")
Back to Journals » Patient Preference and Adherence » Volume 15
Patient and Neurologist Preferences in the United States for Relapsing-Remitting Multiple Sclerosis Treatments: Findings from a Discrete Choice Experiment
Authors Kumar J, Cambron-Mellott MJ , Tencer T, Will O , Mackie dS, Beusterien K
Received 13 February 2021
Accepted for publication 28 May 2021
Published 8 July 2021 Volume 2021:15 Pages 1515—1527
DOI https://doi.org/10.2147/PPA.S306498
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Jinender Kumar,1 M Janelle Cambron-Mellott,2 Tom Tencer,1 Oliver Will,2 deMauri S Mackie,2 Kathleen Beusterien2
1Worldwide Health Economics and Outcomes Research, Bristol Myers Squibb, Princeton, NJ, USA; 2RWE Data and Analytics, Kantar Health, New York, NY, USA
Correspondence: M Janelle Cambron-Mellott
Kantar Health, 3 World Trade Center, 175 Greenwich Street, 35th Floor, New York, NY, 10007, USA
Tel +1 212 706 3961
Email [email protected]
Background and Objective: Relapsing-remitting multiple sclerosis (RRMS) is a chronic inflammatory disease associated with central nervous system dysfunction and accelerated brain volume loss (BVL). There exists a paucity of research examining the importance of BVL to patients and neurologists and exploring whether such preferences may differ between these two groups. This study sought to evaluate the preferences of patients and neurologists for RRMS treatments by considering benefits and risks associated with novel and common disease-modifying therapies (DMTs).
Patients and Methods: US patients diagnosed with non-highly active RRMS and US-based neurologists completed an online cross-sectional survey. A discrete choice experiment was used to assess patient and neurologist treatment preferences, with neurologists considering preferences for patients with non-highly active RRMS. Respondents chose between two treatment profiles with seven attributes identified in qualitative research: 2-year disability progression; 1-year relapse rate; rate of BVL; and risks of gastrointestinal symptoms, flu-like symptoms, infection, and life-threatening events. Attribute-level weighted preferences were estimated using a hierarchical Bayesian model.
Results: Analyses included 150 patients with non-highly active RRMS (mean age: 54 years) and 150 neurologists (65% in private practice). Among patients, the most important treatment attribute was reducing the rate of BVL, followed by reducing the risk of infection and risk of flu-like symptoms. In contrast, the most important treatment attribute among neurologists was reducing the risk of a life-threatening event, followed by slowing the rate of 2-year disability progression and risk of infection.
Conclusion: The findings highlight differences in treatment preferences between US patients and neurologists for non-highly active RRMS. The importance placed by patients on slowing the rate of BVL makes this a key topic that should be covered in the shared decision-making process.
Keywords: relapsing-remitting multiple sclerosis, patient preferences, physician preferences, brain volume loss
Introduction
Multiple sclerosis (MS), a chronic inflammatory disease, involves damage to the central nervous system and impairments in neurologic function.1 More than 2 million people worldwide have MS, with nearly 1 million in the United States alone.2,3 Most often identified in adulthood, and more prevalent among females, the most common symptoms of MS include fatigue, chronic pain, weakened mobility, and cognitive impairment.4,5 The most common form of MS, relapsing-remitting MS (RRMS) is associated with periods of worsened neurologic function and symptomatology followed by partial or complete recovery and has a highly individualized disease course.1,6,7
At present, MS has no cure and treatment has generally focused on symptom mitigation and halting disease progression. Disease-modifying therapies (DMTs) remain at the forefront of RRMS management; however, these therapies vary in their efficacy and safety profiles.8 In addition to more traditional symptoms of MS, studies have documented significant brain volume loss (BVL) beyond that expected in the context of aging alone.9 BVL has been linked with magnetic resonance imaging–based lesion burden, disease duration, and level of impairment.10–13 BVL has also been associated with cognitive impairment, irreversible changes to several cortical structures, and worsening of health-related quality of life.14–16 Importantly, DMTs have been shown to slow the rate of BVL to varying degrees.17–20
Whereas extensive work has documented patient preferences for MS treatments, examining the importance of attributes such as relapse rate, disability progression, route of administration, treatment frequency, and serious and common adverse events,21–24 the importance placed by patients on reducing the rate of BVL has not been explored.
Furthermore, there exists a paucity of research exploring physician preferences in any context or comparing preferences between patients and providers.25 The management of MS requires a high level of communication and shared decision-making between patients and providers;26 thus, insight into the treatment preferences in both groups may help promote more effective care and improved clinical outcomes. Therefore, this study sought to assess treatment preferences among patients and providers in the United States, including their prioritization of the benefits and risks associated with common and novel DMTs in RRMS, including BVL, and to evaluate whether treatment preferences differ between patients and providers.
Patients and Methods
This study was conducted in three phases. First, a targeted literature review and concept elicitation interviews with 10 patients with RRMS and 10 neurologists who treat RRMS were conducted to determine the features (attributes) that most influence treatment choice and inform survey content.27 Second, cognitive interviews were conducted with five patients and five neurologists to confirm the attributes, ensure the questionnaires were clear and interpreted uniformly by participants and that the discrete choice experiment (DCE) exercise was easy to follow, and to refine the survey wording and content, as applicable. Third, online, cross-sectional stated preference surveys were completed in the United States by patients with RRMS and neurologists who treat RRMS.
Panels were used to recruit patients and included the Kantar Profiles Patient Panel and Dynata. Panel members previously identified as having MS were emailed invitations to participate. To boost sample size, prequalification questionnaires were also sent to general panel members; those who qualified were then sent invitations to participate. Neurologists were recruited from the Kantar Profiles Physician Panel and Sermo by sending survey invitations to panel members preidentified as neurologists. Data collection occurred between February 7 and March 19, 2020. The study was designated as exempt from ethics review by Pearl IRB (Indianapolis, IN; IRB study number: 19-KANT-189), as the data from the interview and survey procedures were not linked with personally identifying information (exempt review category DHHS 45 CFR 46.104(d) category 2), and this study was conducted in accordance with the Declaration of Helsinki. The study was submitted to an external IRB as Kantar Health’s internal IRB is used only for studies where there is no defined external IRB channel (eg, when there is no centralized ethics committee or there is no submission destination for the type of work). Informed consent was obtained from all study participants.
To participate, patients had to be ≥18 years of age at the time of survey and to self-report a healthcare provider diagnosis of RRMS. Patients were excluded if they were currently using a medication typically prescribed for highly active RRMS (eg, alemtuzumab, natalizumab, cladribine, rituximab) or if they had never been treated with a DMT for RRMS and were not planning to be treated with a DMT in the next 6 months. Neurologists could participate if they were board-certified or board-eligible in neurology, had practiced for at least 3 years, spent ≥75% of their time in direct patient care, and were managing at least 20 patients with MS and at least 10 patients with RRMS in the past 3 months preceding survey completion.
Survey Content
A DCE was used to assess treatment preferences. With a DCE, participants’ willingness to accept trade-offs in hypothetical treatment profiles could be evaluated. In a series of choice tasks, respondents viewed two hypothetical treatment profiles side by side; the treatment profiles comprised combinations of seven treatment features (attributes), which varied with respect to their attribute levels, and respondents selected their preferred option. Attributes and levels were the same for patients and neurologists (Table 1), and neurologists were asked to consider treatment for a patient with non–highly active RRMS who may or may not previously have received treatment. Attribute levels reflected the range of performance seen among select DMTs approved for the treatment of RRMS.17–20,28–35 Appendix 1 contains detailed information on how the minimum and maximum levels for rate of BVL were identified. A balanced design with minimal overlap, generated in Lighthouse Studio 2018 Version 9.8.0 (Sawtooth Software, Provo, UT), was used to determine the combinations of levels shown across choice tasks in the DCE.36 Three hundred fifty choice sets were created so that each respondent saw a different series of tasks. Each respondent completed a total of nine choice tasks.
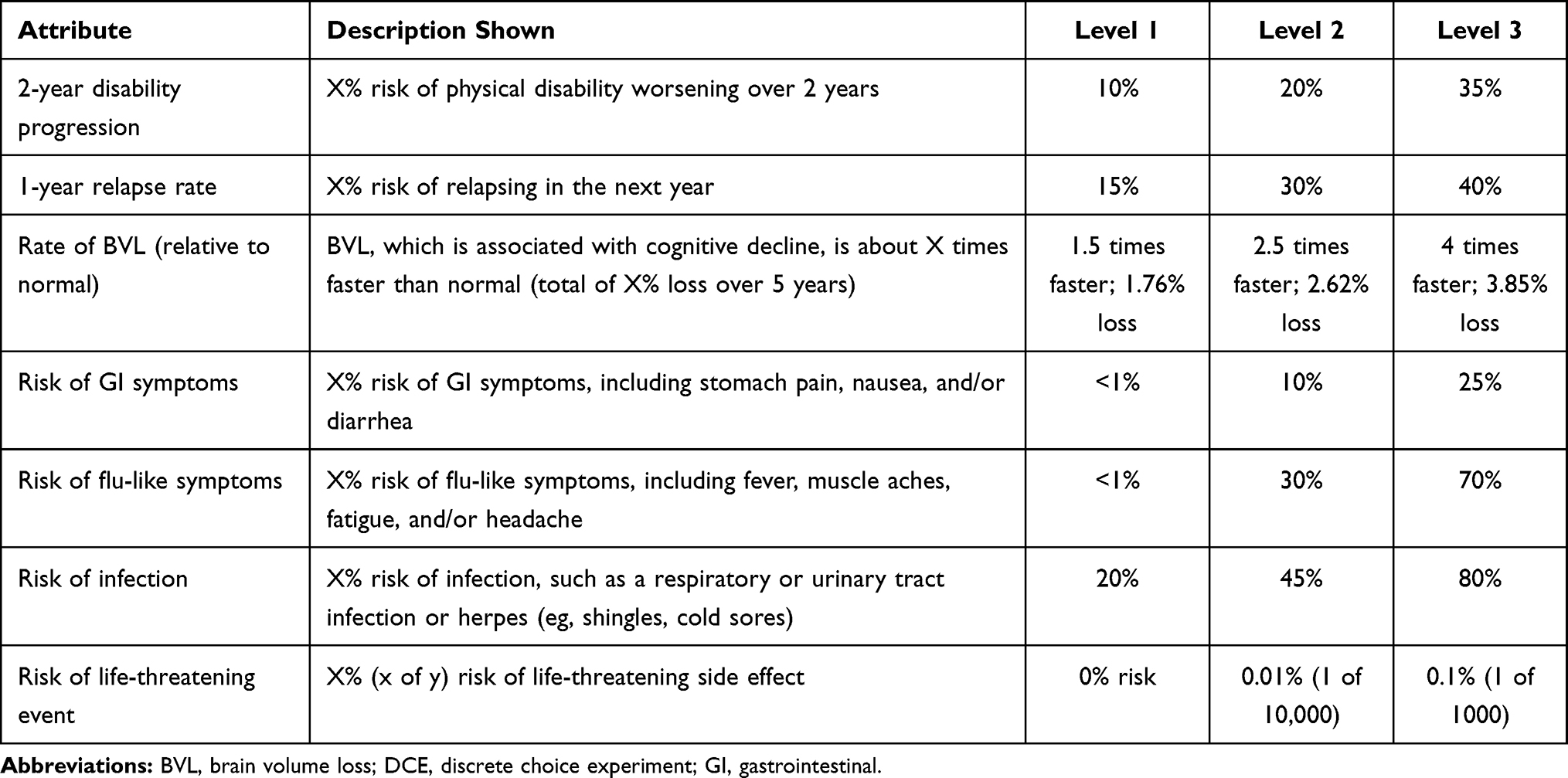 |
Table 1 Attributes and Levels Included in the DCE |
The surveys included an introductory section describing the meaning of BVL, followed by a section in which respondents rated each of the attribute levels on a five-point scale (ie, very bad to very good) to acquaint respondents with the treatment attributes in the DCE choice tasks. These ratings were also used as an indicator of inattentiveness in responses. The DCE exercises then followed.
Patient sociodemographic, clinical, and treatment characteristics and neurologist sociodemographic, professional history, and practice characteristics were also collected. The Multiple Sclerosis Self-Efficacy Scale (MSSE)37 and the 54-item Multiple Sclerosis Quality of Life (MSQOL-54) Cognitive Function subscale, two patient-reported outcome measures, were also collected.38 The MSSE comprises two nine-item scales, Function and Control, which assess confidence with functional abilities and managing symptoms, respectively. Each item is rated on a scale from 10 to 100, in increments of 10 (10 = very uncertain, 50 = moderately certain, and 100 = very certain).39 The two subscale scores were formed by averaging the items composing them (range: 10‒100), and a total score was calculated by summing scores on the two subscales (range: 20‒200).40 Higher scores indicate greater self-efficacy.
The MSQOL-54 Cognitive Function subscale contains four items; patients rate the frequency with which they have had problems with cognitive function in the past month on a scale of 1 (all the time) to 6 (none of the time).38 The Cognitive Function score was calculated by first converting each rating item to a 0 to 100 scale, in increments of 20 (0 = all of the time, 20 = most of the time, 40 = a good bit of the time, 60 = some of the time, 80 = a little of the time, 100 = none of the time) and then computing the average of the four items. Higher scores indicate higher cognitive function.
Statistical Analysis
Descriptive statistics were computed for all study variables. Means and standard deviations, or medians and ranges, were calculated for continuous and count variables, and frequency and percentages were calculated for categorical variables.
To derive preference weights for each attribute and attribute level, a hierarchical Bayesian model was fitted to the choice data from the DCE. Point estimates of the hierarchical Bayesian model coefficients represented mean preference weights. Willingness to make trade-offs was assessed by comparing the magnitude of change between levels of one attribute to the magnitude of change between levels in another attribute. At the individual level, the range of each attribute (utility of most favorable level minus utility of least favorable level) was divided by the sum of the ranges of all attributes and multiplied by 100 to calculate the conditional relative importance of each attribute.
Independent-samples t-tests (for two-group comparisons) or one-way analysis of variance tests (for three-group comparisons) were used to evaluate whether relative importance of attributes differed between patients and neurologists, as well as between select subgroups (patients: age, line of therapy, disability [measured by the MSSE, median split], and cognitive function [measured by the MSQOL-54 Cognitive Function scale, median split]; neurologists: years in practice [median split], most frequently prescribed type of MS medication for non-advanced RRMS [injectable vs oral vs both equally], practice type [university/teaching vs community hospital practice], and RRMS patient volume in past 3 months, median split]).
Data were analyzed using SPSS Statistics 23 (IBM Corp., Armonk, NY) for descriptive statistics and subgroup analyses and Lighthouse Studio 2018 Version 9.8.0 (Sawtooth Software, Provo, UT) for the DCE analysis.
Results
A total of 523 patients and 235 neurologists accessed the survey, and 164 patients and 154 neurologists met the inclusion criteria and completed the survey. In effort to ensure the validity of the DCE, data were examined for evidence of potential inattention to responses; respondents were flagged if they showed evidence of straight-lining, completed the survey in less than half of the median length of time, completed the DCE portion in less than half to the median length of time, and/or had two or more illogical responses to the very bad/very good rating items. These checks resulted in 14 patients and 4 neurologists being flagged for potential inattention. Sensitivity analyses were performed by computing the preference weights with and without these respondents and comparing the results; given that at least one of the preference weights differed significantly, these respondents were removed from further analyses. Therefore, the final sample included 150 patients and 150 neurologists.
On average, patients were 54.0 years of age and predominantly female (84.0%). Less than one third (30.7%) were employed, 26.0% were retired, and 24.0% were on long-term disability. The most frequently reported comorbidities included depression (28.7%) and anxiety (24.0%); 82.7% of patients were currently taking a prescription medication for RRMS, with the majority reporting being on an oral (50.0%) or injection (31.5%) medication. Patients reported a fairly high level of certainty in their ability to perform functional tasks and manage symptoms, with a median MSSE Function score of 88.9 (range: 18‒100) and a median MSSE Control score of 65.0 (range: 16‒100). Overall, the median MSQOL-54 Cognitive Function score of 70 (range: 0‒100) indicated that patients in the sample had problems with their cognitive function between “a little of the time” and “some of the time” in the past month (Table 2).
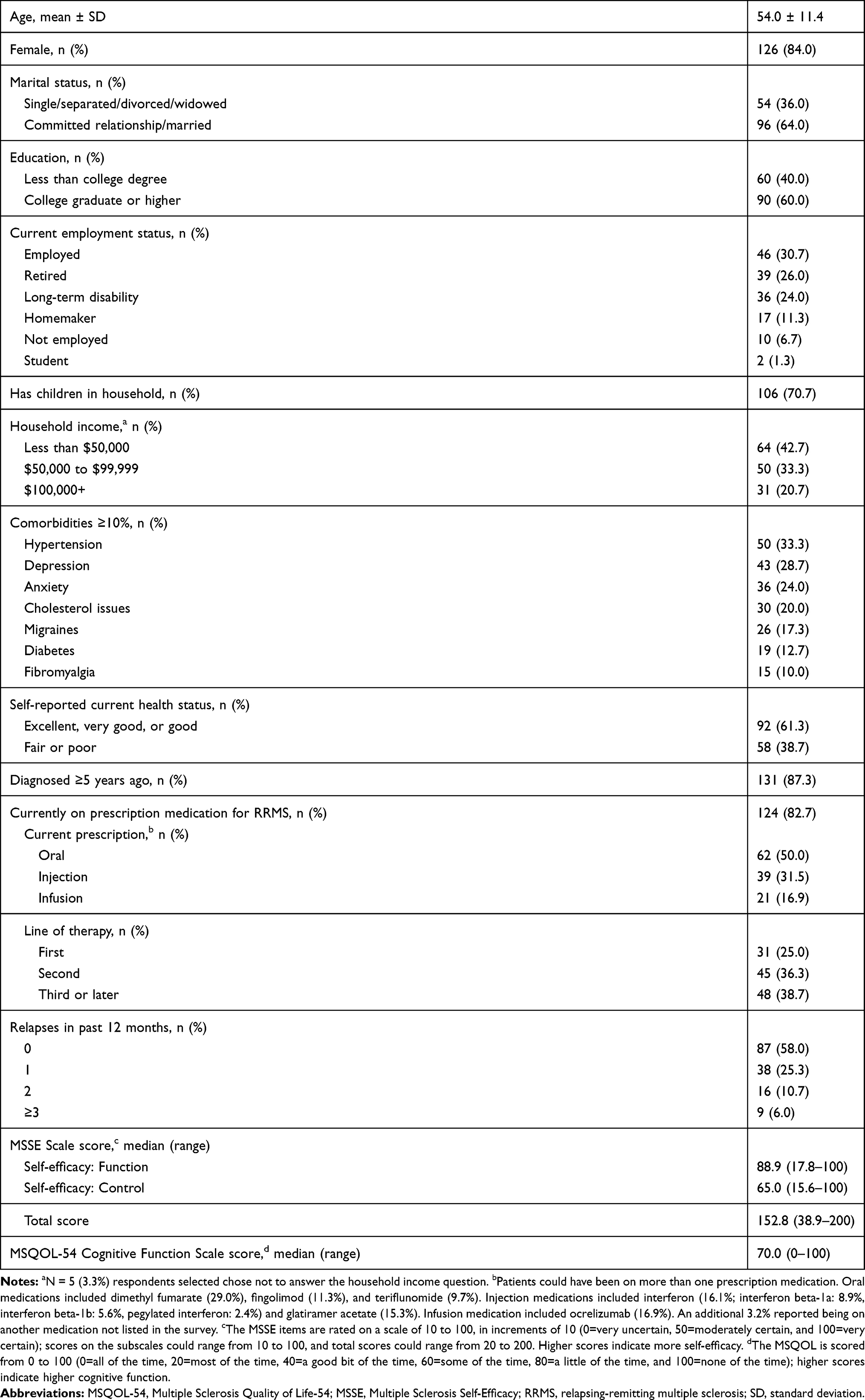 |
Table 2 Patient Characteristics (N=150) |
The majority of neurologists practiced in a nonacademic setting (73.3%), with a mean of 17.4 years in practice, and treated a median of 57 RRMS patients in the past 3 months (Table 3).
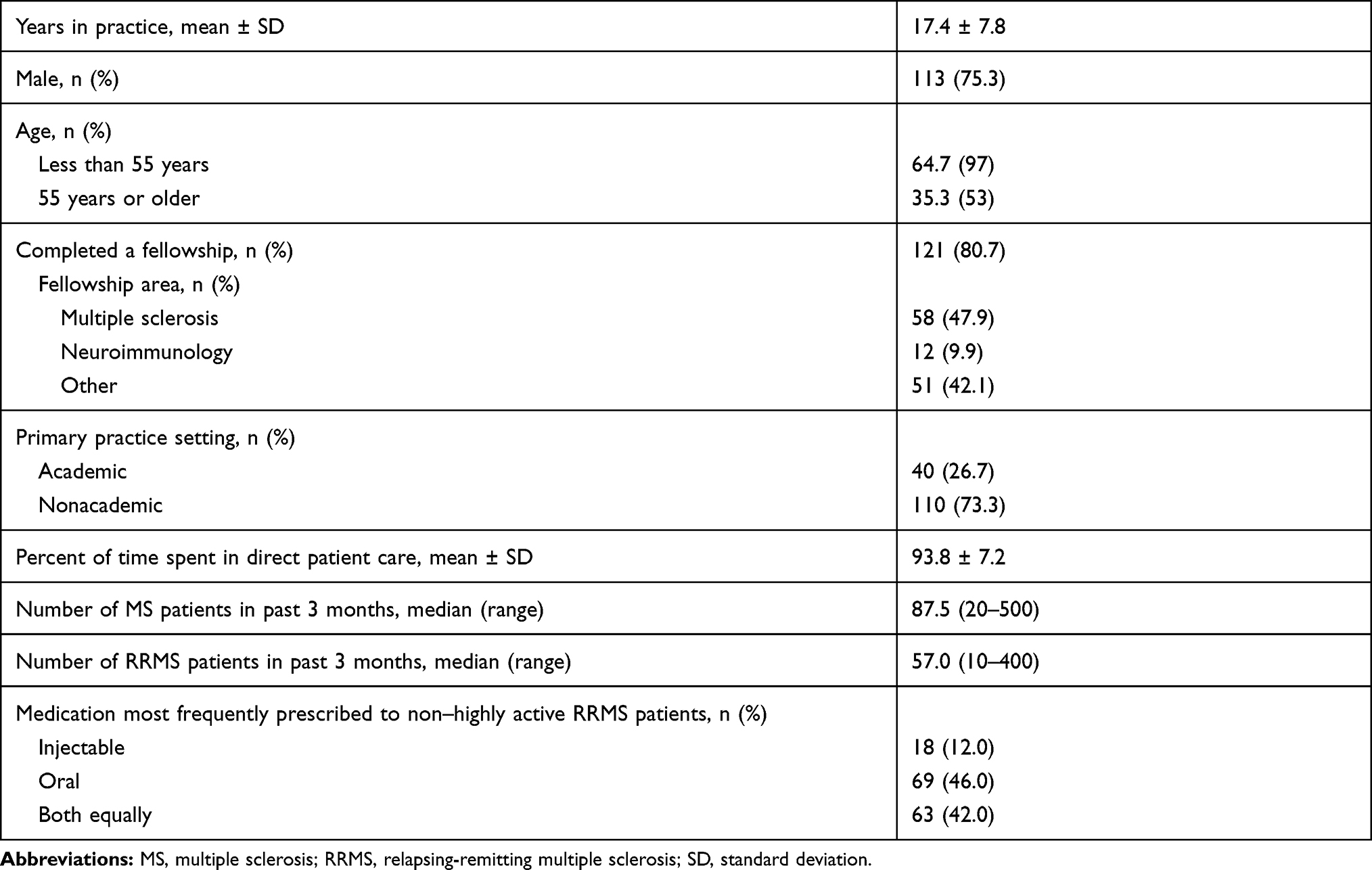 |
Table 3 Neurologist Characteristics (N=150) |
Patient and Neurologist Treatment Preferences
Figure 1 reports relative importance of treatment attributes among patients and physicians. Among patients, the most important treatment attribute was reducing the rate of BVL, followed by the risk of infection and risk of flu-like symptoms. Reducing the rate of BVL was approximately twice as important to patients as reducing the risk of a life-threatening event, the 1-year relapse rate, and the risk of gastrointestinal symptoms. In contrast, the most important treatment attribute among neurologists was reducing the risk of a life-threatening event, followed by slowing the rate of 2-year disability progression and reducing the risk of infection. Reducing the risk of a life-threatening event was approximately twice as important to neurologists as reducing the risk of flu-like symptoms, the risk of gastrointestinal symptoms, and the 1-year relapse rate. Differences in the relative importance of attributes between patients and neurologists, respectively, included rate of BVL (21.1% vs 15.0%; P<0.001), risk of infection (19.7% vs 16.5%; P<0.001), risk of flu-like symptoms (15.9% vs 10.9%; P<0.001), risk of a life-threatening event (11.5% vs 20.6%; P<0.001), rate of 2-year disability progression (15.6% vs 18.5%; P=0.004), and 1-year relapse rate (8.9% vs 10.4%; P=0.005).
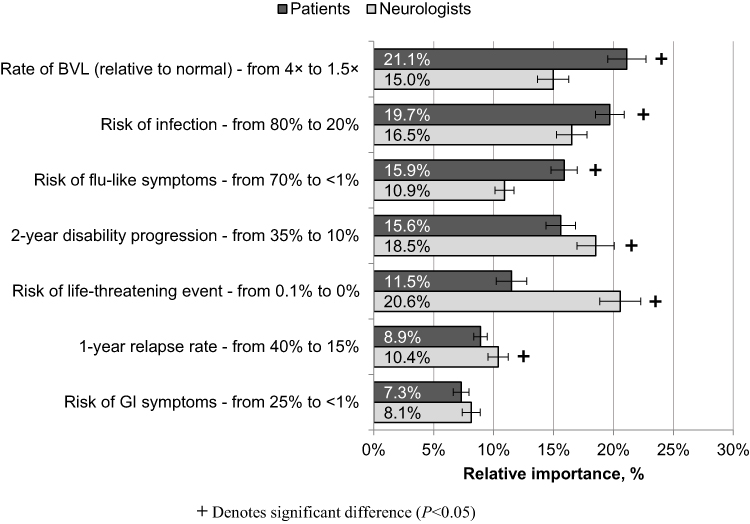 |
Figure 1 Relative importance of treatment attributes. Abbreviations: BVL, brain volume loss; GI, gastrointestinal. Notes: 95% confidence intervals are depicted. |
Figure 2 reports the attribute-level preference weights for patients and neurologists. In general, preference weights increased linearly with improvements across attribute levels. The attribute-level preference weights illustrate the trade-offs that patients and neurologists would be willing to make. For example, patients would be willing to accept an increase in risk of flu-like symptoms from <1% to 30% (change in preference weight: 1.20‒0.43 = 0.77) in exchange for reducing the rate of BVL from 2.5 times to 1.5 times faster than normal (1.85‒0.17 = 1.68). In another example, neurologists would be willing to accept an increase in 2-year disability progression from 10% to 20% (1.22) in exchange for reducing the risk of a life-threatening event from 0.10% to 0.01% (1.91).
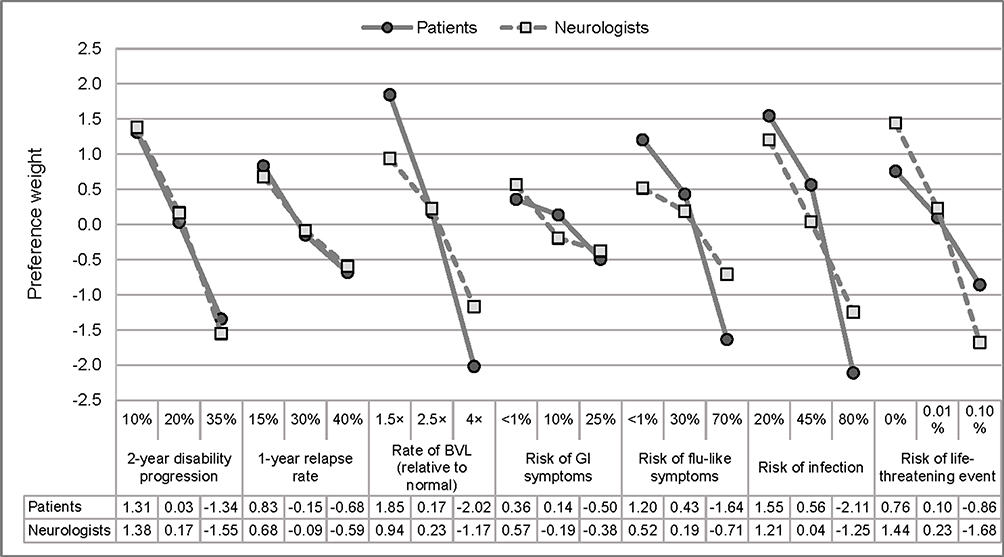 |
Figure 2 Attribute-level preference weights. Abbreviations: BVL, brain volume loss; GI, gastrointestinal. Notes: Preference weights should not be interpreted by themselves. Instead, the magnitude of change within one attribute should be compared to change within another attribute. |
Figure 3 illustrates the value that participants place specifically on BVL relative to changes in the other attributes, showing the amount of worsening in each attribute that patients and neurologists would be willing to accept in exchange for decreasing the rate of BVL from 2.5 times to 1.5 times faster than normal based on attribute-level preference weights. For example, to reduce the rate of BVL from 2.5 times to 1.5 times faster than normal, patients and neurologists would be willing to accept increases of 28% and 14%, respectively, in the 1-year relapse rate (from 15%) and increases of 27% and 17%, respectively, in the risk of infection (from 20%).
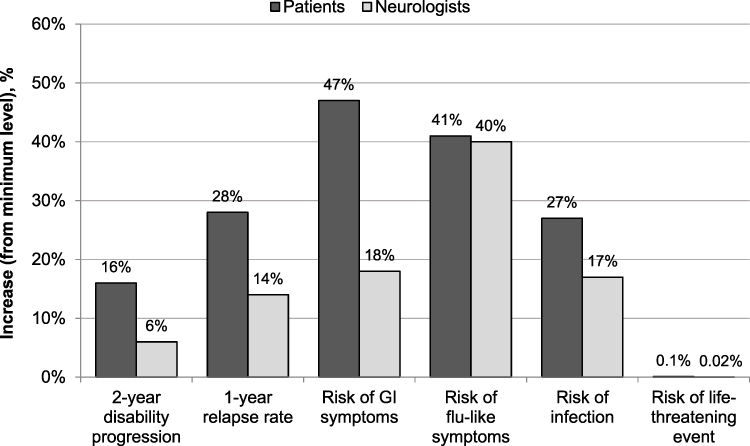 |
Figure 3 Increases in attributes that patients and neurologists are willing to accept in exchange for decreasing rate of BVL from 2.5 times to 1.5 times faster than normal. Abbreviations: BVL, brain volume loss; GI, gastrointestinal. |
Subgroup Analyses
No significant differences in relative importance were found by age, gender, education, line of therapy, disability, and cognitive function among patients or by most frequently prescribed type of MS medication, practice type, and patient volume among neurologists.
Significant differences were identified in the relative importance estimates for risks of a life-threatening event and infection by years in practice (Figure 4). Specifically, although reducing the risk of a life-threatening event was most important to neurologists, regardless of their years in practice, those in practice fewer years (≤17 years) placed greater value on this attribute than those in practice longer (>17 years) (22.3% vs 18.6%, respectively; P=0.036) and valued risk of a life-threatening event more than reducing the rate of 2-year disability progression and the risk of infection. In contrast, neurologists in practice longer (>17 years) valued these three attributes equally.
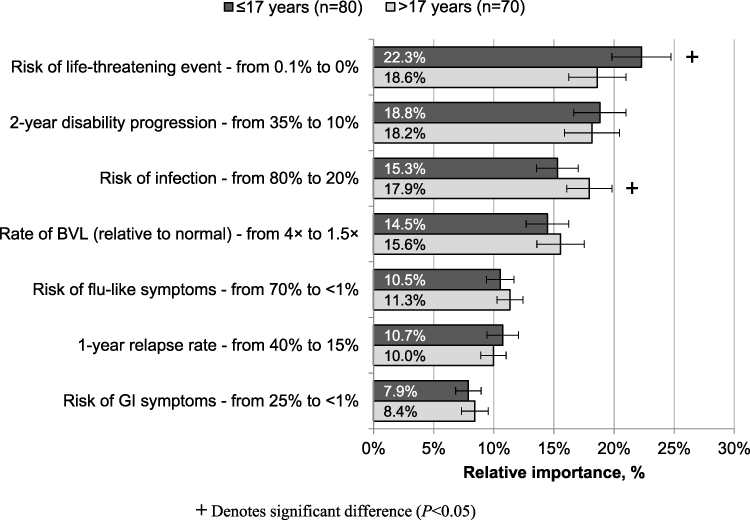 |
Figure 4 Relative importance of treatment attributes: Neurologists by years in practice. Abbreviations: BVL, brain volume loss; GI, gastrointestinal. Notes: 95% confidence intervals are depicted. |
Discussion
This study provides important insight into differences in the perspectives of patients with RRMS and neurologists who treat RRMS in the United States. Whereas patients were most focused on reducing the rate of BVL and the risk of developing infections or flu-like symptoms, neurologists were most focused on reducing the risk of a life-threatening event and slowing the rate of 2-year disability progression.
Differences in treatment priorities between patients and physicians have been observed in other preference studies. For example, in a study of 200 patients with advanced melanoma and 226 treating oncologists, patients valued overall survival over avoidance of adverse events, whereas oncologists were more focused on avoidance of adverse events than overall survival, underscoring potential implications for treatment planning and decision-making in this group.41 In contrast, in a study examining preferences for oral pharmacotherapy for treatment of overactive bladder, patients placed greater value on limiting the risk of side effects, whereas oncologists placed greater value on increasing the benefits.42 In a study of 306 Japanese patients with psoriasis and 161 Japanese treating physicians, preferences were largely similar between patients and physicians; however, patients were influenced by a few key attributes (effectiveness, setting, and availability of a bio-holiday), whereas physicians included a broader range of attributes in their trade-off decision-making.43
Not surprisingly, the current study findings are consistent with those of other preference studies in MS that show preferences are highest for treatments that provide the most improvement with the least risk of side effects.44–46 Nevertheless, patients and neurologists in the current study expressed a willingness to make benefit-risk tradeoffs, as demonstrated by the willingness to accept an increased risk of side effects in exchange for improvements in efficacy. The importance of reducing the rate of BVL among patients is particularly notable given that preference-based studies in MS21–24 have not included this factor in their assessments. BVL has been associated with disease progression and long-term disability;11–14,47,48 thus, it holds notable importance to patients. Furthermore, in prior qualitative research, patients and neurologists cited cognitive functioning as one of the most important impacts of RRMS,27 reinforcing that the associated BVL should be considered in tandem with disability progression and relapse rates in treatment decision-making. The importance of cognitive functioning, which has been associated with BVL, has been observed in other studies of chronic conditions. For example, in a study examining preferences for migraine treatment, patients were willing to pay $59 per month on average to avoid memory problems.49
Patients placed more importance on slowing the rate of disability progression than slowing the relapse rate in the current study. This finding has been similarly observed in prior patient preference studies.45,50,51 However, in a preference study examining patients’ willingness to pay for attributes of DMTs, patients were willing to pay more for a DMT that could reduce the number of relapses in 2 years to one ($2768 per month) than for a DMT that could decrease the percentage of patients who experienced disability progression in 2 years to 1% ($289 per month).44 This difference may be driven by how these attributes were described and the respective levels used; our study examined the importance of reducing the risk of relapsing in the next year from 40% to 10% as opposed to reducing the actual number of relapses in the next year. As such, it could be that relapse rate is more impactful in treatment choice when described in terms of the absolute number of relapses one can expect than when described in terms of percentage risk.
In the current study, physicians also placed more importance on slowing the rate of disability progression than slowing the relapse rate. At first glance, this contradicts findings from a retrospective chart study that found efficacy against relapses was the most predominant driver of treatment choice for RRMS among US patients.52 However, the influence of slowing the progress of disability in treatment selection increased over two-fold from the fourth quarter (Q4) of 2015 to Q4 2017 to become the second most predominant driver of treatment choice. This may reflect a continued upward trajectory of the importance of slowing disability progression in treatment choice. Further, this chart study showed that treatment choices in Q4 2017 were most often made jointly between physicians and patients, indicating the importance of disability progression from the patient perspective. The importance of disability progression was found in another recent preference study conducted with patients and physicians in Germany, in which three groups of physicians differed in their preferences; only in the smallest group (22.2%) was relapse rate more important than disability progression.25
That patients perceived that reducing the risk of a life-threatening side effect as less important than reducing the rate of disability progression is supported by other research, such as a study of 651 patients with MS who were willing to accept increases in the risk of serious adverse events in exchange for improving delays in progression.45 However, patients also prioritized reducing the risk of infection and flu-like symptoms over reducing the risk of life-threatening events, which diverges from prior studies that found patients were more willing to accept increases in the risk of less severe side effects (eg, infection, flu-like symptoms, headaches) over rare but serious side effects.46,53
In contrast with the patients in the current study, the neurologists were most concerned with reducing the risk of a life-threatening side effect. This finding may indicate that US physicians are more risk averse, potentially because of fear of being sued and, as a result, may practice more defensive medicine. This, coupled with the finding that patients were less concerned with the risk of a life-threatening side effect, may lead to differences in the risks that patients and physicians would be willing to accept. Indeed, prior research among MS patients and neurologists in Germany found that patients were willing to accept a higher risk of the potentially life-threatening side effect of progressive multifocal leukoencephalopathy than were neurologists.54
The preferences noted in the current study could have implications for patient care, with our findings suggesting multiple avenues for further research in promoting patient care and quality of life. The routine monitoring of BVL is not currently standard practice, but the importance of BVL could present an opportunity for magnetic resonance imaging to be integrated into clinical practice. Furthermore, given that BVL, disability, and relapses may each be predictors of long-term disease progression, more research is needed to systematically assess the contribution of each risk factor and identify appropriate and effective interventions. This includes the importance of reducing the rate of BVL and the need for novel therapeutic agents that can target this element of disease progression, thus limiting cognitive impairment and promoting long-term functioning. Finally, these results also emphasize the importance of patients and providers both making their preferences explicit during treatment discussions and thus helping to guide shared decision-making and effective care planning. Overall, the study results provide fertile ground for future research examining treatment decision-making in the context of MS and the development of effective interventions to help promote patient care.
This study has limitations. Surveys using a DCE approach rely on participant responses to hypothetical scenarios and, in turn, may not reflect the true preferences of individuals facing such decisions. Despite this inherent limitation, DCE methodology has been widely used and validated in the assessment of treatment preferences and in the context of several disease states. In addition, the patient sample was predominantly female and highly educated; therefore, results may not be generalizable to the entire MS population in the United States. However, it is important to note that preferences did not differ by gender or educational status. Moreover, this study overrepresented physicians under 55 years of age; while 64.7% of neurologists in this study were less than 55 years of age, 45.4% of neurologists in the United States were under 55 years of age in 2017.55 Therefore, results may not be generalizable to the entire neurologist population in the United States. Furthermore, the online survey format may have presented a barrier to those with limited access to online services or lack of comfort with online activities. Whereas efforts were made to recruit a diverse sample of respondents, it is possible that such individuals are underrepresented in the current study.
Conclusion
United States-based patients and neurologists reported different preference profiles for treatment of MS, with patients most concerned with reducing the rate of BVL and their risk of developing infections or flu-like symptoms and neurologists most concerned with reducing the risk of a life-threatening event and slowing the rate of 2-year disability progression. The current study highlights important differences in the treatment preferences of patients and neurologists in the United States, underscoring the importance of considering patients’ perspectives, particularly concerning reducing the rate of BVL, and can help guide shared decision-making and promote effective care of this patient population.
Abbreviations
BVL, brain volume loss; DCE, discrete choice experiment; DMT, disease-modifying therapy; MS, multiple sclerosis; MSQOL-54, Multiple Sclerosis Quality of Life-54; MSSE, Multiple Sclerosis Self-Efficacy; RRMS, relapsing-remitting multiple sclerosis.
Data Sharing Statement
BMS policy on data sharing may be found at https://www.bms.com/researchers-and-partners/independent-research/data-sharing-request-process.html.
Acknowledgments
The authors acknowledge Jenny Cai and Jennifer O’Brien of Kantar Health for assistance with study design and data collection, Errol J. Philip, PhD, for assistance with medical writing, and Peloton Advantage, LLC, an OPEN Health company, for editorial support.
Author Contributions
All authors have made significant contributions to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas. All authors have drafted or written, or substantially revised or critically reviewed, the article; have agreed on the journal to which the article was submitted; have reviewed and agreed on all versions of the article before submission and during revisions, the final version accepted for publication, and any significant changes introduced at the proofing stages; and have agreed to take responsibility and be accountable for the contents of the article.
Funding
This study was sponsored by Bristol Myers Squibb, Princeton, NJ. Third-party medical writing assistance for this manuscript was provided by Errol J. Philip, PhD, a paid consultant of Kantar Health, New York, NY, and editorial support was provided by Peloton Advantage, LLC, an OPEN Health company, Parsippany, NJ, and both were sponsored by Bristol Myers Squibb.
Disclosure
Jinender Kumar and Tom Tencer are employees and shareholders of Bristol Myers Squibb. Janelle Cambron-Mellott, Oliver Will, deMauri S. Mackie, and Kathleen Beusterien are employees of Kantar Health, which received funding from Bristol Myers Squibb to conduct this study. The authors report no other conflicts of interest in this work.
References
1. Lee J, Dunn J. Mobility concerns in multiple sclerosis—studies and surveys on US patient populations of relevance to nurses. US Neurol. 2013;9(1):17. doi:10.17925/USN.2013.09.01.17
2. Feigin VL, Nichols E, Alam T. Global, regional, and national burden of neurological disorders, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459–480. doi:10.1016/S1474-4422(18)30499-X
3. The prevalence of MS in the United States: a population-based estimate using health claims data. Neurology. 2019;93(15):688. doi:10.1212/WNL.0000000000007915
4. Antao L, Shaw L, Ollson K, et al. Chronic pain in episodic illness and its influence on work occupations: a scoping review. Work. 2013;44(1):11–36. doi:10.3233/WOR-2012-01559
5. Schapiro R. Managing the Symptoms of Multiple Sclerosis.
6. Hooper K. Managing progressive MS. National MS society; 2018. Available from: https://www.nationalmssociety.org/NationalMSSociety/media/MSNationalFiles/Brochures/Brochure_Managing_Progressive_MS.pdf.
7. Rae-Grant A, Day GS, Marrie RA, et al. Practice guideline recommendations summary: disease-modifying therapies for adults with multiple sclerosis: report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology. 2018;90(17):777–788. doi:10.1212/WNL.0000000000005347
8. Tran JQ, Hartung JP, Peach RJ, et al. Results from the first-in-human study with ozanimod, a novel, selective sphingosine-1-phosphate receptor modulator. J Clin Pharmacol. 2017;57(8):988–996. doi:10.1002/jcph.887
9. Giovannoni G, Butzkueven H, Dhib-Jalbut S, et al. Brain health: time matters in multiple sclerosis. Mult Scler Relat Disord. 2016;9(Suppl 1):S5–S48. doi:10.1016/j.msard.2016.07.003
10. Bermel RA, Bakshi R. The measurement and clinical relevance of brain atrophy in multiple sclerosis. Lancet Neurol. 2006;5(2):158–170. doi:10.1016/S1474-4422(06)70349-0
11. Eshaghi A, Prados F, Brownlee WJ, et al. Deep gray matter volume loss drives disability worsening in multiple sclerosis. Ann Neurol. 2018;83(2):210–222. doi:10.1002/ana.25145
12. Radue EW, Barkhof F, Kappos L, et al. Correlation between brain volume loss and clinical and MRI outcomes in multiple sclerosis. Neurology. 2015;84(8):784–793. doi:10.1212/WNL.0000000000001281
13. Roosendaal SD, Bendfeldt K, Vrenken H, et al. Grey matter volume in a large cohort of MS patients: relation to MRI parameters and disability. Mult Scler. 2011;17(9):1098–1106. doi:10.1177/1352458511404916
14. Minagar A, Barnett MH, Benedict RH, et al. The thalamus and multiple sclerosis: modern views on pathologic, imaging, and clinical aspects. Neurology. 2013;80(2):210–219. doi:10.1212/WNL.0b013e31827b910b
15. Jacques FH. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology. 2015;84(9):963. doi:10.1212/01.wnl.0000462309.76486.c5
16. Tedeholm H, Lycke J, Skoog B, et al. Time to secondary progression in patients with multiple sclerosis who were treated with first generation immunomodulating drugs. Mult Scler. 2013;19(6):765–774. doi:10.1177/1352458512463764
17. Cohen JA, Comi G, Selmaj KW, et al. Ozanimod vs interferon β-1a: clinical and MRI results of RADIANCE part B - a 2-year phase 3 trial in relapsing multiple sclerosis [abstract 280]. Mult Scler J. 2017;23(3 Suppl):981–982.
18. De Stefano N, Silva DG, Barnett MH. Effect of fingolimod on brain volume loss in patients with multiple sclerosis. CNS Drugs. 2017;31(4):289–305. doi:10.1007/s40263-017-0415-2
19. Khan O, Bao F, Shah M, et al. Effect of disease-modifying therapies on brain volume in relapsing-remitting multiple sclerosis: results of a five-year brain MRI study. J Neurol Sci. 2012;312(1–2):7–12. doi:10.1016/j.jns.2011.08.034
20. Zivadinov R, Dwyer MG, Carl E, Thangavelu K, Cavalier S, Bergsland N. Evaluating the effect of teriflunomide on whole brain atrophy in the phase 3 TOPIC study [abstract P870].
21. Jonker MF, Donkers B, Goossens LMA, et al. Summarizing patient preferences for the competitive landscape of multiple sclerosis treatment options. Med Decis Making. 2020;40(2):198–211. doi:10.1177/0272989X19897944
22. Visser LA, Louapre C, Uyl-de Groot CA, Redekop WK. Patient needs and preferences in relapsing-remitting multiple sclerosis: a systematic review. Mult Scler Relat Disord. 2020;39:101929. doi:10.1016/j.msard.2020.101929
23. Webb EJD, Meads D, Eskyte I, et al. A systematic review of discrete-choice experiments and conjoint analysis studies in people with multiple sclerosis. Patient. 2018;11(4):391–402. doi:10.1007/s40271-017-0296-y
24. Mansfield C, Thomas N, Gebben D, Lucas M, Hauber AB. Preferences for multiple sclerosis treatments: using a discrete-choice experiment to examine differences across subgroups of US patients. Int J MS Care. 2017;19(4):172–183. doi:10.7224/1537-2073.2016-039
25. Poulos C, Wakeford C, Kinter E, Mange B, Schenk T, Jhaveri M. Patient and physician preferences for multiple sclerosis treatments in Germany: a discrete-choice experiment study. Mult Scler J Exp Transl Clin. 2020;6(1):2055217320910778. doi:10.1177/2055217320910778
26. Tullman MJ. A review of current and emerging therapeutic strategies in multiple sclerosis. Am J Manag Care. 2013;19(2 Suppl):S21–27.
27. Tencer T, Will O, Nguyen J, Cambron-Mellott MJ, Berk A, Beusterien K. Neurologist and patient preferences in multiple sclerosis: UK and US qualitative research findings [abstract PND107]. Value Health. 2019;22(3):S757. doi:10.1016/j.jval.2019.09.1877
28. AVONEX (Interferon Beta-1a) Injection [Package Insert]. Cambridge, MA: Biogen; 2020.
29. AUBAGIO (Teriflunomide) Tablets [Package Insert]. Cambridge, MA: Genzyme Corporation; 2020.
30. REBIF (Interferon Beta-1a) [Package Insert]. Rockland, MA: EMD Serono; 2020.
31. Rittmeyer A, Barlesi F, Waterkamp D, et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet. 2017;389(10066):255–265. doi:10.1016/S0140-6736(16)32517-X
32. Vermersch P, Martinelli V, Pfleger C, et al. Benefit-risk assessment of cladribine using multi-criteria decision analysis (MCDA) for patients with relapsing-remitting multiple sclerosis. Clin Ther. 2019;41(2):249–260.e218. doi:10.1016/j.clinthera.2018.12.015
33. TYSABRI (Natalizumab) Injection [Package Insert on the Internet]. Cambridge, MA: Biogen; 2018.
34. COPAXONE (Glatiramer Acetate Injection) [Package Insert]. Parsippany, NJ: Teva; 2019.
35. Novartis. Efficacy and safety of fingolimod in patients with relapsing-remitting multiple sclerosis (FREEDOMS); 2012. Available from: https://clinicaltrials.gov/ct2/show/NCT00289978.
36. Johnson FR, Lancsar E, Marshall D. Constructing experimental designs for discrete-choice experiments: report of the ISPOR Conjoint Analysis Experimental Design Good Research Practices Task Force. Value Health. 2013;16(1):3–13. doi:10.1016/j.jval.2012.08.2223
37. Schwarz R. [Stress and depression are not causes of cancer]. Strahlenther Onkol. 1996;172(11):632–633. German.
38. Vickrey BG, Hays RD, Harooni R, Myers LW, Ellison GW. A health-related quality of life measure for multiple sclerosis. Qual Life Res. 1995;4(3):187–206. doi:10.1007/BF02260859
39. Schwartz CE, Coulthard-Morris L, Zeng Q, Retzlaff P. Measuring self-efficacy in people with multiple sclerosis: a validation study. Arch Phys Med Rehabil. 1996;77(4):398. doi:10.1016/S0003-9993(96)90091-X
40. Chiu CY, Motl RW. Further validation of the Multiple Sclerosis Self-Efficacy Scale. Disabil Rehabil. 2015;37(26):2429–2438. doi:10.3109/09638288.2015.1021022
41. Liu FX, Witt EA, Ebbinghaus S, et al. Patient and oncologist preferences for attributes of treatments in advanced melanoma: a discrete choice experiment. Patient Prefer Adherence. 2017;11:1389–1399. doi:10.2147/PPA.S140226
42. Heisen M, Baeten SA, Verheggen BG, et al. Patient and physician preferences for oral pharmacotherapy for overactive bladder: two discrete choice experiments. Curr Med Res Opin. 2016;32(4):787–796. doi:10.1185/03007995.2016.1142959
43. Bolt T, Kobayashi H, Mahlich J. Patient and physician preferences for therapy characteristics for psoriasis: a discrete choice experiment in Japan. Pharmacoecon Open. 2019;3(2):255–264. doi:10.1007/s41669-018-0104-1
44. Frost N, Freeman J, Brixner D, Mort J, Clem J, Ngorsuraches S. Patients’ preferences and willingness-to-pay for disease-modifying therapies. Mult Scler Relat Disord. 2019;35:55–60. doi:10.1016/j.msard.2019.07.005
45. Johnson FR, Van Houtven G, Ozdemir S, et al. Multiple sclerosis patients’ benefit-risk preferences: serious adverse event risks versus treatment efficacy. J Neurol. 2009;256(4):554–562. doi:10.1007/s00415-009-0084-2
46. Wilson L, Loucks A, Bui C, et al. Patient centered decision making: use of conjoint analysis to determine risk-benefit trade-offs for preference sensitive treatment choices. J Neurol Sci. 2014;344(1–2):80–87. doi:10.1016/j.jns.2014.06.030
47. Horakova D, Kalincik T, Dusankova JB, Dolezal O. Clinical correlates of grey matter pathology in multiple sclerosis. BMC Neurol. 2012;12:10. doi:10.1186/1471-2377-12-10
48. Popescu BF, Lucchinetti CF. Meningeal and cortical grey matter pathology in multiple sclerosis. BMC Neurol. 2012;12:11. doi:10.1186/1471-2377-12-11
49. Mansfield C, Gebben DJ, Sutphin J, et al. Patient preferences for preventive migraine treatments: a discrete-choice experiment. Headache. 2019;59(5):715–726. doi:10.1111/head.13498
50. Poulos C, Kinter E, Yang JC, Bridges JF, Posner J, Reder AT. Patient preferences for injectable treatments for multiple sclerosis in the United States: a discrete-choice experiment. Patient. 2016;9(2):171–180. doi:10.1007/s40271-015-0136-x
51. Wilson LS, Loucks A, Gipson G, et al. Patient preferences for attributes of multiple sclerosis disease-modifying therapies: development and results of a ratings-based conjoint analysis. Int J MS Care. 2015;17(2):74–82. doi:10.7224/1537-2073.2013-053
52. Brown H, Gabriele S, White J. Physician and patient treatment decision-making in relapsing-remitting multiple sclerosis in Europe and the USA. Neurodegener Dis Manag. 2018;8(6):371–376. doi:10.2217/nmt-2018-0023
53. Bauer B, Brockmeier B, Devonshire V, Charbonne A, Wach D, Hendin B. An international discrete choice experiment assessing patients’ preferences for disease-modifying therapy attributes in multiple sclerosis. Neurodegener Dis Manag. 2020;10(6):369–382. doi:10.2217/nmt-2020-0034
54. Heesen C, Kleiter I, Nguyen F, et al. Risk perception in natalizumab-treated multiple sclerosis patients and their neurologists. Mult Scler. 2010;16(12):1507–1512. doi:10.1177/1352458510379819
55. Association of American Medical Colleges. Active physicians by age and specialty; 2017. Physician Specialty Data Report. Available from: https://www.aamc.org/data-reports/workforce/interactive-data/active-physicians-age-and-specialty-2017.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.