")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Patient Safety Culture in Primary Healthcare Centers in the Eastern Province of Saudi Arabia
Authors Aljaffary A , Awad Albaalharith M , Alumran A , Alrawiai S , Hariri B
Received 27 August 2021
Accepted for publication 14 January 2022
Published 15 February 2022 Volume 2022:15 Pages 229—241
DOI https://doi.org/10.2147/RMHP.S336117
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Haiyan Qu
Afnan Aljaffary, Maha Awad Albaalharith, Arwa Alumran, Sumaiah Alrawiai, Bayan Hariri
Department of Health Information Management & Technology, College of Public Health, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Afnan Aljaffary, Tel +9660133338086, Email [email protected]
Purpose: This study aimed to explore health-care workers’ perceptions of patient safety culture (PSC) at primary health-care centers (PHCs) in the Eastern Province of Saudi Arabia and the factors that influence them. An additional aim was to identify the challenges of adopting PSCs in the PHCs of this region.
Methods: This is a cross-sectional study that adopted a PSC questionnaire from the Agency for Healthcare Research and Quality (AHRQ). The questionnaire was administered online and onsite targeted health-care workers at private, governmental, and quasi-governmental PHCs in the Eastern Province of Saudi Arabia, with 310 participants completing the survey.
Results: The overall positive response rate of participants to the survey areas was 43.5% which is lower than the average for the AHRQ data in general. Teamwork scored the highest positive response (68.8%) while Number of Events and non-punitive Response to Error scored the lowest at 10.6% and 30.7%, respectively. In addition, ANOVA and t-tests were used to determine the bivariate associations for the parametric variables. The study reveals statistically significant differences between all demographic variables and overall PSC score, except by age.
Conclusion: The findings highlight a number of areas for improvement, particularly in relation to event reporting, non-punitive responses, and openness in communication. Consequently, establishing a safety culture in health-care organizations necessitates the elimination of three crucial elements regarding errors: blame, fear, and silence. Error reporting should not just be considered a means of learning from mistakes; it should also be considered the first step towards preventing injury and improving patient safety.
Keywords: patient safety culture, teamwork, non-punitive response to error, hospital survey
Introduction
Patient safety is one of the main principles of healthcare. According to the World Health Organization, it can be defined as “the absence of preventable harm to a patient and reduction of risk of unnecessary harm associated with health care to an acceptable minimum”.1 As in any complex system, mistakes can occur in healthcare, and the Institute of Medicine (IOM) released “To Err is Human” in November 1999 to provide clear guidelines around how to fix systemic defects in healthcare delivery that cause patient harm.
The concept of patient safety focuses on three main strategies, namely recognizing risk, preventing harm, and mitigating mistakes.2 This study concentrates on recognizing risks and implementing proactive plans to prevent errors as having as great a potential effect as preventive efforts in public health. Since the IOM report, developing patient safety culture (PSC) has received significant attention in order to build safer health systems. If a comprehensive culture of safety is developed, in which adverse incidents can be reported without blame, individuals have the chance to learn from their mistakes and improvements can be implemented to prevent future human and system harms, thus patient safety will be promoted.
Numerous health-care organizations around the world have shown interest in the PSC concept as a means of reducing potential harm and accidents associated with routine responsibilities.3 A culture or climate of patient safety is a comprehensive and multidimensional concept; it is a component of organizational and individual behavior, beliefs, perceptions, and values. The key aim of building PSC in healthcare is to ensure safety for patients, staff, and visitors by reducing risk, promoting quality of care, improving performance, and lowering costs.
PSC is a complex phenomenon that continues to develop in hospitals worldwide, but there are limited existing studies assessing it specifically in primary health-care centers (PHCs). PHCs are considered the gateway to the healthcare system, focusing on treatment, disease prevention, and improving quality of life,4 and most patients now receive healthcare in primary care settings.5 As with international accrediting organizations, the Saudi health authorities require all health-care organizations, including PHCs, to assess PSC and disseminate to staff to the relevant standards from Joint Commission International,6 the Saudi Central Board for Accreditation of Healthcare Institutions,7 and the Saudi Patient Safety Center.8
This study was initiated, and a modified Agency for Healthcare Research and Quality (AHRQ) survey used to investigate the applicability of PSC in primary health-care settings. The aims of the research were to explore the perceptions of health-care workers about PSC and the challenges of adopting the concept in PHCs across the Eastern Region. The study also aimed to identify the factors influencing PSC at PHCs in KSA as the gateway to advanced health-care services.
Materials and Methods
Research Design
This is a cross-sectional study targeting health-care workers’ perceptions of PSC and the challenges of adopting the concept in PHCs across the Eastern Province of Saudi Arabia.
Study Setting
The questionnaire was administered online and onsite. With regard to online recruitment, the survey was shared as a Google Form with the target population through various social media applications including Telegram, Twitter, and WhatsApp, as well as via email. Using purposive sampling technique, onsite recruitment was conducted at three types of PHC in four cities located in Eastern Province of Saudi Arabia. Specifically, two governmental PHCs in Ras Tanura city, two quasi-governmental PHCs in Dhahran and Dammam cities, and two private PHCs in Dammam in AL Khobar cities. These recruitment techniques were used in order to achieve maximum variation in the study sample.
Participants
All primary health-care workers, whether clinicians, non-clinicians, administrators, or contractors, were eligible to participate in this study. The total number of participants was 310.
Variables
The independent variables were gender, education, organization type, age group, health organization type, participant’s position, and unit. The dependent variables were the 12 dimensions of the PSC questionnaire: Teamwork; Staffing and Work Pace; Organizational Learning; Non-Punitive Response to Error; Supervisor Support for Patient Safety; Communication About Error and Communication Openness; Event Reporting; Organizational Support for Patient Safety; Handoffs and Information Exchange; Number of Events; and Patient Safety Rating.9,10
The survey questions varied between requiring short answers and 5-point Likert scale responses. All questions were marked as required to ensure that none was left unanswered. Participants were moved automatically on to the next section once all questions were answered.
Data Source and Measurement
This assessment of PSC was undertaken by adopting a valid questionnaire from the AHRQ’s Surveys on Patient Safety Culture10 with some slight modifications to ensure applicability in a primary healthcare context.
Study questionnaire consisted of nine sections. The first section concerned demographic and professional information and consisted of six questions (eg, gender, age group, and educational level).
The second section concerned the unit and work area and contained 14 questions using the Likert scale (strongly agree = 5, agree = 4, neutral = 3, disagree = 2, strongly disagree = 1, 0 = Does not apply or do not know). The third section concerned the participants’ reflections on their supervisors, managers, or clinical leaders, and it consisted of three main questions using a 5-point Likert scale. The fourth section concerned communication and consisted of seven questions focused on communication between staff members, staff and their managers, and staff and those in higher authority. The fifth section concerned the reporting of safety-related incidents. The sixth section concerned the patient safety rating. In this section, the participants rated their unit/work area on patient safety using a 5-point Likert scale (from 5 = excellent working environment to 1 = poor environment). The seventh section focused on the health-care organization itself and consisted of five questions measuring the organizational culture in regard to patient safety. The eighth section contained four background questions on, for example, the working period, working hours, and staff position. The ninth and final section provided an opportunity for general comment, which was intended to add value to the study.
The Questionnaire has 13 negative worded questions, reverse coding was used for these negative items reverse coding (strongly agree = 1, agree = 2, neutral = 3, disagree = 4, strongly disagree = 5, 0 = Does not apply or do not know).
The survey questions used either short answers or a 5-point Likert scale. Moreover, all questions were marked as required, which ensured that no question was left without an answer. Participants were moved automatically from one section to another if they answered all the questions.
Bias
Online data collection has some standard challenges such as low response rates, the inability to reach older groups, unequal participant distribution, and participant fraud.11 Attempts were made to minimize this bias by conducting onsite recruitment, although recall bias is expected in both online and onsite questionnaires.
Study Size
The sample size was calculated using the rule-of-thumb advocated by Priyanath et al12 which suggests that every item in a questionnaire should be multiplied five to 10 times to determine the appropriate sample size. The selected questionnaire consists of 12 areas with a total of 35 questions, and so a sample size of 350 would be considered sufficient to produce valid results in the current study. The total number of completed questionnaires was 310.
Statistical Methods
SPSS for Macintosh (IBM Corp., Armonk, NY) was used to conduct the statistical analysis and calculate a total PSC score by computing domain results with reverse scoring for negative questions. A higher score indicates better PSC. Skewness and kurtosis criteria were used to test normality, and the results showed that all dimensions were normally distributed. Thus, t-tests and one-way ANOVA were used. Means and standard deviations were calculated from all variables in the scale, followed by ANOVA and t-tests to determine the bivariate associations for the parametric variables.
Results
As outlined in Table 1, a total of 310 respondents were included in this study (148 male, 162 female) with the largest group aged in their thirties (n = 141; 45%). Most of the participants held bachelor’s degrees (n = 165; 53.2%), and half worked in government hospitals (n = 155; 50%). Just over half of the study population were either nurses (n = 83; 26.8%) or medical professionals (n = 77; 24.8%), and most of the participants had direct interaction or contact with patients. More than half of the respondents worked in patient care or clinical units (n = 182; 58.7%).
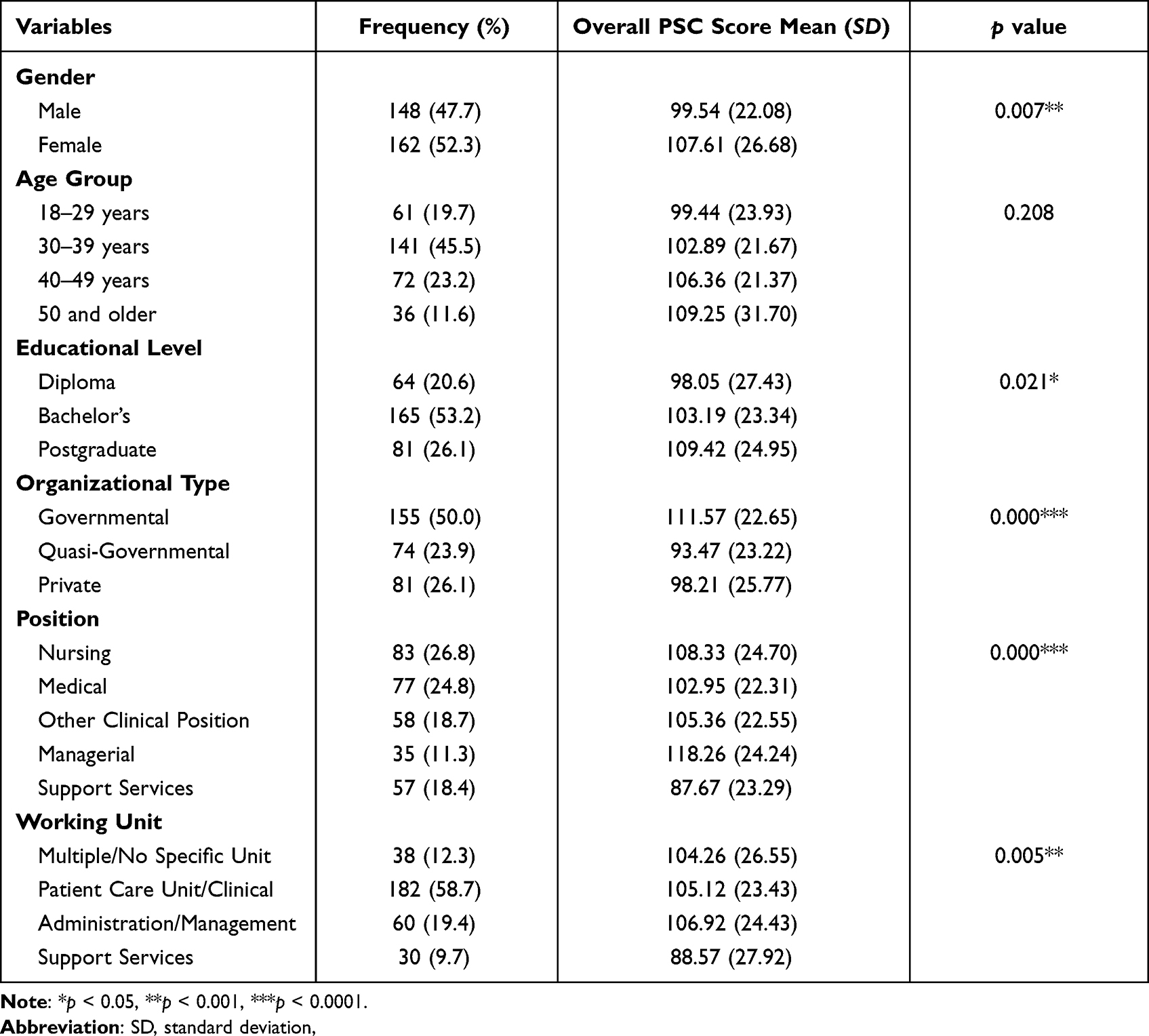 |
Table 1 Overall Patient Safety Culture Score by Demographics (n = 310) |
Table 2 presents the means and standard deviations of the PSC dimensions, all 12 of which are shown to be normally distributed with a range of skewness and kurtosis between 2 and −2.
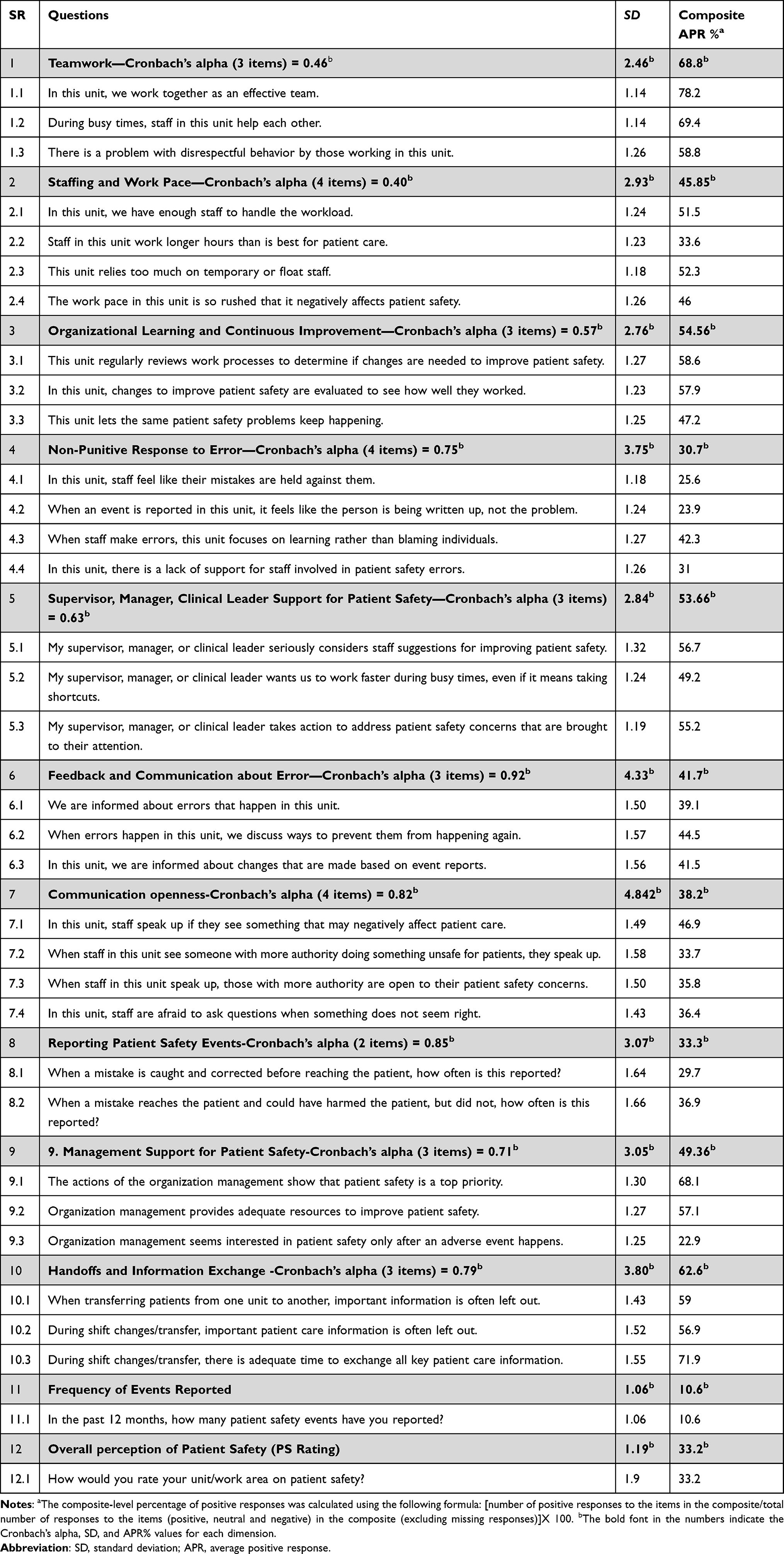 |
Table 2 Cronbach’s a and Distribution of Positive Responses for Survey Composites (n=310) |
Bivariate Analysis
As shown in Table 1, the study reveals statistically significant differences between all demographic variables and overall PSC score, except by age. Independent sample t-tests or ANOVA were conducted for each dimension to determine the factors that significantly influence each subscale.
First, gender was assessed regarding whether male or female participants differed in any of the subscales. Means and standard deviations of gender for each dimension and their significance appear in Table 3. The results show that there is a statistically significant difference between the genders in terms of PSC score (t=−2.887; P=0.007) with female respondents returning a higher average PSC score compared to the male participants.
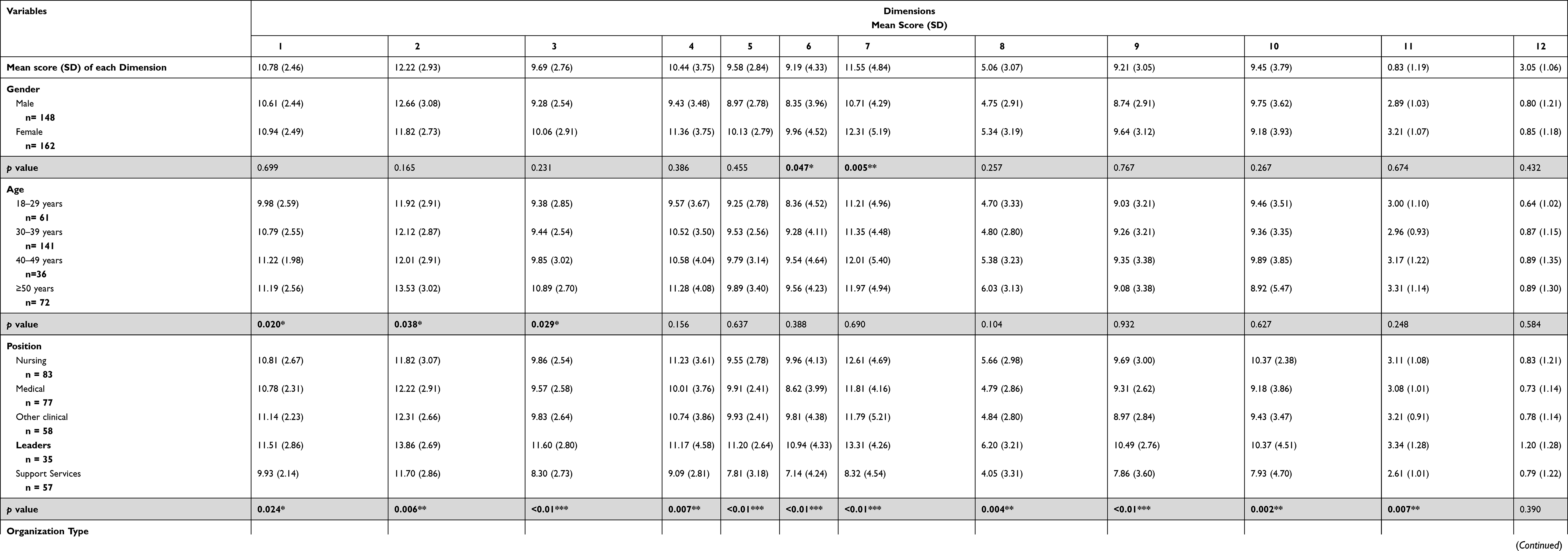 |
Table 3 Mean Scores (SD) of Patient Safety Culture Dimensions by Participant Characteristics |
More specifically, a statistically significant difference was found in Feedback About Errors (t=−3.325; P=0.047). Female participants reported a more positive perception about this dimension than their male counterparts with scores of 9.96 and 8.35, respectively. A statistically significant difference was also observed in relation to Communication Openness (t=−2.952; P=0.005) which achieved mean scores of 12.31 (female) and 10.71 (male).
Although there was no statistically significant difference between overall PSC score and age group, one-way ANOVA was conducted to investigate any differences between the 12 PSC domains and age. There was a statistically significant difference between age and teamwork (f=3.313; P=0.020) with the 40–49 group having the highest mean score (11.2; SD = 1.980). A statistically significant difference was also found between age and staffing (f=2.835; P=0.038), 40- to 49-year-olds again returning the highest mean score (13.53; SD = 3.019), and between age and organizational learning (f=3.041; P=0.029) with the highest mean score from the 40–49 group (10.89; SD = 2.702). The means and standard deviations of each age group for each dimension and their significance appear in Table 3.
Subsequently, ANOVA tests were conducted to investigate possible differences between various educational levels. The means and standard deviations and their significance are shown in Table 3. Statistically significant difference was found between education and overall PSC score (f=3.898; P=0.021). To further examine these differences, Tukey and Bonferroni post hoc tests were conducted which revealed statistically significant differences between diploma and postgraduate participants (P=0.018). Statistically significant differences were also found between educational level and “staffing and work pace dimension”, “supervisor, Managers, clinical leaders support dimension”, and “communication openness dimension”, and “Management support dimension” at f=5.852 (P=0.003); f=4.799 (P=0.009); f=3.132 (P=0.045); and f=3.302 (P=0.038), respectively.
Response variation among the different PHC types was also assessed (Table 3). A statistically significant difference was found between the type of PHC and the overall PSC score (f=17.702; P=0.000), and additional post hoc tests were used to explore this further. Statistically significant differences were found between the governmental and quasi-governmental PHCs (P= 0.000). Statistically significant differences were found between PHC type and all 12 PSC dimensions (Table 3).
As shown in Table 3, a statistically significant difference was found between different staff positions and total PSC score (f=10.966; P=0.000), and post hoc analysis revealed statistically significant differences between support services and other nursing position (P=0.000). Relatedly, ANOVA tests were conducted to investigate differences among work units (Table 3), and a statistically significant difference was observed between unit and overall PSC score (f=4.376; P=0.005). Tukey and Bonferroni post hoc tests showed statistically significant differences between participants working in support roles, in administration, and in management (P=0.005).
Ultimately, the rate of positive responses was compared between the Saudi PHCs in this study and an AHRQ benchmark, specifically 43.54% and 61%, respectively. Table 2 outlines further details about positive responses according to the 12 PSC dimensions and their related items, and Table 4 provides a comparison between the results of this study and the benchmark report that contains trending data on changes in PSC perceptions for more than 300 hospitals.13 The current results are also compared with primary health-care settings in Kuwait (Table 4).
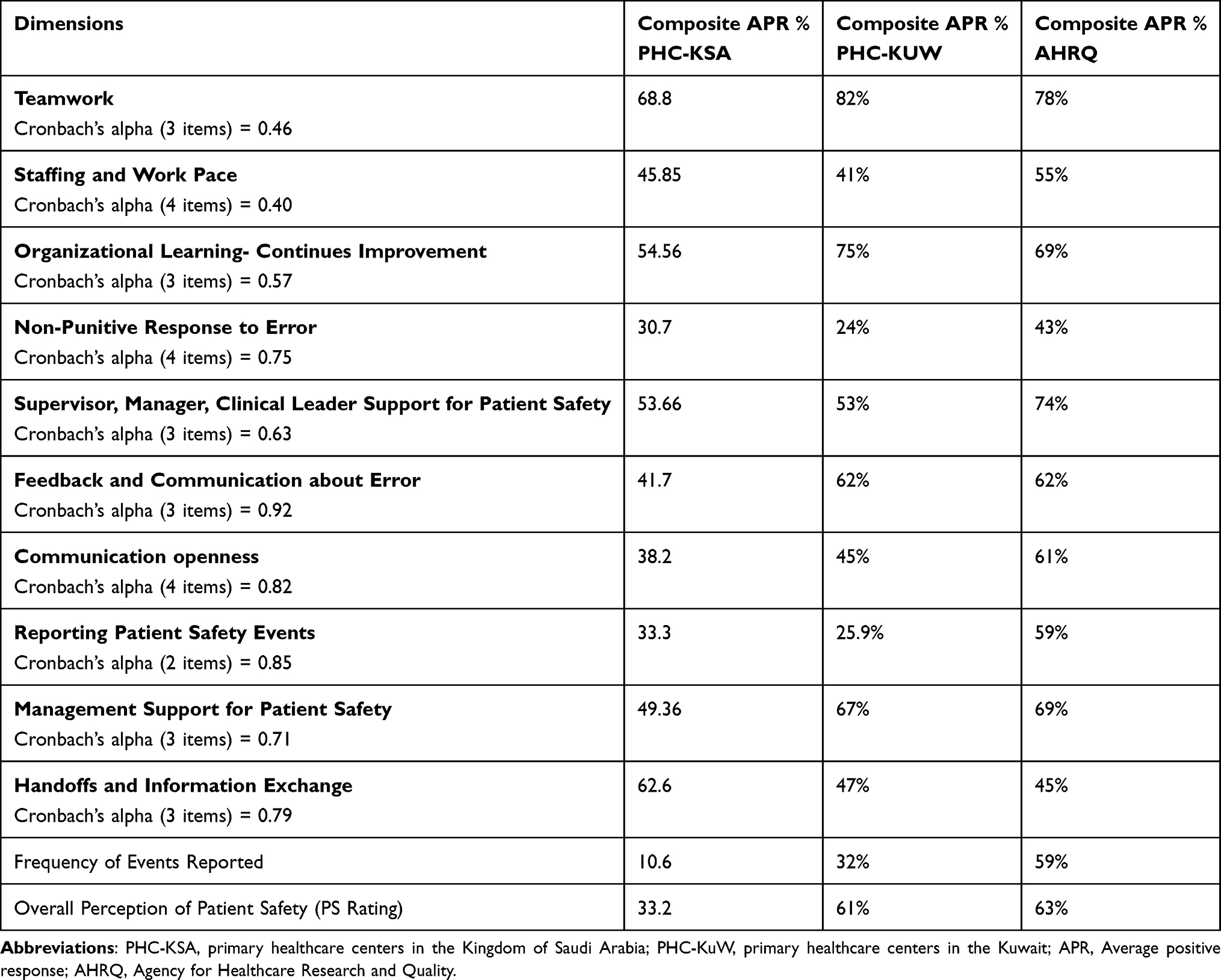 |
Table 4 Average Positive Response Rate for the PHC Results in Saudi Arabia Comparing to PHC in Kuwait and AHRQ Data (n = 310) |
Figure 1 illustrates the PSC strengths and weaknesses in Eastern Province PHCs, and is color coded to identify and prioritize areas for improvement. More specifically, green columns represent strong areas with amber and red showing where further improvement is required and where key challenges lie.
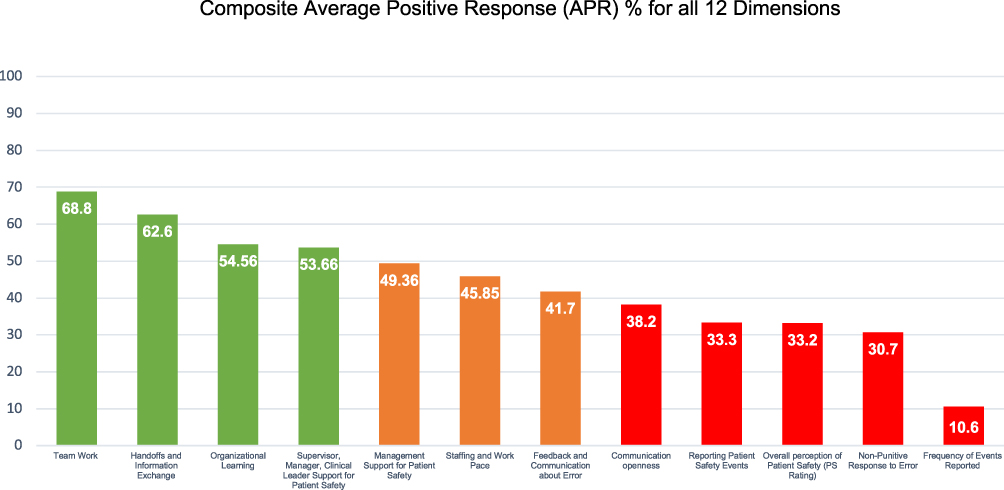 |
Figure 1 Composite average positive response (APR) % for all 12 dimensions. Notes: Illustrates the areas of strength and weakness. It is color-coded to clearly present the areas requiring improvement. AHRQ scoring system was used for the study results, High rating domains (above 75% of positive responses) are shown in green columns and representing areas of strength in PSC, medium rating domains (50% to 75% of positive responses) are shown in amber columns and representing the areas that need further improvement in PSC, and low rating domains (below 50% of positive responses) are shown in red columns and representing the challenging areas in PSC. |
Discussion
This study aimed to explore health-care workers’ perceptions of PSC at PHCs in the Eastern Province of Saudi Arabia, to investigate the challenges of implementing PSC in these settings, and to provide recommendations to help overcome these barriers. Regarding workers’ perceptions, the results of this study demonstrate that positive responses about all PSC dimensions are lower in this region than the average positive response rate for the AHRQ data and lower than similar studies conducted at PHCs in Arab countries such as Yemen and Oman.14,15
Furthermore, the results show that areas of strength in Eastern Province PHCs can be found in Teamwork and in Handoffs and Information Exchange which is consistent with existing findings.16 This accord might be because of the common availability of clear policy and a mandated communication tool, specifically the Situation, Background, Assessment, Recommendation approach, which has been proven to reduce adverse events, improve communication skills among health-care workers, and promote patient safety.17
On the other hand, the participants rated five PSC dimensions with particularly low positivity, namely Number of Events, Non-Punitive Response to Error, Event Reporting, Patient Safety Rating, and Communication Openness. These negatively viewed and interconnected dimensions can be considered a bottleneck in adopting PSC and show how support from organizational leaders is a crucial factor in implementing PSC in health-care settings. A recent study conducted in a teaching hospital in Saudi Arabia revealed similar results to the current study regarding low rating of Non-Punitive Response to Error.18 This finding is also consistent with outcomes of previous studies that describe the importance of organizational leadership in building the cultural principle of balancing safety and staff accountability.14,19,20
According to the IOM, most care errors result from human mistakes, but these mistakes are themselves mostly stimulated by systemic deficiencies that set individuals up to fail.20 In spite of the consequences that will follow an adverse event, establishing such a culture can help empower the health-care workers to proactively monitor their environment, discover the hidden pain points that have the potential to be improved, and make the care system more reliable before the patient is impacted (near miss). In turn, this will increase the frequency of event reporting.21–23
Regarding the factors influencing overall perceptions of PSC, this study has revealed statistically significant differences between gender and PSC score with male health-care workers returning a significantly lower score than their female colleagues. The results also demonstrate that educational level has a significant influence on workers’ perceptions in that those with postgraduate degrees report a more positive view of PSC compared to others with lower levels of education. This finding is consistent with an integrative review that indicated increased care hours and skills are related to improved patient safety, although evidence specifically linking education level remains sparse.24
Despite the different regulations, visions, finances, and management between the private and public sectors, patient safety is a top priority for any health-care organization. Each area has its own challenges and potency in terms of being able to improve and maintain safety. Interestingly, the results of this study show statistically significant differences between the PSC perceptions of those working in governmental, quasi-governmental, and private PHCs with those at quasi-governmental organizations returning lower scores than those at government or private centers. This may be the result of strong investment in regarding quality of care and patient safety by the Saudi Ministry of Health in its PHCs compared with private and quasi-governmental centers.
Another notable result is the statistically significant difference in overall PSC score between staff position and work unit with workers in support services having the lowest positive perception of PSC and managers the highest. Similar results were presented following a study conducted in Virginia hospitals.25 This shows that there is significant variance in PSC perspective across positional levels in that managers and administrators report the highest scores. Moreover, non-clinicians tend to return lower PSC scores which may be because managers understand the safety issues and appreciate that those at the frontline of patient care are best qualified to solve them.26 It is important the health-care leaders and managers have full awareness of the organizational PSC strategy to be able to work proactively towards it and mitigate any risks to quality and safety of care.25
Limitations
This study was carried out in the Eastern Province of KSA with other regions excluded. Its scope should therefore be extended in future studies. Furthermore, online data collection usually involves challenges around low response rates, reaching older age groups, unequal participant distribution, recall bias, and participant fraud.11 Onsite recruitment was used to minimize these issues.
Conclusion
To our knowledge, this is the first study to modify the AHRQ’s Hospital Survey on Patient Safety Culture for use in Saudi Arabia and across all PHC sectors.
The key finding is that PSC at PHCs in the Eastern Province has a very low overall positive response from health-care professionals, and a number of areas for improvement have been highlighted in the reporting of safety events, non-punitive responses to errors, and openness in communication. As a result, it can be said that establishing a safety culture in any health-care organization would necessitate the elimination of three crucial elements: blame, fear, and silence. Error reporting should not be considered solely as a means of learning from mistakes but also as the first step towards preventing injury and improving patient safety.
The current findings are comparable to national and international benchmarks and demonstrate that routine evaluation can help hospitals better understand changes in performance and identify areas for development.
Recommendations
The study’s findings suggest three main recommendations for Saudi health policy to help improve PSC at PHCs. Firstly, a leadership commitment to safety is required, and this can include developing structural documents to guide regular monitoring and updating (ie, policies, procedures, plans, and guidelines); comprehensive staff training and education about the PSC concept and how to maintain it within health-care organizations; and frequent location walks to assess organizational resources and their ability to change.27
Secondly, employee involvement is required. Managers and staff should work together to develop comprehensive and continuous training plans that will ensure each person’s involvement in building a shared culture of safety. More specifically, training should include how to recognize, report, and think critically about fixing a problem without fear of penalty or stigma at its core.28
The final recommendation is to utilize digital health developments and consider medical devices and interfaces as crucial factors in supporting patient safety. In this technological age, health-care organizations need to expand their services and, for example, launch virtual platforms to facilitate collaboration between professionals within or across different facilities. Many studies have found that the emergent role of human factors engineering in healthcare delivery can improve the working conditions and minimize the medical errors related to adverse events.29,30
Abbreviations
KSA, Kingdom of Saudi Arabia; PSC, Patient safety culture; PHC, Primary Healthcare Centre; AHRQ, Agency for Healthcare Research and Quality; IOM, Institute of Medicine; IRB, Institute Review Board.
Data Sharing Statement
The research study data are available upon request from authors.
Ethical Approval and Informed Consent
Ethical approval for this study was obtained from the Institutional Review Board of the Imam Abdulrahman Bin Faisal University-Dammam (IRB-PGS-2021-03-004). All of the participants provided online informed consent. Participants were requested to confirm that they are aged 18 or above and willing to participate in the study before having access to the questionnaire questions. To ensure privacy and confidentiality, the collected data was kept in an electronic database accessible only to the investigators. The survey was anonymous and no identifiable information was obtained from the participants.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Patient safety. Clin Ther. 2020;42(4):551–553. doi:10.1016/j.clinthera.2020.02.019
2. Donaldson MS. An overview of To Err is Human: re-emphasizing the message of patient safety. In: Patient Saf Qual an Evidence-Based Handb Nurses; 2008:20894. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21328772.
3. Cooper MD. Towards a model of safety culture. Saf Sci. 2000;36(2):111–136. doi:10.1016/S0925-7535(00)00035-7
4. Agarwal R. Importance of primary health care in the society. Int J Health Sci (Qassim). 2017;1(1):5–9. doi:10.21744/ijhs.v1i1.17
5. Shi L. The impact of primary care: a focused review. Scientifica (Cairo). 2012;2012:1–22. doi:10.6064/2012/432892
6. Joint Commission International. Joint Commission International Accreditation Standards for Hospitals; 2015.
7. Saudi Central Board for Accreditation of Healthcare Institutions. National Hospital Standards; 2019.
8. Saudi Patient Safety Center. Hospital Survey on Patient Safety Culture National Project in the Kingdom of Saudi Arabia; 2021:2021.
9. Paese F, Dal Sasso GTM. Cultura da segurança do paciente na atenção primária à saúde. Texto Context Enferm. Patient Safety Culture in Primary Health care. 2013;22(2):302–310. doi:10.1590/S0104-07072013000200005
10. Surveys on Patient Safety Culture™. Rockville, MD USA: Agency for Healthcare Research and Quality. Available from: https://www.ahrq.gov/sops/index.html.
11. Rice S, Winter SR, Doherty S, Milner M. Advantages and disadvantages of using internet-based survey methods in aviation-related research. J Aviat Technol Eng. 2017;7(1):58–65. doi:10.7771/2159-6670.1160
12. Ranatunga RV, Priyanath HM, Megama RG. Methods and rule-of-thumbs in the determination of minimum sample size when applying structural equation modelling: a review. J Soc Sci Res. 2020;15:102–107. doi:10.24297/jssr.v15i.8670
13. AHRAQ. Hospital survey on patient safety culture: user comparative data based report; 2014. Available from: www.ahrq.gov.
14. Webair HH, Al-Assani SS, Al-Haddad RH, Al-Shaeeb WH, Bin Selm MA, Alyamani AS. Assessment of patient safety culture in primary care setting, Al-Mukala, Yemen. BMC Fam Pract. 2015;16(1):1–9. doi:10.1186/s12875-015-0355-1
15. AL Lawati MH, Short SD, Abdulhadi NN, Panchatcharam SM, Dennis S. Assessment of patient safety culture in primary health care in Muscat, Oman: a questionnaire-based survey. BMC Fam Pract. 2019;20(1):1–8. doi:10.1186/s12875-019-0937-4
16. Alahmadi HA. Assessment of patient safety culture in Saudi Arabian hospitals. Qual Saf Health Care. 2010;19(5):1–5. doi:10.1136/qshc.2009.033258
17. Shahid S, Thomas S. Situation, background, assessment, recommendation (SBAR) communication tool for handoff in health care – a narrative review. Saf Health. 2018;4(1):21–22. doi:10.1186/s40886-018-0073-1
18. Aljaffary A, Al Yaqoub F, Al Madani R, Aldossary H, Alumran A. Patient safety culture in a teaching hospital in Eastern Province of Saudi Arabia: assessment and opportunities for improvement. Risk Manag Healthc Policy. 2021;14:3783–3795. doi:10.2147/RMHP.S313368
19. Ghobashi MM, El-ragehy HAG, Mosleh H. Assessment of patient safety culture in primary health care settings in Kuwait. Epidemiol Biostat Public Health. 2014;11(3):1–9. doi:10.2427/9101
20. Al-Mandhari A, Al-Zakwani I, Al-Kindi M, Tawilah J, Dorvlo ASS, Al-Adawi S. Patient safety culture assessment in Oman. Oman Med J. 2014;29(4):264–270. doi:10.5001/omj.2014.70
21. Elton M, Band G, Falkenstein M. To err is human. Biol Psychol. 2000;51(2–3):83–85. doi:10.1016/S0301-0511(99)00035-6
22. Boysen PG. Just culture: a foundation for balanced accountability and patient safety. Ochsner J. 2013;13(3):400–406.
23. Kohn LT, Corrigan JM, Molla S. Rapporteur’s report session 1: origin of the problem: Malcolm Ross. Regul Toxicol Pharmacol. 2008;52:S40–S42. doi:10.1016/j.yrtph.2007.09.017
24. Ridley RT. The relationship between nurse education level and patient safety: an integrative review. J Nurs Educ. 2008;47(4):149–156. doi:10.3928/01484834-20080401-06
25. Hartmann CW, Rosen AK, Meterko M, et al. An overview of patient safety climate in the VA. Health Serv Res. 2008;43(4):1263–1284. doi:10.1111/j.1475-6773.2008.00839.x
26. Kobuse H, Morishima T, Tanaka M, Murakami G, Hirose M, Imanaka Y. Visualizing variations in organizational safety culture across an inter-hospital multifaceted workforce. J Eval Clin Pract. 2014;20(3):273–280. doi:10.1111/jep.12123
27. Institute of Medicine (US) Committee on the WE for N and PS. Keeping Patients Safe: Transforming the Work Environment of Nurses.
28. Shehu M, Subramaniam C, Johari J. The effect of safety training and workers involvement on healthcare workers safety behavior: the moderating role of consideration of future safety consequences. Int J Bus Manag. 2016;1(2):46–81.
29. Carayon P. Emerging role of human factors and ergonomics in healthcare delivery - A new field of application and influence for the IEA. Work. 2012;41(SUPPL.1):5037–5040. doi:10.3233/WOR-2012-0096-5037
30. Global Ministerial Summit on Patient Safety. Jeddah declaration on patient safety. Ministry of Health; 2019. Available from: www.moh.gov.sa.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.