")
Back to Journals » Research and Reports in Urology » Volume 15
PCA3 and TMPRSS2: ERG Urine Level as Diagnostic Biomarker of Prostate Cancer
Authors Warli SM, Warli MH, Prapiska FF
Received 12 December 2022
Accepted for publication 11 April 2023
Published 5 May 2023 Volume 2023:15 Pages 149—155
DOI https://doi.org/10.2147/RRU.S401131
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Guglielmo Mantica
Syah Mirsya Warli,1,2 Muhammad Haritsyah Warli,3 Fauriski Febrian Prapiska2
1Department of Urology, Faculty of Medicine Universitas Sumatera Utara – Universitas Sumatera Utara Hospital, Medan, North Sumatera, Indonesia; 2Department of Surgery Urology Division, Faculty of Medicine Universitas Sumatera Utara – Haji Adam Malik General Hospital, Medan, North Sumatera, Indonesia; 3Department of Urology, Faculty of Medicine Universitas Indonesia – Haji Adam Malik General Hospital, Medan, North Sumatera, Indonesia
Correspondence: Syah Mirsya Warli, Tel +62 61-8364930, Email [email protected]
Background: Prostate cancer is a highly prevalent urological carcinoma with an increasing incidence in Indonesia and all around the world. Early diagnosis can greatly affect treatment outcomes and increase life expectancy. Several biomarkers for detecting prostate cancer have been studied and showed great promise.
Purpose: This study aims to analyze prostate cancer antigen 3 (PCA3) as well as transmembrane serine protease 2:ERG (TMPRSS2:ERG) for diagnosing and serving as urine biomarkers in predicting prostate cancer incidences.
Methods: We conducted an analytical study to assess the utility of PCA3 and TMPRSS2:ERG for detecting prostate cancer. Thirty samples were included in this study to see the utilization of PCA3 and TMPRSS2:ERG as diagnostic biomarkers of prostate cancer. A urine sample was taken and the PCA3 test was performed using the PCA3 PROGENSA test, while the TMPRSS2:ERG was performed using the chemiluminescent DNA probe method with a hybridization protection test.
Results: The average age of the subject was 61.07± 8.3 years. Based on calculations using the Mann–Whitney test, there was a significant relationship between prostate-Specific Antigen (PSA) overexpression (p< 0.001), TMPRSS2:ERG (p=0.001), and PCA3 (p=0.003) with prostate cancer incidence. The sensitivity of PCA3 and TMPRSS2:ERG in detecting prostate cancer was 76.9% and 92.3%, respectively. Hence, TMPRSS2:ERG and PCA3 can be used as biomarkers for the occurrence of prostate cancer. We also performed a Kruskal–Wallis test; however, there was no significant relationship between PSA (p=0.236), TMPRSS2:ERG (p=0.801), and PCA3 (p=0.091) with the Gleason score.
Conclusion: There is a significant correlation between overexpression of PSA, TMPRSS2:ERG and PCA3 with the incidence of prostate cancer, and TMPRSS2:ERG and PCA3 can be used as biomarkers of prostate cancer.
Keywords: prostate cancer, PSA, PCA3, TMPRSS2:ERG, urine biomarker
Introduction
Prostate cancer is a prevalent and potentially lethal malignancy, with an incidence rate of 7.2 per 100.000 males per year in Asia.1 In Indonesia, according to Globocan 2020, the incidence rate is about 13.563 males.2 Globally, this number has increased significantly over the past few years and is predicted to grow within the next few years continually. Due to the inadequate accuracy of PSA, which only has a 20% diagnostic sensitivity, 60–70% specificity for prostate cancers, and considerable morbidity associated with biopsies, therein lies the need for a more accurate and less invasive diagnostic tool for a high-risk population for prostate cancer.3 Advent in tumor markers research has identified several biomarkers used for new tests. Some of the most frequently studied biomarkers are Prostate Cancer Gene 3 (PCA3) and TMPRSS2: ERG.
PCA3 is the first urine biomarker for prostate cancer to be approved by the US Food and Drug Administration (FDA) (FDA). It is detected in almost all cases of prostate cancer, expressing abundantly in the tumor site. PCA3 is recognized as messenger noncoding RNA (mRNA) without the protein generated.4 PCA3 mRNA can be identified in prostate cancer patients’ urine and male prostatic fluid. PCA3 mRNA levels is not regulated by serum PSA levels.5 Instead, PCA3 is overexpressed in prostate cancer.6
TMPRSS2, a serine protease group, is highly expressed in the prostate gland. It also serves as an androgen responsive gene that encodes proteins such as type II transmembrane serine protease (TTSP). Aberrant expression of TMPRSS2 and TTSP genes are reported to contribute to prostate cancer. The gene fusion of TMPRSS2 and ETS transcription factors, such as ERG and ETV1 is all prostate cancer stages including castration-resistant prostate cancer (CRPC).7–9 ERG is an oncogene that encodes erythroblast transformation-specific,7 which is the crucial regulator of cell proliferation, differentiation, angiogenesis, swelling, and apoptosis. TMPRSS2:ERG is indicated as a promising novel biomarker for identifying prostate cancer.10
Novel diagnostic markers, such as Piwi-like 2 (PIWIL2) gene expression and systemic immune response (SII) are currently being investigated to detect in prostate cancer.11 Tosun et al found that PIWIL2 expression is correlated with PSA levels. PIWIL2 expression is lower in patients with a PSA level of <4 and correspondingly higher in patients with high PSA level (PSA ≥4). However, PIWIL2 expression had non-significant differences in non-cancer and cancer patients with high PSA level, hence it is less likely to be an accurate diagnostic indicator of prostate cancer.12 Meanwhile, SII has a significant diagnostic value in patients with high PSA levels. However, it did not have significant diagnostic value in low-grade prostate cancer patients (ISUP grade 1 and 2).11
This study aims to evaluate the utilization of PCA3 and TMPRSS2:ERG urine levels in prostate cancer diagnosis.
Methods
It was a cross-sectional study to analyze PCA3 and TMPRSS2:ERG as urine biomarkers in the diagnosis of prostate cancer. This research was conducted at the Universitas Sumatera Utara hospital laboratory from February 2018 to October 2018. Ethical clearance has been granted for this study from the Health Research Ethical Committee of the Medical Faculty of Universitas Sumatera Utara with approval number No. 201/TGL/KEPK FK-USU-RSUP HAM/2018. All patients with lower urinary tract symptoms suggestive of benign prostate hyperplasia of prostate cancer, with PSA level >4 and who underwent prostatic biopsy were included in our study.
The midstream urine sample was taken from the initial portion of urine. The amount of urine taken is 20–30 mL. The whole urine sample was taken after patients had undergone digital rectal examination (DRE) with three strokes on each lateral lobe of the prostate. The urine sample is mixed with a detergent-based buffer solution, stored above −70°C, and processed within 4 hours. The urine sample is then sent to the laboratory for examination. After this procedure, the patients underwent a prostatic biopsy. A standard 12-core biopsy was made for each patient during the first biopsy.
The housekeeping gene, kallikrein 3 (KLK3) gene, was used as the control in the quantitative PCR (qPCR) procedure. The gene was selected based on its stability in patients with or without diseases. It had an essential role as an internal validator and gave certainty that the procedure ran correctly. The gene went through quantification using qPCR and statistical analysis was performed to identify the significant change and relationship between the biomarkers that were tested.
PCA3 examination was done by performing the PCA3 PROGENSA test (Gen Probe Inc., San Diego, CA, USA) using the manual book as a reference for protocols. PCA3 and PSA mRNAs were extracted from the prostate cancer cells found in the urine sample following DRE. The isolated RNAs were mixed with kit solution thus reverse transcription process to develop cDNA took place. They were amplified through hybridization to complement oligonucleotides and subsequently combined using chemiluminescent-labeled DNA probes through qPCR. PCA3 rs was calculated using the 2 (ct) case-(ct) control equation. With the same retrieval technique with a PCA3 examination, the product was detected by a chemiluminescent DNA probe with a hybridization protection test to measure the TMPRSS2:ERG level.
Statistical analysis was done using SPSS Software v.26 (IBM Statistics). Demographic characteristics of study participants are presented using descriptive analysis. Then, both Mann–Whitney and Kruskal–Wallis were performed to determine the relationship of the results of the study.
Results
The characteristics of the participants are presented in Table 1. Thirty samples were included in this study to assess the utility of PCA and TMPRSS2:ERG as a biomarker in diagnosing prostate cancer. The mean age of subjects was 61.07±8.3 years. According to histopathology results, subjects were classified into two categories, benign prostate hyperplasia (BPH) group and prostate cancer/adenocarcinoma (PCa) group because no results indicate any PIN or inflammation. Seventeen subjects (56.7%) in the BPH group and thirteen (43.3%) in the PCa group. Of thirteen subjects, the Gleason scores were obtained. Most of them were 4+4=8 (7 cases; 53.8%). The prostate-specific antigen (PSA) median value was 11.5 ng/mL (0.28–61.51 ng/mL). The median value of prostate weight was 52 grams. Of the thirty patients in this study, 20 (66.7%) had urinary retention, while the other ten (33.3%) had no retention. Of the ten patients who did not experience retention, the mean Qmax value was 7.5 ± 1.18 mL/s, while the mean PVR value was 80 ± 7.27 mL. The median value for TMPRSS2: ERG expression was 0.12 (0.18–0.36), and PCA 3 expression was 0.14 (0.19–0.39).
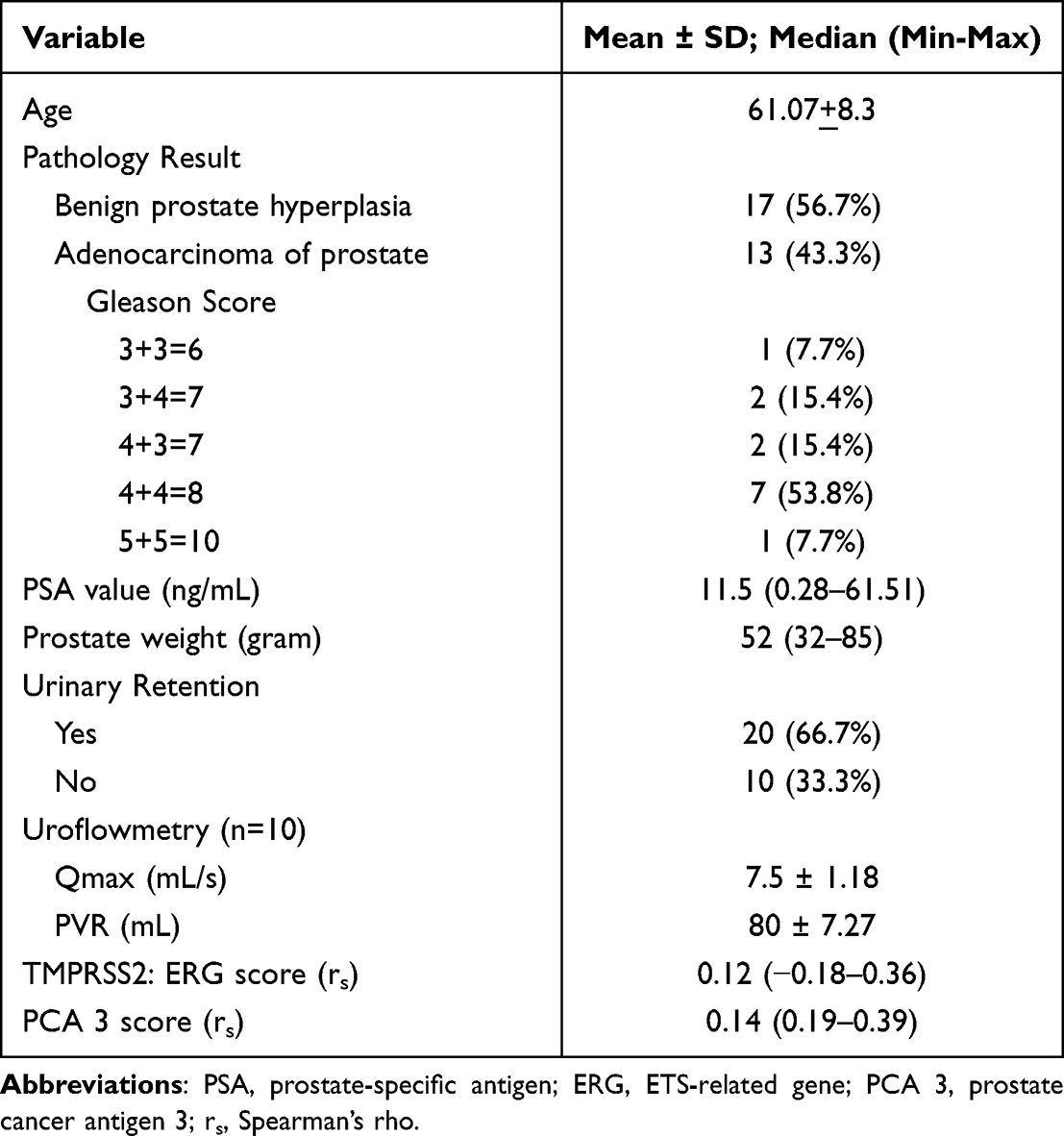 |
Table 1 Demographic Characteristics of Participant |
The mean PSA in the BPH group was found to be 7.84 ng/mL, and for the PCa group was 29.12 ng/mL as shown in Table 2. TMPRSS2:ERG median value, based on the Spearman’s rho (rs) score, was 0.11 in the BPH group and 0.21 in the PCa group. PCA 3 has 0.02 in the BPH group and 0.18 in the PCa group as the median value.
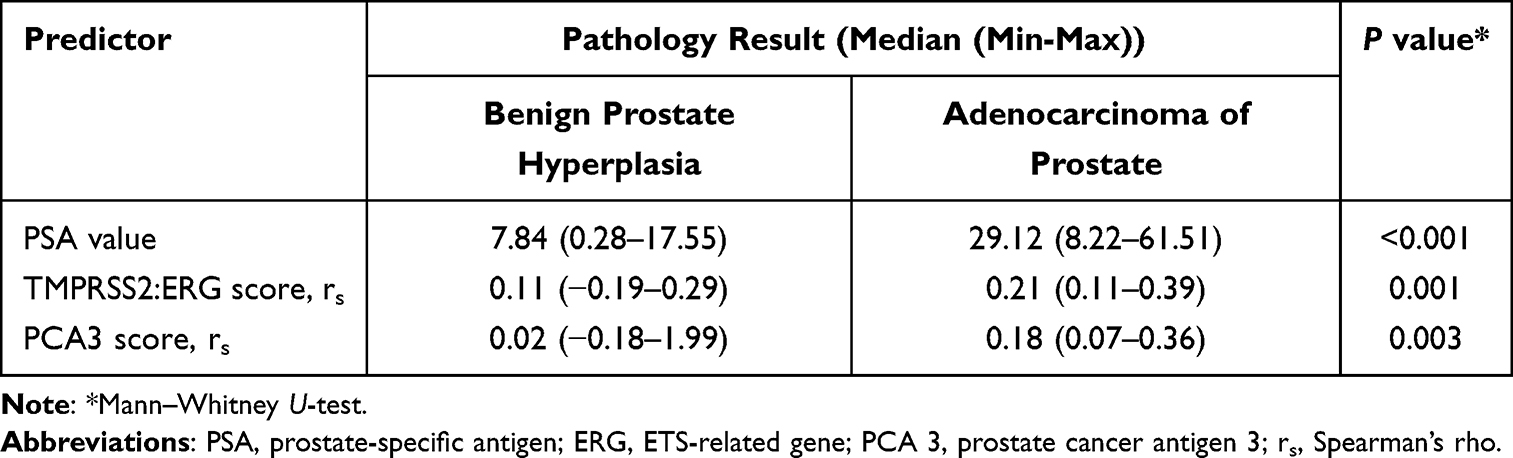 |
Table 2 Expression of Serum PSA, Urinary TMPRSS2:ERG & PCA 3 Based on Pathology Result |
Correlations of urine TMPRSS2:ERG with histopathology parameters showed significant differences (rs=0.12, P = 0.001). A similar result was found in PCA 3 (rs=0.14, P = 0.003) when measured by the Mann–Whitney test. We compared our results with the PSA value. Based on this result, TMPRSS2:ERG and PCA3 can be used as a biomarker in prostate cancer.
The relationship between PSA, TMPRSS2:ERG, and PCA3 with Gleason score were also analyzed using Kruskal–Wallis test as seen in Table 3. From the multivariate analysis, we found no significance between all of them. The p-value for each PSA, TMPRSS2:ERG, and PCA3 was 0.236; 0.801; and 0.091.
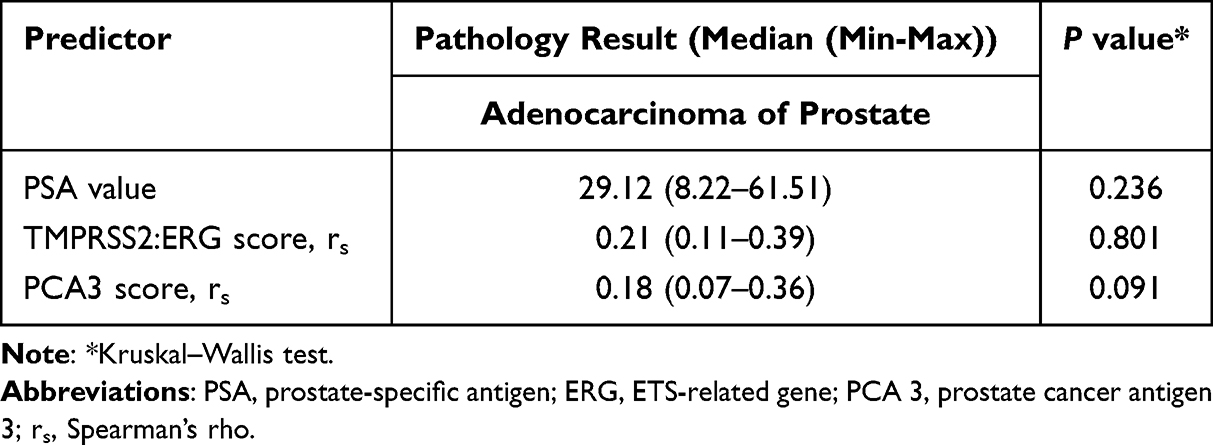 |
Table 3 Expression of Serum PSA, Urinary TMPRSS2:ERG, and PCA 3 Based on Gleason Score |
The sensitivity and specificity of PCA3 in the detection of prostate cancer were 76.9% and 76.5%, respectively. ERG showed higher sensitivity yet lower specificity in detecting prostate cancer than PCA3; there were 92.3% and 70.6%, respectively. The overall cut-off point for both PCA3 and ERG was 0.145 and 0.0855, respectively. These results were determined using the ROC curve.
Discussion
Serum PSA utilization as an early prostate cancer biomarker is very limited in terms of its many false positive and false-negative results because it is not being specifically produced in malignant cases. Nonetheless, PSA is one of the most widely used tumor markers, even with its limitations for PCa detection with its low specificity.10 An urgent need for a specific biomarker is required for prostate cancer, which may improve prostate cancer screening and early detection, thus aiming for a better quality of life.13
This study demonstrates the correlation of TMPRSS2:ERG and PCA3 urine tissues and prostate cancer, thus supporting the predictor effect of this biomarker in urine and tissue, using commonly studied biomarkers, PCA3 being the known messenger noncoding mRNA, which can be detected in urine and male prostate fluids, and TMPRSS2 combined with ERG gene, which shows genomic changes and ERG transcription factors in prostate cancer cases and staging. Immunohistochemistry results revealed that ERG expression was exceedingly rare in benign prostatic acini but exceptionally high (almost 100%) in prostate cancer or HGPIN (High-Grade Prostate Prostatic Intraepithelial Neoplasia). HGPIN is the most important potential precursor of prostate cancer and one of the major clinically significant histological abnormalities discovered by prostate biopsy. The presence of HGPIN is seen in around 9% of prostate biopsy specimens. HGPIN and prostate cancer share genetic and molecular markers, with PIN serving as a transitional stage between benign epithelium and invasive malignant carcinoma.9,14,15
In addition to having similar cytologic traits, HGPIN and prostate cancer have many additional parallels, such as an increased incidence with age and a high rate of occurrence in the prostate’s peripheral zone. HGPIN in the transition zone of the prostate, on the other hand, is far less prevalent, occurring in only 2% to 3% of patients.16,17 The volume of PIN is well documented to have a favorable connection with both pathologic stage and Gleason grade.
Several cohort studies across Asia, Europe, and North America have found that nearly half of all prostate malignancies are caused by the TMPRSS2:ERG fusion. This incidence of such patterns in PSA-screened patients has been observed that the TMPRSS2:ERG fusion exhibits rearrangements in 50% or more of the instances, but HGPIN appears to have a lower frequency of gene fusions.18 The presence of TMPRSS2:ERG fusion in cancer tissues has been linked to a more aggressive natural course of the disease and an increase in prostate cancer-related mortality.19
The analysis reveals that the connection between urine PCA3 score and TMPRSS2:ERG score is minor. Overexpression of PCA3 has been found in 95% of cases. In contrast, gene expression investigations have shown selectivity for the prostate, implying that the decreased correlation between PSA and urine PCA3 contrasted with PSA and urine TMPRSS2:ERG is not due to the malignant foci missing PCA3 expression. In comparison to ERG, very few researchers have studied the specificity of PCA3 across precursor lesions and benign mimics of prostate cancer at the tissue level, given that it is a noncoding gene that does not produce antibody-detectable protein.20
When comparing urine PCA3 to HGPIN, the score has been associated with biopsies in various investigations but with mixed results. Deras et al found no significant difference in the PCA3 score of HGPIN with and without disease, whereas Haese et al found an increase in PCA3 scores in HGPIN men.21 The investigations demonstrated PCA3 score identification and equivalent diagnostic accuracy for biopsy-detectable malignancy. The study’s limitation was that it did not analyze the total prostatic HGPIN burden, but just HGPIN detected patients at biopsy. Finally, a study by Ye et al shows that PCA3 is upregulated in positive biopsy patients and accurately predicts all high-grade prostate cancer. In a population with PSA of less than 20 ng/mL, PCA3 is shown to have 73% sensitivity and 36.7% specificity. This study’s limitation compared to ours is that they only analyze PCA3 because TMPRSS2-ERG fusion transcript is low in the Chinese population.23
TMPRSS2:ERG and PCA3 are related to aggressive disease indicators and are beneficial in predicting prostate cancer at biopsy. Combining PSA level and urine PCA3 and TMPRSS2:ERG can provide a comprehensive assessment of prostate cancer risk as well as an assessment of prostate cancer burden. Prostate malignancies can now be adequately handled by risk stratification of men with increased PSA serum, those with prior negative biopsy results, and men requesting active surveillance (elevated urine TMPRSS2:ERG and PCA3 scores are strongly associated with prostate cancer).24,25 TMPRSS2-ERG has been linked to tumor size, high Gleason score, and Gleason score upgrade upon prostatectomy, in addition to predicting malignancy at biopsy. 26
The commercially available Progensa urine test for PCA3 is superior to total and percent-free PSA for detecting PCa in men with elevated PSA as it shows significant increases in the area under the receiver-operator characteristic curve (AUC) for positive biopsies.27 When detection of TMPRSS2-ERG in urine was added to PCA3 expression and serum PSA (Michigan) Prostate Score [MiPS], cancer prediction improved.26 Both these studies show a promising future for the usage of PCA3 and TMPRSS2-ERG in the detection of prostate cancer.
Although the study has certain limitations, such as a limited sample size, not covering the entire pathological spectrum (ie, Gleason scores and stage), the biopsy was only performed once per patient. Moreover, a fusion prostate biopsy, MRI combined with transrectal ultrasonography (TRUS), was not performed in this study. Fusion prostate biopsy has a higher sensitivity and rate of cancer detection. Therefore, it could lessen false negatives thereby increasing the validity and accuracy of the results.28 Evaluation of PCA3 in conjunction with HGPIN detection could also be used as a potential diagnostic marker to repeat the prostate biopsy for men with elevated PSA. Still, normal prostate biopsy results, as evidence showed that high expression of PCA3 was found in men with HGPIN compared to men without HGPIN, increasing the likelihood of a positive repeat biopsy.25 PCA3 was also associated with males with clinical stage T2 and Gleason score ≥ 7, as opposed to men with clinical stage T1 and Gleason score < 7. This conclusion could serve as a criterion for placing patients on active surveillance.22
Further research is needed to establish a correlation between outcome measures. Furthermore, our study did not represent a prospectively defined prostatectomy cohort despite collecting urine specimens before the biopsy. Additionally, the one-time prostate biopsy operation may result in an undermined benign group.
Conclusion
Early identification of prostate cancer is critical for giving successful therapy to prostate cancer patients. With the emergence of these new biomarkers, TMPRSS2:ERG and PCA 3 could potentially be used as a substitute or in conjunction with serum PSA as a diagnostic tool for prostate cancer owing to the high sensitivity and specificity of both biomarkers, thus enhancing the patient’s prognosis and quality of life. Another advantage is that both indicators can be tested in patients’ urine, which is utilized in the clinical practice. This could be the foundation for a noninvasive, simple-to-use clinical test option for patients who do not want to undergo a more invasive treatment, such as invasive tools to get a prostate cancer diagnosis.
Ethics
Ethical clearance has been granted for this study from the Health Research Ethical Committee of the Medical Faculty of Universitas Sumatera Utara with approval number No. 201/TGL/KEPK FK-USU-RSUP HAM/2018. All human studies were conducted in accordance with the Declaration of Helsinki. Written informed consent from participants was obtained for the sample collection and publication.
Funding
Universitas Sumatera Utara Research Centre supports this research with TALENTA Grant Scheme with Grant number 2590/UN5.1.R/PPM/2018.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Salagierski M, Schalken JA. PCA3 and TMPRSS2-ERG: promising biomarkers in prostate cancer diagnosis. Cancers. 2010;2:1432–1440. doi:10.3390/cancers2031432
3. Moyer VA; U.S. Preventive Services Task Force. Screening for prostate cancer: u.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;157:120–134. doi:10.7326/0003-4819-157-2-201207170-00459
4. Hessels D, Klein Gunnewiek JM, van Oort I, et al. DD3(PCA3)-based molecular urine analysis for the diagnosis of prostate cancer. Eur Urol. 2003;44:8–15. doi:10.1016/S0302-2838(03)00201-X
5. Hessels D, Schalken JA. The use of PCA3 in the diagnosis of prostate cancer. Nat Rev Urol. 2009;6(5): 255–261. doi:10.1038/nrurol.2009.40
6. Nakanishi H, Groskopf J, Fritsche HA, et al. PCA3 molecular urine assay correlates with prostate cancer tumor volume: implication in selecting candidates for active surveillance. J Urol. 2008;179:1804–1810. doi:10.1016/j.juro.2008.01.013
7. Gasi TD, Boormans J, Hermans K, Trapman J. ETS fusion genes in prostate cancer. Endocr Relat Cancer. 2014;21:143–152. doi:10.1530/ERC-13-0390
8. Kissick HT, On ST, Dunn LK, et al. The transcription factor ERG increases expression of neurotransmitter receptors on prostate cancer cells. BMC Cancer. 2015;15:604. doi:10.1186/s12885-015-1612-3
9. Tomlins SA, Palanisamy N, Siddiqui J, Chinnaiyan AM, Kunju LP. Antibody-based detection of ERG rearrangements in prostate core biopsies, including diagnostically challenging cases: ERG staining in prostate core biopsies. Arch Pathol Lab Med. 2012;136:935–946. doi:10.5858/arpa.2011-0424-OA
10. Stephan C, Rittenhouse H, Hu X, Cammann H, Jung K. Prostate-specific antigen (PSA) screening and new biomarkers for prostate cancer (PCa). EJIFCC. 2014;25:55–78. doi:10.1016/j.eururo.2013.08.005
11. Sonmez G, Demirtas T, Tombul S, Akgun H and Demirtas A. Diagnostic efficiency of systemic immune-inflammation index in fusion prostate biopsy. Actas Urológicas Españolas (English Edition). 2021;45(5):359–365. doi:10.1016/j.acuroe.2021.04.006
12. Tosun H, Demirtaş, A, Sönmez, G, Tombul, ST, Akalın, H, Özkul, Y . Can the expression level of PIWIL 2 gene be a serum marker for prostate cancer? A single-center prospective study. Turk J Urol. 2019:45(–1):22–25. doi:10.5152/tud.2019.46416
13. Schröder FH, Hugosson J, Roobol MJ, et al. Screening and prostate cancer mortality in a randomized European study. N Engl J Med. 2009;360:1320–1328. doi:10.1056/NEJMoa0810084
14. Furusato B, Tan SH, Young D, et al. ERG oncoprotein expression in prostate cancer: clonal progression of ERG-positive tumor cells and potential for ERG-based stratification. Prostate Cancer Prostatic Dis. 2010;13:228–237. doi:10.1038/pcan.2010.23
15. Park K, Tomlins SA, Mudaliar KM, et al. Antibody-based detection of ERG rearrangement-positive prostate cancer. Neoplasia. 2010;12:590–598. doi:10.1593/neo.10726
16. Gaudin PB, Sesterhenn IA, Wojno KJ, et al. Incidence and clinical significance of high-grade prostatic intraepithelial neoplasia in TURP specimens. Urology. 1997;49:558–563. doi:10.1016/S0090-4295(96)00542-0
17. Pacelli A, Bostwick DG. Clinical significance of high-grade prostatic intraepithelial neoplasia in transurethral resection specimens. Urology. 1997;50:355–359. doi:10.1016/S0090-4295(97)00249-5
18. Kumar-Sinha C, Tomlins SA, Chinnaiyan AM. Recurrent gene fusions in prostate cancer. Nat Rev Cancer. 2008;8:497–511. doi:10.1038/nrc2402
19. Attard G, Clark J, Ambroisine L, et al. Duplication of the fusion of TMPRSS2 to ERG sequences identifies fatal human prostate cancer. Oncogene. 2008;27:253–263. doi:10.1038/sj.onc.1210640
20. Popa I, Fradet Y, Beaudry G, Hovington H, Beaudry G, Têtu B. Identification of PCA3 (DD3) in prostatic carcinoma by in situ hybridization. Mod Pathol. 2007;20:1121–1127. doi:10.1038/modpathol.3800963
21. Deras IL, Aubin SM, Blase A, et al. PCA3: a molecular urine assay for predicting prostate biopsy outcome. J Urol. 2008;179:1587–1592. doi:10.1016/j.juro.2007.11.038
22. Haese A, de la Taille A, van Poppel H, et al. Clinical utility of the PCA3 urine assay in European men scheduled for repeat biopsy. Eur Urol. 2008;54:1081–1088. doi:10.1016/j.eururo.2008.06.071
23. Ye LF, He S, Wu X, et al. Detection of prostate cancer antigen 3 and prostate cancer susceptibility candidate in non-DRE urine improves diagnosis of prostate cancer in Chinese population. Prostate Cancer. 2020;2020:396461. doi:10.1155/2020/3964615
24. Ploussard G, Durand X, Xylinas E, et al. Prostate cancer antigen 3 score accurately predicts tumour volume and might help in selecting prostate cancer patients for active surveillance. Eur Urol. 2011;59:422–429. doi:10.1016/j.eururo.2010.11.044
25. Durand X, Xylinas E, Radulescu C, et al. The value of urinary prostate cancer gene 3 (PCA3) scores in predicting pathological features at radical prostatectomy. BJU Int. 2012;110:43–49. doi:10.1111/j.1464-410X.2011.10682.x
26. Tomlins SA,Aubin SMJ, Siddiqui J, et al. Urine TMPRSS2:ERG Fusion Transcript Stratifies Prostate Cancer Risk in Men with Elevated Serum PSA. Sci Transl Med. 2011;3(94:94ra72). doi: 10.1126/scitranslmed.3001970
27. Wei JT, Feng Z, Partin AW, et al. Can Urinary PCA3 Supplement PSA in the Early Detection of Prostate Cancer?. J Clin Oncol. 2014;32(36:4066–4072). doi: 10.1200/JCO.2013.52.8505
28. Streicher J, Meyerson BL, Karivedu V and Sidana A. A review of optimal prostate biopsy: indications and techniques. Ther Adv Urol. 2019;11:175628721987007. doi: 10.1177/1756287219870074
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.