")
Back to Journals » International Journal of General Medicine » Volume 15
Pattern and Trends in Adult Hospitalization/Admission and Mortality Among Medical Ward Inpatients at Gadarif Hospital in Eastern Sudan: A Four-Year Retrospective Study
Authors Omar SM , Osman OS , Gasim GI , Adam I
Received 22 March 2022
Accepted for publication 22 June 2022
Published 30 June 2022 Volume 2022:15 Pages 5879—5889
DOI https://doi.org/10.2147/IJGM.S367513
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Saeed M Omar,1 Osama S Osman,1 Gasim I Gasim,2 Ishag Adam3
1Faculty of Medicine, Gadarif University, Gadarif, Sudan; 2Klerksdorp/Tshepong Hospital Complex, the University of Witwatersrand, Johannesburg, South Africa; 3Department of Obstetrics and Gynecology, Unaizah College of Medicine and Medical Sciences, Qassim University, Unaizah, Kingdom of Saudi Arabia
Correspondence: Ishag Adam, Email [email protected]
Purpose: Sub-Saharan Africa suffers from a dual impact of communicable (CDs) and non-communicable diseases (NCDs). There is scarce data on causes, trends of admission, and deaths among patients in Sudan. We aimed to determine the causes, trends of admission, and mortality among adult patients admitted to Gadarif Hospital in Eastern Sudan.
Patients and Methods: The medical records of adult patients admitted to Gadarif medical wards from January 2017 to December 2020 were reviewed for age, gender, causes of admission, and outcomes. Multivariate Cox regression analysis was used to analysis factors (age, sex, years, and disease) associated with the mortality.
Results: Of the 7230 patients who were admitted, 2221 (34.7%) were females and 5009 (69.3%) were males. The median age (interquartile range, IQR) was 47.0 (35.0) years. Of these 7230 patients, 3167 (43.8%) and 4063 (56.2%) patients were admitted with CDs and NCDs, respectively. Cardiovascular diseases (18.4%), snakebites (12.9%), and visceral leishmaniasis (12.0%) were the most common causes of admission. The overall in-patient adult deaths were 674 (9.3%). Cardiovascular diseases (22.3%), neurological diseases (16.9%), sepsis (15.9%), renal diseases (13.9%), and snakebites (8.3%) were the most common causes of inpatient mortality. Malignancy (20.7%), sepsis (20.9%), neurological diseases (17.4%), and cardiovascular diseases (13.8%) comprised the highest case fatality rates among the admitted patients. Using a Cox regression model (adjusted), age (adjusted hazard ratio = 1.02, 95% confidence interval = 1.01‒1.03) was associated with increased mortality hazard. However, the gender and years of admission were not associated with increased mortality hazard.
Conclusion: Admissions and mortality rates for CDs and NCDs are high compared with other African countries. Preventive measures are required to avert the high burden of these diseases. Health care systems in Sudan need to be prepared to deal with the dual burden of the diseases.
Keywords: communicable diseases, cardiovascular diseases, mortality, Sudan
Introduction
The burden of diseases in developing countries is continuing to surpass budgets allocated for healthcare. The medical admissions in impoverished countries account for about two fifths of total hospital admissions as compared to less than a third in rich countries.1,2 This may be a reflection of the big differences in socioeconomic conditions and healthcare systems, or differences in biological and/or environmental factors.3,4 One factor that worsens the healthcare crisis in sub-Saharan Africa (SSA) is the break of the HIV/AIDS epidemic, which disproportionately affects the region.5,6 However, interventions such as antiretroviral medications for the treatment of HIV/AIDS, health education, procurement of clean water, and mass vaccinations have reduced morbidity and mortality caused by communicable diseases (CDs).7–9
The improved life expectancy and the sedentary lifestyles have led to the eminence of non-communicable diseases (NCDs), a new risk to public health.10–12 Infectious and parasitic diseases are the major causes of admission in the different SSA countries.13,14 Moreover, different mortality rates were reported in different SSA countries.13,15 Likewise, while cerebrovascular disease and diabetes mellitus are predominant causes of death in some SSA settings,16 infectious and parasitic diseases are predominant in other settings.13,17,18
In Sudan and other SSA countries, there is an emerging increase in NCDs such as hypertension and diabetes mellitus, thereby impacting the public health.19 Moreover, Sudan has been hosting refugees for decades; particularly, the fleeing conflicts in the African Horn increases the complexity regarding public health in that particular region.20 However, malaria and lower respiratory infections remain the leading causes of years of lives lost.19 Apart from a few studies that has focused on individual diseases, published data examining the major causes of morbidity and mortality in Sudan is scarce.21,22 Understanding the major drivers of morbidity and mortality in one of the largest tertiary level hospitals in the eastern region of Sudan would help inform the country’s health system improvements.23 Thus, we aimed to assess the leading causes of hospital admissions and death among adults admitted to the medical wards in Gadarif hospital in Eastern Sudan.
Patients and Methods
Medical files (paper-based) of adult patients (≥ 18 years) admitted to Gadarif Hospital from January 2017 to December 2020 were retrospectively reviewed. Gadarif Hospital is one of the national referral hospitals in a country (Sudan) which has a population of about 40 million. It includes a bed-capacity of 400 and provides tertiary level care for patients referred from district and regional referral hospitals. The records of admitted patients were reviewed and the retrieved information included the patient’s age, sex, diagnosis, cause and date of death from the patient files during discharge. The diagnosis captured was the final diagnosis in the chart at the time of the patient’s discharge or death. In this work, for classification of causes of death, the tenth revised International Classification of Diseases (ICD-10) in the WHO global burden of disease estimates from 2000 to 2011 was used [23]. Records with missing information on diagnosis and date of admission were excluded. Both mortality rate “is a measure of the frequency of occurrence of death in a defined population during a specified interval” and case fatality rate “is the ratio of deaths occurring from a particular cause to the total number of cases due to the same cause” were calculated in this report.
Statistics
The data were entered into a computer using the Statistical Package for the Social Sciences (SPSS) Statistics for Windows, version 22.0 (IBM, Armonk, NY, USA). Continuous data were checked for normality using the Shapiro–Wilk test, and were found to be not normally distributed and were expressed as a median (interquartile [IQR]), while the categorized data were expressed as frequency (proportion). The Pearson chi-square and Wilcoxon rank-sum tests were used to compare categorical and continuous variables, respectively. Univariate proportional hazards regression was used to analysis factors (age, sex, years, and disease) associated with 30-day mortality. Multicollinearity was evaluated by the presence of high correlations between the variables (r≥ 0.9) or if the variance inflation factor was more than 4. There was no multicollinearity between the variables. Variables in univariate with P < 0.200 were shifted to build multivariate Cox analysis wherein the backward likelihood ratio (LR) was used to evaluate the independent effects of each covariate by controlling the effects of other variables. The hazard ratios (AHR) and 95% confidence intervals (CI) were computed. A p-value of less than 0.05 was considered statistically significant.
Results
Of the 7230 patients who were admitted, 2104 (29.1%) were admitted in 2017, 1999 (27.6%) in 2018, 1666 (23.0%) in 2019, and 1461 (20.2%) in 2020. Of these 7230 patients, 2221 (34.7%) were females and 5009 (69.3%) were males. The median age (IQR) was 47.0 (35) years. Of these 7230, 3167 (43.8%) and 4063 (56.2%) patients were admitted with CDs and NCDs, respectively (Table 1). The median (IQR) of the admission was 4.0 (5.0) days. The patients admitted in 2017 had a significantly higher age, while the age was significantly lower in patients who were admitted in 2019. The female proportions significantly decreased from 2017 to 2020. There was no significant difference in the rate of CDs during this time period (Table 1).
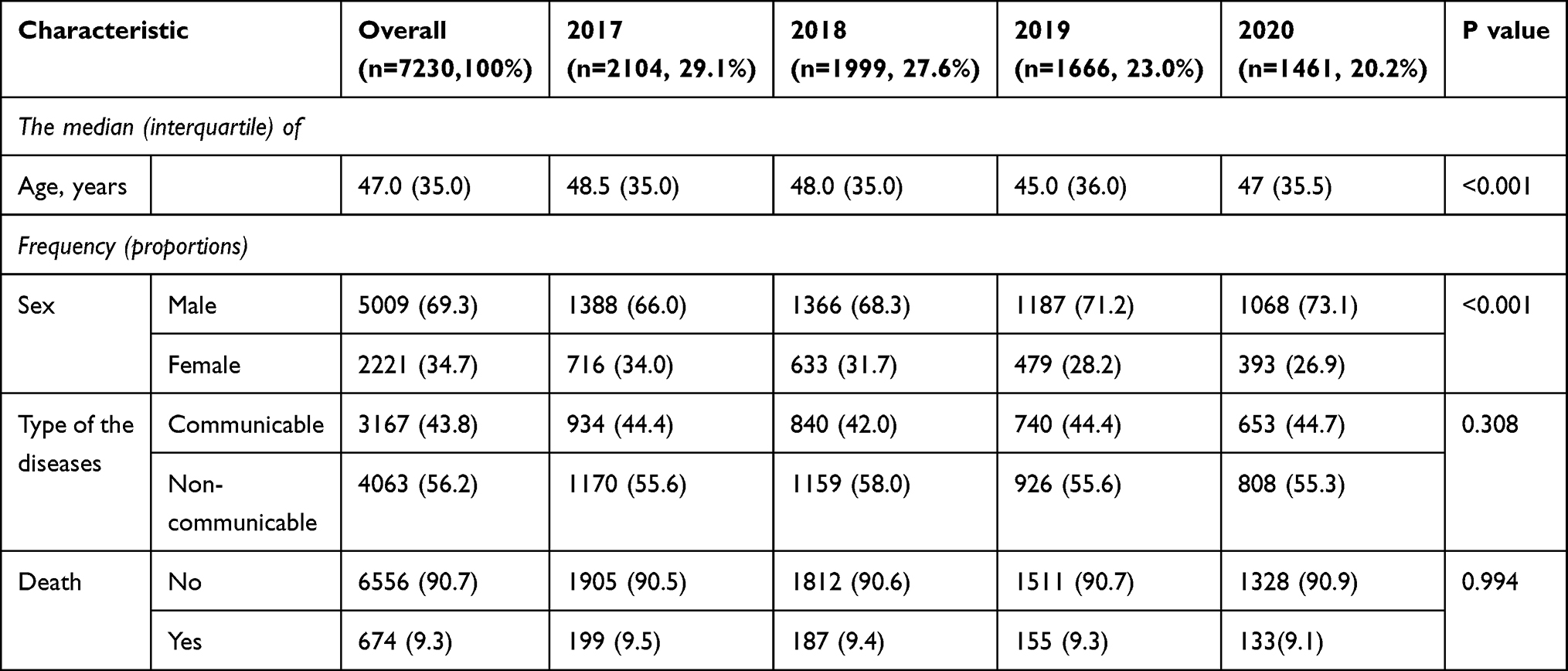 |
Table 1 In Patient Characteristics of the Adult in-Patients (Number=7230) at Gadarif Hospital During 2017–2020 in Eastern Sudan |
Cardiovascular diseases (18.4%), snakebites (12.9%), visceral leishmaniasis (12.0%), renal diseases (9.4%), neurological diseases (9.1%), diabetes mellitus (7.3%), sepsis (7.1%), and severe malaria (6.7%) were the most common causes of admission. The number of patients admitted with cardiovascular diseases was significantly higher in 2017 compared with patients admitted in 2019 [426/ 2104 (20.2%) vs 272/1666 (16.3%), P=0.002]. The number of patients admitted with snakebites was notably higher in 2019 than in 2018 [242/1666 (14.5%) vs 176/1999 (8.8%), P<0.001], (Table 2, Figure 1). While the number of patients admitted with visceral leishmaniasis was significantly higher in 2020, the number of patients admitted with severe malaria was remarkably higher in 2019. There was no significant difference in the number of patients admitted with sepsis during the period 2017–2020 (Table 2, Figure 1).
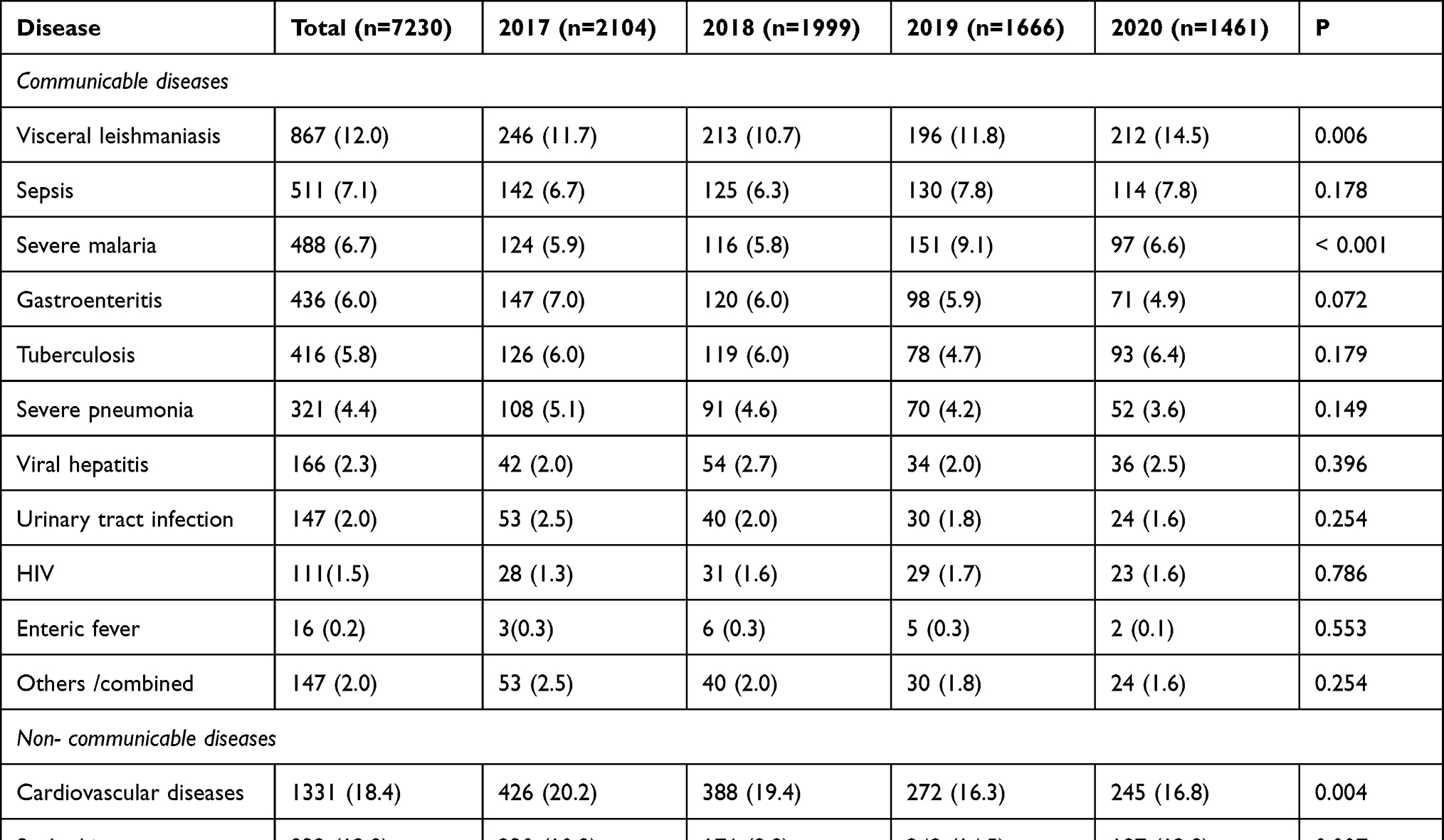 |
Table 2 Frequency (Proportions) of the Pattern of Admission of the Communicable and Non-Communicable Disease During 2017–2020 in Gadarif Hospital in Eastern Sudan |
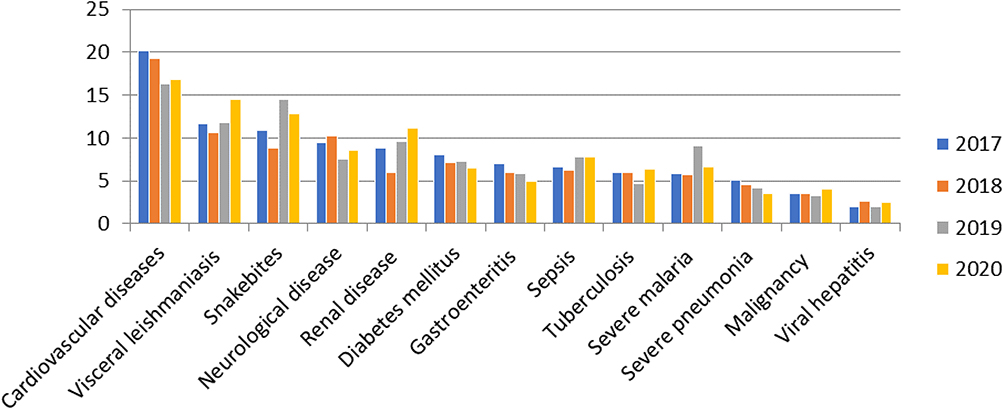 |
Figure 1 Frequency (proportions) of the pattern of admission of communicable and non-communicable diseases from 2017–2020 in Gadarif Hospital in Eastern Sudan. |
The overall in-patient adult deaths were 674 (9.3%); the proportion of patients who died during admission was not significantly different during the time period 2017–2020. There was no significant difference in mortality between patients admitted with CDs (300; 41.5%) and those admitted with NCDs.
Cardiovascular diseases (22.3%), neurological diseases (16.9%), sepsis (15.9%), renal diseases (13.9%), snakebites (8.3%), tuberculosis (7.6%), severe pneumonia (7.3%), visceral leishmaniasis (5.9%), and gastroenteritis (4.2%) were the most common causes of inpatient mortality. Causes of mortality (both CDs and NCDs) were not different during the years 2017–2020 (Table 3, Figure 2). Malignancy (20.7%), sepsis (20.9%), neurological diseases (17.4%), cardiovascular diseases (13.8%), and renal diseases (13.8%) had the highest case fatality rates among the admitted patients (Table 4, Figure 3).
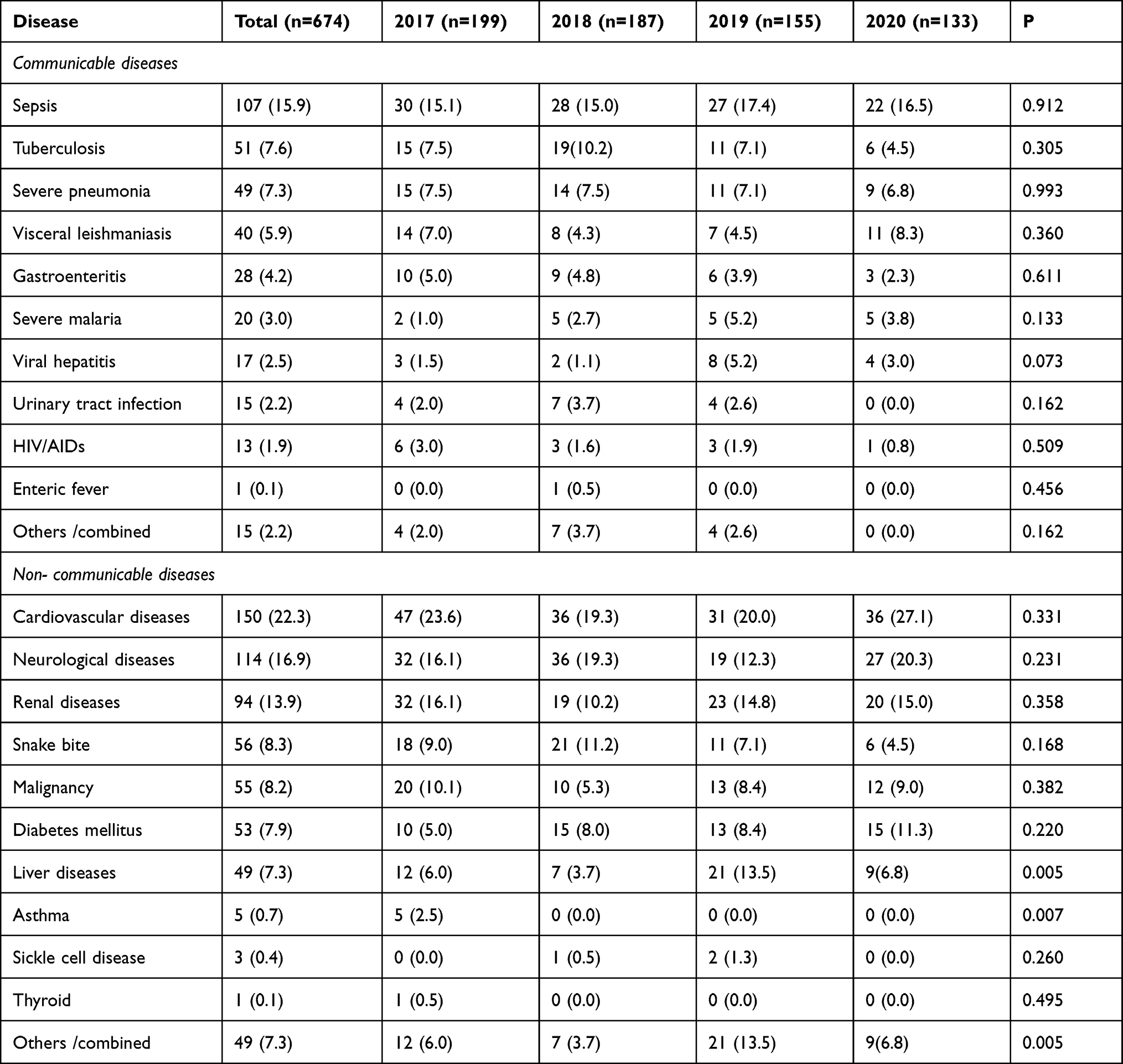 |
Table 3 Frequency (Proportions) of the Pattern of Mortality of the Communicable and Non-Communicable Disease During 2017–2020 in Gadarif Hospital Eastern Sudan |
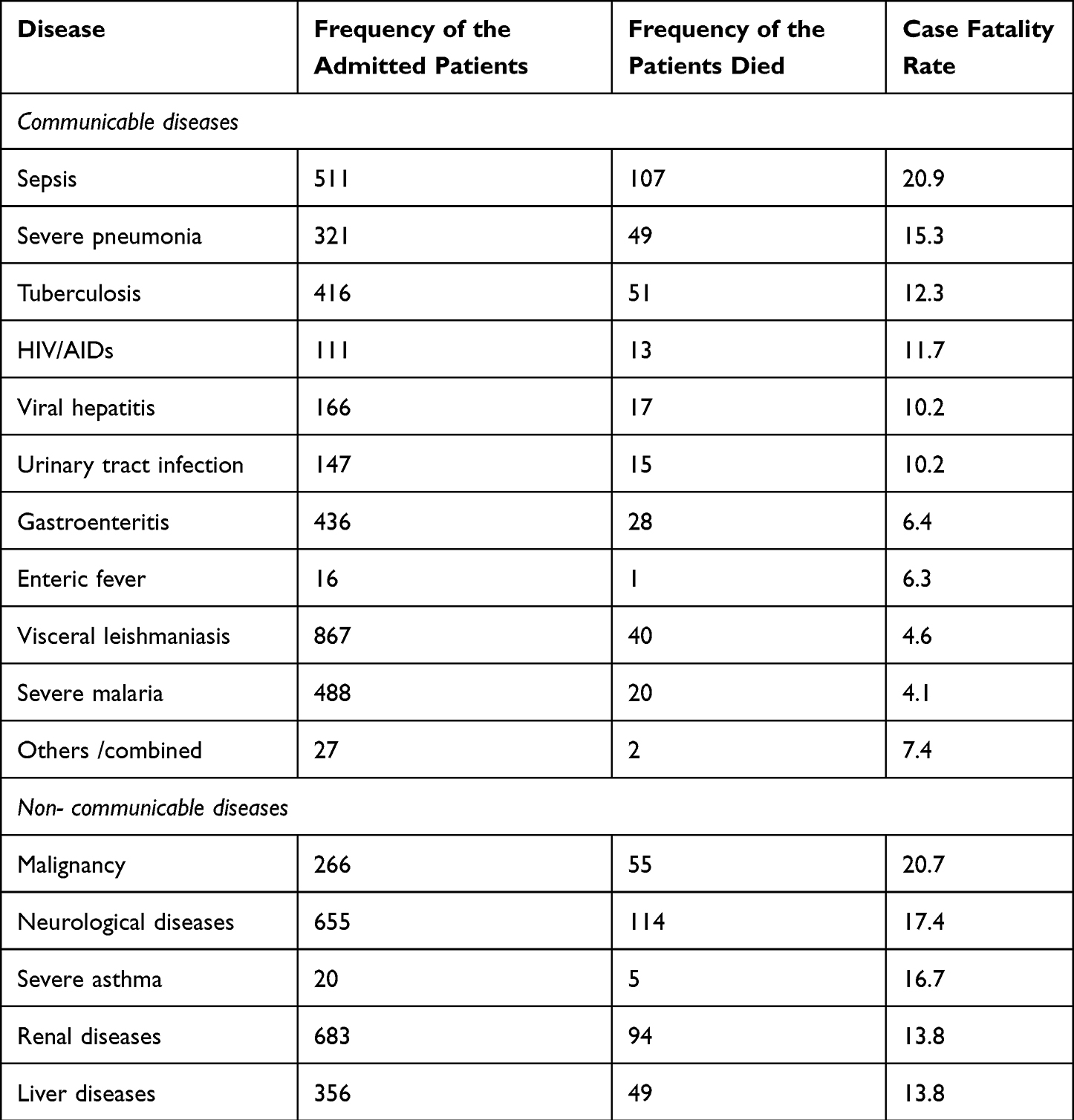 |
Table 4 The Case Fatality Rate of the Communicable and Non-Communicable Disease During 2017–2020 in Gadarif Hospital Eastern Sudan |
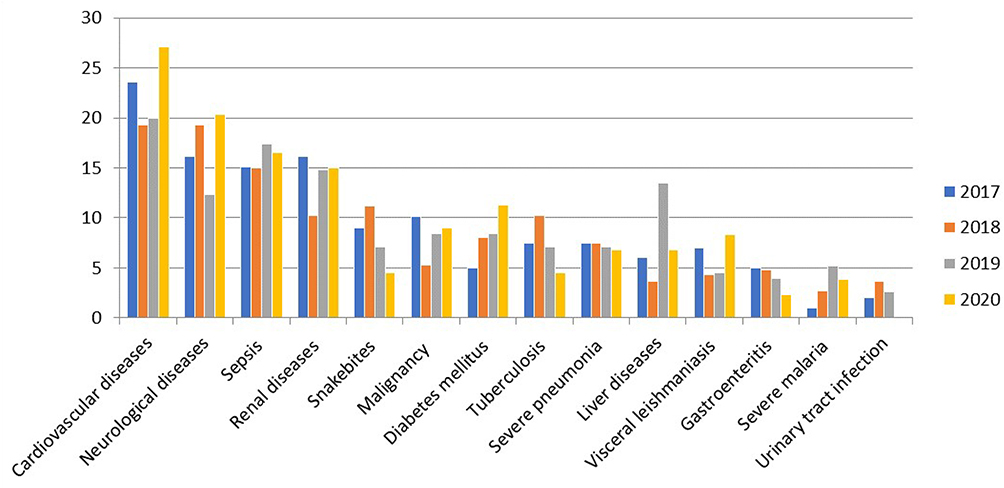 |
Figure 2 Frequency (proportions) of the pattern of mortality of communicable and non-communicable diseases from 2017–2020 in Gadarif Hospital in Eastern Sudan. |
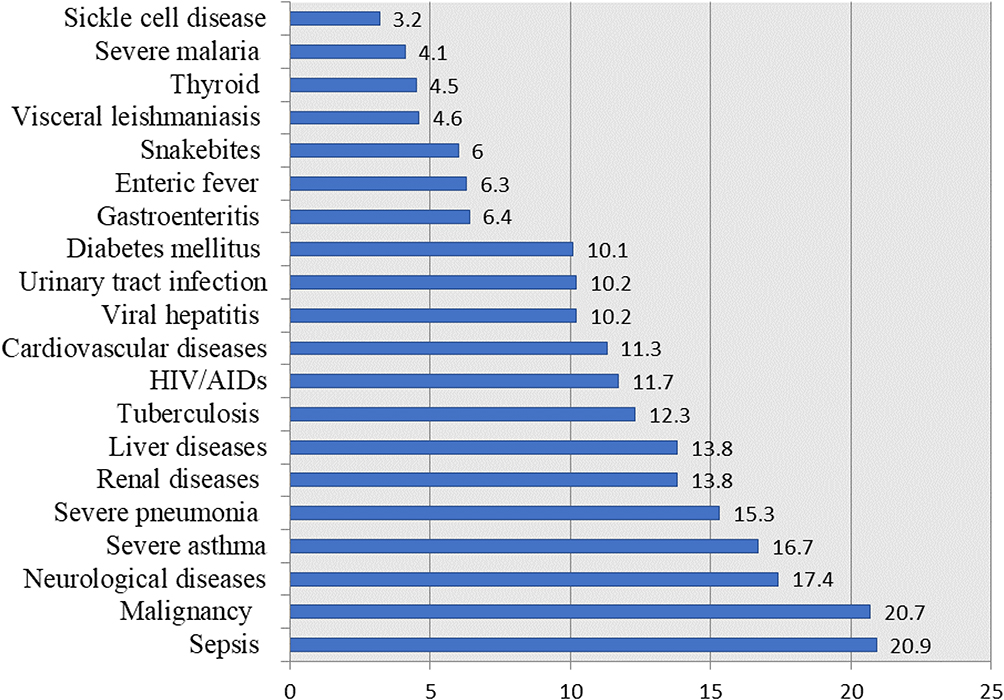 |
Figure 3 The case fatality rate of communicable and non-communicable diseases from 2017–2020 in Gadarif Hospital in Eastern Sudan. |
The median (IQR) age was significantly higher among patients who died compared those who did not. There was no significant difference in the number of males and females and number of patients with cardiovascular diseases between patients who died and those who did not. There were a significantly higher number of patients with sepsis, tuberculosis, neurological diseases, and renal diseases among patients who died compared to those who did not (Table 5).
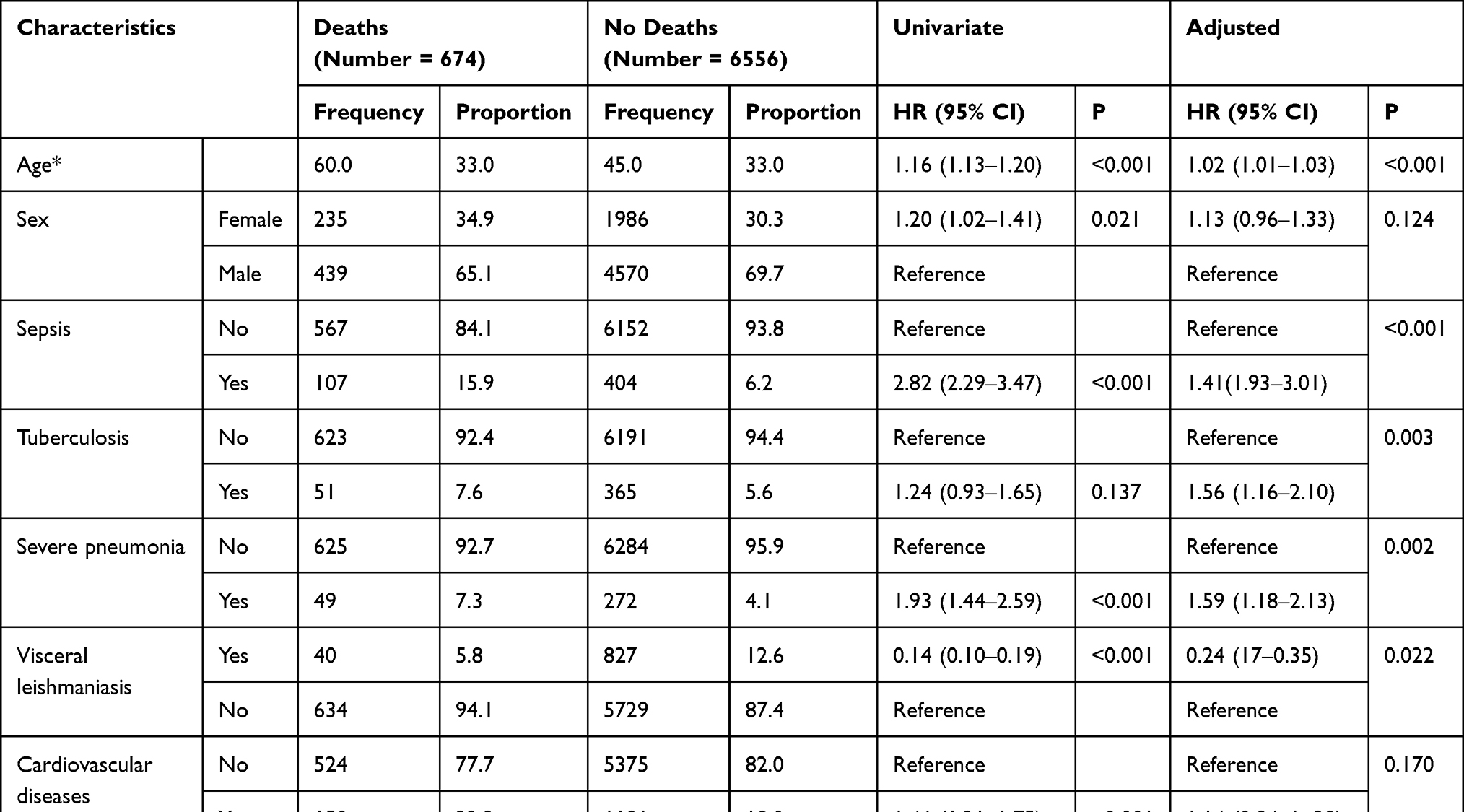 |
Table 5 Cox Regression (Adjusted and Non-Adjusted) Analysis for Factors Determining the In-Patient Mortality During 2017–2020 in Gadarif Hospital Eastern Sudan |
Using a Cox regression model (adjusted), age (AHR=1.02, 95% CI=1.01‒1.03), sepsis (AHR=1.41, 95% CI=1.93‒3.01), tuberculosis (AHR=1.56, 95% CI=1.16‒2.10), severe pneumonia (AHR=1.59, 95% CI=1.18‒2.13), neurological disease (AHR=1.81, 95% CI=1.46‒2.25), and renal disease (AHR=1.33, 95% CI=1.06‒1.66) were associated with increased mortality hazard. Visceral leishmaniasis (versus patients without visceral leishmaniasis) was associated with decreased mortality hazard (AHR=0.24, 95% CI=0.17‒0.35). Gender and cardiovascular disease were associated with increased hazard of death in univariate analysis only. Years of admission were not associated with increased mortality hazard (Table 5).
Discussion
The current study showed that cardiovascular diseases (18.4%), snakebites (12.9%), visceral leishmaniasis (12.0%), renal diseases (9.4%), and neurological diseases (9.1%) were the most common causes of adults’ admission. HIV/AIDS (30%), hypertension (14%), tuberculosis (12%), non-tuberculosis pneumonia (11%), and heart failure (9.3%) were the most common causes of admission in Uganda.13 A meta-analysis of thirty articles including 86,307 admissions showed that infectious and parasitic diseases were the leading causes of admission in Africa.14
Our results showed that 674 (9.3%) adult patients died and the death rate was not (significantly) different during the years 2017–2020. It has been estimated that adult mortality rate in Sudan in 2020 was 31.34 deaths per 100 population as compared to 24.06 deaths per 100 population in 1975. Therefore, the mortality rate has been growing at an average annual rate of 3.01%.24 Our results showed that the mortality rate (9.3%) was higher than the one reported in Nigeria (4.5%).15 However, the mortality rate (9.3%) in our study was lower than the inpatient mortality reported in Uganda (17.1%).13 In-hospital mortality rates did not differ over the four years of the study. These findings are in contrast to the ones reported in other parts of Africa.13,18 Our results have shown that cardiovascular diseases (22.3%), neurological diseases (16.9%), sepsis (15.9%), and renal diseases were the main causes of death. However, malignancy (20.7%), sepsis (20.9%), neurological diseases (17.4%), cardiovascular diseases (13.8%), and renal diseases (13.8%) have the highest case fatality rates. Cerebrovascular disease (12.8%), diabetes mellitus (8.1%), and chronic liver disease (6.3%) were the leading causes of death in Addis Ababa, Ethiopia.16 In case of Kersa, Eastern Ethiopia, 32.4% of deaths occurred due to infectious and parasitic diseases, 11.4% due to circulatory diseases, and 9.2% due to gastrointestinal disorders.17 In Uganda, non-TB pneumonia (28.8%), tuberculosis (27.1%), stroke (26.8%), malignancy (26.1%), and HIV/AIDS (25%) were the major causes of mortality among adults patients.13 Malaria (12.75%), respiratory diseases (10.08%), HIV/AIDS (8.04%), anemia (7.78%), and cardio-circulatory diseases (6.31%) were the principal causes of death in Tanzania.18 In the later study, all age groups were incorporated including neonates. Thus, in the later study, malaria and anemia were the causes of deaths in infants and children under 5 years, while HIV/AIDS and tuberculosis represented the major causes of deaths among adults.18 A meta-analysis of 30 articles and 9695 deaths showed that infectious and parasitic (17.1%), circulatory (16%), and digestive (16.2%) diseases were the leading causes of death in Africa.14 Our results showed that HIV/AIDs constitute only 1.5% of the causes of admission and 1.9% of deaths. HIV/AIDS was the most common (30%) cause of admission in Uganda13 and comprised around half (47%) of hospital deaths in Zambia.25
Our results were different from the other reports in Africa as we have demonstrated that visceral leishmaniasis was the leading (12.0%) communicable disease during admission, constituting 5.9% of the admission deaths and 4.6% of the case fatality rates. Visceral leishmaniasis is endemic in Sudan and is a significant public health problem, especially in Eastern Sudan.26 Eastern Sudan is characterized by high incidence, morbidity, and mortality associated with visceral leishmaniasis.23,27 There are consistently high rates of infection with about 16% death rate attributed to visceral leishmaniasis in Eastern Sudan.26 Another difference between our results and the alternate findings from other SSA countries concern snakebites, which is the second cause of admission (12.9%); it accounts for 8.3% of the causes of deaths and has 6.0% fatality rate. Using the annual health statistical reports of the ministry of health in Sudan during 2014–2018, Gadarif has recorded the highest rate of snakebites, and the death rate of inpatient cases with snakebites in Sudan was 2.5%.28 It has been recently reported that there were no deaths among a total of 2973 snakebite cases that were reported over the 5 years (2014–2018) in Ghana.29 Moreover, there was a low prevalence (0.0037 or 3.7/1000, 19 snakebite cases out of 5195 admissions) of snakebites among children admitted in Nigeria.30 However, the case fatality rate was 5.6% among these children.30 Interestingly, in Kenya, 382 community respondents reported that 9.1% of bitten community members and 14.6% of bitten family members died from snakebites.31 Thus, it seems that snakebite is a neglected health problem in Sudan and more effort is required to address this problem.
In the current study, the hazard of death was positively associated with age (AHR=1.02). Age was associated with increased inpatients’ mortality in Uganda (17.1%)13 and Ghana.32 Old age, frailty, and death are closely linked where aging concerns decline in reserve and function is viewed across various physiological systems culminating in failure to cope with different stressors.33 We have shown that females were at increased hazard of death in univariate analysis only. The absence of females and increased hazard of death indicate that this was only covariate. Recent studies have shown that probability of death was higher in females than in males.13
The retrospective nature study means limited access to other contributory factors that may determine outcomes. It was a single center study and although it might provide a broad idea about the trends and patterns of admissions in the country, however, results should be extrapolated cautiously owing to the special nature of the whole region due a greater endemicity of certain diseases such as visceral leishmaniasis and the high volume of refugee’s traffic that may show a different picture compared to the other regions in the country. The primary diagnosis used in the current study was the one made by the treating team at discharge and it did not look at deaths on arrival as well as re-admissions.
Conclusion
Admissions and mortality rates for communicable and non-communicable disease were high. Preventive measures are required to avert the high burden of these diseases. Health care systems in Sudan need to prepare to deal with the dual burden of the diseases.
Ethics Approval
The study received ethical approval from the Research Board at the Faculty of Medicine, University of Gadarif, Sudan (the reference number is 2020/13). Patients` consent to review their medical records was not required by the Research Board at the Faculty of Medicine, University of Gadarif, Sudan. Data were analyzed anonymously, Patients` data confidentiality and compliance covering patient data confidentiality and compliance were accordance with declaration of Helsinki.
Acknowledgments
The researchers would like to thank the Deanship of Scientific Research, Qassim University, for funding the publication of this project.
Disclosure
The authors report no competing interests in this work.
References
1. Ali EMW. Reasons and outcomes of admissions to the medical wards of Jimma university specialized hospital, southwest Ethiopia. Ethiop J Heal Sci. 2010;20(2):113–120.
2. Marszalek J, De Villiers PJ. Morbidity profile of admissions to GF Jooste Hospital, Manenberg, Cape Town. SA Fam Pr. 2006;48:15e.
3. Mair FS, Jani BD. Comment Emerging trends and future research on the role of socioeconomic status in chronic illness and multimorbidity. Lancet Public Heal. 2020;5(3):e128–e129. doi:10.1016/S2468-2667(20)30001-3
4. Katikireddi SV, Skivington K, Leyland AH, Hunt K, Mercer SW. The contribution of risk factors to socioeconomic inequalities in multimorbidity across the lifecourse: a longitudinal analysis of the Twenty-07 cohort. BMC Med. 2017;15:1–10. doi:10.1186/s12916-017-0913-6
5. Naicker S, Plange-rhule J, Tutt RC, Eastwood JB. Shortage of healthcare workers in developing countries–Africa. Ethn Dis. 2009;19:60.
6. Drimie S, Casale M. Multiple stressors in Southern Africa: the link between HIV/AIDS, food insecurity, poverty and children ’ s vulnerability now and in the future. AIDS Care. 2009;21:28–33. doi:10.1080/09540120902942931
7. Getawa S, Fentahun A, Adane T, Melku M. Antiretroviral treatment failure and associated factors among HIV-infected children on antiretroviral therapy: a retrospective study. Res Palliat Care. 2021;13:229–237.
8. Doherty TM, Del Giudice G, Maggi S. Adult vaccination as part of a healthy lifestyle: moving from medical intervention to health promotion. Ann Med. 2019;51(2):128–140. doi:10.1080/07853890.2019.1588470
9. Darvesh N, Das JK, Vaivada T, Gaffey MF, Rasanathan K, Bhutta ZA. Water, sanitation and hygiene interventions for acute childhood diarrhea: a systematic review to provide estimates for the lives saved tool. BMC Public Health. 2017;17(Suppl 4). doi:10.1186/s12889-017-4746-1
10. González K, Fuentes J, Márquez JL. Physical inactivity, sedentary behavior and chronic diseases. Korean Journal of Family Medicine. 2017;38(3):111–115. doi:10.4082/kjfm.2017.38.3.111
11. Bull FC, Al- SS, Biddle S, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sport Med. 2020;54(24):1451–1462. doi:10.1136/bjsports-2020-102955
12. Posadzki P, Pieper D, Bajpai R, et al. Exercise/physical activity and health outcomes: an overview of Cochrane systematic reviews. BMC Public Health. 2020;20:1–12.
13. Kalyesubula R, Mutyaba I, Rabin T, et al. Trends of admissions and case fatality rates among medical in-patients at a tertiary hospital in Uganda; A four-year retrospective study. PLoS One. 2019;14(5):e0237313. doi:10.1371/journal.pone.0216060
14. Etyang AO, Scott JAG. Medical causes of admissions to hospital among adults in Africa: a systematic review. Glob Health Action. 2013;6:19090. doi:10.3402/GHA.V6I0.19090
15. Okoroiwu HU, Uchendu KI, Essien RA. Causes of morbidity and mortality among patients admitted in a tertiary hospital in southern Nigeria: a 6 year evaluation. PLoS One. 2020;15:1–15. doi:10.1371/journal.pone.0237313
16. Fenta EH, Sisay BG, Gebreyesus SH, Endris BS. Trends and causes of adult mortality from 2007 to 2017 using verbal autopsy method, Addis Ababa, Ethiopia. BMJ Open. 2021;11(11):1–8. doi:10.1136/bmjopen-2020-047095
17. Ashenafi W, Eshetu F, Assefa N, et al. Trend and causes of adult mortality in Kersa health and demographic surveillance system (Kersa HDSS), eastern Ethiopia: verbal autopsy method. Popul Health Metr. 2017;15(1):1–10. doi:10.1186/s12963-017-0144-2
18. Mboera LEG, Rumisha SF, Lyimo EP, et al. Cause-specific mortality patterns among hospital deaths in Tanzania, 2006–2015. PLoS One. 2018;13(10):e0205833. doi:10.1371/journal.pone.0205833
19. Charani E, Cunnington AJ, Yousif AE, et al. In transition: current health challenges and priorities in Sudan. BMJ Glob Heal. 2019;4:e001723. doi:10.1136/bmjgh-2019-001723
20. National Academies of Sciences, Engineering, and Medicine.
21. Elshayeb AA, Ahmed AA, El Siddig MA, El Hussien AA. Prevalence of current patterns and predictive trends of multidrug ‑ resistant Salmonella Typhi in Sudan. Ann Clin Microbiol Antimicrob. 2017;16(17):1–11. doi:10.1186/s12941-017-0247-4
22. Philipp K, Parisi S, Schwienhorst-stich EM, Kasang C, Salah M, Tanyous E. Trends and patterns in leprosy in nine states of the Republic of the Sudan 7 years after the introduction of routine contact screening. Trans R Soc Trop Med Hyg. 2017;111(8):354–359. doi:10.1093/trstmh/trx063
23. Ahmed MAA, Al-nafeesah A, Al-wutayd O, Mahgoub M, Id IA. Severe childhood anemia and emergency blood transfusion in gadarif hospital, eastern Sudan. PLoS One. 2019;e0225731. doi:10.1371/journal.pone.0225731
24. Sudan Adult mortality rate, 1950–2021 - knoema.com. Available from: https://knoema.com/atlas/Sudan/topics/Demographics/Mortality/Adult-mortality-rate.
25. Chanda SL, Liusha N, Chansa A. Medical Ward In-Patient Mortality Patterns at a Tertiary Hospital in Urban Zambia: a one year review June 2018-June 2019. Med J Zambia. 2021;47(2):132–142.
26. Mueller YK, Nackers F, Ahmed KA, et al. Burden of visceral leishmaniasis in villages of eastern Gedaref State, Sudan: an exhaustive cross-sectional survey. PLoS Negl Trop Dis. 2012;6:11. doi:10.1371/JOURNAL.PNTD.0001872
27. Ahmed MAA, Musa IR, Mahgoub HM, Al-Nafeesah A, Al-Wutayd O, Adam I. Patterns, Outcomes and Predictors of Pediatric Medical Admissions at Gadarif Hospital in Eastern Sudan. Front Pediatr. 2022;10. doi:10.3389/FPED.2022.764028.
28. Khalid H, Azrag RS. Retrospective hospital-based study on snakebite envenomation in Sudan. Trans R Soc Trop Med Hyg. 2021;115(9):992–997. doi:10.1093/TRSTMH/TRAB085
29. Ceesay B, Taal A, Kalisa M, Odikro MA, Agbope D, Kenu E. Analysis of snakebite data in Volta and Oti Regions, Ghana, 2019. Pan Afr Med J. 2021;40. doi:10.11604/PAMJ.2021.40.131.28217.
30. Sanni UA, Lawal TO, Musa TL, Alege A, Na’uzo AM. Prevalence and outcome of snake bites among children admitted in the emergency pediatric unit, federal medical centre, Birnin Kebbi, Nigeria. Cureus. 2021;13. doi:10.7759/CUREUS.17413
31. Ooms GI, van Oirschot J, Waldmann B, et al. The Burden of Snakebite in Rural Communities in Kenya: a Household Survey. Am J Trop Med Hyg. 2021;105(3):828–836. doi:10.4269/AJTMH.21-0266
32. Sarfo FS, Awuah DO, Nkyi C, Akassi J, Opare-Sem OK, Ovbiagele B. Recent patterns and predictors of neurological mortality among hospitalized patients in Central Ghana. J Neurol Sci. 2016;363:217–224. doi:10.1016/J.JNS.2016.02.041
33. Qian-Li Xue P. The frailty syndrome: definition and natural history. Clin Geriatr Med. 2012;27(1):1–15. doi:10.1016/j.cger.2010.08.009
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.