")
Back to Journals » Patient Preference and Adherence » Volume 15
Perception of Stigma in Patients with Neuromyelitis Optica Spectrum Disorder
Authors Meca-Lallana JE, Prefasi D, Pérez-Miralles F , Forero L , Sepúlveda M, Calles C, Martínez-Ginés ML, González-Suárez I , Boyero S , Romero-Pinel L, Sempere ÁP , Meca-Lallana V, Querol L, Costa-Frossard L, de Castro-Trapiello H , Canal N, Maurino J
Received 7 February 2021
Accepted for publication 30 March 2021
Published 12 April 2021 Volume 2021:15 Pages 713—719
DOI https://doi.org/10.2147/PPA.S305707
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Jose E Meca-Lallana,1 Daniel Prefasi,2 Francisco Pérez-Miralles,3 Lucía Forero,4 María Sepúlveda,5 Carmen Calles,6 María L Martínez-Ginés,7 Inés González-Suárez,8 Sabas Boyero,9 Lucía Romero-Pinel,10 Ángel P Sempere,11 Virginia Meca-Lallana,12 Luis Querol,13 Lucienne Costa-Frossard,14 Hugo de Castro-Trapiello,2 Neus Canal,15 Jorge Maurino2
1Clinical Neuroimmunology Unit and Multiple Sclerosis CSUR. Department of Neurology. Hospital Universitario “Virgen de la Arrixaca”, IMIB-Arrixaca, Murcia, Spain; 2Medical Department, Roche Farma, Madrid, Spain; 3Unit of Neuroimmunology, Department of Neurology, Hospital Universitari i Politècnic La Fe, Valencia, Spain; 4Department of Neurology, Hospital Universitario Puerta del Mar, Cádiz, Spain; 5Department of Neurology, Hospital Clínic i Provincial de Barcelona, Barcelona, Spain; 6Department of Neurology, Hospital Universitari Son Espases, Palma de Mallorca, Spain; 7Department of Neurology, Hospital Universitario Gregorio Marañón, Madrid, Spain; 8Department of Neurology, Hospital Universitario Álvaro Cunqueiro, Vigo, Spain; 9Department of Neurology, Hospital Universitario Cruces, Bilbao, Spain; 10Department of Neurology, Hospital Universitari de Bellvitge, Barcelona, Spain; 11Department of Neurology, Hospital General Universitario de Alicante, Alicante, Spain; 12Department of Neurology, Hospital Universitario La Princesa, Madrid, Spain; 13Department of Neurology, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain; 14Department of Neurology, Hospital Universitario Ramón y Cajal, Madrid, Spain; 15Department of Statistics, IQVIA, Barcelona, Spain
Correspondence: Jorge Maurino
Roche Farma, Ribera Del Loira, 50, Madrid, 28042, Spain
Tel +34 913 24 81 00
Email [email protected]
Background: Perception of stigma was associated with low self-esteem, psychological problems, and decreased health-seeking behavior among patients with different neurological disorders. The purpose of this study was to assess stigmatization and its impact in patients with neuromyelitis optica spectrum disorder (NMOSD).
Methods: A non-interventional study was conducted at thirteen neuroimmunology clinics in Spain. Patients with a diagnosis of NMOSD (2015 Wingerchuk criteria) were included. The 8-item Stigma Scale for Chronic Illness (SSCI-8), the Expanded Disability Status Scale (EDSS), the 29-item Multiple Sclerosis Impact Scale (MSIS-29), the Beck Depression Inventory-Fast Screen (BDI-FS), the MOS Pain Effects Scale (MOS-PES) and the Fatigue Impact Scale for Daily Use (D-FIS) were used to assess the perception of stigma, disability, quality of life, mood, pain, and fatigue, respectively. Associations between outcome measures were analyzed using Spearman’s rank correlation.
Results: Seventy-one patients were studied (mean age: 47.4 years ± 14.9, 81.7% female, mean time since disease onset: 9.9 years ± 8.1). The median EDSS score was 3.0 (interquartile range 1.5, 4.5). Stigma prevalence was 61.4% (n=43). Thirty-one patients (43.6%) had depression. The SSCI-8 score showed a significant correlation with both physical (rho=0.576, p< 0.0001) and psychological (rho=0.608, p< 0.0001) MSIS-29 scales scores, EDSS score (rho=0.349, p=0.0033), BDI-FS score (rho= 0.613, p< 0.0001), MOS-PES score (rho= 0.457, p< 0.0001), and D-FIS score (rho=0.556, p< 0.0001).
Conclusion: Stigma is a common phenomenon affecting over 6 out of 10 patients with NMOSD. Understanding stigma may be useful to develop educational strategies improving NMOSD knowledge.
Keywords: neuromyelitis optica spectrum disorder, stigma, quality of life, depression, patient-reported outcomes
Introduction
Neuromyelitis optica is a rare chronic inflammatory central nervous system disease characterized by monophasic or recurrent attacks of optic neuritis and transverse myelitis with poor or no recovery.1–3 The term neuromyelitis optica spectrum disorder (NMOSD) was established by an international panel in 2015 to enable early diagnosis in patients with or without aquaporin-4 antibodies.1 Motor and visual impairment, pain, and fatigue are among the most prevalent and debilitating symptoms.4,5 Residual disability usually limit daily function and independence over time.6,7
The definition of stigma traditionally refers to a feeling of disapproval that society has about something, especially when this is unfair.8 Perception of stigma was a common phenomenon among people with neurological disorders in a survey recently conducted by the European Federation of Neurological Associations.8 The impact of stigma has been documented across a number of neurological conditions contributing to lack of confidence, depression, anxiety, decreased health-seeking behavior, and unequal life opportunities.8–12
There is limited information available on the presence of stigma in patients with neuroinflammatory and demyelinating disorders. Perception of stigma has been recently explored in multiple sclerosis (MS).13–17 Different studies showed a prevalence of perceived stigma of 20 and 80% in patients with relapsing-remitting and primary progressive MS, respectively.16,17 Even in patients with low physical disability, stigma was associated with poor quality of life, depression, and unemployment.15,17,18
Depression and psychological distress affect subjective well-being in patients with NMOSD.19–22 However, no studies have focused on stigma and NMOSD. The purpose of this study was to assess stigmatization and its impact on patients living with NMOSD.
Methods
A non-interventional, cross-sectional study was conducted at thirteen hospital-based neuroimmunology clinics in Spain (PERSPECTIVES-NMO study). Eligibility criteria included being at least 18 years old and having a diagnosis of NMOSD according to Wingerchuk 2015 criteria.23 This study was conducted in accordance with the Good Clinical Practice Guidelines of the International Conference on Harmonisation and with the ethical principles of the Declaration of Helsinki and was approved by the investigational review board of Galicia (CEIm-G), Santiago de Compostela, Spain. Written informed consent was obtained from all participants.
Outcome Measures
The 8-item Stigma Scale for Chronic Illness (SSCI-8), the Expanded Disability Status Scale (EDSS), the 29-item Multiple Sclerosis Impact Scale (MSIS-29), the Beck Depression Inventory-Fast Screen (BDI-FS), the MOS Pain Effects Scale (MOS-PES) and the Fatigue Impact Scale for Daily Use (D-FIS) were used to assess the perception of stigma, disability, quality of life, mood, pain and fatigue, respectively.24–30
The SSCI-8 was developed to assess perceptions of stigma across different neurological conditions.24,25 It comprises eight items rated on a 5-point Likert scale from 1 (never) to 5 (always). Total scores range from 8 to 40, with a cut-off score >8 indicating the presence of stigmatization. The MSIS-29 is a self-report questionnaire used to determine the impact of MS on health-related quality of life.27 It consists of two composite domains including physical (20 items) and psychological impacts (9 items). Items are rated using four-point response categories: not at all, a little, moderately, and extremely. Scores on the physical and psychological impact subscales can range from 20 to 80 and from 9 to 36, respectively. Higher scores indicate greater impact. The BDI-FS is a seven-item questionnaire assessing the level of depressive symptoms.28 Responses to the items are provided on a four-point scale (no symptoms to severe symptoms) with total score ranging from 0 to 21. Cut-off scores ≥4 and ≥9 are used to define the presence of depression and moderate-to-severe depression, respectively. The MOS-PES is a validated, six-item, self-report questionnaire to assess how pain and unpleasant sensations interfere with mood, ability to walk or move, sleep, work, recreation, and enjoyment of life.29 Total score ranges from 6 to 30, with higher scores indicating greater impact of pain. The D-FIS is an eight-item, self-report instrument designed to measure subjective daily experience of fatigue.30 Items are rated using a 5-point Likert scale from 1 (never) to 5 (always). Higher scores indicate greater fatigue perception.
Statistical Analysis
Associations between outcome measures were analyzed using Spearman’s rank correlation. Logistic regression was used to assess the contribution of stigma to symptoms of depression (depressed, not depressed).
Results
A total of 71 patients were included in the study. The mean (± SD) age was 47.4 ± 14.9 years and 81.7% were female. The mean time since disease onset was 9.9 years ± 8.1 and the median EDSS score was 3.0 (interquartile range 1.5, 4.5). Thirty-one patients (43.6%) had depression. Demographic and clinical characteristics of the sample are shown in Table 1.
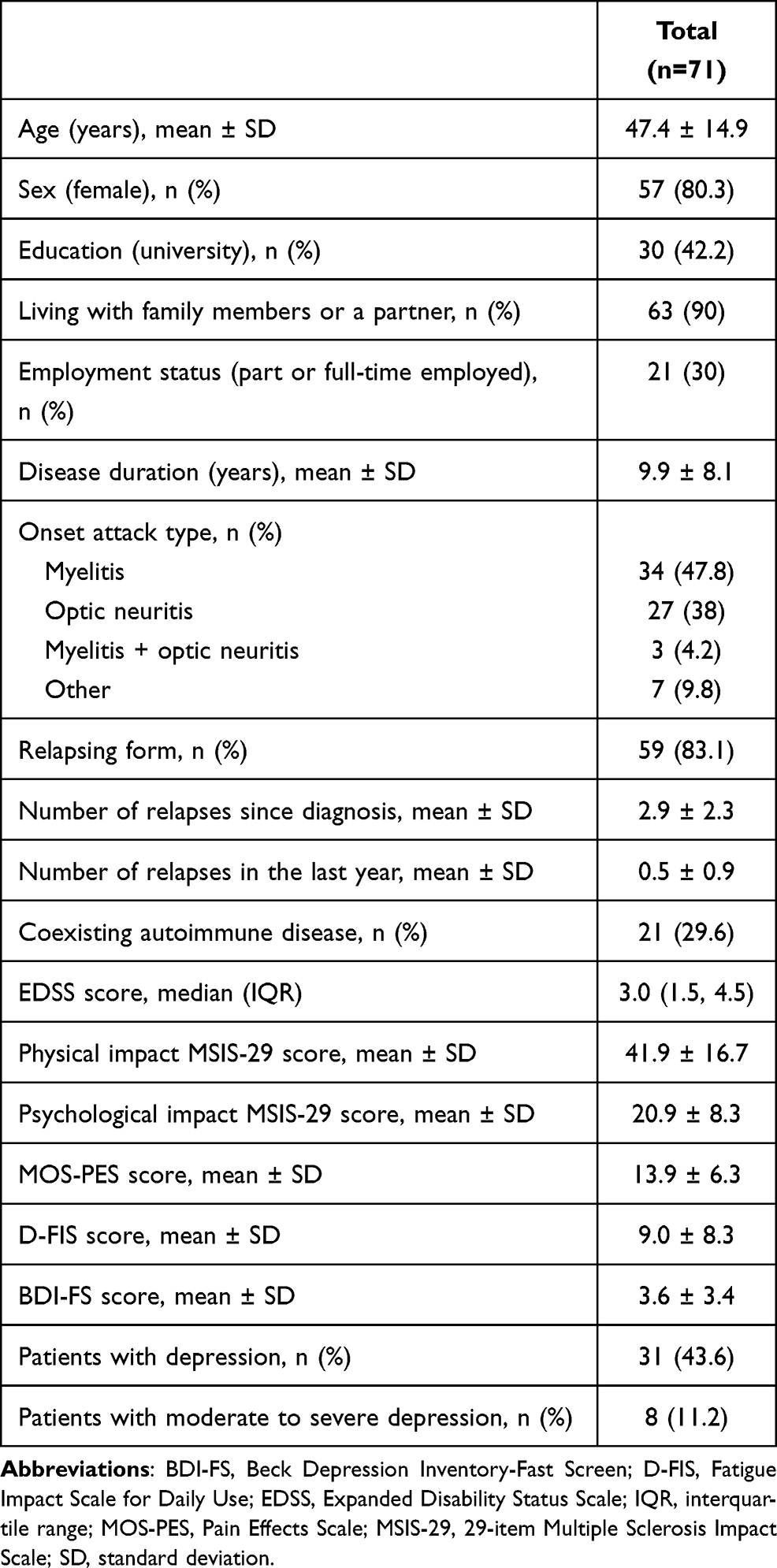 |
Table 1 Demographic and Clinical Characteristics |
The prevalence of stigma was 61.4% (95% CI 46.9, 76.0 [n=43]) (Table 2). Feeling of being left out of things, followed by embarrassment because of physical limitations and people avoided me because of my illness were the items with the highest impact.
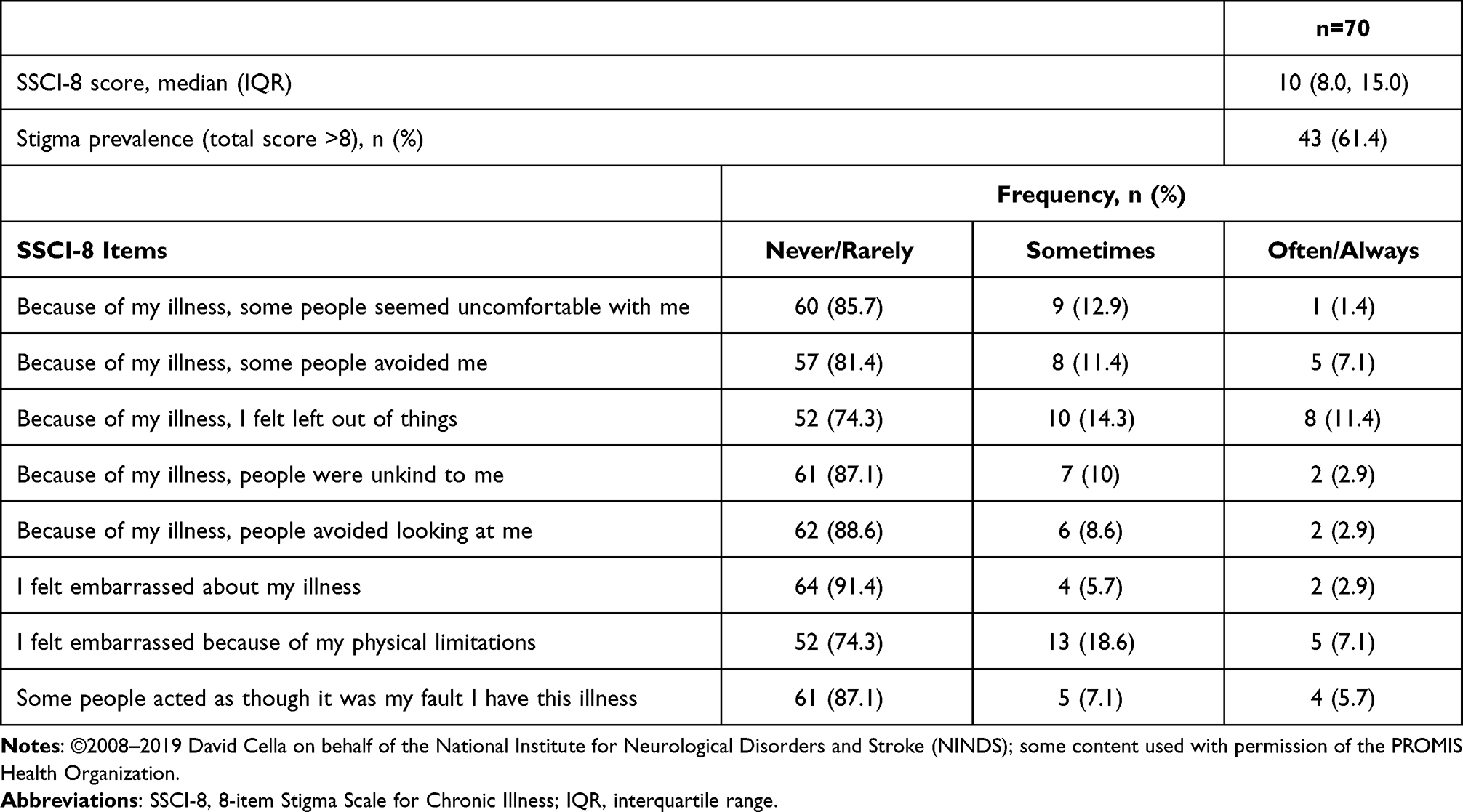 |
Table 2 Perception of Stigma |
The SSCI-8 score showed a significant correlation with physical and psychological MSIS-29 scores (rho=0.576 and 0.608, p<0.0001, respectively), EDSS score (rho=0.349, p=0.0033), BDI-FS score (rho= 0.613, p<0.0001), MOS-PES score (rho= 0.457, p<0.0001), and D-FIS score (rho=0.556, p<0.0001) (Table 3). Stigma was found to positively predict concurrent depression (OR=1.32; 95% CI: 1.13–1.55, p=0.0004).
 |
Table 3 Correlations Between SSCI-8 and BDI-FS, MOS PES, D-FIS, and EDSS |
Discussion
Little is known about the patient´s experience of living with NMOSD.31 Fear of disability and impaired activities of daily living were associated with uncertainty about the disease trajectory.31,32 Limitations in social activities and type of work were reported by most of 522 patients participating in the US online community PatientsLikeMe.4 Somatic complaints and hopelessness were correlated with disease duration.22 Barzegar et al found that NMOSD patients had significantly worse quality of life compared with MS patients, with fatigue being the most important variable for predicting variance.33
The impact of stigma has been documented across a number of neurological disorders, especially Parkinson´s disease, epilepsy, and Alzheimer´s disease.8,10 Stigma was a common phenomenon in a survey with 1,373 patients with different neurological conditions from 37 countries.8 Lack of understanding was seen as the biggest cause of this, followed by misconceptions about these disorders and their hidden nature. More than thirty percent of participants reported regularly being made to feel that their condition is their fault, over twenty percent felt that people avoid them often or always, and forty-five percent felt that they are regularly left out of things.
Perception of stigma in patients with NMOSD using standardized measures has not been previously explored. In our study, more than sixty percent of patients experienced stigmatization. Stigma was found to have a strong negative correlation with physical and psychological quality of life.
There is scarce information regarding psychiatric comorbidities in patients with NMOSD. Based on a retrospective analysis of a US administrative claims database, the prevalence of depression in patients with NMO (n=1,349) and highly active NMO (n=134; defined as at least two relapses within twelve months of the patient’s first NMO encounter in the database) was estimated at 17.9% and 25.4%, respectively.34 Fernandez et al found that ten patients with NMOSD (50%) had current depressive symptoms versus five (28%) patients with MS (p=0.16).35 Six (30%) patients with NMOSD versus only one (5.5%) patient with MS had attempted suicide at least once (p=0.05). Current suicide risk was high in patients with NMOSD (8, 40%) and moderate in patients with MS (4, 22%). In our study, thirty-one patients (43.6%) had depression. Differences regarding our findings could be based on cultural factors and the administration of different instruments to assess depressive symptoms across studies.
Stigma is a previously studied predictor of depression in patients with MS. Cadden et al and Pérez-Miralles et al assessed the association between stigma and depression in MS, concurrently and prospectively.15,36 A moderate bivariate correlation between stigma and depression measured at baseline and one year later was found in a survey with 5,413 participants administered by the North American Research Committee on Multiple Sclerosis.15 Almost eighty percent of a sample of 55 patients with primary progressive MS reported some degree of stigmatization at baseline and one year later.16,36 Increased baseline SSCI-8 scores were associated with a higher risk of depression (OR=1.21, p=0.007) and moderate-to-severe depression (OR=1.37, p=0.003).36
Patients with rare diseases show even worse quality of life compared to the general population and people with common chronic diseases.37 A comprehensive disease information and educational efforts to achieve an adequate public knowledge of NMOSD may help in decreasing its stigma. The ultimate goal of all such initiatives should be to prevent the isolation of NMOSD patients and their families and to facilitate their social integration.
The relatively small sample size and cross-sectional design are the main limitations of this study. A causal relationship between stigma and depression cannot be established. We also cannot rule out the possibility that the perception of stigma was influenced by other factors that have not been analyzed in this study, such as current immunosuppressant drugs and disease-modifying therapies for the management of NMOSD, impact of medical or psychological comorbid conditions, or serologic status. However, the study sample was managed at 13 different hospitals throughout Spain, allowing results to be generalized to clinical practice.
Conclusion
Perception of stigma is a common phenomenon in NMOSD, even in a clinically stable population with low physical disability. Further studies with longitudinal follow-up are needed to confirm the relationships between stigma and quality of life and mood and elucidate the underlying mechanisms.
Data Sharing Statement
Qualified researchers may request access to individual patient-level data through the clinical study data request platform (https://vivli.org/). Further details on Roche’s criteria for eligible studies are available here (https://vivli.org/members/ourmembers/). For further details on Roche’s Global Policy on the Sharing of Clinical Information and how to request access to related clinical study documents, see here https://www.roche.com/research_and_development/who_we_are_how_we_work/clinical_trials/our_commitment_to_data_sharing.htm.
Acknowledgments
The authors would like to acknowledge all patients and their families for making the PERSPECTIVES-NMO study possible.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Medical Department of Roche Farma Spain (ML41397).
Disclosure
D. Prefasi, H. de Castro-Trapiello, and J. Maurino are employees of Roche Farma Spain. N. Canal is an employee of IQVIA Spain and IQVIA has received honoraria from Roche for clinical research services. F. Pérez-Miralles has received compensation for serving on scientific advisory boards or speaking honoraria from Almirall, Biogen Idec, Genzyme, Merck‐Serono, Mylan, Novartis, Roche, Sanofi‐Aventis, and Teva, outside the submitted work. M. Sepúlveda reports personal fees from Roche and UCB; travel reimbursement from Sanofi and Zambon. C. Calles reports personal fees from Biogen, Sanofi, Merck, Novartis, Teva, and Roche, outside the submitted work. S. Boyero reports personal fees from Roche, during the conduct of the study. L. Romero-Pinel took part in the observational study of Neuromyelitis optica: perspective NMO-ML41397. She also received honoraria compensation to participate in advisory boards, collaborations as a consultant and scientific communications and received research support, funding for travel and congress expenses from Biogen Idec, Bayer, Almirall, Merck, Sanofi-Genzyme, Roche, Novartis, and Teva. She reports participation in several clinical trials. Á Sempere reports personal fees from Biogen, Roche, Merck, Sanofi, and Teva, outside the submitted work. L. Querol reports grants from ISCIII, CIBERER, GBS-CIDP Foundation International, personal fees from UCB Pharma as the global principal investigator in clinical trial, grants and/or personal fees from Grifols, Roche, Merck, Akcea, Biogen, Novartis, Sanofi Genzyme, and Annexon, outside the submitted work. L. Costa-Frossard reports personal fees from Roche, during the conduct of the study; speaker fees, travel support, and/or served on advisory boards from Almirall, Bayer, Biogen, Biopass, Bristol-Myers, Ipsen, Merck, Novartis, Sanofi, and Teva, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Marignier R, Cobo Calvo A, Vukusic S. Neuromyelitis optica and neuromyelitis optica spectrum disorders. Curr Opin Neurol. 2017;30(3):208–215. doi:10.1097/WCO.0000000000000455
2. Borisow N, Mori M, Kuwabara S, Scheel M, Paul F. Diagnosis and treatment of NMO spectrum disorder and MOG-encephalomyelitis. Front Neurol. 2018;9:888. doi:10.3389/fneur.2018.00888
3. Papp V, Magyari M, Aktas O, et al. Worldwide incidence and prevalence of neuromyelitis optica: a systematic review. Neurology. 2021;96(2):59–77. doi:10.1212/WNL.0000000000011153
4. Eaneff S, Wang V, Hanger M, et al. Patient perspectives on neuromyelitis optica spectrum disorders: data from the PatientsLikeMe online community. Mult Scler Relat Disord. 2017;17:116–122. doi:10.1016/j.msard.2017.07.014
5. Jarius S, Paul F, Weinshenker BG, et al. Neuromyelitis optica. Nat Rev Dis Primers. 2020;6(1):85. doi:10.1038/s41572-020-0214-9
6. Methley AM, Mutch K, Moore P, Jacob A. Development of a patient-centred conceptual framework of health-related quality of life in neuromyelitis optica: a qualitative study. Health Expect. 2017;20(1):47–58. doi:10.1111/hex.12432
7. Banerjee A, Ng J, Coleman J, Ospina JP, Mealy M, Levy M. Outcomes from acute attacks of neuromyelitis optica spectrum disorder correlate with severity of attack, age and delay to treatment. Mult Scler Relat Disord. 2019;28:60–63. doi:10.1016/j.msard.2018.12.010
8. European Federation of Neurological Associations (EFNA). Survey on stigma and neurological disorder; 2020. Available from: https://www.efna.net/wp-content/uploads/2020/07/SurveyReport2020.pdf.
9. Burgener SC, Berger B. Measuring perceived stigma in persons with progressive neurological disease: Alzheimer’s dementia and Parkinson’s disease. Dementia. 2008;7(1):31–53.
10. Rao D, Choi SW, Victorson D, et al. Measuring stigma across neurological conditions: the development of the stigma scale for chronic illness (SSCI). Qual Life Res. 2009;18(5):585–595. doi:10.1007/s11136-009-9475-1
11. Ochoa-Morales A, Fresan-Orellana A, Hernández-Mojica T, et al. Perceived discrimination in patients with multiple sclerosis and depressive symptomatology. Mult Scler Relat Disord. 2020;48:102705. doi:10.1016/j.msard.2020.102705
12. Elliot VL, Morgan D, Kosteniuk J, et al. Health-related stigma of noncommunicable neurological disease in rural adult populations: a scoping review. Health Soc Care Community. 2019;27(4):e158–e188. doi:10.1111/hsc.12694
13. Anagnostouli M, Katsavos S, Artemiadis A, et al. Determinants of stigma in a cohort of hellenic patients suffering from multiple sclerosis: a cross-sectional study. BMC Neurol. 2016;16:101. doi:10.1186/s12883-016-0621-4
14. Cadden MH, Arnett PA, Tyry TM, et al. Judgment hurts: the psychological consequences of experiencing stigma in multiple sclerosis. Soc Sci Med. 2018;208:158–164. doi:10.1016/j.socscimed.2018.01.015
15. Pérez-Miralles F, Prefasi D, García-Merino A, et al. Perception of stigma in patients with primary progressive multiple sclerosis. Mult Scler J Exp Transl Clin. 2019;5(2):2055217319852717. doi:10.1177/2055217319852717
16. Maurino J, Martínez-Ginés ML, García-Domínguez JM, et al. Workplace difficulties, health-related quality of life, and perception of stigma from the perspective of patients with multiple sclerosis. Mult Scler Relat Disord. 2020;41:102046. doi:10.1016/j.msard.2020.102046
17. Dennison L, Yardley L, Devereux A, et al. Experiences of adjusting to early stage multiple sclerosis. J Health Psychol. 2011;16(3):478–488. doi:10.1177/1359105310384299
18. Shi Z, Chen H, Lian Z, et al. Factors that impact health-related quality of life in neuromyelitis optica spectrum disorder: anxiety, disability, fatigue and depression. J Neuroimmunol. 2016;293:54–58. doi:10.1016/j.jneuroim.2016.02.011
19. Nakazawa K, Noda T, Ichikura K, et al. Resilience and depression/anxiety symptoms in multiple sclerosis and neuromyelitis optica spectrum disorder. Mult Scler Relat Disord. 2018;25:309–315. doi:10.1016/j.msard.2018.08.023
20. Beekman J, Keisler A, Pedraza O, et al. Neuromyelitis optica spectrum disorder: patient experience and quality of life. Neurol Neuroimmunol Neuroinflamm. 2019;6(4):e580. doi:10.1212/NXI.0000000000000580
21. Shin JS, Kwon YN, Choi Y, et al. Comparison of psychiatric disturbances in patients with multiple sclerosis and neuromyelitis optica. Medicine (Baltimore). 2019;98(38):e17184. doi:10.1097/MD.0000000000017184
22. Wingerchuk DM, Banwell B, Bennett JL, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology. 2015;85(2):177–189. doi:10.1212/WNL.0000000000001729
23. Molina Y, Choi SW, Cella D, et al. The Stigma Scale for Chronic Illnesses 8-item version (SSCI-8): development, validation and use across neurological conditions. Int J Behav Med. 2013;20:450–460. doi:10.1007/s12529-012-9243-4
24. Ballesteros J, Martínez-Ginés ML, García-Domínguez JM, et al. Assessing stigma in multiple sclerosis: psychometric properties of the Eight-Item Stigma Scale for Chronic Illness (SSCI-8). Int J MS Care. 2019;21(5):195–199. doi:10.7224/1537-2073.2018-053
25. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. 1983;33(11):1444–1452. doi:10.1212/wnl.33.11.1444
26. Hobart J, Lamping D, Fitzpatrick R, et al. The Multiple Sclerosis Impact Scale (MSIS-29): a new patient-based outcome measure. Brain. 2001;124:962–973. doi:10.1093/brain/124.5.962
27. Benedict RH, Fishman I, McClellan MM, et al. Validity of the beck depression inventory-fast screen in multiple sclerosis. Mult Scler. 2003;9:393–396. doi:10.1191/1352458503ms902oa
28. Archibald CJ, McGrath P, Ritvo PG, et al. Pain prevalence, severity and impact in a clinic sample of multiple sclerosis patients. Pain. 1994;58(1):89–93. doi:10.1016/0304-3959(94)90188-0
29. Benito-León J, Martínez-Martín P, Frades B, et al. Impact of fatigue in multiple sclerosis: the fatigue impact scale for daily use (D-FIS). Mult Scler. 2007;13(5):645–651. doi:10.1177/1352458506073528
30. Mutch K, Methley A, Moore P, et al. Life on hold: the experience of living with neuromyelitis optica. Disabil Rehabil. 2014;36(13):1100–1107. doi:10.3109/09638288.2013.833301
31. Kitley J, Leite MI, Nakashima I, et al. Prognostic factors and disease course in aquaporin-4 antibody-positive patients with neuromyelitis optica spectrum disorder from the United Kingdom and Japan. Brain. 2012;135(Pt6):1834–1849. doi:10.1093/brain/aws109
32. Barzegar M, Badihian S, Mirmosayyeb O, et al. Comparative study of quality of life, anxiety, depression, and fatigue among patients with neuromyelitis optica spectrum disorder and multiple sclerosis: the first report from Iran. Mult Scler Relat Disord. 2018;22:161–165. doi:10.1016/j.msard.2018.04.009
33. Ajmera MR, Boscoe A, Mauskopf J, et al. Evaluation of comorbidities and health care resource use among patients with highly active neuromyelitis optica. J Neurol Sci. 2018;384:96–103. doi:10.1016/j.jns.2017.11.022
34. Fernández VC, Alonso N, Melamud L, et al. Psychiatric comorbidities and suicidality among patients with neuromyelitis optica spectrum disorders in Argentina. Mult Scler Relat Disord. 2018;19:40–43. doi:10.1016/j.msard.2017.11.002
35. Pérez-Miralles F, Prefasi D, García-Merino A, et al. Short-term data on disease activity, cognition, mood, stigma and employment outcomes in a cohort of patients with primary progressive multiple sclerosis (UPPMS study). Mult Scler Relat Disord. 2021;50:102860. doi:10.1016/j.msard.2021.102860
36. Broersma F, Oeseburg B, Dijkstra J, et al. The impact of self-perceived limitations, stigma and sense of coherence on quality of life in multiple sclerosis patients: results of a cross-sectional study. Clin Rehabil. 2018;32:536–545. doi:10.3389/fneur.2018.00888
37. Bogart KR, Irvin VL. Health-related quality of life among adults with diverse rare disorders. Orphanet J Rare Dis. 2017;12(1):177. doi:10.1186/s13023-017-0730-1
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.