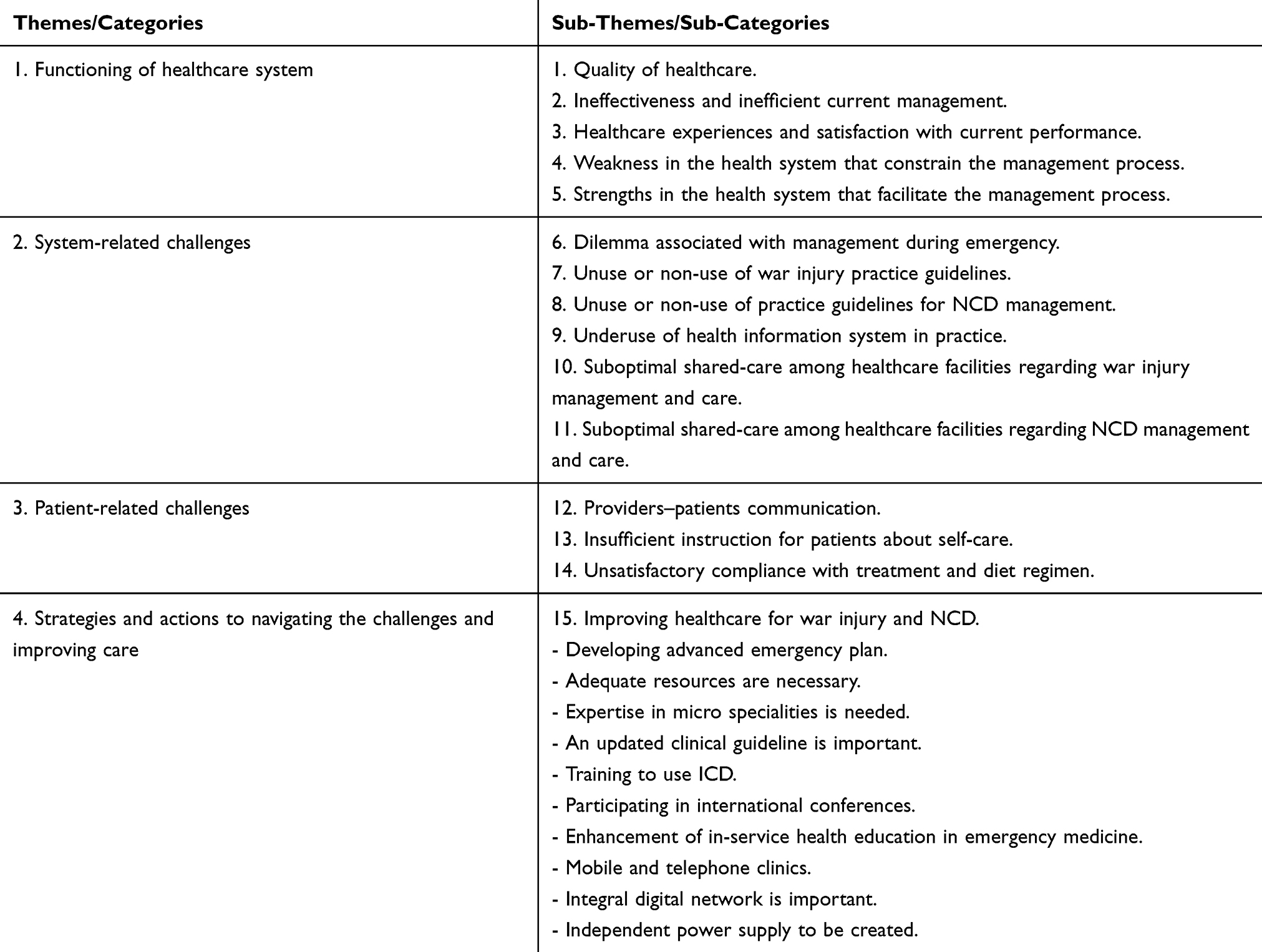 |
Table 1 Main Themes/Categories and Sub-Themes Extracted from Healthcare Providers FGDs |
Theme 1: Functioning of Healthcare System
Sub-Theme 1: Quality of Healthcare
Informants noted some good things in the healthcare system regarding quality of care for war injury and NCD management, however, fundamental changes are needed to make war injury and NCD management work better and to improve and develop quality of care. Some expressed serious concerns about the functioning of the health system that needs comprehensive reform and rebuilding for better case management.
… the quality of care and management of NCD is not as it should be, and significant/major changes are needed, … (internal specialist)
… the management is good but significant improvement and development are needed… (medical nurse)
… Quality of care, in general, is good but fundamental changes are needed … (surgeon)
… the quality of services is good but more development and improvement are required. (surgical nurse)
Sub-Theme 2: Ineffectiveness of and Inefficient Current Management
Healthcare providers expressed that war injury management is still insufficient, and a more effective, integrated plan and emergency system needs to be developed. Head nurses agreed with surgeons regarding the perception of the current management process, but they said that it is better than before.
For NCDs management, most physicians said that the current management is ineffective and inefficient due to over-volume of scheduled cases, work overload, limited manpower, and lack of medical supplies. They expressed that it is not as they hope, and they cannot achieve the best outcome due to impediments. They ranked effectiveness and quality at 50%.
… it is good but major modifications are needed. We can give it 50% for quality and effectiveness … (internal specialist)
… a more effective and efficient health system and integrated plan are needed, as well as significant changes in the current plan … (surgeon)
… despite the insufficient and ineffectiveness of healthcare, however, it was better than before, the care is generally good but needs to be significantly developed more than previously … (surgical nurse)
Sub-Theme 3: Healthcare Experiences and Satisfaction with Current Performance
There was consensus among healthcare providers regarding satisfaction with most or all of the current performance of war injury management and delivery of healthcare, despite limited resources and several impediments such as lack of health workers.
Most physicians were satisfied with their current performance despite the poor effectiveness and efficiency of current management. On the other hand, nurses were less likely to be satisfied and happy with how NCD is currently managed or configured and sometimes they noted underperformance in management.
… the performance is satisfactory in general, but we cannot achieve the best results due to limited resources and interrupted medical supplies. … (internal specialist)
… generally, the performance is good, however, it needs improvement, and we are satisfied with that performance to some extent, we can grade it as moderate, not so good or bad … (surgeon)
… the performance is good, but scientific and professional approach needed to well prepare them more adequately and to improve their morale and loyalty to their work. We are unsatisfied with current performance as required… (medical nurse)
… the current performance in war-injury management is generally good, we are working as a bee cell for organizing and coordinating work quickly… (surgical nurse)
Sub-Theme 4: Weaknesses in the Health System That Constrain the Management Process
Despite few discrepancies seen among healthcare providers, they perceived several important barriers to effective war injury management such as limited hospitals capacity to accommodate influx numbers of patients (overcrowding of cases), shortage of supplies and expertise staff especially in sub and micro-specialities such as “emergency medicine, neurosurgery, vascular surgery and cervical surgery”, overcrowding of attendants and visitors in emergency and surgical wards, coordination troubles among team members as well as delay or failure to transfer complicated cases abroad.
Nurses also noted a lack of security and safety, poor logistic support, bad political situation, malfunction of some essential devices and medical machines, lack of trained staff in emergency facilities, frequent power outages, low wages, and irregularity as common barriers to effective war injury management and quality of care.
Physicians reported the following barriers to effective NCDs management, shortage of important supplies (such as emergency medicines, materials and laboratory agents for PCR and ABG tests), shortage of teamwork, shortage of funding, frequent outages of power supply, shortage of diagnostic tools (such as bronchoscope, spirometer, artificial ventilators, cardiac monitors), delay of referral due to blockage by Israeli forces, frequent malfunction of cardiac monitors and kidney dialysis machines, shortage of medical sub-specialities such as kidney transplantation specialists, and inconsistency or inaccuracy of medical results due to old equipment.
Nurses also expressed that the most common barriers to effective management of NCDs were the shortage of qualified and well-trained manpower, low wages, long waiting-time, non-compliance of patients to medical instructions and diet regimen, overcrowding of visitors, and lack of safety and security, leaving health workers exposed to aggression from visitors or attendants or both.
… several shortcomings in the system including, shortage of well-trained manpower, shortage of medical machines, medicines, and supplies, shortage of power supply and maintenance, and shortage of specialists… (internal specialist)
… the most important disadvantages, were huge numbers of injured people, limited capacity of hospitals, shortage of specialized and trained doctors, shortage of resources, instruments especially during wartime or invasion … (surgeon)
… indeed, shortage of qualified manpower, shortage of resources, long waiting time, low salaries, and frequent outages of power supply and shortages of fuel were the most important impediments toward achieving good quality of care … (medical nurse)
… we think shortage of resources, medicines and supplies, malfunctions of some essential devices, lack of necessary skills and trained staff were observed the most frequent impediments to quality of care … (surgical nurse)
Sub-Theme 5: Strengths in the Health System That Facilitate the Management Process
Physicians/surgeons noted factors that facilitate management of war injury and NCD: loyalty and love of work, coordination, and cooperation in teamwork, distribution of tasks and duties, availability of some aid/diagnostic machines (eg, CT, MRI, histopathology test), and good relationships and respect among staff.
Nurses thought that the most common facilitators were loyalty and sincerity, cooperation in teamwork, planning and organizing of work, emergency plan and schedule, good provision of resources, and some advocacy and support from administration and community.
… the most common facilitators for NCDs management are cooperation with each other and a good relationship and respect among colleagues. … (medical doctor)
… the most important facilitators are the availability of some important diagnostic machines… (medical physician)
… there are many advantages such as loyalty, sincerity, and staff insistence to do their best to give good work despite low salaries and limited resources, cooperation and some donations from some families and NGOs, there is a community role and loyalty which can make us feel not alone … (medical nurse)
… the common factors facilitating our management is teamwork, as working cooperatively … (surgical nurse)
… there are many facilitators such as loyalty, sincerity, and staff insistence to do their best to give good work as can as possible … (medical nurse)
Theme 2: System-Related Challenges
Sub-Theme 6: Dilemma Associated with Management During Emergency
There was a broad consensus from physicians/surgeons that dealing with war injury in emergency is determined by priority, since the highest consideration is given to the most critical cases. They also said that the medical team remained on call during emergency, emergency plan was available, retired physicians were called, simple cases were evacuated, new departments were opened, and some departments were shifted to surgical wards to accommodate the increasing influx of injured people.
Nurses responded similarly, adding that the teamwork was doubled, and work hours were increased in an emergency, holidays were canceled, and a support team was called.
There was broad agreement between physicians and nurses regarding their perception of NCD during an emergency. Almost all healthcare providers said that the priority and more attention were given to complicated and critical cases, and an emergency plan was followed during an emergency. Furthermore, some departments were transformed to surgical departments, simple cases were rescheduled and evacuated to allow dealing with hot or critical cases.
… during emergency, we try to double the team and work hours, evacuation of simple cases, opening a new departments, and transfer the chronic cases to other department in order to receive injured, for example, one day women surgical department was transformed to men surgical department because majority of injured people were males, medical department was transformed to surgical department … (surgical nurse)
…. all medical teams remain on call in case of emergency. The physicians are divided into 3 groups, one in the emergency room, one in the operating room and a part of them working in the departments, and everyone knows his duty, (…) sometimes retired physicians are called … (surgeon)
… during wartime, the more attention is focused on the most critical cases, and stable cases are postponed or rescheduled … (internal specialist)
… in emergency, the more care is, of course, concentrating on hot cases, taking into consideration critical cases, and chronic cases are postponed according to the degree of seriousness … (medial specialist)
Sub-Theme 7: Unuse or Non-Use of War Injury Practice Guidelines
Most informants said that they did not use any evidence-based guidelines in their practice for war injury. They relied on their perception in management and treatment. Some said that they made individual efforts to use guidelines. Physicians reported that the underlying reasons behind not using any guidelines for war injury management were unavailability of official guidelines, lack of interest, absence of official commitment from MOH, and work overload. Nurses also said that they did not use any guidelines in their practice due to the unavailability of guidelines for war injury management.
… frankly, there are no clinical guidelines used for war-injury management … (surgical nurse)
… unfortunately, such guidelines are unavailable in our work, therefore, we do not use any guideline… (physician)
Sub-Theme 8: Unuse or Non-Use of Practice Guidelines for NCD Management
Again, physicians did not use any guideline for NCDs management in their practice because of the unavailability of specific guidelines, no clear universal policy, absence of unified guidelines, lack of interest, lack of knowledge and awareness, absence of collaboration internationally, lack of participation in international conferences, and fragmentation/division of the health system. Nurses agreed with the physicians on the unavailability of guidelines, lack of adoption of guidelines by MOH, no clear policy to adopt or use guidelines, and absence of supervision.
… there is no specific protocol or guidelines used for disease management, but everybody is using his/her perception in managing cases. In short, there is no clear policy to use a protocol … (internal specialist)
… unfortunately, there is no guideline adopted to be used by nurses … (medical nurse)
… the guideline is not officially available … (internal specialist)
Sub-Theme 9: Underuse of Health Information System in Practice
The healthcare providers explained that the health information system is poorly used for war injury and NCD management; its use is limited to radiological images and available at outpatient clinics for administrative use only (eg, reserving appointments and scheduling). Some said that the system is not integrated and still under construction and development. They believed that the health information system will be an important tool for decision making if it is entirely available and integrated.
… the system is limited to radiological images … (surgeon)
… there is no computerized system available in our unit, it is limited to radiological images. … (internal specialist)
… we don’t have any computerized health system to be used in our ward, it is limited to radiological images … (surgical nurse)
… the system is disabled due to unavailability of computers and network … (medical nurse)
… but if such network is available we think it will be a helpful tool in facilitating and coordinating our … (medical nurse)
Sub-Theme 10: Suboptimal Shared-Care Among Healthcare Facilities Regarding War Injury Management and Care
The physicians/surgeons stressed that there are no clear official policy channels and there is a problem with coordination among public health facilities regarding the management of war injury. They were less likely than nurses to perceive that the cooperation was working well. They believed that a shared-care initiative did not run smoothly and efficiently among public hospitals. They said that the shared-care between hospitals and primary health centers (PHCs) is more likely to be neglected or marginal since there was no contribution of PHCs, especially during emergencies, and no communication during wartime. They stressed that significant reform and modification are needed in the public health facilities to make shared-care and co-operation work well. The shared-care and cooperation with private hospitals rely on referral of some cases when there is no capacity at public hospitals to receive more injured patients or in the case of unavailability of specific diagnostic, treatment, or rehabilitation services.
Nurses explained that the shared-care and cooperation were very bad and unsatisfactory in general between different health facilities, especially between public hospitals and PHCs and seem to be completely neglected. They considered that the shared-care and cooperation between public and private hospitals were sometimes available as a “paid-service” but only during wartime were they free of charge for injured people. The nurses were more likely than physicians to perceive that fee-paying injured people experienced problems and difficulty paying for treatment or out-of-pocket expenses for private hospitals after wartimes.
… the shared-care is poor among different healthcare facilities and needs major modification. Since there is no good coordination or obvious official channel or a clear policy between public and private hospitals, the communication relies on referral only. … (surgeon)
… the shared-care between public and private hospitals relies basically on referral, and the service is completely free during emergency such as war, but after the emergency, the service is fully or partially paid or covered by MOH … (surgeon)
… shared-care between PHCs and hospitals is almost unavailable; it depends only on referral from PHCs to hospitals … (surgical nurse)
… actually, shared care among hospitals are very bad … (surgical nurse)
Sub-Theme 11: Suboptimal Shared-Care Among Healthcare Facilities Regarding NCD Management and Care
Physicians expressed that shared-care and co-operation are poor among public hospitals, but some perceived that the shared-care exists with difficulty. There is a consensus that there is still a gap between PHCs and hospitals for shared-care and co-operation, and the PHCs are not activated as required due to the absence of clear policy. They said that the PHCs mainly rely on referral of critical cases to hospitals for advanced care. Despite the expression of physicians that the private sector is considered as an integral part, it sometimes has some concerns such as nepotism and favoritism.
Nurses also stated that there are concerns regarding shared-care and co-operation among public hospitals, and effective care is lacking due to the absence of a clear policy from authorities. They also stressed the unavailability of shared-care between hospitals and PHCs as well as poor co-operation, coordination and shared-care between public and private hospitals. They felt that the two sectors are separated.
… there is still a gap between PHCs and hospitals … (cardiologist)
… the shared-care and relationship among public hospitals are poor regarding managing chronic disease … (internal specialist)
… cooperation is available but not as required. It exists with difficulties … (internal specialist)
… the shared-care between public hospitals and PHCs depends on referral … (internal specialist)
… we do not see that there is shared-care among health facilities, shared-care depends solely on referral. As well, the shared care between hospitals and PHCs is unavailable; it depends on referral from PHCs to hospitals … (medical nurse)
… there is no good cooperation or shared-care between public and private sectors. We feel that they are two separated sectors and no good coordination exists … (medical nurse)
Theme 3: Patient-Related Challenges
Sub-Theme 12: Providers–Patients Communication
Healthcare providers emphasized the importance of communication between medical staff and patients for good case management and facilitation of care. Healthcare providers expressed the poor or unsatisfactory current communication with injured patients, finding it difficult or being unable to communicate with their patients due to a lack of confidence and trust of patients toward healthcare providers.
There were discrepancies between physicians and nurses regarding communication with chronically ill. Nurses indicated good communication between the healthcare providers and patients with chronic illness, whereas physicians expressed poor communication between healthcare providers and patients. The healthcare providers both physicians and nurses stressed that communication is necessary for a better quality of care and management of patients with NCDs as well as encouragement of the patients to adhere to care plans and instructions.
… a good relationship and communication with patients are very important for good management, but it is poor in our case … (surgeon)
… of course, good communication is very important for improving care, but it is unsatisfactory, not at the required level … (surgical nurse)
… actually, poor communication exists, all or most instructions are neglected by the patients and they do the reverse of instruction … (medical specialist)
… in general, the relationship and communication with patients are good … (medical nurse)
Sub-Theme 13: Insufficient Instruction for Patients About Self-Care
There was a consensus between physicians and nurses that they did not give their patients who had war injuries or NCD written instructions about how to manage their care at home (self-management). Instead, some instructions are given verbally rather than in writing, except for patients who had renal failure, kidney transplantation, or those on renal dialysis. Those patients can be given some written instructions about the treatment plan and diet regime.
… generally, the instructions are given to patients more verbally rather than written… (medical specialist)
… a few written instructions were given for patients with renal failure or CKD about their lifestyles, especially diet regimen, other instructions are given verbally… (medical nurse)
… the written medical instructions are limited to medicine prescription and appointments, other instructions such as psychological advice and self-care are provided orally … (surgeon)
… the instructions for self-management are completely given orally rather than written. No written instructions are given … (surgical nurse)
Sub-Theme 14: Unsatisfactory Compliance with Treatment and Diet Regimen
Most healthcare providers (physicians/surgeons and nurses) were dissatisfied with war injured patients’ compliance with treatment plans and instructions. Physicians/surgeons reported noncompliance with injured people, a lack of trust in the staff and regimen and absence of clear rules obliging them to adhere to treatment plans. Nurses perceived that the underlying reasons behind these issues were economic concerns and lack of awareness on the part of the patients.
Most physicians expressed that the compliance of patients with NCD with diet is zero/null, and some patients did not adhere to treatment plans, whereas nurses said that the patient’s compliance with treatment plan is generally good but regarding diet regimen is poor.
… the communication is very poor it is zero, we are unsatisfied with compliance with treatment due to lack of trust and confidence … (surgeon)
… the patients’ compliance with treatment plans and instructions are insufficient for several reasons, especially economic status; some patients are unable to pay for their treatment … (surgical nurse)
… the patients’ compliance with diet regimen is null, but acceptable with medical instruction in general is sometimes good, although some patients do not adhere to the treatment plan … (internal medical specialist)
… the compliance of patients with treatment plan is generally good but poor regarding diet regimen … (medical nurse)
Theme 4: Strategies and Actions to Navigating the Challenges and Improving Care
Sub-Themes 15: Improving Healthcare for War Injury and NCD
The majority of healthcare providers said that the following approaches and initiatives were either necessary or extremely important for improvement of future war injury management within their practice, including advanced emergency plan; more resources like financial and equipment are needed; crisis or emergency commission; attracting well-qualified and trained staff with great focus on micro-specialities (eg, vascular surgery, neurosurgery, cervical surgery, emergency medicine, ICU specialist, plastic and burn surgery specialist); updated treatment guidelines/protocols; training in using international classification of diseases (ICD) codes; and encouraging professionals to actively participate in conferences and workshops. Nurses added that improving wages and incentives; activation of a punishment and reward policy; an integral plan is extremely important to improve war injury management.
… there is an emergency plan available and adopted to be implemented during top emergencies … (surgeon)
… emergency plan and more resources are needed to be available during emergency … (surgeon)
… to improve care an updated treatment protocol is needed … (surgeons)
… adequate supplies, improving staff wages and incentives can help to improve performance and motivate staff to provide quality care … (surgical nurse)
… we suggest activating the policy of punishment and rewarding, which plays a significant role in the improvement of care and performance … (nurse)
… it is necessary to increase the specialized courses on emergency and disaster as well as courses in ICU, emergency medicine, advanced life support … (surgical nurse)
Most physicians thought that micro-specialities (eg, kidney disease specialist, cardiologist, neurologist, endocrinologist, endoscopy specialist, and emergency medical specialist) are important; sufficient staff are required; equipping hospitals with required resources; developing clear policy for healthcare provision; mobile and telephone clinics are important; attending international conferences; active participation in international journals; enhancing in-service emergency education; comprehensive computerized network and creating of independent power supply unit within hospitals are necessary.
Nurses had a similar view toward the improvement of NCD management, but one said there were no plans available right now for improvement of NCD management due to limited resources.
… a clear policy and treatment protocols should be developed for management of disease, and providing hospitals with technical staff and resources. A standard health policy is significant … (medical specialist)
… we don’t need to open new hospitals as much as we need to equip hospitals with required facilities, resources and specialized staff, especially in micro-surgery and specialities … (internal specialist)
… the care can be improved by separation of services and enhancement of micro and sub-specialities … (medical nurse)
… the management can be improved by attracting qualified staff, establishing a unified computerized network, developing the capabilities of manpower as well as the availability of a unified guideline and a clear policy with mandatory use … (medical nurse)
Discussion
One of the most significant missions of healthcare providers is to achieve an optimum level of quality of care and enhancement of health promotion, disease and injury prevention. Ensuring well-functioning healthcare, adequate resources, supplies, well-trained staff and other facilities are necessary. This study was proposed and initiated in response to the immediate call of the healthcare system and management assessment of war injury and NCD in PHS.
To meet our aim, a qualitative research approach was used in order to develop a comprehensive and better understanding on the perceptions of how healthcare providers manage war injury and NCD in the PHS, as well as to capture the insights of healthcare providers who had long experience working with war injury and NCD management. In this approach the previous experience of the healthcare professionals was respected, and production of knowledge was interactive and collaborative.32 The study used the earlier literature and CCM framework to develop a question guide, as this framework is widely and increasingly known as an effective, efficient and patient-centered conceptual method in the management of people with chronic NCD.29 Then the questions guide was judged, critically reviewed, and revised by 13 public health experts in the field to make the final version that could be easily understood and answered.
Despite the interventions and contributions of many actors in the PHS to improve the overall quality of care and management, the burden of disease is still problematic to the Palestinian emergent health system, making big challenges to the improvement of care and management.6,9,11
In the current study, there is a consensus amongst informants supporting the need for significant and fundamental changes within the PHS to make war injury and NCD work better and to facilitate delivery of care. The study also showed that the quality of care needs improvement and development to make healthcare and management work more effectively and efficiently than it does now, with two participants expressing that the healthcare system needs complete rebuilding and comprehensive reform, meaning that the quality of care is unsatisfactory or poor to some extent. Our study clearly shows that the quality of care regarding war injury and NCD management in the PHS was insufficiently correspondent with the WHO definition of the quality of care, in which the healthcare must be safe, effective, timely, efficient, equitable, and people-centered.33
Our findings are in accordance with other research reported by WHO in Palestinian territory, which indicated that the reported barriers and challenges may greatly affect the effectiveness, efficiency, performance, and quality of care before, during, and after emergency situations, due to the collapse of the health system resulting from long-term blockage, ongoing shortages of medicines, shortage of manpower, inadequacy of medical facilities, damage of health infrastructure, and restrictions on medical referrals abroad.18,20,34–38 Furthermore, other evidence reported by WHO showed that there are important healthcare challenges affecting the quality of care in the PHS.38
The findings are in line with a study of Palestine, which showed no evidence that the quality of care has developed or improved, even though significant achievement was reported in the PHS.39 The findings of this study are also in conformity with the findings drawn from a study about quality of healthcare conducted among healthcare providers in other developing countries such as Bangladesh.40
The results of our study correspond to findings of studies conducted in Australia, Canada, Ireland, Germany, Italy, New Zealand, Sweden, the UK, and the US, in which the findings showed that fundamental changes are needed to make the health system work well. However, the findings disagree with the results of the Irish studies, where the outcomes indicated that only minor changes are needed to make it work better.41,42
The study explored that the evidenced-based clinical guidelines were mostly unused at the public hospitals in the Gaza Strip, due to several reasons, including; unavailability of an updated treatment guidelines, absence of clear policy from MOH, lack of interest and awareness, shortage of staff and time.
This finding agrees with the study of Palestine, which assessed the attitudes of Palestinian healthcare providers regarding the most perceived factors affecting adherence to Clinical Practice Guidelines for Diabetes Mellitus at health facilities of the MOH in the Gaza Strip.43 The study indicated that the guidelines were underused in the public hospitals and warrant further incorporation in the system. This finding is in line with the prior Bangladesh study, which revealed that lack of staff was the main reason for non-use or underuse of clinical treatment protocol/guidelines.40
On the basis of literature, clinical practice guidelines are an important tool to help practitioners’ making medical decisions about appropriate health action for specific clinical situations, intending to improve the quality of care and treatment.40 Similarly, strong communication and good relationships between healthcare providers and patient compliance with the care plan and shared-care among different health facilities are a cornerstone for quality of care and effective management.
Strengths and limitations of the study
The strength of a qualitative research method is providing a complex textual explanation of how people experience and perceive research concern. Qualitative research can also help us to better understand and interpret the complex reality of a given condition.44 In this case, FGDs were effective in eliciting knowledge on the norms, experiences, and perception of a specific group and in exploring and accessing a broad range of views on phenomena of concern to the cultural groups or subgroups targeted. Focus groups can also provide a large quantity of information during a relatively short period.44–46
Another advantage in our study is that we addressed the perspectives and opinions of different key healthcare providers from different specialities (physicians, surgeons, and head nurses) on the management and development of both treatment of war injuries and NCD, which was not addressed previously in health research in Palestine. Accordingly, the diversity of opinions and perspectives will considerably contribute to a deeper and better understanding of how Palestinian healthcare professionals manage war injury and NCD considering the important aspects and elements of management. Using focus groups in this study was an important advantage because the participants found it suitable, interactive, informative, and productive to share their experiences and stories in interactive group discussions. Interestingly, the data was very rich in details and gave important insights into how war injuries and NCDs are managed in PHS. Although the number of informants in each of FGDs was small, the amount of data and the consistency of emerging themes indicated that the volume of participants and group sessions were reasonable.
Transferability was enhanced through using a purposive sampling strategy to select and invite participants from a diversity of specialities and locations,46 as well as the description of the setting, the structure of the health system and disease management service, which could help to apply the findings in other similar public settings. However, the findings of this study may never be generalized to all healthcare sectors in Palestine such as non-governmental or private sector.
The information of the current study also seems reliable given its advantages such as the triangulation and consistency of categories/themes highlighted by FGD informants, using a semi-structured topic guide. This study can also be useful to explore the gap between healthcare providers and patient’s relationship regarding their care, and accordingly they can help the patients in determining disease-related health goals that are clinically acceptable and suitable to the patients.
One of the limitations is that analyzing the qualitative data may represent challenges, needing skills from experienced researchers. Besides, the focus group information was translated into English, which was necessary for the involvement of the non-Arabic speaking researchers as well as for this paper. A qualitative approach can be more complicated and time-consuming than a quantitative method, but it can be a step forward in the understanding of complex matters.
Conclusion
The study has concluded that healthcare providers have many criticisms of the current healthcare system, especially regarding the quality of care in managing NCD and war injury. The study findings explored that significant modification and reform of the current healthcare system are needed to improve healthcare for patients with NCDs and war injured survivors and to make healthcare services more effective, timely, and efficient. The study also pointed to the non-use of clinical practice guidelines as well as suboptimal sectorial task-sharing among different healthcare providers. The study confirmed that multiple important perceived barriers, challenges, and gaps exist for optimal case management that should be considered and handled carefully.
The PHS needs a clearer and more comprehensive health policy plan, based on a strategy for health promotion. Finally, further research is recommended.
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest.
References
1. Lauvergeon S, Burnand B, Peytremann-Bridevaux I. Chronic disease management: a qualitative study investigating the barriers, facilitators and incentives perceived by Swiss healthcare stakeholders. BMC Health Serv Res. 2012;12(1):176. doi:10.1186/1472-6963-12-176
2. Maimela E, Van Geertruyden JP, Alberts M, et al. The perceptions and perspectives of patients and health care providers on chronic diseases management in rural South Africa: a qualitative study. BMC Health Serv Res. 2015;15:143. doi:10.1186/s12913-015-0812-5
3. Ng N Chronic disease risk factors in a transitional country: the case of rural Indonesia. Doctoral dissertation. Umeå: Umea University, Sweden; 2006. New Series No.1017 ISSN 0346-6612 ISBN 91-7264-048-0.
4. Russell GM, Dahrouge S, Hogg W, Geneau R, Muldoon L, Tuna M. Managing chronic disease in Ontario primary care: the impact of organizational factors. Ann Fam Med. 2009;7(4):
5. Mathers CD, Ezzati M, Lopez AD. Measuring the burden of neglected tropical diseases: the global burden of disease framework. PLoS Negl Trop Dis. 2007;1(2):e114. doi:10.1371/journal.pntd.0000114
6. World Health Organization (WHO). Innovative Care for Chronic Conditions: Building Blocks for Action. Geneva: Non-Communicable Diseases and Mental Health. Geneva: World Health Organization; 2002.
7. Joint WHO/FAO Expert Consultation group. Diet, nutrition and the prevention of chronic diseases. 2003. available from: http://www.whoint/mediacentre/news/releases/2003/pr20/en/.
8. Rothman AA, Wagner EH. Chronic illness management: what is the role of primary care? Ann Intern Med. 2003;138(3):
9. Dorland J, McColl MA Emerging approaches to chronic disease management in primary health care. Available from: http://www.mqup.ca/emerging-approaches-to-chronic-disease-management-in-primary-health-care-products-9781553391319.php. Accessed August, 20 2018.
10. Canadian Family Physician. Use of Chronic disease management tools. Available from: http://www.ncbi.nlm.gov/pmc/articles/PMC3237522. Accessed September 5, 2018.
11. Focus Area Profile. Chronic disease prevention and management. wisconsin, 2010. Available from: https://www.dhs.wisconsin.gov/publications/p0/p00816-chronic-disease.pdf.
12. World Health Organization (WHO). Injuries and violence: the facts. WHO; 2014. Available from: https://www.who.int/violence_injury_prevention/media/news/2015/Injury_violence_facts_2014/en/.
13. JICA office in Gaza. War on Gaza and JICA challenge Smiles, Hope, and Love, the war didn’t stop the life. Gaza; 2010. Available from: https://www.jica.go.jp/palestine/english/office/topics/c8h0vm0000cjg1n6-att/100909_01.pdf. (
14. Lafta R, Al-Shatari S, Cherewick M, et al. Injuries, death, and disability associated with 11 years of conflict in Baghdad, Iraq: a randomized household cluster survey. PLoS One. 2015;10(8):e0131834. doi:10.1371/journal.pone.0131834
15. World Health Organization (WHO). Violence and injury prevention. Available from: (http://www.who.int/violence_injury_prevention/other_injury/tsunami/en/.) Accessed August 28, 2018.
16. Europe PubMed Central. Reconstructive challenges in war wounds. Reconstructive challenges in war wounds- The Indian Journal of Plastic Surgery. Available from: http://europepmc.org/articles/PMC3495384.).
17. Taylor C, Jeffery S. Management of military wounds in the modern era. Wounds UK. 2009;5(4):50–58.
18. World Health Organization (WHO). Situation report #11: Conflict escalation in Gaza-Complex Emergency, Occupied Palestinian Territory. Palestine; 2014.
19. World Health Organization (WHO). Situation report #9: Conflict escalation in Gaza-Complex Emergency, Occupied Palestinian Territory. Palestine; 2014.
20. World Health Organization (WHO). Situation report #6: Conflict escalation in Gaza-Complex Emergency, Occupied Palestinian Territory. Palestine; 2014.
21. World Health Organization (WHO). Gaza strip Joint Health Sector Assessment Report. Health Cluster in the Occupied Palestinian Territory.Gaza strip, Palestine. 2014: 23–25.
22. World Health Organization (WHO). Health conditions in the occupied Palestinian territory, including east Jerusalem, and in the occupied Syrian Golan. WHO A69/INF./6; 2016.
23. World Health Organization (WHO). Health conditions in the occupied Palestinian territory, including east Jerusalem, and in the occupied Syrian Golan. WHO A71/27; 2017.
24. Vaktskjold A, Yaghi M, Balawi U, Iversen B, Venter W. The mortality in Gaza in July-September 2014: a retrospective chart-review study. Confl Health. 2016;10:10. doi:10.1186/s13031-016-0077-6
25. Maguire M, Delahunt B. Doing thematic analysis: a practical, step-by-step guide for learning and teaching scholars. AISH-J. 2017;(3, Autumn):3351.
26. Dahlgren L, Emmelin M, Winkvist A. Qualitative Methodology for International Public Health.
27. Jack SM. Utility of qualitative research findings in evidence-based public health practice. Public Health Nurs. 2006;23(3):
28. Morgan DL. Focus Groups as Qualitative Research. Newbury Park: Sage Publications Inc; 1997.
29. Wagner EH. Chronic disease management: what will it take to improve care for chronic illness? Eff Clin Pract. 1998;1(1):
30. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):
31. Bengtsson M. How to plan and perform a qualitative study using content analysis. NursingPlus Open. 2016;2(2):8–14. doi:10.1016/j.npls.2016.01.001
32. Ozkal K, Tekkaya C, Cakiroglu J. A conceptual model of relationships among constructivist learning environment perceptions, epistemological beliefs, and learning approaches. Learn Indiv Differ. 2009;19(7):1–9. doi:10.1016/j.lindif.2008.05.005
33. World Health Organization (WHO). What is quality of care and why is it important. Available from: http://www.who.int/maternal_child_adolescent/topics/quality-of-care/definition/en/. Accessed September 7, 2018.
34. World Health Organization (WHO). Report Situation #7. Conflict Escalation in Gaza- Complex Emergency. Gaza, Palestine: Palestinian National Authority; 2014. Available from http://www.who.int/hac/crises/international/wbgs/sitreps/en/.
35. World Health Organization (WHO). WHO statement - Health services close to collapse in Gaza. Available from: http://www.who.int/hac/crises/international/wbgs/sitreps/en/.
36. Health cluster. Gaza Strip Joint Health Sector Assessment Report: Prepared by the Health Cluster in the Occupied Palestinian Territory. Gaza;2014:23–25
37. Waterston T, Nasser D. Access to healthcare for children in Palestine. BMJ Paediatr Open. 2017;1(1):e000115. doi:10.1136/bmjpo-2017-000115
38. World Health Organization (WHO). Health conditions in the occupied Palestinian territory, including east Jerusalem, and in the occupied Syrian Golan. A69/INF./6.20 May 2016:21–27.
39. Giacaman R, Abdul-Rahim HF, Wick L. Health sector reform in the Occupied Palestinian Territories (OPT): targeting the forest or the trees? Health Policy Plan. 2003;18(1):
40. Islam F, Rahman A, Halim A. Perception of health care providers and patients on quality of care in maternal and neonatal health in fourteen Bangladesh government healthcare facilities: a mixed methods study. BMC Health Serv Res. 2015;15:273. doi:10.1186/s12913-015-0918-9
41. Darker C, Whiston L, Jordan S. A National Survey of Chronic Disease Management by Practice Nurses in Ireland. Ireland; 2015.
42. Darker C, Martin C, O’Dowd T. A National Survey of Chronic Disease Management in Irish General Practice. Ireland; 2011.
43. Radwan M, Akbari Sari A, Rashidian A, Takian A, Abou-Dagga S, Elsous A. Attitudes of Palestinian health-care professionals in gaza to clinical practice guideline for diagnosis and treatment of diabetes mellitus. Front Endocrinol (Lausanne). 2017;8:288. doi:10.3389/fendo.2017.00288
44. Mack N, Woodsong C, MCcQueen KM. Qualitative Research Methods: A Data Collectors Field Guide. Family health international; 2011. Available from https://www.k4health.org/sites/default/files/migrated_toolkit_files/datacollectorguideenrh.pdf.
45. Petty NJ, Thomson OP, Stew G. Ready for a paradigm shift? Part 2: introducing qualitative research methodologies and methods. Man Ther. 2012;17(5):
46. AlKhaldi M, Abed Y, Pfeiffer C, Haj-Yahia S, Alkaiyat A, Tanner M. Assessing policy-makers’, academics’ and experts’ satisfaction with the performance of the Palestinian health research system: a qualitative study. Health Res Policy Syst. 2018;16(1):66. doi:10.1186/s12961-018-0341-x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.