")
Back to Journals » Clinical Ophthalmology » Volume 9
Pediatric glaucoma medical therapy: who more accurately reports medication adherence, the caregiver or the child?
Authors Moore D, Neustein R, Jones S, Robin A, Muir K
Received 24 July 2015
Accepted for publication 6 October 2015
Published 25 November 2015 Volume 2015:9 Pages 2209—2212
DOI https://doi.org/10.2147/OPTH.S93038
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Daniel B Moore,1 Rebecca F Neustein,2 Sarah K Jones,1 Alan L Robin,3 Kelly W Muir1,4
1Duke Eye Center, Duke University Medical Center, Durham, NC, 2Emory School of Medicine, Atlanta, GA, 3Department of Ophthalmology, Johns Hopkins School of Medicine and International Health, Bloomberg School of Public Health, Baltimore, MD, 4Health Services Research & Development, Durham VA Medical Center, Durham, NC, USA
Abstract: As they grow older, most children with glaucoma must eventually face the transition to self-administering medications. We previously reported factors associated with better or worse medication adherence in children with glaucoma, using an objective, electronic monitor. Utilizing the same data set, the purpose of the current study was to determine whose report (the caregiver’s or the child’s) corresponded better with electronically monitored adherence. Of the 46 participants (22 girls), the mean age of children primarily responsible, and caregiver primarily responsible for medication administration was 15±2 and 10±2 years, respectively. For the children whose caregiver regularly administered the eyedrops, the caregiver’s assessment of drop adherence was associated with measured adherence (P=0.012), but the child’s was not (P=0.476). For the children who self-administered eyedrops, neither the child’s (P=0.218) nor the caregiver’s (P=0.395) assessment was associated with measured percent adherence. This study highlights potential errors when relying on self-reporting of compliance in patients and caregivers with pediatric glaucoma, particularly when the child is responsible for administering their own eyedrops. Frank discussions about the importance of medication adherence and how to improve compliance may help both the child and caregiver better communicate with the treating provider.
Keywords: glaucoma, children, adherence
Introduction
The majority of children with glaucoma face lifelong monitoring and treatment. Most children, for whom caregivers may administer the prescribed glaucoma eye drops, must transition to take the responsibility for daily drop instillation as they grow older. This responsibility brings significant potential consequences: poor adherence to the prescribed eye drop regimen is associated with the worsening of glaucomatous visual field loss.1 Previously, we described objectively measured medication adherence in children with glaucoma. The proportion of prescribed glaucoma medications taken according to electronic monitors over a 30-day period ranged from 43% to 107%.2 Although useful in research, electronic monitors are not available in everyday clinical practice. Accordingly, clinicians may ask their patients and/or their patients’ caregivers about medication adherence. Adults with glaucoma often overestimate adherence to glaucoma medications when queried by their provider,3 but little is known about the relationship between self-reported or caregiver-reported and medication behavior for children with glaucoma. To better understand perceptions of glaucoma medication adherence, we examined whether the caregiver’s or child’s report of medication adherence is more reflective of objective measurements, and whether this relationship varies depending on who (child or caregiver) is responsible for drop instillation.
Materials and methods
Previously, we described adherence and factors related to adherence to the prescribed glaucoma medication regimen in children with glaucoma, as measured by an electronic monitor in 46 children aged 5–17 years.2 In this Institutional Review Board-approved study, following written informed consent by the child’s caregiver, both the child and the caregiver were administered baseline surveys, separately. The survey included questions regarding who was responsible for drop instillation and how often the survey respondent estimated that the child missed his or her drops (almost never, once a month, once a week, a few times a week, or daily). The survey questions were read aloud by the interviewer (SJ) and repeated as needed. Following the surveys, medication event monitors were provided for each glaucoma medication. The purpose of the monitors was explained to the patient and parent. The medication monitors recorded the date and time that each glaucoma medication was accessed over the subsequent 30 days. After the monitors were returned to the study team, the date and time information was downloaded into a spreadsheet for analysis.
Because the literature suggests that self-reported adherence is generally higher than monitored adherence,3 the responses for both child and caregiver surveys to the question regarding self-reported adherence were dichotomized to missing prescribed drop administration “almost never” versus other responses, with the belief than any admitted nonadherence could be meaningful. Glaucoma medication adherence was defined as the proportion of prescribed doses taken according to the medication event monitor (measured percent adherence). If a child was prescribed more than one glaucoma medication, the mean percent adherence for all glaucoma medications was calculated. Mean percent adherence was compared for the various respondent groups with the Mann–Whitney test, P<0.05 considered statistically significant.
Results
As previously reported,2 24 boys and 22 girls participated in the study, ranging in age from 5 to 17 years (mean 11 years, median 10 years). The most common glaucoma diagnoses of participants were aphakic (n=16) or primary congenital (n=14), followed by multi-mechanism (n=6), juvenile open angle (n=3), Sturge Weber (n=1), traumatic (n=1), aniridic (n=1), and indeterminate (n=4). The mean and median number of topical glaucoma medications prescribed was 2, range 1–4. Percent adherence according to the electronic monitors ranged from 43% to 107% (mean 93%±12%).
The number of respondents in each category of reported adherence (missing prescribed drop administration almost never, once a month, once a week, a few times a week, or daily) and the measured percent adherence for the participants in each respondent category is presented in Table 1.
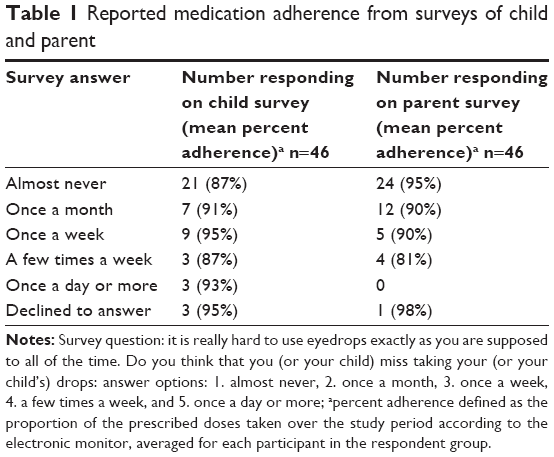 | Table 1 Reported medication adherence from surveys of child and parent |
Both child and caregiver reports of adherence were available for 42 pairs. In 18 of these 42 pairs, the responses to the survey were completely congruent. In 14 pairs, the caregiver’s estimate of adherence was higher than the child’s estimate; the child’s estimate was higher than the caregiver’s estimate in 10 pairs.
For 25 participants, the caregiver was responsible for drop administration and for 21 participants the child self-administered eye drops. The mean measured percent adherence was higher for children whose caregivers responded that the child “almost never” missed a drop, compared to the children whose caregivers responded that the child missed drops more frequently (P=0.005, Table 2). The children’s responses to the self-reported adherence question were not associated with measured percent adherence (P=0.846).
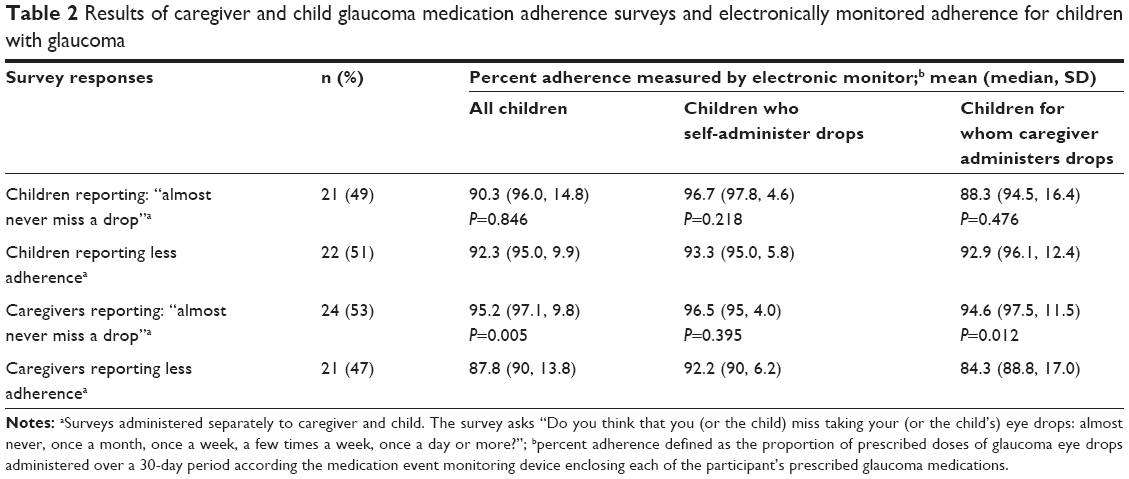 | Table 2 Results of caregiver and child glaucoma medication adherence surveys and electronically monitored adherence for children with glaucoma |
The average age of children who were responsible for administering their own drops was 15±2 years (range 9–17 years, median 14 years) and the average age of children for whom the caregiver was responsible for drop administration was 10±2 years (range 5–16 years, median 10 years). For the children whose caregivers (rather than the child) regularly administered the prescribed eye drops, the caregiver’s response to the survey was associated with the measured adherence (P=0.012), but the children’s response was not (P=0.476). For the children who self-administered eye drops regularly, neither the child’s response (P=0.218) nor the caregiver’s response (P=0.395) was associated with measured percent adherence.
Discussion
Previously, we reported factors associated with better or worse medication adherence in children with glaucoma. Adherence was similar for children prescribed once versus twice daily dosing but decreased as the caregiver’s health literacy level decreased.2 The purpose of the current study was to determine whose report, the caregiver’s or the child’s, corresponded better with electronically monitored adherence. The caregiver’s assessment of his or her child’s adherence to glaucoma medications corresponded with the objective measure of medication adherence captured by the electronic monitor if the caregiver was responsible for administering the drops; the child’s assessment did not. For children who self-administer their glaucoma medications, neither the child’s assessment nor the caregiver’s assessment of medication adherence was closely associated with the objective measurement.
The time during which adolescents transition to self-managing their disease may be a time when it is difficult for caregivers and providers to accurately assess adherence to the prescribed medication regimen. Interestingly, the age ranges are wide both for children who self-administer drops and for children who rely on caregivers to administer drops. Perhaps this is not surprising, as up to 20% of adults with glaucoma rely on others to administer their drops.4 It is an important reminder to clinicians that regardless of the patient’s age, it is worthwhile to inquire as to who is responsible for drop administration.
Although the prevalence of glaucoma in children is low, this study is limited by small sample size and relatively short follow-up period. As reported previously, however, for the 32 participants who used the medication monitors for at least 90 days, average percent adherence was not different between each 30-day period.2 Knowing that their medication use is being monitored may cause patients to adhere more strictly to their prescribed regimen, but the similarity in measured adherence between the first and subsequent 30-day period suggests that this effect is likely small. Alternative methods of capturing medication adherence, such as reviewing pharmacy refill rates may avoid the observation bias but have more problematic limitations, such as underestimation of adherence due to the use of multiple pharmacies or the receipt of sample medications in the clinic. Overall, the children who participated in this study demonstrated high levels of adherence2 compared to the levels of adherence often reported for adults with glaucoma.3 This ceiling effect makes differences in adherence harder to detect and more meaningful when identified. This study is also subject to recall bias, the responses of young children may not be accurate with respect to timing of drop dosing. This limitation was acknowledged in the design of the study but allowed as it was our specific purpose to evaluate the responses of children (and caregivers) compared to objective monitoring.
Several reports in the literature highlight the difficult transition in adolescence to the self-management of disease monitoring in chronic, lifelong conditions like glaucoma, including diabetes5 and inflammatory bowel disease.6 Identified barriers to adherence in this population include forgetting, interfering activities, parent–child conflict, oppositional behavior, and inadequate planning for treatment. Factors associated with improved adherence include strong family support and parent–child relationship, established routines, and parental monitoring.6
As children assume more responsibility for managing their glaucoma, frank discussions about the importance of medication adherence and how to prevent lapses in adherence may help both the child and the caregiver better communicate with the treating provider.
Acknowledgments
This work was funded in part by the American Glaucoma Society’s Mentoring for the Advancements of Physician Scientists Award, the NIH 5K12 EY016333-05. Dr Muir receives salary support from a VA HSR&D Career Development Award.
Disclosure
The authors report no conflicts of interest in this work.
References
Rossi GC, Pasinetti GM, Scudeller L, Radaelli R, Bianchi PE. Do adherence rates and glaucomatous visual field progression correlate? Eur J Ophthalmol. 2011;21(4):410–414. | ||
Freedman RB, Jones SK, Lin A, Robin AL, Muir KW. Influence of parental health literacy and dosing responsibility on pediatric glaucoma medication adherence. Arch Ophthalmol. 2012;130(3):306–311. | ||
Okeke CO, Quigley HA, Jampel HD, et al. Adherence with topical glaucoma medication monitored electronically the Travatan Dosing Aid study. Ophthalmology. 2009;116(2):191–199. | ||
Kass MA, Hodapp E, Gordon M, Kolker AE, Goldberg I. Part I. Patient administration of eyedrops: interview. Ann Ophthalmol. 1982;14(8):775–779. | ||
Rausch JR, Hood KK, Delamater A, et al. Changes in treatment adherence and glycemic control during the transition to adolescence in type 1 diabetes. Diabetes Care. 2012;35(6):1219–1224. | ||
Hommel KA, Odell S, Sander E, Baldassano RN, Barg FK. Treatment adherence in paediatric inflammatory bowel disease: perceptions from adolescent patients and their families. Health Soc Care Commun. 2011;19(1):80–88. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.