")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Perception of Heath Care Providers About COVID-19 and Its Vaccination in Saudi Arabia: Cross-Sectional Study
Authors Alhofaian A , Tunsi A, Alaamri MM, Babkair LA, Almalki GA, Alsadi SM, Saeed Alharthi S, Almarhabi GA
Received 2 July 2021
Accepted for publication 31 August 2021
Published 15 September 2021 Volume 2021:14 Pages 2557—2563
DOI https://doi.org/10.2147/JMDH.S327376
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Aisha Alhofaian, Afnan Tunsi, Marym M Alaamri, Lisa A Babkair, Ghadah Ali Almalki, Safia Mohammed Alsadi, Samaher Saeed Alharthi, Ghadah Ahmed Almarhabi
Faculty of Nursing, King Abdul Aziz University, Jeddah, 21589, Saudi Arabia
Correspondence: Aisha Alhofaian
Faculty of Nursing, King Abdul Aziz University, P.O. Box. 80209, Jeddah, 21589, Saudi Arabia
Tel +966 505848634
Email [email protected]
Purpose: The aim of this study was to assess the perception of health care providers about the COVID-19 and its vaccine in Saudi Arabia.
Patients and Methods: In this study, we used a quantitative, cross-sectional and descriptive design. We recruited healthcare providers (HCPs) from social media platforms such as WhatsApp, Facebook, Twitter and emails that was distributed from March 15, 2021, to April 14, 2021. Chi-square tests were used to compare categorized data between health care workers.
Results: A total of 390 health care providers from different regions of the country began the online survey. A total of 298 respondents (77.8%) accepted the COVID-19 vaccine, whereas 85 (22.2%) HCP disapproved. There was a significant difference in the degree of acceptance of COVID-19 immunization among health care providers (P< 0.001). Moreover, the results showed 200 females (52.63%) were more likely to accept the COVID-19 immunization; 97 (25.5%) males were planning on getting one as soon as possible.
Conclusion: As shown in the results, 77.8% of health care providers agreed to receive the vaccine. Since COVID-19 is still ongoing, we must increase the number of HCPs who get vaccinated. In addition, a comprehensive immunization campaign is necessary to achieve maximum acceptance by the general public.
Keywords: healthcare providers, vaccination, Saudi Arabia, perceptions, acceptance, COVID-19
Introduction
The COVID-19 crisis is a pandemic that has been spreading around the world for more than a year. This illness is caused by a novel coronavirus that has been officially named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2; formerly called 2019-nCoV). COVID-19 is a highly contagious and rapidly spreading virus. When the virus began spreading around the world, the World Health Organization (WHO) classified it as a pandemic on March 12, 2020.1 As of the middle of November 2020, there have been more than 53,700,000 confirmed cases of people infected and more than 1,300,000 reported deaths.2 In Saudi Arabia, 539,698 infections and 8431 coronavirus-related deaths have been reported in the country since the pandemic began. In addition, Saudi Arabia has administered at least 32,281,173 COVID-19 vaccines, accounting for about 47% of the Saudi population.
The virus will not stop entirely, unless people develop strong immunity against the virus, which would be achievable through proper vaccination that is specifically built to fight COVID-19. It is unlikely that even people with an open mind will accept a new vaccine that has not been tested for more than a year because they fear being one of the first to get vaccinated with this new vaccine.3 This is a common feeling among everyone. Compliance generally depends on the opinions of health care professionals (HCPs) and their attitudes toward vaccination. HCPs are the most influential factors for affecting the general population’s acceptance of a vaccine due to their profession and their expertise in these matters. If HCPs do not accept the vaccine, people will not be encouraged to take it. A patient’s acceptance of the vaccine is also strongly affected by whether their HCP has already been vaccinated.4
In China, a study was conducted to uncover the acceptance of future coronavirus vaccines among 352 HCPs and 189 people from the community. The results showed that 76.4% of the HCPs accepted the vaccine, but only 72.5% of society did.5 Another study conducted in Israel concerned the hesitancy of future coronavirus vaccination among health care workers (HCWs) and some people from the Israeli community. The results showed that the HCWs accepted the influenza vaccine more highly than the coronavirus vaccine. The rate of doctors who accepted future coronavirus immunization was 78%, which was more than the rate of nurses at 61%.6
In the Republic of the Congo, a study conducted by Kabamba Nzaji et al in 23 Congolese hospitals found that only 28% of HCWs would get a future coronavirus vaccine if it was available.4 In Romania, Padureanu et al researched the opinions of HCPs regarding the COVID-19 pandemic, including whether, if a vaccine was found against it, they would accept it or not. The result was that only 69% of HCPs agreed with vaccination.
Research conducted in France by Gagneux-Brunon et al examined the COVID-19 vaccine acceptance rate among HCPs. The results showed that 75% of HCPs accepted COVID-19 vaccination. In addition, there was a difference among some occupational categories, such as physicians, who accepted the COVID-19 vaccine at a rate of 92.1% compared with nurses and assistant nurses, who showed less vaccine acceptance.1 Also in France, Verger conducted a survey of HCWs who were involved with the immunization of the general population and their attitudes toward COVID-19 vaccination. The results showed that 48.6% of HCWs were highly accepting, 23% had a moderate acceptance, and 28.4% were not sure if they wanted to take the vaccine, their decision primarily driven by their concerns about the vaccine’s safety.7
In the United States, Pfizer and BioNTech’s first BNT162b2 mRNA vaccine was available only for priority groups such as people living in long-term care facilities and HCPs. By doing this, people in the country will be encouraged to take the vaccine.8 France has also designated HCPs as a priority group for the vaccine. Because HCPs are severely exposed to getting infected due to the nature of their work and their position on the front lines, the WHO has also listed them as a priority group to receive the coronavirus vaccine.1 The aim of our study was to assess the perceptions of HCPs regarding the COVID-19 and its vaccine because they are a key factor in influencing the general population’s decisions on whether they should get the vaccine or not.
Materials and Methods
Ethical Consideration
This study was approved by the Faculty of Nursing at King Abdul Aziz University (ref. no. 2B.65) according to the guidelines (Declaration of Helsinki). Electronic-informed consent was provided to participants, including the aim of the study, inclusion and exclusion criteria, and eligibility to agree or refuse to participate in the research, prior to survey enrolment. In addition, participants were reassuring that online survey would remain anonymous and confidential.
Study Design
The researcher used Google Forms, an online English survey tool, to distribute the survey on social media, and participants were given 10 minutes to answer 14 questions. The survey was distributed from March 15, 2021, to April 14, 2021, and the respondents were recruited from health care providers currently working at private hospitals, government hospitals, or clinics in Saudi Arabia using targeted advertising on social media such as WhatsApp, Facebook, Twitter and emails. The inclusion criteria were health care providers (nurses, physicians, dentists, and pharmacists) and other professionals such as respiratory therapists and nutritionists who were 18 years or older and working at private hospitals, government hospitals, or clinics in Saudi Arabia. The exclusion criteria were individuals younger than 18 years old and future health care providers, including nursing and medical students. The researchers estimated the sample size for this study to be 383 participants, as calculated by z2P (1 ― P) y/d2 with a degree of confidence of 95% and margin of error was 5%.
This study consisted of two parts. The first part of the questionnaire contained six items about the sociodemographic characteristics of the participant: age, gender, region, education level, profession, and years of clinical experience. The second part of the questionnaire was developed based on a validated scale the “Exposure Risk Assessment in the Context of COVID-19” previously used in a study of the perceptions of health care providers.9 This questionnaire contained eight items that inquired about the perception (attitude and beliefs) of health care providers toward COVID-19 and its vaccines. Three items evaluated treatment selection, and five were related to beliefs. The participants’ responses in this section were limited to either yes or no. The questionnaire was disseminated in the English language using an electronic survey to all health care providers via a Google link with no identifiers. The participants returned the electronic survey without identifiers.
Statistical Analysis
Simple descriptive statistics such as mean, mode, and standard deviation (SD) were used for continuous variables whereas frequencies and percentages were applied for categorized variables. Additionally, chi-square tests or Fisher’s exact tests were used to compare categorized data between health care workers. T-test and one-way ANOVA were used to compare continuous data. The significance level was 0.05. The data were analyzed with the IBM SPSS program for Statistics version 25.
Results
The demographic characteristics of health care providers appear in Table 1. A total of 390 health care providers from different regions of the country began the online survey, and 383 participants completed all the questions (a 98% completion rate). More than half of the participants were female (69.5%), and 30.5% were male, with ages ranging from 18 to 72. With regard to educational level, more than half of participants (65.8%) had a bachelor’s degree, whereas 17.2% had a diploma, 11% had a master’s degree, and 6% had a PhD. The majority of participants (n = 169, 44%) were from the Western region, whereas 5% of the participants were from the North region as is shown in the Table 1. The professions of health care providers were various, but the most common was nursing at 207 (54%), then physicians at 54 (14%), and pharmacists 38 (9.9%); the rest of the participants had other medical professions, such as respiratory therapists and nutritionists. The average length of participant’s clinical experience was 7 years.
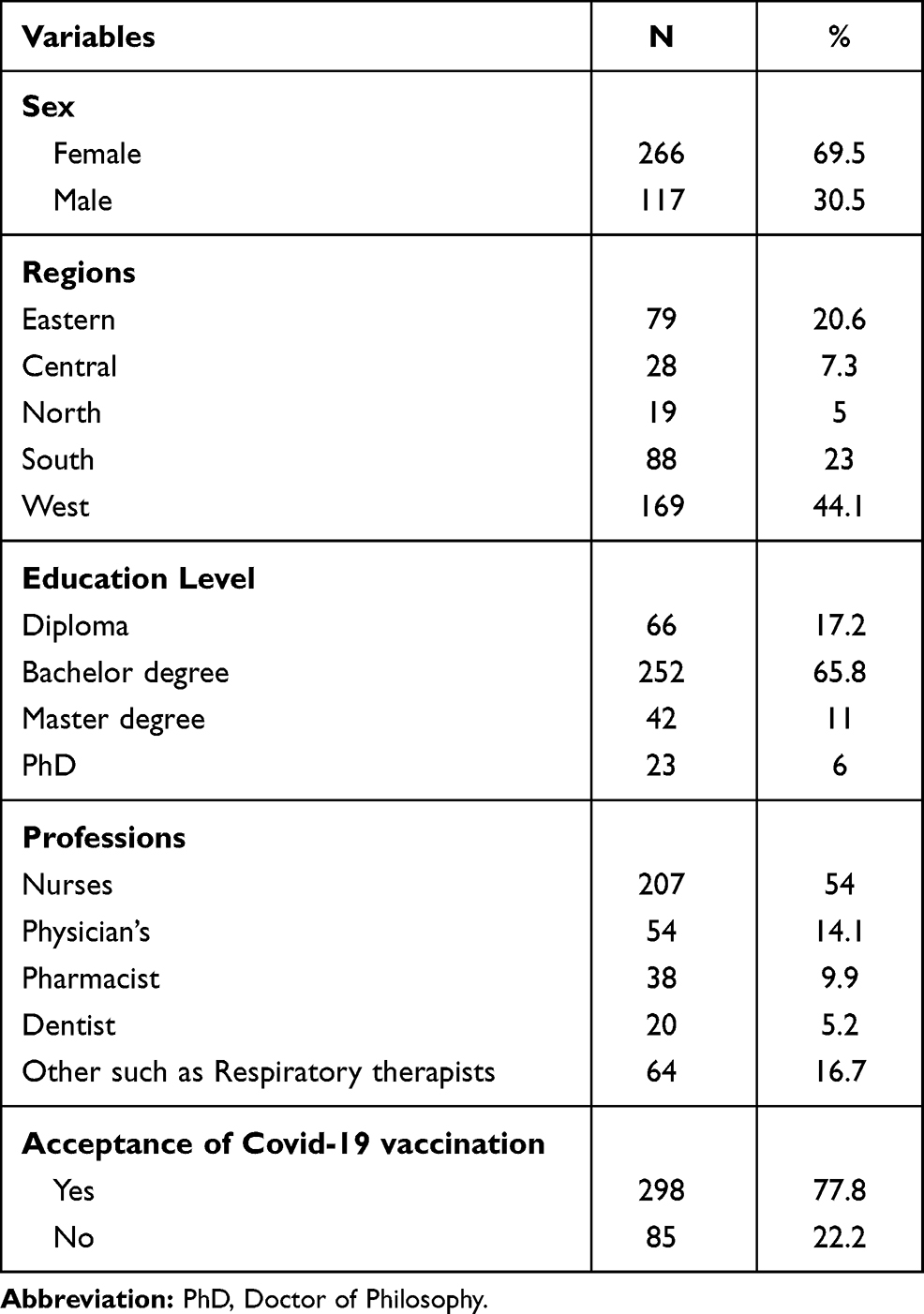 |
Table 1 Demographic Characteristics |
Table 2 shows the perception of health care providers with regard to COVID-19 vaccination and treatment. This table shows that 298 (77.8%) health care providers accepted and supported the COVID-19 vaccine, whereas 85 (22.2%) health care providers disapproved of it. There was a difference in the degree of acceptance of COVID-19 immunization among health care providers as shown in Table 2; the number of nurses who accepted the vaccine was 155 (40.78%), compared with physicians 46 (12.10%) and pharmacists 27 (7.10%). Furthermore, in other professions, the number of respiratory therapists who got vaccines, for example, was 3 (0.79%) and for the nutritionists, 1 (0.26%). Moreover, the results showed 200 females (52.63%) were more likely to accept the COVID-19 immunization; 97 (25.5%) males were planning on getting one as soon as possible.
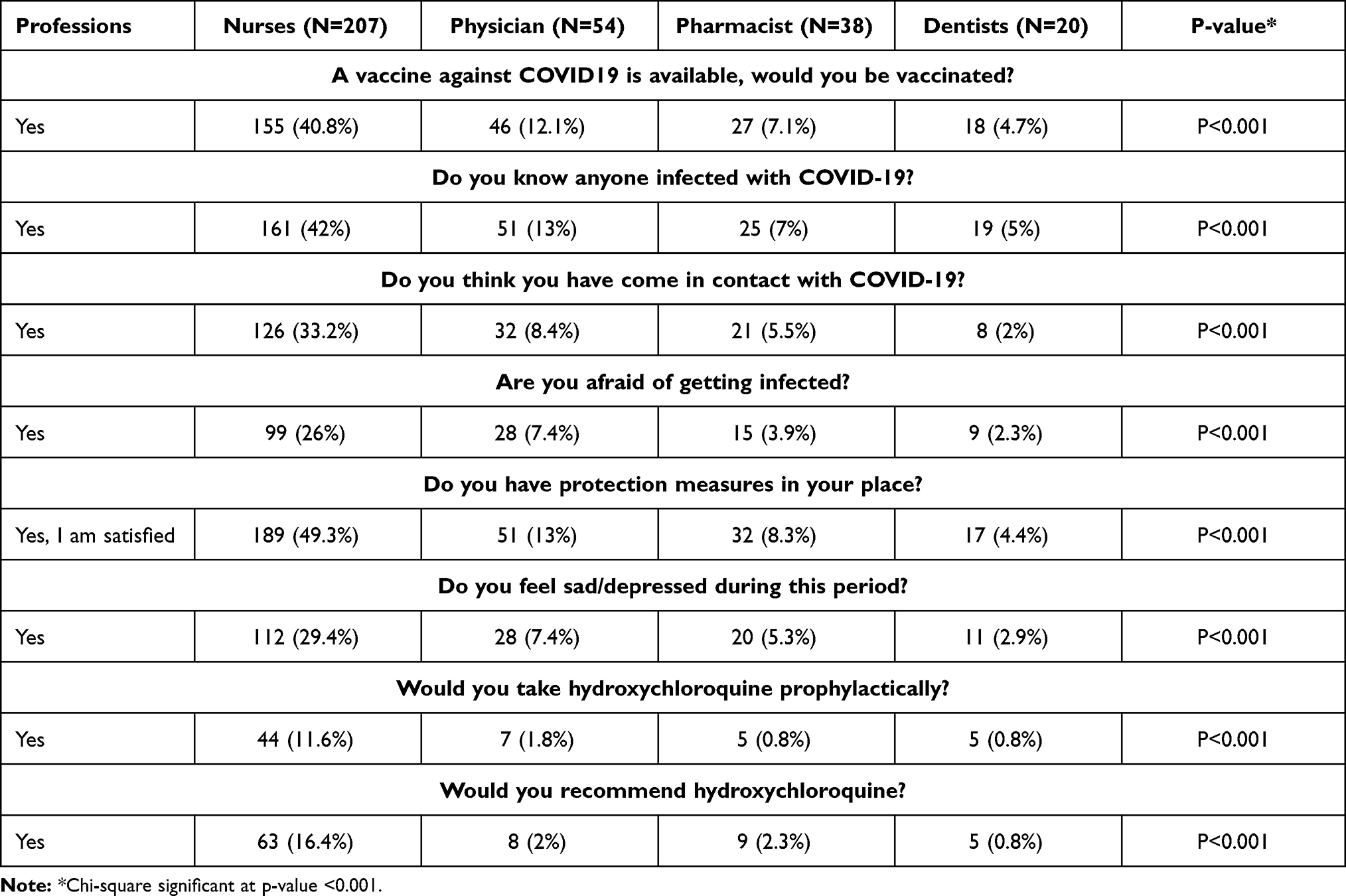 |
Table 2 COVID-19 Vaccination’s Perceptions |
More than half of the health care providers knew people who were infected with COVID-19. The results in the table show that 309 (79.2%) health care professionals knew someone infected with coronavirus, whereas 74 (19.0%) health care professionals did not know anyone infected with coronavirus. Further, 219 (56.2%) of the health care providers had come in contact with people with COVID-19, whereas 164 (42.1%) said they had not come into contact with anyone with COVID-19. Among health care professionals, nurses represented the highest percentage of health care providers who came in contact with COVID-19, at 33.15%; physicians had an 8.4% contact rate, pharmacists 5.5%, respiratory therapists 0.79%, and nutritionists 0.26%.
The results in Table 2 also indicate further differences among health care professionals (P < 0.001). Specifically, 194 (49.7%) of the health care workers said they were not afraid of being infected with COVID-19, whereas 189 (48.5%) said they were afraid. Among the nurses, 108 (28.4%) were not afraid, whereas 99 (26.05%) said they were afraid. Among the physicians, 28 (7.37%) were afraid of getting infected. Also, 23 (6.05%) pharmacists were not afraid of getting infected, whereas 15 (3.94%) were afraid. Additionally, within other professions there were conflicting opinions, such as respiratory therapists, 0.53% of whom said they were afraid of infection and 0.26% said they were not. Out of the nutritionists, only 0.26% said they were afraid of infection. In addition, 347 (89%) of the health care professionals were satisfied with the availability of protection measures, whereas 36 (9.2%) were not satisfied.
During the COVID-19 pandemic 52.6% participants reported having felt sad or depressed. There was significant difference in the depression levels between female and male health care providers (P < 0.001). Female health care providers had the highest level of depression. In addition, of all the groups of professionals, the nurses showed the highest percentage of depressed feelings during the pandemic period at 112 (29.4%), compared with the 95 (25%) nurses who felt the opposite during this period. As for the physicians, 28 (7.37%) reported feeling depressed or sad during this period. Of the nutritionists, only 1 (0.26%) did not feel depressed or sad during this period. As for pharmacists, 20 felt depressed or sad (5.26%), whereas 18 (4.7%) did not feel that way. The total number of respiratory therapists not feeling depressed or sad during this period was 2 (0.53%), leaving 1 (0.26%) who did feel depressed or sad.
Of the participants, 72 (18.5%) said they would actually take hydroxychloroquine prophylactically, whereas 311 (79.7%) of health care workers would not. On another hand, 106 of the respondents (27.2%) would recommend taking hydroxychloroquine as a prophylactic, whereas the other 277 (71%) would not recommend it.
Discussion
This study aimed to investigate the perception of health care providers about the COVID-19 and its vaccine in Saudi Arabia, we found that more than two-third (77.8%) of the health care providers were willing to receive the vaccine. This finding goes in line with a study conducted in France1 in which 75% of the health care providers accepted the COVID-19 vaccine. It also corresponds with the findings of Giuseppe et al, who reported an increased willingness to receive the influenza vaccination during the COVID-19 pandemic among health care workers (n=490) in Italy.10 Yet, it is at odds with the findings of a Taiwanese study exploring COVID-19 vaccination willingness among health care workers (n=500) and outpatients (n=238), which appeared to be low.11
Furthermore, females were more likely to accept COVID-19 vaccines compared to their male counterpart, at the rate of 52.63%, unlike another study conducted in the Republic of the Congo showing that males were more likely to accept the vaccine, at a percentage of 50.9%.4
Health care providers are at significant amount of risk of catching an infection due to being in direct contact with many COVID-19 cases. Additionally, most of the health care providers we surveyed (79.2%) knew people who were infected with COVID-19. Another study has shown that 66% of health care workers believe that they may have been infected with the virus from close contact with people with COVID-19.4
In terms of professions based variations, Studies in Romania and Israel reported that nurses accepted vaccines less than physicians.6,9 Unlike this present study where nurses were actually more accepting of the vaccine than the physicians and pharmacists. We have extrapolated that 56.2% of health care providers have come in contact with patients infected with COVID-19, and the majority of them were nurses.
Fear of catching the virus and becoming infected was also reported among health care workers in the current study. It appeared that almost half of the participants (49.7%) were not afraid of being infected with COVID-19, whereas (48.5%) said they were afraid. This COVID-19-related anxiety and fear were associated with increased acceptance of vaccination. This finding complements those of Bendau et al. They reported a positive correlation between COVID-19 fears and vaccine acceptance among the general population in Germany.
Protection measures against the COVID-19 virus were made in Saudi Arabia during the COVID-19 pandemic period. For example, a lockdown was initiated by the government at the beginning of the pandemic period, when there was a significant increase in the cases of people infected with the virus.12 After the lockdown, many other prevention methods were developed and regulations were set to prevent the spread of infection: fees were charged for not wearing a mask in public; public gatherings with huge numbers of people were disallowed; only a limited amount of people were allowed to be in one place; people’s temperatures were checked at public entrances; and Tawakkalna, an application developed for this exact purpose, was a requirement for entering businesses such as restaurants, malls, or shops. So, we have assessed the health care providers’ thoughts about these strategies, and 347 (89%) were satisfied with the protection measures in Saudi Arabia.
Given that the health care providers are the ones who are at the front line of defense of this virus, a noticeable number felt sad or depressed. Our study demonstrated that 205 (52.6%) out of the total respondents were depressed during the pandemic. As shown in the Romanian study, all of the health care workers of all ages, professions, and genders had a moderate level of depression and sadness.9 However, we found that there were differences within gender. This finding was consistent with other studies’ findings that depression was more common in females and nursing staff.13 A possible reason for this is that female nurses have more family responsibilities than male nurses. It is more difficult for a female nurse to stay away from her family and children, especially if her children are still at a young age. A female nurse may also be breastfeeding, so it could be especially hard for her to stay far away from her child, such as living in a place other than her own house, for the purpose of reducing the risk of transmitting the infection to her family and children.13 All of these could affect her mental health and lead to an increased fear of risking her family’s health.
Initially, the medicine used to treat hospitalized patients infected at the beginning of the pandemic was hydroxychloroquine, even though the proven benefits of this medicine were limited.14 In this case, the health care providers’ decisions involved determining whether to take hydroxychloroquine prophylactically or not as well as determining whether to recommend this medicine for infected patients. Our study’s results showed that 72 respondents (18.5%) would suggest taking hydroxychloroquine prophylactically, whereas 106 (27.2%) would recommend it. However, the Romanian study results showed that 236 (45%) of the health care providers would recommend taking this medicine.9
Our study has several limitations that warrant discussion. First, data were collected once via an online survey. Second, we used the nonprobability sampling strategy to recruit our volunteer participants, which may decrease the generalizability of our findings to the general population. Moreover, most participants were nurses; therefore, perceptions of other HCP professions regarding the COVID-19 vaccine were not assessed. However, the current study has some considerable strengths. It is the first study within the Saudi context that explored health care providers’ perception of COVID-19 vaccination, providing novel insights and expanding the current literature. Similar studies conducted in the same region were focused on the general population rather than health care providers15,16 or were conducted in other countries within the Middle East and not only Saudi Arabia.17 Other strengths include collecting data from multiple regions in Saudi Arabia, a high completion rate (98%), and a large sample size.
Conclusion
A successful COVID-19 vaccination program depends largely on the public’s acceptance of and willingness to get the vaccine. Information about covid-19 vaccination can obtain from health-care providers, and public health communication can increase adherence to vaccination guidelines.18 Thus, health care provider’s role is critical in encouraging not only their own patients but also whole communities to be vaccinated.
Our conclusion is that 77.8% of health care providers accepted the COVID-19 vaccine with discrepancies among occupational categories. According to our results, a high number of nurses who accepted the vaccine was 155 (40.8%), compared with physicians 46 (12.1%) and pharmacists 27 (7.1%). Furthermore, in other professions, the number of respiratory therapists who got vaccines, for example, was 3 (0.79%) and for the nutritionists, 1 (0.26%). Moreover, the results showed 200 females (52.6%) were more likely to accept the COVID-19 immunization; 97 (25.5%) males were planning on getting one as soon as possible.
Given that the health care providers are the ones who are at the front line of defense of this virus, a noticeable number felt sad or depressed. Our result concluded that the number of health care providers who have felt depressed during this period is high. The nurses showed the highest percentage of depressed feelings during the pandemic period at 112 (29.4%) as well as the feminine health care workers.
In order to increase the acceptance of the COVID-19 vaccine, social media companies must implement new strategies. Companies on social media must focus on the dissemination of proper information regarding COVID-19 vaccine and delete any information that is inaccurate or incorrect on social media. Reliable evidence must be available to counter any widespread fake news. There is also a need for more engagement and collaboration between research institutions, pharmaceutical companies and regulatory agencies, thus establishing the Accelerated Therapeutic Intervention and Vaccine (ACTIV) Program for Coronavirus. The World Health Organization and other multilateral institutions must remain focused and relentless in financing and disseminating the vaccine for global use. It must ensure equitable distribution among all countries when it becomes available.
Vaccine safety and efficacy testing must comply with international best practices, and be free from political, religious or racial discrimination. The creation of COVID-19 vaccines should not violate ethical principles such as informed consent and medical privacy. The COVID-19 vaccines have to be safe and effective, and once proven, a comprehensive vaccination campaign is essential to maximize acceptance by the general public.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the ethical committee from the Faculty of Nursing at King Abdul Aziz University (ref. no. 2B.65).
Data Sharing Statement
Data used and analyzed in this study will be promptly available for the publisher upon request.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest for this work.
References
1. Gagneux-Brunon A, Detoc M, Bruel S, et al. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: a cross-sectional survey. J Hosp Infect. 2021;108:168–173. doi:10.1016/j.jhin.2020.11.020
2. Alanezi F, Aljahdali A, Alyousef SM, et al. Investigating healthcare practitioners’ attitudes towards the COVID-19 outbreak in Saudi Arabia: a general qualitative framework for managing the pandemic. Inform Med Unlocked. 2021;22:100491. doi:10.1016/j.imu.2020.100491
3. Smith TC. Vaccine rejection and hesitancy: a review and call to action. Open Forum Infect Dis. 2017;4(3):ofx146. doi:10.1093/ofid/ofx146
4. Kabamba Nzaji M, Kabamba Ngombe L, Ngoie Mwamba G, et al. Acceptability of vaccination against COVID-19 among healthcare workers in the democratic Republic of the Congo. Pragmat Obs Res. 2020;11:103–109. doi:10.2147/por.s271096
5. Fu C, Wei Z, Pei S, Li S, Sun X, Liu P. Acceptance and preference for COVID-19 vaccination in health-care workers (HCWs). medRxiv; 2020. Available from: https://europepmc.org/article/ppr/ppr150866. Accessed September 10, 2021. doi:10.1101/2020.04.09.20060103
6. Dror AA, Eisenbach N, Taiber S, et al. Vaccine hesitancy: the next challenge in the fight against COVID-19. Eur J Epidemiol. 2020;35(8):775–779. doi:10.1007/s10654-020-00671-y
7. Verger P, Scronias D, Dauby N, et al. Attitudes of healthcare workers towards COVID-19 vaccination: a survey in France and French-speaking parts of Belgium and Canada, 2020. Eurosurveillance. 2021;26(3):3. doi:10.2807/1560-7917.es.2021.26.3.2002047
8. Shaw J, Stewart T, Anderson KB, et al. Assessment of U.S. health care personnel (HCP) attitudes towards COVID-19 vaccination in a large university health care system. Clin Infect Dis. 2021:ciab054. doi:10.1093/cid/ciab054
9. Padureanu V, Bogdan M, Subtirelu M-S, et al. Perceptions of covid-19 vaccination among healthcare professionals in Romania. Medi Surg J Rev Med Chir. 2020;124(3):454–460.
10. Di Giuseppe G, Pelullo CP, Paolantonio A, Della Polla G, Pavia M. Healthcare workers’ willingness to receive influenza vaccination in the context of the COVID-19 pandemic: a survey in Southern Italy. Vaccines. 2021;9(7):766. doi:10.3390/vaccines9070766
11. Kukreti S, Lu M-Y, Lin Y-H, et al. Willingness of Taiwan’s healthcare workers and outpatients to vaccinate against covid-19 during a period without community outbreaks. Vaccines. 2021;9(3):246. doi:10.3390/vaccines9030246
12. Alrashed S, Min-Allah N, Saxena A, Ali I, Mehmood R. Impact of lockdowns on the spread of COVID-19 in Saudi Arabia. Inform Med Unlocked. 2020;20:100420. doi:10.1016/j.imu.2020.100420
13. Pappa S, Ntella V, Giannakas T, Giannakoulis VG, Papoutsi E, Katsaounou P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Brain Behav Immun. 2020;88:901–907. doi:10.1016/j.bbi.2020.05.026
14. Schilling WHK, White NJ. Does hydroxychloroquine still have any role in the COVID-19 pandemic? Expert Opin Pharmacother. 2021;22(10):1257–1266. doi:10.1080/14656566.2021.1898589
15. Fayed AA, Al Shahrani AS, Almanea LT, et al. Willingness to receive the COVID-19 and seasonal influenza vaccines among the Saudi population and vaccine uptake during the initial stage of the national vaccination campaign: a cross-sectional survey. Vaccines. 2021;9(7):765. doi:10.3390/vaccines9070765
16. AL-Mohaithef M, Padhi BK, Ennaceur S. Socio-demographics correlate of COVID-19 vaccine hesitancy during the second wave of COVID-19 pandemic: a cross-sectional web-based survey in Saudi Arabia. Front Public Health. 2021;9:698106. doi:10.3389/fpubh.2021.698106
17. Al-Qerem WA, Jarab AS. COVID-19 vaccination acceptance and its associated factors among a middle eastern population. Front Public Health. 2021;9:34. doi:10.3389/fpubh.2021.632914
18. Shekhar R, Sheikh AB, Upadhyay S, et al. COVID-19 vaccine acceptance among health care workers in the United States. medRxiv. 2021;2021:21249184.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.