")
Back to Journals » Advances in Medical Education and Practice » Volume 13
Perceptions of Digital Teaching During COVID-19; A National Survey of 359 Internal Medicine Trainees
Authors Sivananthan A , Nicholas V, Kerry G , Harlow C, Saha P, Younan HC, Williams S, David L, Lisk C, Schofield L
Received 28 December 2021
Accepted for publication 13 May 2022
Published 28 June 2022 Volume 2022:13 Pages 641—647
DOI https://doi.org/10.2147/AMEP.S355786
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Arun Sivananthan1,2 *, Victoria Nicholas3 *, Georgina Kerry,4 Christopher Harlow,5 Pratyasha Saha,6 Helen-Cara Younan,7 Stephanie Williams,8 Lewis David,9 Clifford Lisk,10 Louise Schofield11
1Institute of Global Health Innovation, Imperial College London, London, UK; 2Department of Gastroenterology, Imperial College Healthcare NHS Trust, London, UK; 3Department of Medicine, Chelsea and Westminster NHS Foundation Trust, London, UK; 4Department of Gastroenterology, St George’s University Hospital NHS Foundation Trust, London, UK; 5Department of Cardiology, Epsom and St Heliers University Hospital, London, UK; 6Department of Rheumatology, University College London NHS Trust, London, UK; 7Department of Intensive Care Medicine, Imperial College Healthcare NHS Trust, London, UK; 8Department of Acute Medicine, Royal Free NHS Trust, London, UK; 9Department of Endocrinology, Bart’s Health NHS Trust, London, UK; 10Department of Geriatrics, Royal Free NHS Trust, London, UK; 11Department of Palliative Medicine, Royal Free NHS Trust, London, UK
*These authors contributed equally to this work
Correspondence: Arun Sivananthan, Institute of Global Health Innovation Imperial College London, 10th Floor QEQM Building, London, W2 1NY, UK, Tel +44 0203 3126666, Email [email protected]
Introduction: The Covid-19 pandemic brought significant disruption to post-graduate medical education. Lecture-based training days were rapidly converted to webinars. This study aims to assess the perceptions of digital training in internal medical trainees.
Methods: IMTs (internal medicine trainees) nationally were surveyed on their perceptions of digital training, ease of access, engagement, and interactivity via a 10-item questionnaire. A mixed-method approach using qualitative and quantitative questions was used. Likert scales were analysed using a mean result of above 3 to indicate agreement.
Results: 359 trainees responded. Trainees agreed that they preferred digital training to face-to-face teaching (mean 3.68); digital training was more engaging (mean 4.25), easier to access (mean 4.49), and as effective for learning as face-to-face teaching (mean 4.69). The most reported advantages were no travel (89%) and the ability to watch later on (88%). 63% of trainees reported loss of social interaction as a disadvantage.
Discussion: This survey suggests that digital teaching has a potential role in IMT training beyond the pandemic.
Keywords: medical education, digital training, IMT, webinar, post-graduate training
Introduction
The Covid-19 pandemic brought significant disruption to healthcare, including the delivery of post-graduate medical education. Large group face-to-face teaching was no longer feasible given the introduction of social distancing, and there was a sudden shift towards online teaching.1 In recent years, online medical education has become more widespread,2,3 and its benefits have been demonstrated in undergraduate cohorts.1,4 Notably, a systematic review found that online and offline teaching is equivalent in terms of exam results for undergraduates.5
Evidence for the role of online medical education in postgraduates is more limited. A systematic review of the efficacy of online education by George et al concluded that digital education may be equivalent to face-to-face or self-directed learning for practicing doctors in terms of knowledge, skills, attitude and satisfaction.6 A further review by Tudor Car et al concluded that digital education for healthcare professionals on clinical practice guidelines is at least as effective as traditional teaching.7
Since the start of the pandemic, novel methods of teaching medical students have been introduced.8 Online webinars using platforms such as Zoom were shown to have a high level of student satisfaction and engagement.9 A recent cross-sectional national survey of 2721 medical students has investigated perceptions on the role of online teaching during the COVID-19 pandemic.1 They found that, overall, medical students did not find online teaching engaging and did not find it as effective as face-to-face teaching.1 The main advantages identified included saving time on travel (19.82%), providing flexibility (19.52%), learning at own pace (18.63%), comfort (15.84%) and cost saving (14.24%). Barriers to effective online teaching included family distractions (26.76%), internet connection (21.53%), timing (17.31%), anxiety (11.08%) and lack of space (11.03%). Further limitations included lack of motivation, concentration, difficulty asking questions and loss of social interactions. The survey also suggested that learners would like online teaching to be more interactive.
A core component of IMT training is regional lecture-based training days.10 During the COVID-19 pandemic these became digitalised and delivered remotely. In London, they were provided by the London Medical Trainee Network from August 2020 and made available to IMT trainees nationally from May 2021. To date, no study has investigated the views of IMTs on digital teaching. The educational needs and learning styles of postgraduate doctors are likely different to medical students, and studies relevant to the undergraduate medical education may not be generalisable to a postgraduate cohort.11–17
The utility of digital teaching in the IMT curriculum beyond the pandemic is unclear, but now in place has become the de facto approach in most settings. We aimed to investigate the perceptions of IMTs on digital teaching. Increasing our understanding may influence future postgraduate training curricula.
Methods
A 10-item questionnaire was designed by the authors. The questionnaire was tested on a pilot group of postgraduate doctors and revised to ensure reliability and validity. A mixed-methods approach was used with both quantitative and qualitative data points recorded.
Demographics including age, stage of training and geographical region were collected. IMTs were asked about their experience of digital teaching using a Likert scale, with 1 being strongly disagree and 5 being strongly agree. Questions focussed on ease of access, engagement, interactivity, and compared digital teaching with face-to-face teaching. Trainees were asked to select perceived advantages, disadvantages and barriers to digital teaching (Appendix 1).
A link to a web-based survey using the Google FormTM platform was shared nationally with attendees of the London regional IMT teaching via both email and IMT WhatsApp groups. Internal Medicine Trainees that attended the IMT digital training afternoon on the 11 March 2021 or watched the recording were eligible for inclusion.
The survey was open for 4 weeks after which the survey automatically closed. The complete survey was required to be completed before the response was accepted. Repeat participation was filtered out by removal of duplicate email addresses associated with the Google form pre-anonymisation.
Training days were specialty themed afternoons containing three separate one-hour sessions with a 40-minute presentation and a 10-minute interactive question and answer session (for example, a cardiology session would cover the topics pacing, supraventricular tachycardia and heart failure). Each session had at least six live poll multiple-choice questions throughout the presentation.
Consent and Ethical Considerations
Participation was entirely voluntary; the survey included a mandatory selection box for consenting to take part. Participants were informed that all data would be anonymised and would only be used for research purposes.
This survey was registered and approved by Imperial College London and underwent assessment by the audit and information governance team. All data were anonymised. The work followed the ethical principles set out in the Declaration of Helsinki.
Data Analysis
Data was exported to Microsoft Excel which was used to calculate descriptive statistics. For ordinal data, mean and standard deviation were used if data was normally distributed, and mean and interquartile range (IQR) were used if not. A mean score between 3 and 5 denoted agreement with the statement. IQR was determined as a surrogate marker of variance.
A six-phase thematic analysis with an inductive approach was used for the free-text responses as described by Frith and Gleeson.18 VN and GK performed this separately and agreed on any discrepancies with discussion.
Results
Demographics
There was a 67.4% response rate, with 359 responses to the survey out of 533 attendees. Cohort demographics are summarised in Table 1. 63.5% (n = 228) were female, 36.5% (n = 129) were male, and 0.56% (n = 2) were other. The majority of participants were less than 30-years-old (76.3%). 59.3% (n = 213) were IMT1s and 38.2% (n = 137) were IMT2s or CT2s. In addition, there were five respondents who had completed core medical training, three junior clinical fellows and a foundation doctor.
 |
Table 1 Demographics of Participants Outlining Gender, Age, Stage of Training and Deanery (n = 259) |
Perceptions of Digital Teaching – Likert Scales
Trainees agreed overall that they preferred digital training to face-to-face teaching (mean 3.68, IQR 2) (Table 2). Trainees agreed that digital teaching was easy to engage with (mean 4.25, IQR 1) and, when compared with face-to-face teaching, was easier to access (mean 4.49, IQR 1) and was as effective for their learning (mean 4.69, IQR 1). In addition, they agreed that the quality of teaching had improved since the pandemic (mean 4.27, IQR 1). Trainees did agree that they would like digital teaching to be more interactive (mean 3.59, IQR 1).
 |
Table 2 Trainee Perceptions of Digital Teaching Since the Pandemic, Using a Likert Scale from 1 to 5 with 1 = strongly Disagree and 5 = strongly Agree |
The most reported advantages were no travel (89%) and the ability to watch at a later time (88%) (Table 3). The majority of trainees also reported time (72%), cost saving (63%) and learning at their own pace (64%) as advantages.
 |
Table 3 Perceived Advantages to Digital Teaching |
The disadvantage most reported was loss of social interaction (63%) (Table 3). Other issues reported by some trainees were that it was harder to get study leave (41%), that they had difficulty concentrating (35%), and problems with internet connection (29%).
Perceptions of Digital Teaching – Thematic Analysis
A total of 17 text entries were coded. Figure 1 shows the themes and subthemes identified for both advantages and disadvantages to digital teaching. Advantages and disadvantages were grouped into 4 overarching themes: accessibility, environment, digital webinar technology, and social interaction (Appendices 2 and 3).
 |
Figure 1 Themes and subthemes divided into advantages and disadvantages of digital. |
Advantages
Subthemes reported under advantages included ease of access.
More likely to get time off work in lieu at a later date to watch recordings than be able to make a face to face session (as often not enough staff on wards to allow leave).
Also reported was comfort:
“Able to study in my own space.”
Advantages reported of the webinar technology included the ability to pause and re-watch:
“I used to pause the video to think and write important points.”
Disadvantages
The ease of access was also reported to be a potential disadvantage:
There is also now an attitude of ‘oh you can just watch later’ so it is very rare that I get to participate in real time because I can’t get off the wards.
Some reported issues with watching in the work environment:
“We have no physical space at my hospital to participate in online sessions (we have no wifi and no speakers on the desktops).”
A loss of social interaction was highlighted:
“I find online sessions incredibly isolating and miss getting to know my peers at teaching days.”
Discussion
The Covid-19 pandemic resulted in a shift from face-to-face to digital teaching for IMTs. This study assessed the perceptions of trainees to digital teaching. The feedback was overwhelmingly positive with trainees perceiving digital teaching as being engaging and as effective for their learning. This stands in contrast to the national survey of medical students referenced in the introduction.1 Of note, the perceived benefits of digital teaching were much less pronounced among medical students compared with doctors – for example, saving time on travel (19.82% compared to 88.86% in this survey) and cost saving (14.24% compared to 63.23%). This may be due to the reduced flexible study time for doctors in employment and potentially greater distances of travel to work, compared to living on a university campus for instance.
Teaching was reported to have improved in quality. We postulate that delivering a teaching session to a large audience with the session being recorded may introduce higher accountability to the speaker, and thus, more preparatory work may go into the session. The organisational committee for the teaching also supports its speakers in achieving this outcome, by setting learning objectives and proof-reading the presentations.
The main disadvantage to digital teaching was a lack of social engagement with peers (Table 4). It is difficult to ascertain the impact of this on the training experience of IMTs, but it is also an interesting question as to whether this is a reasonable expectation of a training programme. Digital webinar technology does allow for ‘breakout’ rooms which would allow social engagement.12,16 Other barriers noted included issues with internet connection, reported in a slightly higher percentage of trainees compared with medical students (28.97% versus 26.76%), which may reflect poor provision of Wi-Fi in many hospitals.
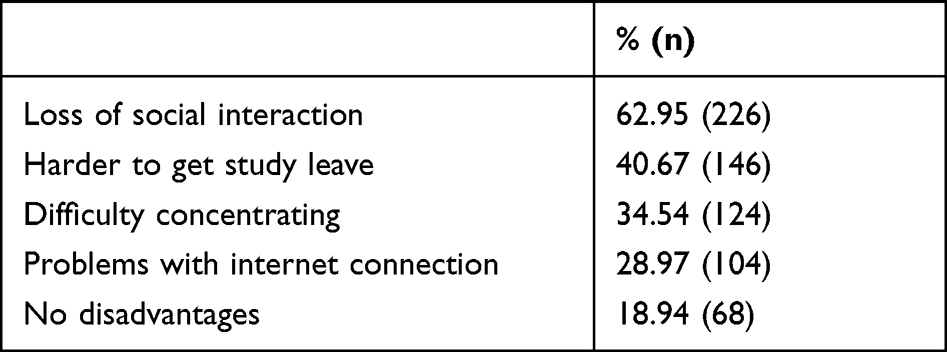 |
Table 4 Perceived Disadvantages and Barriers to Digital Teaching |
Limitations
Limitations of this study include the difficulty of generalising this to IMT trainees' experience of all digital teaching as the majority of their mandatory teaching was supplied by one provider (London Medical Trainee Network). Although the questionnaire asked questions about digital training in general, the responses may be biased to the training sessions provided by the LMTN. However, the signals of preference for digital teaching do suggest that digital teaching has the potential to be preferred by trainees to face-to-face teaching as demonstrated in this cohort.
There is much controversy in the use of parametric tests to analyse Likert scales, but there is good evidence this gives a useful answer in medical education.19
Another limitation of this study is the subjective nature of the questions. It is notoriously difficult to quantify the impact of medical education in terms of both learning and behaviour changes without detailed trials with pre- and post-testing.20 However, we feel in this case that subjective trainee perception is a valuable output when evaluating training with most of these trainees having had at least 8 years of medical education in various forms and therefore are experienced participants.
This study surveyed trainees during the pandemic where face-to-face teaching was not an option. Similar studies looking at medical student teaching have raised the question of the validity of the study outside of the context of a pandemic. In the future, as face to face teaching increases, a survey of the same cohort is important to establish perceptions of face-to-face teaching versus digital outside the context of the pandemic.
Conclusion
This survey suggests that digital teaching has an important potential role in IMT training beyond the pandemic. The main benefit is increased accessibility, with teaching being available from anywhere with high-quality teaching being available to a wide audience, and in a recorded form to those who are on call or too busy to attend. Care must be taken by training programme directors to incorporate digital training whilst protecting study leave and mitigating against potential social isolation.
Data Sharing Statement
AS, VN and GK have access to the data and take responsibility for integrity of the data and analysis.
Consent and Ethical Considerations
Participation was entirely voluntary; the survey included a mandatory selection box for consenting to take part. Participants were informed that all data would be anonymised and would only be used for research purposes. This survey was registered and approved by Imperial College London and underwent assessment by the audit and information governance team. All data was anonymised, and full informed consent was taken from all participants. The work followed the ethical principles set out in the Declaration of Helsinki.
Acknowledgments
Catherine Bryant and Andrew Deaner.
Author Contributions
“All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work”.
Disclosure
Arun Sivananthan and Victoria Nicholas are joint first authors. Clifford Lisk, Louise Schofield are joint senior authors. Dr Clifford Lisk reports personal fees from BMJ live, personal fees from acute general medicine conference, personal fees from healthcare UK conference, outside the submitted work; and Regional training programme director for Stage 1 internal medicine training North Central London; work produced in collaboration with education fellows. At the time of submission all authors declare no relevant competing interests.
References
1. Dost S, Hossain A, Shehab M, Abdelwahed A, Al-Nusair L. Perceptions of medical students towards online teaching during the COVID-19 pandemic: a national cross-sectional survey of 2721 UK medical students. BMJ Open. 2020;10(11):e042378. doi:10.1136/bmjopen-2020-042378
2. O’Doherty D, Dromey M, Lougheed J, Hannigan A, Last J, McGrath D. Barriers and solutions to online learning in medical education – an integrative review. BMC Med Educ. 2018;18(1):130. doi:10.1186/s12909-018-1240-0
3. Moran J, Briscoe G, Peglow S. Current technology in advancing medical education: perspectives for learning and providing care. Acad Psychiatry. 2018;42(6):796–799. doi:10.1007/s40596-018-0946-y
4. Lochner L, Wieser H, Waldboth S, Mischo-Kelling M. Combining traditional anatomy lectures with e-learning activities: how do students perceive their learning experience? Int J Med Educ. 2016;7:69–74. doi:10.5116/ijme.56b5.0369
5. Pei L, Wu H. Does online learning work better than offline learning in undergraduate medical education? A systematic review and meta-analysis. Med Educ Online. 2019;24(1):1666538. doi:10.1080/10872981.2019.1666538
6. George PP, Zhabenko O, Kyaw BM, et al. Online digital education for postregistration training of medical doctors: systematic review by the digital health education collaboration. J Med Internet Res. 2019;21(2):e13269. doi:10.2196/13269
7. Tudor Car L, Soong A, Kyaw BM, Chua KL, Low-Beer N, Majeed A. Health professions digital education on clinical practice guidelines: a systematic review by digital health education collaboration. BMC Med. 2019;17(1):139. doi:10.1186/s12916-019-1370-1
8. Sandhu P, de Wolf M. The impact of COVID-19 on the undergraduate medical curriculum. Med Educ Online. 2020;25(1):1764740. doi:10.1080/10872981.2020.1764740
9. Kay D, Pasarica M. Using technology to increase student (and faculty satisfaction with) engagement in medical education. Adv Physiol Educ. 2019;43(3):408–413. doi:10.1152/advan.00033.2019
10. Joint Royal College of Physicians Training Board. Curriculum for internal medicine stage 1 training; 2019. Available from: https://www.jrcptb.org.uk/internal-medicine.
11. Monaghan AM. Medical teaching and assessment in the era of COVID-19. J Med Educ Curric Dev. 2020;7:2382120520965255. doi:10.1177/2382120520965255
12. Wilcha R-J. Effectiveness of virtual medical teaching during the COVID-19 crisis: systematic review. JMIR Med Educ. 2020;6(2):e20963. doi:10.2196/20963
13. Yusoff MSB, Hadie SNH, Mohamad I, et al. Sustainable medical teaching and learning during the COVID-19 pandemic: surviving the new normal. Malays J Med Sci. 2020;27(3):137–142. doi:10.21315/mjms2020.27.3.14
14. Nik-Ahmad-Zuky NL, Baharuddin KA, Abdul Rahim AF. Online clinical teaching and learning for medical undergraduates during the COVID-19 pandemic: The Universiti Sains Malaysia (USM) experience. Med Educ. 2020;12:75–80. doi:10.21315/eimj2020.12.2.8
15. Singh K, Srivastav S, Bhardwaj A, Dixit A, Misra S. Medical education during the COVID-19 pandemic: a single institution experience. Indian Pediatr. 2020;57(7):678–679. doi:10.1007/s13312-020-1899-2
16. Jiang Z, Wu H, Cheng H, Wang W, Xie AN, Fitzgerald SR. Twelve tips for teaching medical students online under COVID-19. Med Educ Online. 2021;26(1):1854066. doi:10.1080/10872981.2020.1854066
17. Sahi PK, Mishra D, Singh T. Medical education amid the COVID-19 pandemic. Indian Pediatr. 2020;57(7):652–657. doi:10.1007/s13312-020-1894-7
18. Frith H, Gleeson K. Clothing and embodiment: men managing body image and appearance. Psychol Men Masc. 2004;5(1):40–48. doi:10.1037/1524-9220.5.1.40
19. Sullivan GM, Artino AR
20. Artino AR, La Rochelle JS, Dezee KJ, Gehlbach H. Developing questionnaires for educational research: AMEE guide no. 87. Med Teach. 2014;36(6):463–474. doi:10.3109/0142159X.2014.889814
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.