")
Back to Journals » Drug, Healthcare and Patient Safety » Volume 13
Patient Safety Culture and Associated Factors Among Health-Care Providers in the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia
Authors Ayisa A, Getahun Y, Yesuf N
Received 13 November 2020
Accepted for publication 18 June 2021
Published 2 July 2021 Volume 2021:13 Pages 141—150
DOI https://doi.org/10.2147/DHPS.S291012
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rajender R Aparasu
Aynalem Ayisa, Yalemwork Getahun, Nurhussien Yesuf
Department of Surgical Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Aynalem Ayisa
Department of Surgical Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, P. O. Box 196, Gondar, Ethiopia
Tel +251918 04 6090
Email [email protected]
Introduction: Patient safety is an issue of global concern; however, health-care organizations have lately observed to pay more attention to the importance of establishing a culture of safety. The study aimed to assess the level of patient safety culture and associated factors among health-care providers at the University of Gondar comprehensive specialized hospital, Northwest Ethiopia, 2020.
Methods: A cross-sectional study design supported by the qualitative approach was conducted from March 15 to May 15/2020. A stratified simple sampling technique was used to select 575 study participants. The standardized tool, which measures 12 safety culture dimensions, was used for data collection. Bivariate and multivariable linear regression analyses performed using SPSS version 23. The significance level was obtained at 95% CI and p-value < 0.05. For the qualitative part, a semi-structured interview guide with probing was used. Data were analyzed thematically using open code software version 4.02.
Results: The overall level of positive patient safety culture was 45.3% (95% CI: 44.7, 45.9) with a response rate of 92.2%. Factor analysis indicated that female, masters, participation in patient safety program, adverse event report, hospital management encourage reporting event and resource were positively associated with the patient safety culture. Whereas divorced/widowed, midwives, anesthetist, medicine, pediatrics, emergency, outpatient, pharmacy, direct contact with patients, and hospital management blame when medical errors happened were negatively associated. The in-depth interview revealed that teamwork, health-care professionals’ attitude toward patient safety and patient involvement as important factors that influence patient safety culture.
Conclusions and Recommendations: The overall level of positive patient safety culture was low. All variables except age, training, working hour, and working experience were factors significantly associated with the patient safety culture. Health-care policy-makers and managers should consider patient safety culture a top priority, and also create a blame-free environment that promotes event reporting.
Keywords: patient safety, patient safety culture, health care providers, Ethiopia
Introduction
Patient safety culture (PSC) is defined as the values shared among organizational members about what is important, what are their beliefs about how things operate in the organization; and the interaction of this with work unit, organizational structure and system, which together produce behavioral norms that promote safety.1,2
Patient safety is an issue of global concern, but health-care organizations around the world have lately observed to pay more attention to the importance of establishing a culture of safety.3
The major complications that happened to patients are ascribed to poor patient safety owing to poor health-care management rather than by the patient’s underlying disease; and it is likely to be one of the 10 leading causes of death and disability.4 Major medical practices and risks associated with patient safety are medication errors, healthcare-associated infections, unsafe surgical care procedures, unsafe injections practices, diagnostic errors, sepsis, unsafe transfusion practices, radiation errors, and unsafe care in mental health.5–13
A cross-sectional study was done in Yemen, Sri Lanka, Oman, south India, Riyadh, Upper East region of Ghana, and Tunisia, showed that the overall patient safety culture ranged from 50–67%, while 20.13%was in Egypt.14–22 In Ethiopia studies conducted on Nurses showed that the overall patient safety culture ranged from 44%-58%.23–27
Different studies revealed that socio-demographic characteristics such as age, gender, work experience, and educational status significantly affected patient safety culture.23,28–30 Regarding work-related influencing factors; patient involvement, participation in the patient safety program, and reporting adverse drug reaction are important factors that influence patient safety culture.24,26,31 Organizational factors like leadership style, accreditation status, and infrastructure can affect patient safety culture.32–34
A meta-analysis study showed that teamwork within unit, non-punitive response to error, safety perception, management support, supervisor/manager expectations, organizational learning–continuous improvement, staffing, handoffs transitions and teamwork across units were strongest the patient safety culture.35,36
Therefore, this study aimed to assess patient safety culture and influencing factors among nurses working at Gondar University comprehensive specialized hospital Northwest Ethiopia.
Methods
Study Design and Period
An institutional-based cross-sectional study design supported by a qualitative approach was conducted from March 15 to May 15/2020.
Exclusion Criteria
Health-care providers, who had worked less than six months in the hospital, were excluded from the study.
Sample Size Determination
The sample size was calculated with using a single population proportion formula, but since the outcome variable was continuous, to calculate the sample size, the standard deviation was used, where n is the required sample size.
By considering the possible non-response rate, during the final sample size increased by 10%. Therefore,  .
.
In this study, the standard deviation for calculating the sample size was taken from a study in Bale Zone Hospital, Southeast Ethiopia.26
A semi-structured in-depth interview was continued based on the saturation theory. The sample sizes were determined based on a theoretical saturation-the point in data collection when new data no longer bring additional insights to the research questions.
Sampling Procedure and Technique
A stratified simple random sampling technique was employed to select a representative sample of health-care providers from each disciplinary team. A purposive sampling technique was used to select participants for the qualitative study.
Data Collection Tool and Procedure
The Hospital Survey on Patient Safety Culture (HSOPSC) was used to collect quantitative data on patient safety culture which was originally developed, pilot-tested, and revised by Westat in the USA and then released by the Agency of Healthcare Research and Quality (AHRQ).37 In this study, the Cronbach’s alpha for the composites was 0.849. For the qualitative part Face-to-face in-depth interview was conducted by using a semi-structured open-ended question, and for more detailed information additional probing questions were used (Supplementary File).
Data Processing and Analysis
Data were entered, cleaned, and coded using Epi-info version 7.2.1.0 and exported to SPSS Version 23. Composite level scores were computed by summation of the items within the composite scales and dividing by the number of items with non-missing values. Furthermore, bivariate analysis was performed and a variable with p-value ≤0.20 was exported to multivariable linear regression analysis. The significance level was obtained at 95% CI and p-value <0.05. For qualitative data, thematic analysis of the interview was performed using the open code software version 4.02.
Result
Of the total 575 questionnaires distributed, 530 completed and valid questionnaires were returned, which gives a response rate of 92.2%.
Socio-Demographic Characteristics of Respondents
Nearly two-third, 334 (63.0%) of the participants were males. The mean age with the standard deviation of the respondents was 29.4 (4.9) years and the age of the study participants ranged from 22 to 58 years.
Three hundred nine (58.3%) of the respondents were single. Concerning to educational status, 305 (57.5%) of the respondents had a bachelor’s degree, and the majority, 215 (40.6%) of the respondents were nurses (Table 1).
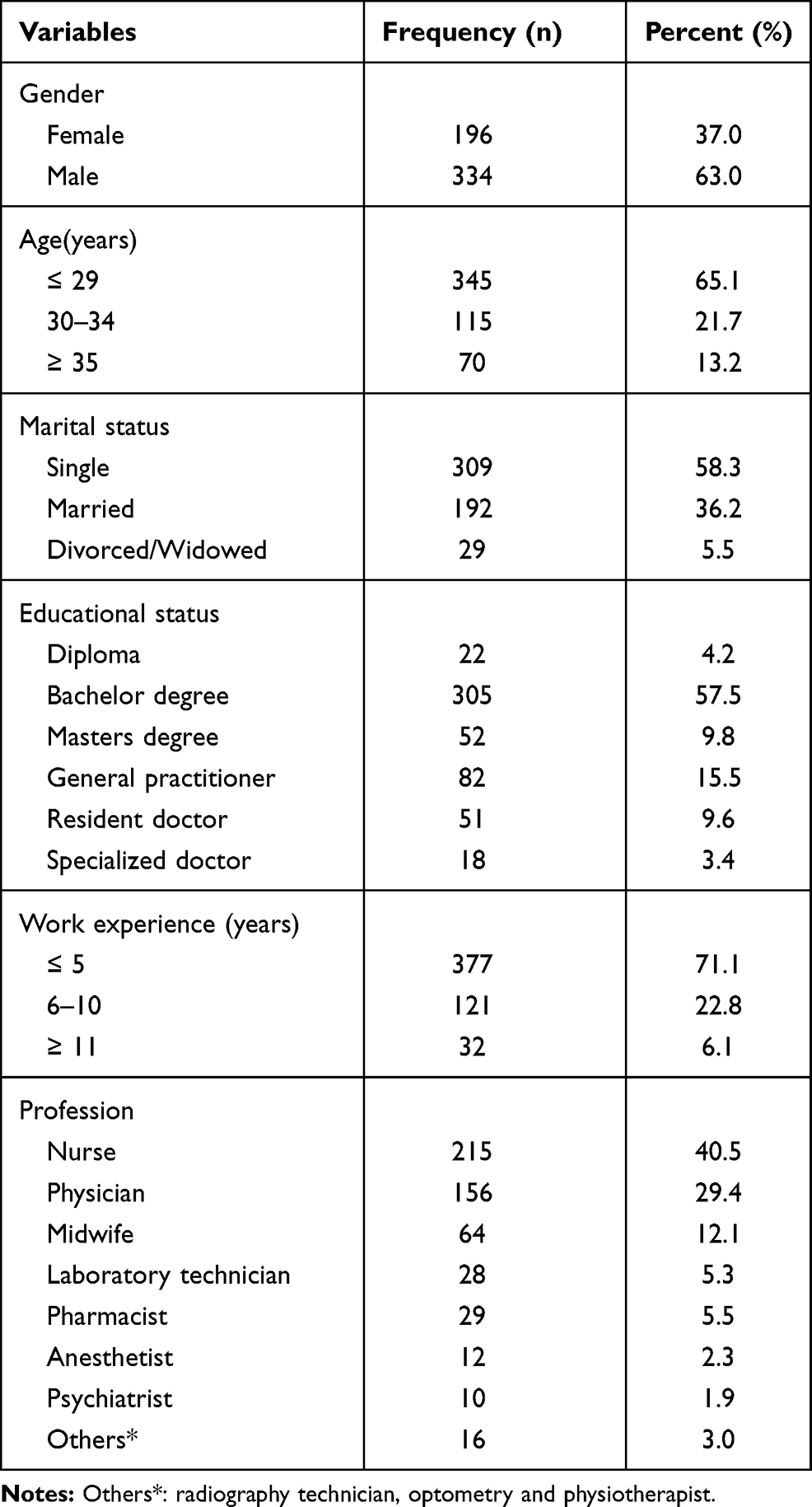 |
Table 1 Socio-Demographic Characteristics of the Study Participants, 2020 (N= 530)* |
For the qualitative study, a total of 8 health-care professionals were successfully interviewed. The participants were 2 female and 6 male professionals, all who had direct patient contact. The average age of participant was 34 years old (range 30–48 years) and their work experience was an average of 9 years (range 5–20 years).
Work-Related and Organizational Characteristics of Study Participants
Among the study participants, 94 (17.7%) of them work at the surgery department, followed by Maternity 87 (16.4%) and internal medicine department 80 (15.1%).
The majority, (83.6%) of the study participants have direct contact with the patients in the course of their work. Only, 95 (17.9%) of respondents reported they have participated in the patient safety program. More than two-thirds (70.2%) of study participants have reported adverse events.
Patient Safety Grade
According to this study, 7.2% and 22.1% of the respondents rated the patient safety grade as excellent and very good, respectively. Among participants, 39.6% of respondents rated patient safety grade as acceptable, while 17.7% and 13.4% of respondents rated the patient safety grade as poor and falling, respectively.
Patient Safety Culture
The overall level of positive patient safety culture was 45.3% (95% CI: 44.7, 45.9).
The dimension with the highest average percentage of positive responses was teamwork within the unit (75%). While the area with the most potential for improvement and the lowest average percentage positive response was feedback and communication about the error (27%).
All composite scores of dimensions were less than 50% except “teamwork within the unit” (75%) and “Organizational Learning Continuous Improvement” (65.3%) (Table 2).
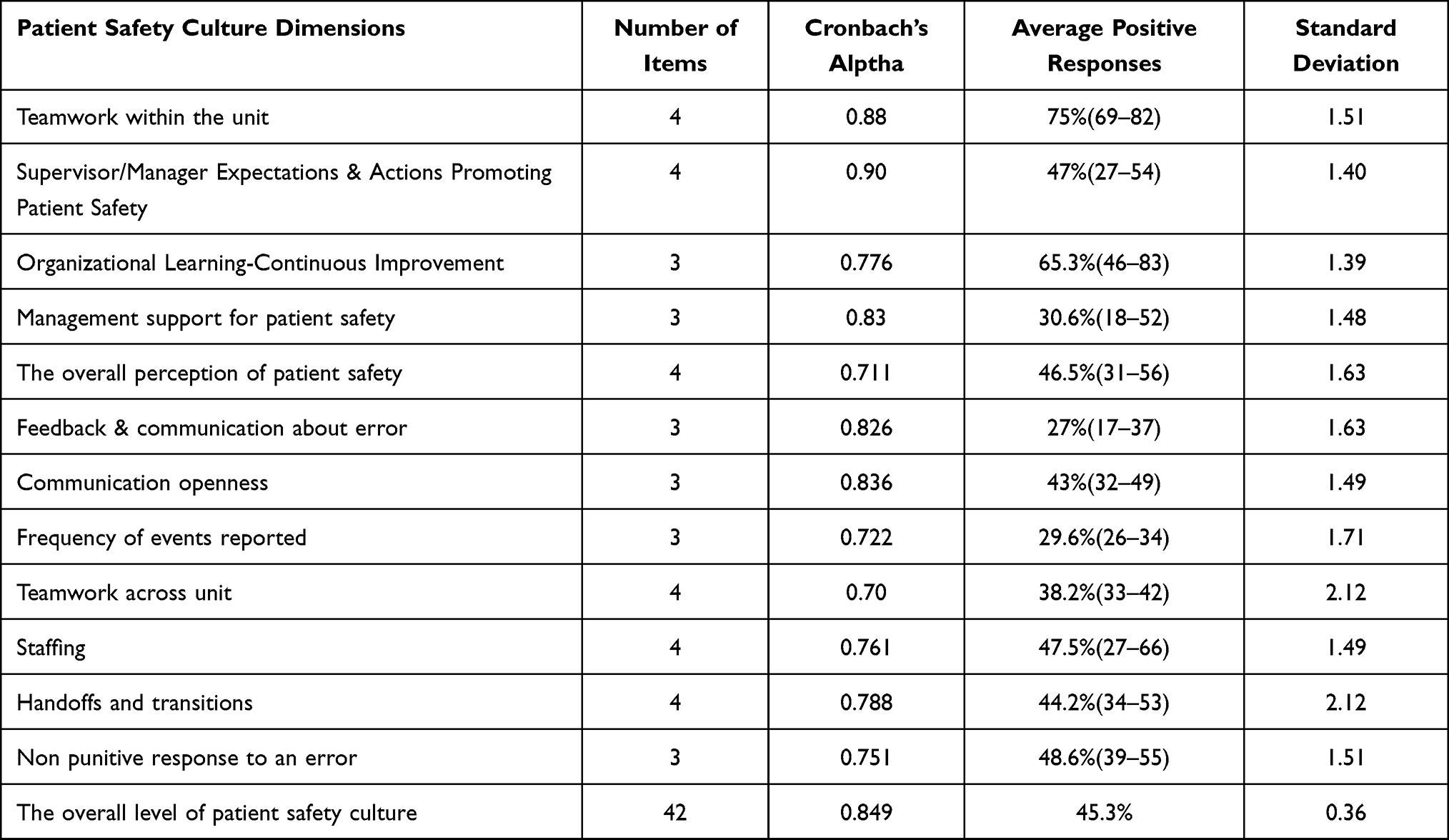 |
Table 2 Patient Safety Culture Composite Level Results (N= 530) |
Factors Associated with Patient Safety Culture
Bivariate analysis showed that all variables except age and training were found to be significantly associated with the patient safety culture.
The enter method was employed in multivariable analysis, then work experience and working hours were insignificant, while the rest of the factors were found to be significantly associated with patient safety culture (Table 3).
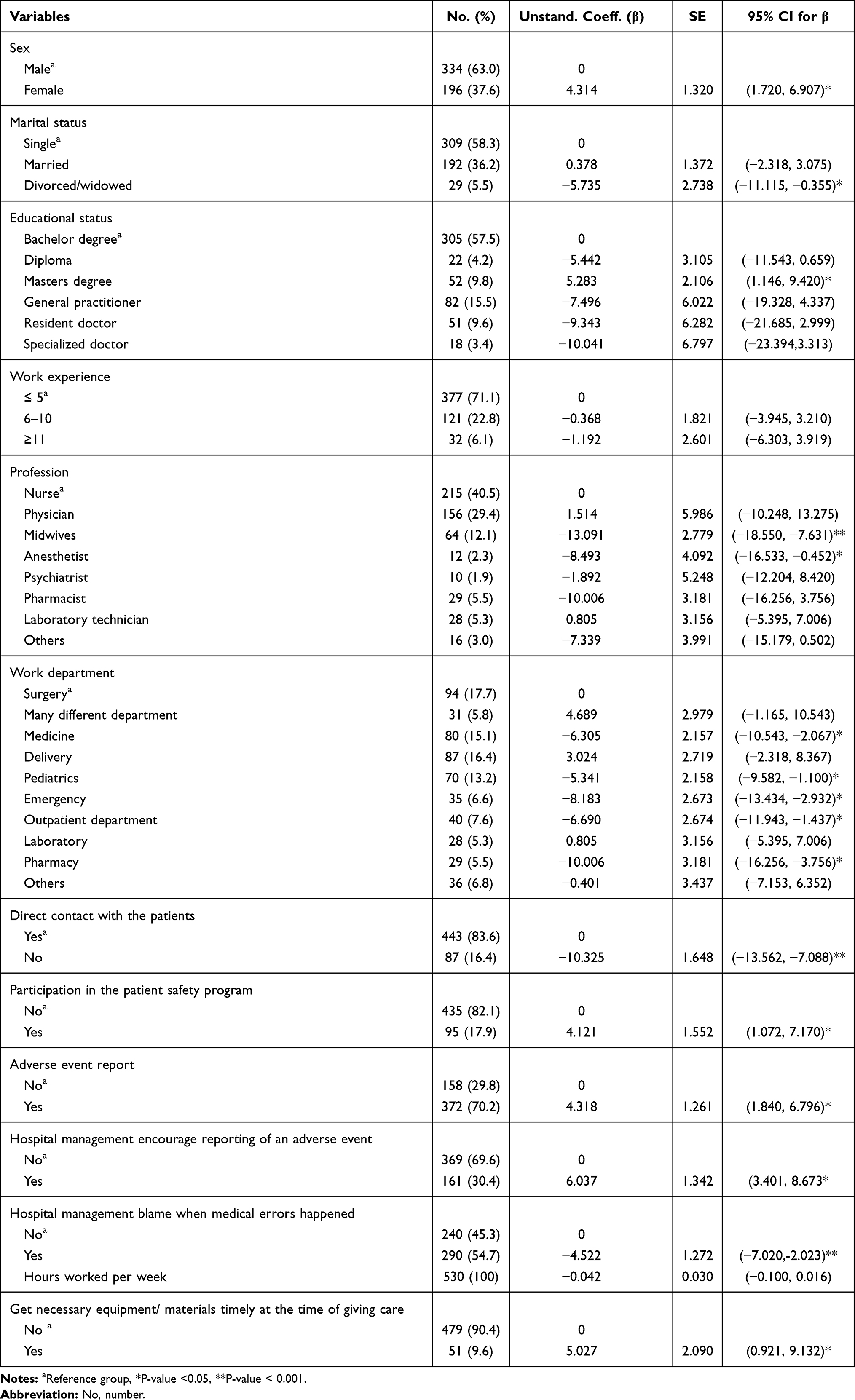 |
Table 3 Adjusted Variables Associated with Patient Safety Culture (Multivariable Linear Regression Analysis) (n=530) |
Among study participants, being female was found to have higher patient safety culture by 4.3.
Study participants who were divorced/widowed found to have lower patient safety culture by 5.735 when compared to single respondents.
Those HCPs who were master’s degree holders have higher patient safety culture score by 5.283 than those HCP’s with a bachelorette degree. From the qualitative study also it is evidenced that teaching quality improvement issues and patient safety standards are factors for the success of establishing a patient safety culture in the hospital.
Educational status improvement and developing patient safety standards are also factors for the success of establishing a patient safety culture in hospitals but we work very little to educate and empower people even if this is so important. (p3)
Anesthetists and midwives were the only two disciplines that reported statistically different PSC scores and these were lower (−8.493 and −13.091, respectively) than other work categories Emergency department and pharmacy department were the only two working area that reported statistically different PSC scores and these were lower (−8.183 and −10.006, respectively) than other working units.
… …The nurse to patient ratio is low, especially around the emergency room, so there is the workload on the professionals. Working in these stressful situations makes the culture of patient safety poor. (P5)
As a teaching hospital, students not only in Medicine but also in other professions will have ward attachment and bedside teaching. In this case, many students may take a test on a patient, and a physical examination may be performed. At this time, many patients are unwilling because they get bored when asked all day, and working in such a crowded environment can seriously damage a culture of patient safety among health care providers. (p7)
The study participants who have indirect contact with the patients reported a statistically lower adjusted score of −10.325. Conversely, staff who had participated in a patient safety education program had a statistically higher adjusted score (4.12) than respondents who had not participated in the patient safety program. Reporting an event/error either orally or in written form increases the score of patient safety culture by 4.318 keeping other constant. This result was supported by an in-depth interview. Interviewee believed that reporting hospital errors, and summarizing and analyzing them is a crucial task:
Knowing which one of our mistakes is related to which group or which segment, or in which shifts we have the most errors, we can apply, analyze, and use them in making decisions, and preventing them from repeating. (P1)
In contrast, another interviewee stated that because of being afraid of getting fired and criticized they were not eager to report an event.
Personnel are not willing to report errors since they think they will be punished and fired if they report it. (P3)
Those respondents whose management encourage reporting was found to improve patient safety culture by 6.037. Those respondents whose management blame when medical errors happened were found to decrease the score of PSC by 4.522.
HCPs who get necessary equipment and materials timely at the time of giving care were found to improve the score of PSC by 5.027 keeping other constant. This result is supported by a qualitative part. Participants described a shortage of supply and equipment as factors that hinder patient safety culture.
Although the hospital is serving a large community, many important tests are done from private clinics, and even medicines and basic items such as clean gloves are being bought from private clinics. There is nothing less than a clean glove. (P4)
… …It lacked a lot of features, such as a screen, charts that should have been placed in separate locks, but if we look at the charts in each room, we see that they are in a place where everyone can access them. (P6)
From the qualitative study different factors influencing the PSC was raised. The factors influencing patient safety culture as perceived by health-care professionals were thematically categorized as organizational factors, health-care provider factors, and patient-related factors.
Organizational Factors
Respondents stated that the event reporting system is an essential component by health-care providers to improve learning culture and then patient safety culture.
The institution or hospital, in turn, makes conditions in terms of providing resources, providing frequent training to professionals, developing guidelines, and developing a system of reporting an adverse event. In this regard, I think we can grow it as a culture or continue it. (P2)
Health Care Provider’s Factor
Participants stated that conflict between professionals and poor teamwork negatively affects patient safety culture. The collaboration of health professionals and respecting each other is an important factor. Some respondents reported a lack of collaboration between HCPs looked like a factor or barrier to improving patient safety culture due to hierarchical differences.
Teamwork is especially important for patient safety. When we say treatment, it is not the result of one specialist: medical doctors, nurses, anesthesiologists, midwives, pharmacists, laboratory technicians, and others should collaborate. But there is a hierarchical difference between them something like despising one another which can reduce the spirit of teamwork. As a result, this leads to a huge impact on the patient’s well-being. (P1)
… … If doctors and pharmacists work closely together and clinical pharmacists go to the ward and discuss with the doctor about the medicines that are prescribed to patients, they will have a better treatment outcome. (P8)
The low attitude of health-care professionals toward patient safety was reported to affect patient safety culture. Respondents accented the perception of health professionals on patient safety as very low. Among professionals, the lack of openness also affects patient safety culture.
If we care for the patient’s well-being, we will be faithful to our oaths and promises, and if we always put ourselves in the patient’s place and feel the patient’s pain, the safety of the patient will not be lost on our conscience for a moment. (P4)
Safety things are still seen as a burden, and it is not cool to speak up about them. Therefore, there should be transparency among professionals to develop a patient safety culture. (P2)
Patient-Related Factors
Participants stated that the role of the patient is very important. Patient education, interaction with patients, and their involvement in the treatment process are significant issues in improving patient safety culture.
Patients may be affected by their problems, especially those who do not know exactly what services they need and do not follow the instructions given by medical professionals. (P1)
The patient must first know the rights and obligations when he or she enters the hospital. He or she must be well-informed. One of the primary problems is the patient does not receive the necessary information. (P6)
Generally, providing enough human resources and medical equipment, running comprehensive educational programs, improving communication and team working, and improving medical error reporting, and by removing existing difficulties and providing required infrastructures, health-care professionals will improve the quality of care and patient safety culture by decreasing adverse events as described by respondents.
Discussion
In this study, the overall level of patient safety culture was found to be 45.3% (95% CI: 44.7, 45.9).
The overall level of the patient safety culture of this study is lower when compared with the study reported 67% in Yemen,14 62.7% in Sri Lanka,15 58% in Oman,16 58% in South India,17 and 58.1% in the upper east region of Ghana.20 This difference might be due to the differences in organizational behavior between countries. Those nations may have higher administration values, organizational commitments, leadership, and relationships inside hospital staff.
The overall level of the PSC of this study is also lower when compared with the study reported 46.7% in Jimma,24 and 46% in Amhara.25 This might be due to the difference in the number of hospitals they included.
The overall level of the PSC of this study is higher when compared with the study conducted in Addis Ababa,23 and Bale Zone hospital of Ethiopia.26 This might be due to the difference in the study setting and the small sample size.
In this study “teamwork within the department” and “organizational learning” dimensions were the area of the highest average positive response rate. This result is concordant with the finding from Jimma Zone,24 Amhara region,25 Bale region,26 Oman,16 and Yemen.14
Although there is good teamwork within departments, this result is in line with the finding of a qualitative study in two East African hospitals.34
The areas with the most potential for improvement in this study area were “feedback and communication about error” and “frequency of event reporting” with an average positive response rate of 27% and 29.6%, respectively. These results were supported by studies done in Jimma,24 Amhara,25 Tunisia,21 Oman,16 and Sri Lanka15 but received a higher rating in Iran.18
In the present study, overall patient safety grade (excellent and very good) was 29.3% which is lower than the study conducted in Addis Ababa 35.7%,25 and Bale Zone hospitals of Ethiopia which found 38.3%.26 This study showed that 22.9% of respondents reported at least one event over the past year. This finding is lower than reports from Jimma Zone,24 SNNPR hospitals,27 and Riyadh.19 This might be due to inadequate training in safety-related issues and encourage reporting errors.
Being female was found to improve the score on patient safety culture by 4.31. This might be biological; females have more sensitivity about others’ wellbeing and when they faced a stressful situation are more likely to respond by socializing, bonding with others, and seeking protection and nurturance within the community.30
In this study, participants who were divorced/ widowed found to decrease the score of PSC by 5.735 compared to single respondents. This might be people who undergo divorce face a variety of psychological issues including increased stress, lower life satisfaction, and depression. So this negatively affects the patient safety culture of HCP.
Those HCPs who were master’s degree holders have higher patient safety culture score by 5.283 than those HCP’s with bachelor's degrees. This result is also supported by an in-depth interview. An advanced education contributes to risk reduction, evidence-based practice, and knowledge of the healthcare environment, leadership, accountability, and professionalism.
The overall score of PSC was found to have decreased by 13.091 and 8.493 for every profession of midwives and anesthetists, respectively, compared to respondents who were nurses. This might be due to stressful workplace and high patient flow.
Indirect contacts with the patients were found to decrease the score on patient safety culture by 10.325 keeping other constant. This result might be due to health professionals who have indirect contact with patients who may not have the ability to quickly understand the patient’s feelings.
Participating in the patient safety program increases patient safety culture score by 4.121. This result is in line with the study reported in Jimma24 and Bale.26 This result might be explained as the staff used more times on patient safety issues in the patient safety program, this state of affairs favors them to deal extra with patient safety culture.
Reporting an event/error either orally or in written form increases the score of patient safety culture by 4.318. This result is also supported by the qualitative finding, in which respondents believed reporting an event has a positive impact on patient safety culture. This finding is in line with the result reported in Jimma24 and Bale.26 This might be due to the truth that event reporting systems preserve relevant information that is necessary to analyze events after the fact and helps to develop a fact-based, appropriate plan to mitigate the hazards and prevent them from, so it provides an opportunity to improve the PSC.
In this study, hospital management encourages reporting event was found to improve PSC by 6.037. This result is in line with the study reported in Bale.26 When people work in areas where there is proper encouragement, induced sense of effectiveness, and insight, and the tasks are well understood, the duties and policies are well explained, the new and diverse approaches come up, and the work environment would be pleasant and desirable.
Limitation of That Study
This study was conducted only on public hospital; therefore, the result cannot apply to other settings.
Also this study included only health-care providers. But the patient safety culture may be affected by Para-medical staff.
Conclusion
The overall level of patient safety culture at the University of Gondar Comprehensive Specialized Hospital was low.
Educational status, working department, adverse event report, hospital management blame when medical errors happened, and get necessary equipment and material at the time of giving care were supported by the qualitative finding.
While teamwork, health-care professional attitude toward patient safety, and patient involvement were additional variables explored as important factors that influence patient safety culture during in-depth interviews.
Abbreviations
AHRQ, Agency of Healthcare Research and Quality; AIDS, Acquired Immune Deficiency Syndrome; CRC, Compassionate and Respectful care; FMOH, Federal Ministry of Health; HSOPSC, Hospital survey on patient safety culture; ICU, Intensive Care Unit; VIF, variance inflation factor; PSC, Patient Safety Culture; WHO, World Health Organization.
Data Sharing Statement
To keep the participants’ confidentiality, the raw data would not be shared. But, they are available from the corresponding author on reasonable request and the summary data are available in the main document.
Ethics Approval
Ethical clearance was obtained from the ethical review committee of the School of Nursing on behalf of the institutional review board of the University of Gondar with reference no. S/N 2012/06/2012 and was approved on 10/06/2012E.C. A permission letter was obtained from the University of Gondar comprehensive specialized hospital management office. The purpose of the study was explained to the participants. Informed written consent was obtained from the participants. Privacy and confidentiality of information given by each respondent were kept properly and personal identifiers were removed. The participant informed consent included publication of anonymized responses, and that this study was conducted in accordance with the Declaration of Helsinki. For the qualitative study recording, the interviews were taken after permission from participants had been taken. The privacy and identity of participants were protected and participants’ confidentiality was also assured through omitting participants’ names informed consent form. Also, the phone number and email address of the principal investigator were provided that could help participants to ask questions related to ambiguous or unclear aspects of the study, before agreeing to participate. The hard copy of the recorded data and all the interviewers’ notes had been kept in a private place to be accessed by only the principal investigator.
Acknowledgments
The authors would like to thank the study participants for their valuable information.
Author Contributions
All authors made substantial contributions to conception and design, analysis and interpretation of data; took part in drafting the article; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be account for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Rasmussen K, Pedersen AHM, Pape L, Mikkelsen KL, Madsen MD, Nielsen KJ. Work environment influences adverse events in an emergency department. safety. 2014;7:8.
2. Achakzai H. Research proposal for assessing patient safety culture in public hospitals under the Essential Package of Hospital Services (EPHS) in Afghanistan. 2014.
3. Wang X, Liu K, You L-M, et al. The relationship between patient safety culture and adverse events: a questionnaire survey. Int J Nurs Stud. 2014;51(8):1114–1122. doi:10.1016/j.ijnurstu.2013.12.007
4. Panagioti M, Stokes J, Esmail A, et al. Multimorbidity and patient safety incidents in primary care: a systematic review and meta-analysis. PLoS One. 2015;10(8):e0135947. doi:10.1371/journal.pone.0135947
5. Aitken M, Gorokhovich L. Advancing the responsible use of medicines: applying levers for change. Available at SSRN 2222541. 2012.
6. Organization WH. Report on the Burden of Endemic Health Care-Associated Infection Worldwide; 2011.
7. Lives SSS. WHO Guidelines for Safe Surgery 2009. Geneva: World Health Organization; 2009.
8. Jha AK, Larizgoitia I, Audera-Lopez C, Prasopa-Plaizier N, Waters H, Bates DW. The global burden of unsafe medical care: analytic modelling of observational studies. BMJ Qual Saf. 2013;22(10):809–815. doi:10.1136/bmjqs-2012-001748
9. Singh H, Meyer AN, Thomas EJ. The frequency of diagnostic errors in outpatient care: estimations from three large observational studies involving US adult populations. BMJ Qual Saf. 2014;23(9):727–731. doi:10.1136/bmjqs-2013-002627
10. Fleischmann C, Scherag A, Adhikari NK, et al. Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations. Am J Respir Crit Care Med. 2016;193(3):259–272. doi:10.1164/rccm.201504-0781OC
11. Janssen M, van Hoeven L, Rautmann G. Trends and Observations on the Collection, Testing and Use of Blood and Blood Components in Europe 2001–2011 Report. Strasbourg: Council of Europe; 2015.
12. Shafiq J, Barton M, Noble D, Lemer C, Donaldson LJ. An international review of patient safety measures in radiotherapy practice. Radiother Oncol. 2009;92(1):15–21. doi:10.1016/j.radonc.2009.03.007
13. Thibaut B, Dewa LH, Ramtale SC, et al. Patient safety in inpatient mental health settings: a systematic review. BMJ Open. 2019;9(12):e030230. doi:10.1136/bmjopen-2019-030230
14. Webair HH, Al-Assani SS, Al-Haddad RH, Al-Shaeeb WH, Selm MAB, Alyamani AS. Assessment of patient safety culture in primary care setting, Al-Mukala, Yemen. BMC Fam Pract. 2015;16(1):136. doi:10.1186/s12875-015-0355-1
15. Amarapathy M, Sridharan S, Perera R, Handa Y. Factors affecting patient safety culture in a tertiary care hospital in Sri Lanka. Int J Sci Technol Res. 2013;2(3):173–180.
16. Al-Mandhari A, Al-Zakwani I, Al-Kindi M, Tawilah J, Dorvlo AS, Al-Adawi S. Patient safety culture assessment in Oman. Oman Med J. 2014;29(4):264. doi:10.5001/omj.2014.70
17. Rajalatchumi A, Ravikumar TS, Muruganandham K, et al. Perception of patient safety culture among health-care providers in a tertiary care hospital, South India. J Nat Sci Biol Med. 2018;9(1):14. doi:10.4103/jnsbm.JNSBM_86_17
18. Sharif MR, Motaghi M, Farrokhian A. Assessment of patient safety culture in viewpoints of Kashan Hospitals nurses 2016. Int J Med Res Health Sci. 2016;5(11):9–16.
19. El-Jardali F, Sheikh F, Garcia NA, Jamal D, Abdo A. Patient safety culture in a large teaching hospital in Riyadh: baseline assessment, comparative analysis and opportunities for improvement. BMC Health Serv Res. 2014;14(1):122. doi:10.1186/1472-6963-14-122
20. Akologo A, Abuosi AA, Anaba EA, Kamolz L-P. A cross-sectional survey on patient safety culture among healthcare providers in the Upper East region of Ghana. PLoS One. 2019;14(8):e0221208. doi:10.1371/journal.pone.0221208
21. Cheikh AB, Bouafia N, Mahjoub M, Ezzi O, Nouira A, Njah M. Patient’s safety culture among Tunisian healthcare workers: results of a cross sectional study in university hospital. Pan Afr Med J. 2016;24. doi:10.11604/pamj.2016.24.299.8466
22. Mahran SM, Ibrahim S. Patient safety culture and application of medication safety rules as perceived by nurses. Am J Nurs Sci. 2016;5(2):52–58. doi:10.11648/j.ajns.20160502.13
23. Mulugeta TT. Patient safety culture among health workers in Addis Ababa regional Hospitals, Ethiopia.
24. Wami SD, Demssie AF, Wassie MM, Ahmed AN. Patient safety culture and associated factors: a quantitative and qualitative study of healthcare workers’ view in Jimma zone Hospitals, Southwest Ethiopia. BMC Health Serv Res. 2016;16(1):495. doi:10.1186/s12913-016-1757-z
25. Mekonnen AB, McLachlan AJ, Brien J-AE, Mekonnen D, Abay Z. Hospital survey on patient safety culture in Ethiopian public hospitals: a cross-sectional study. Saf Health. 2017;3(1):11. doi:10.1186/s40886-017-0062-9
26. Kumbi M, Hussen A, Abate Lette SN, Morka G. Patient safety culture and associated factors among health care providers in Bale Zone hospitals, southeast Ethiopia: an institutional based cross-sectional study. Drug Healthc Patient Saf. 2020;12:1. doi:10.2147/DHPS.S198146
27. Ejajo T, Arega A, Batebo B. Measuring the current patient safety culture in public general hospitals of Southern Nations Nationalities and Peoples Region (SNNPR), Ethiopia: perspective of health care workers. J Fam Med. 2017;4(5):1124.
28. Nordin A, Theander K, Wilde-Larsson B, Nordström G. Health care staffs’ perception of patient safety culture in hospital settings and factors of importance for this. Open J Nurs. 2013;3(8):28–40. doi:10.4236/ojn.2013.38A005
29. Ricklin ME, Hess F, Hautz WE. Patient safety culture in a university hospital emergency department in Switzerland–a survey study. GMS J Med Educ. 2019;36:2. doi:10.3205/zma001222
30. Seppala E. Are Women More Compassionate Than Men. The Greater Good Science Center; 2013.
31. Danielsson M, Nilsen P, Rutberg H, Årestedt K. A national study of patient safety culture in hospitals in Sweden. J Patient Saf. 2019;15(4):328. doi:10.1097/PTS.0000000000000369
32. Nygren M, Roback K, Öhrn A, Rutberg H, Rahmqvist M, Nilsen P. Factors influencing patient safety in Sweden: perceptions of patient safety officers in the county councils. BMC Health Serv Res. 2013;13(1):52. doi:10.1186/1472-6963-13-52
33. El-Jardali F, Dimassi H, Jamal D, Jaafar M, Hemadeh N. Predictors and outcomes of patient safety culture in hospitals. BMC Health Serv Res. 2011;11(1):45. doi:10.1186/1472-6963-11-45
34. Aveling E-L, Kayonga Y, Nega A, Dixon-Woods M. Why is patient safety so hard in low-income countries? A qualitative study of healthcare workers’ views in two African hospitals. Global Health. 2015;11(1):1–8. doi:10.1186/s12992-015-0096-x
35. Simsekler MCE, Qazi A, Alalami MA, Ellahham S, Ozonoff A. Evaluation of patient safety culture using a random forest algorithm. Reliab Eng Syst Saf. 2020;204:107186. doi:10.1016/j.ress.2020.107186
36. Reis CT, Paiva SG, Sousa P. The patient safety culture: a systematic review by characteristics of hospital survey on patient safety culture dimensions. Int J Qual Health Care. 2018;30(9):660–677. doi:10.1093/intqhc/mzy080
37. Sorra J, Nieva VF. Hospital survey on patient safety culture: agency for healthcare research and quality. 2004.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.