")
Back to Journals » Open Access Emergency Medicine » Volume 13
Perception of an Introductory Point-of-Care Ultrasound Course for Thai Medical Students on Emergency Medicine Rotation
Authors Vanichkulbodee A , Inboriboon PC , Balk AH, Sri-on J
Received 20 April 2021
Accepted for publication 11 June 2021
Published 5 July 2021 Volume 2021:13 Pages 291—298
DOI https://doi.org/10.2147/OAEM.S316730
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Hans-Christoph Pape
Alissara Vanichkulbodee,1,2 Pholaphat Charles Inboriboon,3 Andrew H Balk,2 Jiraporn Sri-on1
1Department of Emergency Medicine, Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand; 2Department of Emergency Medicine, Truman Medical Center, University of Missouri-Kansas City (UMKC) School of Medicine, Kansas City, MO, USA; 3Department of Emergency Medicine, University of Illinois at Chicago College of Medicine, Chicago, IL, USA
Correspondence: Alissara Vanichkulbodee Email [email protected]
Introduction: Point-of-care ultrasonography (POCUS) is increasingly utilized in emergency departments (EDs) throughout Thailand. Although emergency medicine (EM) residents are trained in POCUS, Thai medical students receive limited training. An introductory POCUS course was implemented for medical students to prepare them for internships.
Objective: This study described the perception and use of POCUS by graduates of an introductory POCUS course.
Materials and Methods: Medical students who completed the POCUS course were surveyed during their intern year from 2012 to 2015. The survey collected demographic characteristics. The Likert Scale was used to assess POCUS practice patterns and perceptions of the course.
Results: There were 230 respondents (98% response rate). All thought that POCUS was important. Furthermore, 96% of respondents felt that the POCUS course meaningfully impacted their ability to deliver care. POCUS use was greatest for obstetrics/gynecology and trauma cases. Over half of respondents (55.2%) felt very confident with using extended-Focused Assessment with Sonography in Trauma. Most respondents (81.8%) were positively impacted by the course, and 61.7% were satisfied with the scope of the course. Recommendations for improvement included increasing the course length, the content, and the hands-on time for POCUS practice.
Conclusion: Graduates positively perceived the course and felt it dramatically impacted their clinical practice as novice physicians. An introductory POCUS course should be incorporated into the medical school curriculum to prepare graduates for practice. Future goals include increasing the scope of POCUS practice to help guide interns and residents in emergency patient care such as lung ultrasound in COVID-19 or pneumonia patients and studying the impact this course has on patient outcomes.
Keywords: eFAST, intern, medical education, point-of-care ultrasound
Introduction
Prompt diagnosis in the emergency department is key to optimizing patient care. This is especially true for critically ill patients where there are often limitations to obtaining history and physical examination.1,2 Point-of-care ultrasonography (POCUS) in the ED plays a crucial role in obtaining diagnoses and expediting appropriate treatment.1,3,4 The American College of Surgeons has incorporated POCUS into the Advance Trauma Life Support course, a course that is considered the standard for trauma care in the US and abroad.1,5,6
Institutions in developed countries have implemented undergraduate medical students’ ultrasound training to develop and improve ultrasound knowledge and skills in medical school.7–9 In many developed countries, medical students go on to pursue post-residency training where they have the opportunity to develop their ultrasound skills. This is not the case in many other countries.
The Medical Competency Assessment Criteria for Thai National License 2012 recommends that medical students acquire skills in diagnostic ultrasound of the abdomen and retroperitoneum in traumatic conditions and that interns should be skilled in performing and interpreting POCUS after finishing the first year of their internships. There currently is no standardized curriculum for ultrasound training in the Thai medical curriculum. In addition, there is a shortage of subspecialists and emergency physicians to supervise interns, especially in rural areas often with minimal direct supervision.
In 2012, our hospital commenced an introductory POCUS course consisting of lectures and hands-on skills workshops aimed at developing the ultrasound skills of sixth-year medical students on their EM rotation. The objectives of this study were to clarify the interns’ perceptions and practice experiences after completing the hands-on introductory POCUS course and also to assess the usefulness of an ultrasound course integrated into the undergraduate medical curriculum in Thailand.
Materials and Methods
This study was approved by the institutional review board (IRB) of Faculty of Medicine Vajira Hospital, Bangkok, Thailand: COA 80/2559. We have obtained electronic consent from study participants before responding to the survey.
Survey Design and Development
This cross-sectional self-administered online survey was sent via email to interns who graduated from one urban teaching hospital in Bangkok, Thailand during 2012 to 2015 academic years using Survey Monkey (Palo Alto, USA http://www.surveymonkey.com). The criteria for the survey participants were the following: 1) participants who graduated from our hospital between 2012 and 2015; 2) participants served as general practitioners (interns) between 2012 and 2015. There were twelve rotations of final-year medical students in each academic year. The EM ultrasound curriculum included a 1.5-hour lecture on the introduction of emergency ultrasound application including resuscitation, the indication of eFAST exam, anatomy, image orientation, FAST exam with lung ultrasound, case review of each quadrant, pre/post examinations, and a 1.5–2 hour hands-on introductory POCUS (eFAST scanning) session one-on-one with a human volunteer and observed by an attending emergency physician and pass the post-rotation assessment to ensure standards of quality after finishing the rotation. The survey was developed through a process composed of item generation and survey construction, pilot study group testing, and survey clarification, and survey development after emergency physician’s recommendations and testing.
Step 1: Item Generation and Survey Construction
The survey questionnaire was adapted from a study by Gogalniceanu et al.7 The survey comprised 5 categories which included: baseline demographics; the level of the hospital where they are currently working; experience in ultrasound use; the level of confidence in ultrasound use; perception of the introductory POCUS course; and their recommendations about the course. There were 22 questions with 8 multiple choice questions, 7 multiple choice closed-ended questions, 2 open-ended questions, and 5 questions about the Likert scale response format. The initial survey was validated by 5 attending emergency physicians who had worked at this ED but were not involved in the process of survey construction.
Step 2: Pilot Study Group Testing and Survey Clarification
The survey was piloted by 10 emergency medicine residents who did not graduate from this university. Thai medical students and physicians are taught using English textbooks, so the survey was developed in Thai together with some items further explained in English; when the English term is commonly used or is easier to understand than the Thai translation. We have attached the English-translated survey questionnaires to the manuscript as Supplementary File 1.
Step 3: Survey Development After Emergency Physicians’ (EPs) Recommendations and Testing
Survey Administration
The survey was distributed via email list by the undergraduate medical education department of this faculty on three occasions between August 21, 2016, and October 20, 2016. Survey responses were returned anonymously. A reminder to complete the survey was sent out via email at the end of the second, fourth, and sixth weeks after the initial distribution of the survey.
Statistical Analysis
IBM SPSS statistics Red Hat Enterprise Linux version “21.0.0.1” was used to analyze categorical values. Categorized data, such as sex, were presented as percentages. Incomplete questions were recorded as non-response to distinguish them from completed surveys. All incomplete surveys were excluded from the analysis.
Participants
A total of 254 medical students, who graduated and served as interns within 2012 to 2015 academic years, could be contacted with an existing email address. We excluded 20 medical students who did not attend the class, 1 medical student who was not an intern, and 1 medical student who was not practicing medicine. The ultrasound machine used during the course was a Phillips IU22 (USA). The students were trained on, and practiced with, this machine.
Results
234 medical students attended the introductory POCUS course. Ninety-eight percent (230/234) of students who attended the course responded to the survey (Figure 1).
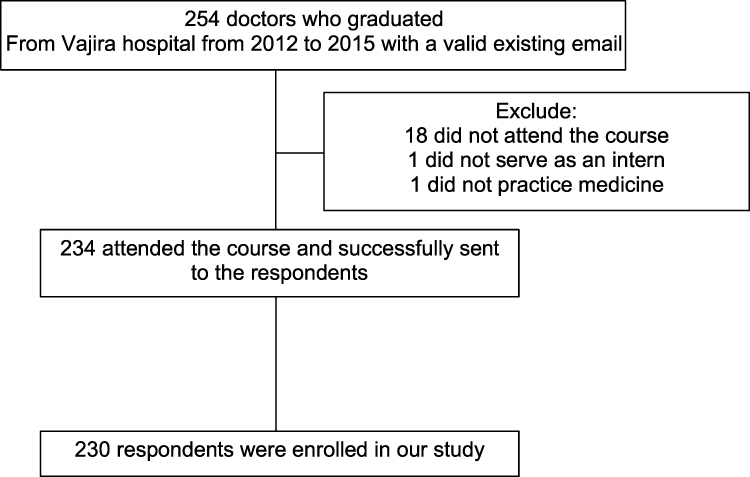 |
Figure 1 Diagram for enrollment of participants. |
Demographics and Current Workplace (Table 1)
According to the size of the hospital; the size of regional hospitals varies from 150 beds to more than 1,000 beds, while general hospitals have capacities of at least 150 beds, and community hospitals have fewer capacities to varying from 10 to 120 beds. The majority (62%) of the respondents were interns at the time of the study, and one-third (34%) of those were residents. Thirty-five percent (80/230) of the respondents worked in university-based medical centers and twenty-four percent (55/230) of the respondents worked in community hospitals. Ninety-nine percent (227/230) of the respondents practiced experience in EDs and ninety-seven percent (222/230) of the respondents were the doctors on the frontlines responsible for taking care of emergency patients.
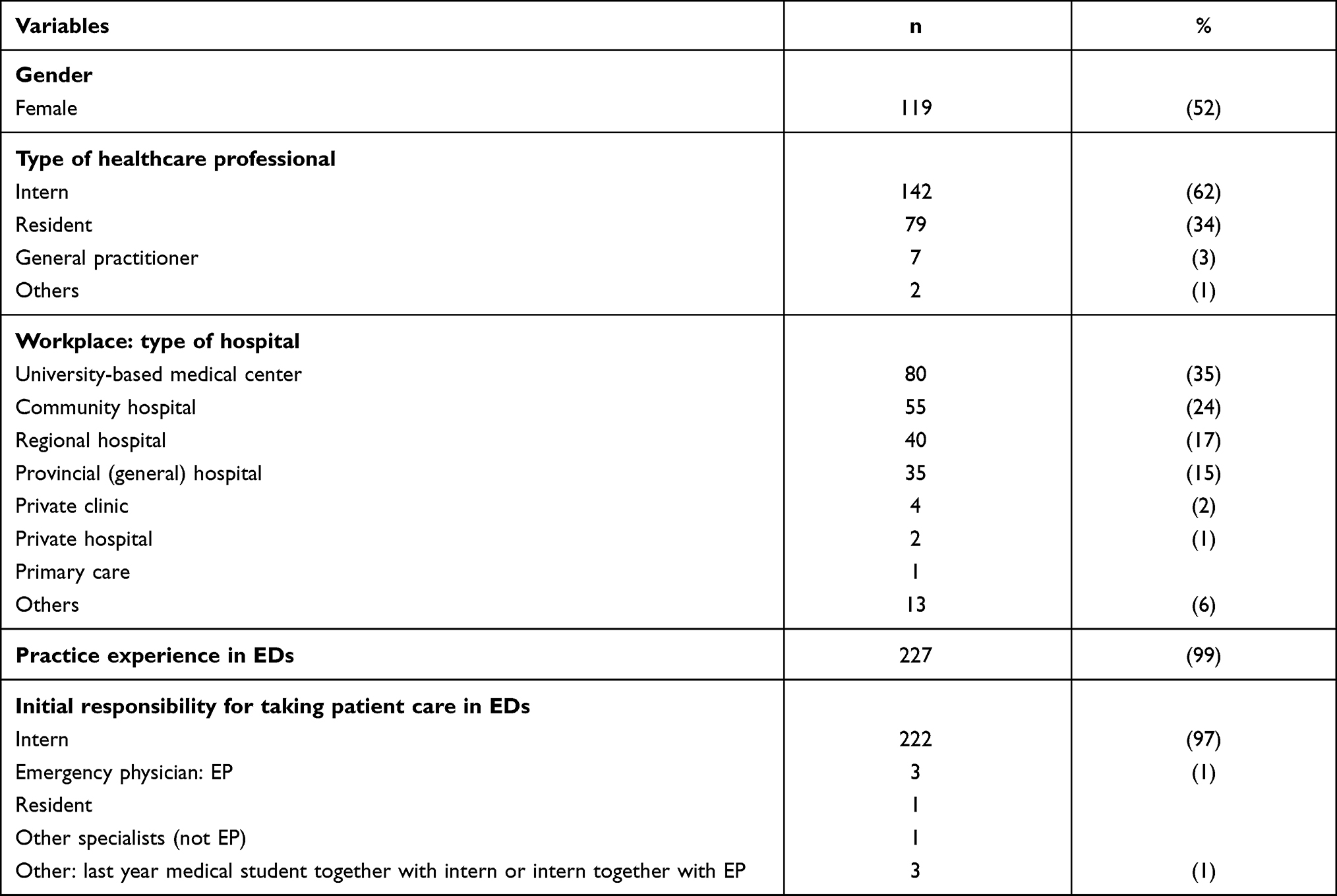 |
Table 1 Demographics of Survey Respondents, n = 230 |
Survey of the Presence or Absence of Ultrasound in Respondents’ Hospitals (Table 2)
Ninety-three percent (213/230) of the respondents’ hospitals had ultrasound machines in ED. Sixty-five percent of respondents’ hospitals (150/230) had the ultrasound machine located in the labor room.
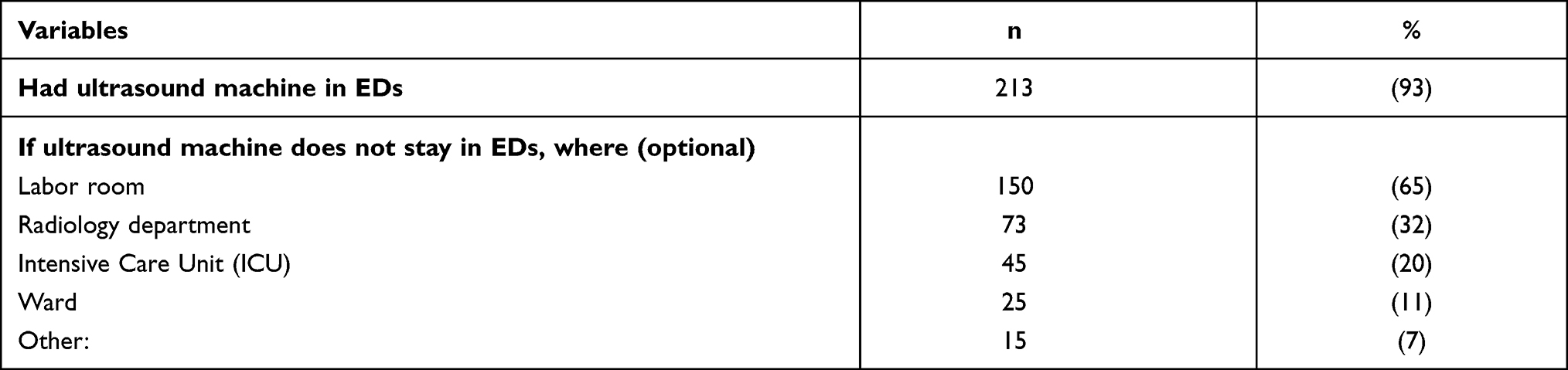 |
Table 2 Survey of the Presence or Absence of Ultrasound Machines in Hospitals of Respondents, n = 230 |
Experience in Ultrasound and Frequency of POCUS Use in ED Patient Care (Table 3)
We asked interns to rate the frequency of use on the 4-point scale of POCUS according to different patients’ categories [obstetrics/gynecology, trauma, cardiopulmonary resuscitation (CPR), internal medicine, surgery]. They reported that POCUS use was greatest for obstetrics/gynecology and trauma cases. Forty-eight and forty-three percent of respondents reported using POCUS often or every day. Whereas, POCUS use for surgical diseases, medical conditions, and cardiac arrest causes were rarely or occasionally performed.
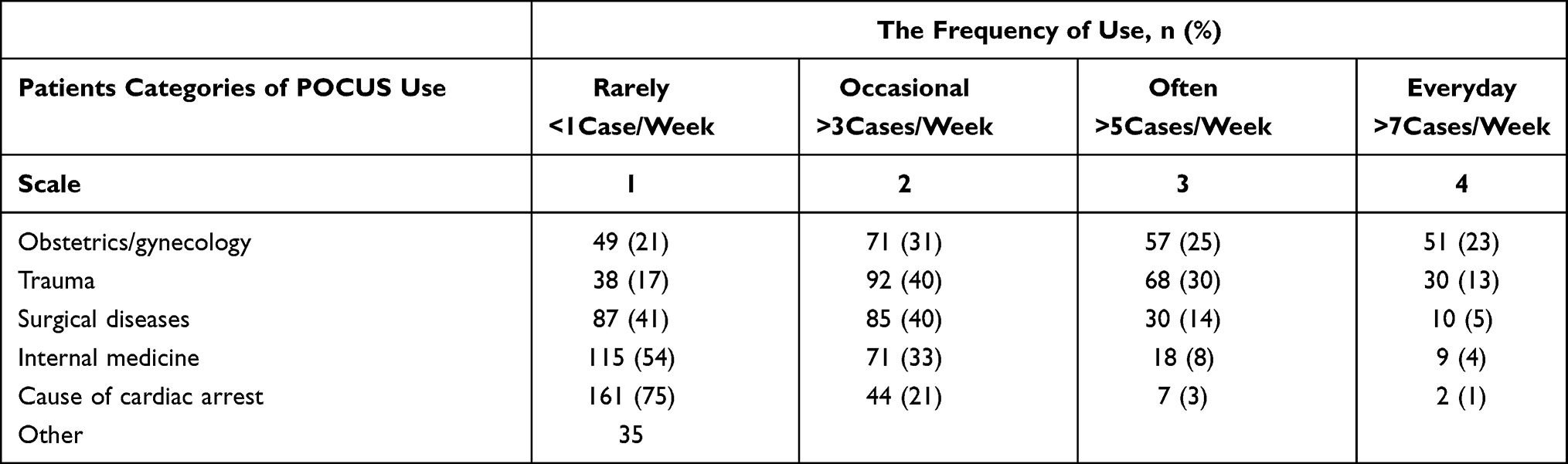 |
Table 3 The Frequency of POCUS Use in Taking Care of ED Patients |
Level of Confidence in eFAST Use (Table 4)
Fifty-five percent of respondents reported that their confidence in eFAST assessment improved after the course (rating of 4 or 5-points on the Likert scale).
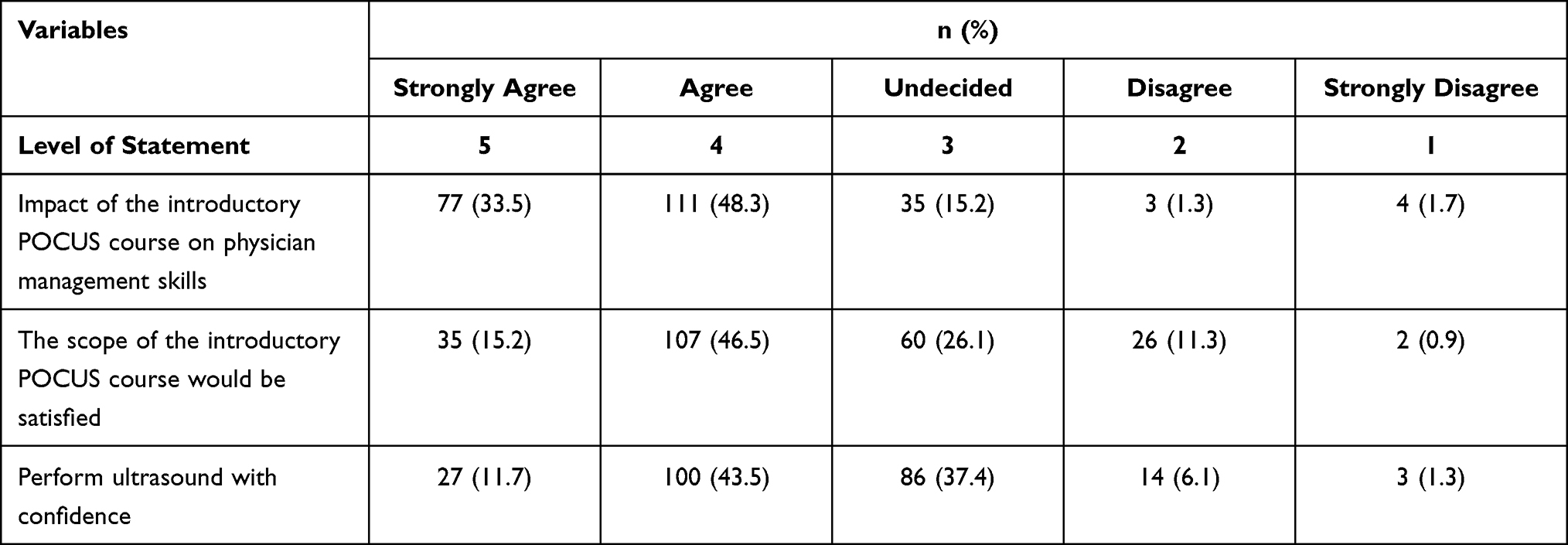 |
Table 4 Level of Confidence in eFAST Assessed by Themselves and Emergency Patient Care Impact of the Introductory POCUS Course |
Perceptions of the Introductory POCUS Course and Recommendations (Tables 4 and 5)
All respondents thought that POCUS was important. Besides, 96% of respondents thought that the introductory POCUS course during EM rotations aides them during their internship, and 81.8% of respondents felt it had a meaningful impact on their emergency medical management skills. Moreover, 61.7% of respondents were satisfied with the scope of the course (rated as 4 or 5 on the 5- point Likert scale). Most of the respondents expected to learn more about the cardiovascular system such as echocardiography (84.5%), obstetric and gynecological conditions (63.9%), abdominal ultrasound (56.8%), and lung ultrasound (46.5%) and they thought the course time should be extended and include more emergency conditions.
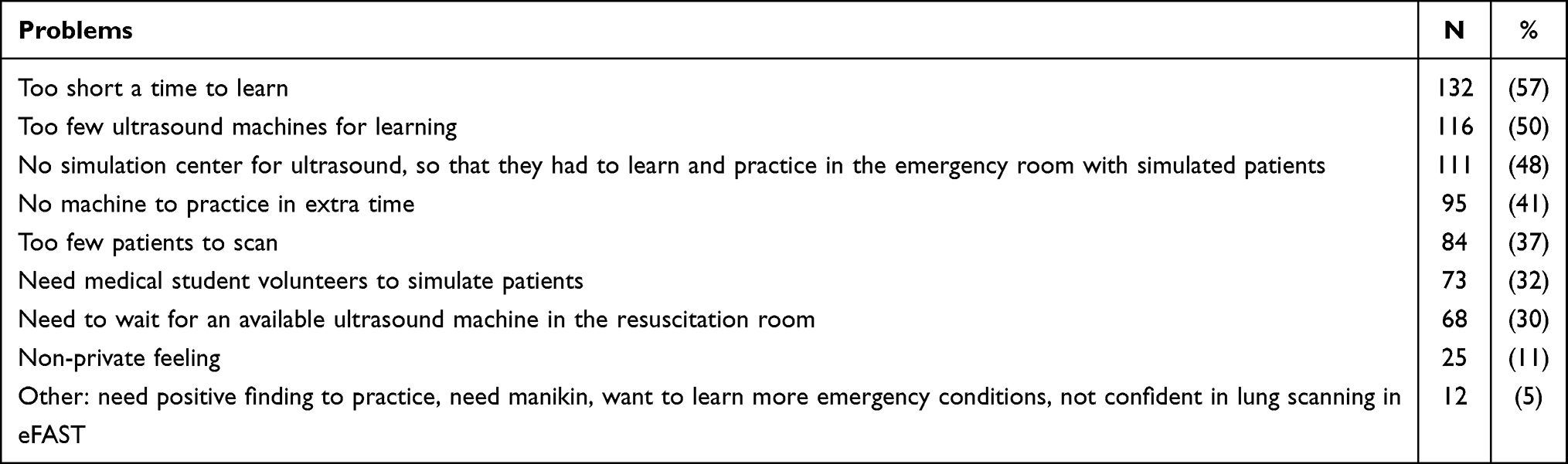 |
Table 5 Further Suggestions of the Introductory POCUS Course |
Further Suggestions During the Course and Areas for Improvement
There were several areas of improvement identified by course respondents (Table 5). Respondents felt that the course was too short to learn ultrasound (57%), there were too few ultrasound machines for learning (50%) and there was not a simulation center for an ultrasound so that they had to learn and practice how to perform ultrasound in the emergency room with simulated patients (48%). Moreover, some of them were not confident in lung ultrasounds, which was a part of the eFAST exam.
Discussion
This study was the first ultrasound training study at the undergraduate level in Thailand, a middle-income country to evaluate the POCUS course training program at the undergraduate medical education level.
Impact of Ultrasound Course on Physician Comfort in the Emergency Department
Our study showed that 96% of respondents thought that the introductory POCUS course during EM rotations had a meaningful impact on their physician management skills in ED. Similar to prior undergraduate-level ultrasound studies, our learners felt confident in performing eFAST by themselves.7 The feedback survey showed how confidence after ultrasound training and their need for formal ultrasound accreditation and curriculum.
Ultrasound Machines and Training Process
Despite maldistribution and a lack of healthcare workers and resources in Thai medical systems,10,11 most hospitals have ultrasound machines in EDs (93%). The limitation to their use is the lack of familiarity and comfort in POCUS by physicians. To address this gap, it is critical to teach medical students how to perform ultrasounds before they graduate because there is no formal ultrasound national curriculum at the undergraduate medical education level. Medical students were eager to learn about and improve their ultrasound skills.
Recommendations and Extending the Course
The survey indicated that POCUS use in EDs was greatest among obstetrics/gynecology and trauma cases. We found that only 55% of respondents feel very confident in their eFAST performance; nevertheless, 45% of them still needed more confidence, and some of them did not feel confident in lung ultrasound, which was a part of eFAST. So the future improvement of our undergraduate ultrasound curriculum would be comprised of pre/post-rotation assessment, lecture, more hands-on time or experience by expanding course length, scenario-based simulation teaching, and objective structured clinical examination (OSCE), as well as an online resource available for medical students to review at any time or developing a longitudinal undergraduate medical curriculum which the longitudinal ultrasound curriculum have been successfully incorporated into undergraduate education in some institutes in the United States.12–16 It appears that medical students need to be able to perform and learn how to improve skills in the use of introductory POCUS before graduation and should become familiar with an emergency ultrasound application such as the eFAST, and expose to additional emergency ultrasound exams throughout their clerkship to increase their ability and confidence as interns, especially those working in underserved areas with limited access to EM residents or EM-trained attending physicians. In addition to the current applications taught in the course, the scope should be expanded to include ultrasound-guided resuscitation and focused lung ultrasound to aid in the diagnosis of pulmonary edema or pneumonia, especially in patients with suspected COVID-19 infection because the physical examination may be limited by the use of the personal protective equipment.
The Limited Supply of EM Specialist in EDs
In the United States, there are 14.9 EM physicians per 100,000 population.17 In Thailand, there are 1.15 EM physicians per 100,000 populations; there is a limited supply of EM-trained physicians to meet the demands of emergency care. Similar to other countries, interns or general practitioners instead of trained EM physicians are often responsible for the delivery of emergency medical care.18–20 The survey data indicated that during their internship almost all of the respondents were frontline ED providers. This shortage of trained EM specialists is faced by many other low and middle-resource environments and even rural hospitals in the United States.20–22 It is imperative that we must be training medical students to meet the needs of emergency patients. POCUS is a tool that improves the timely diagnosis and management of critically ill patients in low-resource or low-income countries.4,21 Enhancing ultrasound medical education through courses like ours is crucial for improving emergency care delivery in underserved communities.
Limitations
There were several limitations of the study. First, it is the nature of surveys that there may be some recall bias and uncertainty over data validity. The survey itself paid attention only to the interns’ ultrasound experience, and confidence in performing ultrasound during the years of internship and the perception of the undergraduate POCUS course, but not the knowledge of ultrasound since they passed the post-rotation assessment, as well as we did not evaluate the quality assurance. Moreover, for the experience, the survey assessed only the frequency of POCUS use, not the frequency of how often cases that could benefit from the ultrasound are seen. According to, there is no formal consensus National Curriculum exists for training POCUS in Thailand, so we developed our introductory POCUS course and would like to find out their practical US application required or needed.
Conclusions
Graduates of the POCUS course have a positive perception of the course and self-reported that it has dramatically improved their clinical practice as novice physicians. We recommend that an introductory POCUS course be formally incorporated into the EM medical student curriculum and National medical competency criteria. Future areas of direction include increasing the scope of US application, providing hands-on ultrasound practice, measuring the impact this introductory course has on patient outcomes, and assessing the quality assurance of POCUS care following the course to aid interns who may not have the benefit of supervising residents or attending EM physicians readily available while working in the emergency department.
Abbreviations
POCUS, point-of-care ultrasonography; EM, emergency medicine; EDs, emergency departments; eFAST, extended Focused Assessment with Sonography in Trauma (eFAST); FAST, Focused Assessment with Sonography in Trauma; GDP, gross domestic product; EPs, emergency physicians; ACEP, American College of Emergency Physicians.
Data Sharing Statement
Data sharing does not applicable to this article as no datasets were generated or analyzed during the current study.
Ethics Approval and Informed Consent
This study was approved by the institutional review board (IRB) of the Faculty of Medicine Vajira Hospital, Bangkok, Thailand: COA 80/2559. The participants were informed about the purpose of the study and electronic consent was obtained before responding to the survey. They had the right to refuse to participate without penalty and stop the survey at any time. The ethics committee approved this consent process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Vajira Hospital Research Foundation Grant for Research Development, grant number CAO 80/2559. The funder had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report that they have no conflicts of interest in this work.
References
1. Link MS, Berkow LC, Kudenchuk PJ; American Heart Association. Part 7: adult advanced cardiovascular life support 2015 American heart association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132:S444–S464. doi:10.1161/CIR.0000000000000261
2. Lichtenstein DA. BLUE-protocol and FALLS-protocol two applications of lung ultrasound in the critically ill. Chest. 2015;147(6):1659–1670. doi:10.1378/chest.14-1313
3. Perera P, Mailhot T, Riley D, Mandavia MD. The RUSH exam 2012: rapid ultrasound in shock in the evaluation of the critically ill patient. Ultrasound Clin. 2012;7(2):255–278. doi:10.1016/j.cult.2011.12.010
4. Becker TK, Tafoya CA, Osei-Ampofo M, et al. Cardiopulmonary ultrasound for critically ill adults improves diagnostic accuracy in a resource-limited setting: the AFRICA trial. Trop Med Int Heal. 2017;22(12):1599–1608. doi:10.1111/tmi.12992
5. American College of Emergency Physicians. Policy Statement Ultrasound Guidelines: Emergency, Point-Of-Care, and Clinical Ultrasound Guidelines in Medicine. The ACEP Board of Directors, editor. Dallas, Texas; 2016:2–46.
6. American College of Surgeons Committee on Trauma. Advanced Trauma Life Support Student Course Manual.
7. Gogalniceanu P, Sheena Y, Kashef E, et al. Is basic emergency ultrasound training feasible as part of standard undergraduate medical education? J Surg Educ. 2010;67(3):152–156. doi:10.1016/j.jsurg.2010.02.008
8. Favot M, Courage C, Mantouffel J, Amponsah D. Ultrasound training in the emergency medicine clerkship. West J Emerg Med. 2015;16(6):938–942. doi:10.5811/westjem.2015.9.27290
9. Connolly K, Beier L, Langdorf M, Anderson C, Fox J. Ultrafest: a novel approach to ultrasound in medical education leads to improvement in written and clinical examinations. West J Emerg Med. 2015;16(1):143–148. doi:10.5811/westjem.2014.11.23746
10. World Health Organization’s global health workforce statistics, OECD supplemented by country data. Physicians (per 1,000 people). 2017.
11. Witthayapipopsakul W, Cetthakrikul N, Suphanchaimat R, Noree T, Sawaengdee K. Equity of health workforce distribution in Thailand: an implication of concentration index. Risk Manag Healthc Policy. 2019;12:13–22. doi:10.2147/RMHP.S181174
12. Wilson SP, Mefford JM, Lahham S, et al. Implementation of a 4-year point-of-care ultrasound curriculum in a liaison committee on medical education-accredited US medical school. J Ultrasound Med. 2017;36(2):321–325. doi:10.7863/ultra.16.03068
13. Kelm DJ, Ratelle JT, Azeem N, et al. Longitudinal ultrasound curriculum improves long-term retention among internal medicine residents. J Grad Med Educ. 2015;7(3):454–457. doi:10.4300/JGME-14-00284.1
14. Minardi J, Ressetar H, Foreman T, et al. Longitudinal ultrasound curriculum incorporation at West Virginia university school of medicine: a description and graduating students’ perceptions. J Ultrasound Med. 2019;38(1):63–72. doi:10.1002/jum.14662
15. Nelson BP, Hojsak J, Dei Rossi E, Karani R, Narula J. Seeing is believing: evaluating a point-of-care ultrasound curriculum for 1st-year medical students. Teach Learn Med. 2017;29(1):85–92. doi:10.1080/10401334.2016.1172012
16. Bahner DP, Goldman E, Way D, Royall NA, Liu YT. The state of ultrasound education in U.S. medical schools. Acad Med. 2014;89(12):1681–1686. doi:10.1097/ACM.0000000000000414
17. Bennett CL, Sullivan AF, Ginde AA, et al. National study of the emergency physician workforce, 2020. Ann Emerg Med. 2020;76(6):695–708. doi:10.1016/j.annemergmed.2020.06.039
18. Cooper A, Davies F, Edwards M, et al. The impact of general practitioners working in or alongside emergency departments: a rapid realist review. BMJ Open. 2019;9(4):1–11. doi:10.1136/bmjopen-2018-024501
19. Denny SP, Minteer WB, Fenning RTH, et al. Ultrasound curriculum taught by first-year medical students: a four-year experience in Tanzania. World J Emerg Med. 2018;9(1):33–40. doi:10.5847/wjem.j.1920-8642.2018.01.005
20. Kannan VC, Tenner A, Sawe HR, et al. Emergency care systems in Africa: a focus on quality. Afr J Emerg Med. 2020;10:S65–72. doi:10.1016/j.afjem.2020.04.010
21. Fitz D. The Latin American school of medicine today. Monthly Review. March, 2011. Available from: https://monthlyreview.org/2011/03/01/the-latin-american-school-of-medicine-today/.
22. Arnoff S Rural emergency departments strained by physician shortages. UW medicine/ Newsroom. June 14, 2018. Available from: https://newsroom.uw.edu/news/rural-emergency-departments-strained-physician-shortages.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.