")
Back to Journals » Patient Preference and Adherence » Volume 14
Patient–Pharmacist Interaction in Ethiopia: Systematic Review of Barriers to Communication
Authors Yimer YS , Mohammed SA , Hailu AD
Received 19 April 2020
Accepted for publication 26 June 2020
Published 28 July 2020 Volume 2020:14 Pages 1295—1305
DOI https://doi.org/10.2147/PPA.S258914
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Yohannes Shumet Yimer,1 Solomon Ahmed Mohammed,2 Abel Demerew Hailu3
1Department of Pharmacy, College of Medicine and Health Science, Debre Tabor University, Debre Tabor, Ethiopia; 2Department of Pharmacy, College of Medicine and Health Science, Wollo University, Dessie, Ethiopia; 3Department of Pharmacy, Dessie Health Science Collage, Dessie, Ethiopia
Correspondence: Solomon Ahmed Mohammed Tel +251910504378
Email [email protected]
Abstract: Despite the fact that pharmaceutical care has been expanding simultaneously with the increasing role of pharmacists and the number of prescriptions dispensed, the extended role of community pharmacists is largely confined to the dispensing of medications. This advancement in pharmacy services demands competent pharmacists and patient-centered communication. The objective of this review was to explore the barriers to patient–pharmacy interaction. Relevant kinds of literature were searched from Google Scholar, PubMed, Hinari, We of Science, Scopus, and Science Direct. A total of 3025 kinds of literature were searched. After excluding redundant and irrelevant literature, 13 kinds of literature were reviewed. Lack of adequate knowledge of drugs, lack of updated drug information, work experience, poor job satisfaction, lack of good communication skills, shortage of time, and clearness of pharmacist’s voice and tone were barriers to communication from the side of pharmacy professionals. Factors like not wanting to talk much, bad attitude toward the pharmacy, being in a rush to leave, lack of willingness, language and educational status of the patient were patients’ communication obstacles while high patient load, the suitability of dispensing area, and waiting time for service were associated challenges for patient-centered communication faced by health facilities. Barriers to patient–pharmacist interactions were related to patients, pharmacy professionals, and health institutions. These factors are not independent and the presence of one factor may trigger others and further compromise the patient–pharmacist interaction and result in poor medication outcomes.
Keywords: patient, pharmacist, communication and Ethiopia
Introduction
Pharmacists are one of the most accessible health care professionals in the community who offer ongoing education on medicine management, monitoring and advice to the population.1 They have a professional and ethical responsibility to consider the needs and situation of the patient holistically.2
Traditionally, pharmacists have been concerned about the pharmacologic and pharmacotherapeutic properties of a drug to meet a patient’s medication-related needs and promote medication compliance.3 Fortunately, modern medicine is moving away from a purely biological model of care to a biopsychosocial model.2 Despite scientific drug knowledge being important, a patient-centered approach requires knowledge of the patient and their individual experience of illness and medication.3
Pharmaceutical care is the contribution of pharmacy professionals to the care of individuals in order to optimize medicine use and improve health outcomes.4 Pharmaceutical care services have been expanding simultaneously with the increasing role of pharmacists and the number of prescriptions dispensed.5 This advancement in pharmacy service demands competent pharmacists and patient-centered communication.3 Patient-centered communication is understanding patient perspectives, patient psychosocial and cultural contexts, and reaching a shared understanding of patient problems concordantly.2
Despite clinical pharmacy programs being practiced in Ethiopia, implementation of pharmaceutical care is still limited.6 The extended role of community pharmacists in developing countries is largely inclined to dispense medications.7 More than 50% of all medicines are prescribed and dispensed inappropriately and 50% of patients fail to take them correctly.8 This inappropriate use of drugs can lead to wasted resources9 and predispose patients to increased risk of adverse drug reactions and fosters the development of drug resistance.10
Various studies have revealed different reasons for malpractice in dispensing, including lack of time and interest, inadequate knowledge and distance of the community pharmacy from hospital.10 Shortage of pharmacy professionals, lack of preparedness of the practicing pharmacist, and patient perception toward practicing pharmacist also contributed to miscommunications.11
Pharmacists should foster patient-centered communication to develop a trusting relationship in order to improve patient health and reduce the number of medication-related errors.2 However, the quality of interaction between pharmacists and patients affects patients’ adherence and satisfaction with the service. Thus, openness, active listening, and plain speaking are skills in which all pharmacists should be competent.5
It is mandatory to counsel patients for both prescribed and non-prescribed drugs on every aspect of the medication like duration of therapy, special directions and precautions, common side effects, therapeutic indications and contraindications, proper storage, refill information and appropriate actions to be taken in case of missed dose.12 This will positively influence patient compliance.13 Moreover, pharmacist counseling can significantly reduce hospitalization14 and health care costs.15
To date, there has not been any review done regarding barriers to the provision of pharmaceutical services. Taking the evidence in Ethiopia into consideration, the present review was conducted with the need to explore the barriers that limit effective communication between pharmacy professionals and patients.
Materials and Methods
Search Strategy
Relevant literature was searched from electronic databases including, Google Scholar, PubMed, Hinari, Web of Science, Scopus, and Science Direct and iterative reviews of reference lists of papers using the key words “patient”, “pharmacist”, “communication”, “Ethiopia” and in combination from February 10 to 13, 2020. From these databases, a total of 3025 studies were extrapolated. After excluding redundant and irrelevant literature, a total of 12 separately published empirical articles in peer-reviewed journals and one gray literature were reviewed. The search process is displayed in Figure 1.
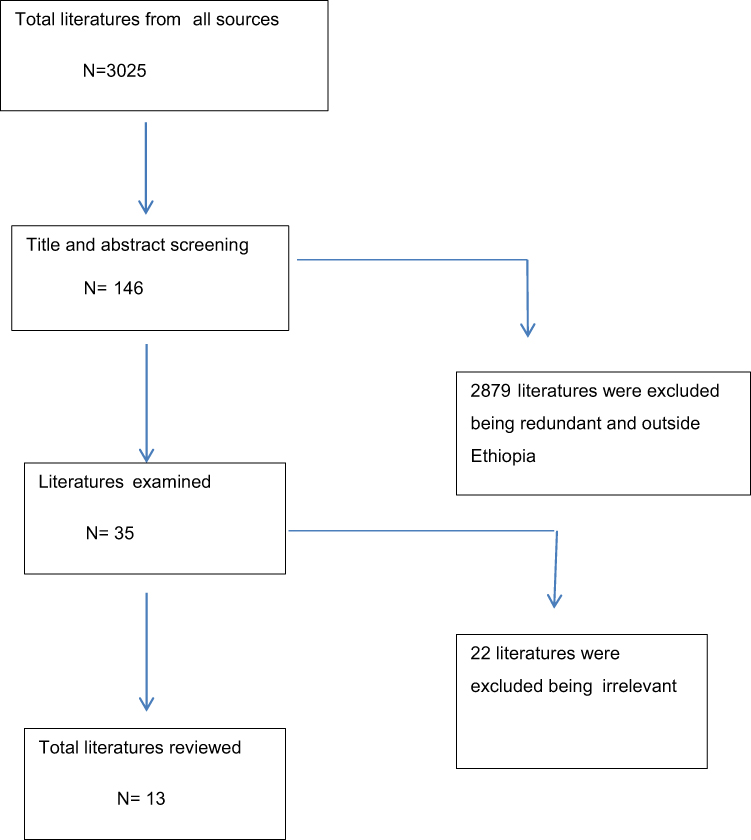 |
Figure 1 Data search process. |
The inclusion criteria were: type of study: all, publication: peer-reviewed and gray literature, population: Ethiopia, time period: 2009 to present, and language: English. Studies that were opinions, critiques of previous studies, and letters to editors were excluded.
Data Abstraction
Screening of the articles was done based on the inclusion/exclusion criteria. Author, year of publication, study area, study subjects, sample size, study design, sampling technique, and barriers to patient–pharmacist interaction were extracted from each study using an abstraction format.
Study Characteristics
All included studies (13) differed in sample size and location. From these articles, all except one were cross-sectional studies, while one study further used patient simulation. Three studies assessed patient–pharmacist interaction at the community level, six assessed in health institutions, and four assessed at both setups. A detailed description of the characteristics of individual studies is displayed in Table 1.
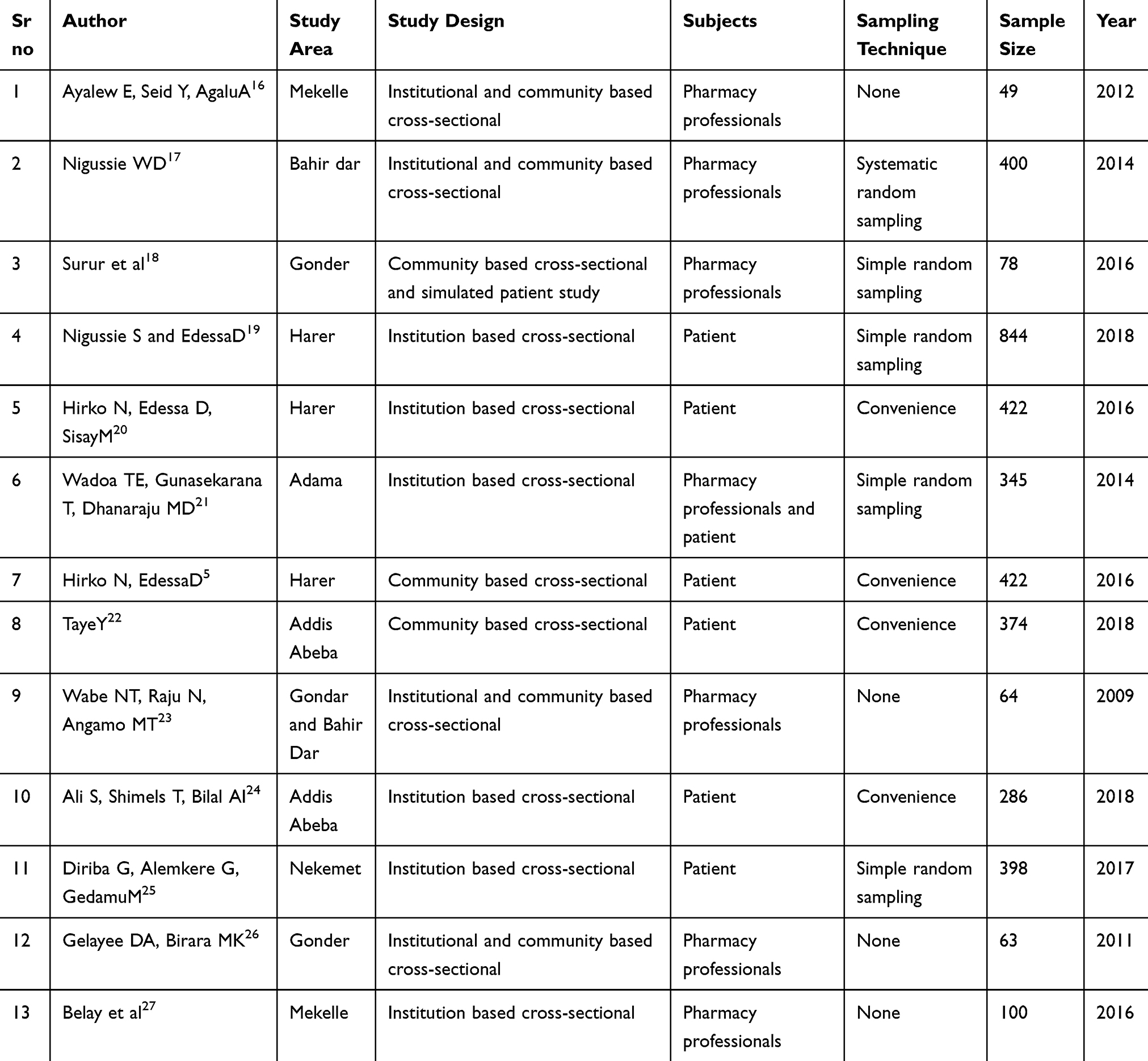 |
Table 1 Detailed Descriptions of Study Characteristics |
Assessment of Methodological Quality
Methodological validity was checked prior to inclusion of selected articles and during the review by undertaking critical appraisal using preferred reporting items for systematic reviews and meta-analysis (PRISMA) flow diagram and guidance set out by the center for reviews and dissemination.28
There were three reviewers in this review and two reviewers appraised the full text of each study independently. Any discrepancies between the two reviewers were resolved through discussion and/or by involving a third reviewer as an arbiter. Finally, the third reviewer validated the final selection of publications.
Results
All studies identified various factors that distort the patient–pharmacist interaction in Ethiopia. These factors were categorized into barriers related to patients, pharmacy professionals and health institutions.
Pharmacy Professionals’ Related Barriers to Communication
Lack of adequate knowledge of drugs, lack of updated drug information, work experience, poor satisfaction on the job, lack of good communication skills, shortage of time, and clearness of pharmacist’s voice and tone were identified barriers to communication from the side of pharmacy professionals (Table 2).
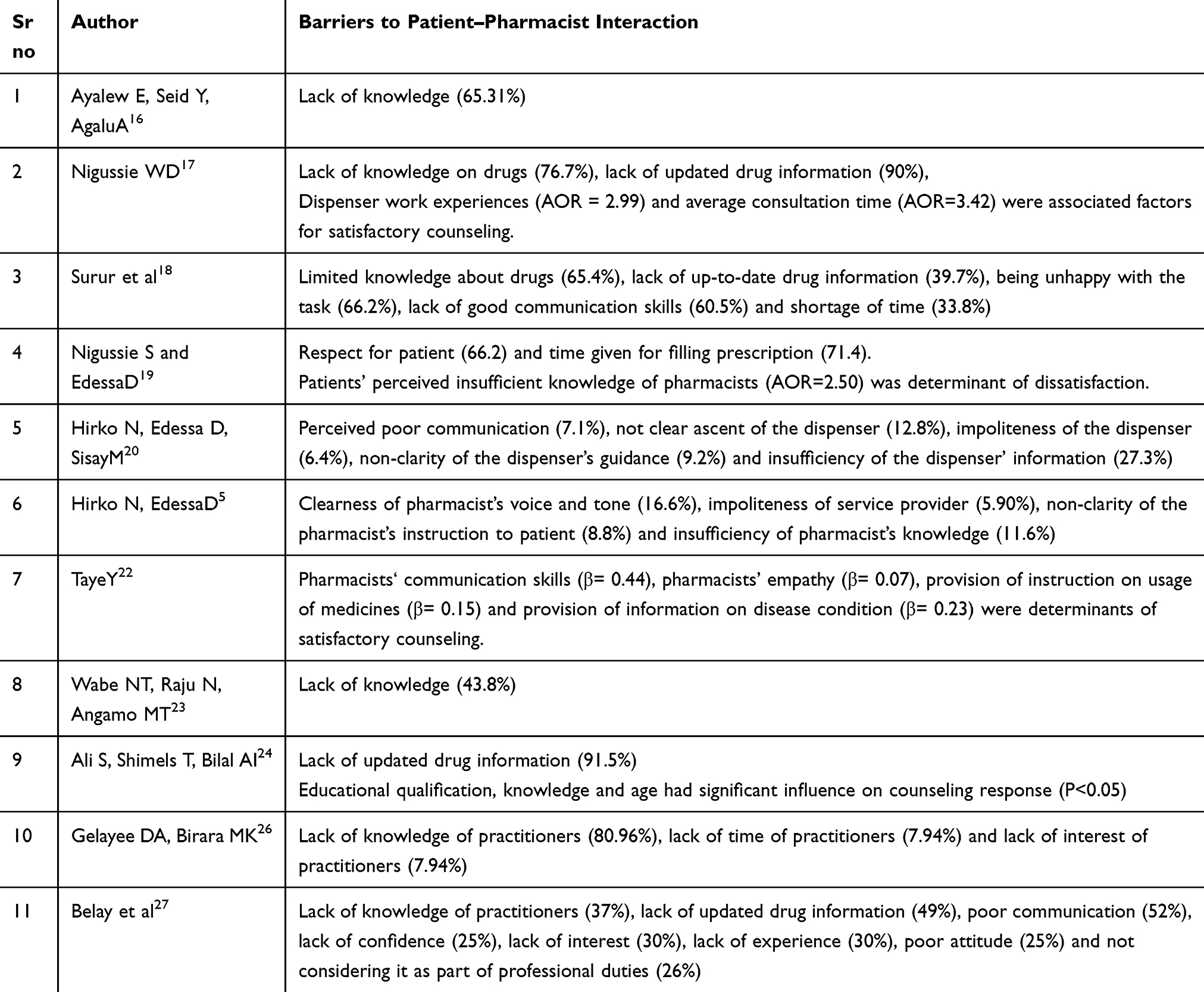 |
Table 2 Pharmacy Professionals’ Barriers to Communication |
Lack of adequate knowledge of drugs was identified as a barrier to communication in eleven of the studies. The time spent for consultation, lack of updated drug information, and lack of good communication skills were identified barriers to dispensing pharmaceuticals from the side of pharmacy professionals in five and four studies, respectively (Figure 2).
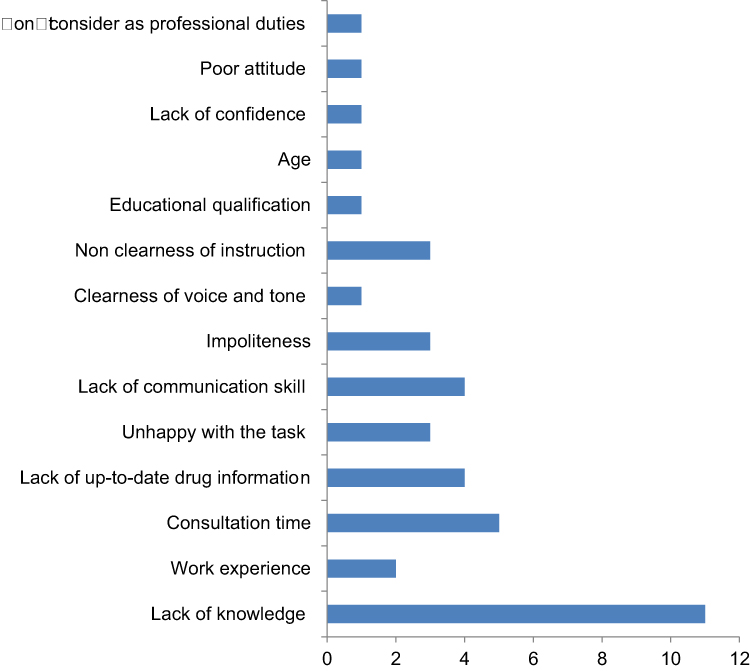 |
Figure 2 Frequency of pharmacy professionals’ related barriers to communication. |
Patients’ Related Barriers to Communication
Factors like not wanting to talk much, bad attitude toward pharmacy, rush to leave, lack of willingness, the language, and educational status of patients were patients’ communication obstacles (Table 3).
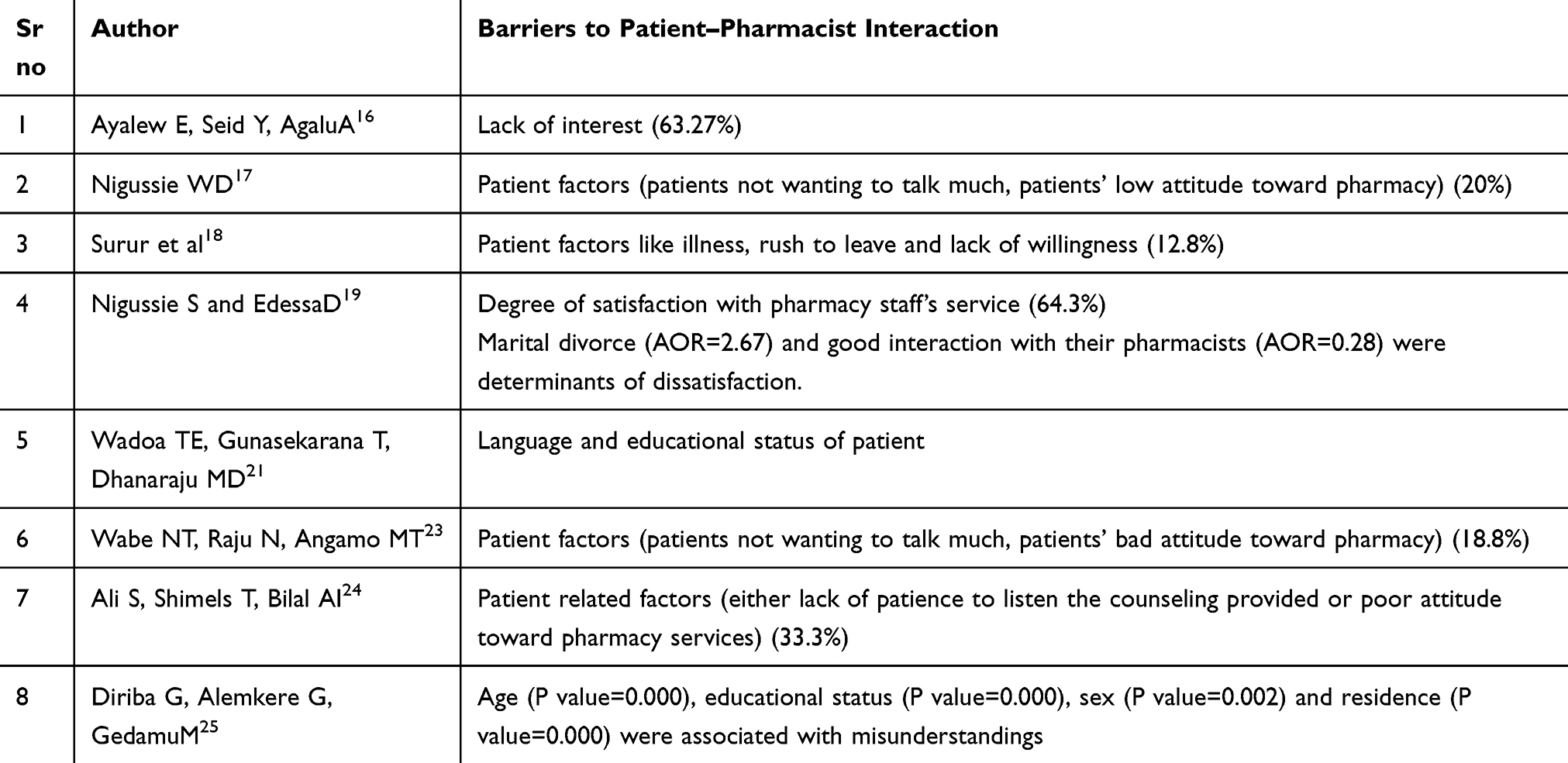 |
Table 3 Patient Barriers to Communication |
The bad attitude of patients toward pharmacy services was the most frequently stated barrier, followed by lack of interest in listening to the information provided and their educational status and rush to leave. The rest of the stated factors were only revealed in the sole study (Figure 3).
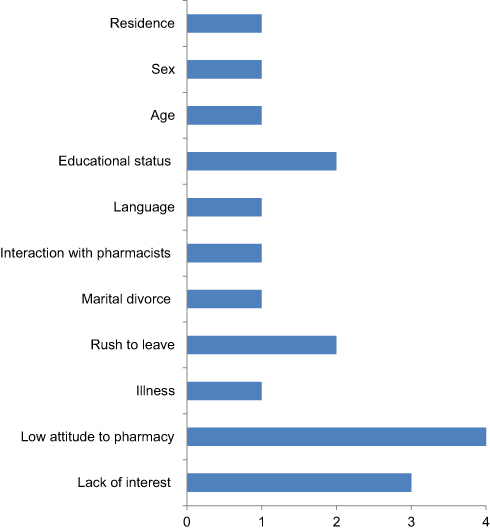 |
Figure 3 Frequency of patients’ related barriers to communication. |
Health Facility-Related Barriers to Communication
The patient load, suitability of dispensing area, and waiting time for service were associated challenges for patient-centered communication by health facilities (Table 4).
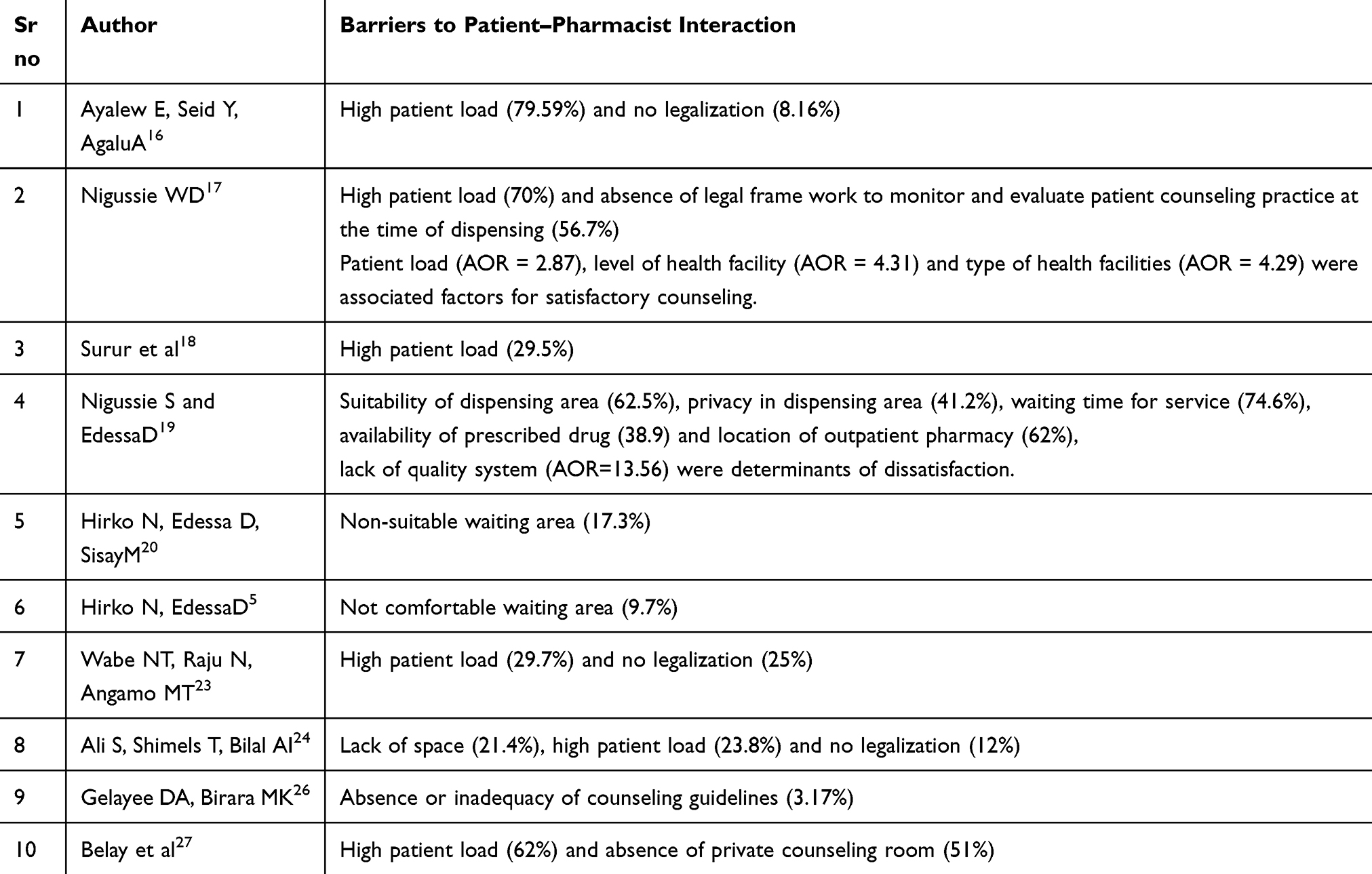 |
Table 4 Health Facility-Related Barriers to Communication |
The patient load, suitability of dispensing area, and absence of legal frame work to monitor and evaluate patient counseling practice were frequent challenges for rational dispensing barriers by health facilities (Figure 4).
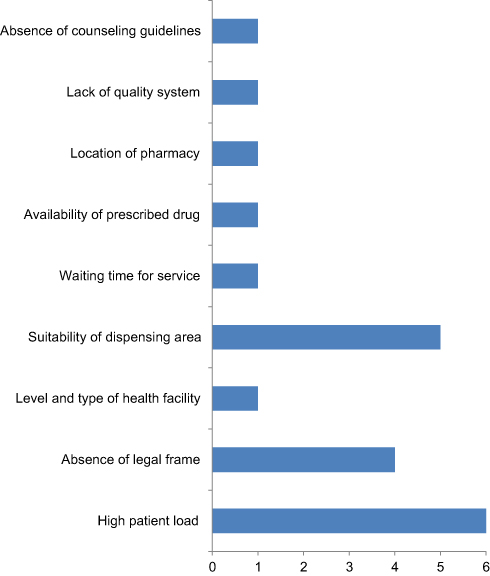 |
Figure 4 Frequency of health facility-related barriers to communication. |
Discussion
Pharmacy professionals’ inadequate knowledge was the barrier of interaction for 11.6–80.96% of communications. Two studies revealed that dispensers’ inadequate knowledge was found to be a statistically significant predictor for satisfactory counseling.19,24 Lack of updated drug information was reported in four studies (39.7–90%) as the major barrier for patient–pharmacist interaction. The educational status of pharmacy professionals was also a significant determinant.24 The majority of community pharmacists revealed that they often provide information on dosing schedule, how to take medication, importance of compliance, contraindication, drug–food interaction, and storage conditions.29 Since new drug products are entering the market and new information is added to the existing drugs, updated information is mandatory. Although academic institutions in Ethiopia have recently tried to revise their curriculum, more emphasis should be given to the provision of pharmaceutical services as the global trend of pharmacy education and service has been changing.6 Moreover, the involvement of trained clinical pharmacists in resource-limited settings leads to clinically relevant and well-accepted optimization of medicine use.30
The provision of instruction on usage of medicines (β= 0.15) and provision of information on disease condition (β= 0.23) increased patient satisfaction of counseling.22 Patient counseling plays an important role in reducing medication-related problems and improving patients’ overall health status.13 Updated drug information provided by pharmacy professionals during counseling can save money and prevent unnecessary hospitalization.8 However, medication counseling is under scrutiny in Ethiopia. This was attributed to poor attitudes and lack of industriousness among professionals, lack of access to up-to-date references, and a loose regulatory system.21
Pharmacy professional sympathy and friendliness had a significant impact on patient satisfaction and affected 5.9–66.2% of patient–pharmacist interactions. It is also a statistically significant determinant of satisfactory counseling.22 A positive attitude toward patients is the most important factor for satisfaction with pharmacy services.31 In Maltese community pharmacies, 44% of consumers visit pharmacies seeking sympathy and friendly service.32
Despite pharmacy professionals having ethical and moral responsibility to offer the best service for their patients, 7.94–66.2% of patient–pharmacy professional communications have been distorted due to lack of interest and being unhappy with the task. In Portugal, dispensers’ loyalty influences pharmacist-patient communication, and humanistic-based skills promote desirable counseling.33 This was due to the presence of limited pharmaceutical care initiatives to the profession and professionals.34
Five of the studies stated that average consultation time was a barrier for satisfactory counseling and was found to be statistically associated (AOR=3.42).17 Being too busy was reported by over half of pharmacists (59.6%) in Saudi Arabia as a barrier for patient counseling.35 Medication counseling in Ethiopia is limited to dispensing, due to patient load and poor attitude among pharmacy professionals and patients.21 A very short dispensing time was considered as a major factor for inadequate provision of medication counseling since patients forget more than half of the information delivered to them via oral communication.36
The work experience of pharmacy professionals was also a barrier for patient counseling (30%)27 and significant factor (AOR = 2.99) for satisfactory counseling.17 Similar findings were reported from Pakistan37 and Botswana.38 When dispensers work more and more, they are more likely to develop better counseling skills and knowledge.
Patient counseling is a vital component of pharmaceutical service delivery and involves the provision of appropriate advice and making certain that the advice is understood. In this review, four studies revealed that poor communication between pharmacy professionals and patients was a barrier for counseling (7.1–60.5%). Pharmacist communication skills (β= 0.44) were also found to be statistically associated with better communication.22 Drug dispensers should provide appropriate, understandable, and relevant medication information to patients.8 Although patients’ better understanding of medicines is critical to having better therapy,39 misunderstanding of dosage regimen was relatively higher.40 Their interaction quality can also be affected by the ascent and confidence of pharmacy professionals.26 Thus, it creates difficulty from both sides and can have adverse consequences that can demotivate patients.41
Patient factors like patients not wanting to talk much and a bad attitude toward pharmacy was reported as a barrier for 12.8–63.27% communications. The illness condition of the patient, being in a rush to leave the dispensary, and lack of willingness to listen to the counselor were major claimed barriers for smooth patient–pharmacist interaction.17 This was attributed to the poor attitude of the patient to their role in rational drug use.22
Exit knowledge of patients for dispensed drugs can show the extent of interaction between patients and dispensers. Patients who are educated were 1.97–2.71 times more likely to have satisfactory counseling than illiterate patients.17 According to World Health Organization drug use indictor, the percentage of satisfactory counseling on dispensed medicines should be 100%.42 However, more than 50% of all medicines are prescribed, dispensed or sold inappropriately.13 This inappropriate use leads to wasted resources and patient harm.43
The patient load at the dispensary was reported as a barrier for 23.8–79.5% of respondents in half of the reviewed studies. Medication counseling with smaller number of patient loads was more likely to have better satisfaction with counseling than high patient load. This was comparable with a study done in Pakistan.37 Accordingly, health centers were four times more likely to provide satisfactory counseling as compared to hospitals in Pakistan37 and Botswana.38 The reason may be due to the heavy work load of dispensers as a result of high patient flow in peak hours.16–18,23 This leads to increased risk of dispensing errors and miscommunications. Moreover, the involvement of trained clinical pharmacists in resource-limited settings leads to clinically relevant and well-accepted optimization of medicine use.30
Private health facilities were four times more likely to practice satisfactory counseling than government health facilities.17 This is due to the fact that private health facilities are often concerned about client attraction to promote and improve their market value, and continuity of care.17 Concerning the issue of legal framework in the country, 3.17–56.7% of respondents responded that the absence of a legal framework to monitor and evaluate patient counseling practice influenced patient–pharmacist interaction. The absence or limited applicability of the medicines regulatory framework distorts the execution of all regulatory functions required for effective medicine regulation.19
Although only one of the reviewed studies reported that the availability of prescribed medications was a factor for 38.9% patient–pharmacy professional interactions, in many poor African countries, 50–60% of the population lack access to medications.44 The overall average availability of essential medicines was 91% in Gonder45 and 55.65% in South West Ethiopia.46 The shortage of pharmaceuticals adversely affects the quality of health care and the condition worsens when the number of drugs stock out is more.44,47
The listed factors are not independent and the presence of one factor may trigger other and further compromise the patient–pharmacist interaction. The identified factors varied across the studies reviewed. The main reasons for this variation may be attributed to differences in social determinants of health, beliefs, and culture of the patients and pharmacy professionals, and the difference in approaches used to collect information by authors.
Based on the findings from the reviewed studies, we feel that all stakeholders will get insight into the two pillars of medication use barriers. While implementing the rules and regulations, all concerned bodies should strive to improve smoothing communication between patients and pharmacy professionals. As all of the reviewed studies used cross-sectional design, the limitation of the cross-sectional type of study will be reflected. The literature search was also limited to the aforementioned databases.
Conclusion
All studies identified various and distinct factors that distort the patient–pharmacist interaction in Ethiopia. These factors are related to barriers related to patients, pharmacy professionals, and health institutions. The listed factors are not independent and the presence of one factor may trigger other and further compromise the patient–pharmacist interaction. When the level of patient–pharmacist interaction becomes low, the knowledge of the patient on medication use decreases, resulting in poor medication outcomes. Pharmacy schools must focus on a more patient-centered curriculum to develop relevant knowledge and skills of their graduates. Improving the awareness of patients on their role in rational drug therapy and improving health institution infrastructure can foster effective communication.
Data Sharing Statement
The datasets are available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to acknowledge Wollo University and the Dessie Health Sciences College.
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Justine Nicholls CM, Braund R. Preventing drug-related adverse events following hospital discharge: the role of the pharmacist. Integr Pharm Res Pract. 2017;6:61.
2. Naughton CA. Patient-centered communication. Mdpi. Pharm. 2018; 6(1):18.
3. De Oliveira DR, Shoemaker SJ. Achieving patient centeredness in pharmacy practice: openness and the pharmacist’s natural attitude. J Am Pharm Assoc. 2006;46(1):56–66. doi:10.1331/154434506775268724
4. Allemann SS, van Mil JF, Botermann L, Berger K, Griese N, Hersberger KE. Pharmaceutical care: the PCNE definition 2013. Int J Clin Pharm. 2014;36(3):544–555. doi:10.1007/s11096-014-9933-x
5. Hirko N, Edessa D. Factors influencing the exit knowledge of patients for dispensed drugs at outpatient pharmacy of Hiwot Fana Specialized University Hospital, eastern Ethiopia. Patient Prefer Adherence. 2017;11:205. doi:10.2147/PPA.S128658
6. Sarkar BR. Progress of clinical pharmacy education and practice in Ethiopia: a review. Int J Pharm Res Health Sci. 2016;4(1):923–929.
7. Hussain A, Ibrahim MI, Malik M. Assessment of disease management of insomnia at community pharmacies through simulated visits in Pakistan. Pharm Pract (Granada). 2013;11(4):179–184. doi:10.4321/S1886-36552013000400001
8. Beardsley R. Review of Literature Oral Patient Counseling by Pharmacists Proceeding of the National Symposium on Oral Counseling by Pharmacists About Prescription Medicines. 1997:19–21.
9. Erku DA, Gebresillassie BM, Mekuria AB, Surur AS. Extent of dispensing prescription-only medications without a prescription in community drug retail outlets in Addis Ababa, Ethiopia: a simulated-patient study. Drug Healthc Patient Saf. 2016;8:65–70. doi:10.2147/DHPS.S106948
10. Dameh M, Norris P, Green J. New Zealand pharmacists’ experiences, practices and views regarding antibiotic use without prescription. J Prim Health Care. 2012;4(2):131–140. doi:10.1071/HC12131
11. Gokcekus L, Toklu HZ, Demirdamar R, Gumusel B. Dispensing practice in the community pharmacies in the Turkish Republic of Northern Cyprus. Int J Clin Pharm. 2012;34(2):312–324. doi:10.1007/s11096-011-9605-z
12. WHO. Promoting Rational Use of Medicines Core Components WHO Policy Perspective on Medicines. Vols. 1–6. Geneva: World Health Organization; 2002.
13. Johana D, Lawrence H. Important Information Regarding Medication Error Preventing and Patient Counseling, Practice Alerts and Guidelines. 2004.
14. Ni W, Colayco D, Hashimoto J, et al. Impact of a pharmacy-based transitional care program on hospital readmissions. Am J Manag Care. 2017;23(3):170–176.
15. Ni W, Colayco D, Hashimoto J, et al. Reduction of healthcare costs through a transitions-of-care program. Bull Am Soc Hosp Pharm. 2018;75(10):613–621.
16. Ayalew E, Seid Y, Agalu A. Knowledge, attitude and practice of patient medication counseling among drug dispensers in Mekele town, Northern Ethiopia. Int Res J Pharm Pharmacol. 2014;4(2):28–34.
17. Nigussie WD. Patient counselling at dispensing of medicines in health care facility outpatient pharmacies of Bahir Dar city, Northwest Ethiopia. Sci J Public Health. 2014;2(2):126–134.
18. Surur AS, Getachew E, Teressa E, Hailemeskel B, Getaw NS, Erku DA. Self-reported and actual involvement of community pharmacists in patient counseling: a cross-sectional and simulated patient study in Gondar, Ethiopia. Pharm Pract (Granada). 2017;15(1).
19. Nigussie S, Edessa D. The extent and reasons for dissatisfaction from outpatients provided with pharmacy services at two public hospitals in Eastern Ethiopia. Front Pharmacol. 2018;9:1132. doi:10.3389/fphar.2018.01132
20. Hirko N, Edessa D, Sisay M. Exit-knowledge of ambulatory patients about medications dispensed in government hospital in eastern ethiopia: the need for focused patient counseling. Front Public Health. 2018;6(254). doi:10.3389/fpubh.2018.00254
21. Wadoa TE, Gunasekarana T, Dhanaraju MD. Pharmacist–patient communication barriers in dispensing practice: a descriptive study in Adama Hospital Medical College, Adama City, Oromia regional state, Ethiopia. J Pharm Health Serv Res. 2015;6(4):219–224. doi:10.1111/jphs.12113
22. Taye Y. The Influence of Consultative Selling on Patient Satisfaction: The Case of Chain Pharmacies in Addis Ababa. 2018.
23. Wabe NT, Raju N, Angamo MT. Knowledge, attitude and practice of patient medication counseling among drug dispensers in North West Ethiopia. J Appl Pharm Sci. 2011;1(7):85.
24. Ali S, Shimels T, Bilal AI. Assessment of patient counseling on dispensing of medicines in outpatient pharmacy of tikur-anbessa specialized hospital, Ethiopia. Ethiop J Health Sci. 2019;29(6):727.
25. Diriba G, Alemkere G, Gedamu M. Assessment of patients misunderstanding regarding dosage regimen instructions at nekemte referral hospital, Ethiopia. J Fam Med. 2018;5(5):1153.
26. Gelayee DA, Birara MK. Patient medication counseling: a survey of knowledge, attitude and practice of pharmacy professionals in Gondar, North West Ethiopia. J Sci Res Pharm. 2015;4(2):74–77.
27. Belay TB, Kassa TT, Welie AG, Alemayehu MS, Dinkashe FK. Assessment of counseling practice in medicine retail outlets in Mekelle City, Northern Ethiopia. Risk Manag Healthc Policy. 2017;10:137–146. doi:10.2147/RMHP.S138300
28. Centre for Reviews and Dissemination. Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care: Centre for Review and Dissemination. York: University of York; 2009.
29. Halila GC, Junior EH, Otuki MF, Correr CJ. The practice of OTC counseling by community pharmacists in Parana, Brazil. Pharm Pract (Granada). 2015;13(4):597. doi:10.18549/PharmPract.2015.04.597
30. Mekonnen AB, Yesuf EA, Odegard PS, Wega SS. Implementing ward based clinical pharmacy services in an Ethiopian University Hospital. Pharm Pract (Granada). 2013;11(1):51. doi:10.4321/S1886-36552013000100009
31. Villako P, Volmer D, Raal A. Factors influencing purchase of and counselling about prescription and OTC medicines at community pharmacies in Tallinn, Estonia. Drug Res. 2012;69:335–340.
32. Wirth F, Tabone F, Azzopardi LM, Gauci M, Zarb-Adami M, Serracino-Inglott A. Consumer perception of the community pharmacist and community pharmacy services in Malta. J Pharm Health Serv Res. 2011;11:1759–1794.
33. Antunes LP, Gomes JJ, Cavaco AM. How pharmacist–patient communication determines pharmacy loyalty? Modeling relevant factors. Res Social Adm Pharm. 2015;11(4):560–570. doi:10.1016/j.sapharm.2014.11.003
34. Tegegn HG, Abdela OA, Mekuria AB, Bhagavathula AS, Ayele AA. Challenges and opportunities of clinical pharmacy services in Ethiopia: a qualitative study from healthcare practitioners’ perspective. Pharm Pract (Granada). 2018;16(1).
35. Alaqeel S, Abanmy NO. Counseling practices in community pharmacies in Riyadh, Saudi Arabia: a cross-sectional study. BMC Health Serv Res. 2015;15(1):557. doi:10.1186/s12913-015-1220-6
36. The American Society on Aging (ASA). The American Society of Consultant Pharmacists (ASCP) Foundation. Adult Medication: Improving Medication Adherence in Older Adults. 2006.
37. Hussain A, Ibrahim MI. Medication counselling and dispensing practices at community pharmacies: a comparative cross sectional study from Pakistan. Int J Clin Pharm. 2011;33(5):859–867. doi:10.1007/s11096-011-9554-6
38. Boonstra E, Lindbaek M, Ngome E. Labeling and patient knowledge of dispensed drugs as quality indicators in primary care in Botswana. Qual Saf Health Care. 2003;12(3):168–175. doi:10.1136/qhc.12.3.168
39. WHO. Operational Package for Assessing, Monitoring and Evaluating Country Pharmaceutical Situations: Guide for Coordinators and Data Collectors. Geneva: World Health Organization; 2007.
40. Terefe A, Chanie T. Assessment of patients misunderstanding of dosage regimen instructions among adolescent and adult outpatients in ethiopia: the case of a primary hospital. Int J Pharm Sci Res. 2014;5:446–453.
41. Teshale C, Hussein J, Mussa S. Assessment of the quality of pharmaceutical service in Jimma Zone, Oromia regional state, South West Ethiopia. Int J Pharm Teach Pract. 2004;5:60–66.
42. WHO. How to Investigate Drug Use in Health Facilities: Selected Drug Use Indicators. Geneva: World Health Organization; 1993.
43. Zewdie D, Jorge Y, Gebre Mariam T. A preliminary assessment of outpatient counseling in four referral hospitals of Addis Ababa. Ethiop Pharm J. 1999;17:44–50.
44. Deed. Defining and Measuring Accessing to Essential Medicines, Vaccines, Health Commodities; Report for WHO-MSH Constitute Meeting: Fernery Voltaire, France. 2004.
45. Fentie M, Fenta A, Moges F, et al. Availability of essential medicines and inventory management practice in primary public health facilities of Gondar Town, North West Ethiopia. J PharmSciTech. 2015;4(2):54–60.
46. Abiye Z, Tesfaye A, Hawaze S. Barriers to access: availability and affordability of essential drugs in a retail outlet of a public health center in south western Ethiopia. J Appl Pharm Sci. 2013;3(10):101–105.
47. Jitta J, Whyte SR, Nshakira N. The availability of drugs: what does it mean in Ugandan primary care. Health Policy. 2003;65(2):167–179. doi:10.1016/S0168-8510(03)00003-4
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.