")
Back to Journals » Patient Preference and Adherence » Volume 9
Patients’ acceptance of corticotomy-assisted orthodontics
Authors Zawawi K
Received 24 May 2015
Accepted for publication 11 July 2015
Published 12 August 2015 Volume 2015:9 Pages 1153—1158
DOI https://doi.org/10.2147/PPA.S89095
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Khalid H Zawawi
Department of Orthodontics, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia
Objective: To study patients’ acceptance of corticotomy-assisted orthodontics as a treatment option.
Methods: Adult patients seeking orthodontic treatment were asked to complete two sets of questionnaires; the first set included questions about age, sex, and level of education and general questions about orthodontic treatment; and the second set was related to the corticotomy-assisted orthodontics. Before answering the corticotomy questions, a brief description of the clinical procedure was explained and photographs of an actual procedure were shown.
Results: A total of 150 subjects were approached and 129 (86%) agreed to answer the questionnaires (72 male and 57 female patients). Of these, only 3.1% did hear about corticotomy and 7.8% selected corticotomy instead of extraction. Fear from the surgery (53.2%) was the most frequent reason for not selecting corticotomy followed by fear from pain (36.9%). The acceptance of corticotomy between males and females was similar. No relationship was found between the level of education and prior knowledge of the procedure, P=0.857. Prior knowledge about corticotomy was not a factor in selecting it as a treatment option (P=0.556) to reduce the treatment time (P=0.427).
Conclusion: The acceptance of corticotomy-assisted orthodontics as a treatment option was low. Fear from the surgery was the main reason for not selecting it. The acceptance of corticotomy-assisted orthodontics was not related to patient’s level of education or sex.
Keywords: orthodontic treatment, corticotomy-assisted orthodontics, patient acceptance, cross sectional survey, alveolar decortication
Introduction
In orthodontics, teeth are repositioned to create a more esthetic and/or functional dental complex. This dictates a series of decisions and procedures that, in turn, require some knowledge of the various disciplines intimately related to orthodontics. These include growth and development of the dentition and the face, tooth movement, and characterization of the form and pattern of the dentofacial complex.1 In cases where tooth-size and arch-length discrepancy is large (moderate to severely crowding), orthodontic treatment necessitates moving the teeth into new positions.2,3 For this purpose, space is required. This space can be gained either by extraction of teeth or by expansion of the arches.4–6
Nowadays, the individual’s appearance, particularly the dental appearance, is considered an essential feature when determining the facial attractiveness and hence plays a requisite role in human social interactions.7–10 It has been shown in a recent report that there was a relationship between dental malocclusion and the psychosocial well-being and self-esteem.11 Furthermore, in recent years, there is an increase in the number of adult patients who are seeking orthodontic treatment, and thus a reduction in orthodontic therapy time is considered to be an important objective.12–15
Adult orthodontic treatment is different and challenging, as it demands special concepts and procedures.16,17 The introduction of corticotomy-assisted orthodontic treatment that paved the way for treating adult cases is different from conventional orthodontic treatment methods and provided a solution to many limitations in adult orthodontic treatment by delivering rapid tooth movement and also avoiding extractions.12,18–22
However, corticotomy-assisted orthodontics is an invasive surgical procedure that requires the elevation of buccal and often a lingual/palatal flap for decortication of alveolar bones followed by bone augmentation.21 This extensive physical injury causes the initiation of transitory demineralization process and increases regional bone turnover leading to the regional accelerated phenomenon.12,19
One might anticipate that because of a decrease in the treatment time, adult patients may be more interested in orthodontic treatment. However, it could be argued that the surgical phase may in fact prevent patients from considering corticotomy-assisted orthodontics as a treatment option. This, however, has not been extensively studied.
So far, utilization of corticotomy-assisted orthodontics is considerably low in Saudi Arabia. This could be because the technique involves significant postoperative injury and periodontal risks, is time-consuming, and is often seen as highly invasive.15
Thus far, no previous study investigated patients’ perception and/or acceptance of this procedure. Therefore, this study was aimed to assess patients’ acceptance of corticotomy-assisted orthodontics and to evaluate whether they prefer this procedure rather than extraction for orthodontic purposes.
Materials and methods
This study was conducted at the Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia. The study was reviewed and approved by the Research Ethics Committee at the Faculty of Dentistry, King Abdulaziz University, and informed consent was obtained. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Adult patients seeking orthodontic treatment were asked to complete two sets of questionnaires; the first set included questions about age, sex, and level of education, and general questions about orthodontic treatment; and the second set of questions was related to the corticotomy-assisted orthodontics. Prior to answering the corticotomy questions, a brief description of the clinical procedure of corticotomy-assisted orthodontics was described and photographs of an actual procedure were shown. Participation was voluntary, all questionnaires were anonymous, and no personal information was collected. Inclusion criteria were as follows: dental patients who were 21 years or older, with no history of orthodontic treatment, with no craniofacial deformity, and not medically handicapped.
Statistical analysis
Frequency distributions were calculated and tabulated for each answer in the questionnaires and the number of subjects responding to each question. Comparison of data between variables was performed using the chi-square tests and the Fisher’s exact tests for nominal data and the independent Student’s t-test for continuous data. The level of statistical significance was considered at P<0.05. Statistical analysis was performed using the Statistical Package for Social Sciences (released 2011, IBM SPSS Statistics for Mac, Version 20.0, IBM Corporation, Armonk, NY, USA).
Results
A total of 150 subjects were approached and 86% (129 subjects) agreed to answer the questionnaires comprising 72 males and 57 females. The mean age among males was 37.4 (±12.8) years and among females was 34.2 (±9.4) years with no significant difference between them, P=0.09.
Most of the subjects had a college degree (63%) as shown in Table 1. Only 3% of the subjects did know about corticotomy-assisted orthodontics before their current dental visit. Only ~8% of the respondents choose corticotomy-assisted orthodontics rather than extraction. But this percentage increased to 50% if the corticotomy was the only available option. Approximately 32% of the sample chose corticotomy in order to reduce the treatment time.
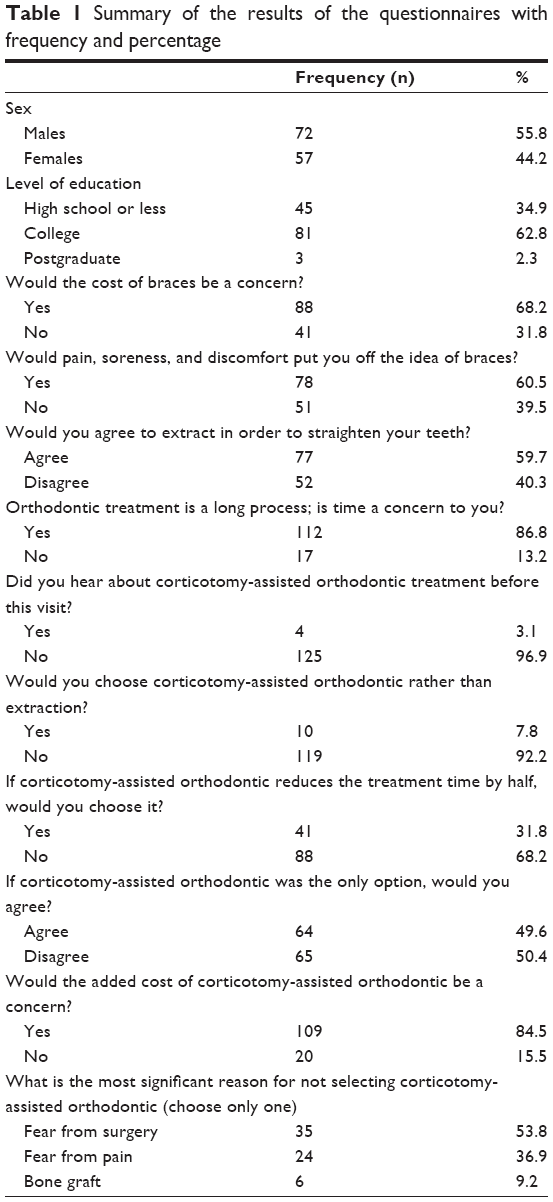 | Table 1 Summary of the results of the questionnaires with frequency and percentage |
Fear from the surgery (53.2%) was the most frequent reason for not choosing corticotomy-assisted orthodontics, followed by fear from pain (36.9%).
The chi-square and the Fisher’s exact analyses showed that the responses for male and female patients were similar (Table 2). Moreover, no significant relationships were found between the level of education and knowledge about the procedure, P=0.857.
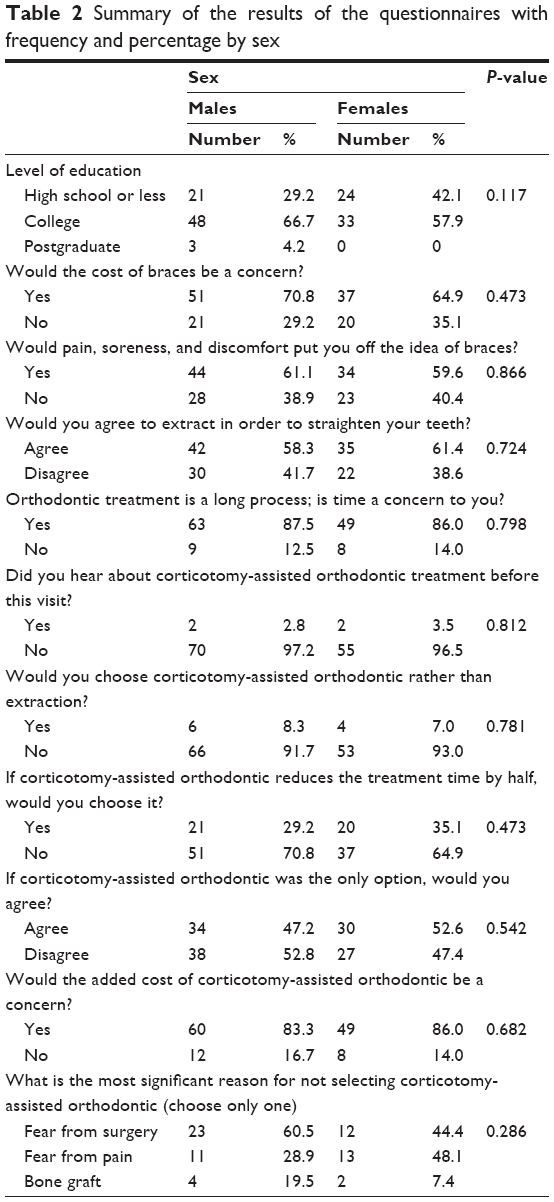 | Table 2 Summary of the results of the questionnaires with frequency and percentage by sex |
Table 3 shows that prior knowledge about corticotomy was not a factor in selecting it as a treatment option even if it was the only treatment option or to reduce the treatment time.
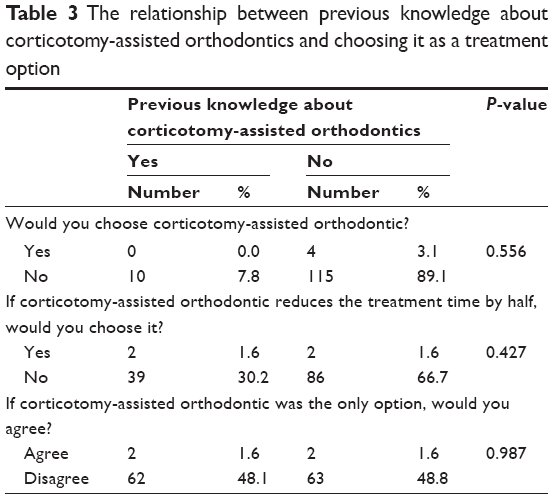 | Table 3 The relationship between previous knowledge about corticotomy-assisted orthodontics and choosing it as a treatment option |
Discussion
In modern society, there is an increased demand to reduce the orthodontic treatment time, particularly in adult patients. Hence, corticotomy-assisted orthodontics has gained considerable attention and is being reported more frequently in recent publications.12,18–21 Corticotomy-assisted orthodontics has the ability to provide faster treatment time and possibly avoid the extraction protocol, since the debate to extract or not to extract to relief dental arch crowding still exists.23–25
The corticotomy technique is generally performed under local anesthesia. After raising a full thickness flap, decortication of the buccal cortical bone is initiated using a round bur, and if required, the palatal/lingual cortical bone as well. Vertical grooves are then made in the interdental spaces and connected with a horizontal scalloped corticotomy cuts around the apices of the teeth. Bone graft is then applied and the flap is repositioned and sutured. Orthodontic activation is initiated 2 weeks after the surgery to take advantage of the regional accelerated phenomenon effect. Activation of orthodontic appliances is then performed every 2 weeks until the end of treatment.18–21,26,27
Corticotomy-assisted orthodontics is thought to provide an increase in the net alveolar bone volume after orthodontic treatment due to the combination of selective decortication and alveolar augmentation. Therefore, teeth can then be moved almost 25%–30% faster compared to traditional orthodontic treatment. This technique is used to treat moderate-to-severe malocclusions and the need for extractions is reduced.28
There is an increase in the number of both case reports and animal studies, in the last 15 years, showing that corticotomy-assisted orthodontics is becoming a popular surgical procedure.18–20,29–31 Nonetheless, this extensive surgery could discourage some patients from accepting it.
It is well known that orthodontic treatment requires significant patient compliance32,33 and that patient compliance is significantly influenced by experiences such as pain. Orthodontic patients often experience pain during treatment.34 Moreover, treatment efficacy and the level to which patients are capable or prepared to accept the proposed treatment steps should be addressed.35 Therefore, orthodontic therapy may fail if it concentrates only on occlusion and function while overlooking the patient’s perceptions.
Thus far, there are no published reports that have investigated patients’ acceptance and expectations from corticotomy-assisted orthodontic treatment and no reports about the pain experienced in corticotomy patients. However, one study evaluated the effect of corticotomy on maxillary canine retraction compared with the conventional technique.36 The results demonstrated that alveolar corticotomy decreased the canine retraction time; however, a moderate degree of pain and discomfort was reported.
There are several orthodontic techniques and devices that can facilitate tooth movement, such as skeletal anchorage devices.37–39 Even though this technique was shown to be acceptable by patients and does not produce pain and discomfort,40 treatment duration does not appear to be decreased.41
This study investigated the acceptance of corticotomy-assisted orthodontics by adults seeking orthodontic treatment. The results showed only 7.8% selected corticotomy-assisted orthodontics rather than extraction. This could be because only 3.1% had prior knowledge of this procedure. Another possible reason is that the associated morbidity may deter patients from selecting this procedure as most of the participants listed fear and pain as the main reasons for not selecting corticotomy.
Corticotomy-assisted orthodontics is considered less invasive; however, some adverse effects to the periodontium have been reported in addition to swelling and pain postoperatively.13,42 That is why modification of this technique has been an on going challenge to reduce the surgical field and time.14,15,43
Currently, there are no reports that investigated patients’ experience with corticotomy-assisted orthodontics. Therefore, further studies that assess the postoperative pain with corticotomy in comparison with traditional orthodontic activation are needed.
It should be noted that an important limitation of the present study is the absence of an adolescent group seeking orthodontic treatment. Another limitation is the sample size. However, the current findings identified the low acceptance of corticotomy-assisted orthodontics among adult patients seeking orthodontic treatment.
In conclusion and based on the results of this study, the acceptance of corticotomy-assisted orthodontics as a treatment option is low. Fear from the surgery was listed as the main reason for not choosing this treatment option. The acceptance of corticotomy-assisted orthodontics was not related to patient’s level of education or sex.
Acknowledgment
The author would like to express his sincere appreciation to Professor Mohammad S Al-Zahrani for his valuable suggestions and advice throughout this study.
Disclosure
The author reports no conflicts of interest in this work.
References
Proffit WR, Fields HW, Sarver DM. Contemporary Orthodontics. 5th ed. St Louis, MO: Mosby Elsevier; 2012. | ||
Kim E, Gianelly AA. Extraction vs nonextraction: arch widths and smile esthetics. Angle Orthod. 2003;73(4):354–358. | ||
Gianelly A. Evidence-based therapy: an orthodontic dilemma. Am J Orthod Dentofacial Orthop. 2006;129(5):596–598; discussion 98. | ||
Konstantonis D, Anthopoulou C, Makou M. Extraction decision and identification of treatment predictors in Class I malocclusions. Prog Orthod. 2013;14:47. | ||
Isik F, Sayinsu K, Nalbantgil D, Arun T. A comparative study of dental arch widths: extraction and non-extraction treatment. Eur J Orthod. 2005;27(6):585–589. | ||
Rinchuse DJ, Kandasamy S. Implications of the inclination of the mandibular first molars in the extractionist versus expansionist debate. World J Orthod. 2008;9(4):383–390. | ||
Newton JT, Prabhu N, Robinson PG. The impact of dental appearance on the appraisal of personal characteristics. Int J Prosthodont. 2003;16(4):429–434. | ||
York J, Holtzman J. Facial attractiveness and the aged. Spec Care Dentist. 1999;19(2):84–88. | ||
Zawawi KH, Malki GA, Al-Zahrani MS, Alkhiary YM. Effect of lip position and gingival display on smile and esthetics as perceived by college students with different educational backgrounds. Clin Cosmet Investig Dent. 2013:577–580. | ||
Richards MR, Fields HW Jr, Beck FM, et al. Contribution of malocclusion and female facial attractiveness to smile esthetics evaluated by eye tracking. Am J Orthod Dentofacial Orthop. 2015;147(4): 472–482. | ||
Perillo L, Esposito M, Caprioglio A, Attanasio S, Santini AC, Carotenuto M. Orthodontic treatment need for adolescents in the Campania region: the malocclusion impact on self-concept. Patient Prefer Adherence. 2014:8353–8359. | ||
Amit G, Jps K, Pankaj B, Suchinder S, Parul B. Periodontally accelerated osteogenic orthodontics (PAOO) – a review. J Clin Exp Dent. 2012;4(5):e292–e296. | ||
Cano J, Campo J, Bonilla E, Colmenero C. Corticotomy-assisted orthodontics. J Clin Exp Dent. 2012;4(1):e54–e59. | ||
Dibart S, Sebaoun JD, Surmenian J. Piezocision: a minimally invasive, periodontally accelerated orthodontic tooth movement procedure. Compend Contin Educ Dent. 2009;30(6):342–344,346,348–350. | ||
Hernandez-Alfaro F, Guijarro-Martinez R. Endoscopically assisted tunnel approach for minimally invasive corticotomies: a preliminary report. J Periodontol. 2012;83(5):574–580. | ||
Gkantidis N, Christou P, Topouzelis N. The orthodontic-periodontic interrelationship in integrated treatment challenges: a systematic review. J Oral Rehabil. 2010;37(5):377–390. | ||
Roblee RD, Bolding SL, Landers JM. Surgically facilitated orthodontic therapy: a new tool for optimal interdisciplinary results. Compend Contin Educ Dent. 2009;30(5):264–275; quiz 76,78. | ||
Aljhani AS, Zawawi KH. Nonextraction treatment of severe crowding with the aid of corticotomy-assisted orthodontics. Case Rep Dent. 2012;2012:694527. | ||
Wilcko MT, Wilcko WM, Pulver JJ, Bissada NF, Bouquot JE. Accelerated osteogenic orthodontics technique: a 1-stage surgically facilitated rapid orthodontic technique with alveolar augmentation. J Oral Maxillofac Surg. 2009;67(10):2149–2159. | ||
Wilcko W, Wilcko MT. Accelerating tooth movement: the case for corticotomy-induced orthodontics. Am J Orthod Dentofacial Orthop. 2013;144(1):4–12. | ||
Murphy KG, Wilcko MT, Wilcko WM, Ferguson DJ. Periodontal accelerated osteogenic orthodontics: a description of the surgical technique. J Oral Maxillofac Surg. 2009;67(10):2160–2166. | ||
Wilcko WM, Ferguson DJ, Bouquot JE, Wilcko T. Rapid orthodontic decrowding with alveolar augmentation: case report. World J Orthod. 2003;4(3):197–205. | ||
Filho HL, Maia LH, Lau TC, de Souza MM, Maia LC. Early vs late orthodontic treatment of tooth crowding by first premolar extraction: a systematic review. Angle Orthod. 2015;85(3):510–517. | ||
Konstantonis D. The impact of extraction vs nonextraction treatment on soft tissue changes in Class I borderline malocclusions. Angle Orthod. 2012;82(2):209–217. | ||
Kumari M, Fida M. Vertical facial and dental arch dimensional changes in extraction vs non-extraction orthodontic treatment. J Coll Physicians Surg Pak. 2010;20(1):17–21. | ||
Lee JK, Chung KR, Baek SH. Treatment outcomes of orthodontic treatment, corticotomy-assisted orthodontic treatment, and anterior segmental osteotomy for bimaxillary dentoalveolar protrusion. Plast Reconstr Surg. 2007;120(4):1027–1036. | ||
Shoreibah EA, Salama AE, Attia MS, Abu-Seida SM. Corticotomy-facilitated orthodontics in adults using a further modified technique. J Int Acad Periodontol. 2012;14(4):97–104. | ||
Wilcko T, Wilcko WM, Bissada NF. An evidence-based analysis of periodontally accelerated orthodontic and osteogenic techniques: a synthesis of scientific perspectives. Semin Orthod. 2008;14(4):305–316. | ||
Baloul SS, Gerstenfeld LC, Morgan EF, Carvalho RS, Van Dyke TE, Kantarci A. Mechanism of action and morphologic changes in the alveolar bone in response to selective alveolar decortication-facilitated tooth movement. Am J Orthod Dentofacial Orthop. 2011;139(4 Suppl):S83–S101. | ||
Sebaoun JD, Kantarci A, Turner JW, Carvalho RS, Van Dyke TE, Ferguson DJ. Modeling of trabecular bone and lamina dura following selective alveolar decortication in rats. J Periodontol. 2008;79(9):1679–1688. | ||
Sanjideh PA, Rossouw PE, Campbell PM, Opperman LA, Buschang PH. Tooth movements in foxhounds after one or two alveolar corticotomies. Eur J Orthod. 2010;32(1):106–113. | ||
Bos A, Vosselman N, Hoogstraten J, Prahl-Andersen B. Patient compliance: a determinant of patient satisfaction? Angle Orthod. 2005;75(4):526–531. | ||
Bos A, Hoogstraten J, Prahl-Andersen B. Towards a comprehensive model for the study of compliance in orthodontics. Eur J Orthod. 2005;27(3):296–301. | ||
Erdinc AM, Dincer B. Perception of pain during orthodontic treatment with fixed appliances. Eur J Orthod. 2004;26(1):79–85. | ||
Feldmann I. Orthodontic anchorage: evidence-based evaluation of anchorage capacity and patients’ perceptions. Swed Dent J Suppl. 2007(191):10–86. | ||
Al-Naoum F, Hajeer MY, Al-Jundi A. Does alveolar corticotomy accelerate orthodontic tooth movement when retracting upper canines? a split-mouth design randomized controlled trial. J Oral Maxillofac Surg. 2014;72(10):1880–1889. | ||
Kyung SH, Lee JY, Shin JW, Hong C, Dietz V, Gianelly AA. Distalization of the entire maxillary arch in an adult. Am J Orthod Dentofacial Orthop. 2009;135(4 Suppl):S123–S132. | ||
Maino BG, Gianelly AA, Bednar J, Mura P, Maino G. MGBM system: new protocol for Class II non extraction treatment without cooperation. Prog Orthod. 2007;8(1):130–143. | ||
Al-Fraidi AA, Zawawi KH. Clinical showcase. Selective intrusion of overerupted upper first molars using a temporary anchorage device: case report. J Can Dent Assoc. 2010;76a9. | ||
Zawawi KH. Acceptance of orthodontic miniscrews as temporary anchorage devices. Patient Prefer Adherence. 2014:8933–8937. | ||
Lee J, Miyazawa K, Tabuchi M, Sato T, Kawaguchi M, Goto S. Effectiveness of en-masse retraction using midpalatal miniscrews and a modified transpalatal arch: treatment duration and dentoskeletal changes. Korean J Orthod. 2014;44(2):88–95. | ||
Hassan AH, Al-Fraidi AA, Al-Saeed SH. Corticotomy-assisted orthodontic treatment: review. Open Dent J. 2010:4159–4164. | ||
Cassetta M, Di Carlo S, Giansanti M, Pompa V, Pompa G, Barbato E. The impact of osteotomy technique for corticotomy-assisted orthodontic treatment (CAOT) on oral health-related quality of life. Eur Rev Med Pharmacol Sci. 2012;16(12):1735–1740. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.