")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 13
Pathogenic beliefs among patients with depressive disorders
Authors Neelapaijit A, Wongpakaran T , Wongpakaran N , Thongpibul K
Received 5 March 2017
Accepted for publication 24 March 2017
Published 10 April 2017 Volume 2017:13 Pages 1047—1055
DOI https://doi.org/10.2147/NDT.S136212
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Wai Kwong Tang
Adam Neelapaijit,1 Tinakon Wongpakaran,1 Nahathai Wongpakaran,1 Kulvadee Thongpibul2
1Department of Psychiatry, Faculty of Medicine, 2Department of Psychology, Faculty of Humanities, Chiang Mai University, Thailand
Introduction: Pathogenic belief is a central construct within control-mastery theory, which is an integrated dynamic-cognitive-relational approach in psychotherapy. Pathogenic beliefs result from traumatic life experiences and are considered the root of any psychological disorders presented clinically. Nevertheless, how and what type of pathogenic beliefs are attributed to clinical depressive disorder is unknown. The present study aimed to examine this issue.
Patients and methods: Thirty patients with depressive disorder, who came for psychotherapy at a psychotherapy clinic, were matched based on age and gender with healthy controls who were medical students. The 54-item pathogenic belief scale (PBS) was administered and compared between depressive and control groups using odds ratio (OR).
Results: The depressed group’s PBS mean score was significantly higher than the healthy controls (t=3.78, P<0.001). Thirteen of 54 items significantly differed between the two groups with ORs ranging from 3.76 to 16.79. The content of pathogenic beliefs centered on the issues of negative sense of self, lack of self-efficacy and control, and relational difficulties related to feelings of fear and humiliation. Influences of culture and gender differences on pathogenic beliefs were discussed.
Conclusion: Pathogenic beliefs relate to depression such that the higher the number of pathogenic beliefs one has, the more the likelihood of having depression. Since the PBS was developed based on clinical data (rather than theory based), cultural issues as well as age and gender may influence the development of pathogenic beliefs. Further study should be warranted and implications for clinical practice are discussed.
Keywords: pathogenic beliefs, control-mastery therapy, depressive disorders, CMT, pathogenic belief scale
Introduction
Control mastery theory (CMT) is a dynamic-cognitive-relational psychotherapy grounded on the premise that psychopathology is caused by pathogenic beliefs. Pathogenic beliefs are the incapacitating and dysfunctional concepts of oneself and others that interfere with healthy interpersonal functioning.1 They are patterns of thought that were developed over time based on a person’s experiences, observations and conscious and unconscious beliefs. These belief systems and interpretations often parallel those of a person’s parents, guardians or other caregivers. For example, a child who was raised by controlling parents may adopt certain beliefs that he/she should yield to the desire of and defer to others instead of pursuing his/her own ideas, needs or interests.
In some instances, pathogenic beliefs are developed by guilt. The types of guilt related to pathogenic beliefs include separation, survival and surpass guilt. From a psychoanalytic perspective, unconscious guilt is a product of repressed irrational beliefs derived from traumatic childhood experiences.2 In psychotherapy, guilt can be a source of resistance and transference, and patient’s unconscious efforts to master problems with guilt can manifest through an ongoing process of testing by the patient. Therapeutic outcome significantly depends on the degree to which therapists accurately analyze patients’ tests of their guilt-based resistances and transferences.2
However, some guilt may be related to culture. For example, in a collectivistic culture like Asia, individuals may experience separation guilt when he/she is the last person to leave his/her parents or family. Individuals with mental issues frequently experience a contention between self-intrigue and sympathy toward others, bringing about maladaptive interpersonal guilt, especially those associated with guilt, shame and submission.3 Although guilt may be a part of depression, research has shown that it could be independent and is concerned with culture.4,5
Individuals who experience psychological distress rooted from pathogenic beliefs typically have severe levels of or multiple pathogenic beliefs. This pushes them to seek psychological treatment.6,7
Beck’s cognitive behavioral model and Young’s early maladaptive schema are compared below.8,9 Based on Beck’s cognitive theory, people who have negative cognitive schemas or core beliefs have higher risk of developing depression, especially when a stressful life event occurs. However, Young’s schema theory expands Beck’s theory to clients who are treatment resistant in not only the core beliefs they have but they are also thought to be preserved by complex characterological underlying. Young et al have identified 18 early maladaptive schemas. The schemas are broad, pervasive character traits illustrated by differing beliefs that develop during childhood in reaction to early traumatic experiences – the same concept as pathogenic beliefs.10 While in Beck’s cognitive model, core beliefs relating to depression center on various kinds of negative senses of the self; Young’s schema has delineated different schemas that relate to depression such as abandonment/instability (the perceived instability or unreliability of significant others) and defectiveness/shame (the belief that one is defective, flawed, unwanted, or unlovable).11
Although all these mentioned beliefs may look similar, CMT (that is based on psychoanalytic theory) proposed that the beliefs are not necessarily false, and they can be stored in both conscious and unconscious levels of the mind.6 These beliefs are affect-laden and obstruct an individual’s goals in life.1
Pathogenic beliefs were used in clinical case studies, for example, substance abuse, nightmare disorder, posttraumatic stress disorder and depressive disorder.12–15 Nevertheless, among clinical disorders, depressive disorder is the leading cause of global burden of diseases and a global health priority.16 Even though psychopharmacological agents are effective for the treatment of depressive disorder,17 ~10% to 20% of patients do not achieve complete recovery and meet the criteria of treatment resistance.18,19 Even though treatment-resistant depression has been documented to be treated effectively by either using pharmacotherapy or cognitive therapy, the cause of this disorder remains unclear.20,21 How pathogenic beliefs can be attributed to treatment-resistant depression is not yet clear. Pathogenic beliefs among depressed individuals have, in fact, never been empirically reported, particularly when compared with nondepressed individuals.
This study is aimed at examining the differences in the number of pathogenic beliefs between clinically depressed and healthy participants. The authors hypothesized that the number of pathogenic beliefs among clinically depressed participants should be higher than those among healthy subjects. In addition, the authors would like to explore which pathogenic beliefs increase the likelihood of having depressive disorder, given the influence of culture and gender.
Patients and methods
Sixty-seven patients with a diagnosis by psychiatrists of major depressive disorder, according to Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-IV) diagnostic criteria, completed the pathogenic belief scale (PBS) at baseline between January 2007 and December 2016 before beginning psychotherapy and were included in the study. Additionally, 94 fourth-year medical students who completed the PBS as part of their personal development activities in the curriculum were matched by age and gender. This study was bound by the ethics tenets of the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of the Faculty of Medicine, Chiang Mai University. Due to its nature of retrospective review, informed consent was exempted by the IRB. There was no identifying information linked to the survey data.
Measurement
PBS
PBS was developed by the San Francisco Psychotherapy Research Group (SFPRG).22 According to Silberschatz et al, PBS was developed from clinical data collected by therapists from psychotherapy cases and was not designed to test theoretical models or identify diagnostic categories such as depression or anxiety.23
The SFPRG seeks to improve the practice of psychotherapy through the further development of CMT. PBS was originally intended to be used by therapists to assess the patient’s pathogenic beliefs. The authors were granted permission by the PBS creator to translate the PBS to Thai. The authors first translated the original English version of the PBS to Thai, then an English–Thai bilingual school teacher with no knowledge of the wording of the original English version back-translated the Thai version of the PBS to English. The two versions were then compared item-by-item and corrected for discrepancies by consensus of all translators.
The PBS was later modified as self-reporting questionnaires with all statements remaining the same. It totaled 54 statements with three possible responses.24 The PBS asked the respondents to rate whether or not they agreed with that particular statement. The respondents could choose to answer “no” (1), “uncertain” (2), or “yes” (3), in contrast to a 5- or 6- point Likert scale used in other studies.23,25 We used the 3-point rating scale because we thought it made sense clinically to learn whether given beliefs existed or not. However, we opened the opportunity to the “preconscious process” by allowing the respondents to answer “not sure” in case they did not feel strongly enough about it.
In terms of psychometric property, PBS yielded an excellent internal consistency with Cronbach’s alpha coefficient of 0.92. According to Silberschatz et al, PBS was seen as a one-factor model.23 In the present sample, PBS provided a good fit as a unidimensional model because the data analyzed using the chi-square test of model fit were 1,423.064, df 1,325, P=0.0305, root mean square error of approximation was 0.021 (90% confidence interval [CI], 0.007 to 0.030); comparative fit index =0.957; Tucker–Lewis index =0.955 and weighted root mean square residual =0.959.
Data analysis
The depressed patients and healthy controls were compared in terms of demographic data using descriptive statistics, for example, mean, standard deviation and percentage. Because both groups of depressed patients and healthy students were unequal with regard to gender and age distribution, it may have led to bias in comparison between the two groups. We, therefore, adopted a case–control matching procedure, which was used to randomly match cases and controls based on age and gender using MedCalc software (Mariakerke, Belgium). This yielded a good match of 30 cases in each group (60 in total). The differences between the two groups were evaluated by the Student’s t-test for continuous data, and the Mann–Whitney U test was used for noncontinuous data. The differences in the distribution of noncontinuous data across the groups were evaluated using odds ratio (OR). P<0.05 was considered statistically significant in all analyses.
To capture the existence of any given item and make it easier for interpretation, we choose only the response “yes” as “positive”, while the response “not sure” was regarded as “negative” – the same as “no” response. This analysis was carried out using Mplus 7.4 software (Muthén & Muthén, Los Angeles, CA, USA).
Results
Participants’ characteristics
The mean age of the participants was 22.53±2.19 years for the 30 depressed subjects and 21.97±1.07 years for the 30 control subjects. No significant difference was found between the groups regarding mean age. A total of 15 males and 15 females were enrolled in the depressed and control groups. The depressed sample had significantly higher PBS total score than the control group, with the mean and standard deviation (SD) =13.17±8.54 and 5.63±6.27, respectively, Mann–Whitney U test z=−6.55, P<0.001 for the depressed and the control group (Table 1).
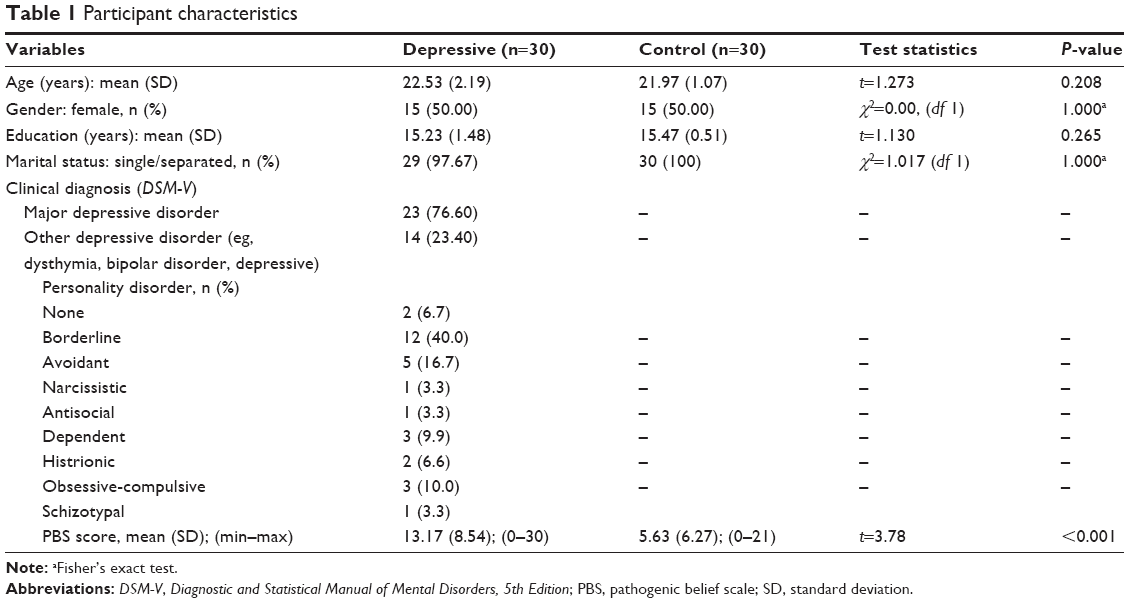 | Table 1 Participant characteristics |
The three most common pathogenic belief items that were endorsed “yes” were item 54, “being burdened, overworked or a martyr is a mark of virtue” (41.67%); item 20, “disagreeing with others will result in contemptuous, angry and rejecting reactions” (40.00%); item 1, “I need to defer to others instead of pursuing my own ideas, needs or interests”; and item 31, “I must remain excessively involved with parents or loved ones because separation would be hurtful, disloyal or make them feel abandoned” (35.00%). In contrast, the least common was item 4, “it is wrong, threatening or disloyal to surpass parents, siblings or significant others” (3.33%); item 16, “I deserve to be mistreated and therefore put myself in self-destructive or abusive situations/relationships”; and item 47, “if I am too sexy, others will feel envious, put me down or threatened”.
Of 54 items, 13 items were found to significantly differ between the two groups (OR ranged from 3.76 to 16.79). The top three OR scores were 16.79 (item 26, “others are superior or more competent than I am”), OR 16.79 (item 22, “I am different from other people, isolated from the rest of the world and/or not part of any group or community”), OR 12.43 (item 3, “I am physically fragile, vulnerable and unhealthy”) and OR 12.25 (item 8, “others will hurt, abuse, humiliate, cheat or manipulate me”) (Table 2).
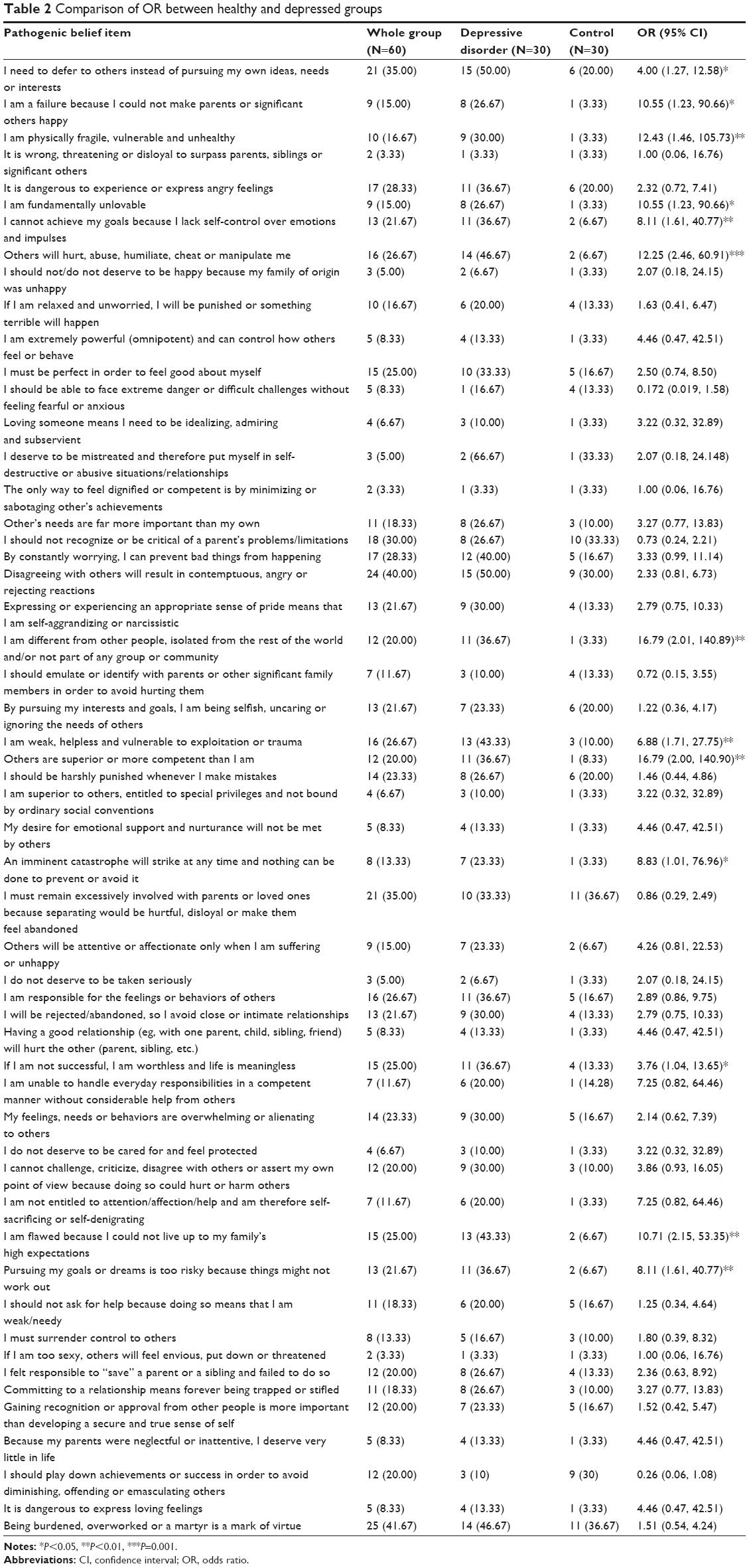 | Table 2 Comparison of OR between healthy and depressed groups |
When comparing PBS between genders, no significant difference was found except for item 54 (“being burdened, overworked or a martyr is a mark of virtue”) by the odds of 0.28 (95% CI, 0.09 to 0.82), denoting this belief 3.6 times more stronger in males than females.
Discussion
As hypothesized, the number of pathogenic beliefs was higher in the depressed group than in the healthy control group. This was supported by a number of studies with regard to the maladaptive belief effect on depression.26–28 The 13 pathogenic belief items that significantly differed between the depressed and healthy control groups focused on how the individuals felt bad about themselves, how effectively they could control the situation and how vulnerable they felt in relation to others. The adjectives found among those 13 items included “defer to others”, “failure”, “vulnerable”, “unlovable”, “lack self-control”, “isolated”, “being hurt/humiliated”, “inferior”, “catastrophe”, “worthless”, “not entitled”, “flawed” and “impossible goal”. In addition, the most influential adjectives were “isolated”, “inferior”, “vulnerable” and “being hurt”, in ranked order. All these 13 beliefs or feelings can be categorized in three areas, 1) negative sense of self, 2) self-efficacy/sense of control, and 3) relational difficulties (being humiliated/isolated/surrender behavior). All these mentioned beliefs have long been documented as fundamental for depression, which were strongly confirmed by other theories/models.29–33 For example, maladaptive beliefs can predict depression based on the following areas: approval, achievement and perfectionism.28 The results are also consistent with the studies of Young’s early maladaptive schemas, which found that all 18 schemas were significantly correlated with depression. For example, in one study with a mixed clinical sample, depression was related to defectiveness/shame (the belief that one is defective, bad, flawed, unwanted or unlovable), subjugation (the excessive surrendering of control to others to avoid anger, retaliation or abandonment) and self-sacrifice (the excessive focus on meeting the needs of others). However, in another study involving a nonclinical sample, depression was related to dependence/incompetence (the belief that one is unable to handle one’s everyday responsibilities in a competent manner, without considerable help from others), vulnerability to harm or illness (the belief that catastrophe is about to strike at every moment), dependency (the belief that one is unable to take care of oneself and needs help from others to handle one’s everyday responsibilities) and failure (the belief that one is fundamentally inadequate compared with others in areas of achievement).11 Taken together, the beliefs among all three models with regard to depression have much in common.
Having pathogenic beliefs does not necessarily mean that one will have depression. On the contrary, some participants who have depression may not report a considerable number of pathogenic beliefs. As we may see, most PBS scores could not help differentiate between those with depressive disorder and healthy controls. This does not necessarily mean that the pathogenic beliefs did not contribute to depression. Rather, individuals who remain healthy may have sufficient coping strategies.34 In addition, personality trait or affective temperament, endorsed by related reports, may be involved in determining such a relationship.35,36 The dysfunctionality related to level of pathogenic belief was not evaluated directly in this study, as the response was dichotomous. Because PBS is a unidimensional model, it allows us to use sum scores to indicate the severity of depression, that is, the number of PBS items should reflect the severity of psychopathology. In other words, the more pathogenic beliefs found, the more severe the psychological distress. The possible cutoff score for depression is, however, an interesting subject for future research.
Some invalid items of pathogenic beliefs that were unable to predict depression may reflect cultural issues. For example, a related report showed that Korean and Asian–American parents endorsed more emotional control than those of European–American parents.37 With respect to guilt, which plays a role in pathogenic belief,38 we found that two of three guilt-derived items significantly differed between the two groups. These included item 1, “I defer to others” (reflecting survivor guilt) and item 43, “I am flawed because I could not live up to my family’s high expectations” (reflecting omnipotent guilt). These results may be attributed to the fact that the studied sample was rather young. Finding omnipotent and surpass guilt rather than separation guilt was more likely and may be found more among older age Thai subjects. The fact that item 54, “being burdened, overworked or a martyr is a mark of virtue” did not significantly differ between two groups may be attributed to cultural diversity as well. As we have already known, Thailand and some other Asian countries are collectivistic societies influenced by Buddhism, in which gratefulness and humbleness are the hallmark of decency and practical social virtues. Some pathogenic beliefs seem to be consistent with these social values such as the belief that “the others-come-first ideology”, with a main concern that their chosen course of action benefit others and not themselves (Thai concept: Kreng-jai).39 However, the term “pathogenic belief” is defined as the belief that is affect-laden and energized that obstructs one’s goal. Thus, whether or not item 54 is valid as a pathogenic belief among Thai subjects requires further exploration. Moreover, pathogenic beliefs among individuals from diverse cultural backgrounds need to be explored.
Gender differences also play a role in developing depression. No related study has reported with regard to the influence of gender on pathogenic beliefs and depression. You et al used dysfunctional attitudes to explore the relationship between gender and depression and found that it had a moderating role on lifetime history of depression and differing effects were found between men and women.40 Gender differences should be explored based on different cultural backgrounds as well. With regard to the Thai sample, it should be said that Thais expect men to be stronger and more responsible as a family leader than women.41 This is echoed in item 54, “being burdened, overworked or a martyr is a mark of virtue”, because men had a higher OR than women to endorse this item. Compared with Chinese populations, men (more than women) are urged to take care of their frail older adults while this issue may be reversed among Thais.42 Therefore, how a pathogenic belief develops in the light of cultural and gender differences is an interesting issue to be examined.
Another important subject that needs to be further examined is whether pathogenic beliefs exist only in acute depression (state marker) or whether they persist even in remission (trait marker). This interesting point should be addressed in a follow-up or a longitudinal study.
Apart from being a predictor for depression, pathogenic belief has also been investigated for mediation effect between negative parenting style, that is, abuse, neglect and intrusiveness and development of psychopathology, that is, anxiety, low self-esteem, emotional instability, pessimistic attitude and depression. Silberschatz et al found that pathogenic beliefs mediated the relationship between negative parenting style and psychopathology in that the significant initial relationship between the negative parenting style and psychopathology became nonsignificant after controlling for the mediator PBS.23
The strength of this present study is that it demonstrates that there may be pathogenic beliefs specific to disorder as well as a possibility to use PBS as a screening tool for depression when a cutoff score can be obtained. According to CMT, pathogenic beliefs attributed to personality traits or personality disorder can be formed. Personality is a predisposing factor for developing a clinical disorder, especially when combined with other factors such as overwhelming stress or lack of social support.43–45 Using PBS also creates the opportunity to explore relationship between personality traits, disorders and pathogenic beliefs, which have never been studied before.
Limitations
This study had several limitations. First, because of the retrospective design of the study, some clinical data that were importantly involved in the study such as severity of depressive disorder (obtained by Hamilton rating scale of depression) were not recorded and quite possibly severity of depression may be related to a number of pathogenic beliefs.
Second, the results cannot be generalized to many populations with depressive disorder as the mean age of the matched samples was rather young, so replication study should be conducted. Third, although a self-reporting version of PBS has been introduced for clinical use,23,25 it has not yet been validated as to what extent it agrees with pathogenic beliefs derived from clinicians or interviewers. Fourth, the way the PBS was dichotomized in two responses (positive and negative) where “not sure (response =2)” was ignored, might be a possible source of bias. How much weight should be given to a particular item remains unclear. Moreover, in terms of item ability, even though all 54 pathogenic belief items fit well with the one-factor model, further testing with item ability, for example, using the Rasch method, may be useful to reduce some redundant items that would make the self-reporting version briefer and more convenient to use.
Finally, even though we intended to explore patients with depressive disorder, not all depressive disorders, for example, major depressive disorder, dysthymic disorder and bipolar depression have the same biological and psychodynamic development. Specific disorders may be useful to study. More importantly, personality factors, which may relate to pathogenic beliefs, should also be further examined.
Conclusion
Pathogenic beliefs were related to depression such that the higher the number of pathogenic beliefs one has, the greater the likelihood one will experience depression. Significant pathogenic beliefs that predict depression concern issues of a negative sense of self, self-efficacy/sense of control and relational problems (exhibiting humiliated/isolated/surrender behaviors). Some pathogenic beliefs are culture related while some are gender related. Replication studies should be encouraged, especially comparing cultures, ages and genders. Not only were pathogenic beliefs significantly related to depression but also served as a mediator for developing psychopathology among individuals, who perceived negative parenting styles. One clinical implication of this study was that clinicians may screen for pathogenic beliefs, particularly along with negative parenting style. This might help identify individuals at risk and provide appropriate interventions to reduce the possibility of developing subsequent psychopathology. Pathogenic beliefs center on relationships with significant persons, so involving family members, especially parents or caregivers, in a session together with a professional may help. This may allow all family members to be aware of the existence of risk for developing psychopathology and discover ways to work further to reduce pathogenic beliefs.
Disclosure
The authors report no conflicts of interest in this work.
References
Silberschatz G, editor. Transformative Relationships. New York, NY: Taylor & Francis; 2005. | ||
Bush M. The role of unconscious guilt in psychopathology and psychotherapy. Bull Menninger Clin. 1989;53(2):97–107. | ||
O’Connor LE, Berry JW, Weiss J, Gilbert P. Guilt, fear, submission, and empathy in depression. J Affect Disord. 2002;71(1–3):19–27. | ||
Venkoba Rao A. Depressive illness and guilt in Indian culture. Asian J Psychiatr. 2009;2(2):84–86. | ||
APA. Diagnostic and Statistical Manual of Mental Disorders. 5th (DSM-5) ed. Washington DC: American Psychiatric Association; 2013. | ||
Weiss J. How Psychotherapy Works. New York, NY: Guilford; 1993. | ||
Shulman K. Clock-drawing: is it the ideal cognitive screening test? Int J Geriatr Psychiatry. 2000;15(6):548–561. | ||
Beck AT. Cognitive Therapy and The Emotional Disorders. New York, NY: International University Press; 1976. | ||
Young JE. Cognitive Therapy for Personality Disorders: A Schema-Focused Approach. Sarasota, FL: Professional Resource Exchange; 1990. | ||
Young JE, Klosko JS, Weishaar ME. Schema Therapy: A Practitioner’s Guide. New York, NY: The Guilford Press; 2003. | ||
Hawke LD, Provencher MD. Schema theory and schema therapy in mood and anxiety disorders: a review. J Cogn Psychother. 2011;25(4):257–276. | ||
Lieb RJ, Young NP. A case-specific approach to the treatment of alcoholism: the application of control mastery theory to alcoholics anonymous and professional practice. J Subst Abuse Treat. 1994;11(1):35–44. | ||
Pole N, Bloomberg-Fretter P. Using control mastery therapy to treat major depression and posttraumatic stress disorder. Clin Case Stud. 2006;5(1):53–70. | ||
Wongpakaran T, Wongpakaran N. Using Control Mastery Therapy with Borderline Patients. 2013. Accessed February 14, 2017. | ||
Wongpakaran T, Elsegood K, Wongpakaran N, Wannarit K, Promkumtan P. Using control-mastery and jungiantheories to treat nightmare disorder: a case from Thailand. J Ment Health Couns. 2014;36(3):189–207. | ||
Ferrari AJ, Charlson FJ, Norman RE, et al. Burden of depressive disorders by country, sex, age, and year: findings from the global burden of disease study 2010. PLoS Med. 2013;10(11):e1001547. | ||
Dold M, Kasper S. Evidence-based pharmacotherapy of treatment-resistant unipolar depression. Int J Psychiatry Clin Pract. 2017;21(1):13–23. | ||
Fava M, Rush AJ, Wisniewski SR, et al. A comparison of mirtazapine and nortriptyline following two consecutive failed medication treatments for depressed outpatients: a STAR*D report. Am J Psychiatry. 2006;163(7):1161–1172. | ||
Petersen T, Gordon JA, Kant A, Fava M, Rosenbaum JF, Nierenberg AA. Treatment resistant depression and axis I co-morbidity. Psychol Med. 2001;31(7):1223–1229. | ||
Serafini G, Howland RH, Rovedi F, Girardi P, Amore M. The role of ketamine in treatment-resistant depression: a systematic review. Curr Neuropharmacol. 2014;12(5):444–461. | ||
Carvalho AF, Berk M, Hyphantis TN, McIntyre RS. The integrative management of treatment-resistant depression: a comprehensive review and perspectives. Psychother Psychosom. 2014;83(2):70–88. | ||
Curtis J, Silberschatz G, Sampson H, Weiss J. The planformulation method. Psychother Res. 1994;4(3–4):197–207. | ||
Silberschatz G, Aafjes-van Doorn K. Pathogenic beliefs mediate the relationship between perceived negative parenting and psychopathology symptoms. J Aggress Maltreat Trauma. 2016:1–18. | ||
Setiati S, Harimurti K, Dewiasty E, Istanti R. Predictors and scoring system for health-related quality of life in an Indonesian community-dwelling elderly population. Acta Med Indones. 2011;43(4):237–242. | ||
Sammet I, Leichsenring F, Schauenburg H, Andreas S. Self-ratings of pathogenic beliefs: a study based on the psychodynamic control-mastery theory. Psychother Res. 2007;17(4):494–503. | ||
Kërqeli A, Kelpi M, Tsigilis N. Dysfunctional attitudes and their effect on depression. Procedia Soc Behav Sci. 2013;84:196–204. | ||
Köhler S, Unger T, Hoffmann S, Mackert A, Ross B, Fydrich T. Dysfunctional cognitions of depressive inpatients and their relationship with treatment outcome. Compr Psychiatry. 2015;58:50–56. | ||
Manojlovic S, Nikolic-Popovic J. EPA-0842 – Dysfunctional attitudes in patients with depressive episode. Eur Psychiatry. 2014;29(Suppl 1):1. | ||
Keefe JR, Webb CA, DeRubeis RJ. In cognitive therapy for depression, early focus on maladaptive beliefs may be especially efficacious for patients with personality disorders. J Consult Clin Psychol. 2016;84(4):353–364. | ||
Millings A, Carnelley KB. Core belief content examined in a large sample of patients using online cognitive behaviour therapy. J Affect Disord. 2015;186:275–283. | ||
Solomon A, Arnow BA, Gotlib IH, Wind B. Individualized measurement of irrational beliefs in remitted depressives. J Clin Psychol. 2003;59(4):439–455. | ||
Blazer DG. Self-efficacy and depression in late life: a primary prevention proposal. Aging Ment Health. 2002;6(4):315–324. | ||
Charoensuk S. Negative thinking: a key factor in depressive symptoms in Thai adolescents. Issues Ment Health Nurs. 2007;28(1):55–74. | ||
Walburg V, Chiaramello S. Link between early maladaptive schemas and defense mechanisms. Eur Rev Appl Psychol. 2015;65(5):221–226. | ||
Taymur I, Ozdel K, Gundogdu I, Efe C, Tulaci RG, Kervancioglu A. Personality-related core beliefs in patients diagnosed with fibromyalgia plus depression: a comparison with depressed and healthy control groups. Nord J Psychiatry. 2015;69(5):386–391. | ||
Pompili M, Innamorati M, Gonda X, et al. Affective temperaments and hopelessness as predictors of health and social functioning in mood disorder patients: a prospective follow-up study. J Affect Disord. 2013;150(2):216–222. | ||
Louie JY, Oh BJ, Lau AS. Cultural differences in the links between parental control and children’s emotional expressivity. Cultur Divers Ethnic Minor Psychol. 2013;19(4):424–434. | ||
O’Connor LE, Berry JW, Weiss J. Interpersonal guilt, shame, and psychological problems. J Soc Clin Psychol. 1999;18(2):181–203. | ||
Intachakra S. Politeness motivated by the ‘heart’ and ‘binary rationality’ in Thai culture. J Pragmat. 2012;44(5):619–635. | ||
You S, Merritt RD, Conner KR. Do gender differences in the role of dysfunctional attitudes in depressive symptoms depend on depression history? Pers Individ Dif. 2009;46(2):218–223. | ||
Saint Arnault D, Sakamoto S, Moriwaki A. The association between negative self-descriptions and depressive symptomology: does culture make a difference? Arch Psychiatr Nurs. 2005;19(2):93–100. | ||
Liu J, Bern-Klug M. “I should be doing more for my parent:” Chinese adult children’s worry about performance in providing care for their oldest-old parents. Int Psychogeriatr. 2016;28(2):303–315. | ||
Candrian M, Schwartz F, Farabaugh A, Perlis R, Ehlert U, Fava M. Personality disorders and perceived stress in major depressive disorder. Psychiatry Res. 2008;160(2):184–191. | ||
Olagunju AT, Olutoki MO, Ogunnubi OP, Adeyemi JD. Late-life depression: burden, severity and relationship with social support dimensions in a West African community. Arch Gerontol Geriatr. 2015;61(2):240–246. | ||
Pedrelli P, Feldman GC, Vorono S, Fava M, Petersen T. Dysfunctional attitudes and perceived stress predict depressive symptoms severity following antidepressant treatment in patients with chronic depression. Psychiat Res. 2008;161(3):302–308. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.