")
Back to Journals » Journal of Pain Research » Volume 15
Patient Perspectives on the Appropriate Use of Prescribed Opioids in Chronic Non-Malignant Pain: Analysis of Online Forums Using Theoretical Domains Framework
Authors Alenezi A , Yahyouche A , Paudyal V
Received 18 January 2022
Accepted for publication 10 April 2022
Published 30 May 2022 Volume 2022:15 Pages 1567—1583
DOI https://doi.org/10.2147/JPR.S357354
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Timothy Atkinson
Aziza Alenezi, Asma Yahyouche, Vibhu Paudyal
University of Birmingham, School of Pharmacy, Institute of Clinical Sciences, Birmingham, B15 2TT, UK
Correspondence: Asma Yahyouche, School of Pharmacy, Institute of Clinical Sciences, University of Birmingham, Edgbaston, Birmingham, B15 2TT, UK, Tel/Fax + 44121 415 8798, Email [email protected]
Purpose: In view of concerns about the harmful effects of long-term use and patient misuse of opioids in chronic non-malignant pain, this study provides insight into patients’ perspectives on their experience of living with chronic non-malignant pain (CNMP), prescribed opioid use, and optimisation.
Patients and Methods: Data were collected from active UK-based CNMP specific or general health forums that do not require registration, with more than 100 members. English written thread posts between 2016 and 2020 were systematically searched from the forum search bar using different keywords and then analysed using the Theoretical Domains Framework (TDF).
Results: Findings showed that chronic pain is a dominant, life-altering experience with physical, psychological and social impact. Findings highlighted that opioid optimisation is facilitated by patients’ knowledge and understanding, practical coping strategies and supportive relationships with healthcare providers and others in their surroundings. The study found that barriers to opioid optimisation included lack of availability of alternatives, difficulties accessing health services and broken relationships with clinicians.
Conclusion: Analysis of CNMP patients’ posts on online forums highlighted the devastating impact of pain on social functioning, relationships and mental health. Patients emerged as knowledge seekers prepared to engage in opioid optimisation.
Keywords: chronic non-malignant pain, medication optimisation, patient perspective, prescribed opioids, theoretical domains framework, qualitative study
Introduction
Medicine optimisation is crucial for the management of chronic non-malignant pain (CNMP). It is defined as a “person-centred approach to safe and effective medicines use, to ensure people obtain the best possible outcomes from their medications.1” Patient-centred principles allow greater contributions by patients to their treatment and promote greater satisfaction with healthcare, as well as maintaining productive patient-provider relationships.2
Guidelines discourage long-term opioid therapy as its effects on CNMP is uncertain, and usually associated with harm including diversion, addiction, overdoses, and death.2 Moreover, Busse et al evaluated the evidence on opioid efficacy by reviewing 96 randomized control trials (RCTs) of opioids’ effects for CNMP and found that opioids provide no benefit compared to placebo, ibuprofen or acetaminophen in pain improvements, other physical and social functioning, as well as no changes in emotional or role functioning. Also, opioids were connected to the increase of negative side effects when compared to placebo.3
The North American opioid crisis of overdose death has been soaring over the past years. Even though the majority of overdose deaths were caused by illegally made fentanyl, prescribed opioids were responsible for 28% of deaths in the United States in 2019.4 With the increased use of prescribed opioids in England, attributed deaths have risen, particularly in areas with higher deprivation.5
In the UK, over five million people each year are diagnosed with CNMP, ie, pain lasting over three months.6,7 It affects patients’ emotional and social wellbeing and the overall quality of life.8 There are significant impacts on patients, families, and carers, as 50% of CNMP patients experience depression, and 66% are unable to work. Patients with CNMP are sometimes considered “intractable” because they fail to respond to repeated surgery or medications or their pain may even worsen. CNMP management is challenging and dissatisfaction among patients reaches up to 60%.9 Patients have reported frustration and ineffective communication with healthcare professionals about opioids and pain management.10 Healthcare providers may be constrained in meeting patients’ expectations due to inaccessibility of alternatives and limited knowledge of CNMP.9 In the UK, not all CNMP patients have access to specialist pain services. A national audit in 2012 indicated that only 40% of pain clinics had a physiotherapist, psychologist and physician, resulting in poor patient outcomes due to unrelieved pain and high healthcare system utilization.11 CNMP patients are driven by the need for pain relief and quality of life improvement. However, their interaction with healthcare providers can be complicated and stressful. Lack of a definitive diagnosis and precise treatment plan lead to unsatisfactory outcomes and poor pain control, with patients often resorting to self-medication and diversion as coping strategies.12,13 These patients’ suffering is multidimensional as they struggle from the their conditions and the misunderstanding with surroundings. Because pain is such a personal experience, the patient’s perspective should be highlighted.14 There is need for an investigation of their struggles related to managing their conditions in an era of pressure on the medical society for prescribed opioid optimisation (reduction or tapering), as evidence indicates that opioids’ harms outweigh the benefit in managing CNMP.
Despite the importance of patient-centred care, little is known about barriers and enablers to optimising prescribed opioids for CNMP from patients’ perspectives. This study was conducted to gain insight from patients’ forums into patients’ experiences of CNMP management and to address this gap in the literature.
Rationale for the Study
Several studies have analysed online forums to explore the nature of forum interaction and patients’ perspectives in relation to their condition experience and online support.15–17 They offer distinctive insight into the experiences of contributors as they chat about topics without researcher influence. Therefore, material from online forums can be deemed as practically authentic natural data.18–20
Aim
The study aims to identify the barriers and enablers to the use of chronic opioid therapy from CNMP patients’ perspectives.
Method
This research utilized a qualitative study design based on analysing the views of CNMP patients who are prescribed opioids, using posts on online forums. The research is innovative in its focus on patients via online discussion forums.
Online forums are websites where users post messages about different issues, looking for health, emotional and informational support. They are a valuable source of data as they are places of free expression without pressure from the medical profession.18–20 Search, data extraction and categorization were undertaken by the primary researcher, AA. Using several keywords, chronic pain health forums and general health forums were systematically identified through the Google and Bing search engines (see Appendix 1). Websites were then screened following the criteria listed in Table 1. Four online support groups were identified: two specifically dedicated to chronic pain and two with forums for various conditions, including chronic pain. One of these forums was excluded as it prohibited any reproduction of posts, even for research use. Relevant sections and threads were defined using the forums’ internal search, using keywords based on previous reviews (See Appendix 1). To enable systematic representation of the forum discussions, a few pages of search results per forum were reviewed, excluding any post before 2016, surveys, advertisements, or links (See Figure 1). Only posts posted by CNMP patients who were either current or former prescribed opioid users were included. Threads posted between January 2016 and December 2020 were downloaded and copied into Microsoft Word, organized according to the keywords and sub keywords. For example, pain medication was sub-categorized into Tramadol, codeine, oxycodone. Due to the extensive volume of data retrieved, the record of 360 threads was divided into two corpora to make the data more manageable (See Data Analysis, below): 237 threads in corpus 1 and 123 threads in corpus 2. Both corpus 1 and corpus 2 were analysed in the same way, applying the same definitions of the TDF dimensions, and in reporting sub-themes, relevant items from both were considered. The data were analysed until saturation, defined as a point where no new perspectives could be detected with enough quotes that represented the same perspective.
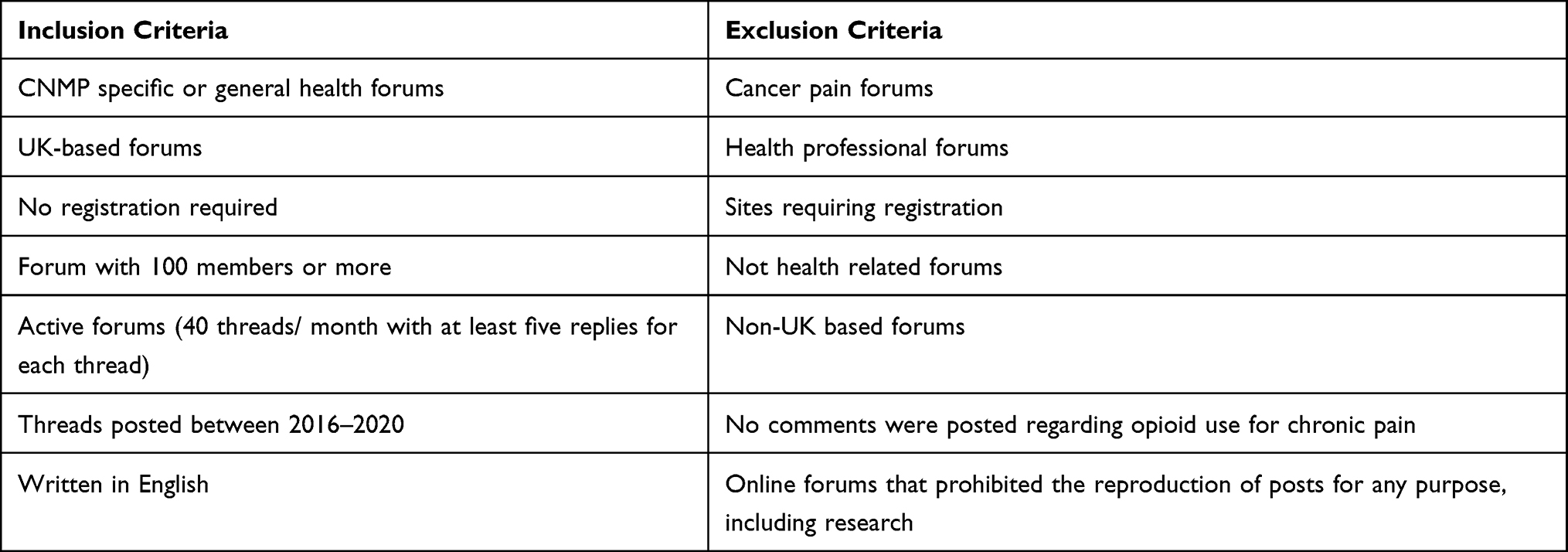 |
Table 1 Forums’ Inclusion and Exclusion Criteria |
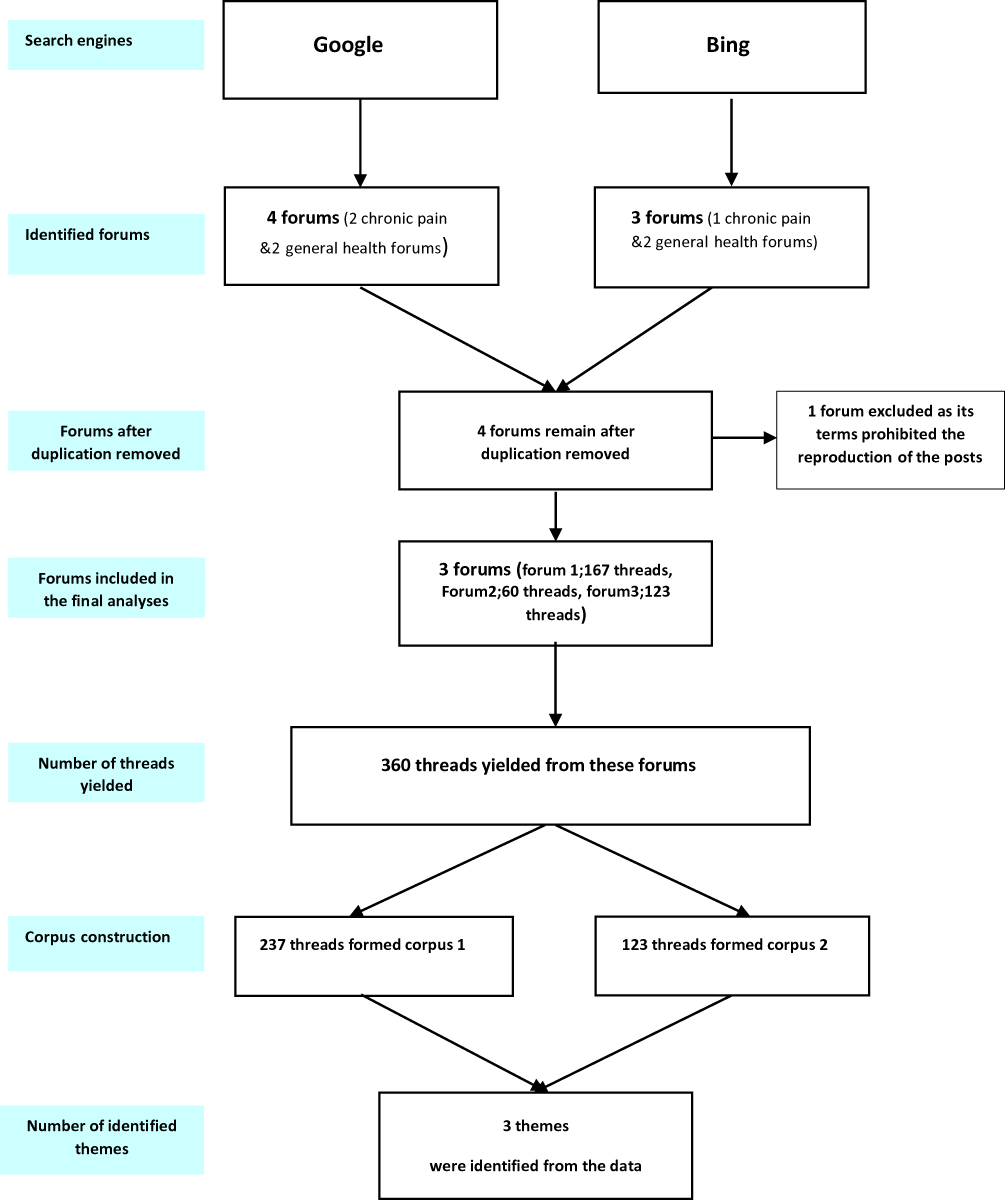 |
Figure 1 Flowchart of online forums and threads search process. |
Data Analysis
The development of the Theoretical Domains Framework (TDF) from a synthesis of psychological theories has helped apply theoretical approaches to behaviour change interventions. TDF domains represent environmental, cognitive, and social factors that may affect behaviour.21–23 The TDF has been widely used to understand behaviours and implementation challenges in various settings and content areas in health care.24 It was used in this study as an analytical tool to assist in identifying and classifying relevant posts from the patient forums. Table 2 shows the 14 domains of the TDF with their definitions and indicates their application to the forum data.
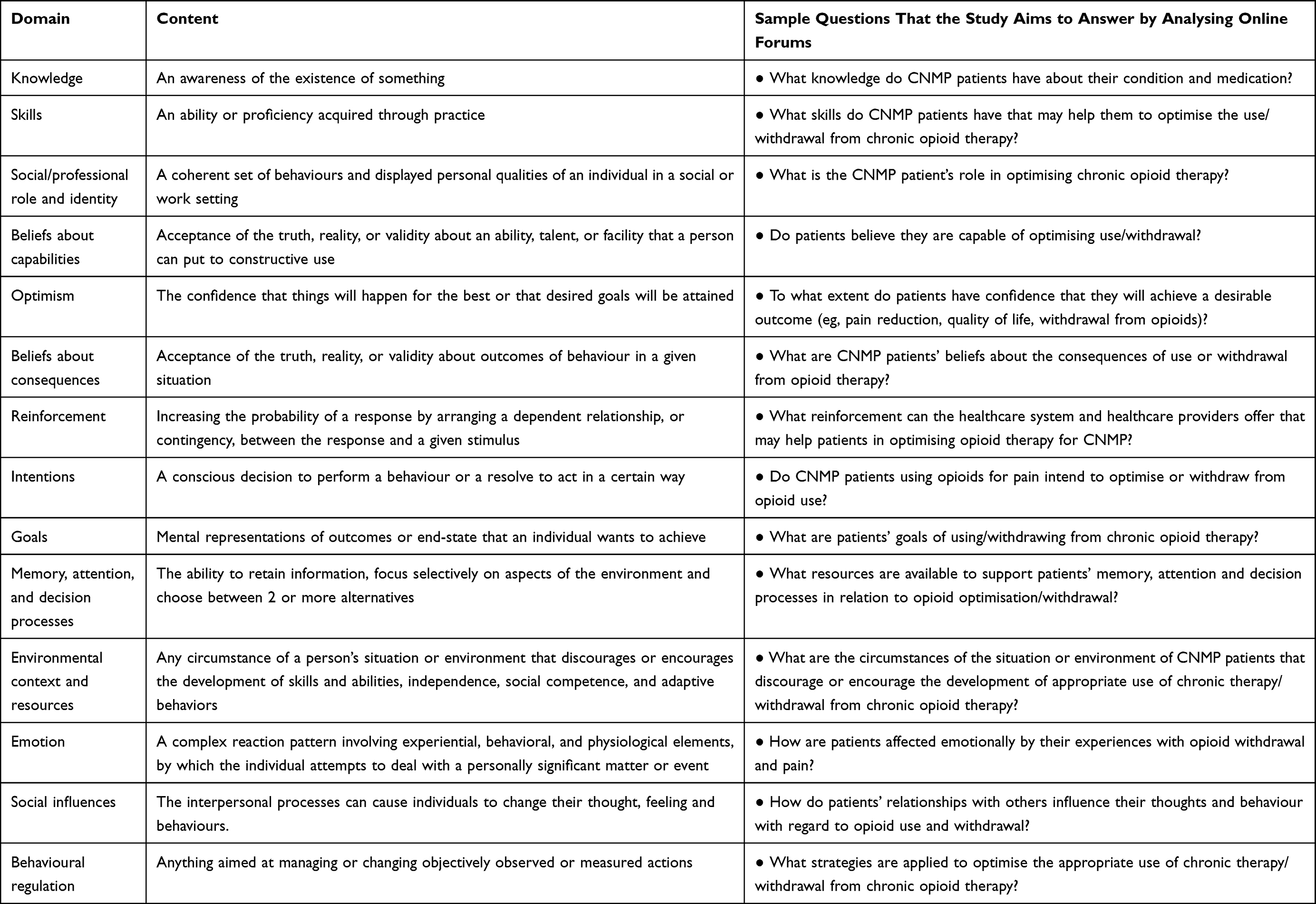 |
Table 2 Mapping Study’ Questions into TDF Domains |
Data were analysed using the Framework method to allow an in-depth reflection of the meaning and patterns of the data to be identified. Extracts from each corpus were coded systematically, using a deductive approach, with each TDF-14 domain used as a coding category.25–27 The data analysis was regularly discussed in research team meetings and any disagreement in coding between the researchers was resolved through discussion until consensus was reached. Multiple posts by the same forum member expressing the same topic were compressed into a single post to prevent the over-counting of an idea or biasing of the data by individual contributors. Threads duplicated between corpora 1 and 2 were reviewed. Coded quotations were organized into a framework table generated in Microsoft Word®. Excerpts were grouped together into topics and then reviewed and refined until meaningful and distinct main themes and subthemes were developed.24 A domain was judged relevant if excerpts were coded frequently or if the researchers believed the posts showed that domain to have a significant impact on the appropriate use of prescribed opioids. A content analysis of the framework table was then undertaken to identify subthemes that shared the same central concept as the main theme and were particularly important for the research question. For example, within the theme, facilitators of COT optimisation, a frequently occurring feature was the need for an individualized approach to opioid prescribing and tapering support. This latter was considered as a subtheme. Subthemes within each domain were summarised to give an overall impression of the potential impact on how each domain may influence the optimisation of opioids in CNMP and illustrated using supporting quotations. Coding stopped once data saturation of the main themes was achieved.
Research Trustworthiness
The research trustworthiness was sought by applying Lincoln and Guba’s principles.27 Credibility was enhanced through the adoption of appropriate, well-recognized research methods informed by previous comparable studies. Rigour was supported by the purposeful inclusion of online forums and following practical guidelines for qualitative research using online forums.18,19,28 The spontaneous nature of the conversations without the researcher’s presence prevents researcher bias. Systematically keeping a logbook of the data collection and analysis process, along with regular research team meetings during the analysis phase to discuss emergent themes, boosted the dependability and confirmability of this study. Public accessibility and the systematic approach of this study to collecting the data enable other researchers to repeat it for other research or/and to reappraise the original researchers’ conclusions.29,30
Ethical Considerations
The study was granted ethical approval from the University of Birmingham and adhered to British Psychological Society (2007) guidelines.31 Consent was not considered essential as all the material was in the public domain and freely available to be viewed without registration with the website, an approach widely used in other studies.15–17 No direct permission was obtained from the forums’ owners, yet the term and conditions statements of the included forums were reviewed by the authors. Any forum that prohibited the accessing, printing, use or storage of the forum content for research or non-commercial professional use was excluded. Also, the anonymity of the data has been protected as forums have not been identified and data excerpts have been paraphrased, with any identifying information removed.
Results
360 threads were identified and a total of 1978 posts were randomly analysed. This study focuses on UK opioid optimisation and following the British Psychological Society (2007) guideline, only UK patients forums that met the inclusion and exclusion criteria have been included. See Table 1.
Three major themes, each with their respective subthemes, were identified from the dataset and mapped against the TDF (See Table 3). Key themes are described below with summary narratives and illustrative quotations.
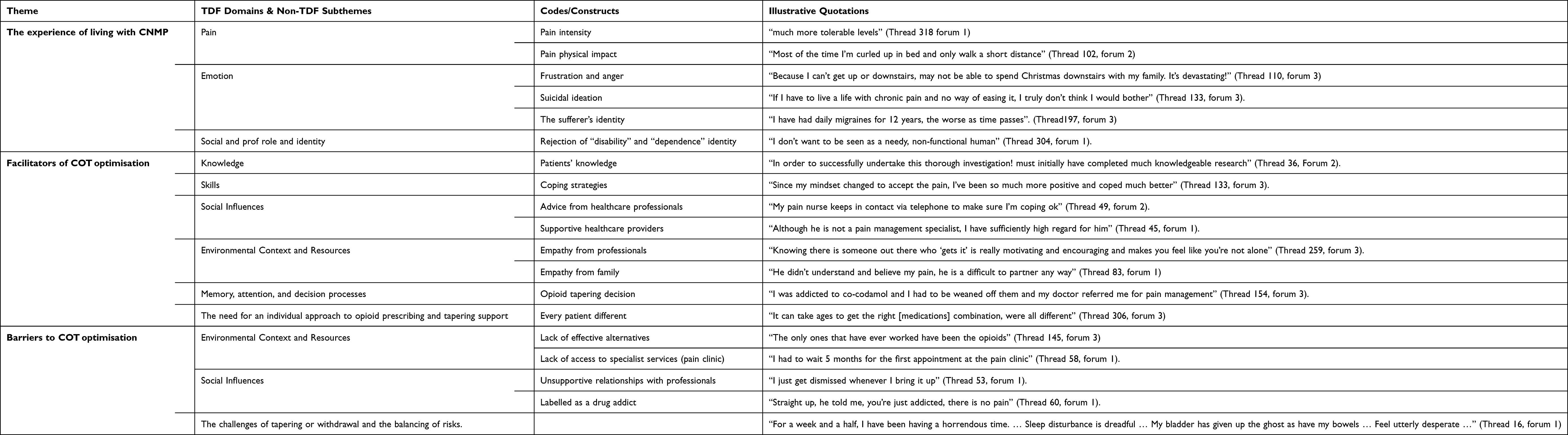 |
Table 3 Theoretical Domains Relevant to Patients’ Perspectives of Barriers and Enablers to the Appropriate Use of Prescribed Opioid Optimisation with Illustrative Quotations |
Theme 1: The Experience of Living with CNMP
A dominant theme throughout the data was patients’ experience of pain. Contributors frequently contextualized their posts by providing information on the location, cause (for example, accident, surgery or health conditions) and duration of their pain. Patients also attempted to describe the intensity of their pain and report improvement or deterioration, either using verbal descriptors such as “excruciating” (Thread 55, forum 3) or in terms of scores on the pain scale:
I had occasions when my pain score was zero and at its worst,4/10 (Thread 16, forum 1).
Posts also revealed how CNMP impacted every aspect of patients’ lives: physical, social, mental and emotional. With regards to the physical impact, for example, they reported impaired function such as being bedridden, unable to walk.
Most of the time I’m curled up in bed and only walk a short distance (Thread 102, forum 2)
Physical limitation, in turn, produced social constraints affecting study, work, leisure and relationships: cancelled outings, inability to spend time with family, financial dependence on others and confinement to home, causing severe psychological impact. For example, a young woman who had to give up university and was confined to her parents’ house, which she said had become her “prison” described her feeling that “the pain is driving me crazy, quite literally” (Thread 233, forum 1).
Patients also experienced a sense of loss resulting from the inability to continue activities that had previously provided satisfaction and meaning in their lives, as in the of case a young man whose inability to continue in his job resulted in losing “the feeling of satisfaction, that my day had meant something” (Thread 128, forum 1). Faced with such losses, patients reported depression extending sometimes to suicidal ideation:
If I have to live a life with chronic pain and no way of easing it, I truly don’t think I would bother (Thread 133, forum 3).
A prominent subtheme was the idea that pain becomes part of the sufferer’s identity, in their own and others’ eyes. Several patients described that they had been assigned, adopted, or even embraced, a social identity /role as “disabled”, with implications, for instance, for support through the welfare system. In contrast, others strenuously rejected the connotations of disability. One participant spoke scathingly of those who “basically give up, quit their jobs, claim disability benefit and sit around their homes all day in pain”, asserting her refusal to become one of them.
A key issue for those who rejected the “disabled” label was the condition of dependence. While there were constraints on their functioning and activities they could not perform without help, some found this difficult to acknowledge. As one contributor posted,
I don’t want to be seen as a needy, non-functional human (Thread 304, forum 1).
Thus, data revealed pain to be a dominant, life-altering experience for constant sufferers. They monitored changes, positive and negative, in pain intensity, shared experience of the social limitations imposed by pain and restricted mobility and sought comfort and reassurance in the face of psychological impacts of often considerable severity. Some accepted a social role as “disabled” and “dependent”, but this was rejected by others, who sought to preserve their former sense of self.
Theme 2: Facilitators of COT Optimisation
The second theme concerned factors that appeared to help and support patients in optimising or reducing their usage of opioids. Some were internal factors, reflecting the TDF domains, Knowledge and Skills. Others were external, reflecting the domains, Social Influences and Environmental Context and Resources. A subtheme was identified here, which is the need for an individual approach to opioid prescribing, tapering and support, in recognition of patients’ different needs and responses.
Patients’ knowledge emerged as a major factor influencing individuals’ perceptions of opioids and alternative treatment options. Posts showed patients to be active seekers of knowledge, who asked questions, exchanged ideas and conducted research in order to better understand their conditions and the benefits and risks of the treatment options available, for example:
“I did some research on pethidine and found out how bad it really was” (Thread 98, forum 2).
Informal sources, particularly print and broadcast media, played a key role in patients’ knowledge search:
I watched a really interesting programme on BBC4 about them [opioids] (Thread 61, forum 3).
Members used the forum to fill gaps in their knowledge and understanding, or to seek a “second opinion” about a proposed new treatment or strategy, appreciating the opportunity to communicate with others who had experienced some of the same challenges:
Maybe you can offer advice on my predicament, especially considering you have been where I currently am and have come off opioids? (Thread 56, forum 1).
Although the forum protocol did not allow members to offer specific medical advice, contributors freely shared information they had read or heard, and recounted their personal experiences of treatments and their effects, good and bad, for example:
There is a longer-acting tablet that should last for 12 hours, then you can occasionally add the liquid as a top-up (Thread 11, forum 2).
The Tens machine is very good for muscular pain. I have one myself. I also found a Tens belt which was much easier to use, requiring no sticky pads (Thread 163, forum 1).
However, patients acknowledged the limitations of their expertise and frequently advised inquirers to consult their GP or other professionals. Patient-provided information and ideas could, however, help to inform such discussion and give patients confidence to ask questions and discuss alternatives.
A prominent sub-theme in the information exchanged, reflecting the Skills dimension of the TDF, related to coping strategies that patients used to manage pain and substitute for or offset the side effects of medication. These fell into two broad categories, physical and psychological. Patients shared their experiences of several physical approaches: diet, exercise, relaxation and heat. For example, one described how she had eliminated carbohydrates to account for her reduced mobility, and increased her fruit and vegetable intake to alleviate constipation associated with her medication. Another described the benefit of having “my trusty special cushion to sit on and a hot water bottle to hand” (Thread 132, forum 3).
The most commonly reported approach was exercise, including exercises prescribed by a physiotherapist (sometimes in private practice), yoga, swimming, Pilates, or simple stretching and walking. Generally, such activities were reported as coping strategies that the patient found useful.
Patients also mentioned psychological approaches such as practising mindfulness, distracting themselves with recreational activities and investing in their sense of personal well-being:
Buy yourself a new book, go out for coffee, plan a holiday … doing something for you will make you feel a whole lot better (Thread 285, forum 1).
For a very small number, however, the solution was simply to accept the pain, rather than having false hopes and unrealistic expectations. As one asserted,” Pain is something you can get used to and learn to cope with” (Thread 289, forum 2) while another reported on the breakthrough she experienced through coming to terms with her pain:
Since my mindset changed to accept the pain, I’ve been so much more positive and coped much better (Thread 133, forum 3).
In coping with their condition, patients made use of a variety of resources available in the surrounding environment, which facilitated their understanding and motivation towards opioid optimisation. Whilst several contributors drew attention to useful material on the internet, such as a website suggesting “gentle physio exercise to try” (Thread 125, forum 3), the majority of resource-related posts highlighted support and advice received from various healthcare professionals, such as nurses at a pain clinic or hospital:
My pain nurse keeps in contact via telephone to make sure I’m coping ok (Thread 49, forum 2).
Supportive relationships with these professionals, reflecting the Social Influence dimension of the TDF, emerged as a crucial facilitator of opioid optimisation. A good doctor was characterized as one who was knowledgeable – though not necessarily a pain specialist, and who showed empathy and understanding. Patients valued having someone who “seemed to get what I was saying” (Thread 58 forum 1) and not only provided information but planned care jointly with the patient.
Health professionals were not, however, the only source of support. A common subtheme was patients’ need for support from a wide range of others including family, friends, an advocate, employers and teachers. The support available from such individuals, however, depended on their knowledge and understanding: “My friends mean well, but really I need support from someone who knows what’s going on” Thread 19, forum 1). This is why the patient forum was so important to many members:
Knowing there is someone out there who ‘gets it’ is really motivating and encouraging and makes you feel like you’re not alone (Thread 251, forum 2).
Such sources of knowledge, practical advice and emotional support seemed to be far more important and relevant to patients (as judged by the number of posts and patients’ emphasis on their importance) than aids to memory, attention and the decision process, such as a tapering chart or pain diary (each mentioned only once) or even behavioural intervention, which rarely appeared in the data. Although a number of patients discussed experiences of opioid tapering or doctors’ prescribing decisions, it was often not clear who initiated the changes, or for what reason. Only one contributor explicitly acknowledged a past addiction and behavioural intervention taken to address it:
I was addicted to co-codamol and I had to be weaned off them and my doctor referred me for pain management (Thread 154, forum 3).
None of the contributors ascribed treatment changes to current addiction. From the variety of resources and strategies mentioned by patients as facilitating their opioid optimisation, one concern emerged clearly: the need for an individual approach to treating CNMP and managing patients’ use of opioids. Posts revealed that patients differ widely in their needs and in their responses to particular medications but perceived this as insufficiently recognized by health practitioners. Rigid imposition of a standardized treatment, or tapering regimes, reportedly led to side effects, increased pain, or withdrawal problems, sometimes causing non-compliance with treatment. Patients wanted doctors to recognize them as individuals, “discuss the pros and cons for your own personal circumstances and to enable and support them in finding their own solutions” (Thread 198, forum 1).
Theme3: Barriers to COT Optimisation
Patients described difficulties they faced in effectively managing their condition and their medication, which reflected the TDF domains: Environmental Context and Resources, and Social Influences, as well as two sub-themes outside the TDF: the challenges of tapering or withdrawal and the balancing of risks.
A major issue affecting medicine use behaviours was the perceived lack of effective alternatives to the medicines patients were currently using. Many patients had tried and discontinued numerous medications that did not sufficiently control the pain, or produced side effects, allergies or intolerance. Consequently, several felt that opioids were the only option remaining:
I have tried everything available and this was the only option for me (Thread 317, forum 1)
The only ones that have ever worked have been the opioids (Thread 145, forum 3).
Regarding non-pharmacological alternatives, some had found physiotherapy helpful, but others found the exercises difficult, and thought they compounded the problem:
The physio keeps giving me exercises that worsen the pain! (Thread 277, forum 1).
Patients also highlighted difficulty accessing formal health services for the support and care they needed. It might be necessary to travel a considerable distance for an appointment with a specialist at a hospital or pain clinic, and there were reports of long waiting lists for a referral.
Moreover, there was a lack of continuity of care, as different professionals were seen on each visit. There were reports of prescribing decisions made by a doctor who did not actually know the patient or rarely saw him or her. As one contributor reported,
I see a different GP every time. My assigned GP is ok, but she’s hardly ever there (Thread 344, forum 3).
There were also reports of a lack of reliable access to the GP, preventing patients from mentioning ideas and questions they wanted to raise. Even when patients gained access to healthcare professionals, many described what they perceived as unhelpful encounters and unsupportive relationships with doctors, who, they claimed had dismissed their worries. For example, one who expressed concerns about medication-related risk declared,
I just get dismissed whenever I bring it up (Thread 53, forum 1).
Another, who sought help with depression, was simply given the telephone number of the Samaritans. Faced with what they perceived as dismissiveness and impatience, some patients were deterred from seeking further help:
I was too afraid to go to the doctor again because I was made to feel I was going too much (Thread 251, forum 2).
Some patients clearly felt misjudged and subject to negative assumptions by health professionals, for example being seen as drug-seeking or uncooperative if they reported difficulties with tapering or having the reality of their pain called into question.
They say I’m drug-seeking, need psych care and don’t want to take part [in the programme offered], which is so untrue (Thread 102, forum 2).
Straight up, he told me, you’re just addicted, there is no pain (Thread 60, forum 1).
The system makes you feel like a junkie at times (Thread 172, forum 1).
One reason for such attitudes on some doctors’ part may be a lack of specialized knowledge in the area of CNMP and its treatment. A number of participants were critical of health professionals’ shortcomings in this area:
There remains a huge lack of knowledge and understanding of the medication needs of CNMP patients (Thread 26, forum 2).
There were suggestions that it may be necessary to change GPs several times before someone suitably knowledgeable and sympathetic was found.
In the face of what was sometimes perceived as an absence of support from the health services, patients reported anger and frustration, as well as fear at the prospect of unremitting pain, which overshadowed thoughts of tapering or withdrawal. Nevertheless, a number of patients described attempts to taper medication or come off opioids by various means, and some were keen to do so, because of worries about harmful effects of long-term opioid use. In many instances, patients resorted to ways of using their medication, which were potentially dangerous. For example, one contributor recommended another to cut a fentanyl patch in two to reduce the side effects associated with it. Others divided slow-release tablets to maximize the benefit of the existing dose, or to achieve gradual reduction and showed no awareness of the risk involved. Others who followed doctors’ directions still faced challenges. Several reported experiences of a sudden drastic reduction in dose of medication without notice or a clear plan for managing the effects, which could be severe. One patient recalled,
I was cut off; two days later, in so much pain, vomiting and had had no sleep, I was admitted to my doc’s clinic for the weekend (Thread 161, forum 1).
Patients frequently referred to the problems associated with withdrawal, which some described as “horrendous”, and if undergone without adequate support, could thwart the best of intentions. The idea that the main concern was to alleviate the pain by any means possible was summed up by one patient, who argued,
Chronic pain is hell … taking medications that help make your life better is the only way to go (Thread 61, forum 3).
Patients saw themselves as struggling to balance competing risks: the harmful effects of long-term opioid use, the impact (experienced and anticipated) of withdrawal and the possibilities of renewed or increased pain and disability if they stopped a medication they found effective.
I’m just so afraid being left in continuous, unbearable pain (Thread 341, forum 3).
Overall, the picture emerging from the patient forums was that patients wanted to manage their medication appropriately and were willing to consider or attempt tapering. However, they were often confused, frightened, and overwhelmed by the severity of the challenges involved, particularly if they had difficulty accessing service or felt they were being unheard, pushed to withdrawal too quickly, or unsupported in balancing the opioid-related challenges with the physical, social and mental effects of constant pain.
Discussion
No previous study has explored the enablers and barriers to optimising the use of prescribed opioids for CNMP using patients’ online forums. This study analysed a sample of posts on CNMP and general health forums and yielded three major themes which reflected patients’ experiences of living with pain, facilitators of prescribed opioid optimisation and barriers to prescribed opioid optimisation.
The first theme highlighted the impact of CNMP patients’ quality of life and a sense of control over their life. This study’s finding is consistent with a large-scale survey of CNMP patients, which concluded that improvement in their energy, concentration, sleep, family, employment, social relationships, enjoyment of life and recreational activities should be appropriate targets of their treatment.10,12,32 Pain was seen to be a multidimensional, dynamic interaction of biological, psychological and social factors, suggesting the potential value of individualised assessment and appropriate management of psychosocial factors in the early stage of pain conditions.
Furthermore, the early establishment of a balanced provider-patient relationship through awareness of social, physical, and physiological aspects in patients’ conditions supports patients’ ability to open up, know and accept their condition.33 The present study emphasizes the importance of the provider-patient relationship, as both an enabler (if positive) and a barrier (if negative) to prescribed opioid optimisation, consistent with previous studies.33–35 Moreover, the literature provides consistent evidence that patient-provider collaboration in the identification of treatment goals and shared decision-making results in improved outcomes.35 Patients place health care continuity with providers as a high priority to optimise their care and facilitate knowledge and trust. High care continuity is linked with lower hospitalization, emergency department visits and medical errors and improved patient safety, as it is easier for the providers to manage medical problems in the office or over the phone and prevent extra redundant healthcare utilization.34
The study findings revealed that some patients showed potentially dangerous ignorance of how to use opioids. For example, cutting fentanyl patches could lead to serious harm, including death, as the dose that is supposed to be delivered over 72 hours could be delivered immediately, leading to overdose.36 Whereas strict adherence to other pain analgesics is not necessary and deviation from them may be acceptable, following the instructions for using opioid medications is vital. Opioid-related overdose and other serious adverse effects have been periodically reported in UK clinical practice.37 Patients’ misinformation results from attempts to fill the gaps in information from professional sources. A recent study exploring the role of UK community pharmacists in optimising prescribed opioids revealed time and systemic constraints on their ability to educate CNMP patients on opioids.38 Yet GPs may lack the required knowledge and specialists can be difficult to access.39 Patient education on CNMP and appropriate opioid use for pain relief, and patients’ discussion of their concerns with healthcare providers are crucial. It is widely accepted that structured educational programmes that include information about CNMP and treatment options emphasise the importance of appropriate medication use and provide practical tools to prevent unintended side effects.40 These programmes might be more effective when offered in a patient-tailored approach and addressing individual needs. This could be achieved by tailored discussions with health care providers, particularly pharmacists.41
Prominent barriers were poor access to pain services or non-pharmacological treatments as well as perceived ineffectiveness of alternatives tried. Uneven distribution of facilities for psychological and physiotherapeutic treatment may explain why pain treatment is frequently solely pharmacologic, although recommendations increasingly promote a multi-modal treatment strategy.42 Kroenke et al suggested that the early engagement with non-pharmacological treatment could be considered a prerequisite for ongoing opioid therapy as part of treatment agreements. They suggested that collaborative care models in which mid-level providers, particularly nurses, provide follow -up, could enhance patient motivation. Non-pharmacological treatment may be critical for improving the quality of care.43 This is also consistent with patient reports that continued encouragement from their care team would be a significant facilitator to their pain treatment engagement.44 This last point is also related to the factor of support, another recurring theme in our data. Besides care management and structured follow up, our findings suggested peer and family support interventions as other potentially effective strategies, models well-supported in the treatment of other chronic conditions.45
This study is a one sided view of chronic pain treatment. The patients’ perspective alone is insufficient evidence that there are major gaps in chronic pain treatment. There are many national programmes that have been started as part of optimisation for treatment of chronic pain with a multimodal focus. For example, according to the 2013 National Directory of Services, there are 97 pain management programmes in the UK. Also The Royal College of Anaesthetists’ Faculty of Pain Medicine and the Royal College of General Practitioners have both emphasised the importance and advantages of a multidisciplinary approach. These programmes are multimodal treatment packages based on cognitive behavioural therapy (CBT) and allied rehabilitation treatments that aim to restore function by supporting and maintaining changes in behaviours that perpetuate or increase pain. They are not mainly concerned with the pain itself, but rather with improving self-management and independence, allowing individuals to live as normally as possible despite the limitations imposed by their pain.46
Strengths and Limitations
Rigorous methods for data collection and thematic analysis were used, and we believe that thematic saturation was achieved. All the posts sampled were posted by CNMP patients who were either current or former prescribed opioid users. The collection of threads related to opioid use from three different forums provided a broad overview of all possible issues related to the study’s objectives. The study may help advance the field by increasing the awareness of health care professionals. By assessing patients’ beliefs and knowledge base about their condition and treatment options, healthcare professionals may be able to focus on perceived gaps in caring for patients with chronic pain, including a focus on dissemination of knowledge about treatment options for chronic pain, including non opioids.
Nevertheless, some limitations should be addressed. The data collected reflected a range of perspectives from CNMP patients with different pain conditions. This means the findings do not provide information related to specific CNMP conditions. The subjectivity of the patients’ statements is the primary limitation of this study. Another limitation of this study is a selection bias. It is not known whether patients who are motivated to feel better and reduce their usage of prescription opioids or use them more appropriately and taper them, may be more likely to engage in online forums and discussions about alternatives to treat chronic pain, or conversely whether patients who are not improving or not motivated to try alternative options may be more prone to posting on online forums. Amongst patients who are forum contributors, there may also be a recall bias related to whether their pain has been better or more poorly controlled in the recent past.
Another flaw in this study that has to be addressed is that the categorization of posts, although guided by published definitions of the TDF domains, inevitably entailed some interpretation by the researchers, especially in identifying implicit meaning rather than simply counting instances of occurrence of specific words (although the latter, too, can risk distortion of qualitative context).47
Another limitation of this research is that it only looked at open access forums and excluded private community forums. Because a constant user ID allows other participants to track and know each other over time, forums that require registration have a greater percentage of repeat participation. This helps forum users to form relationships and develop bonds, while anonymity may hinder the team’s capacity to form relationships that strengthen social harmony. Also, contributors feel safer and more open to collaborate, since their information is only accessible to authorised users who share a same interest or relationship, resulting in high user engagement.48,49
Furthermore, current health models emphasize the importance of healthcare professionals’ and patients’ collaboration in medicine optimisation practices, yet healthcare providers were not included in this study. As such, it is important that their perspectives on opioid optimisation are investigated.
Practical Implications and Recommendations
Online forums may offer patients, especially distressed patients, a unique opportunity for support and sharing experiences. Healthcare providers could encourage their patients to open up about the information sources that they use to look up information about their condition, medication use or any alternative methods to manage their pain. Also, they could suggest useful resources for coping strategies, such as trustworthy websites, articles or books. Adverse outcomes of medications in CNMP have been well documented.50,51 It is imperative that patient perspectives are taken into account when designing pain services. A recent systematic review demonstrated that designing evidence-based and patient-centred intervention that overcomes the recent CNMP practice gaps and address patients’ needs more appropriately is essential.42
Future Research
There was some concern about the applicability of strategies to all pain patients. As such, prospective research could develop and trial a complex intervention to account for identified challenges at the medication, patient, prescriber and health system levels, and also be flexible in nature to allow clinicians to tailor intervention strategies to individual patient needs. There are self-care interventions and alternative approaches that CNMP patients use daily to cope and manage their pain, which they are usually reluctant to share with their clinicians. Therefore future research may investigate these self-care interventions and their associated outcomes using patients’ online forums. Also, exploring the healthcare providers’ perspective around the same topic is crucial for a deep understanding of patients’ need to optimise their prescribed opioid therapy. Research can evaluate the accuracy of information shared via online forums, considering the amount exchanged and the large number of people who view it, as this study revealed that some of the medication information exchanged between users is inaccurate. This study has highlighted the danger of glaring misinformation that could be spread via these forums (e.g, cutting fentanyl patches in half). Nevertheless the data from patients’ online forums could be used as a valuable tool for performance improvement for health care entities, subject to awareness of potential bias in the opinions of forum contributors. It would be worthwhile conducting more studies using these forums.
Conclusion
Analysis of CNMP patients’ posts on online forums highlighted the devastating impact of pain on social functioning, relationships and mental health. The main facilitating factor was the support of knowledgeable and empathetic healthcare providers; too often, however, provider-patient relationships were perceived as unhelpful, the difficulties being compounded by the problems of access and continuity. Patients were left angry, depressed and fearful, leading to potentially dangerous medication use and additional demand on services. The findings highlighted the need for multi-dimensional, individualized treatment approaches to support and enable patients’ appropriate opioid use.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Acknowledgments
We would like to acknowledge the University of Birmingham and the Royal Embassy of Saudi Arabia, London for sponsoring the PhD of the lead author (AA) of this study. The funders had no role in the design and conduct of the research and the interpretation of the data generated.
Funding
This work was funded by the University of Birmingham. AA was sponsored for her PhD by the Royal Embassy of Saudi Arabia, Cultural Bureau in London.
Disclosure
The authors declare no conflicts of interest for this work.
References
1. Rathert C, Wyrwich MD, Boren SA. Patient-centered care and outcomes: a systematic review of the literature. Med Care Res Rev. 2013;70(4):351–379. doi:10.1177/1077558712465774
2. Lamé IE, Peters ML, Vlaeyen JW, Kleef M, Patijn J. Quality of life in chronic pain is more associated with beliefs about pain, than with pain intensity. Eur J Pain. 2005;9(1):15–24. doi:10.1016/j.ejpain.2004.02.006
3. Busse JW, Wang L, Kamaleldin M, et al. Opioids for chronic noncancer pain: a systematic review and meta-analysis. JAMA. 2018;320(23):2448–2460. doi:10.1001/jama.2018.18472
4. Kaboré JL, Pagé MG, Dassieu L, et al. Doctor shopping among chronic noncancer pain patients treated with opioids in the province of Quebec (Canada): incidence, risk factors, and association with the occurrence of opioid overdoses. Pain Rep. 2021;6(3):e955. doi:10.1097/PR9.0000000000000955
5. Alenezi A, Yahyouche A, Paudyal V. Current status of opioid epidemic in the United Kingdom and strategies for treatment optimisation in chronic pain. Int J Clin Pharm. 2021;43(2):318–322. doi:10.1007/s11096-020-01205-y
6. Fayaz A, Croft P, Langford RM, Donaldson LJ, Jones GT. Prevalence of chronic pain in the UK: a systematic review and meta-analysis of population studies. BMJ Open. 2016;6(6):e010364. doi:10.1136/bmjopen-2015-010364
7. Treede R-D, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003–1007. doi:10.1097/j.pain.0000000000000160
8. Wideman TH, Edwards RR, Walton DM, Martel MO, Hudon A, Seminowicz DA. The multimodal assessment model of pain: a novel framework for further integrating the subjective pain experience within research and practice. Clin J Pain. 2019;35(3):212–221. doi:10.1097/AJP.0000000000000670
9. Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10(4):287–333. doi:10.1016/j.ejpain.2005.06.009
10. Gjesdal K, Dysvik E, Furnes B. Living with chronic pain: patients’ experiences with healthcare services in Norway. Nurs Open. 2018;5(4):517–526. doi:10.1002/nop2.160
11. Price C, de CWAC, Smith BH, Bottle A. The national pain audit for specialist pain services in England and Wales 2010–2014. Br J Pain. 2019;13(3):185–193. doi:10.1177/2049463718814277
12. Tsang A, Von Korff M, Lee S, et al. Common chronic pain conditions in developed and developing countries: gender and age differences and comorbidity with depression-anxiety disorders. J Pain. 2008;9(10):883–891. doi:10.1016/j.jpain.2008.05.005
13. McCrorie C, Closs SJ, House A, et al. Understanding long-term opioid prescribing for non-cancer pain in primary care: a qualitative study. BMC Fam Pract. 2015;16(1):121. doi:10.1186/s12875-015-0335-5
14. Jonsdottir T, Gunnarsdottir S, Oskarsson GK, Jonsdottir H. Patients’ perception of chronic-pain-related patient-provider communication in relation to sociodemographic and pain-related variables: a cross-sectional nationwide study. Pain Manag Nurs. 2016;17(5):322–332. doi:10.1016/j.pmn.2016.07.001
15. Attard A, Coulson NS. A thematic analysis of patient communication in Parkinson’s disease online support group discussion forums. Comput Human Behav. 2012;28(2):500–506. doi:10.1016/j.chb.2011.10.022
16. Coulson NS, Buchanan H, Aubeeluck A. Social support in cyberspace: a content analysis of communication within a Huntington’s disease online support group. Patient Educ Couns. 2007;68(2):173–178. doi:10.1016/j.pec.2007.06.002
17. Teasdale E, Clarke H, Chen N, Everitt H. Online forum users’ views and experiences of managing irritable bowel syndrome: a qualitative analysis of discussion content. BJGP Open. 2020;4(5). doi:10.3399/bjgpopen20X101084
18. Holtz P, Kronberger N, Wagner W. Analyzing internet forums: a practical guide. J Media Psychol. 2012;24(2):55–66. doi:10.1027/1864-1105/a000062
19. Im EO, Chee W. Practical guidelines for qualitative research using online forums. Comput Inform Nurs. 2012;30(11):604–611. doi:10.1097/NXN.0b013e318266cade
20. Kozinets RV. Netnography: doing ethnographic research online; 2010.
21. Cane J, O’Connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci. 2012;7(1):37. doi:10.1186/1748-5908-7-37
22. Michie S, Johnston M, Abraham C, Lawton R, Parker D, Walker A. Making psychological theory useful for implementing evidence based practice: a consensus approach. Qual Saf Health Care. 2005;14(1):26–33. doi:10.1136/qshc.2004.011155
23. Phillips CJ, Marshall AP, Chaves NJ, et al. Experiences of using the theoretical domains framework across diverse clinical environments: a qualitative study. J Multidiscip Healthc. 2015;8:139–146. doi:10.2147/JMDH.S78458
24. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
25. Kahlke RM. Generic qualitative approaches: pitfalls and benefits of methodological mixology. Int J Qual Methods. 2014;13(1):37–52. doi:10.1177/160940691401300119
26. Lincoln YS, Guba EG. But is it rigorous? Trustworthiness and authenticity in naturalistic evaluation. New Dir Program Eval. 1986;1986(30):73–84. doi:10.1002/ev.1427
27. Probst B, Berenson L. The double arrow: how qualitative social work researchers use reflexivity. Qual Soc Work. 2014;13(6):813–827. doi:10.1177/1473325013506248
28. Bhamrah G, Ahmad S, NiMhurchadha S. Internet discussion forums, an information and support resource for orthognathic patients. Am J Orthod Dentofacial Orthop. 2015;147(1):89–96. doi:10.1016/j.ajodo.2014.08.020
29. Morse JM. Critical analysis of strategies for determining rigor in qualitative inquiry. Qual Health Res. 2015;25(9):1212–1222. doi:10.1177/1049732315588501
30. Sudweeks F, Rafaeli S. How Do you get a hundred strangers to agree: computer mediated communication and collaboration; 1996.
31. Hewson C, Buchanan T. Ethics guidelines for internet-mediated research; 2013.
32. Nichols VP, Abraham C, Eldabe S, Sandhu HK, Underwood M, Seers K. Process evaluation protocol for the I-WOTCH study: an opioid tapering support programme for people with chronic non-malignant pain. BMJ Open. 2019;9(10):e028998. doi:10.1136/bmjopen-2019-028998
33. Matthias MS, Parpart AL, Nyland KA, et al. The patient-provider relationship in chronic pain care: providers’ perspectives. Pain Med. 2010;11(11):1688–1697. doi:10.1111/j.1526-4637.2010.00980.x
34. Mainous AG 3rd, Baker R, Love MM, Gray DP, Gill JM. Continuity of care and trust in one’s physician: evidence from primary care in the United States and the United Kingdom. Fam Med. 2001;33(1):22–27.
35. Pergolizzi JV, Varrassi G, Paladini A, LeQuang J. Stopping or decreasing opioid therapy in patients on chronic opioid therapy. Pain Ther. 2019;8(2):163–176. doi:10.1007/s40122-019-00135-6
36. Jumbelic MI. Deaths with transdermal fentanyl patches. Am J Forensic Med Pathol. 2010;31(1):18–21. doi:10.1097/PAF.0b013e31818738b8
37. Bedson J, Chen Y, Ashworth J, Hayward RA, Dunn KM, Jordan KP. Risk of adverse events in patients prescribed long-term opioids: a cohort study in the UK clinical practice research datalink. Eur J Pain. 2019;23(5):908–922. doi:10.1002/ejp.1357
38. Alenezi A, Yahyouche A, Paudyal V. Roles, barriers and behavioral determinants related to community pharmacists’ involvement in optimizing opioid therapy for chronic pain: a qualitative study. Int J Clin Pharm. 2021;1–12. doi:10.1007/s11096-020-01222-x
39. Kennedy MC, Henman MC, Cousins G. General practitioners and chronic non-malignant pain management in older patients: a qualitative study. Pharmacy. 2016;4(1). doi:10.3390/pharmacy4010015
40. Timmerman L, Stronks DL, Huygen F. The design of a theory-based intervention to improve medication adherence in chronic pain patients. Curr Med Res Opin. 2017;33(7):1293–1301. doi:10.1080/03007995.2017.1314955
41. Timmerman L, Stellema R, Stronks DL, Groeneweg G, Huygen FJ. Adherence to pharmacological pain therapy in patients with nonmalignant pain: the role of patients’ knowledge of pain medication. Pain Pract. 2014;14(8):701–708. doi:10.1111/papr.12139
42. Alenezi A, Yahyouche A, Paudyal V. Interventions to optimize prescribed medicines and reduce their misuse in chronic non-malignant pain: a systematic review. Eur J Clin Pharmacol. 2021;77(4):467–490. doi:10.1007/s00228-020-03026-4
43. Kroenke K, Krebs EE, Wu J, Yu Z, Chumbler NR, Bair MJ. Telecare collaborative management of chronic pain in primary care: a randomized clinical trial. JAMA. 2014;312(3):240–248. doi:10.1001/jama.2014.7689
44. Amatya B, Young J, Khan F. Non-pharmacological interventions for chronic pain in multiple sclerosis. Cochrane Database Syst Rev. 2018;12(12):Cd012622. doi:10.1002/14651858.CD012622.pub2
45. West C, Usher K, Foster K, Stewart L. Chronic pain and the family: the experience of the partners of people living with chronic pain. J Clin Nurs. 2012;21(23–24):3352–3360. doi:10.1111/j.1365-2702.2012.04215.x
46. Wilson IR. Management of chronic pain through pain management programmes. Br Med Bull. 2017;124(1):55–64. doi:10.1093/bmb/ldx032
47. Krippendorff K. Content Analysis: An Introduction to Its Methodology. Sage publications; 2018.
48. Lovatt M, Bath PA, Ellis J. Development of trust in an online breast cancer forum: a qualitative study. J Med Internet Res. 2017;19(5):e175. doi:10.2196/jmir.7471
49. Kim KK, Lee AR, Lee U-K. Impact of anonymity on roles of personal and group identities in online communities. Inf Manag. 2019;56(1):109–121. doi:10.1016/j.im.2018.07.005
50. Alrashdi S, Paudyal V, Elnaem MH, Cheema E. Causes, nature and toxicology of tramadol-associated deaths reported in the peer-reviewed literature: a systematic review of case studies and case series. Drugs Ther Perspect. 2021;37(9):422–432. doi:10.1007/s40267-021-00859-6
51. Cheema E, McGuinness K, Hadi MA, et al. Causes, nature and toxicology of fentanyl-associated deaths: a systematic review of deaths reported in peer-reviewed literature. J Pain Res. 2020;13:3281–3294. doi:10.2147/JPR.S280462
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.