")
Back to Journals » Infection and Drug Resistance » Volume 14
Perceived Risk of COVID-19 and Related Factors Among University Students in Ethiopia During School Reopening
Authors Tadese M , Haile AB , Moltot T, Silesh M
Received 15 January 2021
Accepted for publication 26 February 2021
Published 11 March 2021 Volume 2021:14 Pages 953—961
DOI https://doi.org/10.2147/IDR.S302126
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Mesfin Tadese, Assalif Beyene Haile, Tebabere Moltot, Mulualem Silesh
Department of Midwifery, College of Health Sciences, Debre Berhan University, Debre Berhan, Ethiopia
Correspondence: Mesfin Tadese
Department of Midwifery, College of Health Sciences, Debre Berhan University, PO. Box: 445, Debre Berhan, Ethiopia
Tel +25915839921
Email [email protected]
Background: The novel coronavirus disease 2019 (COVID-19) has posed a great threat to the public. University students living in school compound with groups and sharing a common cafeteria are more susceptible to contract and spread the virus. Risk perception multiplies fear and anxiety that triggers precautionary action. However, research is scant in this particular field.
Objective: To assess the perceived risk of COVID-19 and its associated factors among University Students in Northeast Ethiopia during school reopening.
Methods: Institution-based cross-sectional study was conducted among 682 Debre Berhan University students from December 1– 15, 2020, when students just get back to school. Data was collected using a structured and pre-tested questionnaire. A multistage sampling technique was used to select study subjects. Data were cleaned and entered into Epi-Data version 4.6 and exported to SPSS version 25 software for analysis. Descriptive statistics, bivariable and multivariable logistic regression analysis were run to summarize the results.
Results: The overall perceived risk of COVID-19 was 296 (43.4%), 95% CI (39.4– 47.4). Age (AOR (CI) =3.27 (1.87– 5.71), open relationship (AOR (CI) =3.17 (1.73– 5.79), fathers’ education (AOR (CI) =2.29 (1.31– 4.02), having diabetes (AOR (CI) =2.64 (1.15– 6.07), and information source from ministry of health (MOH) (AOR (CI) =1.87 (1.27– 2.75) had significantly high-risk perception. However, students who use Facebook (AOR (CI) =0.57 (0.39– 0.82) and Websites/articles (AOR (CI) =0.14 (0.06– 0.34) had significantly low-risk perception. Television (59.8%) and Telegram (66.6%) were the primary sources of information, while the World Health Organization (68.3%) was the most trusted source of information.
Conclusion: University students perceived a low risk towards COVID-19 pandemics at the time of school resumption. It was influenced by students’ demographic characteristics, co-morbidities, social media, and information sources. The Ministry of Health and Ministry of Education should properly promote risk communication among university students.
Keywords: COVID-19, risk perception, factors, university students, Ethiopia
Introduction
Coronavirus disease 2019 (COVID-19) is a highly infectious disease caused by the new coronavirus called SARS-CoV-2, which is a life-threatening respiratory pathogen.1 The virus was first detected from cases in Wuhan, the People’s Republic of China. It is believed to be a result of an animal to human transmission and has close genetic similarity to bat coronaviruses, suggesting it emerged from a bat-borne virus.2 The most common symptoms of the virus are fever (above 38 °C), dry cough, and fatigue. The average incubation period is 5–6 days but can range from 1–14 days. The virus can infect peoples of all ages. However, older people aged 60 and over, and those with chronic diseases like asthma, hypertension, heart and lung problems, diabetes, obesity, or cancer, are at higher risk of developing severe illness.1 The virus primarily spreads through respiratory droplets or secretions generated when an infected person coughs, sneezes, talks, or sings.3
As the number of deaths from the virus rises globally, it is crucial to understand the perceived risk of the infection. Risk perception is the people’s subjective evaluation and/or judgment of hazards that they might be exposed to, regarding the severity, characteristics, and management. It is influenced by individual, social, cultural, and contextual factors, and they are based on experiences, beliefs, attitudes, judgments, misconceptions, and feelings.4 Risk perception multiplies fear and anxiety and triggers precautionary action. People with high-risk perception tend to adopt protective health behavior and this reduces the possibility of infections.5,6
Currently, in Ethiopia, the higher education system has planned to reopen Colleges and Universities. However, there is no risk-free way to reopen. Without adequate prophylactic vaccines and effective treatment for cases, and with a highly contagious virus, bringing together students in traditional ways have a shocking consequence. Besides, communities had a low perceived risk of getting the virus. One study has suggested that only 23% of communities in Ethiopia had a high-risk perception towards COVID-19.7 As of 22 February 2021, in Ethiopia, COVID-19 has caused 151,857 confirmed cases and 2,271 deaths.8
University students are one of the most dynamic groups with strong mobility and socialization. They are young, healthy, and often show mild symptoms after being infected, which can be contagious and easily spread from them to others. Besides, the outbreak of the COVID-19 infection coincides with the time of massive transportation during school re-entry and the Christmas holiday. Further, without adequate personal protective equipment, medical/health students posted inwards may have close contact with affected people and are supposed to be at risk of getting infected. One study in Ethiopia reported that only 31%, 27.4%, 15.9%, 14.5%, and 14.2% of health care providers had access to gloves, facemask, goggles, shoes, and apron respectively in hospitals.9 To limit and terminate the spread of the virus, students should adhere to the control measures, which are largely affected by their risk perceptions. So, attention needs to be given to the risk perception of university students.
To mitigate COVID-19 transmission while continuing the teaching-learning process, Debre Berhan University has set down prevention measures to be strictly adhered by the staff and the students. In-person classroom instruction shall not exceed 30 persons and should be limited to 40 minutes session. All students and staff should maintain 1 to 1.5 meters of physical distance in the library, laboratory, workshops, or other instructional settings while social distancing between the instructor and the students in the classroom should be 1.5 to 2 meters. Acceptable face shield covering both the mouth and nose should be worn at all times in public spaces, both in classrooms and outside classrooms. All students and staff are required to wash hands with soap and running water for at least 20 seconds or use hand sanitizer with 70%+ alcohol when entering and leaving classrooms, laboratories, workshops, or any other shared spaces. Staff and students with COVID-19 symptoms shall stay in their place of residence and report or seek medical attention. Classrooms shall be ventilated for at least 15 minutes after the end of each session. Besides, classrooms shall be cleaned and disinfected at least twice a day and a minimum of one hour of ventilation after disinfection. Further, offices, libraries, laboratories, and workshops shall be cleaned and ventilated regularly for at least an hour a day. Group activities such as team-based sports or games are prohibited.
Lack of adequate risk perception and preventive behavior among students can make them underestimate the situation, reduce fear and anxiety, and may interrupt the appropriate prevention measures. A basic study of university student’s risk perception is necessary since COVID-19 continues to spread at an alarming rate. To the best of our knowledge, there is no study on university students’ perceived risk of COVID-19 in Ethiopia. Therefore, this study aimed to determine the level of risk perception towards COVID-19 and its associated factors among Debre Berhan University Students, Northeast Ethiopia.
Methods and Materials
Study Setting, Design, and Period
An institution-based cross-sectional study was conducted among Debre Berhan University (DBU) students from December 1 to 15, 2020, when students just get back to school. Debre Berhan University is found at Debre Berhan town, which is the capital of the North-Shewa Zone located about 130 km North-East of the capital city of Ethiopia. The university had fourteen colleges and 50 departments. By the year 2020/21, the university had a total number of 27,371 students: 17,397 male and 9,974 females. Of these, 11,573 are regular undergraduate and postgraduate students.
Sample Size Determination
The sample size was computed using Open Epi version 3.03 statistical software. The following assumptions were considered: proportion 65%,10 confidence level 95%, level of significance, α=5%, power of the study (1-β), 80%, a margin of error, d = 5%, and design effect, D = 2. By adding a 5% non-response rate, the final sample size was 713.
Sampling Technique and Procedure
Study participants were selected from all regular students using a multistage sampling technique. Five colleges were selected using simple random sampling (SRS) and the calculated sample size was distributed to each of the selected colleges using the probability proportional to size (PPS) method. In each of the selected colleges’ departments was selected using SRS. Then, in the selected departments, the required sample size was proportionally allocated based on the total number of students. Finally, from all students of the selected departments, SRS was done to pick the required sample size using a pre-determined sampling frame of all departments.
Inclusion and Exclusion Criteria
Regular Debre Berhan university students of both sexes, and who agreed to participate in the study were included. Those who have a physical disability and not competent to fill the questionnaire were excluded.
Data Collection Tool and Measurements
Properly designed, structured, and self-administered questionnaires were employed to collect data. The questionnaire was prepared based on previous, similar works of literature,11–13 and was modified and validated to fit the local situation and the research objectives.
To determine the risk perception, twelve questions with three alternative options were applied. It was measured by two dimensions: perceived susceptibility and perceived severity dimension. Susceptibility was measured by asking the perceived risk/chance of acquiring the disease. Whereas perceived severity was assessed by asking about the likelihood of managing daily activities if get infected, the chance of developing mild illness/symptoms, and the chance of feeling less anxiety and fear. One point was assigned for those who responded “Yes” and zero for (“Not sure”) or (“No”). Higher values indicate higher risk perception. Based on the mean score of risk perception, students who scored above the mean were considered as High-risk and those who scored mean or below were considered Low-risk.11 The Cronbach’s alpha coefficients of the items were 0.74 and this demonstrated a satisfactory internal consistency.7
Data Quality Control
A pre-test was conducted on 5% of the samples among Victory College students. The face and content validity of the questionnaire was checked by a reproductive health expert. Necessary amendments were made following the result of the pre-test and expert opinion. Two supervisors and four facilitators participated in the data collection. The questionnaire was first prepared in English and translated into the Amharic language then back-translated to English to check its consistency. One-day training was given for supervisors and facilitators regarding the purpose, methodologies, and data collection tools. The supervisors review and check the day-to-day activities of the facilitators regarding the completeness, clarity, and proper coding of the responses. Besides, there was continuous supervision to control the data collection procedure by the principal investigator.
Data Management and Analysis
After checking the completeness and consistency of each questioner, the collected data were coded and entered into Epi-data software version 4.6 and then exported to SPSS version 25 statistical package for analysis. Descriptive statistics were done to quantify the risk perception and baseline characteristics of participants. Bivariable and multivariable logistic regression analysis were performed to identify the independent predictors of the outcome variable. Variables with a p-value of ≤0.25 in the bivariable logistic regression analysis were a candidate for the multivariable logistic regression analysis model. The strength of association was interpreted using an adjusted odds ratio (AOR) with a 95% confidence interval and the Hosmer-Lemeshow goodness-of-fit was applied to test for model fitness. The significance level was declared at a p-value of ≤0.05.
Ethical Consideration
Ethical clearance was obtained from the Institutional Review Board (IRB) of Debre Berhan University, College of Medicine, and Health Science (Ref. No: P0007/20). Besides, a formal support letter was written to selected colleges and/or departments to inform them about the study. After the data collectors explained the purpose, procedures, potential risks, and benefits of the study, informed consent was obtained from the study participants. The data was kept confidential and anonymous and was conducted following the declaration of Helsinki ethical principles.
Results
Characteristics of Participants
A total of 682 participants were involved in the study, making a 95.6% response rate. The age of participants ranged from 18–40 years with a mean age of 23.35±3.46 (SD) years. Of the total participants, 296 (43.4%) were females, 534 (78.3%) were single, and 570 (83.6) are undergraduate students (Table 1).
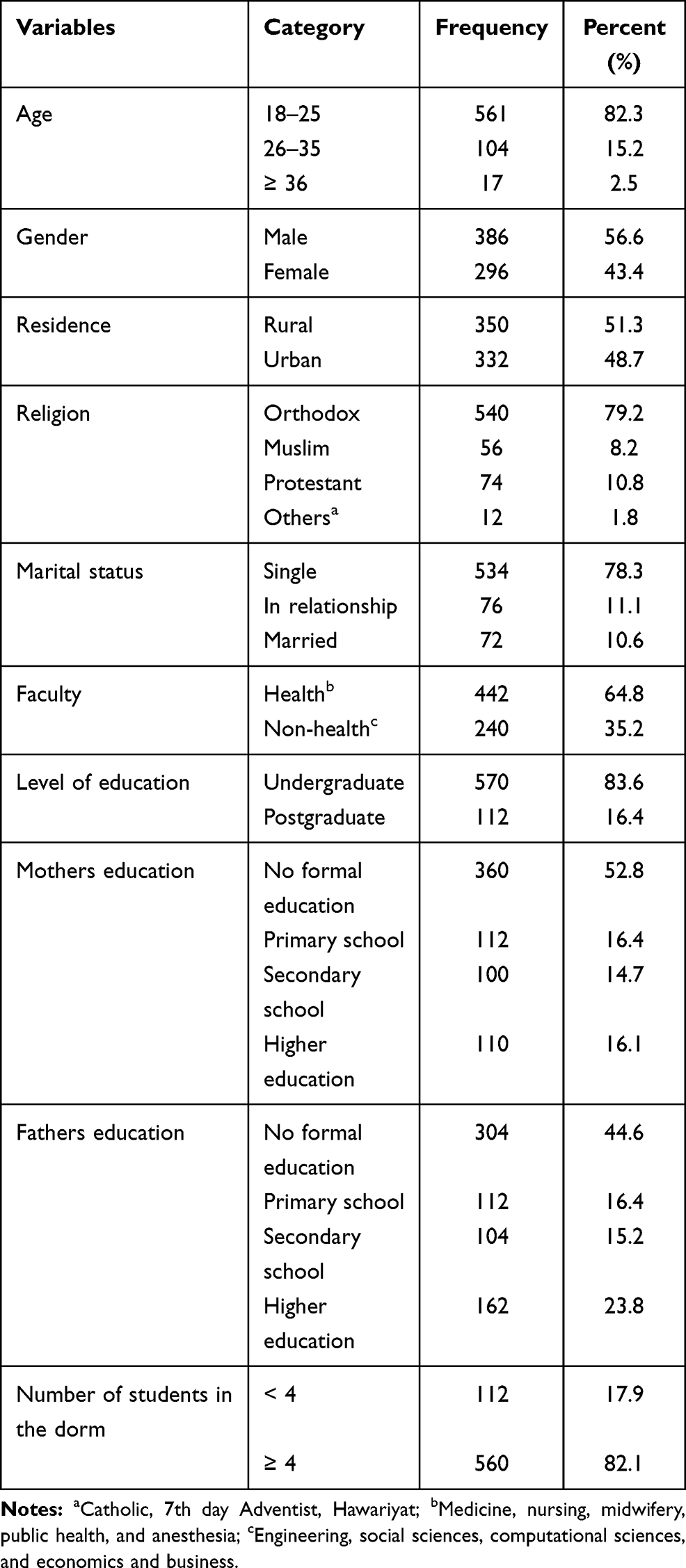 |
Table 1 Characteristics of Study Participants, 2020 (n=682) |
Perceived Risk of COVID-19
About half of students (50.1%) think that their health was severely affected if they get infected with COVID-19. One-third (33.1%) of them will not go to the hospital even if they get sick with another disease because of the risk of COVID-19. Besides, 46.3% of students afraid to contact peoples who just returned from abroad. The overall high perceived risk of COVID-19 among students was found to be 43.4% (N=296), 95% CI (39.4–47.4), and the mean cumulative score of perceived risk was 5.1±2.92 (Table 2).
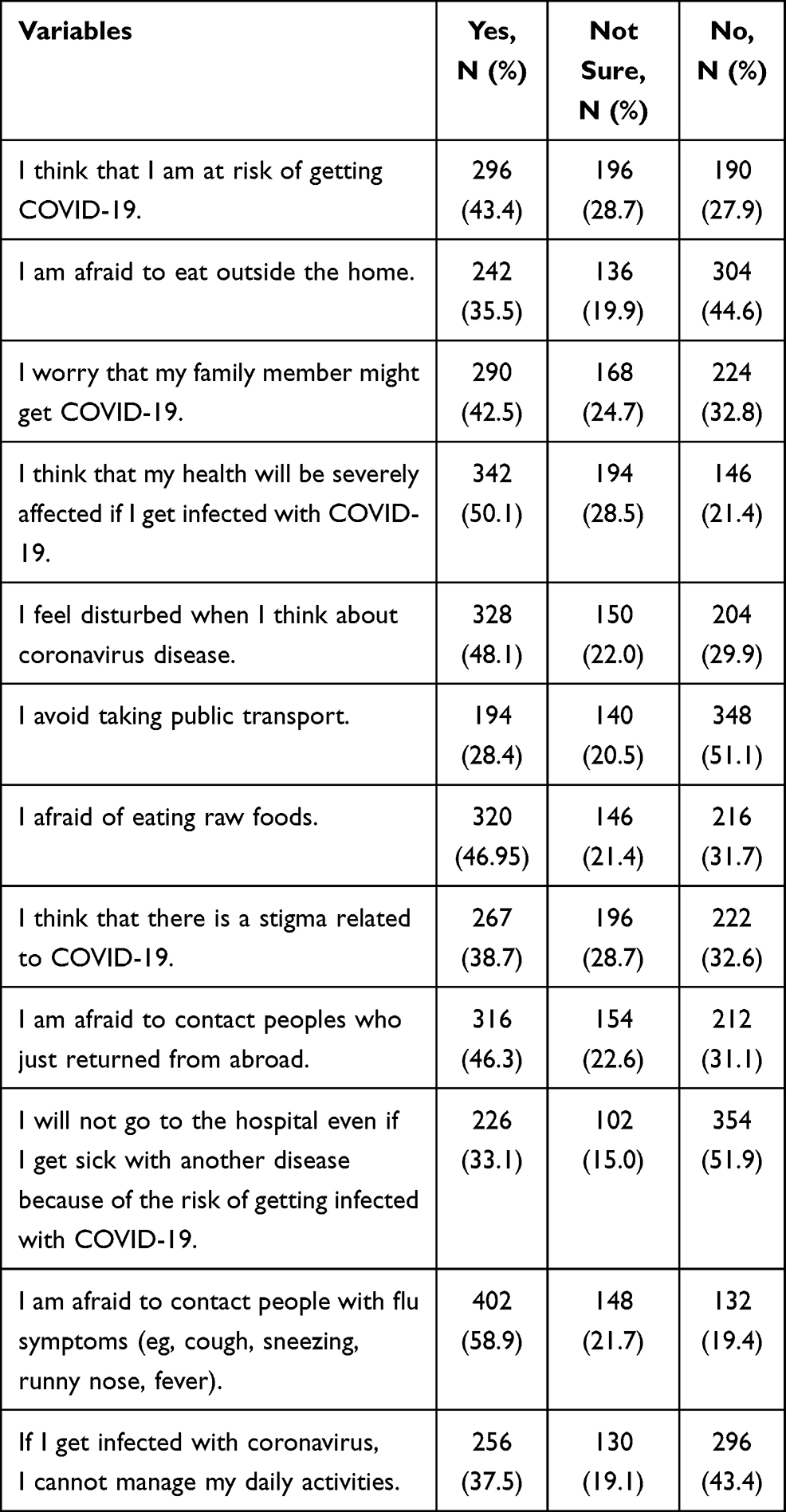 |
Table 2 Perceived Risk of COVID-19 Among DBU Students, 2020 |
History of COVID-19 and Chronic Disease
Regarding chronic illnesses, 4.7% of students had diabetes, and 5.9% had respiratory disease. About 27.3% of students had a history of COVID-19 infection, while 14.4% of them had families/friends tested positive for COVID-19 infection (Table 3).
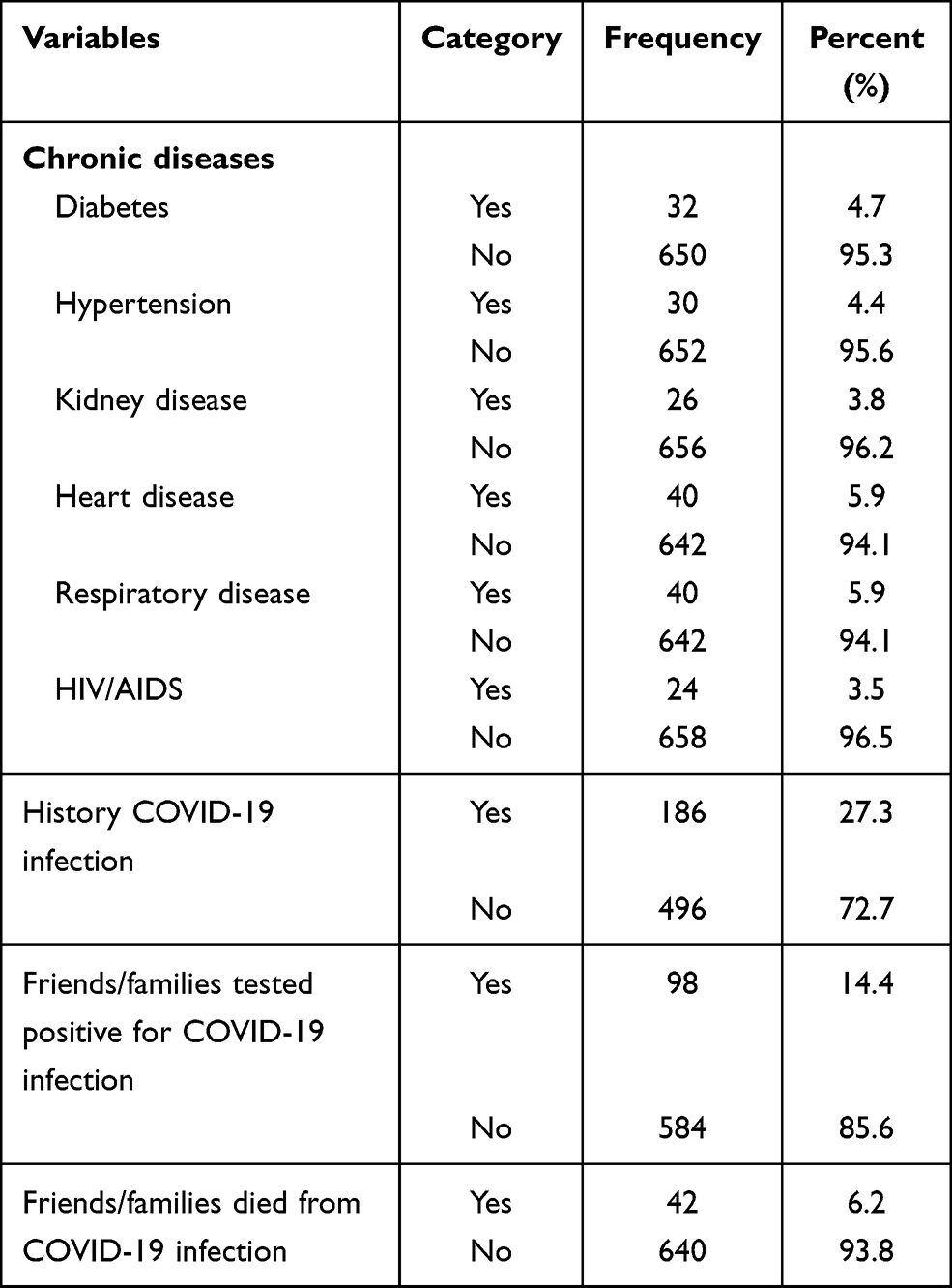 |
Table 3 History of COVID-19 and Chronic Diseases |
Use of Social Media and Trusted Sources of Information
Television (59.8%) and Telegram (66.6%) were the primary sources of COVID-19 information, whereas World Health Organization (68.3%) was the most trusted source of information among university students (Table 4).
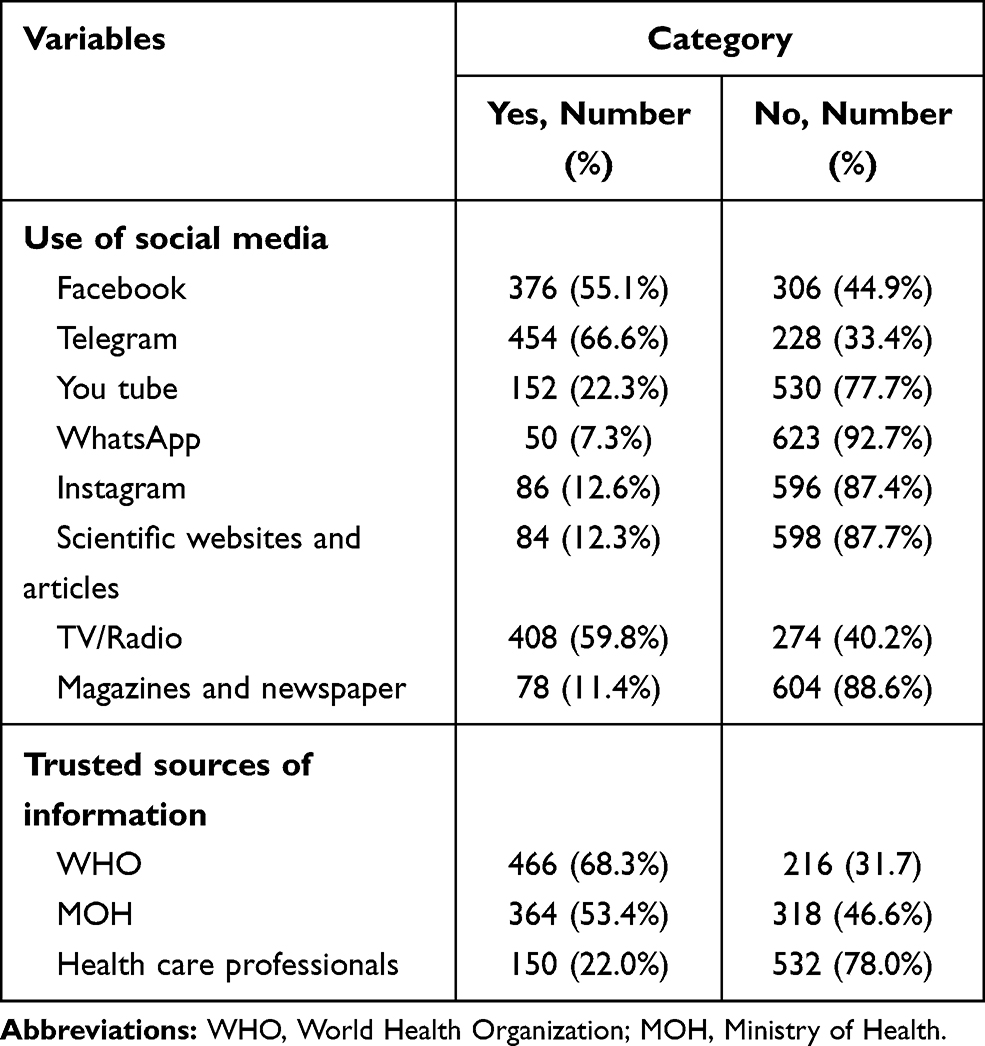 |
Table 4 Use of Social Media and Trusted Sources of Information, 2020 |
Factors Associated with the High Perceived Risk of COVID-19
In the multivariable logistic regression analysis model, factors including age, residence, faculty, marital status, parents’ education, having diabetes, history of COVID-19 infection, family/friend history of death from the virus, use of social media (Facebook, Telegram, YouTube, Instagram …) and trusted sources of information about COVID-19 (World Health Organization (WHO), Ministry of Health (MOH), Health care professionals) were included.
After controlling for confounders, age, marital status, father’s education, having diabetes, use of social media, and information source from MOH were found to have a statistically significant association with perceived high-risk of COVID-19 infection.
High perceived risk of COVID-19 was three times more prevalent among students aged 26–35 years (AOR (CI) =3.27 (1.87–5.71) and those in an open relationship (AOR (CI) =3.17 (1.73–5.79), and two times more common among students whose fathers had attended primary school (AOR (CI) =2.29 (1.31–4.02), who had diabetes (AOR (CI) =2.64 (1.15–6.07) and who obtain information from MOH (AOR (CI) =1.87 (1.27–2.75). However, there is a less perceived risk of coronavirus infection among students who use Facebook (AOR (CI) =0.57 (0.39–0.82) and Websites/articles (AOR (CI) =0.14 (0.06–0.34) compared to their counterparts (Table 5).
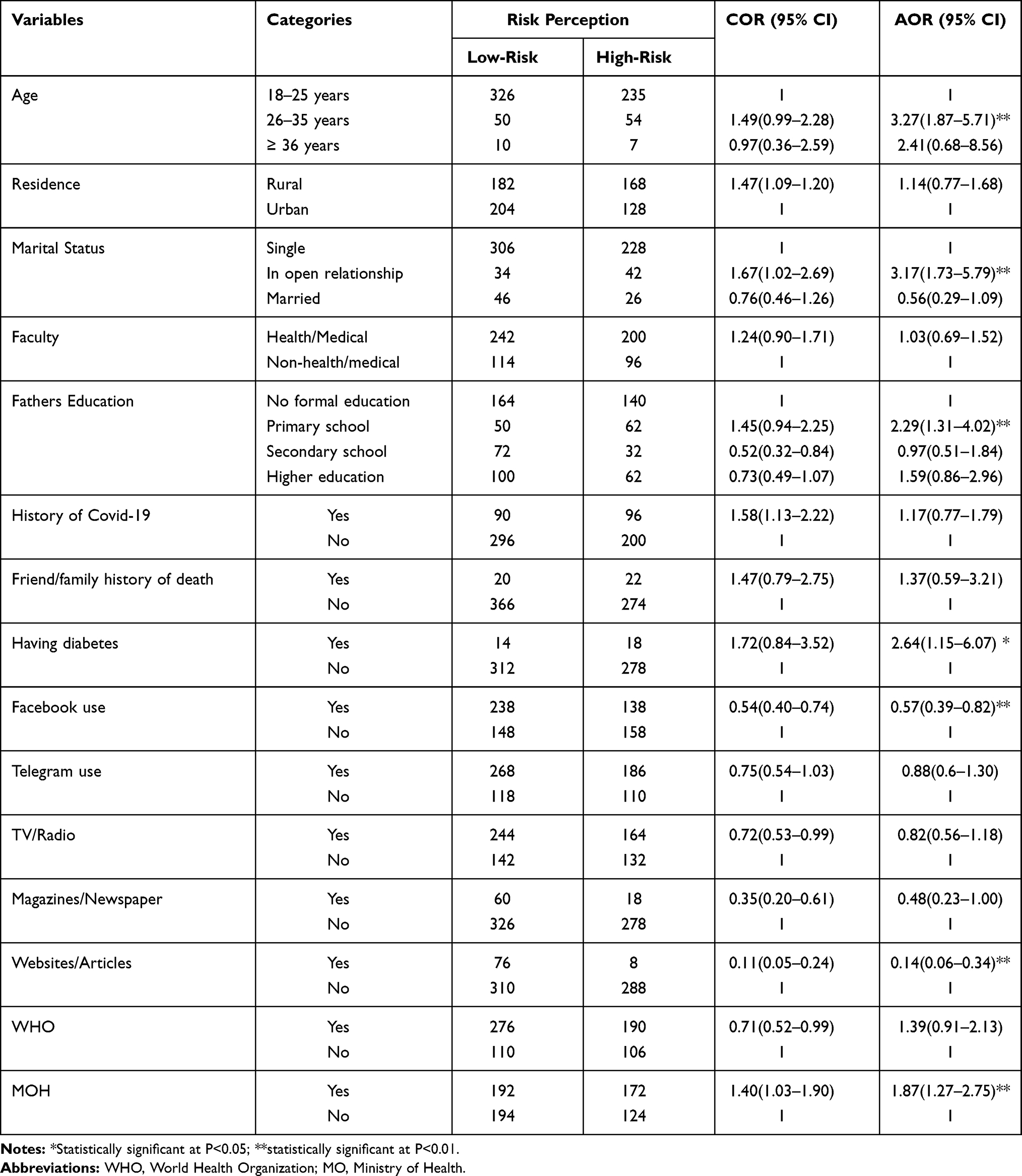 |
Table 5 Factors Associated with Perceived Risk of COVID-19 Among DBU Students, 2020 |
Discussion
In this study, the overall perceived high-risk of COVID-19 was 43.4%, 95% CI (39.4–47.4). Age, marital status, parent’s education, having diabetes, use of social media, and national information source were significant associates of perceived high-risk of COVID-19.
The risk perception in this study was consistent with the previous findings reported in Iran (43.6%).14 However, our result was lower than the study done in Southwest Ethiopia (53.4%),11 Ghana (68.3%),15 and Sierra Leone (75%).16 Moreover, the study found a higher risk perception than 23.11% in Gondar,7 and 7.6% in India.17 This might be due to the differences in the study period, study population, data collection tool and procedures, and level of spread of the virus across countries and communities. Besides, it may account for the variations in socio-demographic backgrounds, access to information, level of knowledge, and risk communication of the local authorities. Risk perception plays a substantial role in disease transmission as healthy individuals are likely to avoid contact with vulnerable groups and sick people are likely to remain at home, which is beneficial for infection control.
Age was found to be a strong determinant factor for the high perceived risk of COVID-19. Students aged 26–35 years were three times more likely to have a high perceived risk compared to those who are younger. This finding was in line with reports from Gondar7 and Southwest Ethiopia.11 Besides, a study in China found that for every one-year increase of age, there is a 4.9% increased perceived risk of COVID-19.18 Even if the virus infects peoples of all ages, the prevalence as well as the risk of death was higher among older people.1 Besides, as age increases, there might be a high level of perceived susceptibility and perceived severity of disease with increased risk perception and the likelihood of adopting prevention measures.
Our result also established a statistically significant association between the educational status of the father and the perceived risk of COVID-19. Students whose fathers had attended primary school were more likely to have a high-risk perception compared to those whose fathers had no formal education (AOR (CI) =2.29 (1.31–4.02). Similarly, another study in Ethiopia established a comparable result.19 This might be due to the parents’ better educational background might have helped in the rational understanding of the pandemics, which might, in turn, influenced a child’s risk perception and precaution measures. Besides, these groups of people may have a better willingness and access to information from various sources. Moreover, low educated people had low knowledge and poor practice of prevention behaviors.14
Risk perception was higher among students in an open relationship compared to those who are single. Similarly, another study in Ethiopia reported higher perceived susceptibility among married respondents.19 Also, a study by18 found that having a marriage/history of marriage was significantly related to a high perceived risk level. The possible reason may be that married individuals might have many family members with various exposure statuses, and just they may feel that one of the family members may acquire and spread to others. In other ways, in an open relationship, one or both partners can engage in romantic or sexual activities outside the relationship, which can increase the risk of contracting the virus.
This study confirmed that having diabetes mellitus (DM) increases the perceived risk of COVID-19. The risk was double among diabetic students. A similar result was obtained from Chongqing, China, where individuals with chronic diseases had a higher level of risk perception.17 Besides, a systematic review, and meta-analysis found that diabetes and hypertension were the two more prevalent co-morbidities among COVID-19 patients.20 The possible explanation might be due to people with pre-existing medical problems like diabetes, asthma, hypertension, heart and lung problems, are prone to infection and progressed to severe illnesses and complications, and hence more perceived risk of infection.1
Students who used social media had a low perceived risk of COVID-2019. A consistent result was reported from Chongqing, China, in which individuals who use WeChat contacts as the main information source perceived a lower risk of infection (OR =0.196).18 This could be due to the students who use social media may get important information and have a better understanding to apply the prevention measures, so that they may have a lower perceived risk of infection. A study in Sierra Leon found that social media was strongly associated with increased knowledge and avoiding crowds.16 This was represented in several studies21,22 that stated those with good knowledge are more likely to adopt precaution measures.
Information source from the national ministry of health was also associated with increased risk perception towards COVID-19. This could be related to the frequent access to information that might have led to good knowledge. The National Health Commission regularly disseminates health counseling, prevention behaviors, the number of screened populations, new cases, and deaths, to ensure the citizen’s safety. In Ambo, Ethiopia, daily access to information reduces the level of poor knowledge by 54.4%.22 In other ways, students with higher knowledge levels have a higher risk perception of COVID-19.23
To mitigate COVID-19 transmission, Debre Berhan University has established general rules and regulations. In-person classroom instruction shall not exceed 30 persons and should be limited to 40 minutes session. All students and staff should maintain physical distance in the classroom, library, laboratory, workshops, or other instructional settings. Face masks covering both the mouth and nose should be worn at all times in public spaces. All students and staff are required to frequently wash hands with soap and water or use hand sanitizer. Staff and students with COVID-19 symptoms shall stay in their place of residence and report or seek medical attention. Classrooms shall be ventilated for at least 15 minutes after the end of each session. Besides, classrooms shall be cleaned and disinfected at least twice a day and a minimum of one hour of ventilation after disinfection. Further, group activities such as team-based sports or games are prohibited. This was in accordance with the WHO infection prevention and control guidance of COVID-19.1 Besides, a similar preparedness plan was established at the University of Minnesota24 and Saudi Arabia.25
Limitation
The findings of this study should be interpreted with the following limitations. First, data were collected using a self-administered questionnaire, which may add social desirability bias. Second, the nature of self-perceived reporting may have resulted in the under/over-reporting of variables. Finally, the cross-sectional nature does not allow to make a causal relationship.
Conclusion and Recommendation
University students perceived a low risk towards COVID-19 pandemics at the time of school resumption. It was influenced by students’ demographic characteristics, co-morbidities, social media, and sources of information. Television and Telegram were the primary sources of information, while the World Health Organization, (WHO) was the most trusted source of information.
The ministry of health should properly promote and monitor risk communication among university students. It may help guide how students should prepare for and respond to the COVID-19 pandemics, and helpful in the information disclosure, designing interventional activities, and policy formulation targeted at improving student’s risk perception. Besides, it can be used as baseline data for future large-scale studies. Further, similar studies with various study designs and measurements should be conducted in different settings for more representative findings.
Abbreviations
AOR, Adjusted Odds Ratio; CI, Confidence Interval; COR, Cruds Odds Ratio; COVID-19, Coronavirus Disease 2019; DBU, Debre Berhan University; MOH, Ministry of Health; SPSS, Statistical Packages for Social Sciences; SRS, Simple Random Sampling; WHO, World Health Organization.
Data Sharing Statement
The datasets are available from the corresponding author and can be presented upon a reasonable request.
Acknowledgment
We are thankful to all the supervisors, data collectors, and study participants for their priceless efforts and valuable information. We also like to thank Debre Berhan University for providing us ethical clearance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Q&As on COVID-19 and related health topics. 2019.
2. Wang LF, Anderson DE. Viruses in bats and potential spillover to animals and humans. Curr Opin Virol. 2019;34:79–89. doi:10.1016/j.coviro.2018.12.007
3. Karia R, Gupta I, Khandait H, Yadav A, Yadav A. COVID-19 and its modes of transmission. SN Comprehensive Clin Med. 2020;1–4.
4. Cori L, Bianchi F, Cadum E, Anthonj C. Risk Perception and COVID-19. Multidisciplinary Digital Publishing Institute; 2020.
5. Dryhurst S, Schneider CR, Kerr J, et al. Risk perceptions of COVID-19 around the world. J Risk Res. 2020;1–13.
6. de Bruin WB, Bennett D. Relationships between initial COVID-19 risk perceptions and protective health behaviors: a national survey. Am J Prev Med. 2020.
7. Kabito GG, Alemayehu M, Mekonnen TH, et al. Community’s perceived high risk of coronavirus infections during early phase of epidemics are significantly influenced by socio-demographic background, in Gondar City, Northwest Ethiopia: a cross-sectional-study. PLoS One. 2020;15(11):e0242654. doi:10.1371/journal.pone.0242654
8. COVID E. Situation update worldwide, as of 10 May 2020. Available from: https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases.
9. Mulu GB, Kebede WM, Worku SA, Mittiku YM, Ayelign B. Preparedness and responses of healthcare providers to combat the spread of COVID-19 among North Shewa Zone Hospitals, Amhara, Ethiopia, 2020. Infect Drug Resist. 2020;13:3171. doi:10.2147/IDR.S265829
10. Tadesse AW, Melese N, Eshetie S, Chane M, Ali A Knowledge, attitude, and practice and associated factors towards COVID-19 among college students in Amhara Region, Ethiopia; a cross-sectional study. 2020.
11. Asefa A, Qanche Q, Hailemariam S, Dhuguma T, Nigussie T. Risk perception towards COVID-19 and its associated factors among waiters in selected towns of Southwest Ethiopia. Risk Manag Healthc Policy. 2020;13:2601. doi:10.2147/RMHP.S276257
12. Hedima EW, Michael SA, David EA. Knowledge and risk perception of the novel coronavirus disease 2019 among adult Nigerians: a cross-sectional study. medRxiv. 2020.
13. Peres D, Monteiro J, Almeida M, Ladeira R. Risk perception of COVID-19 among the Portuguese healthcare professionals and general population. J Hosp Infect. 2020;105(3):434–437. doi:10.1016/j.jhin.2020.05.038
14. Honarvar B, Lankarani KB, Kharmandar A, et al. Knowledge, attitudes, risk perceptions, and practices of adults toward COVID-19: a population and field-based study from Iran. Int J Public Health. 2020;65(6):731–739. doi:10.1007/s00038-020-01406-2
15. Serwaa D, Lamptey E, Appiah AB, Senkyire EK, Ameyaw JK. Knowledge, risk perception and preparedness towards coronavirus disease-2019 (COVID-19) outbreak among Ghanaians: a quick online cross-sectional survey. Pan Afr Med J. 2020;35(44). doi:10.11604/pamj.supp.2020.35.2.22630
16. Sengeh P, Jalloh MB, Webber N, et al. Community knowledge, perceptions and practices around COVID-19 in Sierra Leone: a nationwide, cross-sectional survey. BMJ Open. 2020;10(9):e040328. doi:10.1136/bmjopen-2020-040328
17. Kuang J, Ashraf S, Das U, Bicchieri C. Awareness, risk perception, and stress during the COVID-19 pandemic in communities of Tamil Nadu, India. Int J Environ Res Public Health. 2020;17(19):7177. doi:10.3390/ijerph17197177
18. He S, Chen S, Kong L, Liu W. Analysis of risk perceptions and related factors concerning COVID-19 epidemic in Chongqing, China. J Community Health. 2020;1–8. doi:10.1007/s10900-019-00710-0
19. Asnakew Z, Asrese K, Andualem M. Community risk perception and compliance with preventive measures for COVID-19 pandemic in Ethiopia. Risk Manag Healthc Policy. 2020;13:2887–2897. doi:10.2147/RMHP.S279907
20. Yang J, Zheng Y, Gou X, et al. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: a systematic review and meta-analysis. Int J Infect Dis. 2020;94:91–95. doi:10.1016/j.ijid.2020.03.017
21. Wake AD. Knowledge, attitude, practice, and associated factors regarding the novel coronavirus disease 2019 (COVID-19) pandemic. Infect Drug Resist. 2020;13:3817. doi:10.2147/IDR.S275689
22. Taye GM, Bose L, Beressa TB, et al. COVID-19 knowledge, attitudes, and prevention practices among people with hypertension and diabetes mellitus attending public health facilities in Ambo, Ethiopia. Infect Drug Resist. 2020;13:4203. doi:10.2147/IDR.S283999
23. Ding Y, Du X, Li Q, et al. Risk perception of coronavirus disease 2019 (COVID-19) and its related factors among college students in China during quarantine. PLoS One. 2020;15(8):e0237626. doi:10.1371/journal.pone.0237626
24. Guidance for mitigating COVID-19 at higher education institutions. Available from: https://www.health.state.mn.us/diseases/coronavirus/schools/guideihe.pdf.
25. Acute respiratory infections prevention and control guidelines in universities. Available from: https://covid19.cdc.gov.sa/wp-content/uploads/2020/03/EN_Preventive-measures-of-COVID-19-in-universities.pdf.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.