")
Back to Journals » Patient Preference and Adherence » Volume 9
Perampanel in the management of partial-onset seizures: a review of safety, efficacy, and patient acceptability
Authors Schulze-Bonhage A, Hintz M
Received 1 May 2015
Accepted for publication 3 July 2015
Published 11 August 2015 Volume 2015:9 Pages 1143—1151
DOI https://doi.org/10.2147/PPA.S63951
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Video abstract presented by Andreas Schulze-Bonhage.
Views: 2495
Andreas Schulze-Bonhage, Mandy Hintz
Epilepsy Center, University Medical Center Freiburg, Freiburg, Germany
Abstract: Perampanel (PER) is a novel antiepileptic drug recently introduced for the adjunctive treatment in epilepsy patients aged 12 years or older with partial-onset seizures with or without secondary generalization in the US and Europe. Its antiepileptic action is based on noncompetitive inhibition of postsynaptic AMPA receptors, decreasing excitatory synaptic transmission. Evaluation of efficacy in three placebo-controlled randomized Phase III studies showed that add-on therapy of PER decreased seizure frequencies significantly compared to placebo at daily doses between 4 mg/day and 12 mg/day. PER’s long half-life of 105 hours allows for once-daily dosing that is favorable for patient compliance with intake. Long-term extension studies showed a 62.5%–69.6% adherence of patients after 1 year of treatment, comparing favorably with other second-generation antiepileptic drugs. Whereas these trials demonstrated an overall favorable tolerability profile of PER, nonspecific central nervous system adverse effects like somnolence, dizziness, headache, and fatigue may occur. In addition, neuropsychiatric disturbances ranging from irritability to suicidality were reported in several case reports; both placebo-controlled and prospective long-term extension trials showed a low incidence of such behavioral and psychiatric complaints. For early recognition of neuropsychiatric symptoms like depression, anxiety, and aggression, slow titration and close monitoring during drug introduction are mandatory. This allows on the one hand to recognize patients particularly susceptible to adverse effects of the drug, and on the other hand to render the drug’s full potential of seizure control available for the vast majority of patient groups tolerating the drug well.
Keywords: epilepsy, antiepileptic drugs, AMPA receptor, structural epilepsy, partial-onset seizures, perampanel
Introduction
Perampanel (PER, 2-[2-oxo-1-phenyl-5-pyridin-2-yl-1,2-dihydropyridin-3-yl]benzonitrile hydrate, Fycompa®) is the first antiepileptic drug (AED) available for the treatment of partial-onset seizures exerting its antiepileptic action at the AMPA receptor. PER modulates the receptor in a noncompetitive manner, thus decreasing Na+ influx and reducing the postsynaptic depolarization resulting from presynaptic glutamate release. With glutamate being the major excitatory neurotransmitter in the brain,1 decreasing excitation by blockade of glutamate receptors has long been discussed as a therapeutic option to rebalance excitation and inhibition in epilepsy patients.2
In earlier times, the NMDA subreceptor had been investigated as a potential target for reducing excitability, particularly as this type of glutamate receptor plays a key role in use-dependent synaptic potentiation, including long-term potentiation. Normal functioning of NMDA receptors has, however, been regarded as essential for memory formation, and a number of motor and cognitive side effects were noted in pilot studies of NMDA blockade. NMDA receptor blockade has been shown to be followed by biochemical changes and memory disorder in rodents.3,4 Deficits in memory and learning could be related to NMDA receptor antagonism as discussed in preceding studies5,6 as the NMDA receptor is crucial for growth and maturation of the brain and its cognitive function.7
Whereas NMDA receptor antagonists have shown good antiepileptic efficacy,8 they were associated with major behavioral side effects encompassing motor stereotypies like head weaving/nodding and circling in rats9 and concentration deficits, sedation, disorientation and confusion, depression and impairment of motor coordination, dizziness, and diplopia in humans.8 Disproportionate inhibition of cerebral excitatory amino acid transmission may explain why such adverse effects are particularly frequent in epilepsy patients.10 NMDA receptor antagonists, however, as well caused frequent and major neuropsychiatric side effects consisting of mood changes, agitation, sedation, confusion, or hallucinations, and at high doses, catatonia when given to stroke patients.11,12
Blockade of AMPA receptors can likewise be assumed to have widespread effects on neuronal excitation, including propagation and triggering of epileptic discharges. In an early clinical crossover trial, the AMPA receptor blocker talampanel was found to be effective in reducing particularly simple partial seizures.13 AMPA receptor blockade using PER has been shown to be efficacious in a number of animal models of acute seizures and in the kindling model of epilepsy.14–20 In mice, mostly motor side effects were observed.21
Preclinical aspects of human PER exposure are included in a recent review of Schulze-Bonhage.22 Three clinical trials have shown that adverse motor effects like dizziness and ataxia may occur at plasma peak concentrations but are rarely limiting for dose escalation. In contrast, aside from somnolence, neuropsychiatric side effects occurred more frequently than with placebo treatment. These adverse effects mostly occurred within the first 6 weeks of treatment, were not limited to patients with a history of psychiatric disease, and could become reasons to discontinue PER. In the following, clinical results on efficacy and tolerability of PER are given with particular emphasis on long-term retention, compliance, and neuropsychiatric tolerability.
Pharmacokinetics
PER is readily absorbed following oral ingestion with a bioavailability of 100%. Whereas intake with food lowers the slope of absorption, increases Tmax from 1 hour in fasting state by about 2 hours, and reduces Cmax by one-third,23 the total amount absorbed (area under the curve [AUC]) does not depend on coingestion of food. PER is bound to proteins (predominantly albumins) by >95%, corresponding to a low free serum fraction of <5%. Liver metabolism is slow, resulting in a negligible first pass effect and in an unusually long mean T1/2 with considerable interindividual variance (mean 105 hours, range 53–136 hours) in subjects without concomitant exposure to enzyme-inducing AED. Metabolism occurs by oxidation via the cytochrome P450 (CYP) system, with mainly CYP 3A4 and CYP 3A5 involved, and secondary glucuronidation. The metabolites are inactive and are excreted up to 70% via feces.24
Based on the hepatic metabolism, PER is subject to various interactions. Co-administered enzyme-inducing drugs increase PER clearance considerably: with carbamazepine, AUC is decreased by 67%, with phenytoin and oxcarbazepine by 50%, and with topiramate by 20%. On the other hand, PER is a weak enzyme inducer, decreasing levonorgestrel levels by 40% and lowering midazolam AUC by 13%; there may be decreases to a minor degree (<10%) in the levels of other AEDs. In contrast, oxcarbazepine clearance is reduced by 26% resulting in markedly elevated serum levels.25
Efficacy
Focal epilepsy is a complex and etiologically diverse disease; accordingly, susceptibility to individual drugs in controlling arising seizures has been limited to subpopulations so far. PER adds a new mechanism of action to the available treatment armamentarium; this gave rise to the hope to improve seizure control in those patients unresponsive to available AEDs with different target mechanisms. Three Phase III, randomized, placebo-controlled, double-blind, multicenter trials (studies 304, 305, 306) have demonstrated the efficacy of PER.26–28 Based on these regulatory trials, PER has been approved in the US and Europe for the adjunctive treatment in adolescents and adults (aged 12 years and older) with partial-onset seizures with or without secondary generalization.29
In preparation of these trials, there have been two consecutive Phase II studies with dose escalation and placebo-controlled for dose finding. In patients with refractory focal epilepsy, an adjunctive therapy with oral dosage of 2–12 mg/day was tolerated by substantial proportions of patients.30
Randomized, placebo-controlled trials
Placebo-controlled, randomized Phase III studies compared the once-daily administration of PER 8 mg and 12 mg and placebo in studies 304 and 305, whereas PER doses of 2 mg, 4 mg, and 8 mg and placebo were compared in study 306 in patients of 12 years and older. Following prospective baseline periods of 6-week duration, the schedules of these trials were designed with a starting dose of 2 mg/day and following weekly dose increments by 2 mg to the target dose and a subsequent maintenance period of 13 weeks.26–28
The patients included in study 304 (n=388 randomized and treated, n=387 with seizure frequency data) received placebo (n=121) or once-daily PER doses of 8 mg (n=133) or 12 mg (n=134). For the intention-to-treat (ITT) population, the median percentage change in seizure frequency was −26.3% (8 mg, P=0.0261), −34.5% (12 mg, P=0.0158), and −21.0% (placebo group). Fifty-percent responder rates for the ITT population were 37.6% (8 mg, P=0.0760), 36.1% (12 mg, P=0.0914), and 26.4% (placebo group).26
The patients included in study 305 (n=386 randomized and treated, n=321 completed study) received placebo (n=136) or once-daily PER doses of 8 mg (n=129) or 12 mg (n=121). For the ITT population, the median percentage change in seizure frequency was −30.5% (8 mg, P<0.001), −17.6% (12 mg, P=0.011), and −9.7% (placebo). Fifty-percent responder rates for the ITT population were 33.3% (8 mg, P=0.0018), 33.9% (12 mg, P<0.001), and 14.7% (placebo).27
The patients included in study 306 (n=706 randomized and treated, n=623 completed study) received placebo (n=185) or once-daily PER doses of 2 mg (n=180), 4 mg (n=172), or 8 mg (n=169). For the ITT population, the median percentage change in seizure frequency was −13.6% (2 mg, P= ns), −23.3% (4 mg, P=0.003), −30.8% (8 mg, P<0.001), and −10.7% (placebo). Fifty-percent responder rates for the ITT population were 20.6% (2 mg, P= ns), 28.5% (4 mg, P=0.013), 34.9% (8 mg, P<0.001), and 17.9% (placebo group).28
A pooled analysis of these randomized, controlled studies showed a numerical superior efficacy of PER of 12 mg/day versus 8 mg/day in controlling secondarily generalized tonic–clonic seizures without statement if this difference achieved statistical significance.31
Seizure-free rates were low in the highly pharmacoresistant patient cohorts included in the randomized studies. Depending on the dose applied, the following percentage of patients did not experience any seizures during the maintenance phase when treated with PER: 1.9% (2 mg PER, study 304) and 4.4% (4 mg PER, study 306); 4.8%, 2.8%, and 2.6% (8 mg PER, studies 304, 305, and 306); and 6.5%/2.0% (12 mg PER, studies 305/306) (compared to 1.2%, 1.7%, and 0% in the respective placebo groups).26–28
Open-label extension studies
After termination, the three above-outlined Phase III studies were extended providing the patients (n=1,264) with the opportunity to continue enrollment in an open-label study (study 307) assessing the long-term efficacy of PER. There was an initial 16-week blinded conversion period during which patients initially under placebo therapy were uptitrated with 2 mg increments every 2 weeks; similarly, previously well-tolerated dosages were increased by 2 mg every 2 weeks up to 12 mg/day or to the maximum tolerated dose.30
The patients included in study 307 (n=1,218 randomized and treated, corresponding to 96.4% of those who had completed one of the Phase III studies) received a high mean daily PER dose of 10.6 mg during the maintenance period. The global median value of exposure to PER was 78.4 weeks. Regarding the ITT population (n=1,217), patients were divided into cohorts (same minimum duration of exposure) analyzing the seizure outcomes: at least 6 months of exposure (n=1,090, 89.6%), at least 9 months (n=980), at least 1 year (n=874), and at least 2 years (n=337). Weeks 1–13 and weeks 14–26 (uptitration of PER) were the periods where patients showed an improvement of seizure control. Through the specified four exposure cohorts, the responder rates were similar. Seizure-free rates after 6 months of the maintenance period were 4.9%, and over the last 6 months, 10.6% (at least 2 years of data).32
Also, the patients (n=180) of the two Phase II trials were offered to enroll in an extended study (207). This trial was designed with increments of 2 mg PER every 2 weeks up to target dose of 12 mg/day (titration period) and a subsequent maintenance period for 424 weeks as planned maximum. In contrast to the above-mentioned open-label extension study,30 uptitration was performed much very diligently, resulting in a median maximum tolerated PER dose of 7.3±3.3 mg/day. The trial showed that over a third of the enrolled patients (n=138, 76.7% of whom completed one of the Phase II studies) stayed on PER treatment for a follow-up period of 4 years, and no new safety signals emerged with long-term treatment.33
Whereas in regulatory trials a superior efficacy of high PER doses on secondarily generalized tonic–clonic seizures was noted,31,34 there were no subanalyses in long-term studies suggesting that particular seizure types particularly profit from dose optimization over time.
Tolerability and safety
Adverse effects
To investigate tolerability and safety of PER, two Phase II randomized trials were initiated including patients (18–70 years) with refractory focal epilepsy (greater than or equal to three AEDs). One hundred and fifty-three patients included in trial 206 received placebo or a maximum of 4 mg PER once daily or twice daily with uptitration from 1 mg to 4 mg every 2 weeks following a 4-week baseline period. Once- and twice-daily administration were tolerated similarly well, with overall rates of adverse effects being similar in all groups with 62.7% (placebo) versus 66.7% (PER). Adverse effects were followed by discontinuation in six subjects (placebo =3, BID =2, QD =1). Four were reported as severe adverse effects, two with placebo, and all of them associated with seizure activity. Neither abnormal laboratory tests nor electrocardiogram (ECG) abnormalities occurred in the PER group.
In trial 208 with corresponding design, 48 patients received PER or placebo with dose adjustment every 2 weeks up to higher daily doses of 12 mg/day to assess the maximum tolerated dose. Thirty-two percent of patients reached the dosage of 12 mg/day. Overall rates of side effects were similar in all groups with 80.0% (placebo) versus 84.2% (PER). Adverse effects led to drug discontinuation in three subjects (placebo =1, PER =2). One case in each group suffered from a severe adverse event, considered unrelated to treatment.
In both studies with limited patient numbers, dizziness and somnolence were the most frequently reported adverse events,30 and headache as the most common adverse event indicating a percentage of 93.5% of those suffering from mild or moderate and 15.2% from severe adverse events (convulsion, schizophrenia, status epilepticus, secondarily generalized seizure).33
In Phase III trials, appearance of side effects led to interruption of treatment with PER in 1.7% (4 mg), 4.2% (8 mg), and 13.7% (12 mg) versus 1.4% using placebo due to dizziness, irritability, and aggression, respectively. The most frequently reported adverse effects were dizziness and somnolence. Here, 87.4% represented side events of which 73% were mild or moderate. A severe adverse event (in >1% of patients) was only mentioned based on occurring seizures. A single case of sudden unexpected death in epilepsy was registered in trial 307. Combining all three studies, suicidality was recorded in three cases during PER exposition.35
Neither vital signs nor ECG analyses and laboratory values gave rise to concerns in Phase II and Phase III trials.35 Weight increase above 7% of baseline weight was, however, found in 4.4%–8.3% of placebo versus 11.6%–19.2% of PER-treated patients.26–28 On average, weight increased in PER-treated patients by 1.2 kg (with a wide range from decrease to increase) compared to +0.4 kg with placebo. Overall, 14.6% of PER-treated patients had a weight increase by more than 7%; this ratio, however, appeared not to be dose dependent (ranging from 12.2% with 2 mg/day to 15.4% treated with 12 mg/day35). Long-term studies were inconsistent regarding the risk of further weight gain with long-term intake of PER (+0.2 kg in studies 206 and 208 in contrast to +0.9 kg in study 307); part of the weight gain observed in long-term studies was related to the subgroup of adolescent patients.32
Psychiatric and behavioral reactions such as anger, aggression, hostility, threatening behavior, homicidal ideation, and irritability are considered as probable treatment-related adverse events with PER, even though they occurred infrequently in prospective, randomized trials36 (Table 1). In extension study 207, anxiety was reported in 7.2%, and irritability in 5.8%, as psychiatric side effects, whereas cases of homicide or suicidality were not mentioned. In extension study 307, 5.5% of patients discontinued treatment due to psychiatric symptoms, including 1.3% due to irritability, and 0.4% each due to aggression or abnormal behavior; 3.9% of patients showed one or more psychiatric adverse effects (in 42.6% of patients with a history of psychiatric disease), 1% of patients had aggression, 0.5% had psychotic disorder or suicidal ideation, and 0.3% had affective disorder, depression, or attempted suicide. In addition, paranoia and abnormal behavior, acute psychosis, agitation, or disorientation were reported in 0.2% each.
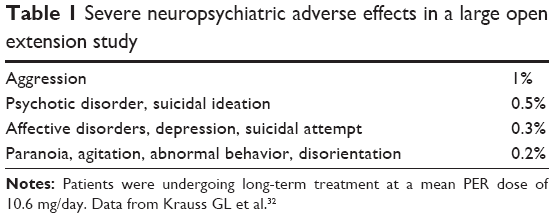 | Table 1 Severe neuropsychiatric adverse effects in a large open extension study |
Controlled Phase III studies showed the following neuropsychiatric adverse events: irritability (7% 8 mg; 12% 12 mg PER versus placebo 3%), aggression (2% 8 mg; 3% 12 mg PER versus 1% placebo), and anger (1% 8 mg; 3% 12 mg PER versus 0.2% placebo) developing mostly during the first 6 weeks of treatment; this led to discontinuation of PER in 0.5%, due to irritability and aggression, and in 0.4% related to anger.
A specific role of neuropsychiatric adverse effects of PER treatment is also suggested by observational studies. In a study of 47 individuals treated with a median PER dose of 8 mg/day (range 2–12 mg/day), behavioral alterations were the most frequent reason for discontinuation of treatment. In this cohort, three patients each were reported to behave aggressive or experience suicidality.37 Patients treated with placebo and concomitant AED showed significantly less neuropsychiatric side effects than PER and concomitant AED. Psychiatric side effects of PER were mostly found at higher dosages.
As a consequence of these treatment-emergent adverse effects, it has been recommended to carefully select patients, to counsel them properly, and monitor them on a regular basis.38
Rare adverse events
Intoxication
The only published report of severe PER intoxication is based on a 34-year-old female German patient participating in a PER add-on trial at a daily dosage of 8 mg. She ingested the total remaining study medication of 204 mg (25.5 times of daily dose) at once in an attempt to commit suicide. This patient suffered from structural epilepsy due to tuberous sclerosis, was treated with three concomitant AEDs, appeared to have a normal intelligence quotient, and had no history of psychiatric disease. First signs of intoxication were dysarthria and tiredness leading to sopor (Glasgow Come Scale 8) with weak reflexes, no need of respiratory support, but impairment of consciousness with subsequent confusion and anxiety for a period of 2 days. Electroencephalogram showed generalized slowing but no epileptiform discharges; there were no laboratory abnormalities or serious ECG alterations. Due to rapid absorption of PER from the intestine, gastric lavage was not considered appropriate, and symptomatic treatment of somnolence and delirium was recommended.39
Suicidality
In a single institution, three cases of suicidality were reported among 23 patients treated with PER (for comparison, in Phase III trials, two cases of suicidality were noted in 1,038 patients, and in extension trials, six cases/1,200 patients). These three cases had refractory focal epilepsy in common as well as cognitive deficits to different degrees. In the beginning, emotional alterations preceding suicidal ideation occurring 3–8 weeks after PER introduction were not noted by the patients’ environment. Suicidal ideation followed after an interval of some weeks (8–16 weeks) at PER doses of 4–10 mg/day. All patients were nonresponders to PER treatment in terms of their seizure frequency. Suicidality was accompanied by other adverse effects like dizziness and blurred vision, evolving into sensitivity, irritability, and adversity or feeling thin-skinned, abnormally sensitive, and aggressive. In the third case, onset of symptoms was “bad thoughts” and repeated visualization of death-related “film scenes”. In cases 1 and 2, the phase of suicidality was accompanied by irritability and sensitivity, whereas case 3 had also signs of depression. Thus, depending on the preexisting disposition of patient cohorts, suicide risk might be higher than reported in controlled trials where patients with psychiatric disease are less common.40
Drug reaction with eosinophilia and systemic symptoms
A 13-year-old female patient with focal epilepsy and cognitive impairment with a baseline medication of lamotrigine and valproic acid developed a rash, cough, and fever as first symptoms 5 weeks after introduction of PER adjunctive treatment at a dose of 4 mg/day. After 1 week, she developed a lethargy combined with an increasing intensity of rash, hypotension, and acute respiratory distress syndrome. Leukocytes were elevated without eosinophilia, increased liver enzymes, acute renal failure with oliguria, and a perihilar infiltrate on chest X-ray. As she presented lesions surrounding lips and nose with xerosis, desquamation, and generalized erythroderma, a skin punch biopsy revealed superficial perivascular and interstitial lymphocytic/eosinophilic infiltrates indicating the diagnosis of a drug reaction with eosinophilia and systemic symptoms. After hospitalization, with interruption of all AEDs (suspecting PER as responsible), and treatment with methylprednisolone and low immunoglobulin G, her clinical status normalized. The alleged attribution to PER remains uncertain as all AEDs were stopped and as the patient was not reexposed to any of them.41
Laboratory abnormalities
Laboratory monitoring was performed in all regulatory and long-term extension trials. The incidence of laboratory abnormalities with adjunctive use of PER was low, and it remained undetermined if any of them were PER-related. Observed abnormalities in the largest long-term extension study55 included hyponatremia (3.7%; in 98% of patients in whom carbamazepine or oxcarbazepine was co-administered), low neutrophils (5.7%), or white cell counts (3.0%), which again are commonly found with various AEDs given as a baseline medication.
Recommended dosing and contraindications
The recommendations for dosage and administration vary between the US and Europe.29 As suggested by the above-mentioned open-label long trials, tolerability considerably depends on the dosing strategy. The best balance between efficacy and tolerability shows major variability between patients, necessitating an individual titration according to the patient’s clinical response and tolerability. The drug requires administration orally and is taken once daily before bedtime, with or without food. It should not be chewed, crushed, or split but swallowed whole with a glass of water.42 According to the long plasma half-life, there is a danger of overdosing when increasing intake at times when a steady state condition is not reached which would allow to assess safety and efficacy.
In Europe, the starting dose recommended is 2 mg/day followed by 2 mg/day increments until achieving a maintenance dose of 4–8 mg/day or up to a maximum target dose of 12 mg/day. It is advised that in patients without concomitant medicinal products that can shorten the half-life of PER or with mild/moderate hepatic impairment titration, increments should not exceed 2-week intervals. With concomitant enzyme inductors like carbamazepine, oxcarbazepine, phenytoin, and topiramate, they should not go below 1-week intervals. Although a risk of withdrawal seizures is unclear, dose reduction is recommended stepwise. Missing a single dose will have only minor effects on plasma levels due to the long half-time of the drug, and dosing should be continued without additional replacement in this case. If more doses have been missed but for a continuous period <5 half-lives, treatment should be resumed from the last dose level, and if misses exceed 5 half-lives, treatment should be restarted at initial dosing. In elderly people, no dose adjustment is recommended, but administration should be monitored carefully especially in polymedicated patients to account for possible drug interactions. Dose adjustments are not recommended with mild renal impairment, but PER use is not recommended in patients with moderate/severe renal impairment or severe hepatic impairment, or in patients undergoing hemodialysis. If mild or moderate hepatic impairment is present, reported dose and uptitration should be managed according to clinical response and tolerability, not exceeding 8 mg/day.24
In the US, treatment is recommended to start off at 2 mg/day without concomitant enzyme-inducing AED and at 4 mg/day with concomitant enzyme inducers. The titration is recommended with increments of 2 mg/week up to a maximum target dose of 12 mg/day or 6 mg/day in patients with mild hepatic impairment or 4 mg/day in patients with moderate hepatic impairment.43 This reflects the predominantly hepatic metabolism of the drug, which suggests that alterations in renal clearance will not have a major effect on PER plasma concentrations.
Use of PER is contraindicated in individuals with known hypersensitivity to any of the excipients or the active substance.24
For treatment during pregnancy, PER is categorized as substance with “developmental toxicity in animals; no adequate and well-controlled studies in pregnant women” belonging to category C43 in the US. The European product information does not recommend PER in women of childbearing potential without contraception and neither during pregnancy, even though data of pregnant women using PER are limited (<300) and animal trials have not reported any teratogenic effects in rats or rabbits, whereas embryotoxicity was witnessed. Also, at breastfeeding, PER is expected to be excreted in human milk leaving infants at risk.24
Patient adherence and acceptability
Key prerequisites for any successful long-term treatment as required for prophylactic intake of AEDs are compliance and adherence of patients to the recommended drug regimen. Aspects relevant for compliance and adherence are thus important when choosing between different treatment/drug options to guarantee optimal satisfaction and consequential efficiency. More than one-third of the reviewed patients in the safety analysis had a baseline medication with additional three AEDs. Treatment cohorts had a baseline median seizure frequency of 10–13/28 days, and more than two-thirds suffered from secondary generalized seizures. In the ITT analysis, 12% of the patients had also prior surgical treatment of their epilepsy, and 6% underwent vagal nerve stimulation. Even though the trials investigating efficacy, tolerability, and safety of the drug were thus performed in patient populations with several features of highly refractory epilepsy, PER is considered to be a well-tolerated and useful drug.34 The previously described long-term extension trials also point out that many, but not all, patients over time may tolerate doses of 10–12 mg. Whereas adverse events played a major role in patients discontinuing PER in the conversion and early treatment phase following randomized trials (in 52%/53% of patients withdrawing), it becomes a more and more rare reason for drug discontinuation over time, playing a role in about 10% of patients discontinuing after 84 weeks of treatment and more.32,33 Overall, most patients discontinuing the drug did so during the randomized blinded phases of the core trials and during conversion to high doses (overall retention about 70%), whereas during further treatment from weeks 35 to 150, about 60% of patients remained on the drug.32
Patient adherence depends on both tolerability and efficacy of treatment. The available long-term extension studies show constant responder rates over time: the median reduction in seizure frequency in one study was 43.7% after 1 year, 52% after 2 years, 49.7% after 3 years, and 48.4% after 4 years; 50% of responders similarly remained in the range of 43%–50%.44 A similar maintenance of efficacy was reported by Krauss et al.32 Responder rates were 32%–35% during the first 3 months, 42%–48% during months 4–6, 52% during months 7–9, and 58% after 10–12 months. Although these data do not give evidence for an increased efficacy over time as they are influenced by drop-outs, these data do not suggest the development of tolerance to the antiepileptic effect of PER over time.
Unlike talampanel, another studied AMPA receptor antagonist, PER advances with a long half-life in humans ensuring the sufficiency of a once-daily administration.45,46 The key role of a once-daily administration for improving compliance with intake has been proven both for AEDs and other medications applied in chronic diseases.47–49 Patient compliance and the prescribed number of doses per day were consistently found to correlate inversely.50
Given comparatively good long-term retention in open-label continuation studies, the infrequent neuropsychiatric side effect played a relevant role in drug withdrawal. Whereas somnolence and dizziness were the most frequently reported adverse effects, bedtime dosing can pass peak plasma levels during sleep.
Slow introduction may additionally promote a reduction in central nervous system toxic adverse reactions.45 In elderly patients, falls, dizziness, and fatigue as potential adverse effects may be more important.51 There are so far insufficient data as to whether there are specific risks of low tolerability in patients with intellectual disability and behavioral problems, as suggested from one case report.52 Similarly, the role of a history of psychiatric disease in the risk of developing PER-related neuropsychiatric adverse effects needs further study.36
Observational reports on patient cohorts may contribute to improve the understanding of factors relevant to tolerability and efficacy. For example, a retrospective analysis of experiences in German and Austrian epilepsy centers reported acceptable tolerability and seizure-free periods of 3 months in 15% of patients.53
Discussion
PER has proven to be an effective new antiepileptic treatment of partial-onset seizures with a novel mechanism of action, noncompetitive antagonism at the AMPA receptor. Its rather specific modulation of this glutamate subreceptor is assumed to exert its antiepileptic action by reducing excitability, relatively independent of presynaptic transmitter release.54 This novel mechanism opens up new options for a rational combination therapy in focal epilepsy. Aside from this new pharmacodynamic approach, the pharmacokinetic profile is also attractive: the long plasma half-time allows for once-daily dosing, favorable for long-term adherence.22 Relevant pharmacokinetic interactions with other AEDs are limited to an elevation of oxcarbazepine levels, whereas the presence of enzyme inducers may shorten the half-life and thus decrease efficacy of PER. Overall, the handling of the drug in adjunctive therapy of epilepsy is easy for prescribing physicians and for patients.
Not only in short-term treatment during regulatory trials but also in prospective open-label trials, efficacy and tolerability were overall good with favorable retention rates over periods of 1–4 years.44 In a comprehensive review of safety data35 also, weight gain was found in PER-treated patients. Even if the mean weight gain on average was low (mean 0.8 kg overall), individual weight increases may be disturbing, and it remains to be seen if this can be an unwanted effect leading to drug withdrawal in patients carefully monitoring their weight. With <1% increases in liver function tests and <2% increases in creatine kinase (CK), laboratory tests did not raise safety concerns so far.55
Whereas overall tolerability is regarded as good, there are concerns about neuropsychiatric adverse effects, including irritability, aggressive behavior, changes in mood, and even suicidality; these unwanted effects occurred at a total rate of <5% in prospective regulatory and extension trials but were highlighted in individual case reports. A higher rate of psychiatric side effects in specific subpopulations compared to published trials may be related to the exclusion of patients with recently manifest psychiatric disease from controlled studies, in contrast to a relevant prevalence of psychiatric disease in the overall group of patients with pharmacoresistant focal epilepsy.56 Whereas central nervous system toxic side effects like somnolence and dizziness may occur at individual thresholds but are clearly dose-related in their incidence, neuropsychiatric side effects may individually occur at various dosages, including the common starting dose for long-term treatment of 4 mg/day.37 In individual case reports, neuropsychiatric side effects mostly occurred during titration or within several weeks after dose increases, whereas in long-term studies, few new treatment-emergent adverse effects were found. A close monitoring of tolerability is thus advisable already during early titration, in particular when patients with a history of psychiatric disease and possibly with a background of intellectual disability are treated.
Long-term data do not give evidence of loss of efficacy over time due to tolerance. In contrast, individual uptitration to high dosages may improve in particular the control of generalized tonic–clonic seizures.31 Thus, long-term treatment may offer efficacy gain with individually selected high PER doses. It remains an important result of studies, however, that efficacy of adjunctive PER treatment starts at relatively low dosages and that many patients do not need to have doses increased beyond a daily dose of 8 mg. Like with other drugs with long plasma half-time, a slow and deliberate drug introduction and a careful analysis of efficacy and tolerability considering the time periods needed to reach steady state are crucial to obtain the best efficacy in the individual patient.
Experience with PER is limited. There are yet open questions as to which combinations with other drugs of different mechanisms of action provide best efficacy and possibly synergy with PER, and if the concomitant administration of enzyme-inducing AED which reduces PER plasma levels impairs its efficacy in clinical practice.57,58
Disclosure
The authors received no financial or other support from the pharmaceutical industry for the preparation of this manuscript. Andreas Schulze-Bonhage has received honoraria for lectures and advice from Cyberonics, Desitin, EISAI, Precisis, and UCB. Mandy Hintz has no disclosures. The authors report no other conflicts of interest in this work.
References
Watkins JC, Jane DE. The glutamate story. Br J Pharmacol. 2006;147(suppl 1):S100–S108. | ||
Meldrum BS, Rogawski MA. Molecular targets for antiepileptic drug development. Neurotherapeutics. 2007;4(1):18–61. | ||
Harris LW, Sharp T, Gartlon J, Jones DNC, Harrison PJ. Long-term behavioural, molecular and morphological effects of neonatal NMDA receptor antagonism. Eur J Neurosci. 2003;18(6):1706–1710. | ||
Janać B, Selaković V, Radenović L. Temporal patterns of motor behavioural improvements by MK-801 in Mongolian gerbils submitted to different duration of global cerebral ischemia. Behav Brain Res. 2008;194(1):72–78. | ||
Wedzony K, Fijal K, Mackowiak M, Chocyk A, Zajaczkowski W. Impact of postnatal blockade of N-methyl-D-aspartate receptors on rat behavior: a search for a new developmental model of schizophrenia. Neuroscience. 2008;153(4):1370–1379. | ||
Nabeshima T, Mouri A, Murai R, Noda Y. Animal model of schizophrenia: dysfunction of NMDA receptor-signaling in mice following withdrawal from repeated administration of phencyclidine. Ann N Y Acad Sci. 2006;1086:160–168. | ||
Freedman R. Schizophrenia. N Engl J Med. 2003;349(18):1738–1749. | ||
Croucher MJ, Collins JF, Meldrum BS. Anticonvulsant action of excitatory amino acid antagonists. Science. 1982;216(4548):899–901. | ||
Löscher W, Hönack D. The novel competitive N-methyl-D-aspartate (NMDA) antagonist CGP 37849 preferentially induces phencyclidine-like behavioral effects in kindled rats: attenuation by manipulation of dopamine, alpha-1 and serotonin1A receptors. J Pharmacol Exp Ther. 1991;257(3):1146–1153. | ||
Sveinbjornsdottir S, Sander JW, Upton D, et al. The excitatory amino acid antagonist D-CPP-ene (SDZ EAA-494) in patients with epilepsy. Epilepsy Res. 1993;16(2):165–174. | ||
Albers GW, Atkinson RP, Kelley RE, Rosenbaum DM. Safety, tolerability, and pharmacokinetics of the N-methyl-D-aspartate antagonist dextrorphan in patients with acute stroke. Dextrorphan Study Group. Stroke. 1995;26(2):254–258. | ||
Lees KR. Cerestat and other NMDA antagonists in ischemic stroke. Neurology. 1997;49(5 suppl 4):S66–S69. | ||
Chappell AS, Sander JW, Brodie MJ, et al. A crossover, add-on trial of talampanel in patients with refractory partial seizures. Neurology. 2002;58(11):1680–1682. | ||
Szabados T, Gigler G, Gacsályi I, Gyertyán I, Lévay G. Comparison of anticonvulsive and acute neuroprotective activity of three 2,3-benzodiazepine compounds, GYKI 52466, GYKI 53405, and GYKI 53655. Brain Res Bull. 2001;55(3):387–391. | ||
Chapman AG, Smith SE, Meldrum BS. The anticonvulsant effect of the non-NMDA antagonists, NBQX and GYKI 52466, in mice. Epilepsy Res. 1991;9(2):92–96. | ||
Yamaguchi S, Donevan SD, Rogawski MA. Anticonvulsant activity of AMPA/kainate antagonists: comparison of GYKI 52466 and NBOX in maximal electroshock and chemoconvulsant seizure models. Epilepsy Res. 1993;15(3):179–184. | ||
Chen C-Y, Matt L, Hell JW, Rogawski MA. Perampanel inhibition of AMPA receptor currents in cultured hippocampal neurons. PLoS One. 2014;9(9):e108021. | ||
Citraro R, Aiello R, Franco V, De Sarro G, Russo E. Targeting α-amino-3-hydroxyl-5-methyl-4-isoxazole-propionate receptors in epilepsy. Expert Opin Ther Targets. 2014;18(3):319–334. | ||
Dirani M, Nasreddine W, Abdulla F, Beydoun A. Seizure control and improvement of neurological dysfunction in Lafora disease with perampanel. Epilepsy Behav Case Rep. 2014;2:164–166. | ||
Hanada T, Hashizume Y, Tokuhara N, et al. Perampanel: a novel, orally active, noncompetitive AMPA-receptor antagonist that reduces seizure activity in rodent models of epilepsy. Epilepsia. 2011;52(7): 1331–1340. | ||
Gigler G, Móricz K, Agoston M, et al. Neuroprotective and anticonvulsant effects of EGIS-8332, a non-competitive AMPA receptor antagonist, in a range of animal models. Br J Pharmacol. 2007;152(1):151–160. | ||
Schulze-Bonhage A. Perampanel for epilepsy with partial-onset seizures: a pharmacokinetic and pharmacodynamic evaluation. Expert Opin Drug Metab Toxicol. 2015;11(8):1329–1337. | ||
Patsalos PN. The clinical pharmacology profile of the new antiepileptic drug perampanel: a novel noncompetitive AMPA receptor antagonist. Epilepsia. 2015;56(1):12–27. | ||
European Medicines Agency EMA. Fycompa SPC. Perampanel (Fycompa). Summary of Product Characteristics; [updated November 13,2013]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002434/WC500130815.pdf | ||
US Food and Drug Administration FDA. Clinical Pharmacologyreview; 2012. Reference ID: 3205587. Available from: http://www.fda.gov/downloads/Drugs/DevelopmentApprovalProcess/DevelopmentResources/UCM332052.pdf | ||
French JA, Krauss GL, Biton V, et al. Adjunctive perampanel for refractory partial-onset seizures randomized phase III study 304. Neurology. 2012;79(6):589–596. | ||
French JA, Krauss GL, Steinhoff BJ, et al. Evaluation of adjunctive perampanel in patients with refractory partial-onset seizures: results of randomized global phase III study 305: Perampanel for Partial-Onset Seizures. Epilepsia. 2013;54(1):117–125. | ||
Krauss GL, Serratosa JM, Villanueva V, et al. Randomized phase III study 306: adjunctive perampanel for refractory partial-onset seizures. Neurology. 2012;78(18):1408–1415. | ||
Franco V, Crema F, Iudice A, Zaccara G, Grillo E. Novel treatment options for epilepsy: focus on perampanel. Pharmacol Res. 2013;70(1):35–40. | ||
Krauss GL, Bar M, Biton V, et al. Tolerability and safety of perampanel: two randomized dose-escalation studies: tolerability and safety of perampanel. Acta Neurol Scand. 2012;125(1):8–15. | ||
Kramer LD, Satlin A, Krauss GL, et al. Perampanel for adjunctive treatment of partial-onset seizures: a pooled dose-response analysis of phase III studies. Epilepsia. 2014;55(3):423–431. | ||
Krauss GL, Perucca E, Ben-Menachem E, et al. Long-term safety of perampanel and seizure outcomes in refractory partial-onset seizures and secondarily generalized seizures: results from phase III extension study 307. Epilepsia. 2014;55(7):1058–1068. | ||
Rektor I, Krauss GL, Bar M, et al. Perampanel Study 207: long-term open-label evaluation in patients with epilepsy. Acta Neurol Scand. 2012;126:263–269. | ||
Steinhoff BJ, Ben-Menachem E, Ryvlin P, et al. Efficacy and safety of adjunctive perampanel for the treatment of refractory partial seizures: a pooled analysis of three phase III studies. Epilepsia. 2013;54(8):1481–1489. | ||
Serratosa JM, Villanueva V, Kerling F, Kasper BS. Safety and tolerability of perampanel: a review of clinical trial data. Acta Neurol Scand Suppl. 2013;197:30–35. | ||
Faulkner MA. Perampanel: a new agent for adjunctive treatment of partial seizures. Am J Health Syst Pharm. 2014;71(3):191–198. | ||
Coyle H, Clough P, Cooper P, Mohanraj R. Clinical experience with perampanel: focus on psychiatric adverse effects. Epilepsy Behav. 2014;41:193–196. | ||
Faulkner MA, Burke RA. Safety profile of two novel antiepileptic agents approved for the treatment of refractory partial seizures: ezogabine (retigabine) and perampanel. Expert Opin Drug Saf. 2013;12(6):847–855. | ||
Hoppner AC, Fauser S, Kerling F. Clinical course of intoxication with the new anticonvulsant drug perampanel. Epileptic Disord. 2013;15(3):362–364. | ||
Huber B. Increased risk of suicidality on perampanel (Fycompa®)? Epilepsy Behav. 2014;31:71–72. | ||
Shimabukuro K, Gibbon F, Kerstetter J, Tinsley C, Ashwal S. DRESS associated with perampanel administration in a child with drug-resistant epilepsy. Neurology. 2014;83(23):2188–2189. | ||
EU0031-crushing and dissolving Fycompa, alternative routes of administration.pdf. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002434/WC500130815.pdf. Accessed July 1, 2015 | ||
[No authors listed] Perampanel (Fycompa) for epilepsy. Med Lett Drugs Ther. 2014;56(1435):9–10. | ||
Rektor I. Perampanel, a novel, non-competitive, selective AMPA receptor antagonist as adjunctive therapy for treatment-resistant partial-onset seizures. Expert Opin Pharmacother. 2013;14(2):225–235. | ||
Templeton D. Pharmacokinetics of perampanel, a highly selective AMPA-type glutamate receptor antagonist. Epilepsia. 2009;50(suppl 11):98. | ||
Gidal BE, Majid O, Ferry J, et al. The practical impact of altered dosing on perampanel plasma concentrations: pharmacokinetic modeling from clinical studies. Epilepsy Behav. 2014;35:6–12. | ||
Cramer J, Vachon L, Desforges C, Sussman NM. Dose frequency and dose interval compliance with multiple antiepileptic medications during a controlled clinical trial. Epilepsia. 1995;36(11):1111–1117. | ||
Parienti J, Bangsberg DR, Verdon R, Gardner EM. Better adherence with once-daily antiretroviral regimens: a meta-analysis. Clin Infect Dis. 2009;48(4):484–488. | ||
Saini SD, Schoenfeld P, Kaulback K, Dubinsky MC. Effect of medication dosing frequency on adherence in chronic diseases. Am J Manag Care. 2009;15(6):e22–e33. | ||
Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose regimens and medication compliance. Clin Ther. 2001;23(8):1296–1310. | ||
Leppik IE, Wechsler RT, Williams B, Yang H, Zhou S, Laurenza A. Efficacy and safety of perampanel in the subgroup of elderly patients included in the phase III epilepsy clinical trials. Epilepsy Res. 2015;110:216–220. | ||
Dolton E, Choudry A. Perampanel and challenging behaviour in intellectual disability and epilepsy: a management dilemma. Case Rep Psychiatry. 2014;2014:1–3. | ||
Steinhoff BJ, Hamer H, Trinka E, et al. A multicenter survey of clinical experiences with perampanel in real life in Germany and Austria. Epilepsy Res. 2014;108(5):986–988. | ||
Rogawski MA. AMPA receptors as a molecular target in epilepsy therapy. Acta Neurol Scand. 2013;127:9–18. | ||
Krauss GL, Perucca E, Ben-Menachem E, et al. Perampanel, a selective, noncompetitive α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor antagonist, as adjunctive therapy for refractory partial-onset seizures: Interim results from phase III, extension study 307. Epilepsia. 2013;54(1):126–134. | ||
Hellwig S, Mamalis P, Feige B, Schulze-Bonhage A, van Elst LT. Psychiatric comorbidity in patients with pharmacoresistant focal epilepsy and psychiatric outcome after epilepsy surgery. Epilepsy Behav. 2012;23(3):272–279. | ||
Wu T, Nagaya Y, Hanada T. Pharmacodynamic and pharmacokinetic interactions of perampanel and other antiepileptic drugs in a rat amygdala kindling model. Seizure. 2014;23(9):732–739. | ||
Gidal BE, Ferry J, Majid O, Hussein Z. Concentration-effect relationships with perampanel in patients with pharmacoresistant partial-onset seizures. Epilepsia. 2013;54(8):1490–1497. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.