")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Peony-Glycyrrhiza Decoction for Antipsychotic-Related Hyperprolactinemia in Patients with Schizophrenia: A Randomized Controlled Trial
Authors Wang Z , Zheng Y, Fan Y, Fan Y, Su X, Wang B, Li J, Chen D, Sun F, Li S, Ma J, Li X, Bai L, Li R
Received 12 February 2023
Accepted for publication 7 April 2023
Published 17 April 2023 Volume 2023:19 Pages 929—938
DOI https://doi.org/10.2147/NDT.S408314
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Zhongbao Wang,1 Yunshao Zheng,2 Yunli Fan,2 Yunming Fan,2 Xianbiao Su,2 Bingrui Wang,2 Jing Li,2 Diancai Chen,2 Fengxia Sun,2 Shen Li,2 Jiashu Ma,1 Xianwei Li,2 Ludong Bai,2 Ranran Li2
1Department of Psychiatry, Jining Medical University, Jining, People’s Republic of China; 2Department of Psychiatry, Shandong Mental Health Center, Shandong University, Jinan, People’s Republic of China
Correspondence: Ranran Li, Department of Psychiatry, Shandong Mental Health Center, Shandong University, 49 East Wenhua Road, Jinan, Shandong, 250014, People’s Republic of China, Tel +86 18678777190, Email [email protected]
Background: Most antipsychotic drugs are dopamine receptor antagonists that usually lead to abnormal increases in prolactin concentrations and the development of hyperprolactinemia (HPRL), which in turn causes sexual dysfunction in patients. Peony-Glycyrrhiza Decoction (PGD) enhanced dopamine D2 receptors (DRD2) and dopamine transporter (DAT) and significantly reversed the expression of DRD2 and DAT. Therefore, we hypothesized that PGD might effectively improve hyperprolactinemia and alleviate sexual dysfunction in patients.
Methods: We performed an 8-week randomized controlled study on 62 subjects with schizophrenia who were randomized into two groups. The experimental group was treated with the PGD intervention, and the control group did not receive treatment. The primary outcome indicators were the levels of sex hormones and the total Arizona Sexual Experience Scale (ASEX) score.
Results: There was a significant difference in PRL levels between the two groups at weeks 4 and 8. From the beginning to the end of the experiment, there was a significant increase in PRL levels in the control group, while there was no significant change in the experimental group. The ASEX scale assessed sexual function in both groups, and patients in the experimental group showed an improvement in sexual function at week 8. During the experiment, the two groups found no differences between Positive and Negative Syndrome Scale (PANSS) scores and Treatment Emergent Symptom Scale (TESS) scores.
Conclusion: PGD significantly improved the patient’s sexual function but was less effective in reducing prolactin levels and may prevent further increases in prolactin levels.
Keywords: hyperprolactinemia, antipsychotics, Peony-Glycyrrhiza Decoction, schizophrenia, sexual function, adverse effects
Introduction
In 2016, mental and addictive disorders affected more than 1 billion people worldwide. Measured by DALYs, they contribute to 7% of the global burden of disease and 19% of disabled life years.1,2 The use of antipsychotic medication remains the primary treatment to stabilize patients’ psychotic symptoms and to help them regain social function and return to society.3,4 However, long-term use of antipsychotic drugs may lead to many adverse effects, such as neurological extrapyramidal reactions, hematological leukopenia, endocrine system prolactin (PRL), and metabolic disorders.5 It greatly affects patients’ physical health, treatment compliance, and treatment outcome. If adverse reactions are not controlled in a timely manner, patients may develop discontinuation dilemma, leading to disease relapse.6
Hyperprolactinemia (HPRL) is a common adverse effect of antipsychotic medications. HPRL occurs in 70% of patients with schizophrenia treated with antipsychotic medications.7 HPRL is usually defined as a fasting serum PRL level >25 ng/mL in women and >20 ng/mL in men after 2 h in the morning.8 HPRL causes a range of physical reactions, including male breast development, breast overflow, sexual dysfunction, infertility, oligomenstrual flow, and amenorrhea.9,10 Long-term adverse effects can reduce patient compliance; in particular, sexual dysfunction often aggravates the patient’s disease stigma, thereby affecting the patient’s family relationships and making treatment difficult.
Therefore, the treatment of HPRL caused by antipsychotic medications is essential. First-line management includes reducing the dose of the offending antipsychotic, discontinuing the antipsychotic, or switching to another antipsychotic associated with a reduced risk of HPRL. Other treatment options include adjunctive treatment with aripiprazole, dopamine agonists (cartegolines, bromocriptine, and topiramate), and metformin.11,12 Bromocriptine, a dopamine receptor agonist, is a specific drug for HPL that can exacerbate psychotic symptoms and cause abnormal involuntary movements. Although metformin causes urinary excretion of PRL levels, metformin decreases prolactin levels only if given at high doses (2550 ~3000 mg/d) to patients with elevated prolactin levels.13 Aripiprazole can reduce antipsychotic-induced HPRL, but it can also cause adverse effects, such as sedation, insomnia, and headache.14 The combination of two antipsychotics increases the incidence of adverse effects. Changing medication or reducing the dose of antipsychotics may lead to other side effects or increase the risk of relapse.15,16
In recent years, traditional Chinese medicine has received an increasing amount of attention in the study of HPRL caused by antipsychotic drugs. Previous studies have found that Peony-Glycyrrhiza Decoction (PGD) can increase the binding capacity of dopamine receptors,17 inhibit the release of prolactin, and significantly reduce the level of prolactin caused by risperidone.18 Currently, the evidence supporting the use of PGD in the treatment of antipsychotic-induced hyperprolactinemia is limited. The conclusion of a meta-analysis that included five randomized controlled trials supports the adjunctive use of PGD in patients with hyperprolactinemia;19 however, the authors also acknowledge that the evidence included has some limitations, and further experiments are still needed to verify the effectiveness of PGD for hyperprolactinemia.
We report an 8-Week randomized controlled trial that tested the effects of PGD on prolactin levels and improvements in sexual function under antipsychotic medication. The safety and impact of this intervention on psychotic symptoms were evaluated.
Method
Participants
Subjects were recruited from inpatients in Shandong Mental Health Center. The study protocol was approved by the medical ethical committee of all hospitals involved before patient recruitment and registered on www.chictr.org.cn (ChiCTR2100050218). All participants and their guardians gave voluntary, informed consent before starting the trial.
Only patients who met the following criteria were included. 1) The type of antipsychotic drug remained unchanged, and the dose used was stable within the effective amount. 2) The diagnostic standard for The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5)20 schizophrenia was fulfilled. 3) The patient had stable mental state, stable treatment for at least 2 months, and Positive and Negative Syndrome Scale (PANSS) scores21 of less than 70. 4) The level of serum PRL was higher than 24 ng/mL.12,22 5) The patient showed sexual dysfunction. Patients with a total Arizona Sexual Experience Scale (ASEX) score of ≧19, any entry of ≧5, or their total 3 entries of ≧4 were considered to have sexual dysfunction. 6) The patient was 18–55 years old. 7) The patient showed no major medical abnormalities, including central nervous system diseases, acute, unstable, or life-threatening medical illnesses (eg, cancer and infections). Patients who had any of the following conditions were excluded from the study: (1) PRL pituitary adenoma, polycystic ovary syndrome, and other serious somatic diseases; (2) a history of neuroleptic malignant syndrome or tardive dyskinesia; (3) suicide ideas or attempts or aggressive behavior; (4) a history of alcoholism and drug abuse in the past 1 year; (5) currently being treated with other endocrine drugs, Chinese medicine, and other natural products; (6) a history of allergy to herbal medicine.
Study Design
This is a randomized controlled study that included 62 patients. Patients were randomized into a control group (n = 30) and an experimental group (n = 32). Patients’ baseline characteristics were tested before this study.
The control group was not treated. The experimental group was given PGD. PGD is produced by Shandong Bokang Traditional Chinese Medicine Co., Ltd. and complies with the Chinese Pharmacopoeia and the Good Manufacturing Practice for Medical Products. White peony (60 mg) and licorice (30 mg) were soaked in eight times the volume of distilled water at a ratio of 2:1 by weight and boiled for 2.5 h.
The contents of the three known pharmacologically active components (Paeoniflorin, Liquiritin, and Glycyrrhizic acid) in PGD were determined by reversed-phase high performance liquid chromatography (HPLC), as shown in Figure 1. It was highly comparable with the PGD used in previous studies.23
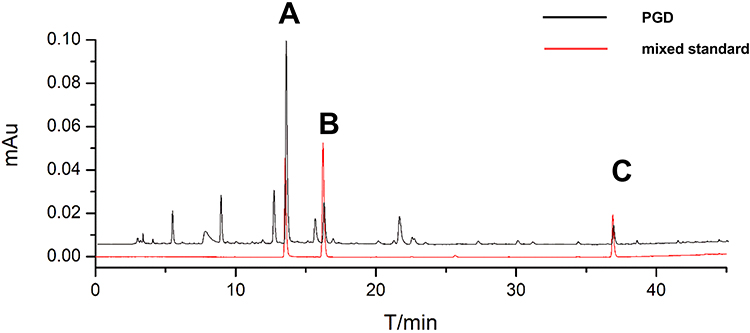 |
Figure 1 Liquid chromatogram of PGD sample and mixed standard, (A), Paeoniflorin. (B), Liquiritin. (C), Glycyrrhizic acid. |
Participants were randomly assigned to an experimental or control group for eight consecutive weeks. They were asked not to change their antipsychotic medication during the intervention. This was monitored at monthly visits. During the study, patients were allowed to receive concomitant treatment with other psychotropic medications. These drugs mainly included drugs for the treatment of extrapyramidal symptoms and insomnia. During the study period, the concomitant use of different herbal and natural products was not permitted.
Measures
All measurements were conducted at baseline and at weeks 4 and 8. Blood samples were tested in the laboratory department of the hospital. The serum concentrations of PRL, estradiol, progesterone, testosterone, FSH, and LH were determined. We used the scale of Treatment Emergent Symptom Scale (TESS)24 to evaluate the side effects of medication in both group.
Clinical symptoms of schizophrenia were assessed using the PANSS at the start of treatment and at 4 and 8 weeks after treatment. The sexual function of the patients at the beginning of the experiment and after the investigation was assessed using the ASEX.25,26 In addition, some unusual adverse reactions such as amenorrhea, irregular menstruation, and non-lactation lactation were recorded.
Statistical Analysis
Statistical analyses were conducted with the Statistical Package for the Social Sciences version 27.0 (SPSS 27.0). Descriptive statistics (mean and standard deviation) were calculated for continuous variables. Categorical data were expressed as frequencies or percentages. Pearson’s χ2 or Fisher’s exact tests were used for categorical variables. Analysis of Covariance (ANOVA) was used to analyze the ASEX scores between the two groups. Generalized estimating equations (GEEs) were used to analyze changes in outcomes before and after treatment in patients with hyperprolactinemia. The quasi-likelihood under the independent model criterion (QIC) value indicates whether the work-related matrix applies to GEE. The lower the QIC value, the better the fitting of the model to the data. The difference in sex hormones and PANSS scores between the two groups was calculated using intention-to-treat (ITT) analysis. After statistical analysis, a value of p less than 0.05 indicated a statistically significant difference.
Results
Baseline Characteristics of Patients
There were 32 patients in the experimental group, among which 21 were male, and 11 were female; 27 patients completed the experiment. They were 18–55 years old, with an average age of 33.03±11.28 years old. The years of education were 1–19 years. The average years of education were 12.28±3.38 years, and the average disease duration was 10.25±9.32 years. There were 30 patients in the control group, among which 14 were male, and 16 were female; 28 patients completed the experiment. They were 18–52 years old, with an average age of 37.77±10.26 years old. The years of education were 6–22 years (average, 13.20±3.78 years). The average disease duration was 10.36±8.93 years. Among the dropout cases in the experimental group, two patients were lost due to serious adverse drug reactions (one patient had acute dystonia after taking the drug, and one had obvious akathisia), one patient changed antipsychotic drugs due to fluctuating condition, and 2 were lost to follow-up after discharge. In the control group, one patient dropped out because of family-related reasons, and one patient was lost due to fluctuating condition. The baseline characteristics of patients are shown in Table 1. No significant differences in baseline variables were observed between these two groups.
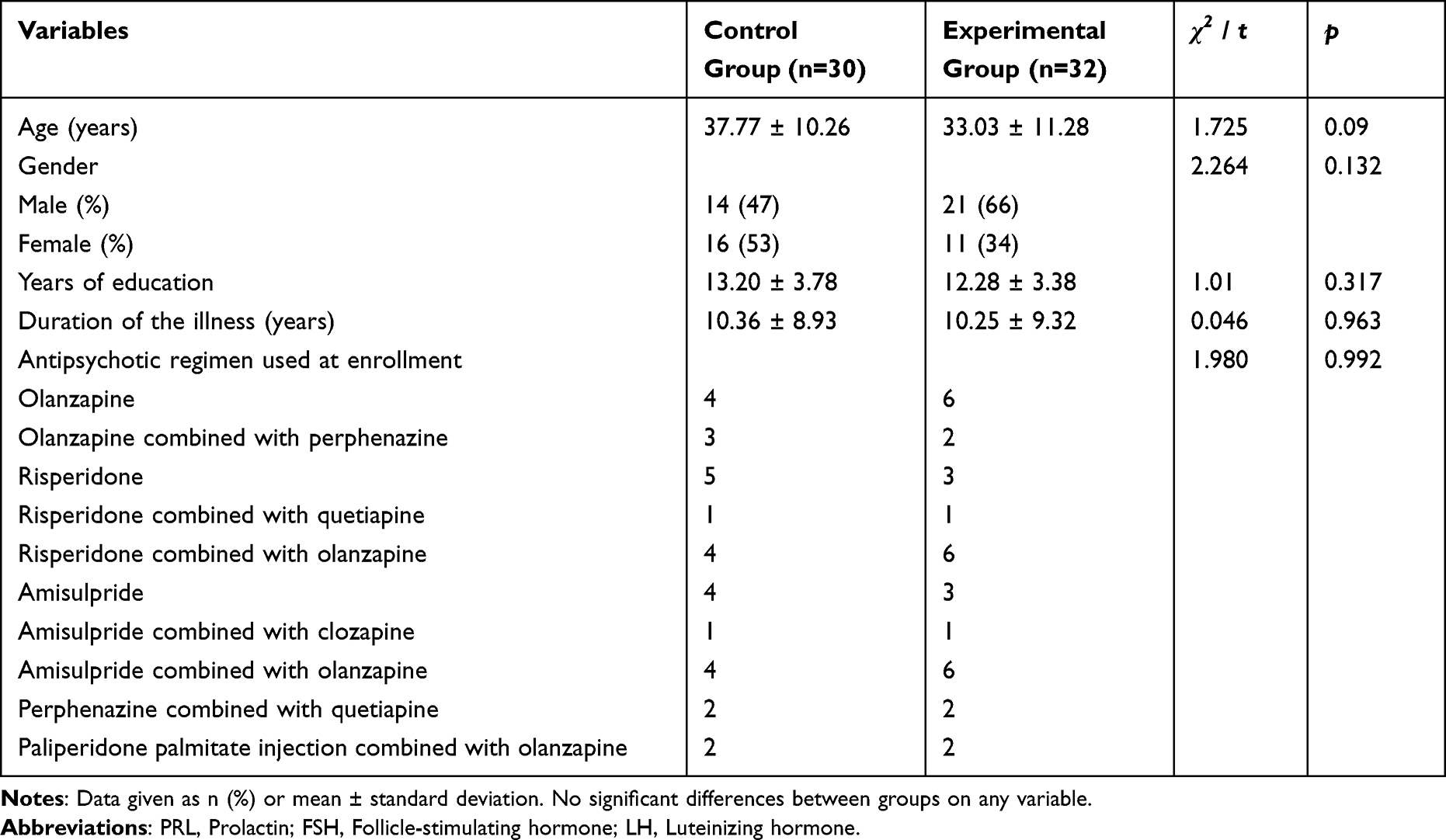 |
Table 1 Baseline Characteristics of Participant |
Antipsychotic Regimen Used at Enrollment
In the beginning, no significant difference was found in the antipsychotic regimen between the two groups (Table 1); 40.3% (25/62) used antipsychotic monotherapy, and 59.7% (37/62) used multiple antipsychotics. The most commonly used antipsychotics among all subjects were olanzapine combined with risperidone (16.1%, 10/62), olanzapine combined with amisulpride (16.1%, 10/62), olanzapine (16.1%, 10/62), risperidone (12.9%, 8/62), amisulpride (11.3%, 7/62), perphenazine combined with olanzapine (8.1%, 5/62), and other drugs (19.4%, 12/62). The antipsychotic regimen of patients who followed patients who completed the entire treatment and evaluation according to the protocol remained unchanged throughout the study period. It was occasionally combined with benzhexol and benzodiazepines for tremor and insomnia, respectively.
Levels of PRL and Other Hormones
The results of the hormone assays are concluded in Table 2 and Table 3 and Figure 2. The serum levels of testosterone, FSH, progesterone, estradiol, and LH were not significantly different between the 2 groups.
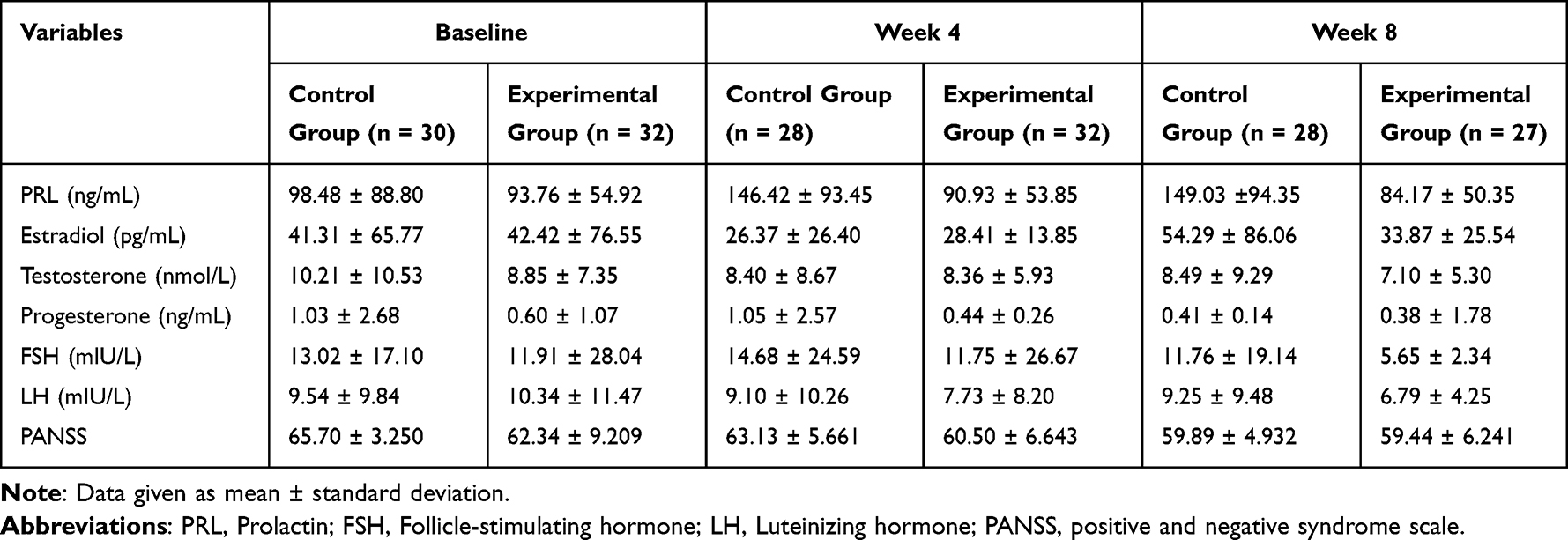 |
Table 2 Changes in Sex Hormones Levels and PANSS Scores Before and After the Study |
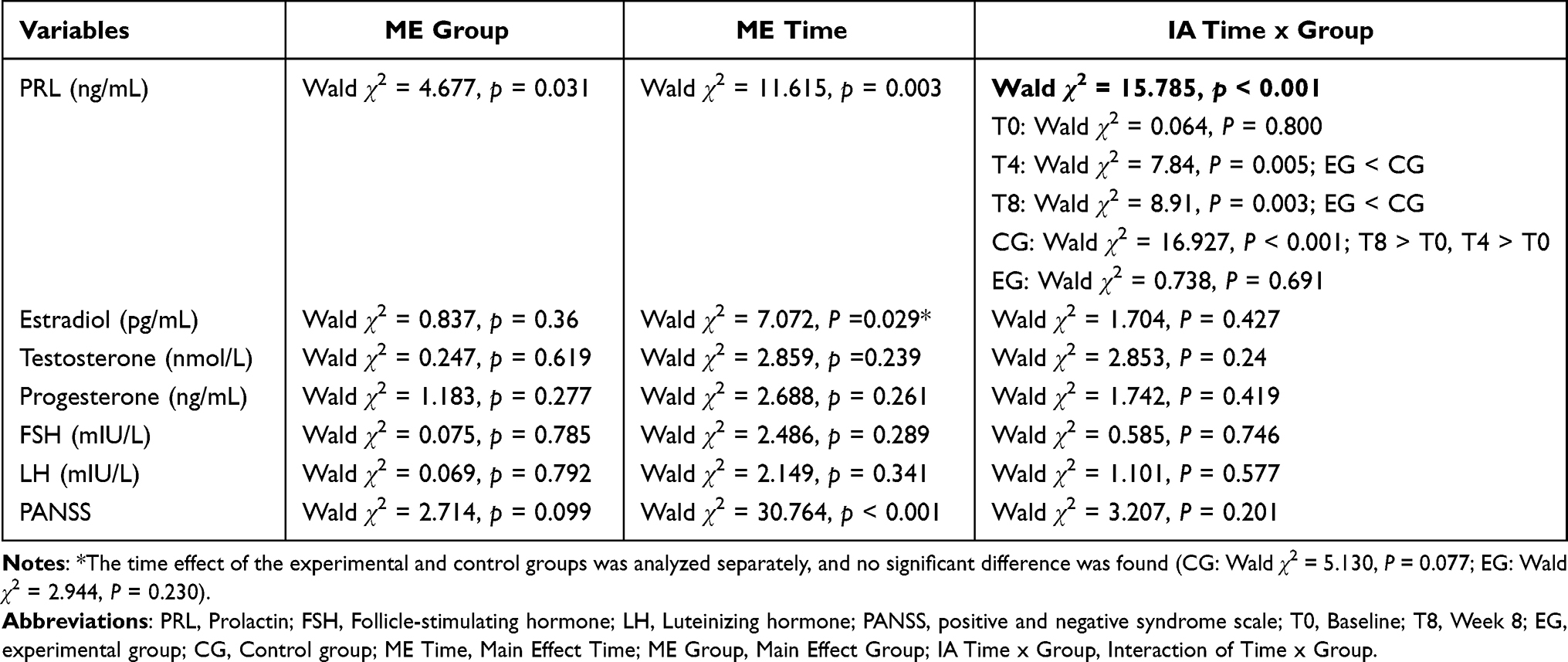 |
Table 3 Statistical Analysis of Hormones Levels and PANSS Scores (Generalized Estimating Equation with the Factors Group and Time) |
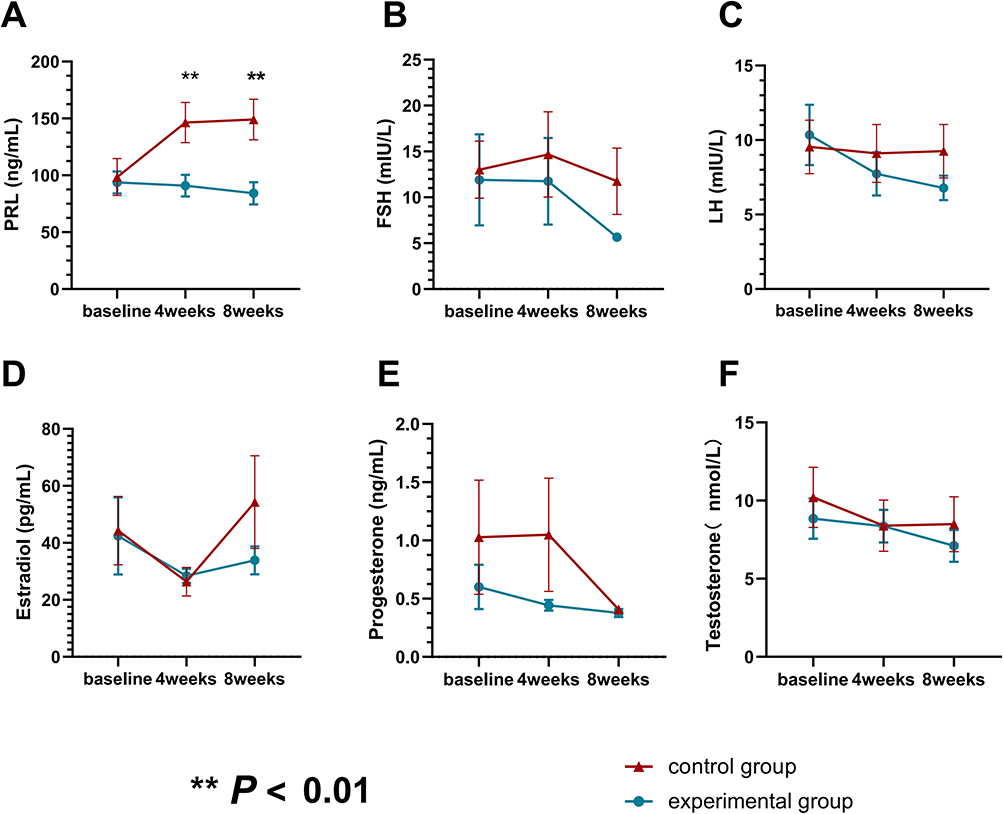 |
Figure 2 The changes in prolactin and other sex hormones between the experimental group and the control group during the experiment. Mean levels of PRL (A), FSH (B), LH (C), Estradiol (D), Testosterone (E) and Progesterone (F) in the study group. Error bars represent standard error. The differences between the two treatment groups at each time point were compared by calculating simple effects and obtaining the between-group effects at different times. (**p < 0.01). |
The comparison of PRL serum levels in the two groups revealed a significant interaction effect, which was further analyzed simple effect. Simple effect results showed statistically significant PRL levels between the two groups at week 4 (Wald χ2 = 7.84, P = 0.005) and week 8 (Wald χ2 = 8.91, P = 0.003). In the experimental group, the simple effect results showed no significant effect of time on PRL serum levels (Wald χ2 = 0.738, P = 0.691), indicating no significant change in PRL serum levels over time (baseline vs week 4, P=0.621; baseline vs week 8, P=0.431). And the simple effect results showed a significant time effect on PRL serum levels in the control group (Wald χ2 = 16.927, P <0.001), indicating an increase in PRL serum levels over time (baseline vs week 4, P < 0.001; baseline vs week 8, P < 0.001).
The Arizona Sexual Experience Scale (ASEX) Scores and Improvement of Other Symptoms (Table 4)
The ASEX scale has five questions, which correspond to five areas: sex drive, sexual arousal, vaginal lubrication (female)/penile erection (male), orgasmic ability, and sexual satisfaction. Each question was scored from 1 to 6 on a scale ranging from hyperfunctioning to hypofunctioning. Patients in the experimental group showed statistically significant changes in the ASEX scores (from 21.72±3.02 to 17.63±2.06; P < 0.001).
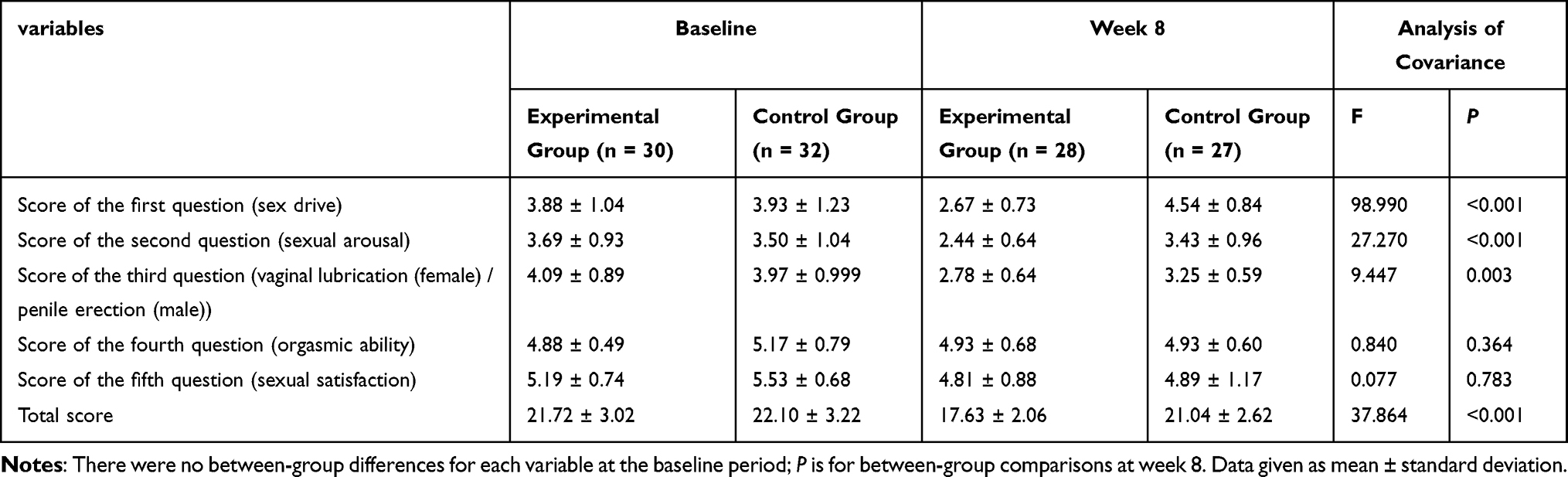 |
Table 4 ASEX Scores for Both Groups Before and After the Experiment |
The analysis revealed no significant differences between the two groups in the scores on question 4, representing orgasmic ability, and question 5, representing satisfaction. Comparing the scores for the first, second, and third questions and the total score in the two groups revealed significant differences at week 8, with the experimental group scoring significantly lower than the control group (P < 0.05). So the patients in the experimental group showed some improvement in sexual dysfunction, mainly in three areas: sexual drive, sexual arousal, and vaginal lubrication (female) / penile erection (male).
Other Symptoms
In the experimental group, there were five patients with menstrual irregularities, two with amenorrhea, and one with non-lactating lactation. In the control group, there were ten patients with menstrual irregularities. During the experiment, four patients with menstrual irregularities, two patients with amenorrhea, and one patient with non-lactating lactation in the experimental group returned to normal. However, only two patients with menstrual irregularities in the control group recovered to normal at the end of the study.
Treatment Emergent Symptom Scale (TESS)
No significant difference was found in TESS scores between the two groups (control group: 11.21±3.91; experimental group: 11.19±2.63, p = 0.974) at the end of the study. The adverse reactions that occurred during the treatment were: insomnia, abnormal liver function, dry mouth, increased saliva, nausea or vomiting, headache, constipation, and electrocardiographic abnormalities without clinical significance. All patients with symptoms were given appropriate treatment, or clinical observation was continued.
Positive and Negative Syndrome Scale (PANSS) Scores (Table 2 and Table 3)
There was no statistically significant difference in PANSS scores between the two groups from the beginning to the end of the study (Wald χ2 = 2.714, p = 0.099). The effect of time on PANSS scores in both groups was significant (Wald χ2 = 30.764, p < 0.001), with PANSS scores decreasing significantly as time changed. Therefore, treatment with PGD did not affect the patients’ psychotic symptoms.
Discussion
Several methods, such as bromocriptine, aripiprazole, and dopamine receptor agonists, have been proven effective in treating HPRL.27,28 However, they may do more harm than good. Drug side effects are still the main reason for the discontinuation of medication.29 Therefore, it is imperative to reduce the side effects of antipsychotic drugs. Previous preliminary experiments and studies in cultured cells and animals have shown that PGD can effectively alleviate risperidone-induced HPRL.30 However, some clinical trials found that after PGD treatment, no significant difference was found in PRL level between the control and experiment groups.23 So, this randomized controlled trial further re-examined the efficacy of PGD in antipsychotic drug-related HPRL. All the patients in the group were relatively stable after receiving antipsychotics, and the antipsychotic regimen was relatively stable The blood PRL levels of all patients were pathologically elevated, and HPRL-related symptoms, mainly irregular menstruation, amenorrhea, and sexual dysfunction, were present.
PGD significantly prevented further elevation of PRL and significantly improved sexual function in patients. This study is the first to assess the effect of PGD on HRPL-induced sexual function. In addition, we analyzed the effects of PGD on testosterone, luteinizing hormone, follicle-stimulating hormone, estradiol, and progesterone.
During the study, the PRL levels in the control group showed an upward trend, and at the 4th and 8th weeks, they were significantly higher than the PRL concentration in the experimental group (P<0.05). The difference between the two groups at the 4th and 8th weeks was statistically significant (P<0.05). There was no statistically significant difference in PRL concentration between the experimental group at the 4th or 8th week and the beginning of the experiment (P>0.05). This finding indicates that although the PRL levels of the experimental group patients did not increase significantly as in the control group, PGD did not significantly reduce the PRL levels of the experimental group patients.Therefore, PGD does not seem to have a substantial impact on PRL concentration.18,31 This difference is unlikely to be caused by changes in the formulation of PGD, as HPLC analysis confirmed that the current PGD formulation contains similar amounts of the main pharmacologically active ingredients as those used in previous studies.23 There are differences in the treatment regimens of antipsychotic drugs used among patients, and because fewer patients are using each regimen, this study did not analyze any relationship between treatment outcomes and different antipsychotic medicines or doses. Therefore, the heterogeneity of antipsychotic drugs may have an impact on the results. Currently, there is limited research on specific antipsychotic drugs for PGD, and only a few studies have reported that PGD has some effect on hyperprolactinemia induced by risperidone, amisulpride, or olanzapine.18,32,33 Moreover, the effects of each antipsychotic drug on PRL are different, with varying proportions and durations of occupancy of dopamine receptors, and there is a clear dose-dependency between the release of PRL and the drugs.29,34 And in females, prolactin levels are closely related to the degree of inhibition of the hypothalamic-pituitary-gonadal axis.35 Therefore, it cannot be determined whether the effect of PGD on PRL is related to specific antipsychotic drugs, and further research is needed.
This study showed that PGD improved sexual function significantly, especially sexual drive, arousal, and vaginal lubrication (female)/penile erection (male). Existing studies have demonstrated that antipsychotic medications are primarily designed to treat psychotic symptoms by binding to and diminishing the function of dopamine receptors; the inhibition of dopamine receptors results in the deregulated release of prolactin, causing HPRL.36–39 Dopamine transporter protein (DAT) is involved in the physiological regulation of PRL, and DAT blockade inhibits PRL gene expression and secretion in female rats.40,41 In the present study, prolactin levels were not significantly improved, but patients’ sexual function was enhanced. So, PGD may improve sexual function through other pathways. Dopamine plays different roles in controlling sexual behavior through its neuronal system and receptor subtypes, and drug-induced increases or decreases in brain dopamine activity or physiological occurrence usually improve or worsen sexual activity, respectively.42–44 PGD enhances D2 receptors and dopamine transporter (DAT), significantly reverses DRD2 and DAT expression, and ameliorates olanzapine-induced hyperprolactinemia in rats by attenuating impairment of D2R and TGF-β1 signaling pathways in the hypothalamus and pituitary gland.17,23,30,31 Thus, a broad range of PGD effects may be vital to ameliorating the symptoms observed in hyperprolactinemia.
The remaining five sex hormones, namely, luteinizing hormone, testosterone, follicle-stimulating hormone, estradiol, and progesterone, did not show significant changes at the end of the study; however, previous experiments mentioned that PGD affected the concentration of progesterone and could keep progesterone level normal.31 However, most other experiments did not mention that PGD significantly affected these hormones.
This study was conducted for a total of 8 weeks. However, the therapeutic effect of PGD on HRPL did not meet our experimental expectations. The improvement of sexual dysfunction in many patients and the possible benefit to patients with menstrual disorders exceeded our expectations. Improving sexual function in patients indirectly suggests that PGD improves dopamine receptor function in humans.
Our study has several limitations. Firstly, the antipsychotic drugs used in this experiment were not uniform. The effect of each antipsychotic medication on PRL was different. Secondly, our research time is relatively short, only eight weeks. Therefore, in the follow-up study, the sample size should be increased, and the study period should be extended to improve the reliability of the experimental results.
Excessive doses of licorice-related preparations can lead to complications, such as hypokalemia or hypertension,45 but no patient experienced such adverse effects during treatment. However, it is also necessary to pay attention to the occurrence of adverse reactions during the process of use.
Conclusions
PGD effectively improves sexual function in patients with antipsychotic-induced schizophrenia. It may work against antipsychotic-induced HPRL, but the effect may be weak, only preventing further progression of HPRL. Its efficacy in HPRL needs further study, and the mechanism underlying its impact on HPRL needs further investigation.
Data Sharing Statement
The datasets used and/or analyzed in this study are available from the corresponding author on reasonable request.
Ethics Statements
This study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Shandong Mental Health Center. All patients had signed an informed consent form for inclusion.
Acknowledgments
This research was supported by the National Natural Science Foundation of China (82101580), Traditional Chinese Medicine Science and Technology Development Plan Project of Shandong Province (2019-0528).
Disclosure
The authors report no conflicts of interest in this work.
References
1. James SL, Abate D, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1789–1858.
2. Rehm J, Shield KD. Global burden of disease and the impact of mental and addictive disorders. Curr Psychiatry Rep. 2019;21(2):10. doi:10.1007/s11920-019-0997-0
3. Lähteenvuo M, Tiihonen J. Antipsychotic polypharmacy for the management of schizophrenia: evidence and recommendations. Drugs. 2021;81(11):1273–1284. doi:10.1007/s40265-021-01556-4
4. McEvoy JP, Byerly M, Hamer RM, et al. Effectiveness of paliperidone palmitate vs haloperidol decanoate for maintenance treatment of schizophrenia: a randomized clinical trial. JAMA. 2014;311(19):1978–1987. doi:10.1001/jama.2014.4310
5. Muench J, Hamer AM. Adverse effects of antipsychotic medications. Am Fam Physician. 2010;81(5):617–622.
6. Keith SJ, Kane JM. Partial compliance and patient consequences in schizophrenia: our patients can do better [CME]. J Clin Psychiatry. 2003;64(11):1308–1315. doi:10.4088/JCP.v64n1105
7. Grigg J, Worsley R, Thew C, Gurvich C, Thomas N, Kulkarni J. Antipsychotic-induced hyperprolactinemia: synthesis of world-wide guidelines and integrated recommendations for assessment, management and future research. Psychopharmacology. 2017;234(22):3279–3297. doi:10.1007/s00213-017-4730-6
8. De Hert M, Peuskens J, Sabbe T, et al. Relationship between prolactin, breast cancer risk, and antipsychotics in patients with schizophrenia: a critical review. Acta Psychiatr Scand. 2016;133(1):5–22. doi:10.1111/acps.12459
9. Haddad PM, Wieck A. Antipsychotic-induced hyperprolactinaemia: mechanisms, clinical features and management. Drugs. 2004;64(20):2291–2314. doi:10.2165/00003495-200464200-00003
10. O’Keane V. Antipsychotic-induced hyperprolactinaemia, hypogonadism and osteoporosis in the treatment of schizophrenia. J Psychopharmacol. 2008;22(2 Suppl):70–75. doi:10.1177/0269881107088439
11. Faje A, Nachtigall L. Current treatment options for hyperprolactinemia. Expert Opin Pharmacother. 2013;14(12):1611–1625. doi:10.1517/14656566.2013.806488
12. Melmed S, Casanueva FF, Hoffman AR, et al. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(2):273–288. doi:10.1210/jc.2010-1692
13. Krysiak R, Kowalcze K, Szkrobka W, Okopien B. The effect of metformin on prolactin levels in patients with drug-induced hyperprolactinemia. Eur J Intern Med. 2016;30:94–98. doi:10.1016/j.ejim.2016.01.015
14. Besag F, Vasey MJ, Salim I. Is adjunct aripiprazole effective in treating hyperprolactinemia induced by psychotropic medication? A narrative review. CNS Drugs. 2021;35(5):507–526. doi:10.1007/s40263-021-00812-1
15. Chen JX, Su YA, Bian QT, et al. Adjunctive aripiprazole in the treatment of risperidone-induced hyperprolactinemia: a randomized, double-blind, placebo-controlled, dose-response study. Psychoneuroendocrinology. 2015;58:130–140. doi:10.1016/j.psyneuen.2015.04.011
16. Huang YL, Peng M, Zhu G. Topiramate in the treatment of antipsychotic-induced hyperprolactinemia. Med Hypotheses. 2020;138:109607. doi:10.1016/j.mehy.2020.109607
17. Huang X, Ren L, Hou L, et al. Paeoniflorin ameliorates antipsychotic-induced hyperprolactinemia in rats by attenuating impairment of the dopamine D2 receptor and TGF-β1 signaling pathways in the hypothalamus and pituitary. J Ethnopharmacol. 2020;257:112862. doi:10.1016/j.jep.2020.112862
18. Yuan HN, Wang CY, Sze CW, et al. A randomized, crossover comparison of herbal medicine and bromocriptine against risperidone-induced hyperprolactinemia in patients with schizophrenia. J Clin Psychopharmacol. 2008;28(3):264–370. doi:10.1097/JCP.0b013e318172473c
19. Zheng W, Cai DB, Li HY, et al. Adjunctive Peony-Glycyrrhiza decoction for antipsychotic-induced hyperprolactinaemia: a meta-analysis of randomised controlled trials. Gen Psychiatr. 2018;31(1):e100003. doi:10.1136/gpsych-2018-100003
20. Tandon R, Gaebel W, Barch DM, et al. Definition and description of schizophrenia in the DSM-5. Schizophr Res. 2013;150(1):3–10. doi:10.1016/j.schres.2013.05.028
21. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–276. doi:10.1093/schbul/13.2.261
22. Kelly DL, Wehring HJ, Earl AK, et al. Treating symptomatic hyperprolactinemia in women with schizophrenia: presentation of the ongoing DAAMSEL clinical trial (dopamine partial agonist, aripiprazole, for the management of symptomatic elevated prolactin). BMC Psychiatry. 2013;13:214. doi:10.1186/1471-244X-13-214
23. Man SC, Li XB, Wang HH, et al. Peony-Glycyrrhiza decoction for antipsychotic-related hyperprolactinemia in women with schizophrenia: a randomized controlled trial. J Clin Psychopharmacol. 2016;36(6):572–579. doi:10.1097/JCP.0000000000000607
24. Zhang J, Rosenheck R, Mohamed S, et al. Association of symptom severity, insight and increased pharmacologic side effects in acutely hospitalized patients with schizophrenia. Compr Psychiatry. 2014;55(8):1914–1919. doi:10.1016/j.comppsych.2014.07.018
25. Byerly MJ, Nakonezny PA, Fisher R, Magouirk B, Rush AJ. An empirical evaluation of the Arizona sexual experience scale and a simple one-item screening test for assessing antipsychotic-related sexual dysfunction in outpatients with schizophrenia and schizoaffective disorder. Schizophr Res. 2006;81(2–3):311–316. doi:10.1016/j.schres.2005.08.013
26. Luft MJ, Dobson ET, Levine A, Croarkin PE, Strawn JR. Pharmacologic interventions for antidepressant-induced sexual dysfunction: a systematic review and network meta-analysis of trials using the Arizona sexual experience scale. CNS Spectr. 2021;1–10. doi:10.1017/S1092852921000377
27. Bliesener N, Yokusoglu H, Quednow BB, Klingmüller D, Kühn KU. Usefulness of bromocriptine in the treatment of amisulpride-induced hyperprolactinemia: a case report. Pharmacopsychiatry. 2004;37(4):189–191. doi:10.1055/s-2004-827176
28. Voicu V, Medvedovici A, Ranetti AE, Rădulescu FŞ. Drug-induced hypo- and hyperprolactinemia: mechanisms, clinical and therapeutic consequences. Expert Opin Drug Metab Toxicol. 2013;9(8):955–968. doi:10.1517/17425255.2013.791283
29. Werner FM, Coveñas R. Safety of antipsychotic drugs: focus on therapeutic and adverse effects. Expert Opin Drug Saf. 2014;13(8):1031–1042. doi:10.1517/14740338.2014.935761
30. Wang D, Wang W, Zhou Y, et al. Studies on the regulatory effect of Peony-Glycyrrhiza decoction on prolactin hyperactivity and underlying mechanism in hyperprolactinemia rat model. Neurosci Lett. 2015;606:60–65. doi:10.1016/j.neulet.2015.08.024
31. Wang D, Wong HK, Zhang L, et al. Not only dopamine D2 receptors involved in Peony-Glycyrrhiza decoction, an herbal preparation against antipsychotic-associated hyperprolactinemia. Prog Neuropsychopharmacol Biol Psychiatry. 2012;39(2):332–338. doi:10.1016/j.pnpbp.2012.07.005
32. Yang P, Li L, Yang D, et al. Effect of Peony-Glycyrrhiza decoction on amisulpride-induced hyperprolactinemia in women with schizophrenia: a preliminary study. Evid Based Complement Alternat Med. 2017;2017:7901670. doi:10.1155/2017/7901670
33. Zhang L, Qi H, Xie YY, et al. Efficacy and safety of adjunctive aripiprazole, metformin, and Paeoniae-Glycyrrhiza Decoction for antipsychotic-induced hyperprolactinemia: a network meta-analysis of randomized controlled trials. Front Psychiatry. 2021;12:728204. doi:10.3389/fpsyt.2021.728204
34. Seeman P. An update of fast-off dopamine D2 atypical antipsychotics. Am J Psychiatry. 2005;162(10):1984–1985. doi:10.1176/appi.ajp.162.10.1984-a
35. Smith S, Wheeler MJ, Murray R, O’Keane V. The effects of antipsychotic-induced hyperprolactinaemia on the hypothalamic-pituitary-gonadal axis. J Clin Psychopharmacol. 2002;22(2):109–114. doi:10.1097/00004714-200204000-00002
36. Amato D, Canneva F, Cumming P, et al. A dopaminergic mechanism of antipsychotic drug efficacy, failure, and failure reversal: the role of the dopamine transporter. Mol Psychiatry. 2020;25(9):2101–2118. doi:10.1038/s41380-018-0114-5
37. Aringhieri S, Carli M, Kolachalam S, et al. Molecular targets of atypical antipsychotics: from mechanism of action to clinical differences. Pharmacol Ther. 2018;192:20–41. doi:10.1016/j.pharmthera.2018.06.012
38. Molitch ME. Dopamine agonists and antipsychotics. Eur J Endocrinol. 2020;183(3):C11–C13. doi:10.1530/EJE-20-0607
39. Strange PG. Antipsychotic drugs: importance of dopamine receptors for mechanisms of therapeutic actions and side effects. Pharmacol Rev. 2001;53(1):119–133.
40. Demaria JE, Nagy GM, Lerant AA, Fekete MI, Levenson CW, Freeman ME. Dopamine transporters participate in the physiological regulation of prolactin. Endocrinology. 2000;141(1):366–374. doi:10.1210/endo.141.1.7281
41. Luan S, Mu M, Sun L. The mechanism of selfheal extract in treating hyperprolactinemia. Cancer Biomark. 2017;20(4):575–580.
42. Giuliano F, Allard J. Dopamine and male sexual function. Eur Urol. 2001;40(6):601–608. doi:10.1159/000049844
43. Giuliano F, Allard J. Dopamine and sexual function. Int J Impot Res. 2001;13(Suppl 3):S18–28. doi:10.1038/sj.ijir.3900719
44. Melis MR, Sanna F, Argiolas A. Dopamine, erectile function and male sexual behavior from the past to the present: a review. Brain Sci. 2022;12(7):826. doi:10.3390/brainsci12070826
45. Smedegaard SB, Svart MV. Licorice induced pseudohyperaldosteronism, severe hypertension, and long QT. Endocrinol Diabetes Metab Case Rep. 2019;2019. doi:10.1530/EDM-19-0109
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.