")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Parental Willingness to Vaccinate Their Children Against SARS-CoV-2 in Jordan: An Explanatory Cross-Sectional Study
Authors Alsulaiman JW, Mazin M, Al-Shatanawi TN , Kheirallah KA , Allouh MZ
Received 4 February 2022
Accepted for publication 4 May 2022
Published 10 May 2022 Volume 2022:15 Pages 955—967
DOI https://doi.org/10.2147/RMHP.S360838
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Haiyan Qu
Jomana W Alsulaiman,1 Mai Mazin,1 Tariq N Al-Shatanawi,2 Khalid A Kheirallah,3 Mohammed Z Allouh4
1Department of Pediatrics, Faculty of Medicine, Yarmouk University, Irbid, Jordan; 2Department of Public Health, Faculty of Medicine, Al-Balqa Applied University, Salt, Jordan; 3Department of Public Health and Community Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 4Department of Anatomy, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates
Correspondence: Mohammed Z Allouh, Department of Anatomy, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, 15551, United Arab Emirates, Tel +971 3713 7551, Email [email protected]
Background: Successful control of the COVID-19 pandemic is largely dependent on vaccine administration to epidemiologically influential groups, including children. Considering that pediatric population comprises a significant portion on the population in developing countries, and their risk of infection and spreading the disease has been underestimated, it is crucial to investigate parental willingness to administer SARS-CoV-2 vaccine to their children between 5 and 11 years old. This study investigates the prevalence and determinants of parental willingness towards vaccinating their children (5– 12 years old) against COVID-19 in a developing country setting, Jordan.
Methods: A cross-sectional study, conducted between October and November 2021, utilized online Google Forms to collect data on parents’ background characteristics, willingness to vaccinate their children, SARS-CoV-2, infection and vaccine, risk perception, and factors affecting decision to vaccinate.
Results: A total of 564 parents completed the questionnaire; 82.8% were mothers, 85.3% were 30 years of age or older, and 75.9% had bachelor’s degrees or higher. Only 25.4% of parents reported willingness to vaccinate their 5– 12 years old children against SARS-CoV-2. Lower parental age, higher income, and having health insurance coverage increased parental willingness. Among participants vaccinated against COVID-19, only 29.0% were willing to vaccinate their children. Healthcare providers’ trust and vaccine recommendations by pediatricians increased parental willingness. COVID-19 risk perception seems to have negative effects on parental willingness.
Conclusion: A significant proportion of parents in Jordan indicated hesitancy towards administering COVID-19 vaccine for their children. Concerns about vaccine safety and trust in the healthcare system appear to be the most important predictors of parents’ hesitancy. Effective vaccine campaigns should focus on risk perception and communication and should consider parental socio-demographic characteristics.
Keywords: SARS-CoV-2, COVID-19, vaccine hesitancy, willingness, children, Jordan, risk perception
Introduction
The ongoing COVID-19 pandemic continues to be a major global public health threat.1 With newly evolving variants of concern, SARS-CoV-2 seems to introduce a surge in numbers of reported cases, hospitalization and deaths. Epidemiologically influential groups affected by the pandemic include children of all ages, among others. This group was initially believed to be immune to the pandemic and recent reopening of schools have shown the critical impact of children in spreading the infection at the community levels.2–4 On November 2021, COVID-19 vaccines have been authorized for use in children above 5 years old as COVID-19 mRNA vaccine was declared safe and effective for this age groups by the CDC.5 Immunization of children and adults will be a cornerstone in combating the spread of COVID-19.6
In Jordan, more than one million of COVID-19 cases have been reported as of March 2022 along with more than 12 thousand COVID-19 related deaths.7 About 20% of the total reported cases were below 18 years of age, with an incidence rate for younger age groups (below age of 18) being 8.2%. These rates were comparable to those of in other age groups.8 Jordan engaged the global efforts to fight COVID-19 crisis and launched the national vaccination campaign in January 2021 targeting people above 18 years, initially, then, on July 25, 2021, children above 12 years old.7 Today, four different COVID-19 vaccines are approved in Jordan, with about 40% of the total population being fully vaccinated, and about 60% of adults.8 Regardless, Jordan mandated, early on during the epidemic, mask wearing in public places and limited gatherings. As of 2022, Jordan also enforced the second COVID-19 vaccination for any public-related event or business.8
While children and adults can be affected by COVID-19, reports suggested that children typically have less severe COVID-19 illness with fewer cases, and deaths, as compared to adults (children below 14 years were 8.1% of global cases and 0.2% of global deaths).9 Yet, serious complications following COVID-19 infection have been observed among children, such as multisystem inflammatory syndrome (MIS-C).7 Children, as well, are an influential group for disease transmission within community settings.2–4 Furthermore, children are considered a major source for transmitting the disease in the community, which would jeopardize successful control.7
Vaccine hesitancy (VH), seems to still be a growing global challenge that might affect the effectiveness of vaccination programs.10 In Western cultures, even before the official declaration of COVID-19 vaccine use among children, caregivers’ intentions toward vaccination, once available, were reported at 65%,11 and the majority of parents reported to “definitely accept” or to be “unsure but leaning towards accepting a COVID-19 vaccine” for their children.12 Novelty and rapid vaccine development were the main reasons behind caregivers’ refusal to vaccinate children.11,12 More recent studies reported relatively positive attitude towards children vaccination against COVID-19 with an overall VH being ranging between 33%13 and 21%.14 In a systematic review, which included 17 studies and 45,783 parents, the overall proportion of parents who intended to vaccinate their children against COVID-19 was 56.8%.15 The main predictors of parental intentions were male gender, older age of parents and children, higher socio-economic status, white race, positive attitudes toward vaccination, higher levels of knowledge, and higher levels of perceived threat from COVID-19.15 A low rate of VH in Jordan, among adults, was reported as “alarming” with a low level reported for vaccinating children as only 20.1% of participants reporting to “agreed/strongly agreed” to vaccinate their children against COVID-19. As well, participants reported more COVID-19 acceptance for the elderly than themselves than for their children. As well, COVID-19 vaccine acceptance rate significantly differed by socio-demographic characteristics, COVID-19 risk perception, and perceived benefits and clinical barriers of the COVID-19 vaccine.16
With a proportion of more than 30%,17 children in Jordan are considered a target group for effective immunization programs. Providing COVID-19 vaccination for this influential age group is a promising step in combating the spread of COVID-19. Still, the decision to vaccinate children (above 12 years) belongs to their parents as a signed consent is needed to administer such. This allocates parents as key element in a successful vaccination campaign as children’s vaccination will be largely influenced by parents’ attitudes and consequently intention to consider the vaccine.18 Understanding such attitudes and intentions are then an urgent need to bridge this knowledge gap and ensure effective vaccine interventions are properly tailored and fine-tuned for the Jordanian population. This is especially true as VH is different between cultures and may be shaped by multiple factors that are then critical in shaping parents’ attitude towards vaccinating their children against COVID-19.19–21 The aim of this study is to investigate the prevalence and determinants of parents’ VH towards vaccinating their children against COVID-19.
Methods
Study Design and Sampling
This is a cross-sectional study that used a self-administered online questionnaire as a framework for data collection. The online questionnaire was administered via Google Forms and was distributed via public Facebook pages of parents’ groups for rapid subject recruitment. Subjects were parents of children between 5 and 12 years old, who agreed to participate in the study. The invitation link emphasized the voluntary participation, inclusion criteria (having a at least one child with the specified age group) and that the survey is not seeking any personal identifiers.
Survey Instruments
The survey was developed by the study researchers in Arabic language to investigate parents’ perceptions and attitude towards COVID-19 vaccination for their children. The questionnaire was pilot-tested among 10 parents, who did not participate in the actual survey, to assess clarity and readability. Based on participants’ comments, the survey was finalized. Data collection was conducted between October and November 2021.
Data collected included participants’ background characteristics (gender, age, locality, educational level, employment status and monthly personal income), age of children, parental history of COVID-19 vaccination, medical history, childhood vaccination record, family history of COVID-19, general attitudes and trust toward COVID-19 vaccines (safety and efficacy), SARS-CoV-2, infection and vaccine, risk perception, factors affecting decision to vaccinate children, and parental willingness to offer the vaccine to their children. Response to parent’s willingness to vaccinate his/her child question was assessed on a 5-point Likert scale (strongly agree, agree, neutral, disagree, and strongly disagree) and collapsed into yes/no accordingly.
The main outcome of the study was parental willingness to vaccinate their children with COVID-19 vaccine. Predictor variables such as SARS-CoV-2, infection and vaccine, risk perception, retrieval of COVID-19 vaccine information, trust in COVID-19 vaccine information, and confidence of effectiveness or safety of COVID-19 vaccines were explored against parental willingness.
Statistical Analysis
SPSS software application was used to analyze the data. Categorical variables were presented using numbers and percentages. Distribution of parental willingness by independent variables was assessed using Pearson’s χ2-test, except for cells with expected values <5. Cells with expected values <5 were assessed using Fisher’s exact test. Alpha level was set at 0.05 for all statistical associations.
Ethical Consideration
Participants invited to complete the questionnaire were consented online, assured no personal data collected, and that participation was voluntary. The conduct of this study complies with the Declaration of Helsinki. This study was approved by the Ethical Committee of Al-Balqa Applied University (26.3.1.206).
Results
Participants Background Characteristics
A total of 564 parents completed the questionnaire. Of which, the majority were mothers (82.8%), 30 years of age or older (85.3%), and in the higher education category (bachelor’s degrees or higher (75.9%)). Respondents were almost equally distributed by income level and one quarter reported lack of health insurance coverage for their children. About two-thirds of participants reported having more than 2 children and about one-fifth (20.9%) reported having children with chronic illnesses. As for COVID-19 vaccination, 83.9% of respondents self-reported COVID-19 vaccination (Table 1).
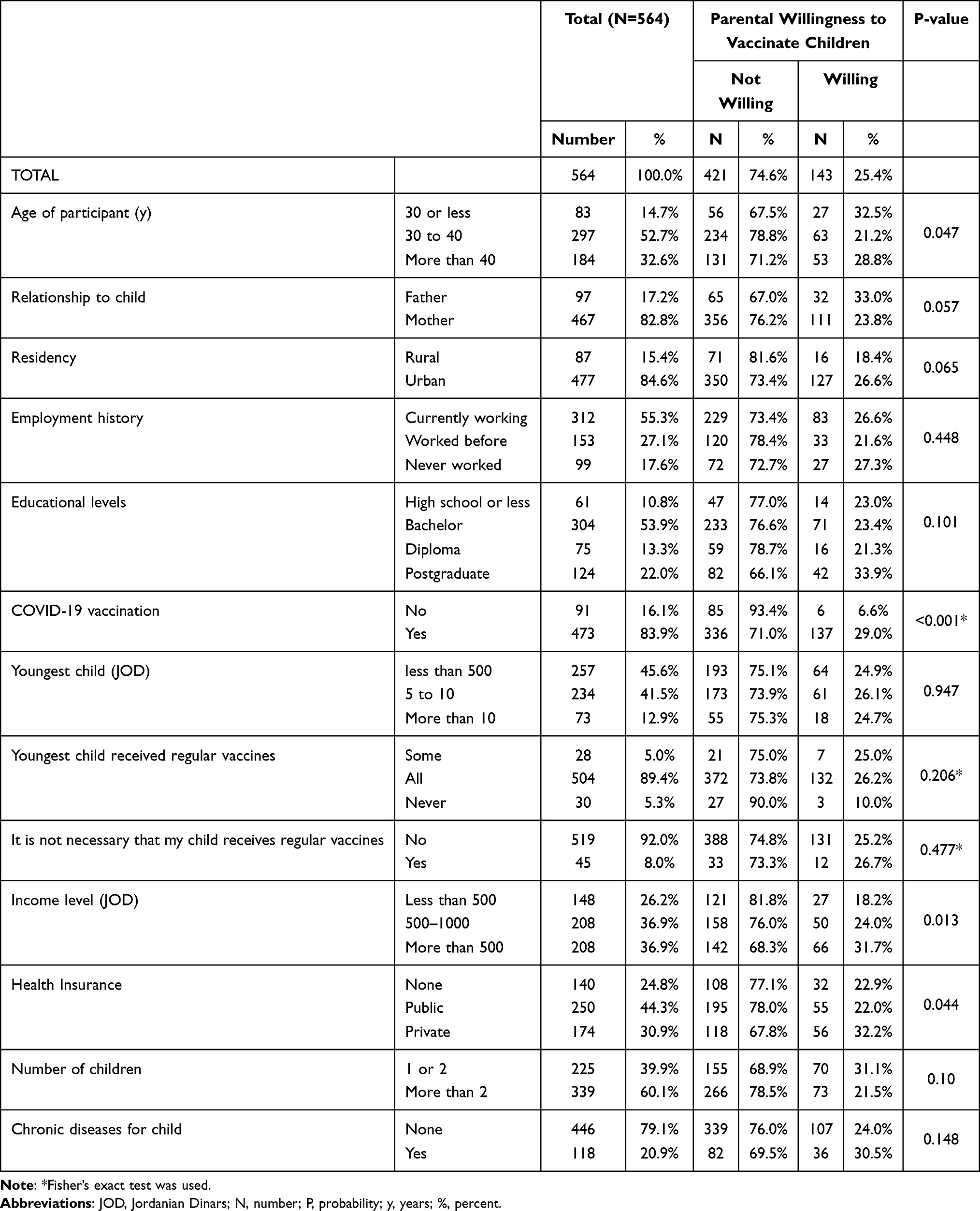 |
Table 1 Distribution of Study Participants by Background Characteristics and Willingness to Vaccinate |
Willingness Estimates
While 25.4% of parents self-reported willingness to vaccinate their 5–12 years old children against SARS-CoV-2, 74.6% reported being not willing (62.4%) or undecided (12.2%). Distribution of study participants by willingness to vaccinate and background characteristics (Table 1) showed significant differences by age of respondents, income levels, and health insurance coverage. Among parents who were less than 30 years old, the percent of parental willingness was 32.5% compared to 21.2% and 28.8% among those in the 30–40 years and older than 40 years’ groups, respectively. As income level increases, parental willingness to vaccinate seems to also increase; 18.2% among less than JOD500 (≈ $700), 24.0% among JOD500 to JOD1000 and 31.7% among >JOD1000. Respondents with private health insurance (32.2%) seems to have higher parental willingness to vaccinate their children compared to those with public insurance (22.0%) and no insurance (22.9%) (Table 1).
Among respondents who reported not receiving COVID-19 vaccine, 93.4% were unwilling to vaccinate their children, whereas 6.6% were willing to do so. While among those who reported to be vaccinated only 29.0% were willing to vaccinate their children and 71.0% were not willing. Significant differences between parental willingness and trusting healthcare providers, as a source of COVID-19 infection and vaccination information, as well as confidence/trust in vaccines if recommended by pediatricians, were detected. The majority of parents who reported willingness to vaccinate their children agreed/strongly agreed with the statements regarding trusting healthcare providers, as a source of COVID-19 information, and confidence in the vaccine, if recommended by a pediatrician, while those who were unwilling to vaccinate were more likely to disagree/strongly disagree with such statements (Table 2).
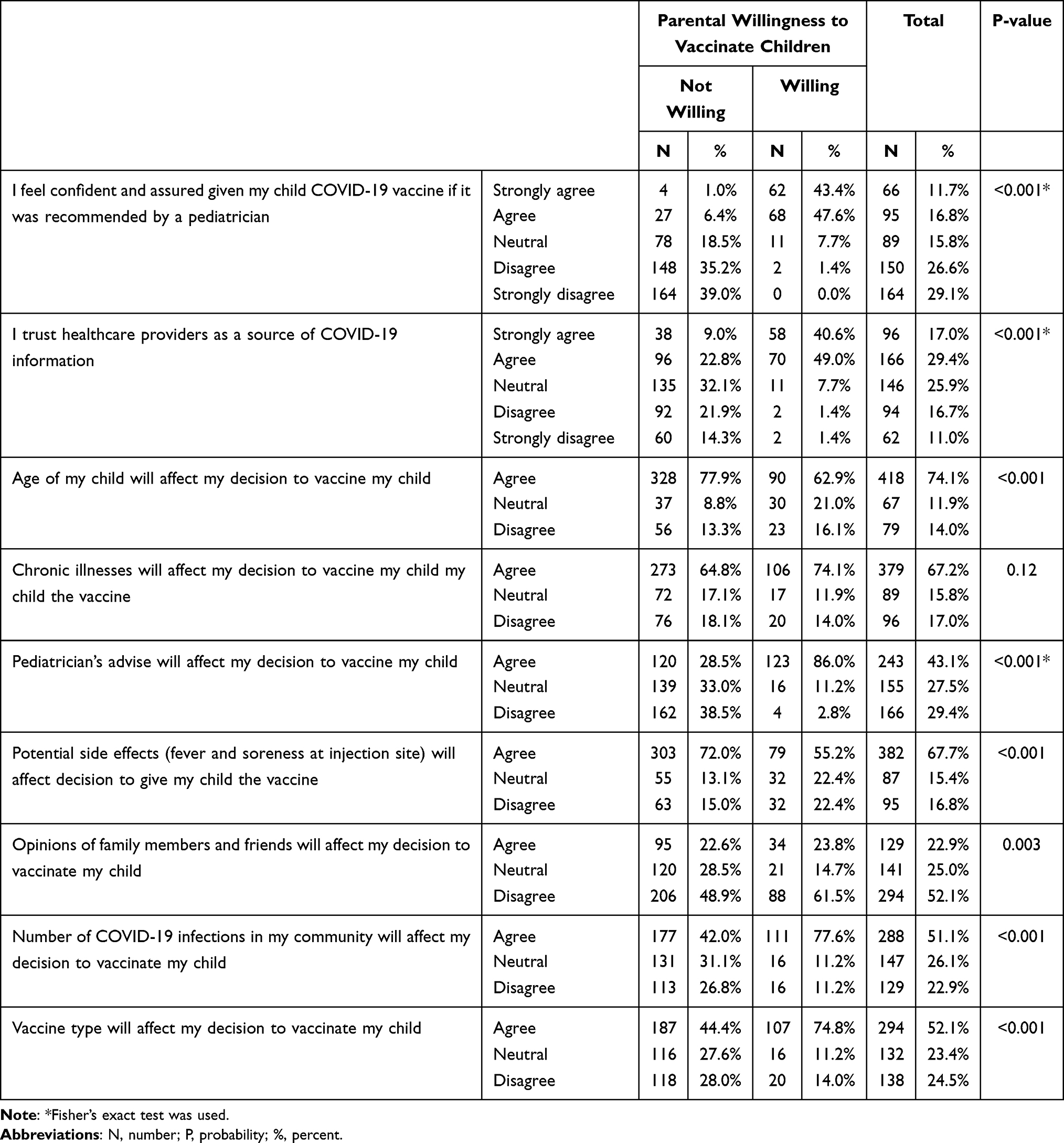 |
Table 2 Distribution of Study Participants by Factors Affecting Decision to Vaccinate and Parental Willingness |
COVID-19 Risk Perception
COVID-19 risk perception seems to have significant effects on parental willingness to vaccinate their children. About 80% of parents who are willing to vaccinate their children reported that “the likelihood that their family and friends catching COVID-19 infection in the next 6 months” as high or extremely high, compares to 66.3% among their unwilling counterparts. As a response to the questions regarding children’s susceptibility and likelihood of catching SARS-CoV-2 infection; 93.7% of willing parents answered “yes they are susceptible” and 46.9% reported that the likelihood of infection is high or extremely high. In comparison, 75.5% of unwilling counterparts responded “yes” to susceptibility question and only one quarter to the likelihood of infection as high or extremely high. Higher percentage (58.1%) of willing parents reported that their children “will suffer from serious health problems if infected with SARS-CoV-2” compared to unwilling parents (42.5%) (Table 3).
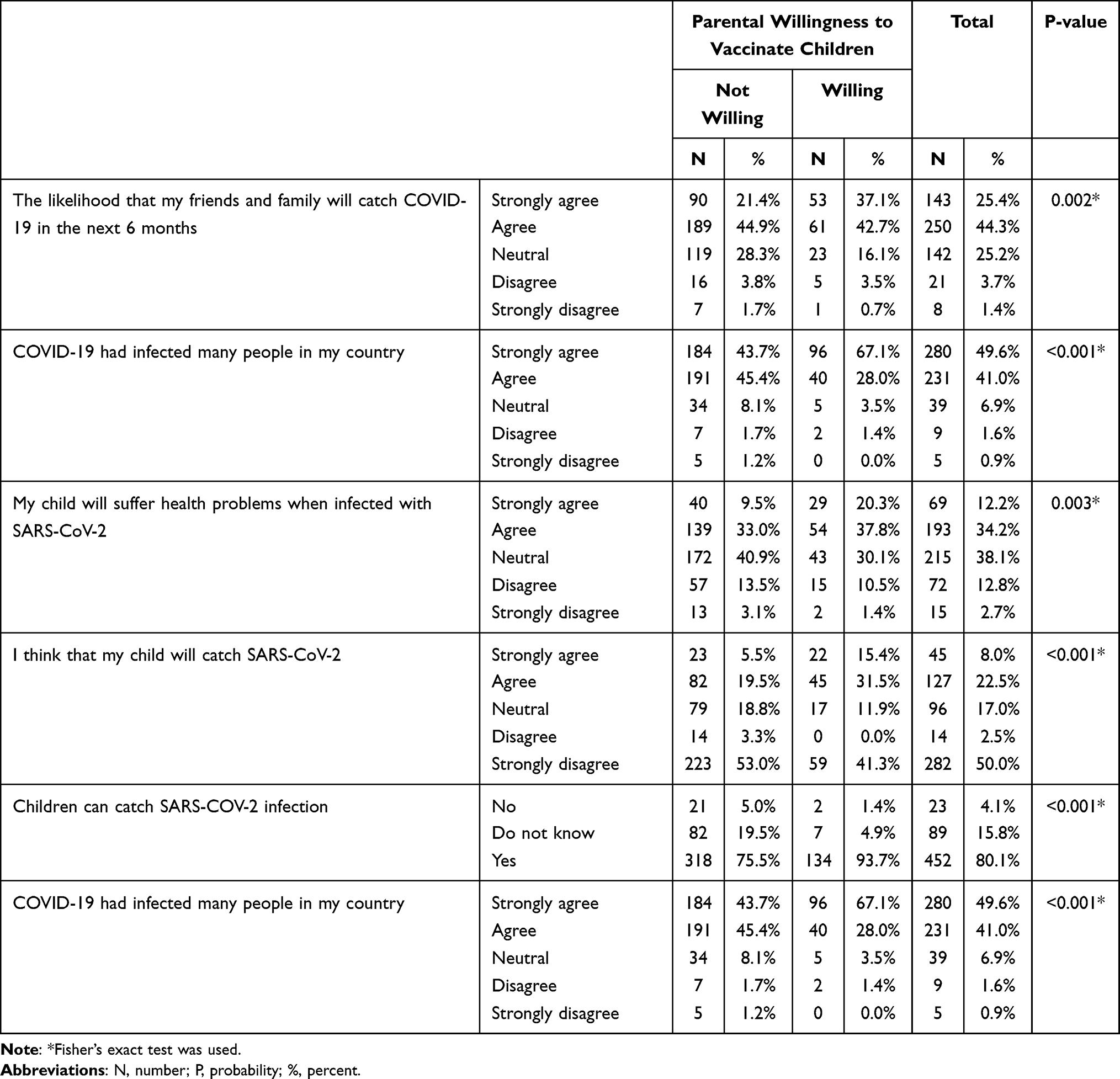 |
Table 3 Distribution of Study Participants by COVID-19 Risk Perception and Parental Willingness |
COVID-19 Vaccine Risk Perception
Regarding the parentals’ perceived risk of COVID-19 vaccine, significant differences were detected by parental willingness. Those who reported to be unwilling to vaccinate their children were more likely to have concerns regarding the safety of the vaccine, including potential side effects, long-term health problems, harmful substances it contains (Table 4). On the other hand, willing respondents were more likely to strongly agree/agree with statements that the vaccine “is effective against SARS-CoV-2 infection” and “is the best approach to reduce chances of infection” (Table 5).
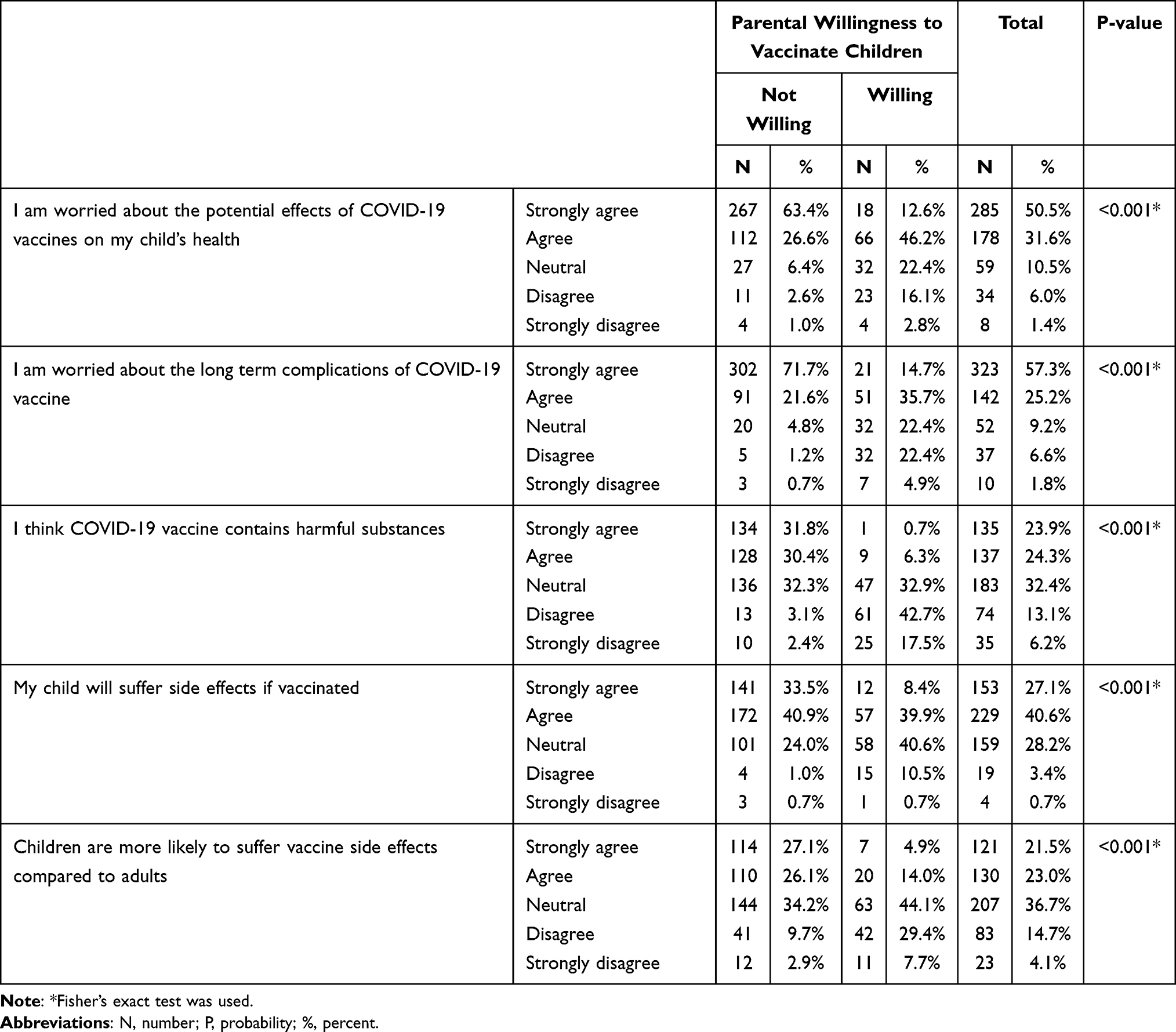 |
Table 4 Distribution of Study Participants by COVID-19 Vaccine Risk Perception and Parental Willingness |
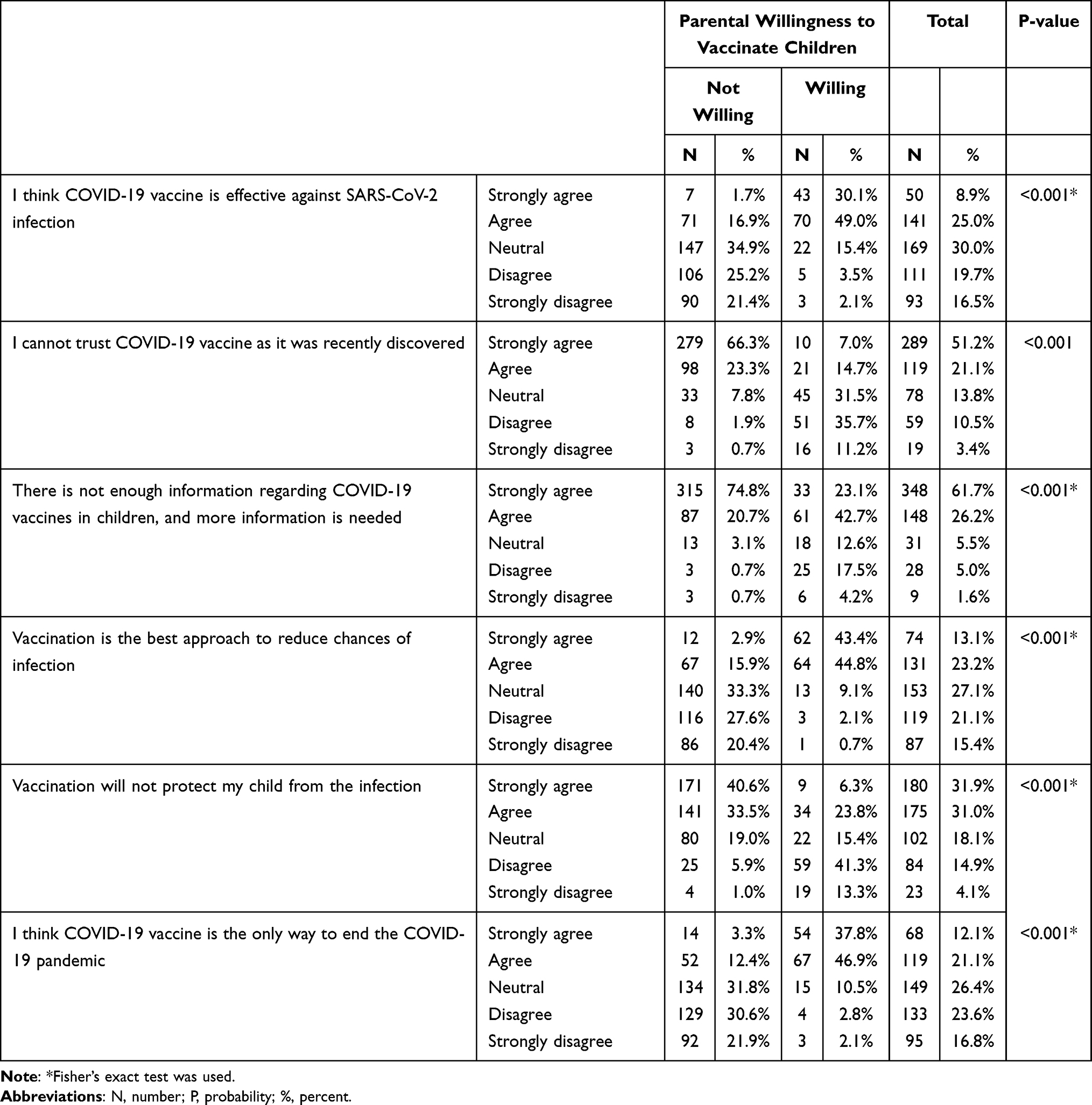 |
Table 5 Distribution of Study Participants by COVID-19 Vaccine Trust and Parental Willingness |
COVID-19 Vaccine Trust
Lack of sufficient information about the vaccine and its expedited release are other factors that significantly affected parental willingness to vaccinate their children (p<0.001 and p<0.001, respectively). Compared to those who reported to be willing to vaccinate their children, those who reported to be unwilling to vaccinate were more likely to strongly agreed or agreed with the statements that they do not “trust COVID-19 vaccine as it was recently discovered” and that vaccine information in children is not “enough” and “more information is needed” (Table 5).
Factors Affecting Decision to Vaccinate
Significant differences were detected between parental willingness and factors affecting decision to vaccinate. The majority of participants who reported willingness “agreed” with the statements that pediatrics’ recommendation (86%), number COVID-19 infection in the community (77.6%), and type of vaccine (74.8%), affect their decisions to vaccinate their children. On the other hand, child’s age (77.9%), and potential vaccine side effects (72.0%), were reported by the majority of unwilling participants to affect their decision to vaccinate their children. Two-thirds of willing parents and less than one half of unwilling ones did not agree that “opinions of family members and friends” affect decisions to vaccinate. Of interest, 74.1% of willing and 64.8% of unwilling agreed that chronic diseases are a major factor affecting participants’ decision to vaccinate (Table 2).
Discussion
In order to reduce COVID-19 pandemic burden and mitigate its spread, herd immunity should be achieved ensuring more than 70% of the population, including children,22 are immune against the SARS-CoV-2 infection. As observed with other respiratory infections, effective paediatric vaccination may contribute to lower infections in adults and will help reduce infection spread in the community.23 Still, vaccine hesitancy, including parental vaccines refusal, is a serious global public health problem. In 2019, the World Health Organization (WHO) identified vaccine hesitancy as one of the top 10 global health threats given its association with outbreaks and deaths from vaccine-preventable diseases.24–26 After that, some COVID-19 vaccines have been declared safe and effective against COVID-19 among children.27 In Jordan, about 200,000 children between 12 and 17 years have received the COVID-19 vaccine as of March 2022. This represents 4.5% of the total 4.4 million vaccinated In Jordan. The national epidemiologic committee recommended to begin vaccination among children between 5 and 12 years. However, Jordan Ministry of Health has not yet administered COVID-19 vaccine to children of this age group. This study explored parental willingness towards administering COVID-19 vaccine for their children 5 to 12 years old in Jordan. Our results indicated that only one in every four parents showed willingness to vaccinate their children against COVID-19 suggesting generally low acceptance of childhood COVID-19 vaccination. This low parental willingness level calls for immediate public health actions to ensure such epidemiologically influential age group is immune against COVID-19 infection as well as the spread of COVID-19 in the community. Without proper immunity among this age group, school children will be a corner stone in the community spread of COVID-19 new variants and a risk group for disseminating SARS-CoV-2 infection to the older age groups, another epidemiologically influential group, including grandparents.
Parental willingness towards vaccinating their 5 to 12 years old children against COVID-19 in Jordan appears to be less positive than that reported in other countries. About 60% of parents in Italy were inclined to vaccinate their children and 29.6% were “considering the opportunity”.28 A high rate of parental acceptance was also reported in China (72.6%).29 In England, most parents showed acceptance of COVID-19 vaccination for their children (definitely 48.2%, unsure but leaning towards yes 40.9%).12 Similar results were also observed among parents of children under 12 years of age in Canada and Israel.30 Saudi Arabia, a country with a borderline with Jordan, reported relatively higher rate of parental acceptance with 53.7% of the parents reported willingness to vaccinate their children below 18 years old31 in one study, and 46.1% willingness to vaccinate their children aged between 5 and 12 years in another study.32 Differences between Jordan and Saudi Arabia may reflect methodological approaches and population structure. The study conducted in Saudi Arabia32 mainly focused on one urban setting, which reflects a diverse population of migrants from almost all over the world as stated in the limitation of the study. As well, the economic power in Saudi Arabia, and the socio-economic characteristics of the population, are different, higher, that that in Jordan. This could explain the observed differences in parental willingness to vaccinate their children. As well, it provides insight that differences in parental willingness levels are not universal and need to be investigated in different population structures.
The reported low level of parental willingness to vaccinate children calls for revisiting the risk communication strategies used to mitigate the spread of COVID-19 measures. Cultural attributes in this regard may also be further investigated to see how such differences could be justified in line with the global impact of the epidemic. Caution, however, should also be considered regarding the time of survey administration. During the early stages of the epidemic, also during early administration of the vaccine, the overall risk of COVID-19 may have been lower than that when Omicron and Delta variants were of greater concerns. Such factors could affect related willingness and hesitancy. Other factors that may help clarify global differences in parental vaccine hesitancy, or willingness, include cultural disparities, level of confidence in authorities, and perceived trustworthiness of healthcare providers when it comes to COVID-19 vaccination programs. Of importance, as well, is the political scheme observed in this epidemic and the way information, or misinformation, is being consumed and translated by parents of children. Shall healthcare providers be left alone to provide guidance to parents in this regard, one can expect that parental willingness to vaccinate their children be higher that this observed in the majority of countries.
Factors associated with higher parental willingness included younger age, higher income levels, and private health insurance coverage, but not educational levels. Considering that parents who are 30 years old or younger are probably those who have the financial means to be married with children suggests that higher social class is associated with higher parental willingness to vaccine their children in Jordan. This is supported by the fact that, in Jordan, education is an asset that has been part of a cultural wealth regardless of the social class. Reports from other countries showed that higher parental willingness rates were associated with older age. In Saudi Arabia, a wealthy Arab state, the highest willingness rate was among parents between 31 and 40 years old while in Latin America and Caribbean, parents between 35 and 54 years have higher intentions to vaccinate their children.31,33 In contrast, other studies reported conflicting results with higher educational achievements presented as a barrier or as a promoter of children vaccination.34,35 Regardless, participants’ socio-demographic characteristics play a crucial role in designing public health interventions to ensure successfully implemented vaccination interventions. Accordingly, country-specific variations in willingness should be considered as a key element in adopting interventions targeting school age children. A one-size-fits-all interventions may carry the risk of failure and more culturally appropriate interventions are then an imminent need. With such tailored interventions, which considers socio-demographic variations in parental willingness, one needs to identify high-risk groups that need immediate interventions. According to our results, low social class parents seem to be the most in need for immediate interventions.
Parental COVID-19 vaccination history seems to be a determinant factor in their willingness to vaccinate their children. With parents who did not receive COVID-19 vaccine being less willing to vaccinate their children, our results were in concordant with other reports from Korea, China and the United States.34,36,37 Parental hesitancy may then reflect not only on themselves but also on their children. Interventions targeting vaccine hesitancy should then focus not only on adults but also children. Accordingly, household-designed interventions may be needed to overcome the issues related to vaccine hesitancy regardless of age. This is critical as overcoming adults’ hesitancy may be needed as the first step in establishing good vaccination programs.
Safety of the vaccine was a major factor associated with parental vaccination refusal to vaccinate children. This has been identified in previous studies as a major concern for children’s COVID-19 vaccination.30,31,38,39 This factor also connects with lack of sufficient information regarding COVID-19 vaccines and their expedited release; factors that are reported in literature to significantly affect decision-making regarding children vaccination.31 On the other hand, COVID-19 risk perception seems to be a primary motivation for vaccination willingness as identified in our results, where an association was noted between vaccination willingness and perceived risk of SARS-Cov-2 infection. This is similar to prior reports of parental plan to vaccinate their child against COVID-19 and other infections, such as H1N1 pandemic.40–43 Overall, our results provide evidence of the major concerns that may define parental hesitancy and provide an insight on what exactly needs to be targeted. With proper information dissemination from family pediatrician, one can expect that perception of risk, along with correct medical information about vaccines, are targets for public health interventions. With proper tools, concerns related to lack of sufficient information and safety, amalgamated with risk evaluation and assessment, can of an added value during routine pediatric visits, and during follow-up calls with parents.
Parents who reported utilizing healthcare providers as sources of information about COVID-19 were more likely to report higher levels of willingness and lower hesitancy towards children vaccination.13 To this end, type of information to be shared with parents is also of critical importance in decision-making. Higher exposure to positive COVID-19 related information was associated with higher parental willingness to vaccinate their children while higher exposure to negative information was negatively associated with parental willingness.29 Directing parents, and local media, to more reliable and trusted sources of information may then improve parental awareness related to COVID-19, which may reflect on their willingness to vaccinate their children.
Overall, while this study reported low parental willingness to vaccine their children, it also identified key target elements to address such willingness levels and key target groups that can boost vaccination program effectiveness. Still, our study has its own limitations. First, Jordan, at the time of data collection, has not yet approved administering COVID-19 vaccines to 5–12 years old children. Accordingly, parental willingness to vaccinate their children may change once the vaccines are locally approved for this age group. Second, the questionnaire was based on online data collection utilizing a convenient sample. With such, results may not be generalizable. Still, some of our results are comparable to the global attitudes related to children’s vaccination. During COVID-19, research activities that involved direct contact with potential study participants were not feasible as it would have exposed them to infection risk. While social media utilization may not be universal in Jordan, it is believed that parents of younger children have good access to social media platforms. Accordingly, we do not believe this study have excluded a significant portion of the population and that it has produce a sample that is probably representative to parents of young children. Regardless of the limitations, our results call for qualitative assessment of attributes to parental willingness as it could further our understanding of this critical issue.
Conclusion
This study provides an insight about the low rate of parents’ acceptability of COVID-19 vaccine for their children in Jordan. Vaccine hesitancy appears to be driven by multiple factors. Perceived risk of COVID-19 and trust in healthcare system are of the most important predictors of parents’ attitude, and concerns about vaccine side effects is a major cause for parental refusal. Addressing these factors is of critical importance to guide the development of future campaigns that involve paediatricians and healthcare professionals to promote vaccine safety and enhance the rate of vaccine uptake.
Funding
Article publication charges were provided by a grant to M.Z. Allouh from the College of Medicine and Health Sciences at the United Arab Emirates University, Al Ain, UAE (Grant # G00003395).
Disclosure
All authors report no conflicts of interest in this work.
References
1. CDC. Coronavirus disease (COVID-19) situation reports. 2022. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports.
2. Auger KA, Shah SS, Richardson T, et al. Association between statewide school closure and COVID-19 incidence and mortality in the US. JAMA. 2020;324:859–870. doi:10.1001/jama.2020.14348
3. Calvani M, Cantiello G, Cavani M, et al. Reasons for SARS-CoV-2 infection in children and their role in the transmission of infection according to age: a case-control study. Ital J Pediatr. 2021;47:1–10. doi:10.1186/s13052-021-01141-1
4. Piraveenan M, Sawleshwarkar S, Walsh M, et al. Optimal governance and implementation of vaccination programmes to contain the COVID-19 pandemic. R Soc Open Sci. 2021;8(6):210429. doi:10.1098/rsos.210429
5. CDC. Different COVID-19 vaccines; 2022. Available from: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines.html.
6. WHO issues its first emergency use validation for a COVID-19 vaccine and emphasizes need for equitable global access; 2022. Available from: https://www.who.int/news/item/31-12-2020-who-issues-its-first-emergency-use-validation-for-a-covid-19-vaccine-and-emphasizes-need-for-equitable-global-access.
7. World Health Organisation. Jordan: WHO coronavirus disease (COVID-19) dashboard with vaccination data. World Health Organization; 2021:1–5. Available from: https://covid19.who.int/region/emro/country/jo.
8. Jordan Ministry of Health. Ministry of Health, the official website of the Jordanian Ministry of Health | Coronavirus disease. Jordan Ministry of Health; 2020. Available from: https://corona.moh.gov.jo/en.
9. World Health Organisation. COVID-19 disease in children and adolescents: scientific brief; 2021. Available from: https://www.who.int/publications/i/item/WHO-2019-nCoV-Sci_Brief-Children_and_adolescents-2021.1.
10. Butler R. Vaccine hesitancy: what it means and what we need to know in order to tackle it; 2022. Available from: https://www.who.int/immunization/research/forums_and_initiatives/1_RButler_VH_Threat_Child_Health_gvirf16.pdf.
11. Goldman RD, Yan TD, Seiler M, et al. Caregiver willingness to vaccinate their children against COVID-19: cross sectional survey. Vaccine. 2020;38:7668–7673. doi:10.1016/J.VACCINE.2020.09.084
12. Bell S, Clarke R, Mounier-Jack S, Walker JL, Paterson P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: a multi-methods study in England. Vaccine. 2020;38:7789–7798. doi:10.1016/j.vaccine.2020.10.027
13. Alfieri NL, Kusma JD, Heard-Garris N, et al. Parental COVID-19 vaccine hesitancy for children: vulnerability in an urban hotspot. BMC Public Health. 2021;21:1–9. doi:10.1186/S12889-021-11725-5/TABLES/2
14. Ruggiero KM, Wong J, Sweeney CF, et al. Parents’ intentions to vaccinate their children against COVID-19. J Pediatr Heal Care. 2021;35:509–517. doi:10.1016/J.PEDHC.2021.04.005
15. Galanis P, Vraka I, Siskou O, Konstantakopoulou O, Katsiroumpa A, Kaitelidou D. Willingness and influential factors of parents to vaccinate their children against the COVID-19: a systematic review and meta-analysis. medRxiv. 2021. doi:10.1101/2021.08.25.21262586
16. Al-Mistarehi AH, Kheirallah KA, Yassin A, et al. Determinants of the willingness of the general population to get vaccinated against COVID-19 in a developing country. Clin Exp Vaccine Res. 2021;10:171. doi:10.7774/CEVR.2021.10.2.171
17. Jordan Department of Statistics. Jordan in figure 2017 – department of statistics; 2022. Available from: http://dosweb.dos.gov.jo/products/jordan-in-figure2017/.
18. Zhou M, Zhao L, Kong N, Campy KS, Wang S, Qu S. Predicting behavioral intentions to children vaccination among Chinese parents: an extended TPB model. Hum Vaccines Immunother. 2018;14:2748–2754. doi:10.1080/21645515.2018.1496765
19. Willis DE, Andersen JA, Bryant-Moore K, et al. COVID-19 vaccine hesitancy: race/ethnicity, trust, and fear. Clin Transl Sci. 2021;14:2200–2207. doi:10.1111/cts.13077
20. Murphy J, Vallières F, Bentall RP, et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat Commun. 2021;12:1–15. doi:10.1038/s41467-020-20226-9
21. Danabal KGM, Magesh SS, Saravanan S, Gopichandran V. Attitude towards COVID 19 vaccines and vaccine hesitancy in urban and rural communities in Tamil Nadu, India – a community based survey. BMC Health Serv Res. 2021;21:1–10. doi:10.1186/s12913-021-07037-4
22. Kwok KO, Lai F, Wei WI, Wong SYS, Tang JWT. Herd immunity – estimating the level required to halt the COVID-19 epidemics in affected countries. J Infect. 2020;80:e32–e33. doi:10.1016/j.jinf.2020.03.027
23. Kao CM, Orenstein WA, Anderson EJ. The importance of advancing severe acute respiratory syndrome coronavirus 2 vaccines in children. Clin Infect Dis. 2021;72:515–518. doi:10.1093/cid/ciaa712
24. Ten threats to global health in 2019; 2022. Available from: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019.
25. Glanz JM, McClure DL, Magid DJ, Daley MF, France EK, Hambidge SJ. Parental refusal of varicella vaccination and the associated risk of varicella infection in children. Arch Pediatr Adolesc Med. 2010;164:66–70. doi:10.1001/archpediatrics.2009.244
26. Glanz JM, McClure DL, O’Leary ST, et al. Parental decline of pneumococcal vaccination and risk of pneumococcal related disease in children. Vaccine. 2011;29:994–999. doi:10.1016/j.vaccine.2010.11.085
27. CDC. CDC recommends pediatric COVID-19 vaccine for children 5 to 11 years | CDC online newsroom. CDC Press Release. 2021:8. Available from: https://www.cdc.gov/media/releases/2021/s1102-PediatricCOVID-19Vaccine.html.
28. Montalti M, Rallo F, Guaraldi F, et al. Would parents get their children vaccinated against sars-cov-2? Rate and predictors of vaccine hesitancy according to a survey over 5000 families from Bologna, Italy. Vaccines. 2021;9:366. doi:10.3390/vaccines9040366
29. Zhang KC, Fang Y, Cao H, et al. Parental acceptability of COVID-19 vaccination for children under the age of 18 years: cross-sectional online survey. JMIR Pediatr Parent. 2020;3:e24827. doi:10.2196/24827
30. Goldman RD, Krupik D, Ali S, et al. Caregiver willingness to vaccinate their children against COVID-19 after adult vaccine approval. Int J Environ Res Public Health. 2021;18:10224. doi:10.3390/ijerph181910224
31. Altulaihi BA, Alaboodi T, Alharbi KG, Alajmi MS, Alkanhal H, Alshehri A. Perception of parents towards COVID-19 vaccine for children in Saudi Population. Cureus. 2021;13. doi:10.7759/cureus.18342
32. Al-Khlaiwi T, Meo SA, Almousa HA, et al. National COVID-19 vaccine program and parent’s perception to vaccinate their children: a cross-sectional study. Vaccines. 2022;10(2):168. doi:10.3390/vaccines10020168
33. Urrunaga-Pastor D, Herrera-Añazco P, Uyen-Cateriano A, et al. Prevalence and factors associated with parents’ non-intention to vaccinate their children and adolescents against COVID-19 in Latin America and the Caribbean. Vaccines. 2021;9:1303. doi:10.3390/VACCINES9111303
34. Lu X, Wang J, Hu L, Li B, Lu Y. Association between adult vaccine hesitancy and parental acceptance of childhood covid-19 vaccines: a web-based survey in a northwestern region in China. Vaccines. 2021;9:1088. doi:10.3390/vaccines9101088
35. Larson HJ, Jarrett C, Eckersberger E, Smith DMD, Paterson P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: a systematic review of published literature, 2007–2012. Vaccine. 2014;32:2150–2159. doi:10.1016/j.vaccine.2014.01.081
36. Rane MS, Robertson MM, Westmoreland DA, Teasdale CA, Grov C, Nash D. Intention to vaccinate children against COVID-19 among vaccinated and unvaccinated US parents. JAMA Pediatr. 2021. doi:10.1001/jamapediatrics.2021.5153
37. Choi SH, Jo YH, Jo KJ, Park SE. Pediatric and parents’ attitudes towards COVID-19 vaccines and intention to vaccinate for children. J Korean Med Sci. 2021;36:1–12. doi:10.3346/jkms.2021.36.e227
38. Xu Y, Xu D, Luo L, et al. A cross-sectional survey on COVID-19 vaccine hesitancy among parents from Shandong vs. Zhejiang. Front Public Heal. 2021;9:1722. doi:10.3389/fpubh.2021.779720
39. Yigit M, Ozkaya-Parlakay A, Senel E. Evaluation of COVID-19 Vaccine Refusal in Parents. Pediatr Infect Dis J. 2021;40:E134–E136. doi:10.1097/INF.0000000000003042
40. Faasse K, Newby J. Public perceptions of COVID-19 in Australia: perceived risk, knowledge, health-protective behaviors, and vaccine intentions. Front Psychol. 2020;11. doi:10.3389/fpsyg.2020.551004
41. Setbon M, Raude J. Factors in vaccination intention against the pandemic influenza A/H1N1. Eur J Public Health. 2010;20:490–494. doi:10.1093/eurpub/ckq054
42. Rubin GJ, Potts HWW, Michie S. Likely uptake of swine and seasonal flu vaccines among healthcare workers. A cross-sectional analysis of UK telephone survey data. Vaccine. 2011;29:2421–2428. doi:10.1016/j.vaccine.2011.01.035
43. Bish A, Yardley L, Nicoll A, Michie S. Factors associated with uptake of vaccination against pandemic influenza: a systematic review. Vaccine. 2011;29:6472–6484. doi:10.1016/j.vaccine.2011.06.107
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.