")
Back to Journals » Patient Preference and Adherence » Volume 13
Patients, health professionals, and the health system: influencers on patients’ participation in ward rounds
Authors Walton V, Hogden A , Long JC , Johnson JK , Greenfield D
Received 3 April 2019
Accepted for publication 13 July 2019
Published 22 August 2019 Volume 2019:13 Pages 1415—1429
DOI https://doi.org/10.2147/PPA.S211073
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Victoria Walton,1 Anne Hogden,1 Janet C Long,2 Julie K Johnson,3 David Greenfield1
1Tasmanian School of Business and Economics, Australian Institute of Health Service Management, University of Tasmania, Sydney, Australia; 2Faculty of Medicine and Health Sciences, Australian Institute of Health Innovation, Macquarie University, Sydney, Australia; 3Department of Surgery, Center for Healthcare Studies, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA
Correspondence: Victoria Walton
Australian Institute of Health Service Management, University of Tasmania, Locked Bag 5052, Alexandria, NSW, 2015, Sydney, Australia
Tel +61 24 0841 7814
Email [email protected]
Background: The ward round is an opportunity to plan and deliver patient-centered care. Benefits include an effective and safer clinician-patient relationship, patient empowerment, reduced anxiety and increased trust in the health care system. Factors contributing to patient involvement in ward rounds is shaped by their preferences, ability, and opportunity.
Aim: To investigate ward rounds and the patient experience with them, the relationship between the patient and clinicians, and how rounds facilitate collaboration between them.
Patients and methods: A multimethod study was conducted in a single Australian facility in acute medicine and rehabilitation specialties. An observational study of ward rounds in each setting was conducted with 14 patients, aged between 55 and 89 years followed by semi-structured interviews conducted with the patients observed. Descriptive and thematic analysis was undertaken.
Results: One third of participants had not heard of the term ward round or could describe their purpose. Three main influencers on the patient experience of rounds were: self; the health system; and medical officers. No meaningful difference was found between patients in acute medicine and rehabilitation although all wanted to receive information from the senior medical officers. Patients more familiar with the health system were more active participants and took greater responsibility for their involvement in rounds and described higher satisfaction.
Conclusion: There is a level of acceptance within the health system that patients understand what a ward round is. However, their role on the round is complex and this may only be developed through experiencing them. High system users teach themselves to navigate rounding processes to ensure their needs are met. To ensure equity in participation patients should be educated on ward rounds, what to expect and how to they can participate.
Keywords: ward rounds, patient participation, interview, education
Introduction
The inpatient ward round is a primary activity for clinicians and patients to assess, interact and negotiate care treatment and goals.1 When doing so, the ward round has also been a traditional means to educate medical officers.2 The ward round is an opportunity to plan for and deliver patient- centered care, through working collaboratively to review and implement care plans.3 Benefits include an effective and safer clinician-patient relationship, patient empowerment, reduced anxiety and increased trust in the health care system.2,4 Factors contributing to patient involvement in ward rounds is shaped by their preferences, capacity, and opportunity.1
Studies have shown that patients desire participation; however issues of health literacy, belief in the medical hierarchy and a submissive patient role were factors contributing to patients not actively participating.5,6 In some cases younger patients may participate, but no relationship between age, or gender, and participation has been established.7 Illness severity can also affect a patient’s capacity and desire to take part in decision making during rounds.7 The inclusion of patients can depend on the type of rounding process being undertaken and whether the patient may, or may not, be nominated as a participant.2 The location8 and timing1 of the round were also found to be external influences affecting patient participation.
Communication was more likely to be longer, interactive and patient-centered in a single room opposed to a more traditional four-bedded hospital room.1,8 Participation can be enhanced by clinicians asking patients direct questions and using language free of medical terminology.1,7
Moreover, patients have been contributing self-reflections about the challenges of ward rounds. Sweet and Wilson6 provide reflections from patients over many decades. They reported the experience of being treated impersonally, as a disease rather than a person, and a feeling of exclusion from relevant conversations concerning them.6 If patient-centered care is to be effectively realized, improvement in clinician-patient collaboration and decision making in ward rounds, leading to a positive patient experience, must be achieved. For patients to take part in a ward round, both patients and clinicians must understand their own and each other’s roles, and the relationship between the two.
Aim
This study examined ward rounds in four wards of a metropolitan hospital, focusing on the patient experience and how they facilitated collaboration with health professionals. We asked three questions: first, what is the patient experience of the ward; second, what is the relationship between the health care team and patient during the ward rounds; and third, how do ward rounds facilitate collaboration between patients and health professionals?
Methods
Setting
The study was carried out in a 165-bed teaching hospital in metropolitan Sydney, Australia. The hospital provided adult medical, critical care, surgical and rehabilitation specialties. The specialties chosen for the study setting were acute medicine and rehabilitation. Acute medicine included patients from two wards. The first specialized in cardiology and general medicine, while the second was a short stay medical assessment unit. Two rehabilitation wards were included. The first specialized in aged care assessment and rehabilitation, and the second specialized in orthopedics, mobility, stroke, and needs assessment. These specialties were chosen as they provided contrasting care provisions: patients from acute medicine had higher acuity needs but shorter lengths of stay; while patients in rehabilitation had lower acuity, but longer lengths of stay.
Study design, study tools and data collection, participants and data analysis
Study design
We conducted a multi-methods study over a five-month period from March to August 2017 to include observations and semi-structured interviews in each setting.10 Ward round observations were used to facilitate patient interviews and provide context for their analysis.
Study tools and data collection
A paper-based ward round observation tool (Table S1) and semi-structured interview guide (Table S2) were designed specifically for the study. They were simultaneously developed based on the literature2 and the research team’s industry experience. In this study ‘participants’ refers to the patients interviewed and not the clinicians observed during the ward rounds. All observations and interviews were conducted by VW (PhD candidate). Interview times ranged between 7 and 23 mins. This did not include the time spent explaining the study or confirming consent documentation.
The observation tool included three categories. The first category observed the health professionals who attended, and if they introduced themselves and their role to the patient. Additionally, specific tasks that each health professional carried out during the round were noted. The second category observed the topics discussed during the round. The health professionals who took part in the conversation were noted, if they involved the patient, and how this occurred. The tool allowed for multiple topic discussions to be observed. The third category was specifically aimed at how the patient participated in the round. This allowed for a summary of what the patient asked during the round and the discussion topics they initiated.
The interview guide included six question topics: participant demographic characteristics; description of a ward round and its purpose; identification of attendees and roles; advantages and disadvantages of the ward round process; health professional and patient collaboration; and additional comments including how the process could be improved. Interviews were digitally audio-recorded, and written notes were taken during the interview to note participants’ non-verbal responses. When asked about specific roles such as allied health professionals, the examples of physiotherapist, occupational therapist, social worker were provided as they are the more common allied health professionals in the study setting.
During the observation, the researcher stayed inside the room if a single bedroom, or if it was a multibed room, inside the curtains that were pulled around the bed space. Patients were interviewed following their individual ward round review. This ensured their immediate perceptions were captured, and that patient follow-up was not lost if they were subsequently transferred off the ward for investigations. If the patient was in a multibed room with other patients being reviewed by the same care team, the researcher waited until the team had left the room to conduct the interview. Patients were offered the opportunity to be interviewed at their bedside or in a private area. When a participant required prompting to elicit more information, the researcher used round observations and previous responses to questions to encourage further explanation.
Participants
Convenience sampling was used to invite patients in medical and rehabilitation wards.11 Participation was voluntary. Nursing Unit Managers (NUMs) and medical officers identified patients that were suitable to participate based on the inclusion and exclusion criteria. Ward patients were eligible if they: had no identified cognitive impairment; were English-speaking; and had a medically stable health status. Surgical or post-operative patients, except those receiving rehabilitation on the rehabilitation wards, were excluded. A member of the research team (VW) approached the patients prior to the ward round, explained the study, and obtained written consent to both observe their ward round with their care team and be interviewed afterwards. Patients were assured anonymity and that responses would remain confidential. The relevant Head of Department gave approval to conduct the research, and verbal consent was obtained from clinicians involved in each round before proceeding.
Recruitment ceased after 14 interviews as data saturation was reached,12 with participants reporting similar responses from that point. Interestingly, this number is similar to the patient sample reported by Swenne and Skytt (2014) in their study on this topic.1
Data analysis
Multi-method analysis9 was undertaken to integrate and understand the observational and interview data collected during ward round observations and interviews. We used descriptive analysis from the ward round observations to support interview analysis. These included counting the number of times different interactions and events occurred, as well as participant demographics. Thematic analysis of the transcripts identified patterns and developed relationships to help understand issues and topics spoken about by participants.13,14 The Schwandt, Lincoln and Guba15 framework for analysis was used as a guide.
Interviews were listened to in their entirety, and observational notes reviewed prior to transcription.14 Patient interviews were transcribed verbatim and annotated with the interviewer’s notes including observational data collected during the round (VW). This allowed for richer understanding and interpretation of the interviews, as emphasis and non-verbal communication were witnessed.16 Following transcription, the interview was listened to again to ensure accuracy. Manual coding was used as it allowed a parallel process of conceptualizing while developing themes within the data.14 Interview questions were used to provide structure to the coding.13 Common words and phrases were first identified by the researcher who conducted the analysis (VW). The concepts were reviewed within the research team to ensure there was a common understanding of the theme. A second member of the research team analyzed and crossed checked a quarter of the material for consistency and reliability (JL) (Figure 1). A third member (AH) moderated any disagreement between coding. Interpretation and implications of themes were discussed by the research team.
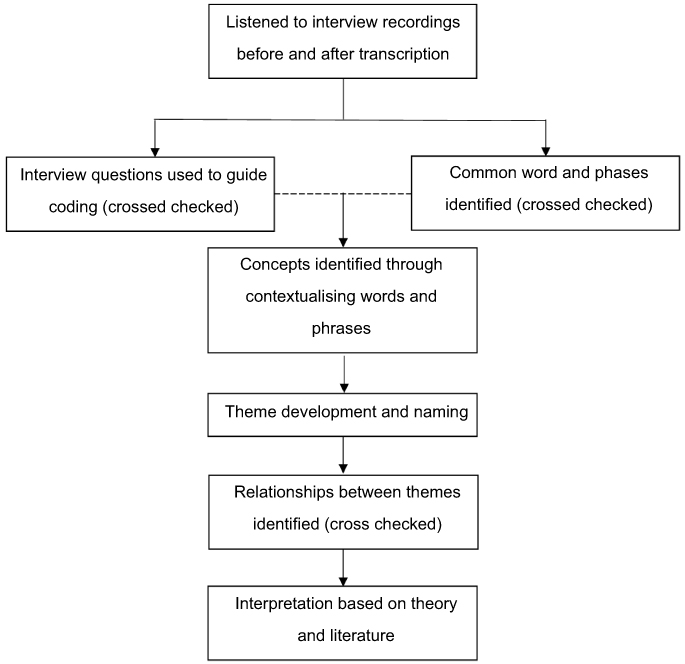 |
Figure 1 Data analysis process for patient interviews. |
Ethics
Ethics approval for the study was granted by a local health district research ethics committee (approval: LNR/13/HAWKE/365) and Macquarie University ( 5201600910).
Results
A total of 24 patients were invited to participate. Of these, 14 consented to take part in the study. Reasons participants declined included: being worried their doctors would find out what they had said; the length of the patient consent form; interview fatigue; and concern at being digitally recorded. All participating patients consented to interviews being conducted at their bedside.
The findings are presented in three parts. First, a summation of ward round observations is provided to give situational context. Demographic data of health professionals who attended rounds, including how they introduced themselves, follows. Finally, the findings from patient interviews are given.
Ward round observations
Of the 14 ward rounds observed, all were conducted in the morning, and apart from one, were the first ward round interaction of the day for the patient.
Attendees
Each round varied in who attended from the clinical team. There were seven participants from acute medical - four from medical ward A and three from medical ward B. There were seven participants from rehabilitation – four from rehabilitation A and three from rehabilitation B. There were eight combinations of health care professionals in attendance (Table 1). The most common attendee was the registrar, who was present at all 14 rounds, followed by the consultant (6 rounds), intern (4 rounds), NUM (3 rounds), and each at one round the bedside nurse and medical student.
 |
Table 1 Health professional attendee combinations on the 14 observed ward rounds |
Introductions
Health professionals were introduced to patients by name just over half of the time (59%). The most senior medical officer was introduced first (Table 2). The NUM, if present, was the final person introduced. The bedside nurse was not introduced. The consultant always made the introductions when present. Registrars took over this role if they were the most senior medical officer. During one round, the consultant introduced herself and only introduced the other attendees by saying “you know the medical team” (P13).
 |
Table 2 Health professional introductions at ward rounds: frequency and by whom |
Roles and responsibilities
Roles and responsibilities were defined by health professional (Table 3). The leader of the round was identified as the individual who made the initial contact with the patient, directed the discussion, and made treatment decisions. When the consultant was present, they assumed this role. When the registrar was the most senior attendee, they assumed the role. During all rounds, the leader revisited the patient’s medical history, the level of detail depended on how long the patient had been in hospital. All patients were included in the conversation and invited to ask questions. During the round, registrars acted as the conduit between the consultant and intern. They listened and confirmed information for the consultant then either relayed the information to or observed what the intern documented. In some cases, the consultant conferred with the registrar about patient details rather than asking the patient directly, however this varied from patient to patient as opposed to consultant. If the consultant or intern had to leave the room the registrar stepped into their role. All medical officers took active roles in the ward round. The NUM was a passive attendee who took separate notes to those documented in the electronic medical record.
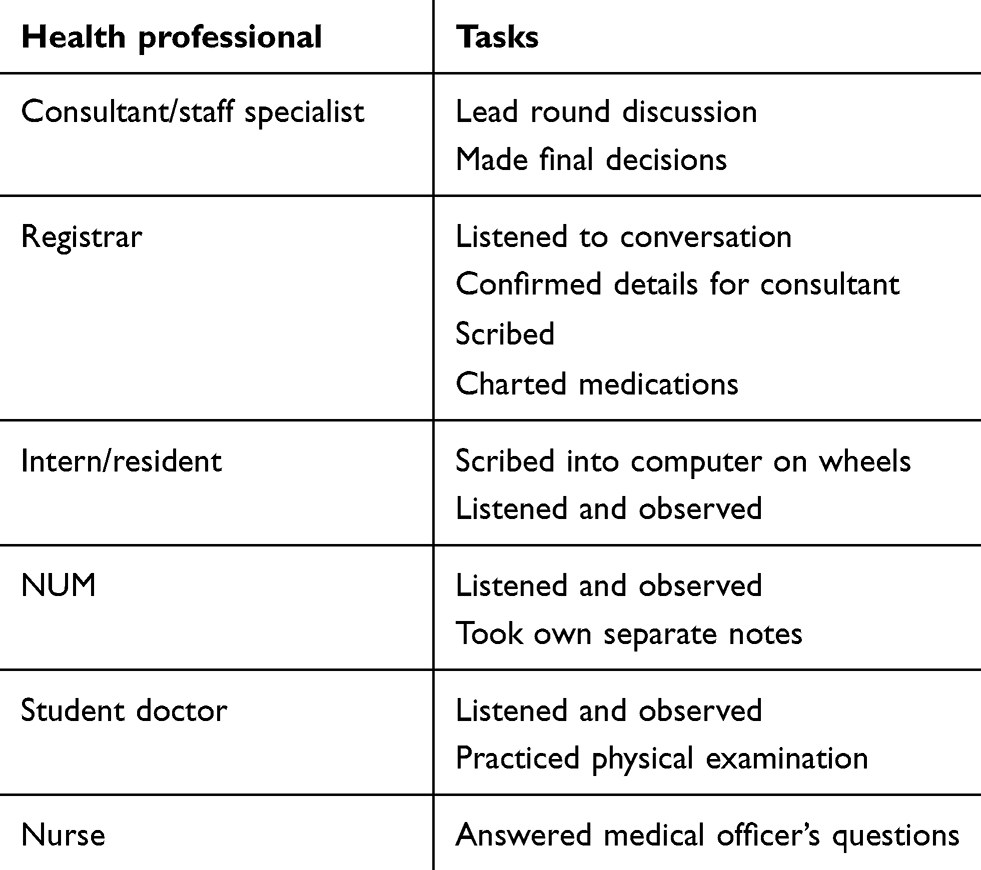 |
Table 3 Health professionals’ roles and responsibilities during the ward round |
Patient demographic characteristics
Of the 14 patients participating, the age range was 55–89 years with a median age of 73 years (Table 4). People over the age of 50 years residing in the local area represent 43.4% of the population.17 All patients were in, or had been, in paid employment, with five in health-related occupations and three now retired. All but one patient had been in hospital before. Patients in rehabilitation ward A and B had a longer length of stay. Of the seven patients, five had been ward more than three days. All both acute medical patients had been in between 0 and 3 days. The gender of participants was provided by the NUM or medical officers at the time they identified possible participants. Patient demographics are summarized in Table 4.
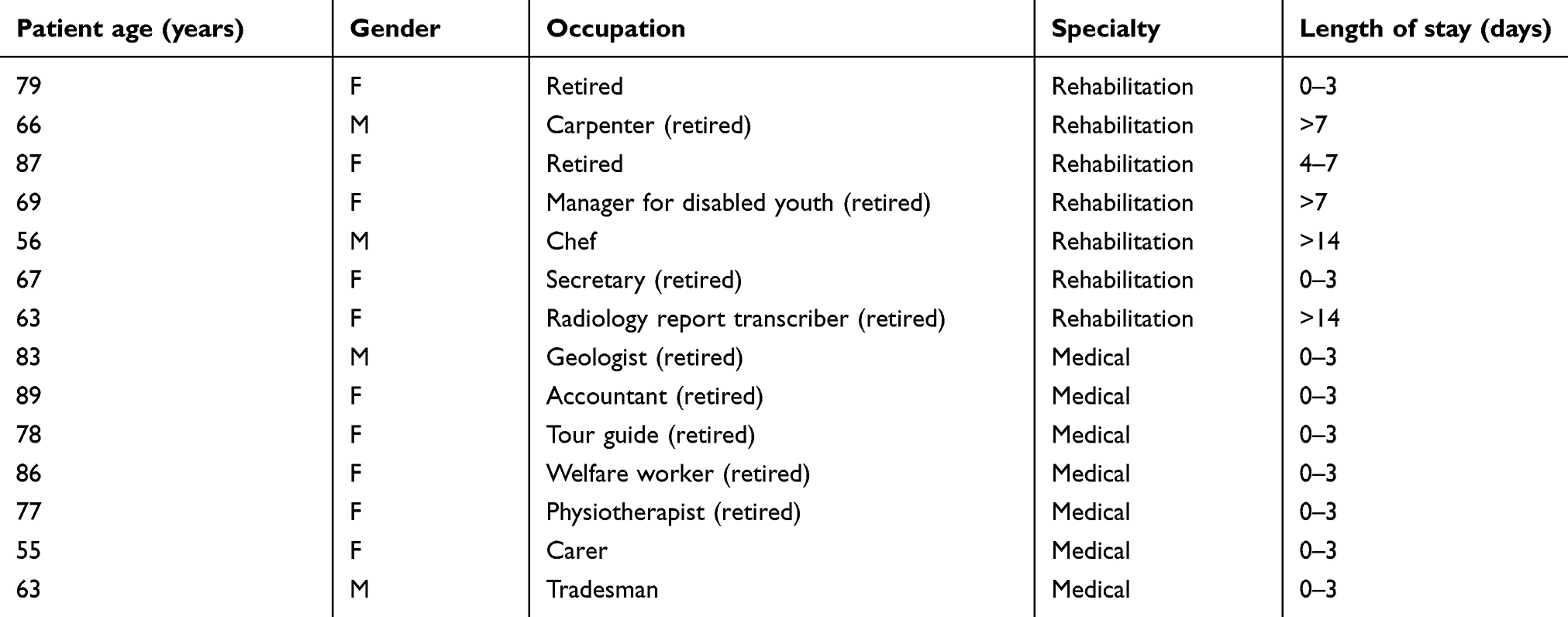 |
Table 4 Patient participant demographics |
Interviews
Responses from the interview data were analyzed by key themes. Findings are presented by question topics and the key themes in each topic identified and presented.
Definition and purpose of ward rounds
Of the 14 patients, 64% (n=9) had heard of the term ‘ward round’ and were able to provide a description of a round. Most participants described a round as a passive process to meet the needs of the health care team: “it is a combination of the team (doctors and maybe a nurse) walking around and discussing” (P13), or “it is there to meet the needs of the doctor” (P2). Participants did describe a more active process involving patients: “doctors and patients interacting” (P4).
When explaining the purpose of a round, participants highlighted it was based upon the nature of the relationship between the patient and health care professionals and, principally, it being directed by medical officers. There were three key concepts that determine the purpose, which involved the exchange of information: medical officers telling patients of the care plan; patients receiving information; and extra activities, which included providing education for students and ensuring written documentation accurately reflected the clinical context. One patient stated the purpose and process of a round was to “update the patient first and the patient tells them how they feel, and a plan is decided on” (P10). Patients reflected this view, simply describing the round as an opportunity “to keep patients informed” (P13).
Health care team and patient relationship during ward rounds
Attendees and roles
Participants identified health professionals attending the round and their perceived roles. The two key concepts emerging from participant responses were: the presence of senior medical officers providing reassurance and knowledge; and knowing the health professionals’ discipline was more valued than their names.
The most frequently identified clinicians attending a round were medical officers, followed by nursing staff. Even when the observed round did not include nurses, participants still included them in the description of a round. No allied health professionals attended the rounds and participants did not include them in the description of attendees.
Most participants (76%) reported clinicians either introducing themselves at the start of a ward round or already knowing them by name from previous introductions. The consultant was the medical officer most likely to be remembered by name and position. It was observed that when the consultant was present, and leading the discussion, participants were less likely to be informed of the rest of the rounding team or be able to recall who the rest of the team were. This view is represented by: “she said ‘they’re my helpers’ but didn’t mention their names, there was no need to” (P3). Recognizing clinicians’ discipline seemed more relevant to participants than their name. This was illustrated during one interview when a medical officer came into the room to chart medications and the participant said: “well she’s a doctor but I still won’t ask her her name” (P4).
When asked about the different role’s health professionals played during the round, all participants replied they were either senior or junior, or a nurse. Medical officers were identified as either “senior” or “junior”. Participants determined senior medical officers lead the conversation and carried out physical examinations. The importance of the senior medical officer present was a consistent theme throughout interviews and is summarized by one participant: “it actually feels nice to have a senior person to come around and not just the junior doctors” (14). Medical officers were again emphasized as the health professionals’ participants wanted to see:
“I do feel reassured when they come rather than just seeing the nurses who when they come, I don’t think they’d have the right answers for me, so the doctor is the one who would have the right answers for me”. (P7)
This importance of medical officers was reinforced by participants. This was illustrated by one who said: “if Dr X were here, she’d be the one in charge, so she is the one I direct my questions to” (P7). Junior medical officers were assumed to be junior as they documented the conversation on the computer. When a nurse was present their role was passive participation and described as “there to listen.” Participants who had previously worked in a health-related field or were chronic care patients were able to articulate the roles in more detail. They described a more comprehensive understanding of the health care team: “his job [junior] is to be familiar with records, to point out to his senior and the nurse what are the important aspects of recent history” (P8). While some participants were able to identify the different roles of the health care team there were also some who either thought they all carried out similar tasks or did not take any notice.
The greatest variety of responses was seen when participants were asked to describe their own role in ward rounds. The key concepts were: taking personal responsibility for understanding the health care system; passive involvement in rounds through listening and “just being”; and active involvement through asking questions and providing information.
Personal responsibility was described as learning how the health care system works. This was reported by people more familiar with the health system (“high users”) of the system, such as participants with chronic care disease as well those who worked in the system. These participants displayed an acceptance that the timing of rounds can be unpredictable. As a result, they described being prepared for rounds. This meant being able to respond to questions from the medical team succinctly by considering information that may be required and preparing for questions that may be asked. One participant encompassed a number of different responses in one explanation: “I think it is very important to write down clearly what you want to say. You’ve got a limited period. If you’ve got things to say and if it’s written down, then it is clear for everybody then” (P8). High users also demonstrated a higher level of confidence in their role particularly around talking to medical officers: Having accurate information was also recognized as important by high users: “Well what I try to do is be as clear as possible. I just think it is so important to the information but I’m not sure I always do” (P12).
Passive involvement in rounds was reported by participants. This was illustrated in two ways. First, when listening to medical officers and waiting for questions to be asked, or when hearing the treatment plan. This behavior was then intertwined or followed by active participation by responding to questions and commenting on the treatment plan.
All but three patients described equal passive and active participation. The three participants, each low users of the health service, stated their role mainly as passive: “to be a guinea pig, to be a patient, to be assessed” (P5), “just a patient” (P14), or “I was just there” (P13).
Patient experience of ward rounds
Participants reported ward rounds both positive and challenging. When describing the overall experience of a ward round three key concepts emerged: the impact of the person’s physical and mental wellbeing; interactions with clinicians; and personal responsibility.
The impact of a person’s physical and mental health made communicating with medical officers challenging. Participants who reported this issue, overall made more negative comments about rounds. It was felt the medical team did not take their physical health into consideration; this was recollected by one participant unable to turn her neck one way due to a physical condition. However, the medical officers stood on the opposite side to the way the participant could turn: “It’s hard when someone is asking you questions, and you can’t be looking there” (P7).
Participants also explained they were in hospital because they were sick and not able to comprehend information as well as they would normally. Hence, interactions with clinicians during rounds revealed the vulnerability some patients felt. Two participants reported feelings of being overwhelmed, in the context of having multiple clinicians present while needing to discuss their medical condition with privacy.
Medical officers being interrupted during rounds influenced how patients communicated with them. Nevertheless, there was a level of acceptance this was part of the hospital environment. Patients with high use of the hospital system identified a greater understanding and acceptance and reported taking personal responsibility. One participant recognized she was the “the one with all the information” (P7) for the medical officers, while another explained that patients “need to assist the system” and be prepared with information. He noted he had learnt over time to “think ahead” (P8). The participant did this by writing down his symptoms, how long he had had them. As a person with a chronic disease he maintained a record of his blood pressure and provided the record to his medical officers in hospital. This assisted him when medical officers asked about his symptoms and meant he did not rely on memory alone.
Participants held a common view of what made them feel valued during a round. The two key interrelated concepts were: communication and time. When positively experienced, participants stated feeling respected and cared for by the health care team. Communication encompassed verbal and non-verbal which included the body language and location of the medical officers.
Participants explained that being listened to by medical officers included in the conversation and subsequently part of the round. This was illustrated by one patient who demonstrated confidence in how the medical officer communicated with her: “I know the doctor will listen to what I have to say” (P7). Another patient took this one step further and felt valued when the medical officer: “repeated to me what I said last night” (P10). Other non-verbal communication included the body language and physical location of the medical officer leading the conversation. As one patient explained: when a medical officer sits on the bed “you sort of feel more relaxed if they sort of relax with you” (P1). The participant who did not feel valued reported “not many doctors” (P2) listen to him or consider his feelings. He explained this from the perspective of past interactions with medical officers.
Two participants who were high users of the health system compared ward rounds previously to now. Both described a shift in collaborating with medical officers: “You know I never thought being a patient has rights, but I do you know, in the past they took away my right.” (P6). This participant also said she had become more confident and this had influenced the way she spoke with medical officers. Another participant also reflected on the change: “It has changed from earlier years. You do not need to be in awe of doctors” (P8).
Participating in the round was viewed as a quarantined time with medical officers. Participants valued medical officers taking time to meet with them, especially if the consultant was present. When this occurred, verbal communication was of increasing importance, where medical officers spoke and explained the plan of care. Roles were reversed, and patients listened while medical officers spoke.
Ward round influences between health care professionals and patients
Advantages of ward rounds
Participants were asked what aspects of ward rounds they did and did not like. Participants initially responded that they felt “reassured” and “cared for”. The key concepts behind these descriptions were: increased confidence in the treatment plan when health professionals are seen working together; and having an opportunity to see and talk with medical officers. These are detailed in the following paragraphs.
When describing the value of having the health care team visiting together, all but one participant referred to the team as medical officers only. Nurses were acknowledged; however, it was seeing senior and junior medical officers working together that patients reflected on. Seeing multiple health professionals discuss a treatment plan in front of them, and with them, provided participants with confidence. One participant explained she felt she was taken seriously: “My condition is being taken so seriously and that everyone is putting their heads together to come up with the best possible remedy” (P12). Another participant described having confidence that having the team together facilitated discussion and provided an opportunity for clarifying information beyond the immediate round interactions: “Well they then go back and discuss what you said, and they could pick up on something they have missed previously” (P9).
The most commonly reported advantage to ward rounds was having the opportunity to see and talk to medical officers, particularly senior doctors. One participant embodied many of the participants’ sentiments:
“Well I like the opportunity to speak to the doctors because you are seeing the nurses you’re seeing other people like social workers and occupational therapists and so forth and you know the rehab people but umm the doctors are sort of the one that ahhhh sort of bringing it all together and making sure that what’s happening in your area is correct”. (P4)
While medical officers were described as providing information, it was equally important to have them visit so participants could inform them: “it lets me voice my opinion” (P6).
Disadvantages of ward rounds
The aspects of ward rounds participants found challenging were linked to how ward rounds could be improved. Key concepts relating to the challenges of rounds are: uncertainty about when the round will take place; confidence to be an active participant; and communication.
Just over half (57%) of participants said not knowing when the round would occur was challenging and something that could be improved. Difficulties in not knowing the time made one participant anxious he was going to miss out on physical therapy. This had been identified as an important part of his treatment plan during the round: “Yeah well I don’t know what is happening. I didn’t know they were coming today. I’ve got occupational therapy from 10 am. Now I don’t know when they’re coming either” (P5). Other participants did not know a specific time but explained they could be “sometime” in the morning. Despite timing being one of the main challenges, high service users were more likely to explain a level of acceptance of this such as: “I know they have to put all the tests together, so you know” (P13), and “time, they probably don’t know themselves, they have to be flexible” (P8).
The second and third key concepts were interrelated. Most participant’s responses illustrated a level of confidence when interacting with health professionals during the round. However, there were different aspects that made interacting challenging. These varied between participants feeling overwhelmed by the number of health professionals present during the round was commented on by two participants and described by one as:
“I’m shy so I don’t like so many people looking at you. You’re not in the best condition you know, no bra on (laughs) they’re resting on my stomach (laughs). Anyway, if you’re really shy it could be anxious and it is intimidating because you have all these people looking at you and you don’t know what is going through their mind” (P13).
This then manifested into not asking questions. As explained by a participant, who described similar feelings multiple times during the interview:
“I think they could have made a comment like “have you got any questions? You don’t really get any opportunities to say any questions but because I knew them [the doctors] I probably should have just asked them, but it would have been nice if someone asked if I had any questions” (P13).
Just under half (43%) of participants mentioned being unable to understand part of the conversations with medical officers, or not knowing what medical officers were talking about between themselves during the round. Of these participants, two said they ask the medical officer to clarify what they meant. Another two participants said it was difficult but not always necessary to know what it means. While for others it led to feeling excluded from conversations. One participant explained:
“It’s when they start using medical terms that you’re not familiar with, I just lose them. You’ve got no idea what they’re talking about and yeah, yeah, so that sort of leaves you feeling left out and not sure what is happening” (P5).
What could be done to improve ward rounds?
Participants were asked based on their experience what could be done to improve the ward round process. Initially most participants responded the rounding process was satisfactory, however two key concepts centering around providing patients with information emerged: having a specified time for the round; and being informed in advance of what will be discussed in a round. Three individual suggestions were also made: having a nurse present; humor; and the patient being prepared.
Participants suggested being told when the ward round was to occur would be helpful, illustrated simply by one participant suggestion of “give us a time” (P5). Holding the round in the afternoon was suggested by one participant because the afternoons were not as busy as morning.
Similar to knowing when rounds were to occur, participants suggested being informed ahead of time of discussion topics would allow them to be prepared: “being forewarned about the questions, because it is “difficult to think ahead” (P11). This was echoed by another participant who said, “you could have time to think” (P9). This enabled participants to prepare their own questions during the round.
Other suggestions made by single participants included having a nurse present to improve communication between medical officers and nurses. It was explained that currently the nurse “is kept in the dark” (P10). Another participant suggested that at times “a bit of humor wouldn’t hurt” (P11); health professionals could be very serious and less intensity at times would be an improvement.
Participants also described elements that patients could do to improve rounds. These included being aware of your own medical history to “to assist the medical people to make sure the facts are right” (P8). Another participant suggested sitting up allowed for improved communication with health professionals during the round.
Discussion
This study investigated the patient experience of participating in a ward round, the relationship between patients and clinicians, and whether rounds facilitate a collaborative partnership. We summarize the findings as follows: patients value ward rounds as an opportunity to speak with the senior medical officers, however patients with more experience as system users have more engagement with the process. This concise and precise result empirically confirms anecdotal evidence from clinical practice. Our findings support and build upon earlier studies conducted internationally. This suggests commonalities between ward rounds and patient participation amongst different health systems.
Most commonly, observational studies of ward rounds and patient focus groups, surveys and interviews have been undertaken independently of each other.1,18 From the literature, we identified one study undertaken on an acute medicine ward that both observed ward rounds and interviewed patients about their involvement.7 Another study conducted in an emergency room observed rounds and conducted patient satisfaction surveys following the round.19 This study builds on this work by exploring ward rounds from the patient perspective, across both acute medicine and rehabilitation specialties, using both observation and interviews.
The age of study participants demographics is representative of the population. They also represent a health system facing an increasing aging population. Over the years, the culture of patient and medical officer relationships has changed to more collaborative20 however patients from different generations will naturally interact differently to health professionals. Health professionals cannot take a “one size fits all” approach to patient interactions. Although each patient is an individual with their own experiences, historical patient-health professional relationships can be seen in population groups.21
While our study found no meaningful difference between acute medicine and rehabilitation participants, it did reveal a difference between high system users compared with those who are infrequently admitted to hospital. High users described more self-directed engagement with medical officers when participating in treatment planning and asking questions. They spoke with more confidence about their role in the ward round. They also showed a level of acceptance that some challenges of ward rounds relate to the health care system. Participants described experiences and collaborative partnerships as ebbs and flows during the duration of the round. Our findings demonstrate the contrast between what patients perceive and the actual process of a ward round. Nearly all participants described a ward round involving medial officers and nurses. This was despite most of the rounds observed including only medical officers. The perception of what a ward round is may be an ingrained concept from traditional rounds when nurses accompanied medical officers. All but one patient considered that nurses were not necessary on the round. This differed from an earlier study undertaken in Sweden where patients identified it was easier to engage with nurses during the ward round, but nurses and medical officer complimented each other.1 The opinion that nurses were not required on the round may reflect that participants were generally satisfied with their experience of rounds that only involved only medical officers. Coupled with this was the desire to receive information from medical officers. This finding illustrates three key contributing factors to the patient experience on ward rounds are: medical officers; health system; and the patient’s previous experiences of ward rounds (Figure 2). This builds upon Swenne and Skytt1 study which found time allocation for rounds and physician – patient communication influenced participation. Although this may appear simplistic and obvious, the importance of this point can be overlooked. This taken-for-granted knowledge, empirically revealed here through rigorous research, highlights the interactional effects of the professionals and the system on patient experience. The finding points to the need for research into the impact of efficient and effective ward rounds on patient outcomes, including, for example, reducing length of stay.
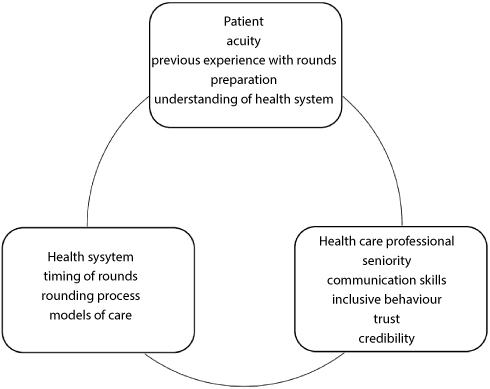 |
Figure 2 Influences on the patient experience of ward rounds. |
Patient-centered care places significant responsibility on medical officers to establish an effective and efficient therapeutic relationship with patients. Confounding this is when professional associations and policy-makers continue to promote rounds that are led by medical officers,22,23 which can imply the balance of power remains with medical officers.
Our findings showed the presence of senior medical officers strongly influences the patient experience. Patients have the most confidence when information and decisions were delivered by the consultant. Anecdotally this is not an unknown concept; nevertheless, little research into this area was found. One study looking at patient preferences for communication styles found self-confidence and competency in conversation were positive attributes.24 The experience that consultants have may contribute to more confidence in decision making and delivery of the message. The same study found when medical officers focused on talking to patients as opposed to documenting and reading notes it was reported favorably.24 In all our rounds involving consultants, they were able to focus their attention on the patient as the junior medical officers were documenting the decisions.
Those more familiar with the hospital system described, and were observed, to have a more collaborative relationship. Patients were more prepared for the round in terms both what was expected for them and what they wanted. This assisted with the efficiency of a round as a key function is to obtain information and plan care through clinician and patient communication.1 This must happen in a limited space of time. Studies investigating how to prepare health professionals for rounds are plentiful, however there is a paucity exploring how best to prepare patients and evaluate their experience. Ensuring patients are prepared for a ward round will facilitate communication and expectations they have when meeting with their health care team.
Clinical and research implications
It is not uncommon to hear the term “ward round” spoken to and by patients. Our results revealed one third of participants had not heard of the term, or not able to describe the purpose. Therefore, is not unreasonable for patients to feel uncertain about their role in them. This may impact on medical teams’ ability to elicit information needed to plan care; patient adherence with treatment; and patient satisfaction. Further exploration into the comparison between male and female, experiences of ward rounds may offer additional insight into the relationship between healthcare self-management and health care team collaboration. Similarly investigating the influence patient age has on how healthcare teams and patients interact may provide additional insight delivering patient-centered care. Further research into how best to prepare patients for a ward round, to meet the needs of the patient and health professional would build upon shared decision making principles.
Methodological considerations
This study was conducted at one facility with a relatively small number of patients. However, the use of multiple methods and multiple wards to triangulate findings, strengthens the study’s credibility. Due to the nature of the setting, patients were from a vulnerable population group, so participant selection was biased towards those capable of engaging in and collaborating for shared decision making. Some participants were acutely unwell or frail aged, therefore exploring their responses in more detail which included extending the interview time was not feasible and this should be taken into consideration for future studies.
Conclusion
Our findings indicate there is a level of acceptance that a ward round is just part of being in hospital and of being a patient. However, with deeper exploration, the complexities of being a patient in a ward round are uncovered. There is a high expectation on senior medical officers to be present at rounds to facilitate patient confidence and yet this may not be always possible. The experiences between high users of the healthcare system and infrequent users suggest participating in rounds over the course of multiple hospital admissions allows patients to have more realistic expectations of this process and increases their engagement and collaboration with the healthcare team for decision making. High system users have learnt to work with rounding process. There is an opportunity for healthcare providers to learn from patients about how they experience ward rounds and so improvements can be developed from both perspectives.
Ethical approval
Northern Sydney Local Health District Human Ethics Committee LNR/13/HAWKE/365.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Swenne CL, Skytt B. The ward round – patient experiences and barriers to participation. Scand J Caring Sci. 2014;28(2):297–304. doi:10.1111/scs.12059
2. Walton V, Hogden A, Johnson J, Greenfield D. Ward rounds, participants, roles and perceptions: literature review. Int J Health Care Qual Assur. 2016;29(4):364–379. doi:10.1108/IJHCQA-04-2015-0053
3. Australian Commission on Safety and Quality in Health Care. Shared Decision Making; 2018. Available from: https://www.safetyandquality.gov.au/our-work/shared-decision-making/.
4. Vahdat S, Hamzehgardeshi L, Hessam S, Hamzehgardeshi Z. Patient involvement in health care decision making: a review. Iran Red Crescent Med J. 2014;16(1):e12454. doi:10.5812/ircmj.12454
5. Smith SK, Dixon A, Trevena L, Nutbeam D, McCaffery KJ. Exploring patient involvement in healthcare decision making across different education and functional health literacy groups. Soc Sci Med. 2009;69(12):1805–1812. doi:10.1016/j.socscimed.2009.09.056
6. Sweet GS, Wilson HJ. A patient’s experience of ward rounds. Patient Educ Couns. 2011;84(2):150–151. doi:10.1016/j.pec.2010.08.016
7. Redley B, McTier L, Botti M, et al. Patient participation in inpatient ward rounds on acute inpatient medical wards: a descriptive study. BMJ Qual Saf. 2019;28(1):15–23.
8. Baathe F, Ahlborg G
9. Creswell J. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches.
10. O’Leary Z. The Essential Guide to Doing Research. London: SAGE; 2009.
11. Robinson OC. Sampling in interview-based qualitative research: a theoretical and practical guide. Qual Res Psychol. 2014;11(1):25–41. doi:10.1080/14780887.2013.801543
12. Francis JJ, Johnston M, Robertson C, et al. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol Health. 2010;25(10):1229–1245. doi:10.1080/08870440903194015
13. Maguire M, Delahunt B. Doing a thematic analysis: a practical, step-by-step guide for learning and teaching scholars. AISHE-J. 2017;8(3):3351–33514.
14. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: strivingto meet the trustworthiness criteria. Int J Qual Methods. 2017;16(1):1609406917733847. doi:10.1177/1609406917733847
15. Schwandt TA, Lincoln YS, Guba EG. Judging interpretations: but is it rigorous? Trustworthiness and authenticity in naturalistic evaluation. New Direction Eval. 2007;2007(114):11–25. doi:10.1002/(ISSN)1534-875X
16. Denham MA, Onwuegbuzie AJ. Beyond words: using nonverbal communication data in research to enhance thick description and interpretation. Int J Qual Methods. 2013;12(1):670–696. doi:10.1177/160940691301200137
17. Australian Bureau of Statistics. 2016 Cenus QuickStats; 2018. Available from: https://www.abs.gov.au/websitedbs/D3310114.nsf/Home/2016%20QuickStats.
18. O’Leary KJ, Killarney A, Hansen LO, et al. Effect of patient-centred bedside rounds on hospitalised patients’ decision control, activation and satisfaction with care. BMJ Qual Saf. 2016;25(12):921–928. doi:10.1136/bmjqs-2015-004561
19. Chow MY, Nikolic S, Shetty A, Lai K. Structured interdisciplinary bedside rounds in an Australian tertiary hospital emergency department: patient satisfaction and staff perspectives. Emergency Med Australas. 2019;31(3):347–354.
20. Frosch DL, Kaplan RM. Shared decision making in clinical medicine: past research and future directions. Am J Prev Med. 1999;17(4):285–294.
21. Ekdahl AW, Andersson L, Wiréhn A-B, Friedrichsen M. Are elderly people with co-morbidities involved adequately in medical decision making when hospitalised? A cross-sectional survey. BMC Geriatr. 2011;11(1):46. doi:10.1186/1471-2318-11-46
22. Commission CE. In Safe Hands; 2017. Available from: http://www.cec.health.nsw.gov.au/quality-improvement/team-effectiveness/insafehands.
23. Royal College of Physicians and Royal College of Nursing. Ward Rounds in Medicine Principals for Best Practice. London: RCP; 2012.
24. Mazzi MA, Rimondini M, Deveugele M, et al. What do people appreciate in physicians’ communication? An international study with focus groups using videotaped medical consultations. Health Expectations. 2015;18(5):1215–1226. doi:10.1111/hex.12097
Supplementary materials
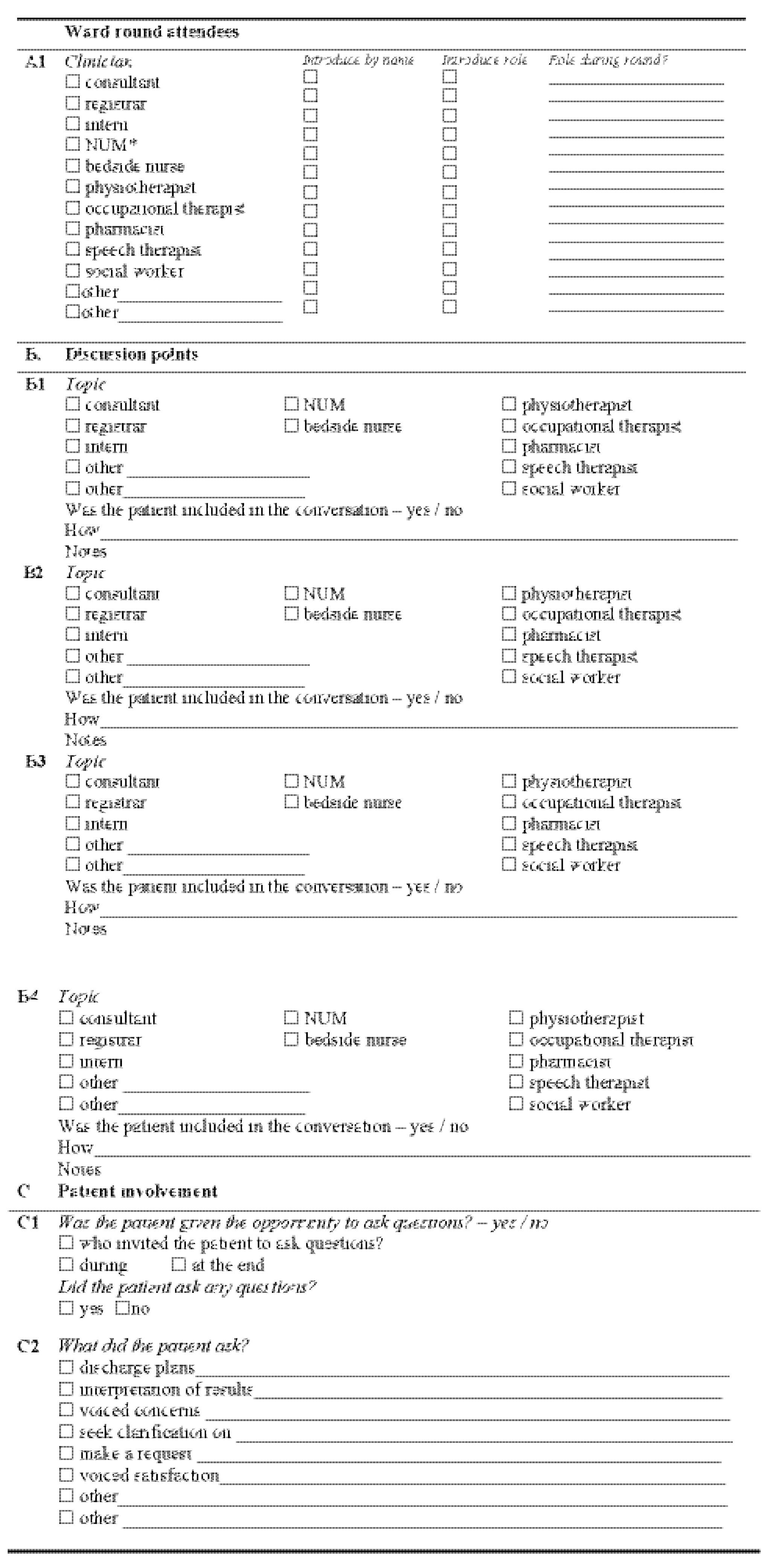 |
Table S1 Ward round observation tool |
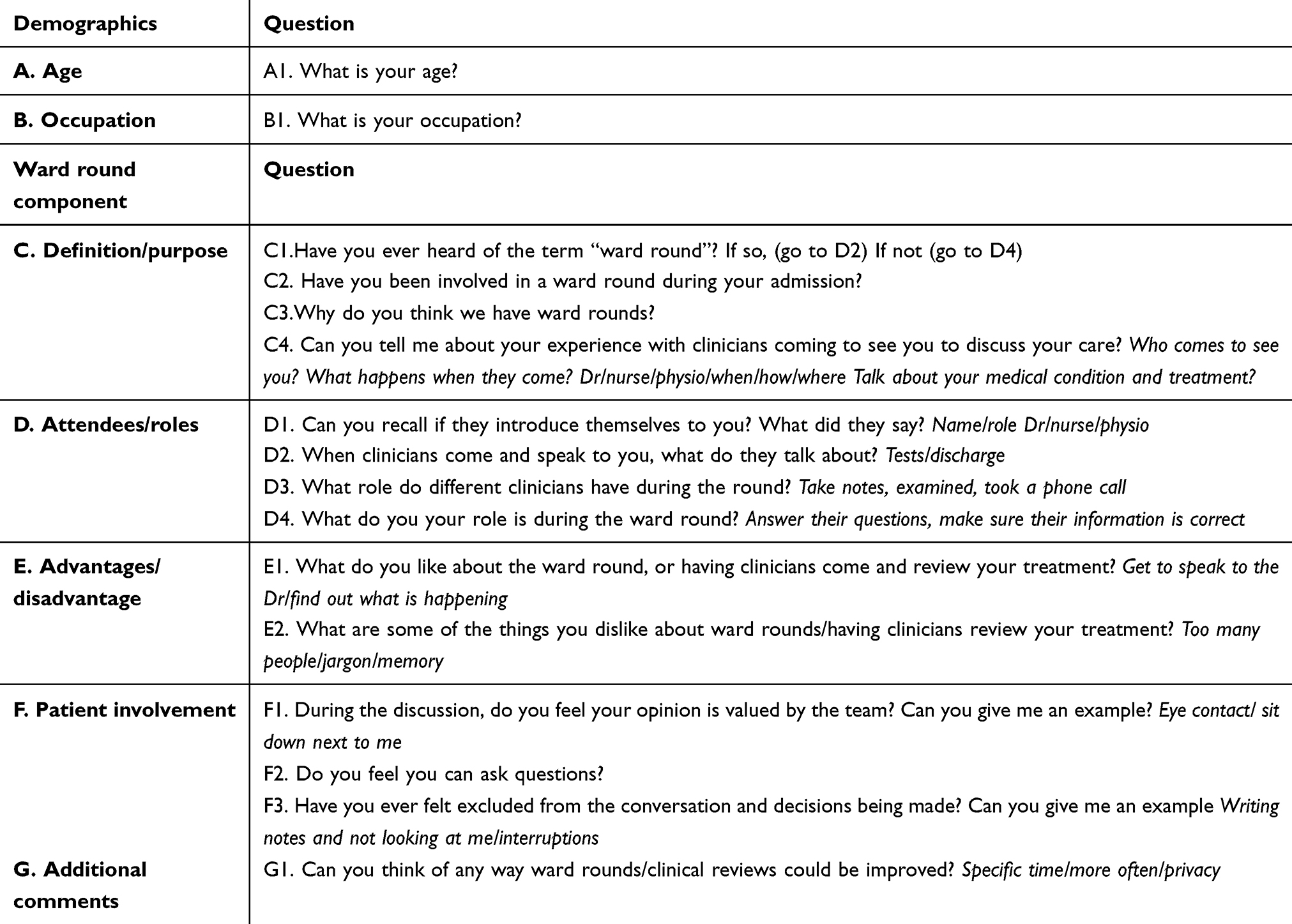 |
Table S2 Patient interview guide |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.