")
Back to Journals » Clinical Ophthalmology » Volume 14
Pathogenesis and Prevention of Worsening Axial Elongation in Pathological Myopia
Authors Pugazhendhi S , Ambati B, Hunter AA
Received 7 December 2019
Accepted for publication 14 February 2020
Published 18 March 2020 Volume 2020:14 Pages 853—873
DOI https://doi.org/10.2147/OPTH.S241435
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sangeethabalasri Pugazhendhi, 1 Balamurali Ambati, 2 Allan A Hunter 3
1PSG Institute of Medical Sciences & Research, Coimbatore, India; 2Pacific ClearVision Institute, Eugene, Oregon, USA; 3Oregon Eye Consultants, Eugene, Oregon, USA
Correspondence: Allan A Hunter
Oregon Eye Consultants, 1550 Oak St. Suite 7, Eugene, Oregon 97401, USA
Tel +1 541-687-1927
Email [email protected]
Purpose: This review discusses the etiology and pathogenesis of myopia, prevention of disease progression and worsening axial elongation, and emerging myopia treatment modalities.
Introduction: Pediatric myopia is a public health concern that impacts young children worldwide and is associated with numerous future ocular diseases such as cataract, glaucoma, retinal detachment and other chorioretinal abnormalities. While the exact mechanism of myopia of the human eye remains obscure, several studies have reported on the role of environmental and genetic factors in the disease development.
Methods: A review of literature was conducted. PubMed and Medline were searched for combinations and derivatives of the keywords including, but not limited to, “pediatric myopia”, “axial elongation”, “scleral remodeling” or “atropine.” The PubMed and Medline database search were performed for randomized control trials, systematic reviews and meta-analyses using the same keyword combinations.
Results: Studies have reported that detection of genetic correlations and modification of environmental influences may have a significant impact in myopia progression, axial elongation and future myopic ocular complications. The conventional pharmacotherapy of pediatric myopia addresses the improvement in visual acuity and prevention of amblyopia but does not affect axial elongation or myopia progression. Several studies have published varying treatments, including optical, pharmacological and surgical management, which show great promise for a more precise control of myopia and preservation of ocular health.
Discussion: Understanding the role of factors influencing the onset and progression of pediatric myopia will facilitate the development of successful treatments, reduction of disease burden, arrest of progression and improvement in future of the management of myopia.
Keywords: pediatric myopia, axial elongation, myopia maculopathies, scleral remodeling, myopic foveoschisis, atropine in the treatment of myopia (ATOM) study, macular buckle
Introduction
Pediatric myopia is a global public health concern affecting 22.9% of the world population,1 and a leading cause of visual impairment with a prevalence of 0.9% to 3.1% worldwide. Asian populations are known to have a higher predominance in comparison to white populations, with a visual impairment prevalence rate of 0.2% to 1.4% and 0.1% to 0.5%, respectively.2 In recent years, myyopia has drastically increased globally, but its prevalence is generally highest in East Asian populations including Taiwan,3 Hong Kong,4 Korea,5 and China.6
Although school age myopia is becoming more common in Asian and Western countries, the pattern of the disease differs in onset, prevalence and severity. In typical cases of school age myopia, the disease onset appears in children of late primary or early secondary school years around ages 8–14. Further disease progression occurs over the next 10–15 years until stabilization of the refractive error.7 While many nations follow these patterns, myopia onset in East Asian countries occurs in children of much younger ages.8–12 As the prevalence of myopia increases, the age of disease onset decreases, which allows more time for myopia to progress before stabilization and increases the chances of progression into high myopia.13
In the past decade, research has focused on halting the progression of myopia and ameliorating the future of the eye. It was once viewed as a benign refractive condition, but has now been proven to be a significant risk factor to future eye diseases such as retinal detachment, glaucoma, cataract, macular degenerative scars, and choroidal neovascularization and other chorioretinal abnormalities, in addition to its hindering effects on vision and quality of life.14 The approximate economic impact of distance vision impairment due to uncorrected refractive error is estimated to be a loss of $ 202 billion of gross domestic product annually.15 Influenced by factors such as visual function, economic burden, psychology, academic performance and aesthetics, the quality of life in patients with myopia is significantly impaired.16,17
Until recent years, the universal therapeutic intervention of choice is to correct the refractive error by spectacles, contact lenses, or rarely, refractive surgery. While these treatment modalities improve visual acuity and prevent amblyopia, they do not impact the growth of the eye, axial elongation, or progression of myopia.
Furthermore, progression and acceleration of myopia in adolescence may preclude future refractive surgery options. This review emphasizes the pathogenesis and etiology of myopia, as well as the mechanics of the different treatment modalities for proper and precise control of myopia to preserve ocular health.
Methods of Literature Search
The MEDLINE and PUBMED Library databases were searched for peer-reviewed publications relevant to the topic of the etiology and pathogenesis of Pediatric Myopia, and its treatment modalities. An in-depth search of the available literature was performed using keywords including, but not limited to, “pediatric myopia”, “refractive error”, “axial elongation”, “atropine”. While it would not be feasible to include a comprehensive list of all relevant search terms use in the preparation of this article, combinations and derivatives of the following words provided most of the manuscripts that were reviewed for inclusion in the article: pathological myopia, pediatric myopia, refractive error, axial elongation, scleral remodeling, accommodation, emmetropization, atropine, pirenzepine, muscarinic antagonists, muscarinic receptors, anti-hypoxic drugs, formononetin, salidroside, posterior pole, myopic maculopathies, myopic foveoschisis, choroidal neovascularization, macular holes, single vision lenses, multifocal lenses, myovision lenses, Progressive Addition Lenses, orthokeratology, ATOM study, ATOM2 study, L-DOPA, dopamine, visual deprivation, positive lenses, negative lenses, primates, chicken, guinea pig, macular buckle, and posterior scleral reinforcement. Searches included all literature published in the English language before August 2018. The abstracts of the resulting articles were carefully reviewed for suitability and inclusion, and the articles that were not relevant were discarded. We selected prospective studies including Randomized Control Trials, Case–Control studies, Cohort studies, Survey studies, Systematic Reviews, Animal model studies, and Meta-Analyses. Case reports or case series were excluded. The bibliographies of all identified literature were reviewed to track additional relevant references, including some that were not published in the English language.
Molecular Concepts Underlying Myopia and Refractive Error
Scleral Remodeling
As the prevalence of myopia increases, researchers have hypothesized on various biological mechanisms of myopia development and progression. The major structural change and determinant in myopic eyes is axial elongation, due to which alterations in the scleral extracellular matrix (ECM) are likely to result in changes in scleral shape.
The human sclera is composed of a single layer of fibrous connective tissue with fibroblasts and myofibroblasts in an encompassing collagenous extracellular scleral matrix.18,19 Collagen is the major component of total scleral protein.20 Fibroblasts secrete Type I collagen, which represents the highest expression of collagen subtypes and acts as a major component of the scleral architecture.18,19 However, collagen gene expression in tree shrew sclera reveals 11 collagen subtypes (I, III, V, VI, VII, VIII, IX, XIII, XV, XVI, and XVII) in the total scleral collagen composition.21 Collagen type I mRNA expression was reduced in sclera of myopic eyes, while the levels of subtypes III and V remained relatively similar to normal sclera. The reduced the collagen subtype ratio (III/I and V/I) alters the collagen accumulation, degradation and synthesis in myopia.21
The sclera of the myopic human eye is described as thinning of collagen fiber bundles as well as a reduction in the size of the individual collagen fibrils, with an increase in the dispersion of the range of fibril diameters averaging below 60–70nm.22 Additionally, studies reveal an increase in abnormal star-shaped fibrils and a predominantly lamellar arrangement of collagen fibers in myopic eyes in comparison to tighter interwoven collagen fibers in emmetropic eyes.22,23 Such microscopic structural alterations in the human myopic sclera suggest a disruption of collagen fibril growth and organization.
The biomechanical properties of sclera are primarily dependent on the components of the scleral extracellular matrix. In accordance with studies, the ultramicroscopic changes to scleral collagenous structure are thought to be a result of a significant reduction in scleral glycosaminoglycans (GAG) synthesis in myopic eyes, especially in the posterior pole.24,25 Such findings were reported in myopic experimental models in tree shrews, which are mammals closely related to primates. Deprivation myopia was induced in tree shrews with occluders in front of the eye, and the ocular growth was modulated to adjust to the defocus of the eye.26,27 The tree shrew models have revealed reduced levels of scleral hydroxyproline and sulfated glycosaminoglycans at the posterior pole. This suggests a reduced collagen accumulation and proteoglycan content in myopic eyes, which allows the sclera to be more distensible and permitting axial elongation and resultant myopia.28 The results from the studies in tree shrews reaffirm that an internal mechanism for ocular growth and scleral remodeling occurs to increase the axial length of the eye.
Myopia inducing experiments, such as visual form deprivation, have revealed that the majority of the molecular scleral changes may be reversed upon termination of the experiment. In the recovery period, the expression of mRNA levels of scleral collagen and the levels of GAG synthesis reverted to baseline levels.24,29 Such experiments provide sufficient grounds for salvaging the myopic sclera through intervention at molecular levels.
While fibroblasts secrete Type I collagen, myofibroblasts are contractile cells that arise from a trans-differentiation of fibroblasts.18,19 A study by Wu et al reported that scleral hypoxia plays a pivotal role in myopia induced scleral remodeling.30 The triggers for scleral hypoxia are multifold. The retina contains the highest consumption of oxygen in the body and has continuous light exposure, which is highly susceptible to generating Reactive Oxygen Species (ROS).31 Oxidative stress is a result of an imbalance between such free radical production and anti-oxidant defenses, which result in oxidative damage and ultimately hypoxia. Hence, damage to the retina by oxidative stress is highly likely to be linked to myopia.32
Additionally, it is suggested that decrease in choroidal blood flow resulting from external visual stimuli may lead to myopia. A high choroidal blood flow is a required force for diffusion of oxygen and nutrients through the retinal layers. The ocular pulse amplitude decreases along with the choroidal blood flow. Since the retina is thinner in myopic eyes, the high driving force is no longer needed, resulting in a decrease in the choroidal blood flow. Such vascular modifications result in circulatory disturbance causing hypoxia in myopia.33,34
Visual signals are conveyed to the retina and choroid, which produce mediators that result in myofibroblast transdifferentiation and resultant remodeling in the sclera. Scleral hypoxia is induced by Hypoxia-Inducible Factor-1α (HIF-1α), which triggers a signaling cascade for myofibroblast trans-differentiation resulting in scleral extracellular matrix (ECM) remodeling in worsening myopia. Wu et al postulated that hypoxia-induced myofibroblast trans-differentiation down-regulates type I collagen synthesis, which results in scleral structural changes, thus emphasizing the potential role of hypoxia in myopia.30
Scleral architecture alterations with resultant staphyloma are detected using color fundus photography, ultrasonography, 2-dimensional Computed Tomography (CT) and Magnetic Resonance Imaging (MRI), and more recently a 3-dimensional MRI. The new high-resolution 3D MRI with volume rendering techniques analyzes the entire shape of the eye to delineate the posterior staphyloma in highly myopic eyes.35–37 Using the 3D MRI, Ohno-Matsui reported posterior outpouching of the eye, suggestive of staphyloma, in 50.5% of highly myopic patients with mean axial length of 30.0 ± 2.3mm.35 In addition, Ohno-Matsui utilized a combination of 3D MRI and Optos to analyze the morphological features and structural changes observed in staphyloma in highly myopic patients in Japan and Spain with mean axial length greater than 26.5mm.38 It was reported that more staphylomatous eyes had additional features such as patchy chorioretinal atrophy and myopic choroidal neovascularization than eyes without evident staphyloma.35 It is suggested that myopic eyes with staphyloma and other structural modifications have a worse prognosis for visual acuity and other degenerative changes in the eye.
Etiology of Myopia
Although numerous etiological studies have been conducted, the exact mechanism of myopia has been a historical dilemma and hitherto remains unknown. It has been suggested that both genetic and environmental factors play a significant role in its development. Myopia prevalence varies according to different ethnic and geographic populations.
It is evident that Asian populations, specifically East Asian, have the highest prevalence rates of myopia. In China, the prevalence of pediatric myopia in an urban Chinese population increased from 5.7% in 5 year-year-olds to 78.4% in 15-year-olds.9 The prevalence in rural China in junior high children increased from 36.8% in 13-year-olds to 53.9% in 17-year-olds.39 In India, the prevalence of pediatric myopia in the urban population increased from 4.68% in 5-year-olds to 10.8% in 15-year-olds.40 In rural India, the prevalence of pediatric myopia increased from 2.8% in 7-year-olds to 6.72% in 15-year-olds.41 Similarly in Taiwan from 1983 to 2000, the myopia prevalence rate increased from 5.8% to 21.0% in 7-year-olds, 36.7% to 61.0% in 12-year-olds, 64.2% to 81.0% in 15-year-olds, and 74% to 84% in 16 to 18-year-olds.42 In Korea, the prevalence of myopia increased from 50% in 5 to 11-year-olds to 78% in 12 to 18-year-olds, and decreased to 45.7% in high school children.43 In Hong Kong, the prevalence of myopia in Chinese school children was 18.3% for 6-year-olds and 61.5% for 12-year-olds.
While it is known that East Asian populations have a higher prevalence rate of pediatric myopia, the prevalence and trend vary among the Non-Asian populations. In the United States, the prevalence of myopia among ages 12 to 54 increased from 25.0% in 1971–1972 to 41.6% in 1999–2004.44 In Australia, the prevalence of myopia was 1.43% in 6-year-olds.45 In the United Kingdom, the prevalence of myopia in a predominantly white population was 2% in 6 to 7-year-olds and 15% in 12 to 13-year-olds.46
The recent Multi-ethnic Pediatric Eye Study of preschool children aged 6–72 months revealed the prevalence of 1.2% in non-Hispanic White, 3.7% in Hispanic, 3.98% in Asians and 6.6% in African American children.47,48 The incidence of myopia increases with advancing age as demonstrated by multiple studies, including the multi-ethnic observational study conducted on older children aged 5–17 years reveals an overall 9.2% of myopia in the study subjects with 4.4% in non-Hispanic whites, 6.6% in African Americans, 13.2% in Hispanic and 18.5% in Asian children.49–51 The high prevalence of myopia in children and adolescents indicates that refractive error and its associated health concerns are a major public health concern that visually incapacitates children in educational, recreational and social settings.
Studies have also demonstrated that myopia risk increases with the number of myopic parents. In comparison to children with non-myopic parents, children with one myopic parent are 2.91 times more likely to have myopia while those with 2 myopic parents have 7.79 times elevated risk. The associated development risk rates are 7.6% for non-myopic parents, 14.9% for one myopic parent and 43.6% for 2 myopic parents.52,53 Zadnik et al reported that children with two myopic parents have longer axial lengths and less hyperopic refractive error, suggesting that the premyopic eye in children with a family history of myopia resembles to the elongated myopic eye.54 Additional studies reveal that the annual axial length increases with the number of myopic parents: 0.20mm for no myopic parents, 0.26mm for one, and 0.37mm for two myopic parents.55 Furthermore, myopia recurrence risk increases with the number of myopic siblings.56 Therefore through sharing of genes and environmental factors, the probability of inheriting myopia is suggested to be significantly higher in families with myopia. Ghorbani Mojarrad et al reported that the number of myopic parents was a weak predictor of the refractive error in children since it reveals information regarding the shared environmental risk factors for myopia. Hence, it is suggested that a genetic risk score was better at detecting children at risk of myopia.57
The investigation of genetic influence on refractive error and myopia is demonstrated in numerous Genome Wide Association Studies (GWAS) conducted over the past decade. Major development in myopia genetics occurred from the international Consortium for Refractive Error and Myopia (CREAM) study and from the genotyping company 23andMe. The CREAM study identified 24 chromosomal loci associated with refractive error between subjects of European ancestry and Asians, and uncovered a tenfold increase in the risk of myopia among these alleles.58,59 Similarly, the genome-wide association study conducted by 23andMe company conducted a survival analysis on the age of myopia onset obtained from questionnaire data, and identified 20 novel chromosomal loci. The study’s findings reveal multiple genetic factors and complex interactions, such as interactions between extracellular matrix remodeling, neuronal development and visual signals from the retina, in the development of myopia.59,60 In total, both studies identified the same 25 chromosomal loci that are associated with refractive error.59 The collective inference from GWAS performed in the past decade has explained a portion of the genetic variants associated with refractive error. Table 1 reveals the genes identified in experimental myopia studies. Further investigation of the mechanism by which the various loci affect the refractive error indicates potential to identify genetic targets for treatment and prevention strategies for adequate myopia control.
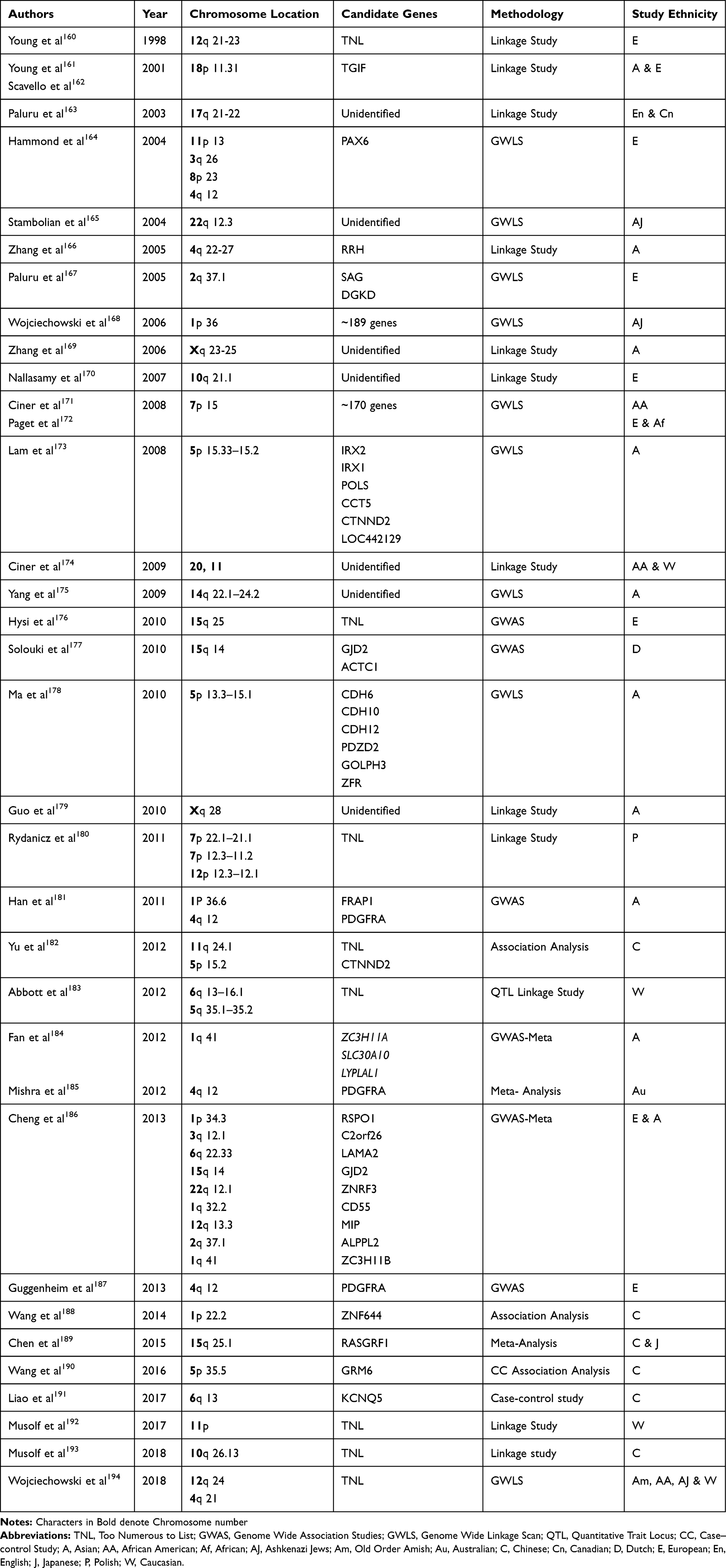 |
Table 1 Genes Analyzed in Experimental Myopia Studies |
While it is evident that genetic factors play a role in myopia development, rapid growth in incidence and prevalence is likely due to associated environmental factors. Numerous studies have identified environmental influences such as higher education, scholastic performance, and near work to contribute to myopia development and progression.
It has been suggested that adults with higher education, near work-related occupations and accordingly higher incomes are more likely to have longer axial lengths and higher myopic refraction. For example, individuals with 10 years of more of education could be expected to have 0.60mm longer axial lengths and 1.50 diopters more myopic refraction than those with fewer years of education. Similarly, individuals with near work occupations could be expected to have 0.28mm longer axial lengths and 0.71 diopters more myopic refraction.61,62 It is suggested by Mendelian randomization that every additional year of education was associated with a more myopic refractive error of −0.18 diopters per year.63 Williams et al displayed that education was significantly associated with myopia, as the age-standardized prevalence was 25.4% for those completing primary education, 29.1% for secondary education and 36.6% for those who completed higher education. However, it is suggested that education levels act as an additive rather than explanatory factor for increased myopia prevalence.64 Based on these and additional study results, higher education has been closely associated with high refractive error as a result of axial elongation.
Similarly, studies have attempted to display a more direct association between reading and near work activity by measuring the number of books read by children per week. Saw et al observed that myopic children spend more time reading than non-myopic children, and that the proportion of children with more than −3.00 Diopters of myopia was higher if children read more than 2 books per week.65 Studies further report that highly myopic children spend more time reading, studying and in near work activities, than in outdoor activity. In a sample of Australian school children, it was reported that children of European Caucasian ethnicity spent 26.0 hrs a week in near work activities and children of East Asian ethnicity spent 32.5 hrs per week. As a result, activities such as near work, close distance reading and continuous reading are strongly associated with myopic refractive error.66 Furthermore, myopic discordant twin studies confirm these findings and show additional findings on the impact of outdoor activity on myopia development or progression.67
Outdoor activity has been associated with a protective effect on myopia in several epidemiological studies. While it remains independent of the amount of time spent in near work activities such as reading, the type of outdoor activity has also remained irrelevant. Studies reveal that time spent in outdoor activities is inversely correlated with myopic refraction in children. It is hypothesized that distant stimuli effect on vision for 2 to 3 hrs neutralizes the effects of 9 to 12 hrs of hyperopic defocus experienced during near work activity.68–71 Additionally, it is suggested in experiments of form-deprivation myopia that outdoor light exposure exerts a protective effect of normal vision by stimulating dopamine release from the retina. This is known to inhibit eye growth and inhibit progression of myopia.72 Hence, it is of public health concern to promote outdoor activity in school curriculums to exert its protective effects on normal vision in children.
Animal Models Influence on Current Understanding
To better understand the etiological factors of myopia, researchers have relied on a variety of animal models for studies in stringently controlled environments. Animal studies widely report that while genetics determine myopic susceptibility, environmental factors significantly modulate the growth of the eye. Researchers have reported that intervening with the visual experience of animal models results in alterations in the growth of the eye. In 1978, Raviola and Wiesel first described that visual deprivation by eyelid suture or corneal opacification of primates induced axial elongation and high degrees of deprivation myopia. These results initiated parallel animal studies showing that stimulation of the retina with blurred image results in alteration of growth signals within the eye.73–75
Additional animal studies show that using both positive and negative lenses triggers the eye to alter its axial length to accommodate according to the lens placed in front of the eye. This mechanism is reversible when the visual stimuli are removed and can even occur when the optic nerve is severed, which reveals that the mechanism involved lies within the eye itself. Moreover, chicken eye models demonstrated the signaling cascade of growth modulators such as acetylcholine, dopamine, vasoactive intestinal polypeptide and glucagon as they trigger retinal, choroidal and scleral growth.27,74,75
There is extensive evidence suggesting that deprivation myopia in animal models result in a reduction in retinal dopamine levels, suggesting that retinal dopamine release is linked to visual stimuli and axial growth of the eye.76–78 Studies report that direct intravitreal injections of dopamine in rabbit eye models hinder the ocular changes in form deprivation myopia such as myopic shift, vitreous chamber and axial elongation.79,80 Dopamine molecules interact with its receptors D1 to D5 to exert their pharmacological action. The D1-like family receptors (D1R) include D1 and D5, which mediate responses by activating adenylate cyclase. Contrastingly, D2-like family receptors (D2R) include D2, D3, and D4, which inhibit adenylate cyclase.81 A large body of evidence suggests that stimulation of dopamine release in addition to activation of D2-Dopamine receptors exerts protective effects of normal vision against form-deprivation myopia in animal models.72,82,83 Contrastingly, a study by Zhang et al demonstrated that D1R activation inhibited, while D2R activation enhanced form-deprivation myopia in guinea pigs.84
In addition to dopamine, there is sufficient evidence in support of the role of neuropeptides such as Substance P, Vasoactive Intestinal Peptide (VIP) and Calcitonin gene-related peptide (CGRP) in experimental myopia in animal models. Substance P and VIP, which are localized in amacrine cells, were among the first neuropeptides investigated for its role in modulation of eye growth in myopia.85–87 Primate study reports that the immunohistochemical reactivity of the retina for VIP was higher in the myopia inducing fused eyes than the open eyes. The same was not reported for Substance P.85 Additionally, the ophthalmic sensory nerve fibers that innervate the choroid contain vasodilatory substances such as Substance P and CGRP.88 Studies have investigated the influence of these sensory fibers on choroidal blood flow in deprived chick eye models.89–91 It is suggested that the vasodilatory effect of the neuropeptides may play a role in sensing changes in ocular temperature and consequently modifying the choroidal blood in myopic eyes.88
Based on animal models, we assume that experimental manipulation of eye growth resembles the myopic changes in the human eye. Accordingly, interventions such as progressive-addition lenses, bifocals, and pharmacological interventions such as atropine eye drops have been attempted on human subjects to reduce myopic progression. Fortunately, the changes in axial growth and myopic refraction in human eyes were consistent with the predictions based on animal models.
Lifetime Risks of the Myopic Eye
The definition of pathological myopia, though inconsistent, is commonly associated with refractive error greater than −6.00 D with an axial length greater than 26 mm. This signifies a high degree of myopia and accounts for up to 33% of the myopic population.92 The increased axial elongation of the eye results in degenerative changes in the retina and associated maculopathies, such as posterior staphyloma, choroidal neovascularization, RPE atrophy, macular holes, and foveoschisis.93,94
Choroidal neovascularization (CNV) is the formation of abnormal blood vessels under the retinal pigment epithelium capable of penetrating the Bruch membrane and extending into the subretinal space.95 It is a vision-threatening complication of myopia and has been estimated to develop in 5–10% of patients with high myopia and is frequently associated with lacquer cracks or RPE tears and atrophy. Due to the excessive elongation of the myopic eyeball, there is mechanical stretching of the retina leading to an imbalance between pro-angiogenic and anti-angiogenic factors.96
Myopic CNV is classified into 3 stages: active, scar and atrophic. In the active stage, a small, grey, fibrovascular membrane forms around the lesion with occasional bleeding, and patients present with rapid decrease in central vision, often with central scotoma or metamorphopsia. In the scar stage, there is formation of a scar and absorption of the bleeding, which may result in temporary improvement of vision. In the atrophic stages, there is regression of the neovascularization and presence of an area of chorioretinal atrophy, which leads to further deterioration of the vision.
A study by Yoshida et al reported that the long-term visual outcome of myopic CNV is extremely poor as chorioretinal atrophy develop around the regressed CNV in 96.3% of the patients at 5 and 10 years after CNV onset.97 Peripherally located CNV is usually asymptomatic, while CNV located centrally present with symptoms such as metamorphopsia, scotoma, and reduced visual acuity. The visual prognosis of myopic macular CNV is poor, as patients have visual acuity of 20/200 or worse in 5 years; therefore, ophthalmologists should consider active interventions for early myopic treatment.92,93,98
Myopic foveoschisis is increasingly prevalent as a vision-threatening complication. It is characterized by the splitting of retinal layers in the macula, which is more frequently seen in myopic eyes of greater than 8 diopters.99 With progressive elongation of the highly myopic eye, patients develop posterior bulging of the globe resulting in a posterior staphyloma. Based on 3-dimensional MRI scans of the entire eye, Ohno-Matsui classifies posterior staphyloma according to its location and distribution.35 This abnormal contour contributes to abnormal vitreous traction and posterior vitreous detachment.48,49 Additionally, it is hypothesized that the inner retinal layers are less flexible than the outer retinal layers as a result of the adherent vitreous cortex to the retina, the epiretinal membrane and the internal limiting membrane.100,101 Such traction on the inner retinal layers results in splitting of the retina leading to retinoschisis and subsequent retinal detachment at the fovea.
Takano and Kishi reported in the first study that myopic foveoschisis was detected using time domain OCT in 11 out of 32 eyes of patients with severe myopia.99 A study by Panozzo and Mercanti reported that foveoschisis occurred in 34.4% of 218 eyes in patients with severe myopia ranging from 8 to 26 diopters.102 Myopic foveoschisis is reported to contain variations of foveal architecture such as foveal cysts in 47%, lamellar hole in 29% and foveal detachment in 29% of cases.103 Consequently, the prognosis is poor and early diagnosis is a challenge due to a slow visual decline, which is usually gone unnoticed by patients in early stages.48,49
Myopic foveoschisis in its later stages may result in the formation of a macular hole from the abnormal vitreous traction and the foveal detachment. Studies show that protein, collagen, and hyaluronic acid content of vitreous humor was considerably lower in patients with myopia compared with those without myopia, suggesting that myopic eyes are affected by the degenerative process in comparison to non-myopic eyes. Additionally, the volume of the vitreous cavity is increased in highly myopic eyes, which may explain the early development of vitreous degeneration and macular holes.104,105
With a myopic macular hole, patients experience severe vision loss, and an eventual retinal detachment if left surgically untreated. Regrettably, patients may require multiple surgeries, as reopening of the macular hole and retinal re-detachment are not uncommon.93,104
Treatment of Myopia
Optical Correction
Single Vision Lenses
The most common therapeutic intervention for myopia utilized by clinicians is single vision lenses (SVLs) with periodic alteration of the spectacle prescription to correct the increasing refractive error. SVLs emulate the process of emmetropization by regulating the refractive error of cornea and the axial length of the eye to focus the rays on the retina. While this enhances visual outcomes, it does not interrupt the myopic progression or axial elongation of the eye. As described previously, animal studies have shown compensatory growth of the eye in spectacle induced emmetropization, which negates SVL use as it may increase progression of myopia.106,107 Additionally, animal studies have implied that under-correction of the refractive error reduces the axial growth of the eye and progression of myopia. Based on the results of animal models, clinical trials on human subjects prescribed SVLs under corrected by 0.5 to 0.75D in order to reduce axial growth and myopia progression. In a 2-year clinical trial, Chung et al demonstrated that under correction speeds up myopia development and axial elongation, which is contrary to the animal studies. At the end of the clinical trial, the progression of myopia in the under-corrected group was 0.5 D per year, while that of the fully corrected group was 0.38 D per year.108 Adler et al confirmed the results by reporting that under-correction produced a slight increase of 0.17 D progression of myopia over the 18-month trial period, compared to the full-correction.109 Such studies report that under-correction is not an effective manner of slowing the rate of myopic progression. Additionally, while SVLs attend to the refractive error and vision complaints of the child, it does not have a protective role in the health and growth of the eye that the myopia epidemic entails.
MyoVision Lenses
MyoVision Lenses are novel spectacle lenses that were designed to reduce the peripheral hyperopia and have reported to be effective in preventing myopia progression in subgroup of children in China and more recently Japan.110,111 The study reported no statistically significant difference in the rate of myopia progression between children wearing the MyoVision lenses and the control group. However, an unplanned subgroup analysis revealed a possible effect in children with myopic parents.110 However, such results have not yet been replicated in other studies. MyoVision lenses were utilized to reduce relative peripheral hyperopia on myopia progression in Japanese children. However, the mean-adjusted change in spherical equivalent refraction and the axial elongation were not significantly different in the MyoVision Lenses group in comparison to the control group wearing Single Vision Lenses.111 This mandates additional studies to examine the efficacy of the MyoVision lenses as well as studies to design lenses that can more effectively reduce the peripheral hyperopic defocus and reduce myopia progression.
Multifocal Lenses
Multifocal lenses have largely been investigated to slow the progression of myopia and the axial elongation of the eye. The theoretical mechanism of action of these lenses is to decrease the accommodative effort for near vision, reduce peripheral hyperopic defocus and ultimately decrease rate of myopic progression. Multifocal lenses and the newer, more aesthetically pleasing Progressive Addition Lenses (PAL) have been widely explored by studies such as the Correction of Myopia Evaluation Trial (COMET) study—a 3-year multicenter, randomized double-masked clinical trial. The COMET study compared myopia progression in children treated with PALs versus SVLs, where progression was measured by cycloplegic autorefraction and A-Scan ultrasonography axial length. The cumulative 3-year treatment result of the trial was statistically noteworthy, as the mean increase of myopia in children treated with PALS was 1.28 ± 0.06D compared to 1.48 ± 0.06D for those treated with SVLs. Since these results spanned over a treatment period of merely 3 years, however it was considered clinically insignificant.106,112 Additionally, patient compliance may pose problems regarding cosmetic acceptance and adaptability. Future large population based, and long duration studies may substantiate the significance of the multifocal lenses in preventing the progression of myopia.
Rigid Gas Permeable Contact Lens
Contact lenses are accepted for optical correction with cosmetic benefits, and has largely been utilized to treat pediatric myopia, retard its progression and decrease axial elongation. Several options are available for myopia correction and slowing of progression such as rigid gas permeable contact lens, soft bifocal contact lens and orthokeratology contact lens.
Studies such as Contact Lens and Myopia Progression (CLAMP) study investigated the impact of contact lenses on myopic progression. CLAMP study evaluated the progression of myopia in 8 to 11-year-old children over a period of 3 years and demonstrated that rigid gas permeable contact lens wearers experienced reduced progression vs soft lens controls. Walline et al reported that rigid gas permeable lens wearers progressed −1.56 ± 0.95 D in 2 years in comparison to soft contact lens wearers who progressed to −2.19 ± 0.89D.14,113 Unfortunately, upon cessation of lens wear, myopia progression increased. Similarly, the 3-year Houston study of rigid gas permeable contact lenses compared 100 myopic children of ages 8–13 years who were fitted with Paraperm oxygen plus contact lenses with 20 spectacle wearers. The study reported that the average progression of myopia was statistically and significantly different with 0.48D progression for Rigid gas permeable contact lens wearers and −1.53 D progression for spectacle wearers.50 The study and several others revealed that the temporary decrease in progression was a result of altering the corneal curvature, and not the axial length.113–115 Contrastingly, a larger randomized Singapore study involving 383 children aged 6–12 years revealed a lack of significant difference in the myopia progression rate or axial length for the contact lens and spectacle-wearing group.116
Soft Bifocal Contact Lens
Soft bifocal contact lenses have been designed for distance in the center with additional power in the periphery, or vice versa. Some studies have demonstrated that soft bifocal contact lenses slow myopic progression due to decrease in accommodation effort and axial length. These contact lenses are designed to correct central myopia while reducing relative peripheral hyperopia. Walline et al conducted a study among 40 participants aged between 8 and 11 years, who were fitted with soft multifocal lenses with a −2.00 D add versus 40 children wearing soft single-vision contact lenses. A-scan ultrasound and cycloplegic autorefraction were performed at baseline, after 1 year, and after 2 years. It was found that the average myopic progression at 2 years was 0.41 ± 0.03 D for the single-vision contact lens wearers and 0.29 ± 0.03 D for the soft multifocal contact lens wearers.117 Anstice and Phillips used a contralateral eye study design, and demonstrated that the eye wearing soft bifocal contact lens has a slower axial growth when compared to the eye wearing soft single-vision contact lens.118 This warrants the need for further large-scale investigations on the effect of soft bifocal contact lenses on myopic progression and axial elongation, and a comparison to rigid gas permeable contact lenses.
Based on the successful correlation between myopia and reduction of axial length with multifocal contact lenses, an ongoing clinical trial by Beasley et al aims to determine whether axial growth can be accelerated in children with hyperopia by imposing relative peripheral hyperopic defocus using center-near multifocal contact lenses.119
In a 2-year clinical trial on myopic children between ages 8–13, a newer lens design was evaluated for preventing myopic progression. A Defocus Incorporated Soft Contact (DISC) lens design applies concentric zones of alternating distance correcting and defocusing areas that cover the pupil. The correcting zones allow clear vision, while the defocusing zones simultaneously incorporate constant myopic defocus on the retina. The DISC lens was worn for 6–8 hrs per day. At the end of the 2 years, DISC lens wearers reported 25% less myopia progression and 31% less axial elongation than those wearing SVLs.120
Defocus Incorporated Multiple Segments (DIMS) Spectacle Lens
In a recent two-year Randomized Control Trial, Lam et al designed a concentric dual-power lens called Defocus Incorporated Multiple Segments (DIMS) spectacle lens to investigate if the spectacle lenses can slow myopia progression in school children. The DIMS lens provides the same optical stimulus as the DISC lens but avoids the disadvantages regarding contact lens wear and subject compliance. The subjects of the trial were instructed to wear the DIMS lens in full-time mode, except during sleeping and showering. With increased compliance and lens satisfactions, the DIMS lens proved to be more effective. The progression of myopia was 52% slower in children wearing the DIMS lens than those wearing SVLs, and had less axial elongation by 62% than in children wearing SVLs.121 The DIMS lens was applied to a recent study investigating the adaptability and the acceptance of the lens in a prospective, cross-over study using DIMS lens and SVLs in study with Chinese Children. The study reported a higher preference for the DIMS lens, with +3.50D defocus, in comparison to the SVLs, with minor complaints of mid-peripheral visual changes.122 Although early results display good tolerance, future investigation with a large sample size is warranted for accurate presentation of the lens acceptability in school children, and for determining the optimal amount of defocus for myopia control.
MiSight Lenses
MiSight soft contact lenses contain a dual-focus optic design for slowing juvenile onset myopia progression. The hydrophilic lens contains a 2D add power, producing a second focus in front of the retina, which creates a defocused image in the retinal plane that is superimposed with the distance vision image. The central correction zone of the contact lenses, which are surrounded by alternating concentric regions of near and distant powers, provide good distance visual acuity for the patient. The MiSight Assessment Study Spain (MASS) was a 2-year randomized clinical trial reported a slower progression of myopia in MiSight lenses compared with Single Vision Spectacles as control (0.45 D vs 0.74 D).123 A recent 3-year, double-masked, randomized clinical trial at four investigational sites in four countries, and reported a change in spherical equivalent refraction of −0.73 D and axial length change 0.32mm, which was 59% and 52% less, respectively, in the test group than control group.124 In view of the MASS study, this study incorporates an ethnically diverse subject population to demonstrate the effectiveness of MiSight contact lenses in slowing change in spherical equivalent and axial length.
Orthokeratology
Orthokeratology contact lens is rigid contact lenses that flatten the cornea until its shape is altered to ultimately reduce myopia. The lenses are removed during the day and worn overnight to temporarily alter the corneal shape through central corneal thinning, thereby correcting the myopia for short periods of time. In the Berkeley Orthokeratology study, 80 subjects were randomized to orthokeratology versus the control group.125,126 The results displayed a significantly larger reduction of myopia in orthokeratology lens group compared to the control, but the study had overall minimal clinical significance.
The Longitudinal Orthokeratology Research in Children was a study conducted in Hong Kong, where children wore Orthokeratology lenses for 2 years. The results of the study reported that axial length in children wearing orthokeratology lenses increased by 0.29 mm, less than the 0.54mm observed in the control group.127,128 These studies are promising and demonstrate the demand for a large population-based study with adequate control groups and long-term follow-up of patients to reach clinical significance. The most serious complication of Orthokeratology lenses is microbial keratitis, which may lead to significant vision loss.129,130 While it is commonly used in East Asia due to its effectiveness, these lenses require proper lens fitting, compliance from the child, adherence to routine follow-ups, and proper and timely treatment of any complications for long-term success.
Pharmacological Management
Atropine
Atropine is a non-selective muscarinic antagonist that has shown the most encouraging results for slowing the progression of myopia in children. Atropine was initially tested in animal models and was deemed effective in preventing myopia progression and reduction of axial length.
Studies have been devoted to understanding the pharmacological and molecular mechanism of action of muscarinic antagonists on the eye, and specifically on the signaling pathway of axial elongation. While there has not yet been a confirmation on the precise mechanism, several theoretical mechanisms of actions have been postulated. Molecular studies have revealed the presence of muscarinic receptor (mAChRs) subtypes M1, M2, M3, M4, and M5 in both human and mouse sclera, which carries a fundamental role in the biochemical and molecular regulation of scleral remodeling.131 Expression of the mAChRs results in the proliferation of human and mouse scleral fibroblasts present in the scleral collagenous matrix, thereby promoting scleral remodeling. Atropine receptor blockage theoretically halts scleral fibroblast proliferation and consequential axial elongation of the eye; however, the hypothesis is currently under evaluation. Additional studies using Real-time PCR have determined that M1, M3, and M4 gene expression levels were upregulated, while M2 and M5 gene expression showed little change, in experimental mouse eyes following atropine treatment. The understanding of the mechanism of atropine on gene expression level provides future gateway to the exploration at the molecular and protein level.132
The Atropine in the Treatment of Myopia study (ATOM) was a randomized, double-masked, placebo-controlled trial conducted from 1999 to 2004 involving 400 Singapore children aged between 6 and 12 years old, where 1% atropine was instilled nightly for 2 years. The study had a 2-year treatment phase followed by a 1-year washout phase. The two-year results demonstrated a 77% reduction in progression of myopia with an unchanged axial length, in comparison to the control group.133,134 Although successful at the end of two-year treatment phase, the 1-year washout phase displayed significant rebound phenomenon in both the refraction and the axial length. The topical instillation of atropine was overall well tolerated but contained both short term and long-term side effects. Short-term side effects include red eyes, photophobia, blurred near vision, allergic dermatitis, increased intraocular pressure and angle closure glaucoma. Rarer long-term side effects are ocular diseases such as retinal vascular disease, and cataract.133,134
The ATOM1 study was followed by a 5-year clinical trial entitled ATOM2, which examines the efficacy of lower doses of atropine on reducing the myopic progression, while simultaneously decreasing the side effects of the drug. Participants were randomly assigned to receive 0.5%, 0.1% or 0.01% concentration of atropine for 24 months, followed by a 1-year washout phase. The third phase consisted of restarting the treatment with the optimal concentration from Phase 1 on children showing progressive myopia. The ATOM2 study concludes that while all three concentrations of atropine remain effective in reducing progression of myopia when compared to placebo group, 0.01% is a viable concentration for reducing myopic with minimal side effects thereby increasing safety profile.135,136 Shih et al have compared the effects of multifocal lens wearers treated with 0.5% atropine with placebo control groups, and have found that myopic control was greater with a reduced elongation length in the atropine treated group than the placebo.137
Studies also reveal a dose dependent rebound effect after cessation, which was more common in eyes treated with 1.0% (ATOM1), 0.5% and 0.1% (ATOM2) atropine. A recent study conducted by Yam et al states that 0.05%, 0.025% and 0.01% atropine eye drops reduce myopia progression and exert a concentration-dependent reaction, of which 0.05% atropine was the most effective in controlling progression of spherical equivalent and axial elongation.138 It is evident that atropine plays a significant role in controlling myopia progression either alone or in combination with another therapeutic regimen. Table 2 displays the role of atropine in the treatment of myopia progression over the years. Currently, the prescription of atropine eye drops has not yet been adopted as standard practice in Western countries; but it is commonly used in Asian countries including Singapore and Taiwan.
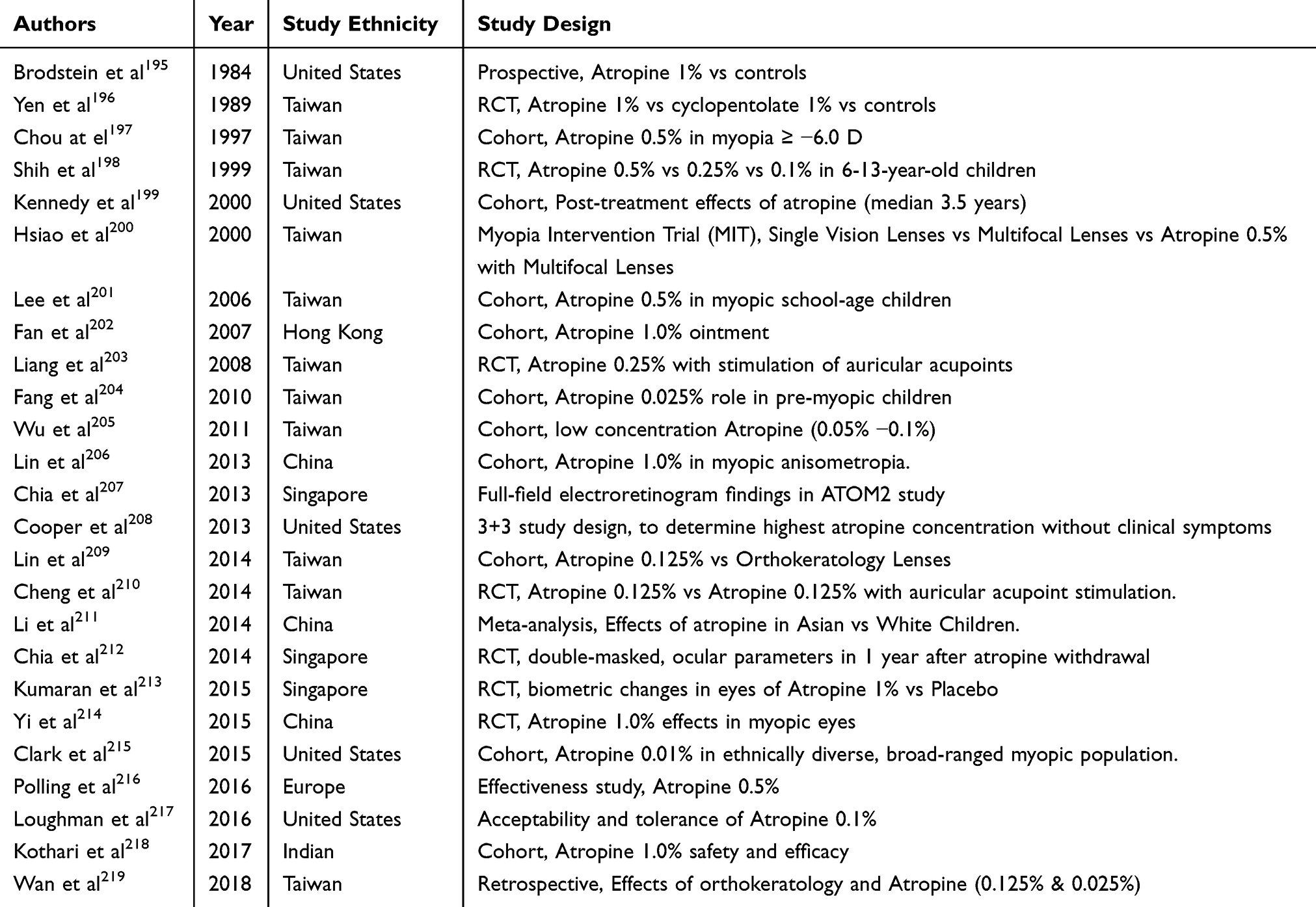 |
Table 2 Studies on Atropine-Induced Control of Myopic Progression |
Pirenzepine
Pirenzepine has been used as an alternative to atropine treatment for pediatric myopia. Pirenzepine is a selective M1 muscarinic receptor antagonist with actions similar to atropine in arresting myopia progression and axial elongation. Pirenzepine is known to have reduced mydriatic and cycloplegic effects compared to atropine and is prone to fewer side effects in patients.
A study conducted by Siatkowski et al formulated a 2% ophthalmic gel, with an acceptable safety profile, instilled twice daily for one year on children aged 8 to 12 years old, with a spherical equivalent of −0.75 D to −4.00 D with astigmatism of 1.00 D or less. The study demonstrated the efficacy of pirenzepine for anti-myopia treatment, as the mean increase of myopia was 0.26 D in the pirenzepine group versus 0.54 D in the placebo group. In addition, the average axial length increase at 1 year was 0.19 mm for patient in the pirenzepine group and 0.23 in the placebo group; however, this was considered statistically insignificant.
Adverse events were mild to moderate in severity, with the most frequent events being mydriasis, erythema of eyelids and ocular itching.125,139,140 In general, the study has proven the efficacy and safety of pirenzepine used for anti-myopia treatment. Further exploration comparing atropine versus pirenzepine will provide an accurate depiction of its efficacy and safety profile.
Anti-Hypoxia Drugs
Drugs such as salidroside and formononetin have been known to exhibit anti-hypoxic effects in cardiac myocytes, which may hold great potential to treat scleral hypoxia in myopia.141,142 Salidroside has a protective effect for hypoxia-induced cardiac apoptosis and pulmonary hypertension.143,144 In cardiac myocytes, the extrinsic apoptotic pathway occurs though the binding of the death receptor Fas and FasL, which initiates a pathway of cytosolic death through aggregation of Fas-Associated Death Domain (FADD) adaptor protein and activation of caspase 8.143,145 The activity of the Fas receptor dependent apoptotic pathway in cardiac tissue of mice with chronic intermittent hypoxia decreased after treatment with salidroside. It was reported that salidroside treatment resulted in the decrease in Fas ligand, Fas receptor, FADD, activated caspase-8 and activated caspase-3.143 The same mechanism is thought to occur in the case of scleral hypoxia-induced myopia, for which treatment with salidroside can exert anti-hypoxic effects to minimize scleral remodeling.
Formononetin has shown to have protective effects in hypoxia-induced retinal neovascularization by decreasing the expression of HIF-1α, Vascular Endothelial Growth Factor (VEGF) and Prolyl Hydroxylase Domain-2 (PHD-2).142 Both drugs have shown to antagonize chloride-induced hypoxic effects.146,147
In experimentally induced myopic animal models, Wu et al documented that the anti-hypoxic drugs down-regulated HIF-1α expression and the phosphorylation levels of eIF2α and mTOR to inhibit the development of form deprivation myopia, without affecting the normal ocular growth in guinea pigs.30 The suppression of myopia in the animal models suggests the potential of these agents in the treatment of myopia in human eyes. The role of scleral hypoxia induced scleral ECM remodeling in the pathogenesis of myopia bears further investigation. This may lead to future clinical approaches in the prevention of myopia development and treatment of myopia progression.
Surgical Management
High myopia is characterized by progressive axial elongation as well as progressive thinning and weakening of the posterior sclera. Surgical intervention to halt the progression of myopic axial elongation and scleral weakening has sparked the interest of many vitreoretinal surgeons. One such surgical management is the macular buckle surgery.
Macular buckle or posterior scleral reinforcement (PSR) surgery uses a scleral buckle to apply direct mechanical force onto the posterior pole. It was first proposed by Shevelev in 1930,148 and later modified by Thompson in 1978.149 The surgery is believed to slow the axial elongation as the reinforcement buckle band surrounds and applies direct mechanical force onto the posterior pole, and causes scleral remodeling from the non-specific inflammatory reaction between the posterior sclera and the reinforcement band. Shen et al documented significantly higher Best-Corrected Visual Acuity (BCVA) and lower refractive error in the PSR surgery group of pre-school childrencompared to the control group. The study proposed that PSR surgery combined with patching therapy is a reliable method for arresting the progression of myopia.150 Patients who underwent PSR surgery have shorter mean axial length and lower mean refractive error in comparison to the control group.151,152
In accordance with studies, newer buckle shapes, buckle materials, techniques and modifications have emerged for treatment of pathological myopia and its complications.153–155 Studies have evaluated the anatomic and functional perspective of macular buckling surgery in myopic macular hole with retinal detachment and posterior staphyloma, which reported high reattachment rates and improved visual acuity.156,157 These published results, however, are often limited by study size and non-standardized materials and surgical techniques to limit its broad adoption, to date.
Implications for Future Research
The world is currently experiencing myopia epidemic making it imperative to develop viable treatment options for adequate correction and decreased disease progression. For the past decades the environment and surroundings that children are exposed to have drastically changed, which could explain the relatively recent rapid rise in the myopic population.
In addition, children are participating in more near work activities, which has interestingly made the pediatric population more near-sighted. For example, the leisurely habit of watching TV at moderate distance of 10 feet has now evolved into using computers, tablets and cell phone at arm’s length or closer, which requires more accommodation of their eyes. With the increasing pace, technologically advanced and the competitive society, children are seldom involved in outdoor activities on a regular basis. When such factors are considered, it warrants a more efficient and successful method to treat myopia and halt its progression in young children.
To date, atropine has been the most effective and widely accepted pharmaceutical treatment for adequate control of myopic progression, but it has not yet been utilized to its greatest potential. Single-vision lenses, unlike atropine, do not prevent continued myopia progression. Atropine, on the other hand, reduces the progression of myopia and more importantly, axial elongation.
Although many theories have been postulated for understanding the mechanism of action of atropine, it remains undetermined thereby creating hesitation for its use in pediatric eyes. However, several studies have been conducted worldwide, and it has shown promising results.158,159 Overall, topical atropine has been proven to be quite effective and safe for use in most children. Despite atropine’s global success, unwanted side effects and the undetermined mechanism of action have kept society skeptical for its use in myopic correction in children.
As this and previous studies have reported, there are numerous unconventional treatment options proven to be effective for the treatment of pediatric myopia. Although none of these interventions have FDA approval, an appropriate treatment plan with informed consent must be instituted in ophthalmology clinics at once.
While many hypotheses are being generated by modern studies, there are additional areas requiring further research. First, the proposed alternative therapies will be more attractive with a thorough understanding of their mechanism of action, and the precise mechanism of the process of accommodation and emmetropization. This is achieved through additional human and animal studies.
Interventional focus must be directed towards the prevention of the myopia onset rather than the slowing of its progression. To achieve this, it is vital to educate society on the various modifiable risk factors that have been proven to be a cause of pediatric myopia. Children should be encouraged to spend more time engaging in outdoor activities, and parents, schools and policymakers should be informed of the potential benefits of outdoor activities. Furthermore, researchers must focus on investigating the alterations in the current lifestyle of children that could have been the leading cause in the recent myopia boom.
It is evident that identification of an effective and acceptable treatment to slow myopia progression has the potential for a global public health impact on children and families. This will be vital to reduce the risk of future myopia-induced ocular complications, retain the ability of myopes to remain candidates for refractive surgery in adulthood, and improve the quality of life of this expanding group of patients.
Conclusion
Myopia is a major public health concern, for which the advent of potential treatments methods for adequate correction of refractive error and decrease in disease progression is essential. Understanding the role of environmental and genetic factors in myopia onset and progression will allow for the development of more successful treatments and lifestyle modifications. Although numerous studies remain unconventional in the treatment of pediatric myopia, atropine has been widely accepted worldwide in reducing myopia progression and axial elongation. Alternative myopia treatments, including other pharmacological, optical and surgical modalities, have shown promise, but require additional studies to validate its significance. Further research will be necessary to derive a conventional treatment modality capable of reducing personal and societal burden and arresting the progression of myopic disease including worsening refraction, axial elongation and retinal degeneration.
Disclosure
Dr Balamurali Ambati reports a pending patent PCT/US2019/012501. The authors report no other conflicts of interest in this work.
References
1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
2. Wong TY, Ferreira A, Hughes R, et al. Epidemiology and disease burden of pathologic myopia and myopic choroidal neovascularization: an evidence-based systematic review. Am J Ophthalmol. 2014;157(1):9–25.e12. doi:10.1016/j.ajo.2013.08.010
3. Lee YY, Lo C-T, Sheu S-J, et al. What factors are associated with myopia in young adults? A survey study in Taiwan Military Conscripts. Invest Ophthalmol Vis Sci. 2013;54(2):1026–1033. doi:10.1167/iovs.12-10480
4. Lam CS, Lam C-H, Cheng SC-K, et al. Prevalence of myopia among Hong Kong Chinese schoolchildren: changes over two decades. Ophthalmic Physiol Opt. 2012;32(1):17–24. doi:10.1111/opo.2011.32.issue-1
5. Lim DH, Han J, Chung T-Y, et al. The high prevalence of myopia in Korean children with influence of parental refractive errors: the 2008–2012 Korean National Health and Nutrition Examination Survey. PLoS One. 2018;13(11):e0207690. doi:10.1371/journal.pone.0207690
6. Wu JF, Bi HS, Wang SM, et al. Refractive error, visual acuity and causes of vision loss in children in Shandong, China. The Shandong children eye study. PLoS One. 2013;8(12):e82763. doi:10.1371/journal.pone.0082763
7. Morgan I, Rose K. How genetic is school myopia? Prog Retin Eye Res. 2005;24(1):1–38. doi:10.1016/j.preteyeres.2004.06.004
8. Zhao J, Pan X, Sui R, et al. Refractive error study in children: results from Shunyi District, China. Am J Ophthalmol. 2000;129(4):427–435. doi:10.1016/S0002-9394(99)00452-3
9. He M, Zeng J, Liu Y, et al. Refractive error and visual impairment in urban children in southern china. Invest Ophthalmol Vis Sci. 2004;45(3):793–799. doi:10.1167/iovs.03-1051
10. Fan DSP, Lam DSC, Lam RF, et al. Prevalence, incidence, and progression of myopia of school children in Hong Kong. Invest Ophthalmol Vis Sci. 2004;45(4):1071–1075. doi:10.1167/iovs.03-1151
11. You QS, Wu LJ, Duan JL, et al. Prevalence of myopia in school children in greater Beijing: the Beijing Childhood Eye Study. Acta Ophthalmol. 2014;92(5):e398–406. doi:10.1111/aos.12299
12. Guo K, Yang DY, Wang Y, et al. Prevalence of Myopia in schoolchildren in Ejina: the Gobi desert children eye study Myopia in the Gobi desert children eye study. Invest Ophthalmol Vis Sci. 2015;56(3):1769–1774. doi:10.1167/iovs.14-15737
13. Morgan IG, French AN, Ashby RS, et al. The epidemics of myopia: aetiology and prevention. Prog Retin Eye Res. 2018;62:134–149. doi:10.1016/j.preteyeres.2017.09.004
14. Walline JJ. Myopia control: a review. Eye & Contact Lens. 2016;42(1):3–8. doi:10.1097/ICL.0000000000000207
15. Fricke TR, Holden BA, Wilson DA, et al. Global cost of correcting vision impairment from uncorrected refractive error. Bull World Health Organ. 2012;90(10):728–738. doi:10.2471/BLT.00.000000
16. Yokoi T, Moriyama M, Hayashi K, et al. Predictive factors for comorbid psychiatric disorders and their impact on vision-related quality of life in patients with high myopia. Int Ophthalmol. 2014;34(2):171–183. doi:10.1007/s10792-013-9805-8
17. Rose K, Harper R, Tromans C, et al. Quality of life in myopia. Br J Ophthalmol. 2000;84(9):1031. doi:10.1136/bjo.84.9.1031
18. Watson PG, Young RD. Scleral structure, organisation and disease. A review. Exp Eye Res. 2004;78(3):609–623. doi:10.1016/S0014-4835(03)00212-4
19. Matthijs Blankesteijn W. Has the search for a marker of activated fibroblasts finally come to an end? J Mol Cell Cardiol. 2015;88:120–123. doi:10.1016/j.yjmcc.2015.10.005
20. Keeley FW, Morin JD, Vesely S. Characterization of collagen from normal human sclera. Exp Eye Res. 1984;39(5):533–542. doi:10.1016/0014-4835(84)90053-8
21. Gentle A, Liu Y, Martin JE, et al. Collagen gene expression and the altered accumulation of scleral collagen during the development of high myopia. J Biol Chem. 2003;278(19):16587–16594. doi:10.1074/jbc.M300970200
22. Curtin BJ, Iwamoto T. Normal and staphylomatous sclera of high myopia. An electron microscopic study. Arch Ophthalmol. 1979;97(5):912–915. doi:10.1001/archopht.1979.01020010470017
23. McBrien NA, Gentle A. Role of the sclera in the development and pathological complications of myopia. Prog Retin Eye Res. 2003;22(3):307–338. doi:10.1016/S1350-9462(02)00063-0
24. McBrien NA, Lawlor P, Gentle A. Scleral remodeling during the development of and recovery from axial myopia in the tree shrew. Invest Ophthalmol Vis Sci. 2000;41(12):3713–3719.
25. Harper AR, Summers JA. The dynamic sclera: extracellular matrix remodeling in normal ocular growth and myopia development. Exp Eye Res. 2015;133:100–111. doi:10.1016/j.exer.2014.07.015
26. Sherman SM, Norton TT, Casagrande VA. Myopia in the lid-sutured tree shrew (Tupaia glis). Brain Res. 1977;124(1):154–157. doi:10.1016/0006-8993(77)90872-1
27. Schaeffel F, Feldkaemper M. Animal models in myopia research. Clin Exp Optom. 2015;98(6):507–517. doi:10.1111/cxo.12312
28. Norton TT, Rada JA. Reduced extracellular matrix in mammalian sclera with induced myopia. Vision Res. 1995;35(9):1271–1281. doi:10.1016/0042-6989(94)00243-F
29. Siegwart JT
30. Wu H, Chen W, Zhao F, et al. Scleral hypoxia is a target for myopia control. Proc Natl Acad Sci U S A. 2018;115(30):E7091–e7100. doi:10.1073/pnas.1721443115
31. Sickel W. Electrical and metabolic manifestations of receptor and higher-order neuron activity in vertebrate retina. In: Arden GB, editor. The Visual System: Neurophysiology, Biophysics, and Their Clinical Applications. Boston, MA: Springer US; 1972:101–118.
32. Li S-Y, Fu ZJ, Lo ACY. Hypoxia-induced oxidative stress in ischemic retinopathy. Oxid Med Cell Longev. 2012;2012:10. doi:10.1155/2012/426769
33. Shih Y-F, Fitzgerald MEC, Norton TT, et al. Reduction in choroidal blood flow occurs in chicks wearing goggles that induce eye growth toward myopia. Curr Eye Res. 1993;12(3):219–227. doi:10.3109/02713689308999467
34. Yancey CM, Linsenmeier RA. The electroretinogram and choroidal PO2 in the cat during elevated intraocular pressure. Invest Ophthalmol Vis Sci. 1988;29(5):700–707.
35. Ohno-Matsui K. Proposed classification of posterior staphylomas based on analyses of eye shape by three-dimensional magnetic resonance imaging and wide-field fundus imaging. Ophthalmology. 2014;121(9):1798–1809. doi:10.1016/j.ophtha.2014.03.035
36. Moriyama M, Ohno-Matsui K, Hayashi K, et al. Topographic analyses of shape of eyes with pathologic myopia by high-resolution three-dimensional magnetic resonance imaging. Ophthalmology. 2011;118(8):1626–1637. doi:10.1016/j.ophtha.2011.01.018
37. Moriyama M, Ohno-Matsui K, Modegi T, et al. Quantitative analyses of high-resolution 3D MR images of highly myopic eyes to determine their shapes software to analyze 3D MR of highly myopic eye. Investigative Opthalmology & Visual Science. 2012;53(8):4510–4518. doi:10.1167/iovs.12-9426
38. Ohno-Matsui K, Alkabes M, Salinas C, et al. Features of posterior staphylomas analyzed in wide-field fundus images in patients with unilateral and bilateral pathologic Myopia. Retina. 2017;37(3):477–486. doi:10.1097/IAE.0000000000001327
39. He M, Huang W, Zheng Y, et al. Refractive error and visual impairment in school children in rural southern China. Ophthalmology. 2007;114(2):374–382. doi:10.1016/j.ophtha.2006.08.020
40. Murthy GV, Gupta SK, Ellwein LB, et al. Refractive error in children in an urban population in New Delhi. Invest Ophthalmol Vis Sci. 2002;43(3):623–631.
41. Dandona R, Dandona L, Srinivas M, et al. Refractive error in children in a rural population in India. Invest Ophthalmol Vis Sci. 2002;43(3):615–622.
42. Lin LL, Shih YF, Hsiao CK, et al. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann Acad Med Singapore. 2004;33(1):27–33.
43. Yoon K-C, Mun G-H, Kim S-D, et al. Prevalence of eye diseases in South Korea: data from the Korea national health and nutrition examination survey 2008–2009. Korean J Ophthalmol. 2011;25(6):421–433. doi:10.3341/kjo.2011.25.6.421
44. Vitale S, Sperduto RD, Ferris FL
45. Ojaimi E, Rose KA, Morgan IG, et al. Distribution of ocular biometric parameters and refraction in a population-based study of Australian children. Invest Ophthalmol Vis Sci. 2005;46(8):2748–2754. doi:10.1167/iovs.04-1324
46. O’Donoghue LS, McClelland KJ, Logan JF, Rudnicka NS, Owen AR. Prevalence of childhood refractive error in the United Kingdom. Invest Ophthalmol Vis Sci. 2009;50(13):2562.
47. Wen G, Tarczy-Hornoch K, McKean-Cowdin R, et al. Prevalence of myopia, hyperopia, and astigmatism in non-Hispanic white and Asian children: multi-ethnic pediatric eye disease study. Ophthalmology. 2013;120(10):2109–2116. doi:10.1016/j.ophtha.2013.06.039
48. Multi-Ethnic Pediatric Eye Disease Study, G. Prevalence of myopia and hyperopia in 6- to 72-month-old african american and Hispanic children: the multi-ethnic pediatric eye disease study. Ophthalmology. 2010;117(1):140–147.e3. doi:10.1016/j.ophtha.2009.06.009
49. Kleinstein RN, Jones LA, Hullett S, et al. Refractive error and ethnicity in children. Arch Ophthalmol. 2003;121(8):1141–1147. doi:10.1001/archopht.121.8.1141
50. Ying G-S, Maguire MG, Cyert LA, et al. Prevalence of vision disorders by racial and ethnic group among children participating in head start. Ophthalmology. 2014;121(3):630–636. doi:10.1016/j.ophtha.2013.09.036
51. Theophanous C, Modjtahedi B, Batech M, et al. Myopia prevalence and risk factors in children. Clin Ophthalmol. 2018;12:1581–1587. doi:10.2147/OPTH
52. O’Donoghue L, Kapetanankis VV, McClelland JF, et al. Risk factors for childhood myopia: findings from the NICER study. Invest Ophthalmol Vis Sci. 2015;56(3):1524–1530. doi:10.1167/iovs.14-15549
53. Ip JM, Huynh SC, Robaei D, et al. Ethnic differences in the impact of parental myopia: findings from a population-based study of 12-year-old Australian children. Invest Ophthalmol Vis Sci. 2007;48(6):2520–2528. doi:10.1167/iovs.06-0716
54. Zadnik K, Satariano WA, Mutti DO, et al. The effect of parental history of myopia on children’s eye size. JAMA. 1994;271(17):1323–1327. doi:10.1001/jama.1994.03510410035029
55. Lam DSC, Fan DSP, Lam RF, et al. The effect of parental history of myopia on children’s eye size and growth: results of a longitudinal study. Invest Ophthalmol Vis Sci. 2008;49(3):873–876. doi:10.1167/iovs.06-1097
56. Liang C-L, Yen E, Su J-Y, et al. Impact of family history of high myopia on level and onset of myopia. Invest Ophthalmol Vis Sci. 2004;45(10):3446–3452. doi:10.1167/iovs.03-1058
57. Ghorbani Mojarrad N, Williams C, Guggenheim JA. A genetic risk score and number of myopic parents independently predict myopia. Ophthalmic Physiol Optics. 2018;38(5):492–502. doi:10.1111/opo.2018.38.issue-5
58. Verhoeven VJM, Hysi PG, Wojciechowski R, et al. Genome-wide meta-analyses of multiancestry cohorts identify multiple new susceptibility loci for refractive error and myopia. Nat Genet. 2013;45(3):314–318. doi:10.1038/ng.2554
59. Hysi PG, Wojciechowski R, Rahi JS, et al. Genome-wide association studies of refractive error and myopia, lessons learned, and implications for the future. Investigative Opthalmology & Visual Science. 2014;55(5):3344–3351. doi:10.1167/iovs.14-14149
60. Kiefer AK, Tung JY, Do CB, et al. Genome-wide analysis points to roles for extracellular matrix remodeling, the visual cycle, and neuronal development in Myopia. PLoS Genet. 2013;9(2):e1003299. doi:10.1371/journal.pgen.1003299
61. Wong TY, Foster PJ, Johnson GJ, et al. Education, socioeconomic status, and ocular dimensions in Chinese adults: the Tanjong Pagar Survey. The British Journal of Ophthalmology. 2002;86(9):963–968. doi:10.1136/bjo.86.9.963
62. Mutti DO, Mitchell GL, Moeschberger ML, et al. Parental Myopia, near work, school achievement, and children’s refractive error. Invest Ophthalmol Vis Sci. 2002;43(12):3633–3640.
63. Mountjoy E, Davies NM, Plotnikov D, et al. Education and myopia: assessing the direction of causality by mendelian randomisation. BMJ. 2018;361:k2022–k2022. doi:10.1136/bmj.k2022
64. Williams KM, Bertelsen G, Cumberland P, et al. Increasing prevalence of Myopia in Europe and the impact of education. Ophthalmology. 2015;122(7):1489–1497. doi:10.1016/j.ophtha.2015.03.018
65. Saw S-M, Hong C-Y, Chia K-S, et al. Nearwork and myopia in young children. The Lancet. 2001;357(9253):390. doi:10.1016/S0140-6736(05)71520-8
66. Ip JM, Saw S-M, Rose KA, et al. Role of near work in Myopia: findings in a sample of Australian school children. Investigative Opthalmology & Visual Science. 2008;49(7):2903–2910. doi:10.1167/iovs.07-0804
67. Ramessur R, Williams KM, Hammond CJ. Risk factors for myopia in a discordant monozygotic twin study. Ophthalmic Physiol Opt. 2015;35(6):643–651. doi:10.1111/opo.12246
68. Jones LA, Sinnott LT, Mutti DO, et al. Parental history of myopia, sports and outdoor activities, and future myopia. Invest Ophthalmol Vis Sci. 2007;48(8):3524–3532. doi:10.1167/iovs.06-1118
69. Rose KA, Morgan IG, Ip J, et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology. 2008;115(8):1279–1285. doi:10.1016/j.ophtha.2007.12.019
70. Dirani M, Tong L, Gazzard G, et al. Outdoor activity and myopia in Singapore teenage children. Br J Ophthalmol. 2009;93(8):997–1000. doi:10.1136/bjo.2008.150979
71. Guggenheim JA, Northstone K, McMahon G, et al. Time outdoors and physical activity as predictors of incident myopia in childhood: a prospective cohort study. Invest Ophthalmol Vis Sci. 2012;53(6):2856–2865. doi:10.1167/iovs.11-9091
72. McCarthy CS, Megaw P, Devadas M, et al. Dopaminergic agents affect the ability of brief periods of normal vision to prevent form-deprivation myopia. Exp Eye Res. 2007;84(1):100–107. doi:10.1016/j.exer.2006.09.018
73. Raviola E, Wiesel TN. Effect of dark-rearing on experimental myopia in monkeys. Invest Ophthalmol Vis Sci. 1978;17(6):485–488.
74. Crewther DP. The role of photoreceptors in the control of refractive state. Prog Retin Eye Res. 2000;19(4):421–457. doi:10.1016/s1350-9462(00)00004-5
75. Fredrick DR. Myopia. BMJ. 2002;324(7347):1195–1199. doi:10.1136/bmj.324.7347.1195
76. Iuvone PM, Tigges M, Fernandes A, et al. Dopamine synthesis and metabolism in rhesus monkey retina: development, aging, and the effects of monocular visual deprivation. Vis Neurosci. 1989;2(5):465–471. doi:10.1017/s0952523800012360
77. Stone RA, Lin T, Laties AM, et al. Retinal dopamine and form-deprivation myopia. Proc Natl Acad Sci U S A. 1989;86(2):704–706. doi:10.1073/pnas.86.2.704
78. Dong F, Zhi Z, Pan M, et al. Inhibition of experimental myopia by a dopamine agonist: different effectiveness between form deprivation and hyperopic defocus in guinea pigs. Mol Vis. 2011;17:2824–2834.
79. Gao Q, Liu Q, Ma P, et al. Effects of direct intravitreal dopamine injections on the development of lid-suture induced myopia in rabbits. Graefes Arch Clin Exp Ophthalmol. 2006;244(10):1329–1335. doi:10.1007/s00417-006-0254-1
80. Junfeng M, Shuangzhen L, Wenjuan Q, et al. Levodopa inhibits the development of form-deprivation myopia in guinea pigs. Optom Vis Sci. 2010;87(1):53–60. doi:10.1097/OPX.0b013e3181c12b3d
81. Beaulieu J-M, Gainetdinov RR, Sibley DR. The physiology, signaling, and pharmacology of dopamine receptors. Pharmacol Rev. 2011;63(1):182–217. doi:10.1124/pr.110.002642
82. Schmid KL, Strasberg G, Rayner CL, et al. The effects and interactions of GABAergic and dopaminergic agents in the prevention of form deprivation myopia by brief periods of normal vision. Exp Eye Res. 2013;110:88–95. doi:10.1016/j.exer.2013.02.017
83. Huang F, Yan T, Shi F, et al. Activation of dopamine D2 receptor is critical for the development of form-deprivation myopia in the C57BL/6 mouse. Invest Ophthalmol Vis Sci. 2014;55(9):5537–5544. doi:10.1167/iovs.13-13211
84. Zhang S, Yang J, Reinach PS, et al. Dopamine receptor subtypes mediate opposing effects on form deprivation Myopia in pigmented guinea pigs. Invest Ophthalmol Vis Sci. 2018;59(11):4441–4448. doi:10.1167/iovs.17-21574
85. Stone RA, Laties AM, Raviola E, et al. Increase in retinal vasoactive intestinal polypeptide after eyelid fusion in primates. Proc Natl Acad Sci U S A. 1988;85(1):257–260. doi:10.1073/pnas.85.1.257
86. Stone RA, Kuwayama Y, Laties AM. Regulatory peptides in the eye. Experientia. 1987;43(7):791–800. doi:10.1007/BF01945357
87. Seltner RL, Stell WK. The effect of vasoactive intestinal peptide on development of form deprivation myopia in the chick: a pharmacological and immunocytochemical study. Vision Res. 1995;35(9):1265–1270. doi:10.1016/0042-6989(94)00244-G
88. Shih Y-F, Fitzgerald M, Cuthbertson SL, et al. Influence of ophthalmic nerve fibers on choroidal blood flow and myopic eye growth in chicks. Exp Eye Res. 1999;69(1):9–20. doi:10.1006/exer.1999.0692
89. Stone RA, Kuwayama Y. Substance P-like immunoreactive nerves in the human eye. Arch Ophthalmol. 1985;103(8):1207–1211. doi:10.1001/archopht.1985.01050080119031
90. Corvetti G, Pignocchino P, Sisto Daneo L. Distribution and development of substance P immunoreactive axons in the chick cornea and uvea. Basic Appl Histochem. 1988;32(1):187–192.
91. Denis P, Fardin V, Nordmann JP, et al. Localization and characterization of substance P binding sites in rat and rabbit eyes. Invest Ophthalmol Vis Sci. 1991;32(6):1894–1902.
92. Raecker ME, AK L. Diagnosis of CNV in Myopic Macular Degeneration. EyeNet; 2015:35–37.
93. Yokoi T, Ohno-Matsui K. Diagnosis and Treatment of Myopic Maculopathy. RetinaToday; 2014:37–40.
94. Saw S-M, Gazzard G, Shih-Yen EC, et al. Myopia and associated pathological complications. Ophthalmic Physiol Optics. 2005;25(5):381–391. doi:10.1111/j.1475-1313.2005.00298.x
95. Green WR, Wilson DJ. Choroidal neovascularization. Ophthalmology. 1986;93(9):1169–1176. doi:10.1016/S0161-6420(86)33609-1
96. Wong TY, et al. Myopic choroidal neovascularisation: current concepts and update on clinical management. Br J Ophthalmol. 2015;99(3):289–296.
97. Yoshida T, Ohno-Matsui K, Yasuzumi K, et al. Myopic choroidal neovascularization: a 10-year follow-up. Ophthalmology. 2003;110(7):1297–1305. doi:10.1016/S0161-6420(03)00461-5
98. Muller B, Joussen AM. Myopic traction maculopathy - vitreoretinal traction syndrome in high myopic eyes and posterior staphyloma. Klin Monbl Augenheilkd. 2011;228(9):771–779. doi:10.1055/s-0031-1281714
99. Takano M, Kishi S. Foveal retinoschisis and retinal detachment in severely myopic eyes with posterior staphyloma. Am J Ophthalmol. 1999;128(4):472–476. doi:10.1016/S0002-9394(99)00186-5
100. Ikuno Y, Tano Y. Vitrectomy for macular holes associated with myopic foveoschisis. Am J Ophthalmol. 2006;141(4):774–776. doi:10.1016/j.ajo.2005.11.044
101. Bando H, Ikuno Y, Choi J-S, et al. Ultrastructure of internal limiting membrane in myopic foveoschisis. Am J Ophthalmol. 2005;139(1):197–199. doi:10.1016/j.ajo.2004.07.027
102. Panozzo G, Mercanti A. Optical coherence tomography findings in myopic traction maculopathy. Arch Ophthalmol. 2004;122(10):1455–1460. doi:10.1001/archopht.122.10.1455
103. Benhamou N, Massin P, Haouchine B, et al. Macular retinoschisis in highly myopic eyes. Am J Ophthalmol. 2002;133(6):794–800. doi:10.1016/S0002-9394(02)01394-6
104. Gohil R, Sivaprasad S, Han LT, et al. Myopic foveoschisis: a clinical review. Eye (Lond). 2015;29(5):593–601. doi:10.1038/eye.2014.311
105. Kobayashi H, Kobayashi K, Okinami S. Macular hole and myopic refraction. Br J Ophthalmol. 2002;86(11):1269–1273. doi:10.1136/bjo.86.11.1269
106. Gwiazda J. Treatment options for myopia. Optometry Vision Sci. 2009;86(6):624–628. doi:10.1097/OPX.0b013e3181a6a225
107. Hung L-F, Crawford ML, Smith EL. Spectacle lenses alter eye growth and the refractive status of young monkeys. Nat Med. 1995;1(8):761–765. doi:10.1038/nm0895-761
108. Chung K, Mohidin N, O’Leary DJ. Undercorrection of myopia enhances rather than inhibits myopia progression. Vision Res. 2002;42(22):2555–2559. doi:10.1016/S0042-6989(02)00258-4
109. Adler D, Millodot M. The possible effect of undercorrection on myopic progression in children. Clin Exp Optom. 2006;89(5):315–321. doi:10.1111/cxo.2006.89.issue-5
110. Sankaridurg P, Donovan L, Varnas S, et al. Spectacle lenses designed to reduce progression of myopia: 12-month results. Optometry Vision Sci. 2010;87(9):631–641. doi:10.1097/OPX.0b013e3181ea19c7
111. Kanda H, Oshika T, Hiraoka T, et al. Effect of spectacle lenses designed to reduce relative peripheral hyperopia on myopia progression in Japanese children: a 2-year multicenter randomized controlled trial. Jpn J Ophthalmol. 2018;62(5):537–543. doi:10.1007/s10384-018-0616-3
112. Gwiazda J, e A. Progressive-addition lenses versus single-vision lenses for slowing progression of myopia in children with high accommodative lag and near esophoria. Invest Ophthalmol Vis Sci. 2011;52(5):2749–2757.
113. Walline JJ, Mutti DO, Jones LA, et al. The contact lens and myopia progression (CLAMP) study: design and baseline data. Optom Vis Sci. 2001;78(4):223–233. doi:10.1097/00006324-200104000-00011
114. Grosvenor T, PERRIGIN D, PERRIGIN J, et al. Rigid gas-permeable contact lenses for myopia control: effects of discontinuation of lens wear. Optom Vis Sci. 1991;68(5):385–389. doi:10.1097/00006324-199105000-00011
115. Khoo CY, Chong J, Rajan U. A 3-year study on the effect of RGP contact lenses on myopic children. Singapore Med J. 1999;40(4):230–237.
116. Katz J, Schein OD, Levy B, et al. A randomized trial of rigid gas permeable contact lenses to reduce progression of children’s myopia. Am J Ophthalmol. 2003;136(1):82–90. doi:10.1016/S0002-9394(03)00106-5
117. Walline JJ, Greiner KL, McVey ME, et al. Multifocal contact lens myopia control. Optom Vis Sci. 2013;90(11):1207–1214. doi:10.1097/OPX.0000000000000036
118. Anstice NS, Phillips JR. Effect of dual-focus soft contact lens wear on axial myopia progression in children. Ophthalmology. 2011;118(6):1152–1161. doi:10.1016/j.ophtha.2010.10.035
119. Beasley IG, Davies LN, Logan NS. Effect of peripheral defocus on axial eye growth and modulation of refractive error in hyperopes: protocol for a nonrandomized clinical trial. JMIR Res Protoc. 2018;7(9):e173–e173. doi:10.2196/resprot.9320
120. Lam CSY, Tang WC, Tse DY-Y, et al. Defocus Incorporated Soft Contact (DISC) lens slows myopia progression in Hong Kong Chinese schoolchildren: a 2-year randomised clinical trial. Br J Ophthalmol. 2014;98(1):40–45. doi:10.1136/bjophthalmol-2013-303914
121. Lam CSY, Tang WC, Tse DY, et al. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomised clinical trial. Br J Ophthalmol. 2019;
122. Lu Y, Lin Z, Wen L, et al. The adaptation and acceptance of defocus incorporated multiple segment lens for Chinese children. Am J Ophthalmol. 2019. doi:10.1016/j.ajo.2019.12.002
123. Ruiz-Pomeda A, Pérez-Sánchez B, Valls I, et al. MiSight Assessment Study Spain (MASS). A 2-year randomized clinical trial. Graefes Arch Clin Exp Ophthalmol. 2018;256(5):1011–1021. doi:10.1007/s00417-018-3906-z
124. Chamberlain P, Peixoto-de-Matos SC, Logan NS, et al. A 3-year randomized clinical trial of MiSight lenses for myopia control. Optom Vis Sci. 2019;96(8):556–567. doi:10.1097/OPX.0000000000001410
125. Saw SM, Gazzard G, Au Eong K-G, et al. Myopia: attempts to arrest progression. Br J Ophthalmol. 2002;86(11):1306–1311. doi:10.1136/bjo.86.11.1306
126. Polse KA, BRAND RJ, SCHWALBE JS, et al. The Berkeley Orthokeratology Study, Part II: efficacy and duration. Am J Optom Physiol Opt. 1983;60(3):187–198. doi:10.1097/00006324-198303000-00006
127. Leo S-W, Young TL. An evidence-based update on myopia and interventions to retard its progression. J AAPOS. 2011;15(2):181–189. doi:10.1016/j.jaapos.2010.09.020
128. Cho P, Cheung SW, Edwards M. The longitudinal orthokeratology research in children (LORIC) in Hong Kong: a pilot study on refractive changes and myopic control. Curr Eye Res. 2005;30(1):71–80. doi:10.1080/02713680590907256
129. Liu YM, Xie P. The safety of orthokeratology–a systematic review. Eye Contact Lens. 2016;42(1):35–42. doi:10.1097/ICL.0000000000000219
130. Kam KW, Yung W, Li GKH, et al. Infectious keratitis and orthokeratology lens use: a systematic review. Infection. 2017;45(6):727–735. doi:10.1007/s15010-017-1023-2
131. Barathi VA, Weon SR, Beuerman RW. Expression of muscarinic receptors in human and mouse sclera and their role in the regulation of scleral fibroblasts proliferation. Mol Vis. 2009;15:1277–1293.
132. Barathi VA, Beuerman RW. Molecular mechanisms of muscarinic receptors in mouse scleral fibroblasts: prior to and after induction of experimental myopia with atropine treatment. Mol Vis. 2011;17:680–692.
133. Lee C-Y, Sun -C-C, Lin Y-F, et al. Effects of topical atropine on intraocular pressure and myopia progression: a prospective comparative study. BMC Ophthalmol. 2016;16:114. doi:10.1186/s12886-016-0297-y
134. Chua W-H, Balakrishnan V, Chan Y-H, et al. Atropine for the treatment of childhood myopia. Ophthalmology. 2006;113(12):2285–2291. doi:10.1016/j.ophtha.2006.05.062
135. Chia A, Chua W-H, Cheung Y-B, et al. Atropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology. 2012;119(2):347–354. doi:10.1016/j.ophtha.2011.07.031
136. Chia A, Lu Q-S, Tan D. Five-year clinical trial on atropine for the treatment of Myopia 2: myopia control with atropine 0.01% eyedrops. Ophthalmology. 2016;123(2):391–399. doi:10.1016/j.ophtha.2015.07.004
137. Shih Y-F, Hsiao CK, Chen C-J, et al. An intervention trial on efficacy of atropine and multi-focal glasses in controlling myopic progression. Acta Ophthalmol Scand. 2001;79(3):233–236. doi:10.1034/j.1600-0420.2001.790304.x
138. Yam JC, Jiang Y, Tang SM, et al. Low-Concentration Atropine for Myopia Progression (LAMP) study: a randomized, double-blinded, placebo-controlled trial of 0.05%, 0.025%, and 0.01% atropine eye drops in Myopia control. Ophthalmology. 2019;126(1):113–124. doi:10.1016/j.ophtha.2018.05.029
139. Siatkowski RM, et al. Safety and efficacy of 2% pirenzepine ophthalmic gel in children with myopia: a 1-year, multicenter, double-masked, placebo-controlled parallel study. Arch Ophthalmol. 2004;122(11):1667–1674. doi:10.1001/archopht.122.11.1667
140. Truong H-T, Cottriall CL, Gentle A, et al. Pirenzepine affects scleral metabolic changes in myopia through a non-toxic mechanism. Exp Eye Res. 2002;74(1):103–111. doi:10.1006/exer.2001.1107
141. Xu Z-W, Chen X, Jin X-H, et al. SILAC-based proteomic analysis reveals that salidroside antagonizes cobalt chloride-induced hypoxic effects by restoring the tricarboxylic acid cycle in cardiomyocytes. J Proteomics. 2016;130:211–220. doi:10.1016/j.jprot.2015.09.028
142. Wu J, Ke X, Ma N, et al. Formononetin, an active compound of Astragalus membranaceus (Fisch) Bunge, inhibits hypoxia-induced retinal neovascularization via the HIF-1α/VEGF signaling pathway. Drug Des Devel Ther. 2016;10:3071–3081. doi:10.2147/DDDT
143. Lai M-C, Lin J-G, Pai P-Y, et al. Protective effect of salidroside on cardiac apoptosis in mice with chronic intermittent hypoxia. Int J Cardiol. 2014;174(3):565–573. doi:10.1016/j.ijcard.2014.04.132
144. Huang X, Zou L, Yu X, et al. Salidroside attenuates chronic hypoxia-induced pulmonary hypertension via adenosine A2a receptor related mitochondria-dependent apoptosis pathway. J Mol Cell Cardiol. 2015;82:153–166. doi:10.1016/j.yjmcc.2015.03.005
145. Bishopric NH, Andreka, P., Slepak, T., & Webster, K. A, et al. Molecular mechanisms of apoptosis in the cardiac myocyte. Curr Opin Pharmacol. 2001;1(2):141–150. doi:10.1016/S1471-4892(01)00032-7
146. Zhong X, Lin R, Li Z, et al. Effects of Salidroside on cobalt chloride-induced hypoxia damage and mTOR signaling repression in PC12 cells. Biol Pharm Bull. 2014;37(7):1199–1206. doi:10.1248/bpb.b14-00100
147. Sun M, Zhou T, Zhou L, et al. Formononetin protects neurons against hypoxia-induced cytotoxicity through upregulation of ADAM10 and sAbetaPPalpha. J Alzheimers Dis. 2012;28(4):795–808. doi:10.3233/JAD-2011-110506
148. Shevelev M. Operation against high myopia and scleralectasia with aid of the transplantation of fascia lata on thinned sclera. Russ Oftalmol J. 1930;11:107–110.
149. Thompson FB. A simplified scleral reinforcement technique. Am J Ophthalmol. 1978;86(6):782–790. doi:10.1016/0002-9394(78)90121-6
150. Shen Z-M, Zhang Z-Y, Zhang L-Y, et al. Posterior scleral reinforcement combined with patching therapy for pre-school children with unilateral high myopia. Graefes Arch Clin Exp Ophthalmol. 2015;253(8):1391–1395. doi:10.1007/s00417-015-2963-9
151. Li X-J, Yang X-P, Li Q-M, et al. Posterior scleral reinforcement for the treatment of pathological myopia. Int J Ophthalmol. 2016;9(4):580–584. doi:10.18240/ijo.2016.04.18
152. Liu XD, Lu JH, Chu RY. Long-term studies on clinical therapeutic efficiency of posterior scleral reinforcement surgery. Zhonghua Yan Ke Za Zhi. 2011;47(6):527–530.
153. Parolini B, Frisina R, Pinackatt S, et al. Indications and results of a new L-shaped macular buckle to support a posterior staphyloma in high Myopia. Retina. 2015;35(12):2469–2482. doi:10.1097/IAE.0000000000000613
154. Devin F, Tsui I, Morin B, et al. T-shaped scleral buckle for macular detachments in high myopes. Retina. 2011;31(1):177–180. doi:10.1097/IAE.0b013e3181fc7e73
155. Stirpe M, Ripandelli G, Rossi T, et al. A new adjustable macular buckle designed for highly Myopic eyes. Retina (Philadelphia, PA). 2012;32(7):1424–1427. doi:10.1097/IAE.0b013e3182550648
156. Theodossiadis GP, Theodossiadis PG. The macular buckling procedure in the treatment of retinal detachment in highly myopic eyes with macular hole and posterior staphyloma: mean follow-up of 15 years. Retina. 2005;25(3):285–289. doi:10.1097/00006982-200504000-00006
157. Sasoh M, Yoshida S, Ito Y, et al. Macular buckling for retinal detachment due to macular hole in highly myopic eyes with posterior staphyloma. Retina. 2000;20(5):445–449. doi:10.1097/00006982-200005000-00003
158. Vagge A, Ferro Desideri L, Nucci P, Serafino M. Prevention of progression in Myopia: a systematic review. Diseases. 2018;6(4).
159. Sankaridurg P, et al. Controlling progression of Myopia: optical and pharmaceutical strategies. Asia Pac J Ophthalmol (Phila). 2018.
160. Young TL, Ronan SM, Alvear AB, et al. A second locus for familial high myopia maps to chromosome 12q. The American Journal of Human Genetics. 1998;63(5):1419–1424. doi:10.1086/302111
161. Young TL, Atwood LD, Ronan SM, et al. Further refinement of the MYP2 locus for autosomal dominant high myopia by linkage disequilibrium analysis. Ophthalmic Genet. 2001;22(2):69–75. doi:10.1076/opge.22.2.69.2233
162. Scavello GS, Paluru PC, Ganter WR, et al. Sequence variants in the Transforming Growth β-Induced Factor (TGIF) gene are not associated with high Myopia. Invest Ophthalmol Vis Sci. 2004;45(7):2091–2097. doi:10.1167/iovs.03-0933
163. Paluru P, Ronan SM, Heon E, et al. New locus for autosomal dominant high myopia maps to the long arm of chromosome 17. Invest Ophthalmol Vis Sci. 2003;44(5):1830–1836. doi:10.1167/iovs.02-0697
164. Hammond CJ, Andrew T, Tat Mak Y, et al. A susceptibility locus for myopia in the normal population is linked to the PAX6 gene region on chromosome 11: a genomewide scan of dizygotic twins. The American Journal of Human Genetics. 2004;75(2):294–304. doi:10.1086/423148
165. Stambolian D, Ibay G, Reider L, et al. Genomewide linkage scan for myopia susceptibility loci among Ashkenazi Jewish families shows evidence of linkage on chromosome 22q12. Am J Hum Genet. 2004;75(3):448–459. doi:10.1086/423789
166. Zhang Q, Guo X, Xiao X, et al. A new locus for autosomal dominant high myopia maps to 4q22-q27 between D4S1578 and D4S1612. Mol Vis. 2005;11:554–560.
167. Paluru PC, Nallasamy S, Devoto M, et al. Identification of a novel locus on 2q for autosomal dominant high-grade Myopia. Investigative Opthalmology & Visual Science. 2005;46(7):2300–2307. doi:10.1167/iovs.04-1423
168. Wojciechowski R, Moy C, Ciner E, et al. Genomewide scan in Ashkenazi Jewish families demonstrates evidence of linkage of ocular refraction to a QTL on chromosome 1p36. Hum Genet. 2006;119(4):389–399. doi:10.1007/s00439-006-0153-x
169. Zhang Q, et al. Novel locus for X linked recessive high myopia maps to Xq23-q25 but outside MYP1. J Med Genet. 2006;43(5):e20. doi:10.1136/jmg.2005.037853
170. Nallasamy S, Paluru PC, Devoto M, et al. Genetic linkage study of high-grade myopia in a Hutterite population from South Dakota. Mol Vis. 2007;13:229–236.
171. Ciner E, Wojciechowski R, Ibay G, et al. Genomewide scan of ocular refraction in African-American families shows significant linkage to chromosome 7p15. Genet Epidemiol. 2008;32(5):454–463. doi:10.1002/gepi.v32:5
172. Paget S, Julia S, Vitezica ZG, et al. Linkage analysis of high myopia susceptibility locus in 26 families. Mol Vis. 2008;14:2566–2574.
173. Lam CY, Tam POS, Fan DSP, et al. A genome-wide scan maps a novel high myopia locus to 5p15. Invest Ophthalmol Vis Sci. 2008;49(9):3768–3778. doi:10.1167/iovs.07-1126
174. Ciner E, Ibay G, Wojciechowski R, et al. Genome-wide scan of African-American and white families for linkage to myopia. Am J Ophthalmol. 2009;147(3):512–517.e2. doi:10.1016/j.ajo.2008.09.004
175. Yang Z, Xiao X, Li S, et al. Clinical and linkage study on a consanguineous Chinese family with autosomal recessive high myopia. Mol Vis. 2009;15:312–318.
176. Hysi PG, Young TL, Mackey DA, et al. A genome-wide association study for myopia and refractive error identifies a susceptibility locus at 15q25. Nat Genet. 2010;42(10):902–905. doi:10.1038/ng.664
177. Solouki AM, Verhoeven VJM, van Duijn CM, et al. A genome-wide association study identifies a susceptibility locus for refractive errors and myopia at 15q14. Nat Genet. 2010;42(10):897–901. doi:10.1038/ng.663
178. Ma J-H, Shen S-H, Zhang G-W, et al. Identification of a locus for autosomal dominant high myopia on chromosome 5p13.3-p15.1 in a Chinese family. Mol Vis. 2010;16:2043–2054.
179. Guo X, Xiao X, Li S, et al. Nonsyndromic high myopia in a Chinese family mapped to MYP1: linkage confirmation and phenotypic characterization. Arch Ophthalmol. 2010;128(11):1473–1479. doi:10.1001/archophthalmol.2010.270
180. Rydzanicz M, Nath SK, Sun C, et al. Identification of novel suggestive loci for high-grade myopia in Polish families. Mol Vis. 2011;17:2028–2039.
181. Han S, Chen P, Fan Q, et al. Association of variants in FRAP1 and PDGFRA with corneal curvature in Asian populations from Singapore. Hum Mol Genet. 2011;20(18):3693–3698. doi:10.1093/hmg/ddr269
182. Yu Z, Zhou J, Chen X, et al. Polymorphisms in the CTNND2 gene and 11q24.1 genomic region are associated with pathological myopia in a Chinese population. Ophthalmologica. 2012;228(2):123–129. doi:10.1159/000338188
183. Abbott D, Li Y-J, Guggenheim JA, et al. An international collaborative family-based whole genome quantitative trait linkage scan for myopic refractive error. Mol Vis. 2012;18:720–729.
184. Fan Q, Barathi VA, Cheng C-Y, et al. Genetic variants on chromosome 1q41 influence ocular axial length and high myopia. PLoS Genet. 2012;8(6):e1002753–e1002753. doi:10.1371/journal.pgen.1002753
185. Mishra A, Yazar S, Hewitt AW, et al. Genetic variants near PDGFRA are associated with corneal curvature in Australians. Investigative Opthalmology & Visual Science. 2012;53(11):7131–7136. doi:10.1167/iovs.12-10489
186. Cheng C-Y, Schache M, Ikram M, et al. Nine loci for ocular axial length identified through genome-wide association studies, including shared loci with refractive error. Am J Hum Genet. 2013;93(2):264–277. doi:10.1016/j.ajhg.2013.06.016
187. Guggenheim JA, McMahon G, Kemp JP, et al. A genome-wide association study for corneal curvature identifies the platelet-derived growth factor receptor α gene as a quantitative trait locus for eye size in white Europeans. Mol Vis. 2013;19:243–253.
188. Wang H, Yang M, Su S, et al. Association of ZNF644, GRM6 and CTNND2 genes polymorphisms with high myopia. Zhonghua Yi Xue Za Zhi. 2014;94(17):1289–1293.
189. Chen T, Shan G, Ma J, et al. Polymorphism in the RASGRF1 gene with high myopia: a meta-analysis. Mol Vis. 2015;21:1272–1280.
190. Wang H, Su S, Yang M, et al. Association of ZNF644, GRM6, and CTNND2 genes with high myopia in the Han Chinese population: Jiangsu Eye Study. Eye (Lond). 2016;30(7):1017–1022. doi:10.1038/eye.2016.8
191. Liao X, Yap MKH, Leung KH, et al. Genetic association study of KCNQ5 polymorphisms with high Myopia. Biomed Res Int. 2017;2017:3024156. doi:10.1155/2017/3024156
192. Musolf AM, Simpson CL, Moiz BA, et al. Caucasian families exhibit significant linkage of Myopia to chromosome 11p. Investigative Opthalmology & Visual Science. 2017;58(9):3547–3554. doi:10.1167/iovs.16-21271
193. Musolf AM, Simpson CL, Long KA, et al. Myopia in Chinese families shows linkage to 10q26.13. Mol Vis. 2018;24:29–42.
194. Wojciechowski R, Stambolian D, Ciner E, et al. Genomewide linkage scans for ocular refraction and meta-analysis of four populations in the Myopia family study. Investigative Opthalmology & Visual Science. 2009;50(5):2024–2032. doi:10.1167/iovs.08-2848
195. Brodstein RS, Brodstein DE, Olson RJ, et al. The treatment of myopia with atropine and bifocals. A long-term prospective study. Ophthalmology. 1984;91(11):1373–1378. doi:10.1016/S0161-6420(84)34138-0
196. Yen MY, Liu JH, Kao SC, et al. Comparison of the effect of atropine and cyclopentolate on myopia. Ann Ophthalmol. 1989;21(5):180–2, 187.
197. Chou A-C, SHIH Y-F, HO T-C, et al. The effectiveness of 0.5% atropine in controlling high myopia in children. J Ocul Pharmacol Ther. 1997;13(1):61–67. doi:10.1089/jop.1997.13.61
198. Shih Y-F, CHEN C-H, CHOU A-C, et al. Effects of different concentrations of atropine on controlling myopia in myopic children. J Ocul Pharmacol Ther. 1999;15(1):85–90. doi:10.1089/jop.1999.15.85
199. Kennedy RH, Dyer JA, Kennedy MA, et al. Reducing the progression of myopia with atropine: a long term cohort study of Olmsted County students. Binocul Vis Strabismus Q. 2000;15(3 Suppl):281–304.
200. Hsiao CK, Chen CJ, Shih YF, et al. Design and statistical analysis for the Myopia intervention trial in Taiwan. In: Myopia Updates II. Tokyo: Springer Japan; 2000:161-164..
201. Lee J-J, Fang P-C, Yang I-H, et al. Prevention of myopia progression with 0.05% atropine solution. J Ocul Pharmacol Ther. 2006;22(1):41–46. doi:10.1089/jop.2006.22.41
202. Fan DSP, Lam DSC, Chan CKM, et al. Topical atropine in retarding myopic progression and axial length growth in children with moderate to severe myopia: a pilot study. Jpn J Ophthalmol. 2007;51(1):27–33. doi:10.1007/s10384-006-0380-7
203. Liang C-K, Ho T-Y, Li T-C, et al. A combined therapy using stimulating auricular acupoints enhances lower-level atropine eyedrops when used for myopia control in school-aged children evaluated by a pilot randomized controlled clinical trial. Complement Ther Med. 2008;16(6):305–310. doi:10.1016/j.ctim.2008.04.007
204. Fang P-C, Chung M-Y, Yu H-J, et al. Prevention of myopia onset with 0.025% atropine in premyopic children. J Ocul Pharmacol Ther. 2010;26(4):341–345. doi:10.1089/jop.2009.0135
205. Wu PC, Yang YH, Fang PC. The long-term results of using low-concentration atropine eye drops for controlling myopia progression in schoolchildren. J Ocul Pharmacol Ther. 2011;27(5):461–466. doi:10.1089/jop.2011.0027
206. Lin L, Weizhong L, Yunru L, et al. Treatment outcomes of myopic anisometropia with 1% atropine: a pilot study. Optom Vis Sci. 2013;90(12):1486–1492. doi:10.1097/OPX.0000000000000097
207. Chia A, Li W, Tan D, et al. Full-field electroretinogram findings in children in the atropine treatment for myopia (ATOM2) study. Doc Ophthalmol. 2013;126(3):177–186. doi:10.1007/s10633-012-9372-8
208. Cooper J, Eisenberg N, Schulman E, et al. Maximum atropine dose without clinical signs or symptoms. Optom Vis Sci. 2013;90(12):1467–1472. doi:10.1097/OPX.0000000000000037
209. Lin H-J, Wan L, Tsai F-J, et al. Overnight orthokeratology is comparable with atropine in controlling myopia. BMC Ophthalmol. 2014;14(1):40. doi:10.1186/1471-2415-14-40
210. Cheng HC, Hsieh YT. The effect of low-concentration atropine combined with auricular acupoint stimulation in myopia control. Complement Ther Med. 2014;22(3):449–455. doi:10.1016/j.ctim.2014.03.004
211. Li S-M, Wu -S-S, Kang M-T, et al. Atropine slows myopia progression more in Asian than white children by meta-analysis. Optom Vis Sci. 2014;91(3):342–350. doi:10.1097/OPX.0000000000000178
212. Chia A, Chua W-H, Wen L, et al. Atropine for the treatment of childhood myopia: changes after stopping atropine 0.01%, 0.1% and 0.5%. Am J Ophthalmol. 2014;157(2):451–457.e1. doi:10.1016/j.ajo.2013.09.020
213. Kumaran A, Htoon HM, Tan D, et al. Analysis of changes in refraction and biometry of atropine- and placebo-treated eyes. Invest Ophthalmol Vis Sci. 2015;56(9):5650–5655. doi:10.1167/iovs.14-14716
214. Yi S, Huang Y, Yu S-Z, et al. Therapeutic effect of atropine 1% in children with low myopia. J AAPOS. 2015;19(5):426–429. doi:10.1016/j.jaapos.2015.04.006
215. Clark TY, Clark RA. Atropine 0.01% eyedrops significantly reduce the progression of childhood Myopia. J Ocul Pharmacol Ther. 2015;31(9):541–545. doi:10.1089/jop.2015.0043
216. Polling JR, Kok RGW, Tideman JWL, et al. Effectiveness study of atropine for progressive myopia in Europeans. Eye (Lond). 2016;30(7):998–1004. doi:10.1038/eye.2016.78
217. Loughman J, Flitcroft D. The acceptability and visual impact of 0.01% atropine in a Caucasian population. The British Journal of ophthalmology. 2016;100(11):1525–1529. doi:10.1136/bjophthalmol-2015-307861
218. Kothari M, Rathod V. Efficacy of 1% atropine eye drops in retarding progressive axial myopia in Indian eyes. Indian J Ophthalmol. 2017;65(11):1178–1181. doi:10.4103/ijo.IJO_418_17
219. Wan L, et al. The synergistic effects of orthokeratology and atropine in slowing the progression of Myopia. J Clin Med. 2018;7(9):259.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.