")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Perceived Barriers and Awareness of Mammography Screening Among Saudi Women Attending Primary Health Centers
Authors Abdel-Salam DM , Mohamed RA , Alyousef HY, Almasoud WA , Alanzi MB, Mubarak AZ, Osman DM
Received 17 August 2020
Accepted for publication 28 September 2020
Published 12 November 2020 Volume 2020:13 Pages 2553—2561
DOI https://doi.org/10.2147/RMHP.S277375
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Doaa M Abdel-Salam,1,2 Rehab A Mohamed,3 Hind Y Alyousef,4 Wahaj A Almasoud,4 Mashael B Alanzi,4 Atheer Z Mubarak,4 Doaa M Osman2
1Family and Community Medicine Department, College of Medicine, Jouf University, Aljouf 42421, Saudi Arabia; 2Public Health and Community Medicine Department, Faculty of Medicine, Assiut University, Assiut 71526, Egypt; 3Family Medicine Department, Faculty of Medicine, Suez Canal University, Ismailia 41522, Egypt; 4College of Medicine, Jouf University, Aljouf 42421, Saudi Arabia
Correspondence: Doaa M Abdel-Salam
Public Health and Community Medicine Department, Faculty of Medicine, Assiut University, Assiut 71526, Egypt
Tel +966537242691
Fax +966146542256
Email [email protected]
Purpose: Mammography screening (MS) is an underutilized screening tool; although it is provided free of charge to the Saudi community. The present study aimed at assessing knowledge and barriers of mammography screening among women attending primary health centers in Aljouf region, Saudi Arabia.
Materials and Methods: A cross-sectional study was carried out among 423 women aged 41– 75 years attending ten primary health centers in Aljouf region, Saudi Arabia. Structured interviewing questionnaires were used for data collection. SPSS program, version 24 was used for data analysis.
Results: The least reported risk factors of BC in this study were early menarche (14.9%), first pregnancy after the age of 30 years (18%), and late menopause (18.7%). Concerning knowledge of MS, 50.8% of the women correctly identified that mammogram is the ideal method for detecting BC. The most encountered personal barriers towards MS were lack of information about mammogram (69.5%), fear of exposure to radiation (67.4%), fear of discovery of BC (62.9%), being busy all the time (62.2%), and fear of cancer treatment (61.9%). Regarding economic barriers, 40% of the participants reported that taking sick leave from work is difficult while 37.8% revealed that mammogram is costly. Concerning health system barriers, the most common barriers were fear of error in diagnosis (62.6%), long time to take medical appointment (57%), and preferring not to have a mammogram except after a doctor recommendation (52.7%). The present study showed that women’s education and residence significantly predicted their knowledge. Furthermore, women’s education and income significantly predicted their barriers towards MS.
Conclusion: Many barriers toward mammography screening were encountered in the present study. Addressing these barriers and raising awareness about MS may be of great value to increase its uptake by Saudi women.
Keywords: knowledge, barriers, health services, secondary prevention, Saudi Arabia
Introduction
Breast cancer (BC) is a very serious health problem affecting both the developing and developed world and the prevalence is greater in many developed countries.1 Nearly 55% of BC cases exist in developed countries, but the incidence rates are rapidly increasing in the developing world.2 BC is considered the most prevalent cancer and the most important cause of cancer deaths among the women forming 23% of cancer cases and 14% of cancer mortality.3 In the Kingdom of Saudi Arabia, BC is responsible for 29% of all the cancers diagnosed in Saudi women as reported by the Saudi Health Council in 2014.4 There is clear evidence that detecting breast cancer early is associated with a more favorable outcome and a reduction in breast cancer deaths, and for this reason, strategies to detect breast cancer early, such as regular physical exams (BSE and CBE), heightened breast cancer awareness, and regular mammography have been promoted.5 There are different guidelines for recommending the starting age and frequency of doing MS. Based on the recommendations of the American Cancer Society, women should have the option to begin screening at age 40, but should begin annual screening at age 45, and should undergo annual screening from ages 45–54, and biennial screening after that, but retain the option to continue annual screening after age 55.6 According to the United States Preventive Services Taskforce, the decision to start MS in women before age 50 years should be an individual one and biennial screening mammography is recommended for women aged 50 to 74 with average risk.7 Although MS has been available in all areas of Saudi Arabia since 2005, the national Saudi Health Interview Survey (NSHIS) in 2015 had shown a very low rate of MS utilization as 92% of eligible women reported not having a mammogram in the previous year.8 Mammogram is a known screening method for BC, but to enhance its uptake, women should be knowledgeable about MS.9 A significant number of Saudi women were complaining of an advanced stage of BC because of a lack of awareness and knowledge of MS.10 Knowledge about MS is influenced by numerous factors, including socio-demographic characteristics of the women, their awareness of BC risk factors, and having a family history of BC.11–13 There were many barriers towards MS and these barriers were classified into three main groups: personal, health system, and economic barriers.14,15 In Saudi Arabia, cultural norms concerning violation of modesty, how women should interact with males other than their husbands, and beliefs about the privacy of the body may restrict women’s use of MS.16 Previous studies conducted on MS, did not comprehensively address the barriers towards mammography despite its availability in all regions of Saudi Arabia. Barriers that influence women’s practice towards MS need to be recognized to efficiently enhance the uptake of MS. Therefore, the present study endeavored to determine the knowledge and barriers of MS among women attending primary health centers in Aljouf region, Saudi Arabia. To the best of the authors’ knowledge, no study had been conducted in Aljouf region regarding this issue.
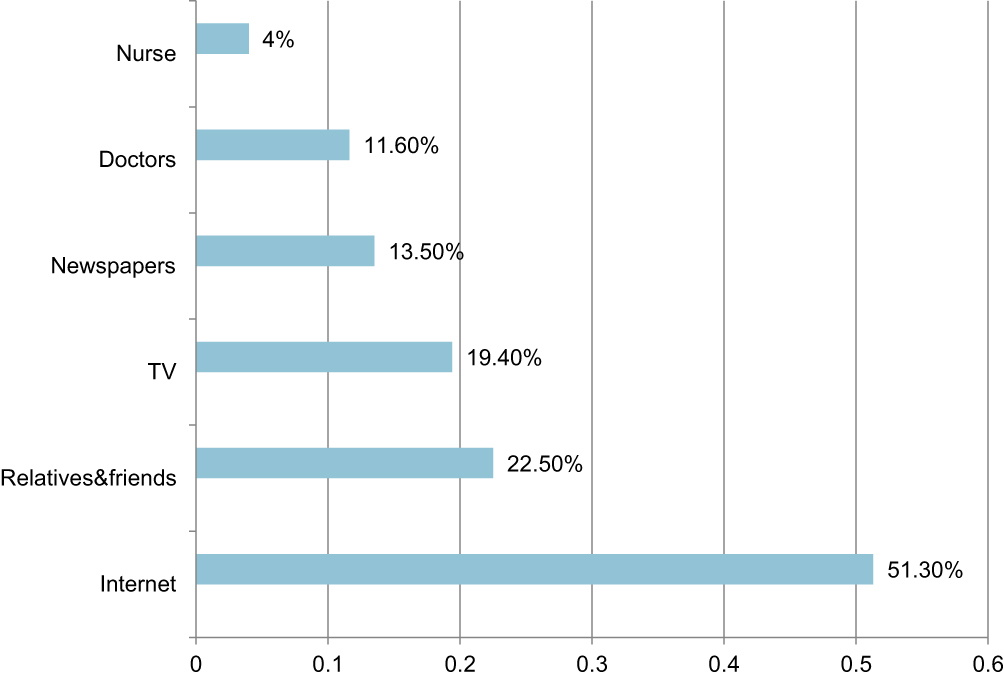 |
Figure 1 Sources of knowledge of BC risk factors and MS among Saudi women attending primary health centers (more than one response had been identified). |
Materials and Methods
Participants and Procedures
A cross-sectional study was done to determine knowledge and barriers of MS among women attending primary health centers in Aljouf region, Saudi Arabia. The present study was carried out in the primary health centers of Aljouf region. The participants were recruited from the waiting areas in the primary health centers and informed about the objectives of the present study. Data collection was carried out during the period from October 2019 to February 2020. The non-response rate among the interviewed Saudi women was 6% in the present study.
Sample Size
Sample size calculation was done utilizing n = P (1-P)z2/d2 after considering prevalence of 50%, d = 0.05, and Z = 1.96, applying a confidence level of 95% and 80% power of the study. The estimated sample size was 384. After adding 10% as a non-response rate, the sample size was raised to 423.
Sampling Technique
There were 43 primary health centers in Aljouf region, Saudi Arabia. A simple random sampling technique was applied to select ten centers out of 43. Then, the number of women selected in each primary health center was proportional to the number of women served by this center until reaching the estimated sample size.
Inclusion Criteria
A woman aged 40 years or more who had not had MS before and had not been diagnosed with BC was included in the present study.
Exclusion Criteria
Women who did not fulfill the above criteria were precluded from the present study.
Measurement Tools
A structured interviewing questionnaire composed of three parts was constructed after reviewing the available literature. The first part included background characteristics such as age, residence, education, occupation, marital status, income per month, and family history of BC. The second part of the questionnaire was composed of 14 questions and inquired about participants’ knowledge of BC risk factors and MS. The answer to each question was given a score “one” if correct and “zero” if wrong. Scores of the 14 questions were then summed. Cronbach’s alpha of the knowledge scale was 0.7. The third part of the questionnaire was about personal, economic, and health service barriers towards MS. These barriers were tested through 19 questions. Each question inquired about a certain barrier. MS barriers’ score was determined by summing all personal, health services, and economic barriers. The overall barrier score was constructed by giving two points for each question that was in agreement with a specific barrier, zero points for non-agreement, whereas one point for not defined answers. Cronbach’s alpha of this scale was 0.8. The barriers in the present study could be classified as follows:
- Personal barriers (Lack of information about MS/Do not know where MS has done/MS is not safe/Embarrassment of breast examination/Fear of pain/Fear of radiation/Fear of discovery of BC/Fear of cancer treatment/Busy with no free time),
- Economic barriers (Transport problems/Taking sick leave from work is difficult/MS is too costly),
- Health system barriers (Takes too long to get a medical appointment/No female doctor or nurse/Not considering privacy during the examination/The site that provides MS is far/No adequate description about MS by doctor/I will not do MS except if recommended by the doctor/Fear of errors in diagnosis).
Testing the clarity and understanding of the questionnaire was ensured by conducting a pilot study on 30 women. No modifications were done on the used questionnaire. The results of this pilot study were not included in the present study. The questionnaire was distributed during face to face interviews with the participants after a full explanation of the objectives of the study.
Statistics
Data analysis was done utilizing the SPSS program (IBM Corporation, Armonk, NY, USA), version 24. Descriptive statistics were performed using number and percentage for categorical variables, mean ±SD for continuous variables. Two linear regression models were done to detect factors that independently influence participants’ knowledge and participants’ barriers. Statistical significance was accomplished at P-value < 0.05.
Ethical Considerations
The study was done with the approval of the Ethical Review Committee of Jouf University, Saudi Arabia (Approval No: 17-8-6/40). The researchers guaranteed the ethical aspects in the present study by explaining the aims and objectives of the study to the participants before filling the questionnaire, taking informed written consent from women who welcomed to take part in the study, and ensuring privacy and confidentiality of collected data by using anonymous questionnaires.
Results
Table 1 shows the socio-demographic features of the respondents. The present study consisted of 423 females, aged 41–75 years with mean ±SD 49.12±6.98. Most of the respondents were urban residents (87.9%) and married (82%). Most of the participants had university/postgraduate education (74%) and 82.3% of them were employed. Almost 76% had a monthly income >7000 RS and 22.7% reported a family history of BC. Knowledge of participants regarding BC risk factors and MS is depicted in Table 2. Regarding knowledge of BC risk factors, 71.2%, 68.1% and 65.5% of the women respectively correctly identified that women consuming unhealthy food, with smoking behavior and non-lactating were more liable to have BC. Concerning knowledge of MS, 50.8%, 43.5% and 42.1% of the women respectively correctly identified that mammogram is the ideal method for detecting BC, frequency and the recommended age of doing it. The mean knowledge score (±SD) was 6.53±3.11. Table 3 shows the barriers towards MS among the respondents. The most encountered personal barriers towards MS were lack of information about mammogram (69.5%), fear of exposure to radiation (67.4%), fear of discovery of BC (62.9%), being busy all the time (62.2%), and fear of cancer treatment (61.9%). Regarding economic barriers, 40% reported that taking sick leave from work is difficult while 37.8% revealed that mammogram is costly. Concerning health system barriers, the most common barriers were fear of error in diagnosis (62.6%), long time to take medical appointment (57%) and not preferring doing mammogram except after doctor recommendation (52.7%). The mean barrier score (±SD) was 20.93±7.88.The most prevalent source utilized by the participants of this study for having information about BC risk factors and MS was the internet (51.3%) (Figure 1). Linear regression revealed that women’s residence and educational level were significantly affecting their level of knowledge (P=0.002 and 0.005 respectively). Urban residence and high educational level significantly influenced participants’ knowledge (Table 4). Table 5 shows that women’s educational level and monthly income significantly predicted the barriers score (P=0.001 and 0.037 respectively). The barrier score increased significantly among women with low education and low income.
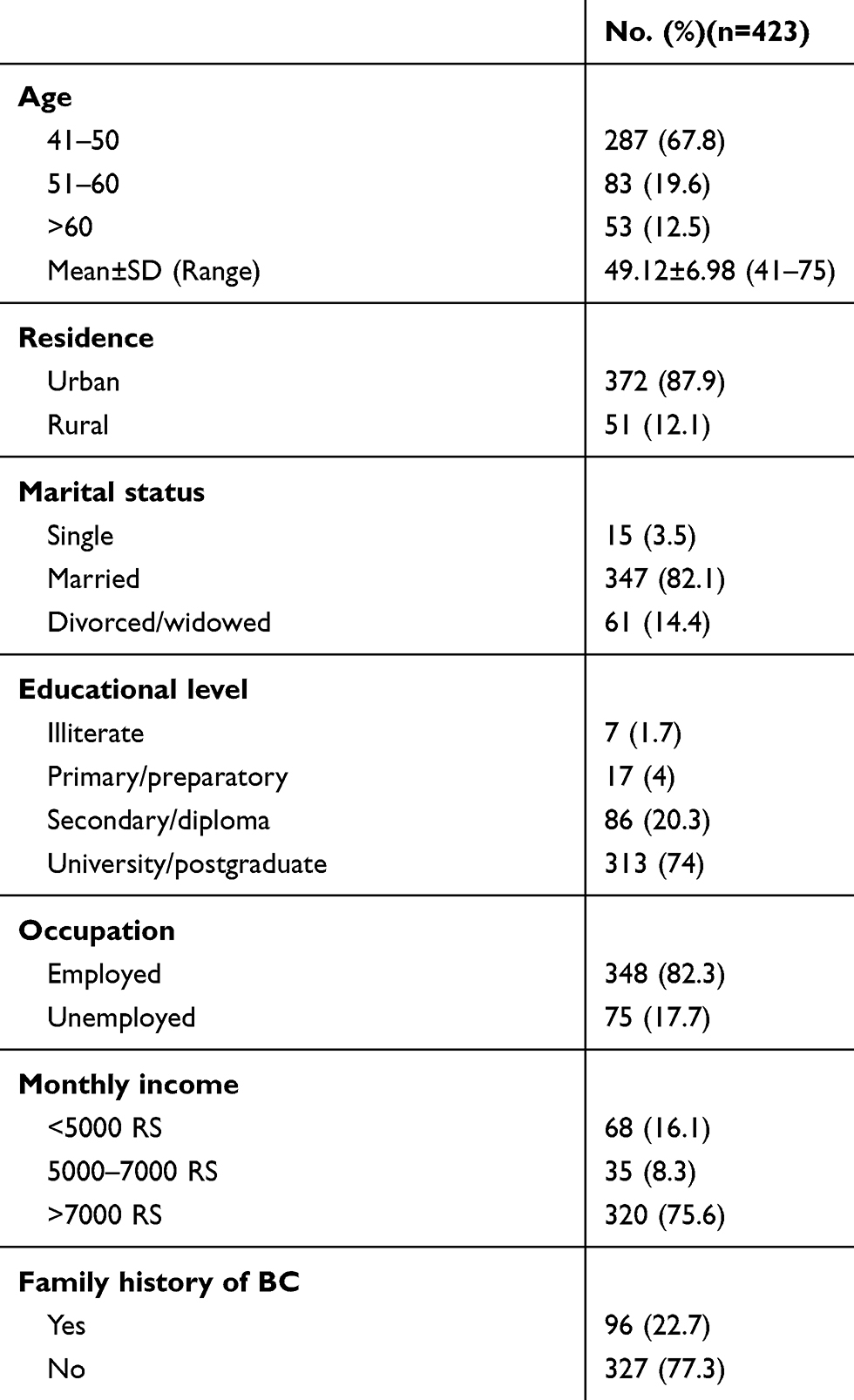 |
Table 1 Socio-Demographic Features and Family History of BC Among Saudi Women Attending Primary Health Centers |
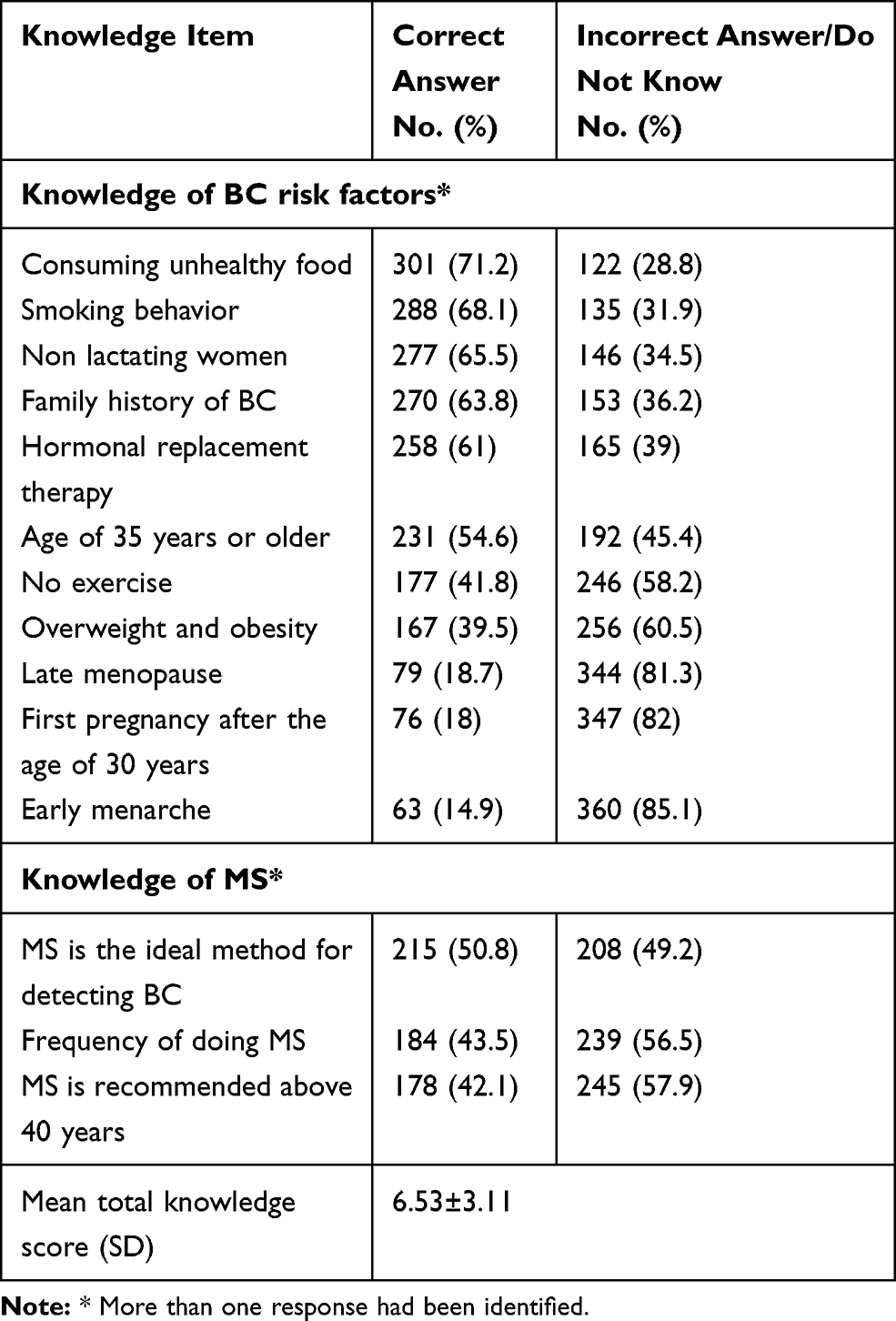 |
Table 2 Knowledge of BC Risk Factors and MS Among Saudi Women Attending Primary Health Centers |
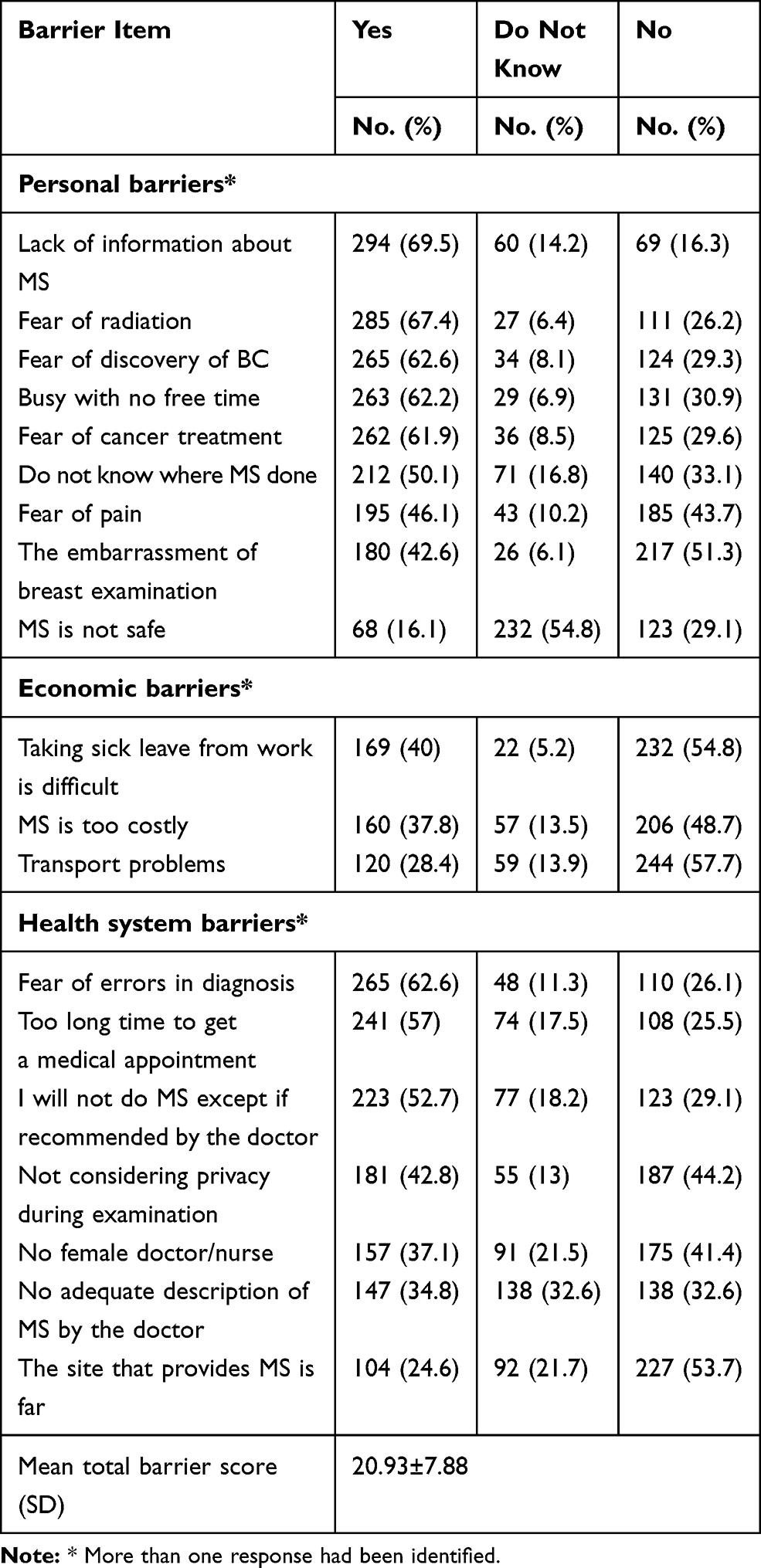 |
Table 3 Barriers Towards MS Among Saudi Women Attending Primary Health Centers |
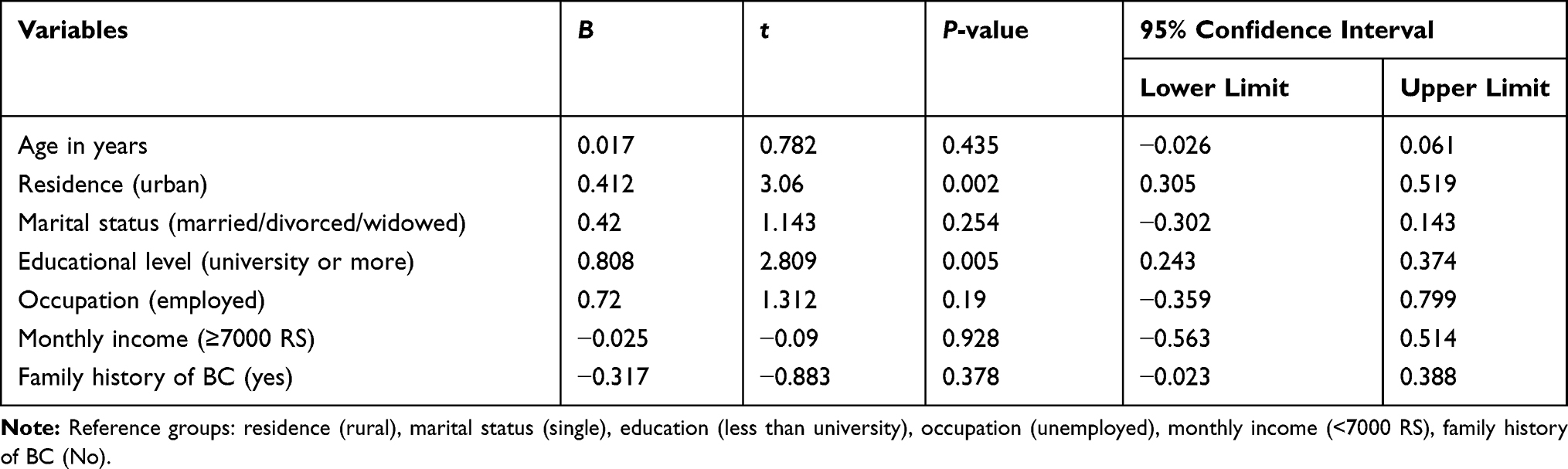 |
Table 4 Linear Regression Showing the Predictors of Participants’ Knowledge Among Saudi Women Attending Primary Health Centers |
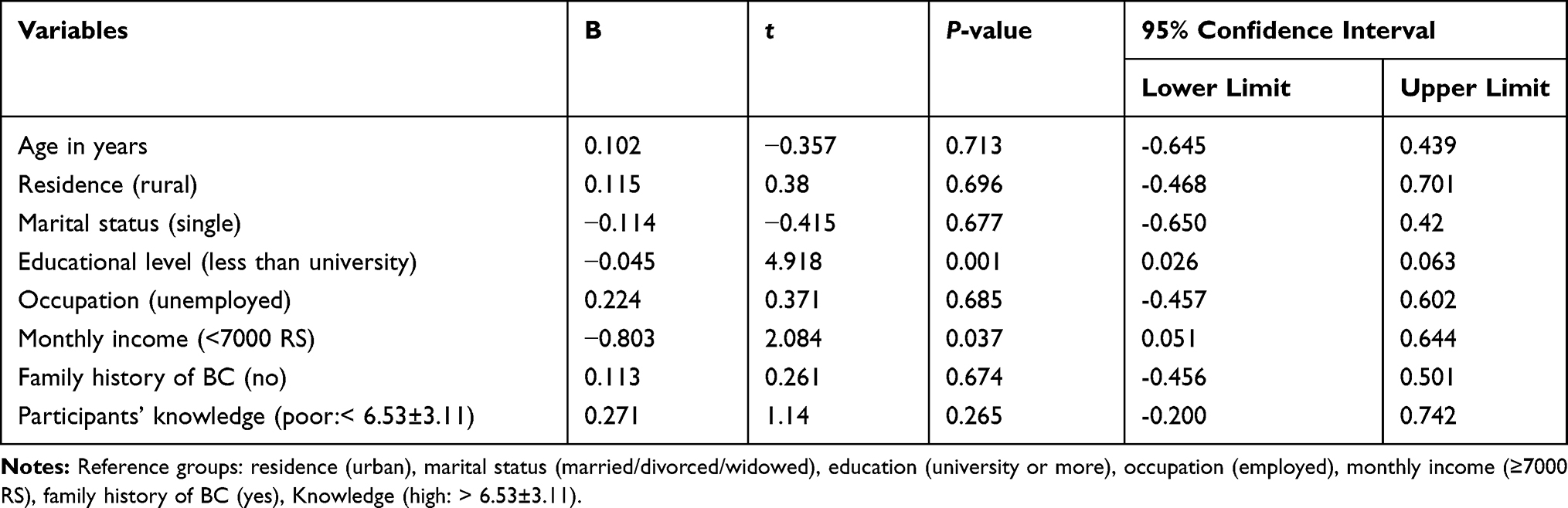 |
Table 5 Linear Regression Showing the Predictors of Participants’ MS Barriers Among Saudi Women Attending Primary Health Centers |
Discussion
Mammogram is an effective screening method for early recognition of BC.17 Despite the fact that a free mammography service has been available in all regions of Saudi Arabia since 2005; most Saudi women do not utilize it at all.8,18
The early signs of BC can be an abnormal mass detected on mammography, before being felt by the women or her physician.19 Nearly half of the respondents in the present study revealed that mammography is the ideal method for BC detection. However, mammography was recognized by more than 70% of the women, as the ideal method for BC detection in a study conducted by Schneider et al.11 In addition, 42% of the respondents in this study reported that MS was recommended above 40 years of age. This is inconsistent with a study conducted by Ojewusi and Arulogun who showed that only 3.3% of their respondents reported that the recommended age of MS was 40 years.20
Concerning knowledge of BC risk factors in this study, nearly two thirds of the participants did not know that obesity and overweight are risk factors for BC in agreement with a study conducted among Egyptian women.21 Boulos and Ghali showed that 45% of their respondents did not report that obesity is a risk factor for BC.22 The majority of the participants (82%) in this study did not know that having a first pregnancy after the age of 30 years was another risk factor for BC which is much higher than that reported in other studies.21–23
Nearly 46% of the respondents in this study were not aware that the incidence of BC increases with age. Furthermore, 71.4% of Indian women did not know that the probability of BC increases with age.23 Deficient knowledge regarding this non modifiable risk factor of BC was also shown in a Nigerian study.20 The least reported risk factor of BC in this study was early menarche which is inconsistent with a study conducted by Pohls et al.24
Concerning sources of knowledge of BC risk factors and MS, most of the participants in this study had gained their knowledge from the internet (Figure 1). The internet has played a substantial role in the rapidly transforming Saudi community. Furthermore, the majority of the women recruited in the present study was highly educated and consequently depended mainly on the internet as an integral part of their daily lives. However other studies21,22,25 revealed that the most common source of knowledge was TV, maybe because their participants were illiterates who understood television easily. In addition, a study carried out by Dandash and AL-Mohaimeed26 showed that the most common source of information among their participants was newspapers (83.2%) followed by TV (68.2%), and family and friends (28.6%) while health care providers (14.1%) were the least common source.26
Several personal, health system, and economic barriers to mammography have been reported among the studied participants, who had never sought MS before. The most common personal barriers towards MS that have been explored in this study were deficient information about mammogram, fear of radiation, fear of cancer discovery, fear of cancer treatment, and being busy all the time. The insufficient knowledge and misunderstandings concerning MS in this study will influence women’s decisions regarding mammography uptake. Lack of information about mammogram was the most reported personal barrier towards MS in some studies.27,28 A study conducted in the United States among Jordanian and Palestinian immigrant women revealed that the respondents experienced certain fears such as fear of cancer treatment, fear of pain, and fear of cancer discovery.29 Shirzadi et al30 showed that perception of mammography harmfulness was an established barrier towards MS as the women experienced their worries about radiation exposure in addition to the fear of the procedure itself.30 Overcoming of the personal barriers can be done by enhancing health-seeking behavior in the awareness campaigns through informing the women about the benefits of early recognition of BC and empowering them to take care of own health even if they were busy. In addition, these awareness campaigns should provide all the information necessary about MS to the women. Fear of error in the diagnosis and too long time to get an appointment were the most common health system barriers in the present study. These health system barriers highlight the importance of ensuring that health care providers should have positive attitudes towards their clients and provide proper counseling to correct the misconceptions about MS. In addition, the unwillingness to have MS except after doctor recommendations was another health system barrier in this study. Other studies also acknowledged the pivotal role of health care provider in persuading the women to do MS.31–33
Low educated women have poor knowledge and negative attitude towards BC risk factors and MS.34 The current study demonstrated that highly educated women had more knowledge about BC risk factors and MS, which is consistent with other studies.21,35 The deficient knowledge among less educated women in this study reflects the presence of social imbalance in the access to information regarding the early detection of BC. Furthermore, low educated women in this study were more likely to perceive different barriers towards MS in agreement with other studies.28,36 The health behaviors and attitude towards BC screening is higher among women residing in urban regions compared to women residing in rural regions.37,38 The current study explored that knowledge of the participants was significantly higher among urban residents, which is consistent with a study conducted among Egyptian women.25 Future outreach programs should reach women living in rural areas to enhance their awareness of BC risk factors and MS. A population survey with female adults about knowledge of MS and its associated factors revealed that old age, high income, and high education were correlated with knowledge about mammography.11 Brito et al39 revealed an association between education and knowledge about MS, in which females with high educational levels had a 50% greater chance of having adequate knowledge.39 In a Malaysian study, higher education and increased income were correlated with knowledge about MS, and women aged 50–59 years old had 50% more liability of presenting good knowledge compared to those aged 60 years old or more.40 A study carried out by Amin et al41 in Saudi Arabia; revealed that the predictors associated with increased knowledge about MS were high educational level, positive family history of BC, being employed, and having a clinical breast examination.41
The present study demonstrated that women with lower incomes were more susceptible to perceive different barriers towards MS in agreement with other studies.28,35 Poor women have other priorities in their life that places BC screening practice low compared to other priorities.42 Raising the awareness of the women and their empowerment will have a substantial role in overcoming these barriers. Health education campaigns about the importance of MS with the assistance of civil societies in the community may be of great value in increasing knowledge about this screening tool and enhancing its uptake among Saudi women.
Some limitations have been shown in the present study. The results of this study cannot be generalized because the respondents were only from Aljouf area, not from all Saudi Arabia areas. In addition, this study is cross sectional with more vulnerability to recall and interview biases.
Conclusion and Recommendation
The highest reported risk factors of BC were consumption of unhealthy food (71.2%), smoking behavior (68.1%) and no lactation (65.5%). Nearly half of the participants reported that MS is the ideal method for BC detection. Urban residence and high educational level of the participants in this study significantly affected their knowledge. Numerous personal, economic, and health system barriers to MS have been revealed in the present study. The barriers towards MS increased significantly among women with low education and low income. More well-designed health education programs leaded by healthcare providers are needed to eliminate the barriers towards MS and accentuate the importance of early detection in the management of breast cancer. This eventually can lead to a decrease in morbidity and mortality because of BC among Saudi women.
Acknowledgment
The researchers would like to express their extreme thanks to the administrators of primary health centers for facilitating carrying out the present study and all the participating women for their cooperation.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work. Hind Y. Alyousef, Wahaj A. Almasoud, Mashael B. Alanzi, and Atheer Z. Mubarak are medical students.
Funding
This study was self-funded.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Colditz GA, Bohlke K, Berkey CS. Breast cancer risk accumulation starts early: prevention must also. Breast Cancer Res Treat. 2014;145(3):567–579. doi:10.1007/s10549-014-2993-8
3. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. doi:10.3322/caac.21262
4. Kingdom of Saudi Arabia, Saudi Health Council, National Health Information Center, Saudi Cancer Registry. Cancer Incidence Report in Saudi Arabia 2015. Available from: https://nhic.gov.sa/eServices/Documents/E%20SCR%20final%206%20NOV.pdf.
5. Sadler GR, Dhanjal SK, Shah NB, et al. Asian Indian women: knowledge, attitudes and behaviors toward breast cancer early detection. Public Health Nurs. 2001;18(5):357–363. doi:10.1046/j.1525-1446.2001.00357.x
6. Oeffinger KC, Fontham ET, Etzioni R, et al. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;314(15):1599–1614. doi:10.1001/jama.2015.12783
7. CDC,2020: Centers for disease control and prevention. Breast Cancer Screening Guidelines for Women. Available from: www.cdc.gov/cancer/breast/pdf/BreastCancerScreeningGuidelines.pdf.
8. El Bcheraoui C, Basulaiman M, Wilson S, et al. Breast cancer screening in Saudi Arabia: free but almost no takers. PLoS One. 2015;10:1–10. doi:10.1371/journal.pone.0119051
9. Alshahrani M, Alhammam SYM, Al Munyif HAS, Alwadei AMA, Alzamanan SSM, Aljohani NSM. Knowledge, attitudes, and practices of breast cancer screening methods among female patients in primary healthcare centers in Najran, Saudi Arabia. J Cancer Educ. 2019;34(6):1167–1172. doi:10.1007/s13187-018-1423-8
10. Madkhali N, Santin O, Noble H, Reid J. Breast health awareness in an Arabic culture: a qualitative exploration. J Advan Nurs. 2019;75(8):1713–1722. doi:10.1111/jan.14003
11. Schneider I, Corseuil M, Boing A, D’Orsi E. Knowledge about mammography and associated factors: population surveys with female adults and elderly. Rev Bras Epidemiol. 2013;16(4):930–942. doi:10.1590/S1415-790X2013000400013
12. Kotepui M, Piwkham D, Chupeerach C, Duangmano S. Knowledge, attitudes and practice of breast cancer screening among female personnel of Walailak University. Health Expect. 2015;18(6):3069–3078. doi:10.1111/hex.12292
13. Bawazir A, Bashateh N, Jradi H, Breik AB. Breast cancer screening awareness and practices among women attending primary health care centers in the Ghail Bawazir District of Yemen. Clin Breast Cancer. 2019;19(1):20–29. doi:10.1016/j.clbc.2018.09.005
14. Katapodi MC, Lee KA, Facione NC, Dodd MJ. Predictors of perceived breast cancer risk and the relation between perceived risk and breast cancer screening: a meta-analytic review. Prev Med. 2004;38(4):388–402. doi:10.1016/j.ypmed.2003.11.01
15. Thompson HS, Littles M, Jacob S, Coker C. Post treatment breast cancer surveillance and follow-up care experiences of breast cancer survivors of African descent: an exploratory qualitative study. Cancer Nurs. 2006;29(6):478–487. doi:10.1097/00002820-200611000-00009
16. Azaiza F, Cohen M. Health beliefs and rates of breast cancer screening among Arab women. J Womens Health (Larchmt). 2006;15(5):520–530. doi:10.1089/jwh.2006.15.520
17. Tolma EL, Batterton C, Hamm RM, Thompson D, Engelman KK. American Indian women and screening mammography: findings from a qualitative study in Oklahoma. Am J Health Educ. 2012;43:18–30. doi:10.1080/19325037.2012.10599214
18. Alhazmi FG. Comparison of breast and colorectal cancer screening programs in the Netherlands and the Kingdom of Saudi Arabia. Int J Acad Sci Res. 2016;4:157–165.
19. Brennan PC, Gandomkar Z, Ekpo EU, et al. Radiologists can detect the ‘gist’ of breast cancer before any overt signs of cancer appear. Sci Rep. 2018;8(1):8717. doi:10.1038/s41598-018-26100-5
20. Ojewusi AA, Arulogun OS. Breast cancer knowledge and screening practices among female secondary school teachers in an urban local government area, Ibadan. Nigeria J of Public Health Epidemiol. 2016;8(5):72–81. doi:10.5897/JPHE2015.0781
21. Manzour AF, Gamal EDA. Awareness about breast cancer and mammogram among women attending outpatient clinics, Ain Shams University Hospitals, Egypt. J Egypt Public Health Assoc. 2019;94:26. doi:10.1186/s42506-019-0026-5
22. Boulos DN, Ghali RR. Awareness of breast cancer among female students at Ain Shams University, Egypt. Glob J Health Sci. 2013;6(1):154–161. doi:10.5539/gjhs.v6n1p154
23. Dahiya N, Basu S, Singh MC, Garg S, Kumar R, Kohli C. Knowledge and practices related to screening for breast cancer among women in Delhi, India. Asian Pac J Cancer Prev. 2018;19(1):155–159. doi:10.22034/APJCP.2018.19.1.155
24. Poehls UG, Hack CC, Wunderle M, et al. Awareness of breast cancer incidence and risk factors among healthy women in Germany: an update after 10 years. Eur J Cancer Prev. 2019;28(6):515–521. doi:10.1097/CEJ.0000000000000500
25. Allam MF, Abd Elaziz KM. Evaluation of the level of knowledge of Egyptian women of breast cancer and its risk factors. A cross sectional study. J Prev Med Hyg. 2012;53(4):195–198.
26. Dandash KF, AL-Mohaimeed A. Knowledge, attitudes, and practices surrounding breast cancer and screening in female teachers of Buraidah, Saudi Arabia. Int J Health Sci (Qassim). 2007;1(1):61–71.
27. Parkington SR, Faine N, Nguyen MC, Lowry MT, Virginkar PA. Barriers to breast cancer screening in a managed care population. Manag Care. 2009;18(4):34–45.
28. Abdel-Aziz SB, Amin TT, Al-Gadeeb MB, et al. Perceived barriers to breast cancer screening among Saudi women at primary care setting. J Prev Med Hyg. 2018;59(1):20–29. doi:10.15167/2421-4248/jpmh2018.59.1.689
29. Kawar LN. Barriers to breast cancer screening participation among Jordanian and Palestinian American women. Eur J Oncol Nurs. 2013;17(1):88–94. doi:10.1016/j.ejon.2012.02.004
30. Shirzadi S, Allahverdipour H, Sharma M, Hasankhani H. Perceived barriers to mammography adoption among women in Iran: a qualitative study. Korean J Fam Med. 2020;41(1):20–27. doi:10.4082/kjfm.18.0054
31. Mamdouh HM, El-Mansy H, Kharboush IF, et al. Barriers to breast cancer screening among a sample of Egyptian females. J Family Community Med. 2014;21(2):119–124. doi:10.4103/2230-8229.134771
32. Alexandraki I, Mooradian AD. Barriers related to mammography use for breast cancer screening among minority women. J Natl Med Assoc. 2010;102(3):206–218. doi:10.1016/s0027-9684(15)30527-7
33. Davis TC, Arnold C, Berkel HJ, Nandy I, Jackson RH, Glass J. Knowledge and attitude on screening mammography among low-literate, low-income women. Cancer. 1996;78(9):1912–1920. doi:10.1002/(sici)1097-0142(19961101)78:9<1912:aid-cncr11>3.0.co,2-0
34. Peek ME, Han JH. Disparities in screening mammography. Current status, interventions and implications. J Gen Intern Med. 2004;19(2):184–194. doi:10.1111/j.1525-1497.2004.30254.x
35. Gürdal SÖ, Saraçoğlu GV, Oran ES, Yankol Y, Soybir GR. The effects of educational level on breast cancer awareness: a cross-sectional study in Turkey. Asian Pac J Cancer Prev. 2012;13(1):295–300. doi:10.7314/APJCP.2012.13.1.295
36. Al-Wassia RK, Farsi NJ, Merdad LA, Hagi SK. Patterns, knowledge, and barriers of mammography use among women in Saudi Arabia. Saudi Med J. 2017;38(9):913–921. doi:10.15537/smj.2017.9.20842
37. Solikhah S, Promthet S, Hurst C. Awareness level about breast cancer risk factors, barriers, attitude and breast cancer screening among Indonesian women. Asian Pac J Cancer Prev. 2019;20(3):877–884. doi:10.31557/APJCP.2019.20.3.877
38. Allahverdipour H, Asghari-Jafarabadi M, Emami A. Breast cancer risk perception, benefits of and barriers to mammography adherence among a group of Iranian women. Women Health. 2011;51(3):204–219. doi:10.1080/03630242.2011.564273
39. Brito LG, Brito LM, Chein MB. Knowledge about mammography of women from a Northeastern city in Brazil. Prev Med. 2011;52(3–4):285–286. doi:10.1016/j.ypmed.2011.02.009
40. Sim HL, Seah M, Tan SM. Breast cancer knowledge and screening practices: a survey of 1000 Asian women. Singapore Med J. 2009;50(2):132–138.
41. Amin TT, Al Mulhim AR, Al Meqihwi A. Breast cancer knowledge, risk factors and screening among adult Saudi women in a primary health care setting. Asian Pac J Cancer Prev. 2009;10(1):133–138.
42. Ahmed NU, Fort JG, Elzey JD, Belay Y. Empowering factors for regular mammography screening in under-served populations: pilot survey results in Tennessee. Ethn Dis. 2005;15(3):387–394.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.