")
Back to Journals » Patient Preference and Adherence » Volume 14
Patients’ Preferences Regarding Osteoarthritis Medications: An Adaptive Choice-Based Conjoint Analysis Study
Authors Al-Omari B , McMeekin P
Received 25 September 2020
Accepted for publication 26 November 2020
Published 22 December 2020 Volume 2020:14 Pages 2501—2515
DOI https://doi.org/10.2147/PPA.S283922
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Basem Al-Omari,1 Peter McMeekin2
1College of Medicine & Health Sciences, Khalifa University, Abu Dhabi, United Arab Emirates; 2School of Health & Life Sciences, University of Northumbria, Newcastle-Upon-Tyne, UK
Correspondence: Basem Al-Omari
College of Medicine and Health Sciences, Khalifa University, PO Box 127788, Abu Dhabi, United Arab Emirates
Tel +971 2 3124412
Email [email protected]
Background and Objective: Osteoarthritis (OA) patients consider ranges of harms and benefits offered by alternative pharmaceutical treatments. Choice-based experiments provide a mechanism to value outcomes, but they can pose a significant burden on respondents. Thus, the number of attributes studied is typically artificially restricted. We used an adaptive choice-based conjoint (ACBC) method that allows the inclusion of more attributes affecting patients’ preferences regarding non-invasive pharmaceutical treatment for OA than traditional choice-based technique to better understand the trade-offs that OA patients consider, without increasing respondents’ burden.
Methods: After consulting with OA patients and public involvement (PPI) group, we constructed an online ACBC survey consisting of 9 attributes and a total of 31 levels (two benefits, four harms and three concerning the availability and modality of treatment). A cohort of patients with a diagnosis of OA and reporting joint pain within the last 12 months were recruited.
Results: Our study (n 43) showed that the most important factor in choosing OA medication was the risk of heart attacks and strokes (19.5%), followed by the risk of addiction (18.4%), risk of kidney and liver side effects (17.5%), risk stomach side effects (14.6%), availability (11.6%), frequency of use (5.3%), pain reduction (5%), way of taking medication (4.6%) and mobility improvement (3.5%).
Conclusion: ACBC provides a mechanism for understanding patient preferences that address the limitations of traditional choice-based experiments. For OA patients, avoidance of the risk of side effects were the most affecting medication choices, and reductions in pain and mobility were the least. Clinicians discussing options for medication with OA patients should discuss the potential trade-offs in terms of risks and benefits.
Keywords: osteoarthritis, adaptive choice-based conjoint, conjoint analysis, patient preferences
Plain Language Summary
This study is using the novel online adaptive choice-based conjoint (ACBC) technique to collect and quantify patient preferences for osteoarthritis treatment. It addresses the limitations that were reported in previous similar studies by allowing researchers to include a large number of medication characteristics without complicating the conjoint task. It is an extension of previously published feasibility and pilot studies and it includes 9 attributes and a total of 31 levels, which makes it the most comprehensive choice experiment study regarding pharmaceutical treatment for osteoarthritis.
The study is potentially underpowered (n = 43) and the generalisability to osteoarthritis population might be limited in terms of treatment preferences. However, there is no consensus in relation to the sample size for conjoint studies and the novelty and contribution that the ACBC method introduces such as including a large number of attributes and levels compensates for this limitation. An ACBC questionnaire generally takes a longer time to complete than the traditional choice-based experiments but captures more information from each participant.
The results of this study indicate that patients’ preferences for pharmaceutical treatment for osteoarthritis is predominantly driven by patients desire to avoid the risk of side effects. This study also introduces ACBC as a practical tool that can be used to elicit patients’ preferences for the pharmaceutical treatment of OA.
Background
Pharmaceutical treatments for osteoarthritis (OA) are preference-sensitive.1,2 Studies have consistently shown that patients consider a range of implications of different treatments.3,4 More specifically, patients explicitly consider the trade-offs between different attributes of alternatives, in terms of benefits and harms.5–7 To date, the benefit of pain reduction and the harms from adverse events have been most often identified as the most important attributes to OA patients.1,3,8 However, some studies found that other benefits including improvement in function or reduction in pain were the most important.9,10 Other studies found that patients were more concerned about the risk of side effects.11–13 Costs and mode of administration have also been shown to be predictors of preferences in some studies.14–17 Therefore, eliciting patients´ preferences for OA treatment may enable therapists to better develop and implement patient-oriented treatment.18
The methods used to elicit patient preferences are referred to as stated-preference methods.19,20 The use of these methods in estimating the value of different attributes of health care is increasing.21,22 Stated-preference methods such as conjoint analysis require participants to make explicit choices between scenarios described in terms of levels of attributes.23 Where the level of an attribute refers to the amount or degree of that attribute, for example, an attribute could be “pain level” and levels of that attribute could be “no pain, mild pain, moderate pain, and severe pain”. Conjoint analysis is one of the survey methodologies that can be used to study preferences and quantify the trade-off that patients make between the different treatment factors on decision-making.24,25 Unlike traditional questionnaires, conjoint analysis poses several hypothetical scenarios and ask patients to rate/rank (rating/ranking approach) them or choose their preferred scenario (choice-based approach). If appropriately designed, implemented, analysed and interpreted, choice-based experiments offer practical alternatives and complement to the existing methods of valuation and preference elicitation by providing rich data sources for decision-making, allowing investigation of many types of questions, some of which otherwise would be intractable analytically.26
Choice-based experiments require an attribute-based measure of benefits.27 The value of healthcare is the sum of the values of each attribute.22 By modifying the levels and making choices between sets of attributes at differing levels, the additional amount of one attribute required to compensate for a reduction in others can be estimated and a set of values determined for all attribute levels. This means that choice-based designs assume that something can be valued in terms of the sum of the values of the set of attributes that define that thing, rather than the thing per se.26 It is consistent with consumer choice theory because it assumes the observed choices made reveal the true preferences of the participant. However, as the number of attributes and their associated levels increase, the complexity of choices increases along with the number of choices that need to be made in order to estimate these values.28 A full factorial design is usually used to generate all possible combinations of all levels of the included attributes.29 An omission of an attribute from a choice-based experiment means that the preferences of the participant would not be completely nor accurately captured.26
Techniques, where patients are given overlapping subsets of choices and responses combined, can address the issue of respondent burden.29 However, this is at the cost of increasing the number of patients needed to complete the questionnaire. Generally, the higher number of attributes in a traditional choice study requires a larger sample.30 For example, Laba and colleagues required a sample of 503 participants for a study that included 7 attributes and 20 levels,11 while Ratcliffe and colleagues recruited 412 participants to study 5 attributes and 15 levels.12 Alternatively, the number of attributes and their levels can also be restricted, such as Fraenkel and colleagues study,9 that included 4 attributes and 12 levels in a sample of 304 participants and Byun and colleagues,10 who recruited 100 participants to quantify the values of 4 attributes and 12 levels. Therefore, the choice of the design for a choice experiment is critical as it determines which attributes’ effects and their interactions are identifiable.31
In this paper, we estimate patients’ preferences for OA treatments using a novel adaptive choice-based conjoint (ACBC) technique. ACBC analysis is a technique that uses choice data and incorporates it into an adaptive interviewing experience,32 and it accommodates a greater number of attributes and levels than previous conjoint-analysis methods.33 Previous conjoint studies were unable to include all medication characteristics such as kidney and liver side effects, as that would have overly complicated the questionnaire and suggested that the inclusion of these additional adverse effects. Even if by doing so, it may improve our understanding of patient preference regarding OA treatment.14–16,34 The use of ACBC addresses this reported limitation. The advantages of ACBC that it provides more information about patient preferences.35 ACBC is implemented in software and seeks to reduce the number of choices a patient is presented with by eliminating irrelevant choices from the choice sets presented to a patient, the patient is required to complete shorter choice sets compared to non-adaptive technique.33,35 This means that it is not easily possible to compare sample sizes between ACBC studies and other traditional conjoint methods where one responded may only contribute data about a small number of characteristics. Furthermore, due to the format of ACBC studies, respondents may be more engaged in the survey‐taking experience and provide answers that are more in‐line with their actual choice behaviour.32
Taking into consideration the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) guidelines for conjoint-analysis to pilot conjoint studies,36 we conducted a pilot test of the ACBC questionnaire with a research user group (RUG) to gather patient feedback.8 In another study, we have previously established that ACBC is a feasible method for eliciting patients’ preferences regarding OA treatment.37 The pilot study considered the patients’ preferences for OA treatment by collecting date from 11 OA patients who were members of patients and public involvement (PPI) group.8 Furthermore, we have also used this method to generate an individual patient’s preferences.28
Methods
Patient and Public Involvement
The research design, attributes and levels, questionnaire development, and presentation of data were developed and tailored based on the feedback provided by the research users’ group (RUG) members, part of the wider public and patient involvement (PPI) group in the Arthritis Research UK Primary Care Centre at Keele University, UK. This study is an extension of a pilot study,8 two feasibility studies,37 and individual patient preference analysis study.28 Due to geographical distance the initial RUG members were not directly involved in the recruitment of participants. However, their recommendation regarding the inclusion criteria was considered and applied. The previous feasibility studies were comprehensive and had established 1). the clarity of the ACBC question formats; 2). the amount of information that participants needed to understand the ACBC task; 3). participants acceptance of the design and wording of the ACBC task; 4). the practicality of completing the ACBC task; and 5). whether the stated preference from the ACBC task reflected the participants’ beliefs of their preferences.37
Participants and Recruitment
Patients were from Newcastle-upon-Tyne and surrounding areas in the north-east of England. Posters, emails, and newsletters about the study were published via Healthwatch Newcastle, Healthwatch North-East, and staff and students at the faculty of health and life sciences at Northumbria University. Healthwatch Newcastle is 1 of the 152 Healthwatch that work in each local authority area in England,38 and they have statutory powers under the Health and Social Care Act 2012.39 Healthwatch aims to help children, young people and adults to have a say about health services and to include people who sometimes struggle to be heard and are independent of health-care providers.38 For this ACBC study, the aim was to recruit a total of 40 for analysis of patients’ preferences regarding the non-invasive pharmaceutical treatment of OA. This number of participants was determined after consultation with the Healthwatch team and based on the available resources and anticipated rates of recruitment.
Patients were included in the study if they 1). are adults above the age of 18 years old, 2). have a diagnosis of OA from their doctor, 3). reporting joint pain in the past 12 months. Patients were excluded if they 1). are not complaining of joint pain, 2). have other illnesses that may contribute to or cause their joint pain such as rheumatoid arthritis or osteoporosis. Patients who were interested in taking part in the study contacted either the Healthwatch team or the researcher directly. This method of recruitment provided patients with the choice to participate or not, as the researcher and Healthwatch team had no patient–provider relationship that may impact actual healthcare based on the patients’ decision to participate.
Attributes and Levels
Defining attributes and levels is one of the most critical aspects of designing a good conjoint analysis study.40 The attributes and levels were identified based on being factors that influence patient preference regarding the non-invasive pharmaceutical treatment of OA. The inclusion of the attributes and levels were based upon 1). a full systematic search to identify the attributes used in similar studies, 2). recommendation to include more side effect attributes by experts in the field,34 3). an ACBC feasibility study,37 4). discussion with a rheumatologist, rheumatology pharmacist, research methodologists, PPI coordinators, and RUG members. For example, patients at the RUG were given the choice of having evidence-based percentage levels representing the actual risk of medication or other wording and they opted to “No, Low, Moderate, and High” as levels for the risk of adverse effects. The RUG patients felt that the actual percentage of risks such as “2%, 4%, and 8%” for a medication adverse effect would not mean much to them and they will not be able to understand it in terms of trading-off levels against each other. The RUG suggested using percentage for the benefit attributes to make it easier for them to differentiate between a benefit and adverse event attribute. Furthermore, the RUG suggested eliminating 0% and 100% as they must expect some benefit but this will never be 100% from the medications. Similar free choices were given to the patients in all attributes and levels and the wording was developed based on their suggestions. The financial cost was not included in this study because the cost of medications for older persons in the UK healthcare system is rarely a direct issue. In this study, we formulated attributes and levels that are realistic within the context of the study and are credible to respondents.35,40
In this study, the ACBC value-set had a total of 9 attributes and 31 levels compared to a total of 8 attributes and 28 levels in the pilot (Table 1). To address the limitation identified during the pilot,8 (imbalance between risks and benefits attributes 4 to 1), an additional benefit attribute was added. While OA treatments aim to reduce pain and improve mobility.41,42 The previously used benefit attribute in the pilot,8 and feasibility,37 studies (Expected percentage of benefit) was split into two attributes in this study (How much you would expect mobility improvement AND How much you would expect pain reduction), representing pain reduction and mobility improvement. These two attributes were originally developed with the assistant of the RUG and experts in the field, and the decision to combine them was a result of a need to reduce the number of attributes. The wording used in all attributes and levels were based on RUG recommendations and suggestions in the pilot and feasibility studies.8,37
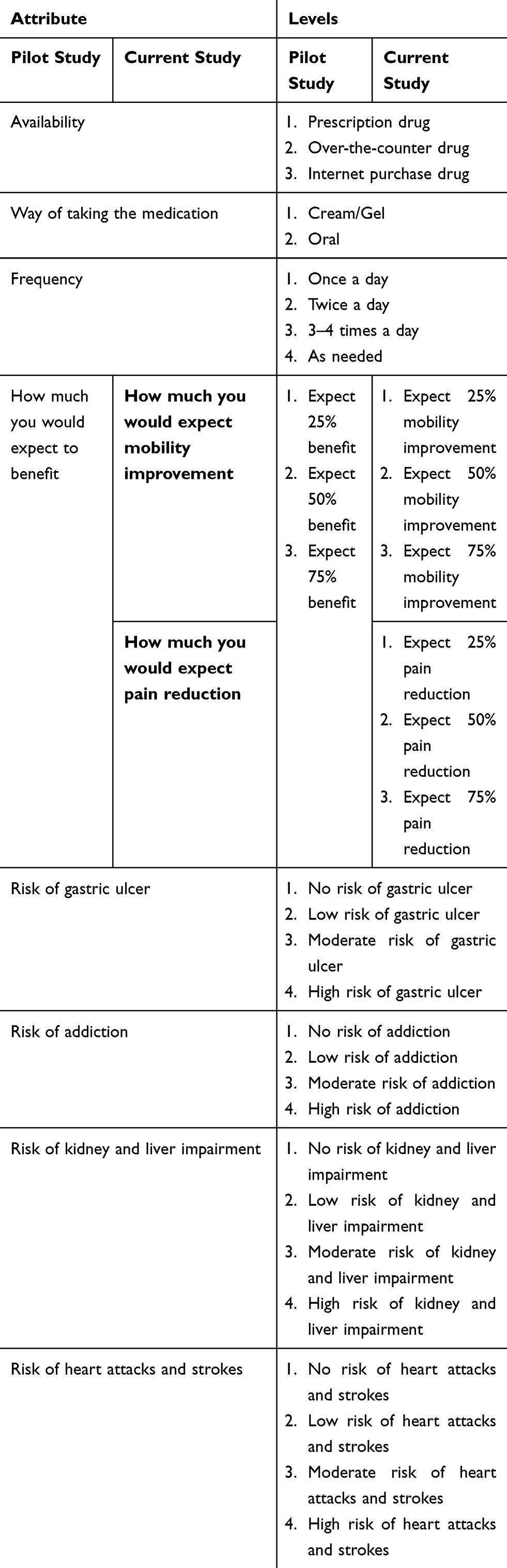 |
Table 1 Attributes and Levels Used the Pilot and in This ACBC Study |
ACBC Questionnaire and Data Collection
Patients who expressed an interest in taking part in this study were contacted by phone and/or email to determine their eligibility to be included. Eligible participants were given the option of completing the ACBC questionnaire online independently or being visited at home to complete the ACBC questionnaire online. All patients were given a Uniform Resource Locator (URL), their unique username, and the password. A Prompt email was sent after two weeks and three weeks to remind participants who did not complete the ACBC questionnaire. All questionnaires were completed between January/June 2017.
The web-based interactive ACBC questionnaire was developed by the lead researcher BA using the SSI web version (8.2.4). The process of developing the ACBC questionnaire was the same as that used previously by Al-Omari and colleagues,8,28,37 and was consistent with the PPI recommendations in these studies. The first screen in the ACBC questionnaire introduced the task and included the consent form. This was followed by questions on demography and the respondents’ health. The main ACBC task consisted of three stages:
Stage 1: Build your own (BYO) section, which introduces all attributes and levels and asks the respondents to indicate the preferred level for each attribute (see Figure 1 for an example of this question).
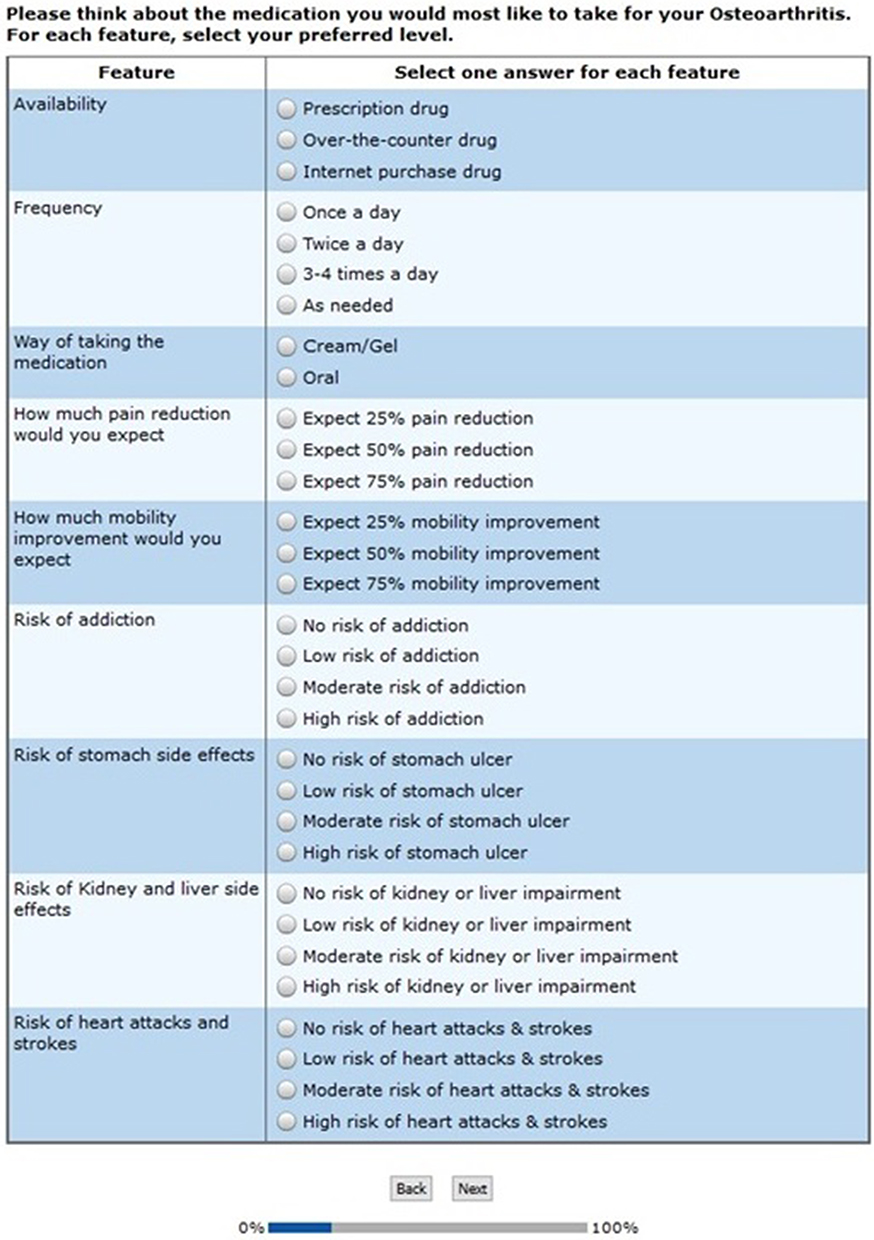 |
Figure 1 An example of Build Your Own (BYO) question. |
Stage 2: Screening section, which includes three different types of questions: 2.1). Screening questions, these are scenarios questions generated by the software based on each respondent’s preferred levels in the first stage (see Figure 2 for an example of this question). 2.2). Unacceptable questions, these are questions where respondents indicate if they are trying to avoid a specific level (see Figure 2 for an example of this question). 2.3). Must-Have questions, these are questions where respondents indicate the most important level that they are not willing trade-off (see Figure 2 for an example of this question).
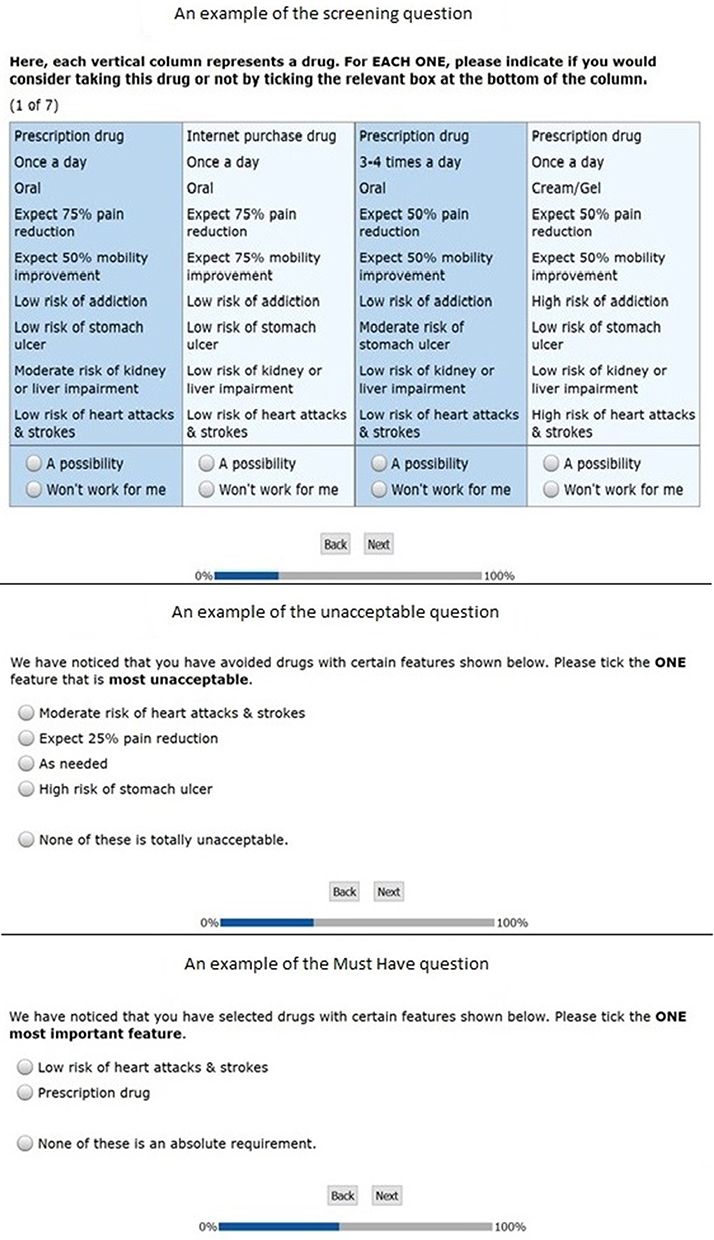 |
Figure 2 Examples of the screening section questions. |
Stage 3: Choice tasks section, which includes a series of choice tasks presenting three scenarios in each screen and asks the participants to choose their preferred scenario (see Figure 3 for an example of this question).
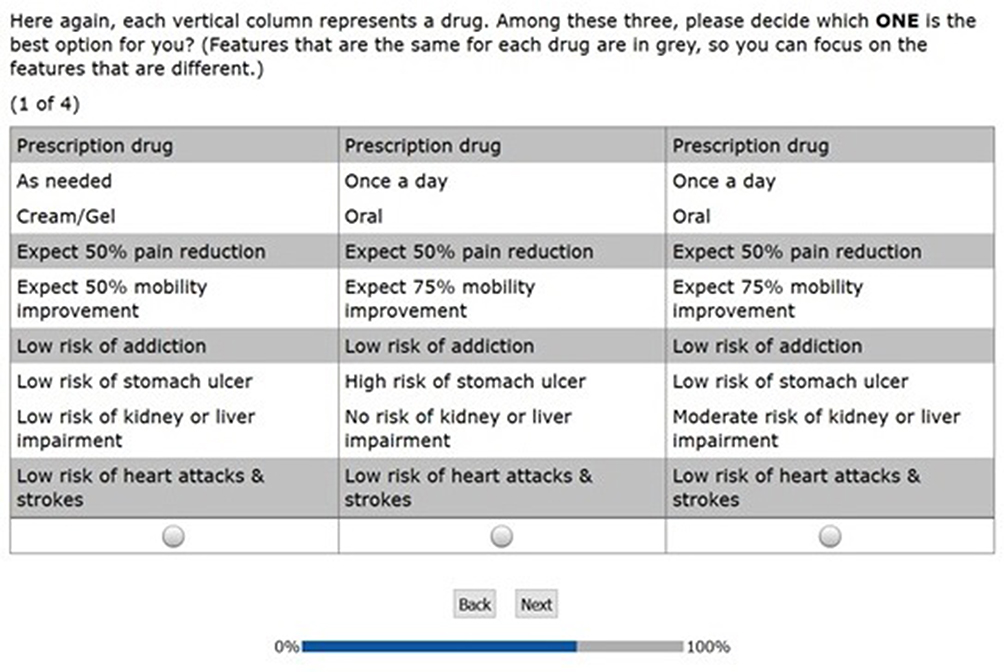 |
Figure 3 An example of the choice task question. |
Our study addressed the key recommended points before fielding an ACBC study, as recommended by Sawtooth (the developer of the ACBC software) (Table 2).43
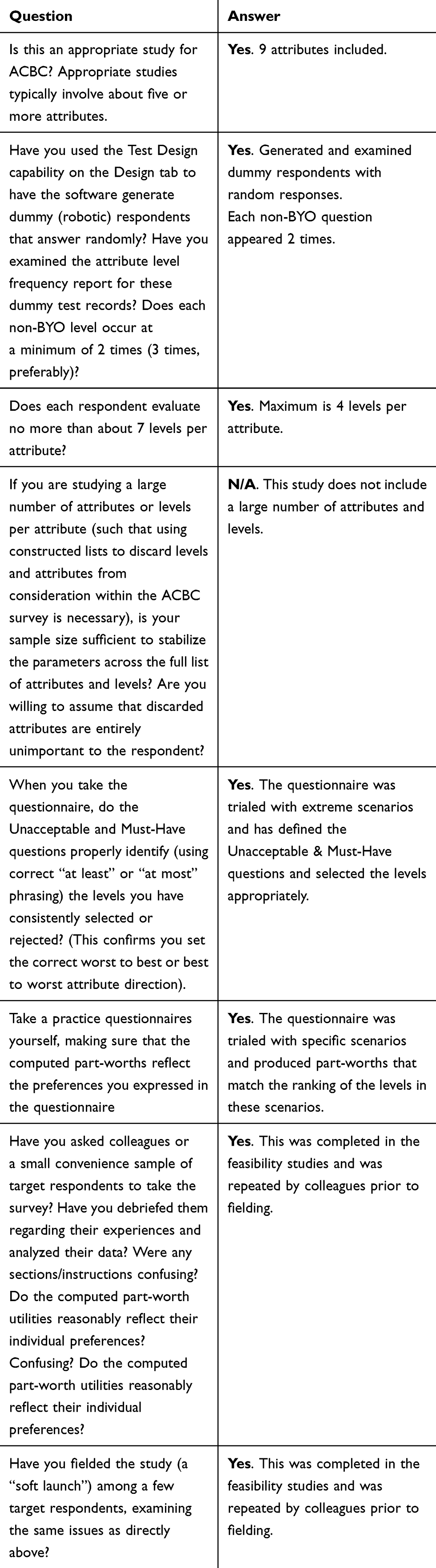 |
Table 2 Sawtooth recommended 8 Points to Be Checked Before Fielding an ACBC Study |
Data Analysis
Descriptive statistics were used to summarise frequencies with percentages for categorical variables. The ACBC software has a built-in Hierarchical Bayes (HB) analysis model which was used to analyse the relative importance and part-worth of the attributes and levels. HB model requires less information per subject than other statistical models for choice analysis.44 The attributes are measured by the relative importance, which represents the weight that patients place on each attribute in comparison to the remaining attributes.28 The levels of the attributes are measured by part-worth (utilities), which represent the weight that patients place on each level in comparison to the remaining levels of the same attribute.33
An attribute relative importance is estimated “by considering how much difference each attribute could make in the total utility of a product. That difference is the range in the attribute’s utility values”.45 The relative importance is ratio-scaled and relative. The combined relative importance for all attributes sums up to 100%. An attribute with the relative importance of 20% is twice as important as an attribute with the relative importance of 10% within the same set of attributes used in the study.45 For example, if a study included attributes A, B, C, and D and the relative importance of these attributes were 20%, 30%, 10%, and 40%, respectively, this would mean that the most important attribute is “D” and the least important is “C”. It also means that attribute “D” is twice as important as attribute “A” and four times as important as attribute “C”.
The ACBC HB analysis estimates individual-level utility coefficients and rescales all levels in each attribute using zero-centred differences method.28 This analysis allows the estimation of individual utility coefficients to be constrained based on each participant’s response to additional questions, or globally when all respondents are assumed to have the same preference order.46 The utility for each level is a number that represents the weight that a respondent puts on that particular level in the context of other levels within the same attribute.28 The level that holds the highest utility value in each attribute is the most preferred one. The level that holds the lowest utility value (in the minus) is that the patient least prefers and does not represent negative utilities or disutility. Utilities of all levels in each attribute are scaled to sum to zero.47 Unlike traditional conjoint-analysis, ACBC utility scores are arbitrary given by the software and they present interval data scaled to an arbitrary additive constant within each attribute.45 Therefore, the utility value of one level in an attribute cannot be arithmetically compared with the value of another level in another attribute. The utility values and the intervals between the values have a meaning within each attribute but cannot be compared across several attributes.
Results
Participants’ Characteristics
Forty-three participants in total were recruited and completed the online ACBC questionnaire (response rate (RR) 100% - 43 recruited and the same 43 completed the study). All participants were adults (13 males [30.2%] and 30 females [69.8%]), who reported joint pain within the last 12 months and have a diagnosis of OA confirmed by their doctors in at least one joint. The mode age categories were 40–49 and 70–79 years old. Only one participant was under the age of 30 years old. (Table 3).
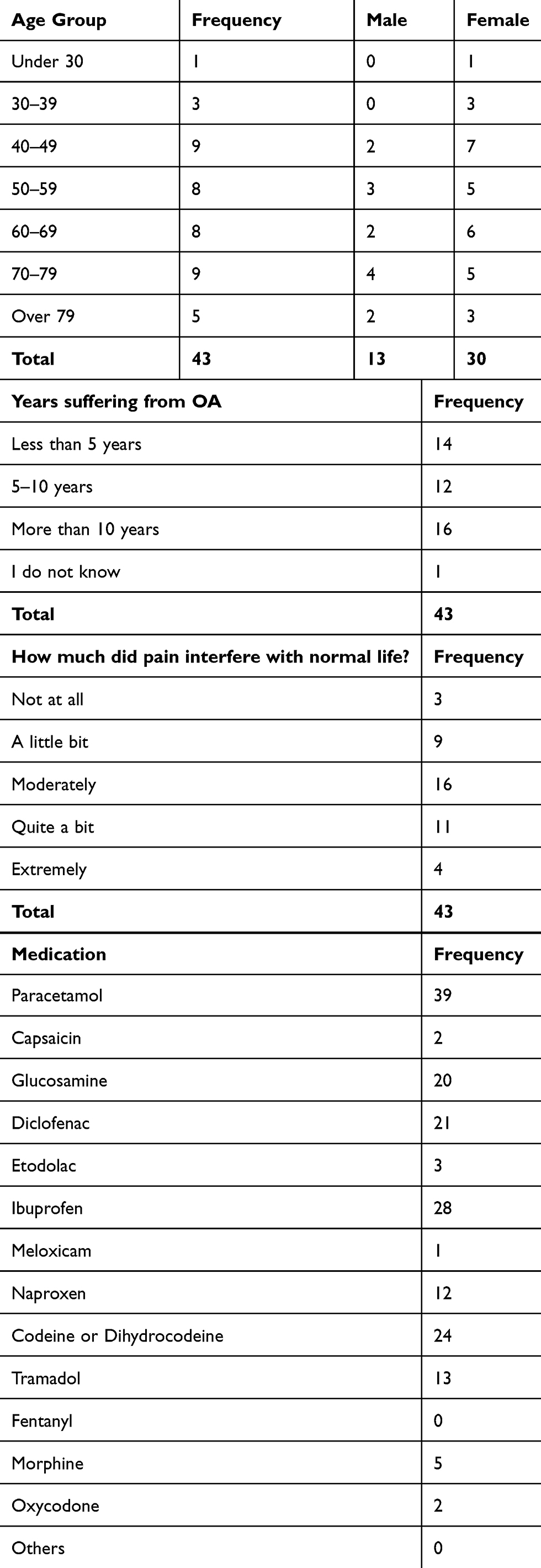 |
Table 3 Frequency of the Participants’ Age Groups, Gender, Years Suffering from OA, Pain Interfere with Normal Life, and Using Medications for OA Treatment |
The majority of participants (65.1%) had OA for over 5 years. About 93% of the participants reported that joint pain affected their normal life, 72.1% reported that effect to be moderate to extreme, and 7% reported that joint pain does not interfere with their normal life at all (Table 3).
The majority of patients (39 patients - 90.7%), reported using or have used paracetamol for the treatment of OA, while only two participants (4.7%) reported using Capsaicin. NSAIDs and COX-2 inhibitors were used by (83.7%), opioids were used by (67.4%), and glucosamine was used by (46.5%) for the management of OA (Table 3).
Patients Preferences
The Relative Importance of Attributes
The most important factor in selecting the non-invasive pharmaceutical treatment of OA was “risk of heart attacks and strokes”, which accounted for 19.5% of the relative importance of all attributes. The second most important factor was “risk of addiction”; 18.4% of the relative importance. Followed by “risk of kidney and liver side-effects”; 17.5% of the relative importance. The least important factor was “how much mobility improvement would you expect”; only 3.5% of the relative importance (Figure 4).
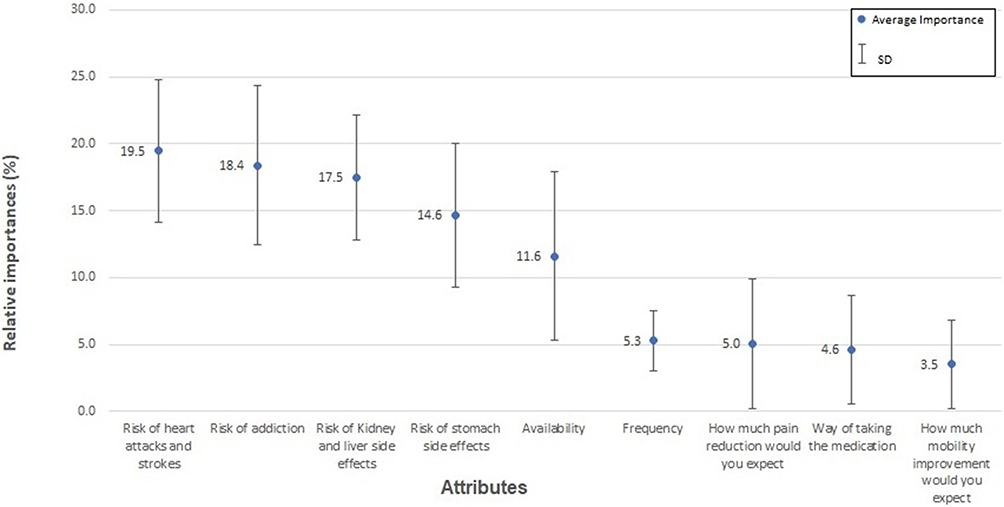 |
Figure 4 The average (relative) importance and Standard Deviation (SD) for all attributes. |
The combined relative importance of the four risk factors (kidney and liver, heart attacks and strokes, stomach, and addiction side effects) adds up to 70% (17.5% +19.5%+14.6% +18.4%) of the total relative importance that impact on patients’ decisions when selecting OA medication. The combined relative importance of both benefits attributes (pain reduction and mobility improvement) accounted only for 8.5% (5%+3.5%) of the total relative importance. The highest standard deviation between respondents in relation to relative importance was 6.3 for the “availability” attribute and the lowest was 2.2 for “frequency” attribute.
Utilities of Levels of Attributes
The most preferred medication scenario for participants would be prescribed medication that is taken orally, as needed, provides 75% pain reduction and 75% mobility improvement, and has no risk of any of the associated side effects.
The interval utility values in each attribute represent how likely the participants would be willing to change their mind to trade off a level against another level within the same attribute. For example, the utilities for the “no” and “low” risk levels in the four risk attributes are in the positive value and within close interval values of each other in comparison to other levels (“Moderate” and “high” risk) that are in the minuses value and within large interval values from the most preferred level. This means that participants are more likely to trade off the “no” and “low” risk levels against each other than they would trade them off against levels that are set at the other side of the scale. The risk of addiction utilities for “No” and “Low” risks are 67.3 and 37.4, and the “Moderate” and “High” risks are −6.4 and −98.2, respectively. Therefore, moving from “No” through “Low” and “Moderate” to “High” risk, would result in interval losses of 29.9, 43.8 and 91.8. This is showing that increasing risks of addiction are associated with increasing interval disutilities. On the other hand, the risk of liver and kidney side effects utilities for “No” and “Low” risks are 91.8 and 36.8, and the “Moderate” and “High” risks are −63.1 and −65.5, respectively. Therefore, moving from “No” through “Low” and “Moderate” to “High” risk, would result in interval losses of 55, 99.9 and 2.4. This indicates that regarding the risk of liver and kidney side effects, it is easier for patients to trade off “High” with “Moderate” risk (utility interval 2.4) than trading off “Low” risk with “Moderate” risk (utility interval 99.9) (Table 4).
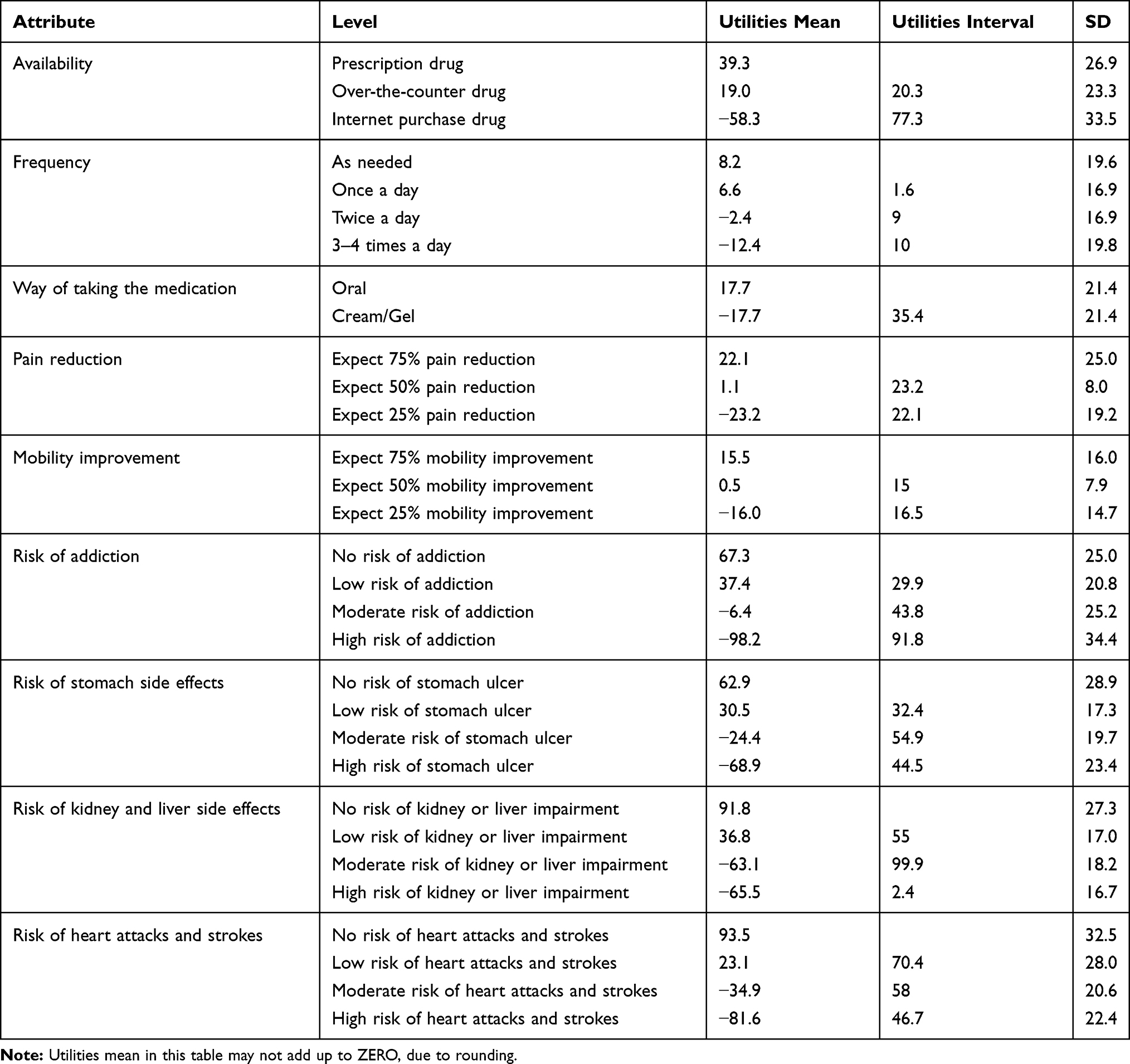 |
Table 4 The Utilities of All Levels |
Discussion
Summary
The results of our study indicate that OA patients are most keen to reduce the risk of side effects. For three of the attributes of the adverse event (risk of addiction, stomach side effects, and heart attacks and strokes), the utility loss increases as the risk increases from “no” to “low”, to “moderate” to “high”. In the case of the forth adverse events attribute (kidney and liver side effects), there is only a small difference between moderate and high risk of impairment. Across our sample, no reduction in pain or improvement would be acceptable if it involved anything other than “no” or “low” risk of side effects.
Beyond a relatively strong dislike internet purchases (an interval utility of 77 from an over the counter purchase compared to a 20.3 interval between prescribed drugs and over the counter drugs), the within attribute preferences also reveal important other information concerning patient preferences for OA: There is little difference between the optimal choice of taking medication as needed and once per day, but the disutility interval increases when the medication is required to be taken more than twice per day. This suggests OA patients, on average, most prefer medications that are taken most infrequently, that are over the counter and taken orally. However; on average across the participants, no changes in the frequency of medication would compensate for a move from oral to cream/gel and no means of taking or frequency would compensate a move to internet purchasing, although an over the counter oral medication would likely be preferred to a prescription cream or gel.
The results of our study are broadly consistent with previous research into the preferences for the pharmaceutical treatment of OA. Specifically, patients do make trade-offs between the benefits treatments might offer and the harms that may result from their use and it is the harms that drive patient decisions. However, our extensive value set consisting of nine attributes paints a richer picture of the factors that affect the medication choices that OA patients make. Consistent with previous studies, patient’s medication choices are not driven by the benefits a treatment might offer. Rather it is the risk of adverse side effects that most influences choices.1,8 Availability, frequency and how the medication is taken are more and as least as important as any gains in mobility or reductions in pain. Our findings reiterate the importance of providing appropriate risk/benefit information to patients making decisions about medication for their OA.11 They also show that any risk-benefit trade-offs should be considered alongside availability and modality.
Although financial attributes were excluded from our value set, patients preferred prescription medication over medications available without the need to see a doctor. This may be related to the age distribution of participants and the situation that, in the UK, prescriptions for the over 60 years of age are free.48 The age profile may also explain the dislike of online purchases of medication, as older people tend to be generally less perceptive to products offered by online shopping.49 Our results indicates that the lower frequency of medication and oral administration were preferred, although the strength of preferences was smaller than those associated with availability. Generally, this is consistence with the patients’ attitude toward medication preference in relation to route and frequency.50,51
Strengths and Limitations
By adopting a novel methodology for collecting patient preferences, our study addresses the limitations of previous studies (and of our previously based pilot study) in terms of the numbers of attributes of medication choices for OA patients using choice-based experiments. It is the most comprehensive study for pharmaceutical treatment for OA, including 9 attributes and a total of 31 levels.
Our study recruited 43 respondents; it is potentially underpowered and the generalisability to OA population might be limited in terms of treatment preferences. However, there is no consensus in relation to the sample size for conjoint studies. As statistical depends on many factors such as the distribution of preferences in the population of interest, the number of questions and scenarios included in the questionnaire.33 Additionally, ACBC has the ability to collect more information from a smaller sample, potentially reducing required sample sizes and the novelty and contribution that the ACBC method proposes such as the inclusion of a large number of attributes and levels and being a practical tool that can be used to elicit patients’ preferences compensate for the study limitation.
In terms of limitations, despite the adaptive nature of the process, ACBC interview generally takes longer than CBC to complete, the samples needed are smaller than standard CBC because more information is captured from each individual.52 However, smaller sample sizes may compensate for the additional time required to complete ACBC surveys and make these methods more useful in health service contexts where it might be difficult to recruit patient samples large enough to conduct conventional choice-based CA surveys.46
Conclusion
Patients preference for non-invasive pharmaceutical treatment for OA is predominantly driven by patients desire to avoid the risk of side effects. In our study, patients were not willing to accept any moderate to high risk of side effects, even when 50–75% improvement in movement or pain reduction was offered. Incorporating patients views into decisions about their care has obvious benefits, this study introduced ACBC as a practical tool that can be used to elicit patients’ preferences for non-invasive pharmaceutical treatment of OA. Further study is required to address the validity of the revealed preference in comparison to the stated preference and significance of ACBC to practitioners and shared decision-making.
Data Sharing Statement
The data for the research presented in the publication may be available from the corresponding author, on reasonable request.
Code availability: Sawtooth Software Incorporated (SSI) web version (8.2.4).
Ethics Approval
This project was approved by the Ethics Committee of the Faculty Health and Life Sciences at Northumbria University, and it was conducted in accordance with the Declaration of Helsinki. All procedures performed in this project involving human participants were in accordance with the ethical standards of the ethics committee of the faculty health and life sciences at Northumbria University, Newcastle Upon Tyne, UK.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Acknowledgments
The authors are grateful to all participants involved in this study and to Healthwatch – Newcastle Upon Tyne and Healthwatch – North East England for assisting in participants’ recruitments, as this research would not have been possible without their contribution. We are also grateful to Dr Joanne Gray and Dr Mujahed Shraim for providing feedback regarding the design and analysis of this study. We are grateful to the members of the Research Users’ Group part of the Patient and Public Involvement (PPI) group at the Arthritis Research UK Primary Care Centre, and to Carol Rhodes, Adele Higginbottom, Dr Peter Croft, Dr Martin Frisher, and Dr Julius Sim at Keele University, UK, for their contribution to the primary development of the pilot that led to this study.
Results dissemination to study participants: A copy of this article will be distributed to all participants involved, Healthwatch Newcastle-upon-Tyne and north-east of England, and the PPI group in the Arthritis Research UK Primary Care Centre at Keele University.
Patient and Public Involvement (PPI): PPI group contributed to the development and presentation of the attributes and levels included in this study. Then, tested the ACBC questionnaire for user-friendliness, contents, and clarity.
Funding
The research was supported by the school of health and life sciences at Northumbria University, Newcastle Upon Tyne, UK.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Hiligsmann M, Pinto D, Dennison E, et al. Patients’ preferences for osteoarthritis treatment: the value of stated-preference studies. Aging Clin Exp Res. 2019;31(1):1–3. doi:10.1007/s40520-018-1098-3
2. Brembo EA, Kapstad H, Eide T, Månsson L, Van Dulmen S, Eide H. Patient information and emotional needs across the hip osteoarthritis continuum: a qualitative study. BMC Health Serv Res. 2016;16(1):88. doi:10.1186/s12913-016-1342-5
3. Al-Omari B. The shared decision for osteoarthritis treatments. OPROJ. 2019;5(5). doi:10.31031/OPROJ.2019.05.000625
4. Onishi K, Utturkar A, Chang E, Panush R, Hata J, Perret-Karimi D. Osteoarthritis: a critical review. Crit Rev Phys Rehabil Med. 2012;24(3–4):251–264. doi:10.1615/CritRevPhysRehabilMed.2013007630
5. Angelis A, Kanavos P. Multiple Criteria Decision Analysis (MCDA) for evaluating new medicines in health technology assessment and beyond: the advance value framework. Soc Sci Med. 2017;188:137–156. doi:10.1016/j.socscimed.2017.06.024
6. Committee on Improving the Quality of Cancer Care: Addressing the Challenges of an Aging Population, Board on Health Care Services, Institute of Medicine. Delivering High-Quality Cancer Care: Charting a New Course for a System in Crisis. Levit L, Balogh E, Nass S, Ganz PA, eds. Washington (DC): National Academies Press (US); 2013. doi:10.17226/18359
7. Hauber AB, Arden NK, Mohamed AF, et al. A discrete-choice experiment of United Kingdom patients’ willingness to risk adverse events for improved function and pain control in osteoarthritis. Osteoarthr Cartil. 2013;21(2):289–297. doi:10.1016/j.joca.2012.11.007
8. Al-Omari B. Patient preferences for the pharmacological treatment of osteoarthritis using adaptive choice-based conjoint (ACBC) analysis: a pilot study. Eur J Pers Cent Healthc. 2017;5(2):220. doi:10.5750/ejpch.v5i2.1293
9. Fraenkel L, Suter L, Cunningham CE, Hawker G. Understanding preferences for disease-modifying drugs in osteoarthritis. Arthritis Care Res (Hoboken). 2014;66(8):1186–1192. doi:10.1002/acr.22280
10. Byun J-H, Kwon S-H, Lee J-E, Cheon J-E, Jang E-J, Lee E-K. Comparison of benefit-risk preferences of patients and physicians regarding cyclooxygenase-2 inhibitors using discrete choice experiments. Patient Prefer Adherence. 2016;10:641–650. doi:10.2147/PPA.S98228
11. Laba T-L, Brien J, Fransen M, Jan S. Patient preferences for adherence to treatment for osteoarthritis: the MEdication Decisions in Osteoarthritis Study (MEDOS). BMC Musculoskelet Disord. 2013;14(1):160. doi:10.1186/1471-2474-14-160
12. Ratcliffe J. Patients‘ preferences for characteristics associated with treatments for osteoarthritis. Rheumatology. 2003;43(3):337–345. doi:10.1093/rheumatology/keh038
13. Turk D, Boeri M, Abraham L, et al. Patient preferences for osteoarthritis pain and chronic low back pain treatments in the United States: a discrete-choice experiment. Osteoarthr Cartil. 2020;28(9):1202–1213. doi:10.1016/j.joca.2020.06.006
14. Fraenkel L, Bogardus ST, Concato J, Wittink DR. Treatment options in knee osteoarthritis: the patient’s perspective. Arch Intern Med. 2004;164(12):1299–1304. doi:10.1001/archinte.164.12.1299
15. Fraenkel L, Wittink DR, Concato J, Fried T. Informed choice and the widespread use of antiinflammatory drugs. Arthritis Rheum. 2004;51(2):210–214. doi:10.1002/art.20247
16. Fraenkel L, Wittink DR, Concato J, Fried T. Are preferences for cyclooxygenase-2 inhibitors influenced by the certainty effect? J Rheumatol. 2004;31(3):591–593.
17. Byrne MM, Souchek J, Richardson M, Suarez-Almazor M. Racial/ethnic differences in preferences for total knee replacement surgery. J Clin Epidemiol. 2006;59(10):1078–1086. doi:10.1016/j.jclinepi.2006.01.010
18. Mühlbacher AC, Junker U, Juhnke C, et al. Chronic pain patients’ treatment preferences: a discrete-choice experiment. Eur J Health Econ. 2015;16(6):613–628. doi:10.1007/s10198-014-0614-4
19. Soekhai V, Whichello C, Levitan B, et al. Methods for exploring and eliciting patient preferences in the medical product lifecycle: a literature review. Drug Discov Today. 2019;24(7):1324–1331. doi:10.1016/j.drudis.2019.05.001
20. Soekhai V, de Bekker-grob EW, Ellis AR, Vass CM. Discrete choice experiments in health economics: past, present and future. Pharmacoeconomics. 2019;37(2):201–226. doi:10.1007/s40273-018-0734-2
21. Clark MD, Determann D, Petrou S, Moro D, de Bekker-grob EW. Discrete choice experiments in health economics: a review of the literature. Pharmacoeconomics. 2013;14(1):883–902. doi:10.1186/1471-2474-14-160
22. Ryan M, Scott DA, Reeves C, et al. Eliciting public preferences for healthcare: a systematic review of techniques. Health Technol Assess. 2001;5(5):1–186. doi:10.3310/hta5050
23. Rao VR. Conjoint Analysis. In: Sheth J, Malhotra N, editors. Wiley International Encyclopedia of Marketing. Chichester, UK: John Wiley & Sons, Ltd; 2010. doi:10.1002/9781444316568.wiem02019.
24. Wong DW, Chan F, Da Silva Cardoso E, Lam CS, Miller SM. Rehabilitation counseling students’ attitudes toward people with disabilities in three social contexts. Rehabil Couns Bull. 2004;47(4):194–204. doi:10.1177/00343552040470040101
25. Lamiraud K, Geoffard P-Y. Therapeutic non-adherence: a rational behavior revealing patient preferences? Health Econ. 2007;16(11):1185–1204. doi:10.1002/hec.1214
26. Lancsar E, Louviere J. Conducting discrete choice experiments to inform healthcare decision making: a user’s guide. Pharmacoeconomics. 2008;26(8):661–677. doi:10.2165/00019053-200826080-00004
27. Ryan M, Gerard K. Using discrete choice experiments to value health care programmes: current practice and future research reflections. Appl Health Econ Health Policy. 2003;2(1):55–64.
28. Al-Omari B, Sim J, Croft P, Frisher M. Generating individual patient preferences for the treatment of osteoarthritis using Adaptive Choice-Based Conjoint (ACBC) analysis. Rheumatol Ther. 2017;4(1):167–182. doi:10.1007/s40744-017-0056-4
29. Louviere JJ, Hensher DA, Swait JD, Adamowicz W. Stated Choice Methods: Analysis and Applications. Cambridge: Cambridge University Press; 2000. doi:10.1017/CBO9780511753831
30. Reed Johnson F, Lancsar E, Marshall D, et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR conjoint analysis experimental design good research practices task force. Value Health. 2013;16(1):3–13. doi:10.1016/j.jval.2012.08.2223
31. Jaynes J, Wong W-K, Xu H. Using blocked fractional factorial designs to construct discrete choice experiments for healthcare studies. Stat Med. 2016;35(15):2543–2560. doi:10.1002/sim.6882
32. Jervis SM, Ennis JM, Drake MA. A comparison of adaptive choice-based conjoint and choice-based conjoint to determine key choice attributes of sour cream with limited sample size. J Sens Stud. 2012;27(6):451–462. doi:10.1111/joss.12009
33. ACBC technical paper; 2014. Available from: https://www.sawtoothsoftware.com/support/technical-papers/adaptive-cbc-papers/acbc-technical-paper-2009.
34. Fraenkel L, Fried T. If you want patients with knee Osteoarthritis (OA) to exercise: tell them about NSAIDS. Patient. 2008;1(1):21–26.
35. A new approach to adaptive CBC; 2007. Available from: https://sawtoothsoftware.com/resources/technical-papers/a-new-approach-to-adaptive-cbc.
36. Bridges JFP, Hauber AB, Marshall D, et al. Conjoint analysis applications in health–a checklist: a report of the ISPOR good research practices for conjoint analysis task force. Value Health. 2011;14(4):403–413. doi:10.1016/j.jval.2010.11.013
37. Al-Omari B, Sim J, Croft P, Frisher M. Patient preferences for the pharmacological treatment of osteoarthritis: a feasibility study using adaptive choice-based conjoint analysis (ACBCA). Eur J Pers Cent Healthc. 2015;3(2):253. doi:10.5750/ejpch.v3i2.975
38. About us - healthwatch newcastle. Available from: https://www.healthwatchnewcastle.org.uk/about-us/.
39. Health and social care act; 2012. Available from: https://www.legislation.gov.uk/ukpga/2012/7/contents/enacted.
40. Formulating attributes and levels in conjoint analysis; 2002. Available from: https://sawtoothsoftware.com/resources/technical-papers/formulating-attributes-and-levels-in-conjoint-analysis.
41. Overview | osteoarthritis: care and management | guidance | NICE. Available from: https://www.nice.org.uk/guidance/cg177.
42. Al-Omari B, Hill B. Nursing people with osteoarthritis. Br J Nurs. 2020;29(18):1060–1063. doi:10.12968/bjon.2020.29.18.1060
43. Lighthouse studio help. Available from: https://sawtoothsoftware.com/help/lighthouse-studio/manual/index.html?checklistpriortofielding.html.
44. Lenk PJ, DeSarbo WS, Green PE, Young MR. Hierarchical bayes conjoint analysis: recovery of partworth heterogeneity from reduced experimental designs. Marketing Sci. 1996;15(2):173–191. doi:10.1287/mksc.15.2.173
45. Orme BK. Getting Started with Conjoint Analysis: Strategies for Product Design and Pricing Research.
46. Cunningham CE, Deal K, Chen Y. Adaptive choice-based conjoint analysis: a new patient-centered approach to the assessment of health service preferences. Patient. 2010;3(4):257–273. doi:10.2165/11537870-000000000-00000
47. Steiner M, Meißner M. A user’s guide to the galaxy of conjoint analysis and compositional preference measurement. MAR. 2018;40(2):3–25. doi:10.15358/0344-1369-2018-2-3
48. NHS. Am I entitled to free prescriptions? Available from: https://www.nhs.uk/using-the-nhs/help-with-health-costs/get-help-with-prescription-costs/.
49. Kwon W, Noh M. The influence of prior experience and age on mature consumers’ perceptions and intentions of internet apparel shopping. J Fash Marketing Manage. 2010;14(3):335–349. doi:10.1108/13612021011061825
50. Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86(4):304–314. doi:10.4065/mcp.2010.0575
51. Zhang J, Xie Z, Zhang N, Zhong J. Chapter 13 - Nanosuspension drug delivery system: preparation, characterization, postproduction processing, dosage form, and application. In: Ecaterina Andronescu, Alexandru Mihai Grumezescu, editors. In Micro and Nano Technologies, Nanostructures for Drug Delivery. Elsevier. 2017:413–443. doi:10.1016/B978-0-323-46143-6.00013-0
52. Which conjoint method should I use? 2013. Available from: https://sawtoothsoftware.com/resources/technical-papers/which-conjoint-method-should-i-use.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.