")
Back to Journals » Patient Preference and Adherence » Volume 15
Patients’ Perception of the Impact of Innovation on Hemophilia Care Management Organization: A Qualitative Study Protocol (INNOVHEMO Study)
Authors Beny K , du Sartz de Vigneulles B, Chamouard V , Guilloux R, Gay V , Negrier C, Dussart C
Received 31 May 2021
Accepted for publication 21 July 2021
Published 18 August 2021 Volume 2021:15 Pages 1807—1815
DOI https://doi.org/10.2147/PPA.S322531
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Karen Beny,1,2 Benjamin du Sartz de Vigneulles,1 Valerie Chamouard,3,4 Ronald Guilloux,5 Valérie Gay,6 Claude Negrier,3 Claude Dussart1,2
1EA 4129 Laboratory P2S (Health Systemic Process), University of Lyon, University Claude Bernard Lyon 1, Lyon, France; 2Central Pharmacy, Hospices Civils de Lyon, Lyon, France; 3Reference center on hemophilia and other constitutional hemorrhagic diseases, Groupement Hospitalier Est, Hospices Civils de Lyon, Lyon, France; 4Pharmacy, Groupement Hospitalier Est, Hospices Civils de Lyon, Lyon, France; 5Laboratory S2HEP, University of Lyon, University Claude Bernard Lyon 1, Lyon, France; 6Hemophilia Care Center, Centre hospitalier Métropole Savoie, Chambéry, France
Correspondence: Karen Beny
Central Pharmacy, Hospices Civils de Lyon, 57 rue Francisque Darcieux, CS 60004, 69563 Saint Genis Laval Cedex, Lyon, France
Tel +33 4 78 86 66 92
Fax +33 4 72 67 88 74
Email [email protected]
Background: New therapies provide a favorable evolution in the care management of persons with hemophilia. However, the impact of these new therapies on patient care organization remains to be determined. A qualitative study will be implemented to analyze patients’ perception regarding the impact of innovation on the organization of their care management. Secondary objectives will include refining specific factors related to persons with hemophilia (barriers or facilitators, especially the place of treatment) to consider within an organizational impact analysis.
Patients and Methods: Semi-structured individual interviews will be conducted via videoconferencing or by phone by two researchers using an interview guide. Participants will be recruited from the Rhône-Alpes region, in France. Physicians from two hemophilia treatment centers will identify eligible patients. Moreover, a call for volunteers will be launched by the Rhône-Alpes committee of the French hemophilia association. Interviews will be conducted with adult patients, adolescent patients or parents of a minor with hemophilia regularly treated prophylactically or on demand. Data analysis will be performed with NVivo® software. Each interview will be analyzed by two researchers using an inductive content analytic method.
Discussion: The INNOVHEMO study is an original study analyzing the way patients perceive the impact of an innovation on their care management organization. The resulting patient-specific factors, identified as barriers or facilitators, will need to be integrated into a more comprehensive analysis of the impact of innovation on care management organization.
Keywords: therapeutic innovation, hemophilia, care pathway, qualitative research, organizational aspect, patient experience data
Introduction
Hemophilia is a rare chronic genetic disorder due to deficient or absent coagulation factors (factor VIII in hemophilia A and factor IX in hemophilia B). It leads to spontaneous or traumatic bleeding; its main complication is hemophilic arthropathy. The worldwide incidence of hemophilia is one boy per 5000 male births for hemophilia A and one boy per 30,000 male births for hemophilia B.1 In the past decades, the organization of hemophilia care has greatly evolved. One reason was the development of replacement therapies for the treatment and prophylaxis of hemorrhages; another was the structuring of specific care networks to optimize the management of this rare, severe and chronic disease.
In the seventies, the development of whole blood fractionation and emergence of the first clotting factor concentrates (CFCs), promoted care pathway advances with a shift from exclusive hospital-based care to the possibility of home-based treatment administration.2–4 The contaminated blood products, in the eighties, made hemophilia care management more complex with a disastrous impact on the quality of life of persons with hemophilia (PWH). Afterwards, improved blood product safety and the development of recombinant CFCs helped promote the dissemination of prophylactic treatments.5,6 All these advances contributed to an increased life expectancy in PWH, and transformed the disease into a chronic condition. However, CFCs are not curative and should be administered several times per week via infusion. One CFC-related complication is the development of inhibitors. The management of patients with inhibitors is more burdensome (increased CFC dosage, treatment with by-passing agents (less effective, shorter half-life, longer infusion duration), implementation of immune tolerance induction protocol).7,8 Acute pain (eg infusion-related), chronic pain (joint pain), treatment burden (eg reconstitution problems, venous access difficulties, infusion rejection in children) impairs quality of life for PWH and their caregivers. As such, quality of life improvements in PWH and caregivers represents a real challenge.9–15
In parallel, specific care networks have become more organized over the years. On an international level, the world federation of hemophilia (WFH), created in 1963, has developed actions to promote optimal hemophilia care around the world.16 Since the creation of the first specialized care center for persons with hemophilia in the United Kingdom in the late forties, hemophilia comprehensive care centers have been developed all around the world.17,18 In France, regional centers for the treatment of hemophilia (CRTH) were created in the late eighties. Since 2005, national plans have been implemented to improve the care management of persons with rare diseases. This led to the labeling of a reference center on hemophilia and other constitutional hemorrhagic diseases (CRH) in 2006. Rare diseases networks were also set up to reinforce coordinated actions, such as the French network on inherited bleeding disorders (MHEMO). Specialized treatment centers are disseminated over the entire French territory (CRH, Constitutional Hemorrhagic Diseases Resource and Competencies Center (CRC-MHC) and Center for Hemophilia Care (CTH)). This contributed to a structured care pathway for PWH to improve their care management. Nowadays, hemophilia care management is articulated within this dedicated network encompassing various structures and different healthcare professionals, for the specific care management of the disease and its associated disorders (osteoarticular complications, infectious conditions). PWH are very involved in their care management (self-treatment). Expert patients and parents during therapeutic education training courses, French Hemophilia Association (AFH), school-based physicians, companies providing at-home care services are also implicated. The patient care pathway is punctuated with transition landmarks (childhood, adolescence, adult) and ruptures (city-hospital). This French care pathway is very hospital-centered. CRH, CRC-MHC and CTH are structures integrated within public hospitals. Patients regularly go to the hospital for their follow-up consultations. The early care management, right from childhood, associated with regular follow-up visits result in a very strong link between patients and specialist healthcare teams. The dispensing of CFCs by hospital pharmacies strengthens this closeness with the hospital. However, the accessibility of CFCs needs to be improve, especially in an emergency context.19 Therefore, in France, the evolution of the drug distribution system represents a real challenge for patient care.
Today, new therapies are or will be implemented to improve hemophilia care. They represent new therapeutic approaches via 1) extending the circulating half-life of CFCs to reduce infusion frequency, 2) non-substitutive mechanisms of actions (mimicking Factor VIII function, acting on other pathways of hemostasis), 3) subcutaneous administration mode, and 4) gene correction.20–23 Some therapies are already available (extended half-life CFCs, bispecific monoclonal antibody restoring the hemostatic activity) and promoted quality of life improvements in PWH.24–27
In addition to this favorable evolution in hemophilia care, several changes are to be expected. First, in patients’ care pathway. Indeed, a reduction in treatment-related constraints and clinical improvements could drive patients away from specialized structures and involve new actors in the management of these patients. Furthermore, in France, to improve this care pathway, some new therapeutics could be available in community pharmacies, closer to patients. This will lead to a shift from hospital-center care pathway to outpatient care pathway. In light of scarce data on long-term adverse events and efficacy, management of emergencies and surgeries with a high hemorrhagic risk, and the biological monitoring of these new therapeutics, a sustainable follow-up in expert centers remains essential for quality care.28–31 Thus, the use of these new therapies must be properly secured and coordinated while training all new actors involved.
Second, an evolution of patient care organization is to be expected (new therapeutics protocols, new formation programs, variation in frequency of consultation). In a complex healthcare system, the clinical and medical-economic evaluations of healthcare innovations, essential to their marketing and financing, are no longer sufficient. The financing and evaluation of healthcare innovations represent a major Public Health issue. Since many therapeutic innovations will become available, studying the organizational impact of these new therapies could bring additional elements and facilitate healthcare decisions.32
Consequently, the impact of innovation on care pathway and on care organization needs to be clearly identified and analyzed. This makes it possible to study how to improve the care pathway and the experience of care for PWH while maintaining a high level of safety. Given that patients are at the heart of the care pathway, it is essential to consider their point of view on changes at these different levels (individual and institutional).
Patients and Methods
Objectives
The main objective of this study is to analyze patient perceptions regarding the impact of innovation on the organization of their care management.
Secondary objectives are:
- Analyzing the place of treatment in this care organization.
- Highlighting specific factors related to patients with hemophilia (barriers or facilitators), which should be taken into account when analyzing the impact of innovation on the organization of care management.
Type of Study
Several parameters are involved in the patient care pathway: patient characteristics, access to care, characteristic of the disease, and patient environment. Since sociological or cognitive factors can influence the care pathway,33 we aimed to implement a qualitative study, best suited to collecting participants’ experiences and perceptions on the organization of their care management.
Semi-structured individual interviews will be conducted by two researchers, one woman and one man, both trained in the qualitative study methodology. KB is a hospital pharmacist working on her PhD, BdSdV graduated in Public Health and Political Sciences and is an associate researcher in a university research lab. The interview-based analytic method is geared to explore disease-related behaviors, attitudes and experiences.34 It is designed to analyze patients’ perception on the impact innovation could have on the organization of their care management.35 This method is indeed the best suited to guarantee the feasibility of this study. Hemophilia being a rare condition, patients sometimes reside far away from their care setting and it can be difficult to organize group meetings, whereas one-on-one interviews are more adapted to the patients’ constraints. Even though face-to-face interviews are more effective, these will be conducted remotely to limit risks related to today’s COVID-19 pandemic context.
Inclusion Criteria
The objective is to collect patients’ perspectives on innovations at large but also on therapeutic innovations, since most future innovations in hemophilia will be therapeutic drugs. Thus, interviewed participants must be regularly treated for their hemophilia, in prophylaxis, or on demand.
In order to explore the greatest patient diversity, the cohort must include patients with associated comorbid conditions, patients with inhibitors, patients who participated in a clinical study, patients who experienced a change in treatment, patients who had issues with treatment adherence, and patients of all ages. This is an essential point, since the perception of the care pathway can vary according to one’s experience.
Consequently, inclusion criteria are:
- Adult patient (>18 years) or adolescent patient (12–18 years) with congenital hemophilia A or B with on-demand or prophylactic anti-hemophilic treatment (factor VIII, factor IX, prothrombin complex concentrate, activated factor VII, bispecific monoclonal antibodies),
- Adult parent caregiver (>18 years) involved in the therapeutic management of a child (<18 years) with congenital hemophilia A or B with on-demand or prophylactic anti-hemophilic treatment (factor VIII, factor IX, prothrombin complex concentrate, activated factor VII, bispecific monoclonal antibodies).
- Patient or caregiver with prior experience in hemophilia care
Exclusion Criteria
Exclusion criteria: patients or parents without a regular specific anti-hemophilic treatment (on demand or prophylactic), patients coming for a first consultation, patients under the age of 12, as well as persons having difficulties with the French language.
Recruitment and Sample Size
To ensure effective recruitment, with the required number of participants to meet the above listed criteria, participants will be recruited within one unique territory, the Rhône-Alpes, where the care pathway network is similar, ensuring homogenous data collection.
Participants will be recruited from a call for volunteers through the Rhône-Alpes committee of the French hemophilia association (AFH). Eligible participants will also be identified by physicians from two hemophilia treatment centers: Lyon and Chambery.
The Lyon center is the hemophilia national reference center on hemophilia with the higher number of patients for the region. The Chambery center is characterized by its history. In the sixties, a boarding school for patients with hemophilia opened in a nearby town called St Alban Leysse, attracting a population of patients with hemophilia to the region. It is one of the region’s largest centers.
A first contact by phone will be followed by sending out an information letter and consent form.
We must include a sufficient number of patients to explore the greatest patient diversity. An initial sample is estimated at 15 participants per center, ie a total of 30 persons interviewed. Reaching representativeness of this population is not the objective. The topics for which a saturation need to be reached have not been previously identified. In this exploratory study, the collection of multiple perceptions will be prioritized. The final sample size could be adapted if the diversification of patient characteristics is not sufficient to yield enough exploitable data.
Description of the Interviews
The interviews will preferably be conducted by videoconferencing, to collect non-verbal visual communication elements (posture, voice, facial expression, gestures), when impossible it will be done by phone adapting to the agenda of the patient or parent.
The two researchers, KB and BdSdV, using an interview guide, will conduct semi-structured individual interviews. Each interview will be conducted one-on-one by one of the two researchers (according to their schedule). Each time the researcher deems it necessary he or she can prompt participants, reformulate an answer or even do a synthesis during the interview.36,37 These interviews will be recorded on a voice recorder. If possible, additional elements, especially non-verbal attitudes, could be noted on paper.
The interview guide is structured gradually to bring participants to progressively change dimensions. The 1st part of the guide is designed to collect patients’ perceptions on their care pathway and the impact of their ongoing treatment on care organization. The second part of this guide focuses on the notion of innovation with first the notion of change in general followed by the care organization.
To cover these different notions, the interview guide elaboration were based on: 1) different observations previously collected from healthcare professionals, during visits to the hemophilia treatment centers (actors identified, coordination, involvement of the different actors, identification of rupture points); 2) national hemophilia management and diagnostic protocol (PNDS);38 and 3) a review of the literature that identified qualitative studies on patients with cancer or asthma and their care pathway perceptions.39,40 A qualitative analysis, conducted on patients with hemophilia and caregivers, explored patients’ knowledge and perceptions regarding their treatment. This analysis contributed to the interview guide framework.14
The guide starts by presenting the research and detailing the objective of the interview as well as reminding the patient of the study’s confidentiality and anonymity parameters. Then it contains one introductory question which is followed by transition questions and examples of rephrasing and prompting (Table 1).
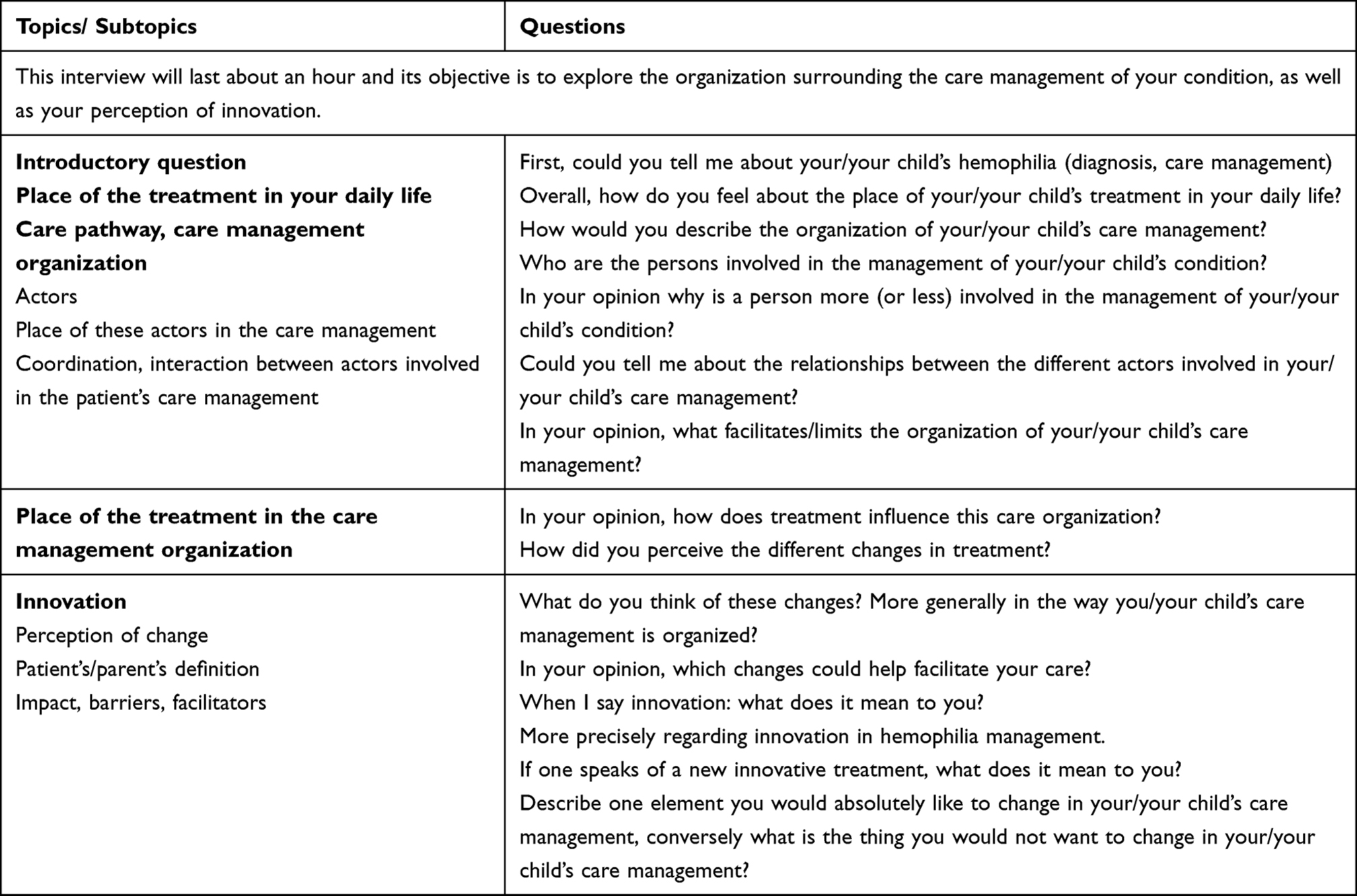 |
Table 1 Interview Guide Used to Conduct Semi-Structured Individual Interview |
Sociodemographic, disease and treatment characteristics are collected at the end of the interview. Since these data could influence one’s care pathway and perception of innovation, they are needed for the study analysis.
Beforehand, the interview guide will be tested on two participants per center: these four test participants will be part of the initial sample if the guide does not undergo major modifications.
Data Analysis and Validity
There will be verbatim transcriptions of the interviews, following the exact course of the interview and mentioning all communication elements, including non-verbal cues, to fully comprehend the interactions (laughs, hesitations, attitudes). Interviews will be transcribed by a company specialized in verbatim transcriptions.
Data collection and analysis will be done simultaneously. After the interview, each researcher will proceed with a thorough reading of each verbatim transcription. The NVivo® software is used for data analysis. Each interview will be analyzed by two researchers using an inductive content analytic method41–44 following the steps described in Figure 1. A confrontation of results will be done after coding to reach a consensus. In case of divergent analysis, a third researcher opinion will be required. After reaching a consensus on the identified categories and themes, occurrences will be measured to weigh the results.
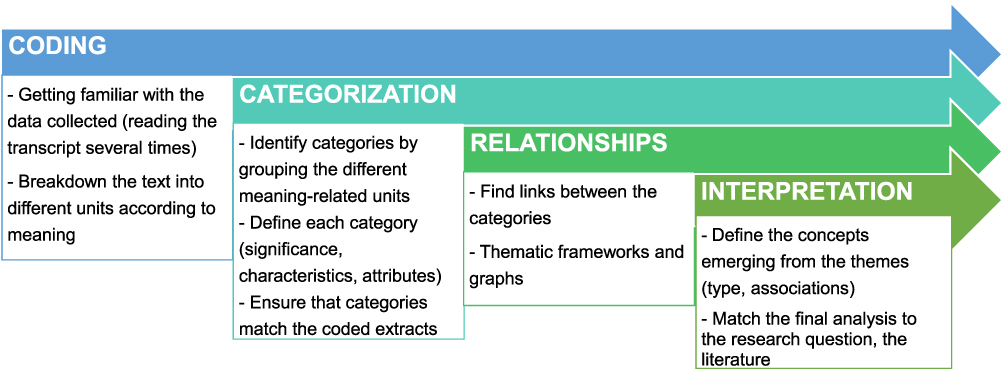 |
Figure 1 Steps from the inductive content analysis method. |
At the end of the analysis, we plan to conduct 2 or 3 additional interviews with study participants to present the emerging concepts and discuss their coherence to corroborate our results.
Ethics
Anonymity is mandatory. This point is underlined at the beginning of the interview and in the information letter distributed to eligible PWH or caregivers. Participants are invited to read this letter and a signed consent form is collected before the beginning of the interviews. The participant is free to terminate the interview at any time. Email exchanges with the transcription company are digitally secured. The downloadable files (recording and transcriptions) are protected with passwords sent via a separate channel.
This study will be conducted in accordance with the Declaration of Helsinki. This study was declared at the French national data protection agency CNIL on March 4, 2021. The Ethics Committee of the Lyon University Hospital reviewed this research project and approved the study on April 18, 2021.
Discussion
To our knowledge, this is the first study evaluating the perception of the impact of innovation on the organization of hemophilia care from a patient’s perspective. Several qualitative studies were conducted to integrate the patient’s perspective into the decision-making process for using innovative therapies. These studies highlighted acceptability criteria involved in shared decision making, such as treatment ease of use, efficacy on bleeds, safety and impact on daily life.45,46 Another study underlined the importance for patients to communicate with a clinical team from an expert center in hemophilia to implement a new patient-centered care approach.47 This confirms the relevance to explore patient perceptions regarding the impact of new therapies on care organization. This approach could help identify risks of rupture in the patient care pathway and be useful to patients, caregivers and healthcare teams along with new actors involved in the care pathway. It could also facilitate the decision-making process when there are different therapeutic options by including an organizational dimension. In this chronic condition, where patients become actors or even partners of their care management, it is essential to collect their perspectives.
In this study, we will focus on patients’ perception of innovation at large, then medical innovations followed by therapeutic drug innovations. In fact, future innovations in hemophilia management will be therapeutic ones. In the past, new therapies led to organizational and medical innovations.48 One can expect similar consequences in the upcoming years. Evolutions of the care pathway could lead to the implementation of innovative tools (ie to improve care coordination with expert centers) or innovative organizations (ie to develop the competencies of new actors in the management of this rare condition). It seems important not limit the analysis to therapeutic innovations.
The relevance of an interview-based qualitative analysis methodology lies in collecting a large amount of data while giving participants the opportunity to share their perspectives and feelings.36 It can improve our understanding of participants’ behaviors and motivations. Proposing two interview modalities (videoconference or phone) can lead to a data collection bias. It will be impossible to collect non-verbal cues if the interview is conducted by phone. The analysis is mainly centered on speech content analysis. Non-verbal communication cues are added elements in this study, knowing that they remain limited via video-conferencing in comparison with in person interview. However, it will be essential to take this element into account when interpreting the results.
There are biases with this type of study such as interviewer’s characteristics (gender, experience, academic rank), relationships between the interviewer and study participant, which could influence data collection.49 Having two different interviewers could limit biases related to the individual’s characteristics. Using an interview guide and testing it beforehand is necessary to limit data collection dispersion. One of the difficulties in this study is collecting the perception of the person interviewed in the right dimension. In fact, our objective is to determine the perception of the impact on the care organization. It is important to avoid generating some confusion during the interview between the impact of innovation on the patient’s life vs on the patient’s care pathway. The order of topics was determined to drive the participant through the various topics from 1) the place of treatment in his/her daily life, 2) perception of the care organization, 3) place of treatment in this organization, 4) perception of innovation, and finally 5) perception of innovation on this care organization. The implementation of a qualitative study via semi-structured interviews is a good method to describe the care pathway and care organization. Hannane et al, described the care pathway of asthmatic patients, by conducting interviews on 30 patients.40 This analysis described the perception of patients on actors of their care management and their involvement. This highlighted the perception of a faulty communication and coordination in care management.
The INNOVHEMO study can propose a method for increasing the accountability of patient perception in organizational impact studies. This preliminary exploratory study is also designed to test the adequation of our study method. The objective was not to extrapolate the results. However, method reproducibility will enable to replicate this analysis in other regions or even other countries where the issue of innovation-related organizational impact is relevant. The resulting patient-specific factors, identified as barriers or facilitators, will need to be integrated into a more comprehensive analysis of the impact of innovation on care management organization.
Abbreviations
CFCs, clotting factor concentrates; CRC-MHC, constitutional hemorrhagic diseases resource and competencies center; CRH, reference center on hemophilia and other constitutional hemorrhagic diseases; CTH, center for hemophilia care; HIV, human immunodeficiency virus; PWH, persons with hemophilia.
Acknowledgments
We acknowledge the Rhône-Alpes committee of the French Hemophilia Association for the support of our work. We would like to thank Mrs Bénédicte Clément for her help in manuscript preparation.
Disclosure
Mr Benjamin du Sartz de Vigneulles reports being an employee until march 2019, Oncology Department for Pierre Fabre Laboratories. The authors report no other conflicts or competing interests in this work.
References
1. Mannucci PM, Tuddenham EGD. The hemophilias — from royal genes to gene therapy. N Engl J Med. 2001;344(23):1773–1779. doi:10.1056/NEJM200106073442307
2. Peyvandi F, Garagiola I, Young G. The past and future of haemophilia: diagnosis, treatments, and its complications. Lancet. 2016;388(10040):187–197. doi:10.1016/S0140-6736(15)01123-X
3. Franchini M, Mannucci PM. Past, present and future of hemophilia: a narrative review. Orphanet J Rare Dis. 2012;7(1):24. doi:10.1186/1750-1172-7-24
4. Rosendaal FR, Smit C, Briët E. Hemophilia treatment in historical perspective: a review of medical and social developments. Ann Hematol. 1991;62(1):5–15. doi:10.1007/BF01714977
5. Berntorp E. Haemophilia treatment in 2030. Haemophilia. 2016;22(Suppl 5):15–19. doi:10.1111/hae.13025
6. Key NS, Negrier C. Coagulation factor concentrates: past, present, and future. Lancet. 2007;370(9585):439–448. doi:10.1016/S0140-6736(07)61199-4
7. DiMichele D. Inhibitor development in haemophilia B: an orphan disease in need of attention. Br J Haematol. 2007;138(3):305–315. doi:10.1111/j.1365-2141.2007.06657.x
8. Hay CRM, Brown S, Collins PW, Keeling DM, Liesner R. The diagnosis and management of factor VIII and IX inhibitors: a guideline from the United Kingdom haemophilia centre doctors organisation. Br J Haematol. 2006;133(6):591–605. doi:10.1111/j.1365-2141.2006.06087.x
9. Westesson LM, Sparud‐Lundin C, Baghaei F, et al. Burden on parents of children with haemophilia: the impact of sociodemographic and child’s medical condition. J Clin Nurs. 2019;28(21‑22):4077–4086. doi:10.1111/jocn.15003
10. Lorenzato CS, Santos RB, Fagundes GZZ, Ozelo MC. Haemophilia Experiences, Results and Opportunities (HERO study) in Brazil: assessment of the psychosocial effects of haemophilia in patients and caregivers. Haemophilia. 2019;25(4):640–650. doi:10.1111/hae.13774
11. Witkop M, Wang M, Hernandez G, Recht M, Baumann K, Cooper DL. Impact of haemophilia on patients with mild-to-moderate disease: results from the P-FiQ and B-HERO-S studies. Haemophilia. 2021;27(Suppl 1):8–16. doi:10.1111/hae.14251
12. Witkop M, Neff A, Buckner TW, et al. Self-reported prevalence, description and management of pain in adults with haemophilia: methods, demographics and results from the Pain, Functional Impairment, and Quality of life (P-FiQ) study. Haemophilia. 2017;23(4):556–565. doi:10.1111/hae.13214
13. Osooli M, Steen Carlsson K, Baghaei F, et al. The association between health utility and joint status among people with severe haemophilia A: findings from the KAPPA register. Haemophilia. 2017;23(3):e180–e187. doi:10.1111/hae.13231
14. Novais T, Duclos A, Varin R, Lopez I, Chamouard V. Treatment-related knowledge and skills of patients with haemophilia and their informal caregivers. Int J Clin Pharm. 2016;38(1):61–69. doi:10.1007/s11096-015-0207-z
15. Mahlangu J, Oldenburg J, Callaghan MU, et al. Health-related quality of life and health status in persons with haemophilia A with inhibitors: a prospective, multicentre, non-interventional study (NIS). Haemophilia. 2019;25(3):382–391. doi:10.1111/hae.13731
16. Skinner MW, Myles E. World Federation of Hemophilia: 50 years of advancing treatment for all. Haemophilia. 2013;19(4):475–480. doi:10.1111/hae.12200
17. Page D. Comprehensive care for hemophilia and other inherited bleeding disorders. Transfus Apher Sci. 2019;58(5):565–568. doi:10.1016/j.transci.2019.08.005
18. Hoots K. Comprehensive care for hemophilia and related inherited bleeding disorders: why it matters. Curr Hematol Rep. 2003;(2):395–401. Available from: https://www.researchgate.net/publication/10603031_Comprehensive_care_for_hemophilia_and_related_inherited_bleeding_disorders_Why_it_matters .
19. Leroy V, Freyssenge J, Renard F, Tazarourte K, Négrier C, Chamouard V. Access to treatment among persons with hemophilia: a spatial analysis assessment in the Rhone-Alpes region, France. J Am Pharm Assoc. 2019;59(6):797–803. doi:10.1016/j.japh.2019.07.006
20. Croteau SE, Wang M, Wheeler AP. 2021 clinical trials update: innovations in hemophilia therapy. Am J Hematol. 2021;96(1):128–144. doi:10.1002/ajh.26018
21. Mancuso ME, Mahlangu JN, Pipe SW. The changing treatment landscape in haemophilia: from standard half-life clotting factor concentrates to gene editing. Lancet. 2021;397(10274):630–640. doi:10.1016/S0140-6736(20)32722-7
22. Spadarells G, Di Minno A, Milan G, et al. Paradigm shift for the treatment of hereditary haemophilia: towards precision medicine. Blood Rev. 2020;39(39):100618. doi:10.1016/j.blre.2019.100618
23. Butterfield JSS, Hege KM, Herzog RW, Kaczmarek R. A molecular revolution in the treatment of hemophilia. Mol Ther. 2020;28(4):
24. Khair K, Pollard D, Harrison C, Hook S, O’Driscoll M, Holland M. HOw patients view extended half-life products: impressions from real-world experience (The HOPE study). Haemophilia. 2019;25(5):814–820. doi:10.1111/hae.13803
25. Wells JR, Gater A, Marshall C, Tritton T, Vashi P, Kessabi S. Exploring the impact of infusion frequency in hemophilia a: exit interviews with patients participating in BAY 94-9027 extension studies (PROTECT VIII). Patient. 2019;12(6):
26. Mühlbacher AC, Sadler A, Lamprecht B, Juhnke C. Patient preferences in the treatment of hemophilia a: a best-worst scaling case 3 analysis. Value Health. 2020;23(7):862–869. doi:10.1016/j.jval.2020.02.013
27. Kempton C, Trask P, Parnes A, et al. Development and testing of the satisfaction questionnaire with intravenous or subcutaneous hemophilia injection and results from the Phase 3 HAVEN 3 study of emicizumab prophylaxis in persons with haemophilia A without FVIII inhibitors. Haemophilia. 2021;27(2):221–228. doi:10.1111/hae.14222
28. Hart DP, Kessler CM, Aledort L. Re-personalization and stratification of hemophilia care in an evolving treatment landscape. Hematology. 2019;24(1):737–741. doi:10.1080/16078454.2019.1687798
29. Trinchero A, Sholzberg M, Matino D. The evolution of hemophilia care: clinical and laboratory advances, opportunities, and challenges. Hamostaseologie. 2020;40(3):311–321. doi:10.1055/a-1175-6530
30. Mahlangu J, Cerquiera M, Srivastava A. Emerging therapies for haemophilia - Global perspective. Haemophilia. 2018;24(Suppl 6):15–21. doi:10.1111/hae.13510
31. Spadarella G, Di Minno A, Brunetti-Pierri N, Mahlangu J, Di Minno G. The evolving landscape of gene therapy for congenital haemophilia: an unprecedented, problematic but promising opportunity for worldwide clinical studies. Blood Rev. 2021;46:100737. doi:10.1016/j.blre.2020.100737
32. Lvovschi VE, Maignan M, Tazarourte K, et al. Multiple criteria decision analysis approach to consider therapeutic innovations in the emergency department: the methoxyflurane organizational impact in acute trauma pain. PLoS One. 2020;15(4):e0231571. doi:10.1371/journal.pone.0231571
33. Berger M, Séchet R. Accessibilité et parcours de soins des hémophiles: analyses à partir du cas de la Bretagne [Accessibility and care pathways for hemophiliacs: analyzes based on the case of Bretagne, France]. Cah Geogr Que. 2011;55(156):511–527. French.
34. Desanti R, Cardon P. Initiation À L’enquête Sociologique [Initiation to the Sociological Survey].
35. Huston P, Rowan M. Qualitative studies. Their role in medical research. Can Fam Physician. 1998;(44):2453–2458.
36. Bréchon P. Enquêtes Qualitatives, Enquêtes Quantitatives [Qualitative Surveys, Quantitative Surveys].
37. Blanchet A, Gotman A. L’enquête Et Ses Méthodes: L’entretien [The Survey and Its Methods: The Interview].
38. Haute Autorité de Santé. Protocole national de diagnostic et de soins Hémophilie [national hemophilia management and diagnostic protocol]. Lyon: Reference Center on Hemophilia and other constitutional hemorrhagic diseases, French network on inherited bleeding disorders MHEMO; 2019. Available from: https://www.has-sante.fr/jcms/c_483032/fr/hemophilie.
39. Mirat W. Suivi INterprofessionnel des PATients atteints de cancer (Etude SINPATIC): une étude exploratoire auprès de patients [INTER-professional follow-up of PATIents with cancer (SINPATIC study): an exploratory study on patients] [doctoral dissertation]. Creteil: University of Paris Est; 2018. French.
40. Hannane A, Misane L, Devouassoux G, Colin C, Letrilliart L. Asthma patients’ perception on their care pathway: a qualitative study. NPJ Prim Care Respir Med. 2019;29(1):1–8. doi:10.1038/s41533-019-0121-2
41. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
42. Pope C, Ziebland S, Mays N. Qualitative research in helth care. Analysing qualitative data. BMJ. 2000;320(7227):114–116. doi:10.1136/bmj.320.7227.114
43. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
44. Thomas DR. A general inductive approach for analyzing qualitative evaluation data. Am J Eval. 2006;27(2):237–246. doi:10.1177/1098214005283748
45. van Overbeeke E, Michelsen S, Hauber B, et al. Patient perspectives regarding gene therapy in haemophilia: interviews from the PAVING study. Haemophilia. 2020;27(1):129–136. doi:10.1111/hae.14190
46. van Balen EC, Wesselo ML, Baker BL, et al. Patient perspectives on novel treatments in haemophilia: a qualitative study. Patient. 2020;13(2):201–210. doi:10.1007/s40271-019-00395-6
47. van Balen EC, Krawczyk M, Gue D, et al. Patient-centred care in haemophilia: patient perspectives on visualization and participation in decision-making. Haemophilia. 2019;25(6):
48. Carricaburu D. Innovation thérapeutique et acceptabilité du risque iatrogène: l’introduction des produits antihémophiliques concentrés dans les années soixante-dix [Therapeutic innovation and acceptability of iatrogenic risk: the introduction of concentrated antihemophilic products in the 1970s]. Sci Soc Sante. 1999;17(4):
49. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.