")
Back to Journals » Integrated Pharmacy Research and Practice » Volume 9
Patterns and Practices of Self-Medication Among Students Enrolled at Mbarara University of Science and Technology in Uganda
Authors Niwandinda F, Lukyamuzi EJ , Ainebyona C , Ssebunya VN , Murungi G, Atukunda EC
Received 9 November 2019
Accepted for publication 31 January 2020
Published 13 February 2020 Volume 2020:9 Pages 41—48
DOI https://doi.org/10.2147/IPRP.S237940
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jonathan Ling
Faith Niwandinda, Edward John Lukyamuzi, Calvin Ainebyona, Veronica Nambi Ssebunya, Godwin Murungi, Esther C Atukunda
Department of Pharmacy, Mbarara University of Science and Technology, Mbarara, Uganda
Correspondence: Edward John Lukyamuzi
Department of Pharmacy, Mbarara University of Science and Technology, P.O. Box 1410, Mbarara, Uganda
Tel +256 774-555726
Fax +256 48520782
Email [email protected]
Purpose: Self-medication is drug use without advice from a medical professional. Proper self-medication can reduce health expenses and physician waiting time. However, prescription or over-the-counter drugs are considered unsafe when used irrationally. Presumably, university students can make informed decisions regarding their lives. However, there are limited studies documenting self-medication in Ugandan universities. This study sought to document the prevalence, patterns and factors associated with self-medication among students enrolled at Mbarara University of Science and Technology (MUST).
Patients and Methods: A descriptive cross-sectional study was done on 385 medical and non-medical students. Data were collected by interviewer-led semi-structured questionnaires and analyzed using the Statistical Package for Social Sciences (SPSS) version 20. The statistical significance was considered as p < 0.05 for both univariate and multivariate analyses.
Results: This study showed a 63.5% prevalence of self-medication. Self-medication reasons were classifying illnesses as minor (33%), time-saving (15%), having old prescriptions (11%) and high consultation fees (9%). Not self-medicating reasons included risk of using wrong drugs (19%), insufficient knowledge (17%), fear of side effects (15%), wrong drug use (15%) and misdiagnosis (14%). Respondents accessed drugs from pharmacies (56%), friends/family (17%) or private clinics (15%). Headache relievers, pain relievers and antibiotics were most commonly self-medicated. In adjusted analysis, being female, existing allergies, and being in advanced years of study were associated with increased odds of self-medication. No statistically significant difference existed between medical and non-medical students regarding self-medication. Self-medication likelihood increased with a lack of access to medical services.
Conclusion: There is a high rate of self-medication amongst female students, those in advanced years of study and those with existing allergies. Medical services access significantly reduced the chances of self-medication. Vital medical services need to be extended to the university students to receive information on medicines, diagnosis, prescription and treatment. More studies should evaluate the impact of a high rate of self-medication among these students.
Keywords: over-the-counter drugs, irrationally, prescription, drugs
Introduction
Self-medication is the use of drugs or herbs to treat health conditions without advice from a medical professional in terms of the dose, indication, route and frequency. It also entails the continuous use of a previously prescribed medication to treat a recurrent illness.1 Over the counter (OTC) drugs are mainly used for self-medication because such medicines are easily accessible at pharmacies without the doctor’s prescription. Such drugs include pain relievers (acetaminophen), cough and cold medicines. However, due to regulation challenges, self-medication may be practiced, mainly in developing countries, using Prescription-Only Medications (POMs).2,3
Self-medication is a worldwide health problem with serious public health implications such as public health risks that include drug resistance, organ damage and contributes 2.9% to 3.7% of the deaths in the world, mainly due to drug–drug interactions.4 The unregulated access to both POMs and OTC drugs is likely to increase the prevalence of self-medication and its associated complications. Drugs should therefore be taken under the supervision of a qualified health practitioner in order to minimize the risks of inaccurate self-diagnosis, incorrect choice of therapy, inadequate or excessive dosage, food and drug interaction.5
Attitudes towards health care, gender, education, insurance policies, cost savings, convenience and age are among the factors that influence self-medication.6,7 Noteworthy, self-medication using OTC drugs may be safe and acceptable if the consumer has adequate knowledge of the drug and the illness.8 When practiced properly among the knowledgeable populations, self-medication can reduce the time spent waiting on physicians and some health expenses like the doctor’s consultation fees.6 However, POMs and OTC drugs are often considered unsafe when used irrationally8 leading to misdiagnosis or delayed diagnosis, different drug interactions and eventually increase disease burden in a population due to resistance.9
A prevalence of 96.8% was reported in Jordan,10 38.5% in Ethiopia,11 and 39.3% was documented among students of the Malaysian national defence university.7 In Northern Uganda, prevalence of self-medication with antimicrobials among the respondents was 75.7%.12 Universities are known to be the highest institutions of learning, with the students able to access accurate information on health. It is assumed that such a population can make important informed decisions regarding their lives. However, there are limited studies documenting self-medication in universities, specifically in Uganda. This research sought to document the prevalence, as well as patterns and factors associated with self-medication among students enrolled at MUST.
Methods
Study Design
A descriptive cross-sectional study design was utilized for this research.
Study Setting
The study was conducted at Mbarara University of Science and Technology which is a public university in Southwestern Uganda accredited by the National Council for Higher Education (NCHE). It has two campuses, that is, the Mbarara and Kihumuro campuses. The Mbarara campus is in Mbarara Municipality along the Kabale highway, 266km south west of Kampala, the capital city of Uganda. The Kihumuro campus is approximately 7km along the Mbarara-Bushenyi road. The total student population in both campuses is 4142 students. MUST offers Certificates, Diplomas, Bachelors and Masters Degrees and PhD studies in all disciplines. These programs are offered across six (6) faculties of Medicine, Science, Computing and informatics, Business and Management science, Applied sciences and Technology, Interdisciplinary studies, and two (2) institutes of Tropical forest conservation and Maternal newborn and child health.
Study Population
This study considered students currently enrolled at MUST. They were classified into medical and non-medical students. The medical students were students of medicine and surgery, pharmacy, pharmaceutical sciences, nursing, physiotherapy and medical laboratory sciences. The non-medical students included students in other faculties other than the Faculty of Medicine.
Inclusion Criteria
Students who were 18 years and above, mentally stable and enrolled at MUST during the study time were included in the study. All students approached expressed willingness to participate in this study.
Sample Size Determination
Sample size was determined using the Cochran formula for cross-sectional studies.13 Assuming maximum variability (p = 0.05), 95% confidence level, at 90% power, the sample size required was 384.
Sampling Technique
A multistage, stratified, cluster sampling technique was used to select research participants. The student population was first categorized into two (2) strata, that is, medical and non-medical students. Sawalha demonstrated that the patterns of self-medication between medical and non-medical students are likely to differ in most populations. Sample size determination for each stratum was done using the proportional allocation method.14 This is because the proportionality of medical students to non-medical students is not even. For the medical students’ stratum constituted 154 participants, while the non-medical students’ stratum constituted 230. Participants from either stratum were then selected by random sampling. From the non-medical stratum, random sampling was used to select three out of the total five faculties. Two departments from each of the selected faculties were selected. This gave a total of six departments. The required 230 participants were divided into six clusters. The medical stratum had six departments. Considering the 154 required participants, 25 were sampled from each of the six departments.
Data Collection
Data collection took place from January to April 2019. After self-introductions, the purpose of the study was explained to the participants in a private area identified by the investigators. Participation in the study was voluntary. An informed consent was sought from all participants, which they signed to indicate acceptance to participate in the study. An interviewer-led questionnaire was used to collect data in a quiet and private place. The interview was conducted in English. All filled forms were collected and kept securely in a lockable cabin.
The semi-structured questionnaire, contained both open and close-ended questions in the three sections. The first section sought information on socio-demographic and clinical characteristics such as age, sex, place of residence, faculty and year of study, religion, health insurance, alcohol use, social support, depression, and allergies. The Duke–UNC Functional Social Support15 tool was used to assess social support and the Alcohol Use Disorders Identification Test16 for alcohol consumption. The Hopkins Symptom Checklist (DHSCL) tool for depression was modified by adding a 16th item “feeling like I don’t care about my health” to reflect the local context as shown by previous studies on depression in Uganda.17,18 A test score of ≥1.75 denoted probable diagnosis of depression.19 The second section contained socio-economic variables that influence self-medication behavior. These included queries on health-seeking behavior, source of information that influenced self-medication, type and source of medication used and types of ailment treated through self-medication. The third section contained questions that intended to assess the knowledge of the respondents on self-medication. The tool was pretested on 20 randomly selected respondents in order to eliminate any ambiguous questions. The results of the pilot testing were not included in the final results.
Data Analysis
Each questionnaire was assigned a serial identification number. Data were entered and statistically analyzed using SPSS version 20. Descriptive data were presented in numbers and percentages. Chi-square (χ2) test was used for comparison between groups. Odds ratios and their 95% Confidence Interval were calculated. Significant predictors and all the other variables with a p value of less than 0.25 within the univariate model were entered into the regression model. Binary stepwise logistic regression analysis was used to control for confounders to self-medication. The statistical significance was considered at p < 0.05 for both univariate and multivariate analyses.
Ethical Approval
This study was approved by the Faculty Research Committee of Mbarara University of Science and Technology. All consenting participants gave written informed consent, or for those who could not write, a thumbprint was made on the consent form as approved by the ethics committees.
Results
The student respondents had a mean age of 21.5 ± 1.6 years (Table 1). Of the 385 respondents, there were 175 (45.5%) females and 210 (54.5%) males. Up to 27% were in the third year of study and above. Medical students were 153 (39.7%) while non-medical students were 232 (60.3%). Over 90% of respondents were Christians. Only 60 participants (15.6%) had health insurance and 310 (80.5%) respondents could access medical services whenever they needed them. The majority of the students interviewed spent ≤20,000 Ugandan shillings on health care per month. Thirty percent of the students interviewed had consumed alcohol in the previous 6 months and the median score for alcohol consumption was 0 (IQR = 0–2). Two hundred and fifty-six (66%) students reported to be active members of social support groups within their communities and the median social support score was 5 (IQR = 2–5). Participants had a median depression score of 1.83 (IQR = 1.5–2.1), with almost 60% categorized as being depressed. About half of the students (51.4%) were knowledgeable about self-medication.
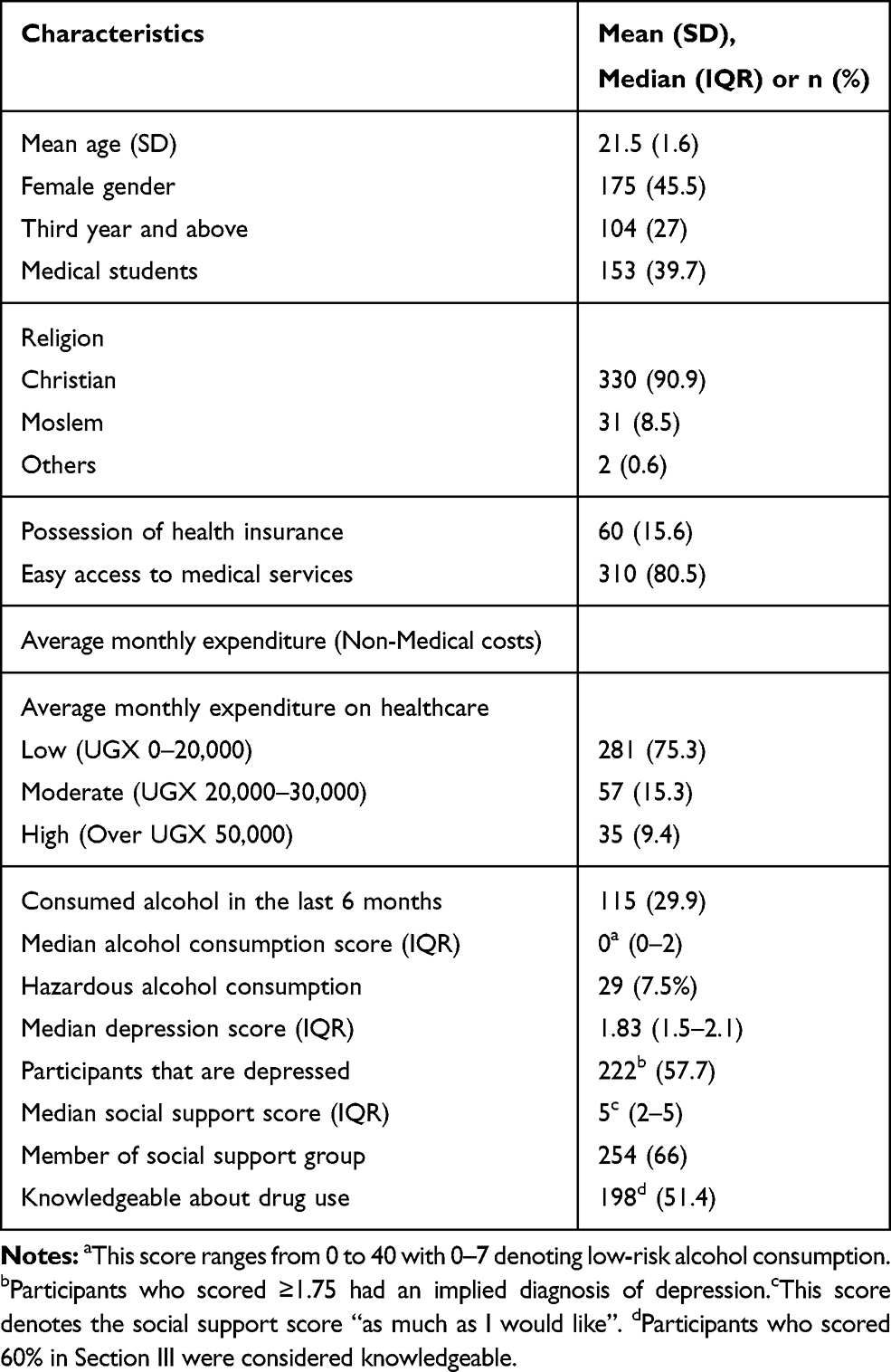 |
Table 1 Socio-Demographic and Clinical Characteristics of Students Enrolled at MUST |
The prevalence of self-medication was 63.5% (Table 2). The most frequently reported reasons for self-medication were that they classified their illnesses as minor (33%), self-medication saved time (15%), “had an old prescription” (11%) or high consultation fees (9%). Of those that self-medicate, the future preferred choices of care were the desire to consult a physician (60%) or continue to self-medicate (38%). The main reasons for not self-medicating included the risk of using wrong drugs (19%), insufficient knowledge (17%), fear of side effects (15%), wrong drug use (15%) or misdiagnosis (14%). The majority of respondents accessed these drugs from the pharmacy (56%), friends/family (17%) or clinics (15%). The drugs most commonly used for self-medication were headache relievers (20%), flu remedies (17%), cough remedies (12%), pain relievers (11%) and antibiotics (7%).
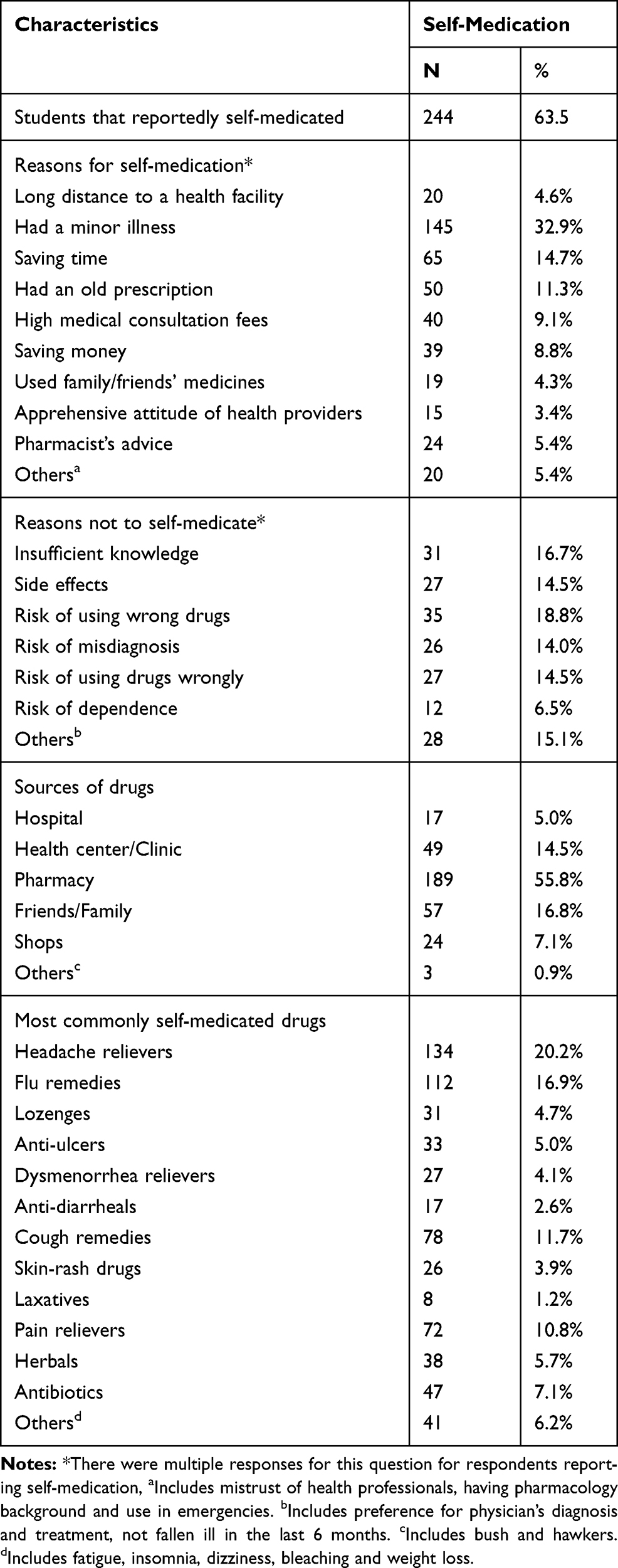 |
Table 2 Patterns of Self-Medication |
Considering the univariate model, the female respondents have higher odds of self-medicating compared to their counterpart males (OR = 1.91 [1.25–2.93], p = 0.03). The likelihood to self-medicate also increased with age (OR=1.71 [1.12–2.62], p=0.013), among students who have spent at least 3 years at the university (OR = 2.34[1.42–3.98], p = 0.001), reported to have an existing allergy (OR = 1.91[1.19–3.06, p = 0.007) and those respondents that were assessed to possess adequate knowledge on drug use (OR=1.76[1.16–2.67], p=0.008). Being a medical versus non-medical student, having an insurance cover, religion, alcohol use, depression, size of household, belonging to a social support group and having a monthly expenditure of greater or equal to 20,000 UGX were not associated with self-medication. From the multivariate model, likelihood to self-medicate increased among females (AOR = 1.83[1.15–2.90], p = 0.01), having existing allergies (AOR = 2.42[1.27–4.64], p = 0.009), and advance in the years of exposure at the university and/or age (AOR = 2.24[1.29–3.91], p = 0.004). On the other hand, self-medication strongly and significantly reduced with adequate access to medical services amongst respondents (AOR = 0.41[0.22–0.79, p = 0.007) (Table 3).
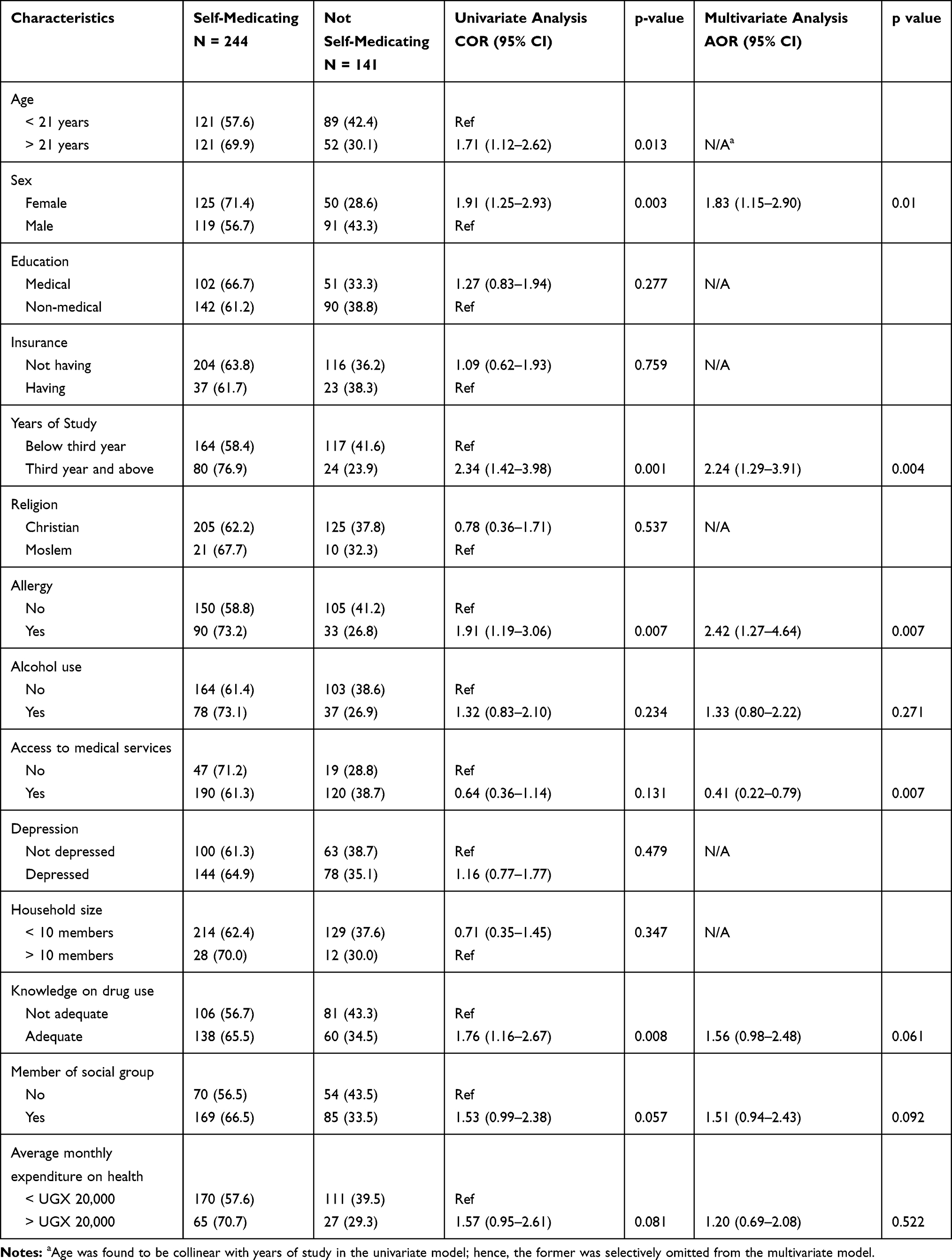 |
Table 3 Factors Associated with Self-Medication |
Discussion
We conducted a cross-sectional study to assess the prevalence, patterns and factors associated with self-medication amongst students currently enrolled at MUST in southwestern Uganda. The rate of self-medication was high at 64%, especially amongst female students, those in advanced years of study and those persons having an existing allergy. Access to medical services significantly reduced the chances of self-medication.
Studies in Northern Uganda-75.7%,12 Karachi university-76%,20 Egypt-62.9%6 and Nepal-84%9 have documented similar high rates of self-medication. While these scholars found a high rate of self-medication among university students, differences were observed in variations in sociocultural-demographic characteristics. Some studies were also limited by a relatively small sample size. The most commonly self-medicated drugs reported from this study were headache relievers, pain relievers, flu and cough remedies. This was in line with previous studies in Pakistan, Nigeria and India that documented symptoms of headaches, flu, cough, cold, fever and pain leading to self-medication.2,20,21
We reported major reasons for self-medication as; minor illnesses and saving time, consistent with previous studies,9,21,22 posing a great health risk to those that self-medicate in cases of misdiagnosis and/or wrong treatment. These minor illnesses could also develop into further health complications.23 Just like reported in previous studies, students at MUST that did not self-medicate in the last 6 months were afraid of the risk of using wrong drugs, were cautious of adverse side effects or lacked knowledge about medicines.24 Similarly, and as reported elsewhere, most of the students who self-medicated obtained their drugs from the pharmacy and friends and/or family.6,11
Our study observed correlations between gender and self-medication, with females self-medicating more than males. According to Obermeyer and colleagues, women were shown to have a higher concern for their health and therefore often self-medicated more than men who tended to be more concerned about affordability. Similar correlations have been documented in Ethiopia8 and Spain.25 Other reasons for self-medication peculiar to females such as monthly dysmenorrhea may be responsible for high rates of self-medication using pain and headache relievers.
We observed higher chances of self-medication amongst students with the current or previous record of allergies. According to Jain and colleagues, this is probably because many anti-allergy medicines in the form of anti-histamines are OTC medicines that lack stringent restrictions on access, hence their increased use in self-medication.26 A study in Brazil also showed that continuous treatment of a long-term allergy may bring about familiarity with the different medications leading to increased self-medication.27 Students in their first and second years of study self-medicated less than their counterparts in higher years, which was similar to other previous studies done in Malaysia,7 Slovenia28 and Ethiopia29 which attributed it to increased knowledge, with students reporting feelings of confidence in their ability to handle their own health challenges especially ones that they termed as minor illnesses. Access to medical services was also significantly associated with reduced rates of self-medication. Scholars have attributed easy access to medical services’ potential to prompt a person’s ability or intention to seek medical consultation and/or prescription within their communities, and thus reducing the chances of self-medication.30
Unlike other studies in Brazil, alcohol use was not statistically associated with self-medication among university students.31 Although reported alcohol consumption was high in our study (73.1%), hazardous alcohol consumption was low (8%) among this student population. The differences brought about by the negative effects of alcohol consumption on proper self-care, accounting for the tendency by alcoholics to self-medicate25 could, therefore, have been minimized in this population. In this study, just like previously reported elsewhere, medical students had a higher prevalence of self-medication than non-medical students.32 In both studies, findings indicated that there was no statistical significance between these two groups. However, other studies have shown that medical students self-medicated more than non-medical students because they may be more knowledgeable about the drugs and their access to drugs in the teaching hospitals is high.20
Most of the students interviewed spent less than 50,000 UGX per month on general costs and less than 20,000UGX per month on health care. Only 16% possessed a health insurance. Previous studies have associated increasing monthly expenditure on healthcare with increased chances of self-medicating.33 Although this association was not statistically significant for our study, this difference could possibly be due to the low income afforded by these students and the inconvenience afforded by lack of funds to purchase self-prescribed drugs out-of-pocket at the nearest drug store, opting to obtain free consultancy services and prescriptions from either the university clinic or government health facilities. This observation was similar to studies among university students of Rwanda and Ethiopia that cited higher purchasing power as a reason for increased self-medication.
This work presents data for students currently enrolled at MUST, a publicly funded and operated university in a rural low-resource setting with over 4000 students from various social and demographic backgrounds, making results generalizable to similar settings. The population considered in this setting as highly educated, also enabled us to document the prevalence, patterns and effect of age, year of study, income, gender, past/present medical or social status and access to medical care to self-medication. There were also limitations to this work. The questionnaire was interviewer-led and this could have led to social desirability bias where respondents may not have answered truthfully especially on sensitive questions. However, this approach ensured accurate assessment and completeness of the tool and maintained statistical power to detect differences.
Conclusion
Our study showed a 63.5% prevalence of self-medication among the university students currently enrolled at Mbarara University of Science and Technology. The most commonly self-medicated drugs were headache relievers, pain relievers, antibiotics, cough and flu remedies. Majority of respondents accessed these drugs from the pharmacy, friends and/or family and clinics. There were no differences in self-medication between medical and non-medical students. In adjusted analysis; females, having an existing allergy and being in advanced years of study beyond the third year increased the odds of self-medication. Access to medical facility/services reduced the chances of self-medication. These findings point to the vital need to extend the needed medical services to the students’ communities such as universities so that individuals receive appropriate diagnosis, prescription and treatment whenever needed. More studies are required to further evaluate the impact of this high rate of self-medication among this student population.
Disclosure
All authors report no conflicts of interest.
References
1. Bennadi D. Self medication; a current challenge. J Basic Clin Pharm. 2014;5:19. doi:10.4103/0976-0105.128253
2. Ehigiator O, Azodo CC, Ehizele AO, Ezeja EB, Ehigiator L, Madukwe IU. Self medication practices among dental,midwifery and nursing students. European J Gen Dent. 2013;2(1):54. doi:10.4103/2278-9626.106813
3. Chang FR, Trivedi PK. Economics of self-medication: theory and evidence. Health Econ. 2003;12(9):721–739. doi:10.1002/hec.841
4. Osemene K, Lamikanra A. A study of the prevalence of self medication practice among university students in south-western Nigeria. Trop J Pharm Res. 2012;11. doi:10.4314/tjpr.v11i4.21
5. WHO. Guidelines for the Regulatory Assessment of Medicinal Products for Use in Self Medication. 2000. Available from: https://apps.who.int/medicinedocs/en/d/Js2218e/. Accessed 11 February, 2020.
6. Helal RM, Elwafa HSA. Self Medication in University students from the city of Mansoura, Egypt. J Environ Public Health. 2017;7.
7. Haque M, Rahman NAA, McKimm J, et al. Self-medication of antibiotics: investigating practice among university students at the Malaysian National Defence University. Infect Drug Resist. 2019;12:1333–1351. doi:10.2147/IDR
8. Gutema BG, Gadisa DA, Kidanemariam ZA, et al. Self-medication practices among health sciences students: the case of Mekelle University. J Appl Pharm Sci. 2011;01(10):183–189.
9. Mehta RK, Sharma S. Knowledge, attitude and practices of self medication among students. IOSR J Nurs Health Sci. 2015;4(1).
10. Alshogran OY, Alzoubi K, Khabour O, et al. Patterns of self-medication among medical and nonmedical University students in Jordan. Risk Manag Healthc Policy. 2018;11:169–176. doi:10.2147/RMHP
11. Abay S, Amelo W. Assessment of self medication practices among medical, pharmacy and health sciences students in Gondar University, Ethiopia. J Young Pharm. 2010;2(3):306–310. doi:10.4103/0975-1483.66798
12. Ocan M, Bwanga F, Bbosa GS, et al. Patterns and predictors of self medication in Nothern Uganda. PLoS One. 2014;9(3). doi:10.1371/journal.pone.0092323
13. Cochran WG. Sampling Techniques. New Delhi: John Wiley & Sons; 1977.
14. Bowley AL. Measurements of precision attained in sampling. Bull Int Stat Inst. 1926;22.
15. Broadhead WE, Gehlbach SH, De Gruy FV, Kaplan BH. The DukeUNC functional social support questionnaire: measurement of social support in family. Med Care. 1988;26(7):709–723. doi:10.1097/00005650-198807000-00006
16. Babor TF, Higgins-Biddle JC, Saunders JB, Monteiro MG. The Alcohol Use Disorders Identification Test: Guidelines for Use in Primary Care, Second edition. 2001:17. Available from: https://apps.who.int/iris/bitstream/handle/10665/67205/WHO_MSD_MSB_01.6a.pdf;jsessionid=A8CA68CCE63DB108677533F245E4D850?sequence=1. Accessed 11 February 2020.
17. Bolton P. Cross-cultural validity and reliability testing of a standard psychiatric assessment instrument without a gold standard. J Nerv Ment Dis. 2001;189:4. doi:10.1097/00005053-200104000-00005
18. Tsai AC, Bangsberg DR, Frongillo EA, et al. Food insecurity, depression and the modifying role of social support among people living with HIV/AIDS in rural Uganda. Soc Sci Med. 2012;74(12). doi:10.1016/j.socscimed.2012.02.033
19. Derogatis LR. The Hopkins Symptom Checklist (HSCL): a measure of primary symptom dimensions. Mod Probl Pharmacopsychiatry. 1974;7(p):79–110.
20. Zafar SN, Syed R, Waqar S, et al. Self-medication amongst university students of Karachi: prevalence, knowledge and attitudes. J Pak Med Assoc. 2008;58(4):214–217.
21. Pandya RN, Jhaveri K, Vyas F, et al. Prevalence, pattern and perceptions of self-medication in medical students. Int J Basic Clin Pharmacol. 2013;2:1. doi:10.5455/2319-2003.
22. Tuyishimire J, Okoya F, Adebayo AY, et al. Assessment of self-medication practices with antibiotics among undergraduate university students in Rwanda. Pan Afr Med J. 2019;33:307. doi:10.11604/pamj.2019.33.307.18139
23. Banerjee I, Bhadury T. Self-medication practice among undergraduate medical students in a tertiary care medical college, West Bengal. J Postgrad Med. 2012;58(2):127–131. doi:10.4103/0022-3859.97175
24. James H, Handu SS, Al Khaja KA, Otoom S, Sequeira RP. Evaluation of the knowledge, attitude and practice of self-medication among first-year medical students. Med Princ Pract. 2006;15(4):270–275.
25. Carrasco-Garrido P, Jiménez-García R, Barrera VH, et al. Predictive factors of self‐medicated drug use among the Spanish adult population. Pharmacoepidemiol Drug Saf. 2008;17(2):193–199. doi:10.1002/pds.v17:2
26. Jain S, Malvi R, Kumar P. Concept of self medication: a review. Int J Pharm Biol Arch. 2011;2(3):831–836.
27. Emilia da Silva P, Knauth DR, Vigo Á, Mengue SS, PNAUM Research Group. Predisposing factors to the practice of self-medication in Brazil. PLoS One. 2017;12(12).
28. Klemenc-Ketis Z, Hladnik Z, Kersnik J. Self-medication among healthcare and non-healthcare students at University of Ljubljana, Slovenia. Med Princ Pract. 2010;19:395–401. doi:10.1159/000316380
29. Abebe D, Tenaw G, Dessalegn H, et al. Knowledge, attitude and practice of self-medication among health science students at Debre Markos University, Northwest Ethiopia. J Public Health Epidemiol. 2017;9(5):106–113. doi:10.5897/JPHE
30. Worku S, Mariam AG. Practice of self-medication in Jimma Town. Ethiop J.Health Dev. 2003;17(2):111–116.
31. da Silva MG, Soares MC, Muccillo-Baisch AL. Mucillo-Baisch, Self-medication in university students from the city of RioGrande, Brazil. BMC Public Health. 2012;12(1):339. doi:10.1186/1471-2458-12-339
32. Ullah H, Khan SA, Alietal S. Evaluation of self-medication amongst university students in Abbottabad, Pakistan; prevalence, attitude and causes. Acta Pol Pharm. 2013;70(5):919–922.
33. Awad A, Eltayeb IB, Capps PA. Self-medication practices in Khartoum State, Sudan. Eur J Pharmacol. 2006;62(4):317–324.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.